")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Correlation Between Family Functioning and Health Beliefs in Patients with Stroke in Beijing, China
Authors Zhang L, Shu Y, Han C, Liu J
Received 27 October 2022
Accepted for publication 14 February 2023
Published 18 April 2023 Volume 2023:16 Pages 1067—1074
DOI https://doi.org/10.2147/JMDH.S394396
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Lingli Zhang,1,* YaoYa Shu,2,* Chunjie Han,3,* Jihong Liu1
1Department of Neurology, Beijing Luhe Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Department of Nursing, The Second Affiliated Hospital of Nanchang University, Nanchang, People’s Republic of China; 3Department of Rehabilitation Medicine, Beijing Luhe Hospital, Capital Medical University, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jihong Liu, Department of Neurology, Beijing Luhe Hospital, Capital Medical University, No. 82 of Xin Hua South Road, Tongzhou District, Beijing, 101149, People’s Republic of China, Tel +86 10-69543901-1041, Fax +86 10 69531069, Email [email protected]
Objective: To explore the relationship between family functioning and health beliefs in patients with stroke.
Methods: A total of 253 patients with stroke were selected from Beijing Luhe Hospital, Capital Medical University from May 2021 to November 2021. All patients were of Chinese nationality, and 240 valid questionnaires were obtained. The Family Assessment Device and Champion’s Health Belief Model Scale were used to collect patients’ family functioning and health beliefs information, and correlation analysis was used to analyse it.
Results: The total score for family functioning in patients with stroke was 130.5 (22). The highest mean score was 2.46 for behaviour control, and the lowest score was 2.00 for total function. The items were ranked from high to low in this order: behaviour control, emotional response, role, communication, emotional intervention, problem solving and total function. The total score of the patients’ health beliefs was 116 (33), The items were ranked from high to low in this order: were self-efficacy, health motivation, perceived benefit, susceptibility, severity and perceived impairment. The scores for family functioning were negatively correlated with the total scores for health beliefs (P < 0.05).
Discussion: Stroke can reduce the self-care ability of the patients and aggravate the burden of family care. This can lead to abnormal function roles for patients and their families, emotional reactions in patients with stroke and weaker levels of family functioning.
Conclusion: The health beliefs scores of patients with stroke were at the middle level, and family functioning was at the general level. There was a negative correlation between the family functioning score and the total score for health beliefs in patients with stroke.
Keywords: health belief, family function, stroke
Introduction
Stroke is the second leading cause of death in the world because of its high incidence, recurrence, disability and mortality.1 Due to the rapidly ageing population in China, in which unhealthy lifestyles are prevalent, the disease burden of stroke is expected to increase in the future.2 Another investigation shows that the recurrence rate of ischemic stroke in China is about 20% within 5 years, and the longer the hospitalisation duration of the patients due to recurrence, the worse the prognosis. The subsequent medical costs will also cause great economic pressure on families and society.3
Stroke is a behaviour-related disorder. A full understanding of the relevant factors affecting the health behaviours of patients with stroke and adopting effective interventions to encourage the establishment and maintenance of health-promoting behaviours may reduce the risk of stroke recurrence to some extent and improve the health statuses and outcomes of patients. The Health Belief Model (HBM) is a widely used theory of health behaviours.4 Many studies have confirmed the explanatory and predictive roles of beliefs in health-related behaviours in different populations.5,6 According to the HBM, the health behaviours of patients with stroke can be improved through interventions in their health beliefs. In this system, the external life backgrounds and intrinsic physiological states exert a comprehensive influence on the subjective cognition and beliefs of individuals, which govern human behaviour.7
According to the McMaster family functioning model theory, the factors that influence the physical and mental health and emotional changes of family members do not lie in the family type or characteristics of its internal structure, but in the process by which the family system achieves various functions.8 The family is the basic unit of social life and an important external factor in the development of an individual’s health and diseases. Studies have shown that behaviour patterns among family members are mutually influenced. Family functioning is not only directly related to an individual’s health behaviours,9,10 but it also indirectly affects the production of health behaviours through some intermediate variables.11,12 Therefore, family functioning, as an important life background of patients with stroke, needs further analysis and validation to determine whether health beliefs are affected. This study investigates the relationship between family functioning and health beliefs using cross-sectional questionnaires and provides evidence for improving health beliefs and behaviours in patients with stroke.
Materials and Methods
Subjects
This study uses a cross-sectional design. The convenience sampling method was used to select patients with stroke diagnosed from May 2021 to November 2021 in Beijing Luhe Hospital, Capital Medical University. The inclusion criteria were as follows: 1) the patient met the diagnostic criteria set by the ESC Council on Stroke/EAPCI/EBNI position paper in 2021 and was diagnosed with stroke using cranial computed tomography or magnetic resonance imaging;13 2) two or more months must have elapsed since the patient’s discharge from hospital after their stroke; 3) the patient could communicate with the researcher in words; 4) the patient knew and agreed to complete the survey and was willing to cooperate. The exclusion criteria were as follows: subarachnoid haemorrhage; severe respiratory failure; heart, liver or kidney dysfunction; malignant tumours; history of mental illness, mental illness or dementia; and living alone. This study obtained the informed consent of the patients and their families and was approved by the Ethics Approval Council of Beijing Luhe Hospital, Capital Medical University (approval number: 2022-LHKY-075-01).
Study Methodology
General Information Questionnaire
Data were collected from the stroke speciality outpatient department, and a questionnaire survey was conducted among the patients who had been followed up and re-examined in the outpatient department for two or more months after the first stroke. The questionnaire was filled out by the patients with the assistance of their family members. The contents of the general information questionnaire included the patients’ sex, age, education level, marital status, occupation, work, family average monthly income, family structure, main caregivers, family history, mode of payment for medical expenses, type of stroke, course of the disease, complicated chronic diseases and sequelae. A total of 253 questionnaires were distributed and 253 were recovered on-site, with a recovery rate of 100%. After eliminating 13 invalid questionnaires, such as incomplete forms and contradictions in the filled contents, 240 effective questionnaires were obtained, with an effective recovery rate of 94.86%.
Family Assessment Device
This scale was compiled by Miller et al14 in 1983 and included seven dimensions: problem solving, communication, roles, emotional responses, emotional intervention, behavioural control and total function. There are 60 items on this scale, and each item has four options: very like my home, like my home, not like my home and not like my home. A total of 34 items were scored in reverse, and the total score and the scores of each dimension were the sums of the corresponding items. The total score was between 60 and 240, and the higher the score, the worse the family functioning was. According to the total score, family functioning can be divided into favourable (60–120 points), general (121–180 points) and unfavourable (181–240 points). The results of the Family Assessment Device (FAD) scale showed that the reliability coefficient was 0.72–0.92, and the correlation coefficient was 0.4–0.6, suggesting that the scale has good reliability and validity. The Cronbach’s α coefficient of the scale was 0.916.
Champion’s Health Belief Model Scale
The scale was first designed by the Champion team in 1894, and this study adopted Peng Huijiao’s health belief scale for patients with stroke based on the original scale and the Chinese version.15 There were 35 items and 6 dimensions on the scale: susceptibility, severity, perceived benefit, perceived disability, health motivation and self-efficacy. The 5-point Likert scale was used as follows: “strongly disagree”, “disagree”, “did not think about it”, “agree” and “strongly agree”, counting 1–5 points. The total score on the scale is 35–175, and the higher the total score, the better the beliefs in healthy behaviours. The CVI was 0.80 and Cronbach’s α coefficient was 0.73–0.89. The Cronbach’s α coefficient of the scale was 0.894.
Statistical Analysis
Double data entry, logical error checking and checking with the Chinese version of Epidata 3.1. After data input, SPSS 22.0 were used for analysis. The frequency and constituent ratio (%) were used to describe the count data, and the chi-square test was used to compare the groups. The measurement data used the Kolmogorov–Smirnov normality test. The mean ± standard deviation ( ± s) was used to describe the data that conforms to a normal distribution, and the median and interquartile range M (IQR) were used to describe the non-normally distributed data. Spearman correlation analysis was used to analyse the correlation between family functioning and health beliefs. Moreover, P < 0.05 indicated a statistical significance.
± s) was used to describe the data that conforms to a normal distribution, and the median and interquartile range M (IQR) were used to describe the non-normally distributed data. Spearman correlation analysis was used to analyse the correlation between family functioning and health beliefs. Moreover, P < 0.05 indicated a statistical significance.
Results of the Study
General Demographic Characteristics of the Participants
A total of 240 patients with stroke were included in this study, and most of them were men (70.4%). The average age was 60.46 ± 11.04 years old, and elderly patients accounted for more than half of the participants (58.8%). In terms of the educational level, patients with junior middle school education accounted for the majority (46.3%). In terms of marriage and work, 81.3% of the patients were married, 15.8% were divorced or widowed, 35.4% were workers and 50% were retired. In terms of income, 36.3% earned 3001–5000 Yuan per person per month. 40% in terms of family structure. 72.5% of the patients had their spouse as their primary caregivers. In terms of disease data, 89.2% of the patients had an ischemic stroke, 59.6% had no family history of stroke, and in most of them (42.5%), the course of the disease was between two months and one year. Most of the patients (93.7%) had at least one other chronic disease. Only 6.3% of the patients had no other chronic disease, and none of the enrolled patients had a history of COVID-19 infection.
The Status Quo of Family Functioning and Health Beliefs
Family Functioning Score in Patients with Stroke
The total score of family functioning of patients with stroke in this study was 130.5 (22). The highest mean score was 2.46 for behaviour control, and the lowest score was 2.00 for total function. The family functioning level of 170 (70.8%) for patients with stroke was average (Table 1 and Figure 1).
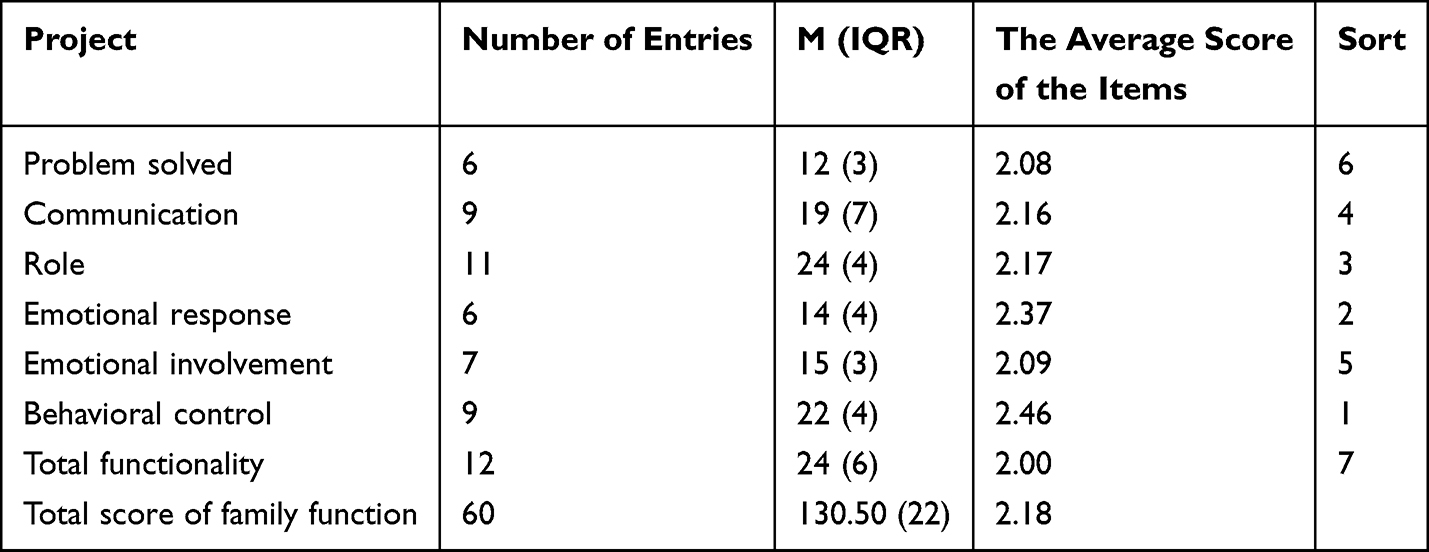 |
Table 1 Family Function Scores and Total Scores of Stroke Patients |
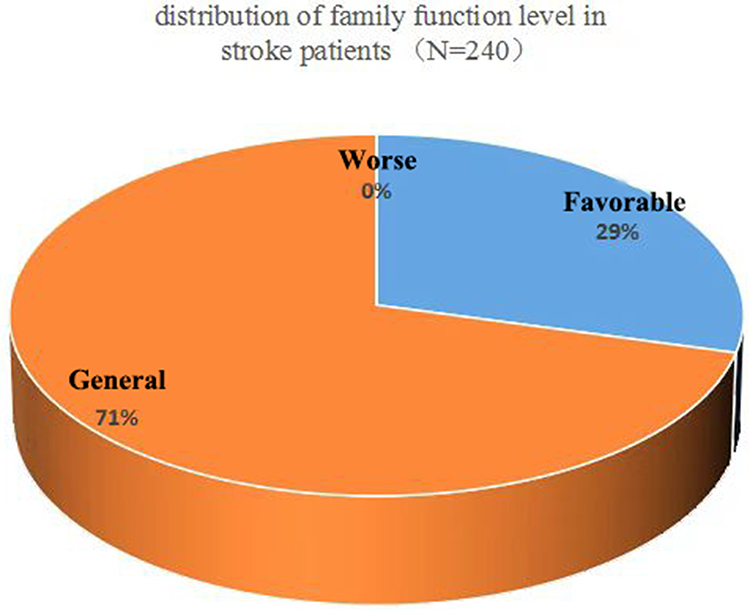 |
Figure 1 Distribution of family function level in stroke patients. |
Health Beliefs in Patients with Stroke
The total score of health beliefs in patients with stroke was 116 (33) and the average score of each dimension was as follows: 3.61 for self-efficacy, 3.48 for health motivation, 3.33 for perceived benefit, 3.07 for susceptibility, 3.06 for severity and 2.39 for perceived impairment (Table 2).
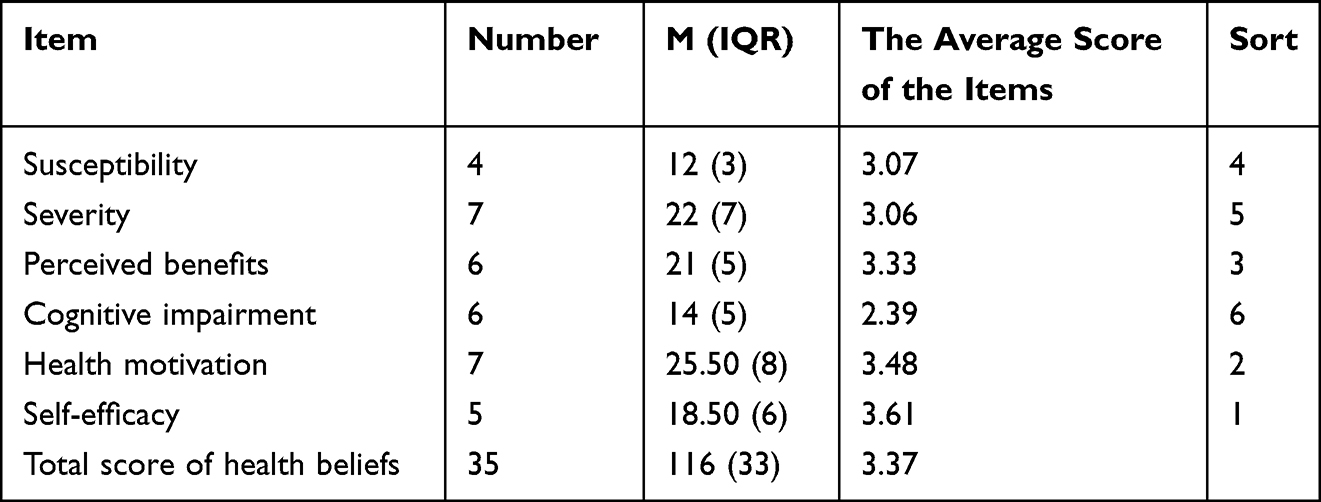 |
Table 2 The Scores of Each Dimension and Total Score of Health Belief in Stroke Patients |
Correlation Between Family Functioning and Health Beliefs in Patients with Stroke
The results showed that the family functioning score of patients with stroke was negatively correlated with the total score of health beliefs, severity, perceived benefit, health motivation and self-efficacy (0.209 < | r | < 0.454). There was a positive correlation between the family functioning and cognitive impairment (r = 0.234) (Table 3).
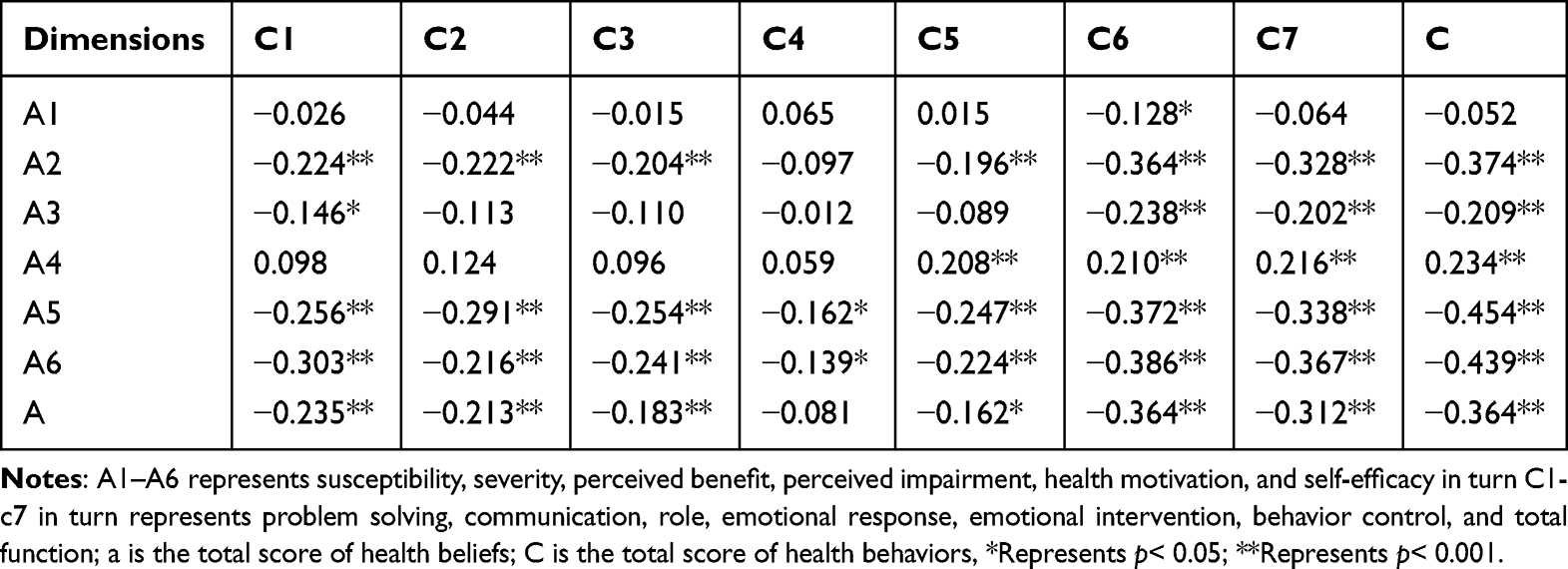 |
Table 3 The Relationship Between Family Function and Health Beliefs in Stroke Patients |
Discussion
Analysis of the General Demographic Data of Patients with Stroke
The average age of the patients was 60.46 ± 11.04 years. The number of male patients was about twice as many as that of female patients, which is consistent with the results of the epidemiological investigations of stroke populations in China and abroad.1,16 Most of the subjects had junior high school education, accounting for 61.7%, which was related to the fact that most of the patients with stroke in this study were middle-aged and elderly. Cultural education influenced by the patients’ backgrounds was generally not high. In terms of marital status, 81.3% of the patients had a spouse, and the majority (72.5%) of the spouses were their primary caregivers. This indicates that most of the patients in this study had a relatively intact family structure, which can play a certain role in family care. In this study, 89.2% of the patients had an ischemic stroke, and about 10% of them had a haemorrhagic stroke, which was consistent with the reported values of the epidemiological sampling survey of cerebrovascular diseases in China.17
Patients with stroke usually have a combination of multiple underlying diseases. This study found that 93.7% of patients with stroke had at least one other chronic disease, and the most common underlying diseases were diabetes mellitus and cardiovascular disease. A previous study showed that approximately 26% of haemorrhagic strokes and 33% of ischemic strokes were present in patients with diabetes, and the relative risk of stroke was increased by 1.8-fold in men with diabetes and 2.3-fold in women with diabetes.18 Coronary heart disease and peripheral artery disease are frequently present in patients with stroke and are positively associated with dementia risk after stroke,19,20 which was also further validated in this study. This suggests that when analysing the prognosis, quality of life and family support of patients with stroke, emphasis should be placed on the inclusion of studies and analyses of patients’ underlying diseases.
Analysis of the Family Functioning Status of Patients with Stroke
The results of this study showed that the total score of the family functioning of patients with stroke was 130.5 (22) points, which was at the general level (121–180 points), according to the score grade of the FAD scale. This is consistent with the findings of Hou Kunhua et al.21 A total of 29.2% of the patients were in a good state of family functioning, with a good rate lower than that of Yang Dan et al22 in the results of a survey of family functioning of patients with hand trauma (good rate: 38%). It is suggested that the occurrence of a stroke may have some influence on family functioning. Gawulayo et al23 have also demonstrated that stroke can have a significant negative effect on the normal functioning patterns of the family. In this study, higher scores in behavioural control, emotional responses and role dimensions indicated a poor level of family functioning in these three dimensions, which is similar to the findings of Li Na et al24 and Sun Xiaoyin et al.25 This may be because family members are more tolerant of the patient’s behaviours due to a busy schedule or because of the patient’s illness, which results in the lack of behaviour rules and restrictions in the family. In addition, due to the influence of traditional Chinese culture and thought, “emotional expression embarrassment” is common in Chinese families, and family members are not good at expressing their feelings directly and clearly. In addition, the disease may reduce the self-care ability of the patients and aggravate the burden of family care, resulting in abnormal role functioning for patients and family members. Therefore, the level of emotional response and family functioning in patients with stroke is weak.
Analysis of the Health Beliefs of Patients with Stroke
The results of this study showed that the total score of the health beliefs of patients with stroke was 116 (33), and the average score of the 5-point Likert was 3.36, which was in the middle level. This was similar to the findings of domestic scholars Cao Hui,26 Rong Yanqin and others.27 This study showed that most patients’ beliefs about stroke need to be improved. In this study, the average score of self-efficacy was 3.61, which indicated that most of the patients were confident in their ability to follow health behaviours and believed that they could persist in them. However, the scores of susceptibility and severity were low (3.07, 3.06), and the patients’ attitudes were mostly in the state of “unclear opinion”, which indicated that their perception of the risk of stroke was not clear. There was also a lack of awareness of the serious consequences that can result from this disease, which is largely the same as the results of previous studies in China28–30 and slightly different from those of foreign scholars Townend31 and Sullivan et al.32 First, because the condition of the patients in this study was generally mild, and they had a certain amount of cultural knowledge, they often had high confidence in their own recovery. But the knowledge about stroke was not enough, so the cognition was limited. On the other hand, perhaps because most Chinese people are willing to believe in fatalism, many patients said that life and death were fated, so they could instead calmly deal with and follow the treatment, but at the same time, this concept made it easy to make patients let their guard down. Research by Chang et al33 confirmed that the perception of stroke susceptibility and severity varied among ethnic groups; therefore, cultural factors may also be responsible for different findings in domestic and foreign studies. In addition, the perception impairment score was the lowest score in this study, but this dimension was scored in reverse. Therefore, most patients chose “Agree” on the 5-point Likert scale, which indicated that the patients thought that there were some difficulties and obstacles in the process of following health behaviours.
Correlation Analysis Between Family Functioning and Health Beliefs
Based on the findings, the level of family functioning in patients with stroke was positively correlated with health beliefs (r = 0.364, P < 0.01), which was consistent with the conclusions of Chen Gang et al.34 The family is the most basic unit of a person’s life, and family functions represent the ability to maintain the normal functioning of the family and meet the basic needs of its members.26 Good family functioning makes it easier for patients with stroke to get help and support in material and mental aspects. Family members can provide a stable rehabilitation environment for patients with stroke and enhance their confidence in facing this disease. This, in turn, improves patients’ health belief levels. However, if the family of the patient cannot carry out proper care and communication, solve problems and give the patient psychological support in time, their needs for care and support will not be satisfied. The illness may then result in a deficiency in self-care ability, which makes patients prone to depression.35 This affects the establishment of positive health beliefs. In addition, this study also found that family functioning levels were inversely associated with perceived impairment: better family functioning and less perceived impairment when patients engaged in health behaviours, which is similar to the findings of Wen et al.36 The level of the cognitive impairment was the lowest, which may be because good family functioning can provide backup support for patients in solving practical problems in the process of adopting health behaviours.
Limitations
However, this study also had some limitations. First, the sample source was limited, which may have resulted in bias in the survey results. The influence of health beliefs on health behaviours and the correlation between health behaviours and family functioning should be deeply analysed in future studies.
Conclusion
The family functioning of patients with stroke was poor in behaviour control, emotional responses and role dimensions. The level of health beliefs in patients with stroke should be improved, and family functioning can promote this. Health education should be strengthened to improve the family functioning of patients with stroke, which is beneficial to the promotion of health beliefs in patients with stroke. These findings provide useful insights for rehabilitation clinicians to develop interventions that are tailored to Chinese culture and cantered on home-based therapies to improve outcomes for stroke survivors.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of Beijing Luhe Hospital, Capital Medical University. All patients signed an informed consent form for inclusion in the study.
Disclosure
All of the authors had no any personal, financial, commercial, or academic conflicts of interest separately for this work.
References
1. Tsao CW, Aday AW, Almarzooq ZI, et al. Heart disease and stroke statistics-2022 update: a report from the American Heart Association. Circulation. 2022;145(8):e153–e639. doi:10.1161/CIR.0000000000001052
2. Collaborators GS. Global, regional, and national burden of stroke and its risk factors, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021;20(10):795–820. doi:10.1016/S1474-4422(21)00252-0
3. Liu J, Yang YL, Yan K, Zhu CR, Jiang M. Nomograms can predict the recurrence of the first ischemic stroke. Acta South Med Univ. 2022;42(01):130–136.
4. Janz NK, Becker MH. The health belief model. Health Educ Q. 1984;11(1):1–47. doi:10.1177/109019818401100101
5. Lin IP, Chung DT, Lee LY, Hsu HJ, Chen SC. Health belief, behavior intention, and health behaviors related to colorectal cancer screening in Taiwan. Int J Environ Res Public Health. 2020;17(12). doi:10.3390/ijerph17124246
6. Price J, Barrett-Bernstein M, Wurz A, Karvinen KH, Brunet J. Health beliefs and engagement in moderate-to-vigorous-intensity physical activity among cancer survivors: a cross-sectional study. Support Care Cancer. 2021;29(1):477–484. doi:10.1007/s00520-020-05515-9
7. Becker ME. The health belief model and personal health behavior. Health Educ Monogr. 1974;2(4). doi:10.1177/109019817400200407
8. Fang XY, Xu J, Sun L, Zhang JT. Family function: theory, influencing factors and its relationship with social adaptation of adolescents. Adv Psychol Sci. 2004;8(04):544–553.
9. Shu MC, Hong XC, Xu J, Yu YT, Lin SL, Lu ZQ. Effect of family function on self-management behavior and relapse of stroke patients. J Nurs. 2019;34(02):75–78.
10. Yu TT, Zhao RH, Xu BX, Li YL. Study on the relationship between family function and health behavior in patients with diabetes mellitus. Chin General Pract. 2018;21(19):2308–2312.
11. Luo D, Xu JJ, Cai X, et al. The effects of family functioning and resilience on self-management and glycaemic control among youth with type 1 diabetes. J Clin Nurs. 2019;28(23–24):4478–4487. doi:10.1111/jocn.15033
12. Jiang SS, Wan LH, Shen LP, Gao LL. The mediating effect of depression on family function and health behavior in stroke patients. Chin J Pract Nurs. 2014;30(26):39–43.
13. Nardai S, Lanzer P, Abelson M, et al. Interdisciplinary management of acute ischaemic stroke: current evidence training requirements for endovascular stroke treatment. Position paper from the ESC council on stroke and the European Association for Percutaneous Cardiovascular Interventions with the support of the European Board of Neurointervention. Eur Heart J. 2021;42(4):298–307. doi:10.1093/eurheartj/ehaa833
14. Miller IW, Epstein NB, Bishop DS, Keitner GI. The McMaster family assessment device. J Marital Fam Ther. 1985;11(4):345–356. doi:10.1111/j.1752-0606.1985.tb00028.x
15. Pang WK. Correlation between health beliefs and health behaviors in stroke patients master’s thesis. Guangzhou: National Sun Yat-sen University Nursing, 2010.
16. Gan Y, Yang TT, Liu JX, Hu S, Qiao Y. Research progress on the epidemic trend and influencing factors of stroke at home and abroad. Chin J Prev Vet Med. 2019;20(02):139–144.
17. Wang W, Jiang B, Sun H, et al. Prevalence, incidence, and mortality of stroke in china: results from a nationwide population-based survey of 480 687 adults. Circulation. 2017;135(8):759–771. doi:10.1161/CIRCULATIONAHA.116.025250
18. Bloomgarden Z, Chilton R. Diabetes and stroke: an important complication. J Diabetes. 2021;13(3):184–190. doi:10.1111/1753-0407.13142
19. Yang Z, Edwards D, Burgess S, Brayne C, Mant J. Association of prior atherosclerotic cardiovascular disease with dementia after stroke: a retrospective cohort study. J Alzheimers Dis. 2020;77(3):1157–1167. doi:10.3233/JAD-200536
20. Rezapour M, Asadi R, Marghoob B. Machine learning algorithms as new screening framework for recommendation of appropriate vascular access and stroke reduction. Hospital Res. 2021;10(3):5.
21. Hou KH. The status quo of family function and its influencing factors in patients with stroke master’s thesis. Shenyang: China Medical University; 2021.
22. Yang D, Niu ME, Lu Y. Analysis of family function status and its influencing factors in patients with moderate and severe hand injury. Contemp Nurse. 2019;26(12):23–26.
23. Gawulayo S, Erasmus CJ, Rhoda AJ. Family functioning and stroke: family members’ perspectives. Afr J Disabil. 2021;10:801. doi:10.4102/ajod.v10i0.801
24. Li N, Wu LM, Liu ZJ. The correlation between anxiety, depression and family function in elderly stroke patients with disability in Beijing-Tianjin-Hebei region. Chin J Gerontol. 2021;41(19):4401–4404.
25. Sun XY, Jiang MD, Jin LM. Analysis of family function status and its influencing factors in patients with stroke. General Nurs. 2020;18(12):1520–1523.
26. Cao H. Correlation between stroke outcomes, health beliefs and self-management behaviors in stroke patients master’s thesis. Yanji: Yanbian University; 2014.
27. Rong YQ. Health behavior status and influencing factors of stroke patients master’s thesis. Baoding: Hebei University; 2017.
28. Liu XX, Wan LY, Yan T, Wang C, Zhou ZY, Wang T. Investigation of health belief and health behavior in elderly patients with stroke. Hainan Med Sci. 2019;30(03):370–373.
29. Zhao CJ, Zou JQ, He PP, Xiao D, Peng H. Study on the correlation between health belief and functional exercise compliance in hospitalized stroke patients with hemiplegia. Integrated Chin Western Med Nurs. 2019;5(12):24–28.
30. Chen DD, Qiao TT, Zheng W. Investigation of health belief and analysis of influencing factors in hospitalized patients with stroke. Chin J Pract Neurol Dis. 2015;18(21):43–44.
31. Townend E, Tinson D, Kwan J, Sharpe M. Fear of recurrence and beliefs about preventing recurrence in persons who have suffered a stroke. J Psychosom Res. 2006;61(6):747–755. doi:10.1016/j.jpsychores.2006.09.006
32. Sullivan KA, White KM, Young RM, Chang A, Roos C, Scott C. Predictors of intention to exercise to reduce stroke risk among people at risk of stroke: an application of an extended Health Belief Model. Rehabil Psychol. 2008;53(4):505–512. doi:10.1037/a0013359
33. Chang E, Choi S, Kwon I, et al. Characterizing beliefs about stroke and walking for exercise among seniors from four racial/ethnic minority communities. J Cross Cult Gerontol. 2018;33(4):387–410. doi:10.1007/s10823-018-9356-6
34. Chen G, Cao YF, Wang YC, Liu B, Wang K. Correlation between family function and health beliefs in stroke patients. Chin J Mod Nurs. 2015;21(15):1760–1762.
35. Yang L, Zhao Q, Liu H, Zhu X, Wang K, Man J. Family functioning mediates the relationship between activities of daily living and poststroke depression. Nurs Res. 2021;70(1):51–57. doi:10.1097/NNR.0000000000000472
36. Wen LK, Parchman ML, Shepherd MD. Family support and diet barriers among older Hispanic adults with type 2 diabetes. Fam Med. 2004;36(6):423–430.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.