Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
Correlation Between Aggressive Behavior and Impulsive and Aggressive Personality Traits in Stable Patients with Schizophrenia
Authors Gao L, Yang R, Fan HZ, Wang LL, Zhao YL, Tan SP, Xiao CL, Zhou SJ ![]()
Received 11 January 2023
Accepted for publication 5 April 2023
Published 12 April 2023 Volume 2023:19 Pages 801—809
DOI https://doi.org/10.2147/NDT.S404176
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yu-Ping Ning
Lan Gao,1,* Rui Yang,2,* Hong-Zhen Fan,1 Lei-Lei Wang,1 Yan-Li Zhao,1 Shu-Ping Tan,1 Chun-Ling Xiao,1 Shuang-Jiang Zhou1
1Beijing HuiLongGuan Hospital, Peking University HuiLongGuan Clinical Medical School, Beijing, People’s Republic of China; 2Beijing Anding Hospital, Capital Medical University, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chun-Ling Xiao; Shuang-Jiang Zhou, Beijing HuiLongGuan Hospital, Peking University HuiLongGuan Clinical Medical School, Beijing, 10096, People’s Republic of China, Email [email protected]; [email protected]
Purpose: To explore the correlation between aggressive behavior and impulsive and aggressive personality traits in inpatients with schizophrenia.
Methods: In total, 367 inpatients with schizophrenia were divided into two groups: the aggressive group and the non-aggressive group. We assessed inpatients’ psychotic symptoms as well as their aggressive and impulsive personality traits using the Positive and Negative Symptom Scale, the Barratt Impulsiveness Scale, and the Buss-Perry Aggression Questionnaire.
Results: Compared with the scores of inpatients in the non-aggressive group, the total Buss-Perry Aggression Questionnaire, subscale, and Barratt Impulsiveness Scale behavioral factor scores in those in the aggressive group were higher (p < 0.05). The results of logistic regression analysis suggested that a high Positive and Negative Symptom Scale positive factor score (odds ratio = 1.07) and a high Buss-Perry Aggression Questionnaire physical aggression score (odds ratio = 1.02) were risk factors for aggressive behavior.
Conclusion: Hospitalized patients with schizophrenia with more severe positive symptoms and aggressive traits may be more prone to aggressive behavior.
Keywords: schizophrenia, aggressive behavior, impulsivity trait, aggressive trait, stable patients
Introduction
Compared to the general population, individuals with schizophrenia have a 49–68% increased risk of aggressive behavior.1 Aggressive behavior is one of the main reasons for admission of psychiatric inpatients and may manifest at any stage, from outpatient to hospitalization.2 The results of a meta-analysis showed that the incidence of aggressive behavior in inpatients with schizophrenia was 15.3–53.2%;3 such behavior may not only cause serious harm to the patient’s family, society, and medical staff,4 which have a severe impact on invested time and related costs,5 but may also greatly impact the opportunity for the patient’s social and vocational rehabilitation,1 leading to increased medical costs through frequent and prolonged hospitalization.6 Besides, the link between schizophrenia and murder has not only been established in the public mind and law, but has also been confirmed in epidemiological studies.7 Therefore, it is of great significance to study the aggressive behavior of schizophrenia patients.
To find ways to better prevent and cope with the aggression of patients with schizophrenia, an increasing number of studies worldwide have begun to focus on its risk factors. Previous studies have identified factors that may be associated with aggressive behavior in patients with schizophrenia involving aspects from biology to sociology and psychology. Multiple causes often coexist in a single aggressive event:8 for example, imaging studies have found that patients with aggressive behavior have abnormalities in brain structure and function.9,10 In terms of social demography, reported risk factors include youth,11 male sex,12 low education level,13 singleness, unemployment,14 etc. Comorbidities of substance abuse have been suggested to be strong predictors of aggressive behavior in patients with schizophrenia.15 A very large population based study carried out in Sweden16 concluded that despite schizophrenia was associated with an increased risk of violent crime, the association was attenuated by adjustment for substance abuse, suggesting a mediating effect. Most studies in psychiatric symptomatology have identified positive psychiatric symptoms as a risk factor for aggressive behavior.17 Meanwhile, studies have shown that poor growth history in childhood increases the risk of aggressive behavior in adults with mental disorders.18,19
Other studies have focused on personality traits that are prone to violence, including aggressive traits and impulsive traits. A personality trait is a relatively enduring mode of thought, emotion, and behavior, reflecting the tendency to react in a certain way in a particular situation.20 Aggression is a behavioral trait that is defined by behavior directed toward another individual with an intent to cause harm.21 Previous research has shown that aggressive trait are an important personality basis for individuals to engage in physical or verbal harm to others and themselves.22 Some prior researches have also found that individuals with an aggressive personality behave more violently,23 have more aggressive-related attitudes and cognitions,24 and consume more violence.25 The definition of impulsivity is an individual’s “tendency to make rapid, unplanned reactions to internal or external stimuli, without regard to the negative consequences of these reactions for oneself or others”26 Studies have shown that people with high levels of impulsivity are more likely to engage in risky behavior because they lack the self-control to avoid doing so.27 Impulsivity trait are believed to play a significant role in the emergence of aggressive behaviors.28 We hypothesize that aggressive and Impulsivity traits may also influence aggressive behavior in schizophrenia after controlling for confounding factors. However, previously studies on Impulsivity and aggressive personality traits in patients with schizophrenia with aggressive behaviors had inconsistent conclusions.2,21,29,30 In addition, researchers in the United States have pointed out racial differences in impulsive behavior.31 As differences in cultural background, living environment, and even religious belief may affect aggressive behavior,11 we need to conduct corresponding research on the personality traits of patients with schizophrenia with aggressive behaviors in China. To address this need, and the shortcomings of the previous research conducted in China, the current study used a large sample size and multi-stratified in-depth exploration was conducted to explore the influence of impulsivity and aggressive personality traits on aggressive behavior in stable patients with schizophrenia. Overall, our study was designed to provide a reference for the clinical prediction and management of aggressive behavior.
Materials and Methods
Participants
According to a previous study,28 the mean and standard error of the Buss–Perry Aggression Questionnaire (BPAQ) physical aggression subscale in aggressive behavior (40 cases) and non-aggressive behavior (34 cases) groups were 22.88 ± 1.40 and 15.88 ± 1.24, respectively. As calculated by the formula N = 2 × (Uα + Uβ)2 × б2/δ2, α = 0.05, β = 0.10, the minimum sample size required for a single group was 23.22, rounded up to 24 cases. At the same time, regression analysis generally requires a sample size to be at least five times the number of variables. The final number of participants enrolled in this study was 367, which met these sample size requirements.
The participants were consecutively recruited who were hospitalized at Beijing Huilongguan Hospital from July 2016 to July 2019. These patients were with schizophrenia according to the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition,32 ranged in age from 18–80 years, and had more than 5 years of formal education. Mental symptoms were required to be stable, with no acute exacerbation or medication adjustment within two months prior to the administration of the BPAQ scale. The exclusion criteria included some factors that might influence the aggressiveness of patients with schizophrenia or interfered with their ability to fill out the questionnaire correctly. These factors were history of head trauma or organic brain diseases; intellectual disability; serious recession or adverse drug reactions or uncooperativeness; severe depression, anxiety; alcohol or drug abuse or addiction; currently on clozapine or mood stabilizers, which can reduce aggressiveness among patients with schizophrenia;33 history of electroconvulsive therapy; serious physical diseases; auditory or visual perception disorders; and pregnancy or breastfeeding.
The 211 males (57.5%) and 156 females (43.5%) patients enrolled in this study were divided into aggressive and non-aggressive groups based on whether there was at least one obvious and recorded personal attack episode (including obvious wounding and self-injurious behavior) following diagnosis. Thus, there were 198 patients (54.0%) in the aggressive group and 169 patients (46.0%) in the non-aggressive group.
This cross-sectional study was reviewed and approved by the Ethics Committee of Beijing Huilongguan Hospital. All the patients and their primary caregivers were informed of the study protocol and submitted written informed consent to participate. This study was conducted in accordance with the Declaration of Helsinki.
Measures
Sociodemographic Factors
This included questions about age, sex, number of years of education, ethnicity, occupation, age at onset, course of disease, timing of recurrence, and family history.
Positive and Negative Symptom Scale (PANSS)
A general assessment of clinical symptoms was performed using the PANSS.34 There were 30 items in total, including the positive symptoms, negative symptoms, and general psychopathology subscales. Each item was graded from 1 (asymptomatic) to 7 (extremely severe), and the higher a person’s score, the more severe their symptoms. The main statistical analysis indexes included the positive symptom subscale, negative symptom subscale, general psychopathological subscale, and total scores.
Barratt Impulsiveness Scale-11th Revision (BIS-11)
The Barratt Impulsivity Scale is the most commonly used scale for assessing impulsivity,28 and the Chinese version has good reliability and validity.35 It comprises 30 items and three subscales (non-planning, motor impulsiveness, and cognitive impulsiveness), each rated on a scale of 1 to 5. However, the items in the non-planned and cognitive impulsivity subscales were all inversely related; that is, the corresponding score ranged from 5 to 1. The higher a person’s score is, the more impulsive they are. The BIS-11 has shown good internal consistency, with Cronbach’s α of the total scale and three subscales ranging from 0.77–0.89.
Buss-Perry Aggression Questionnaire (BPAQ)
The BPAQ is the most commonly used scale for assessing aggressive traits,28 and the Chinese version36 which has good reliability and validity contains 30 items and five subscales: physical aggression, verbal aggression, anger, hostility, and self-directed aggression. The score range of each item is 1 to 5, and the score of the scale is the sum of the scores of the items contained in it. The higher a person’s score, the more aggressive that person is. The internal consistency of the scale was good, with Cronbach’s α ranging from 0.60–0.89.
Clinical General Impression-Severity Scale (CGI-S)
CGI-S was used to evaluate the total severity of the current disease in patients with schizophrenia based on the clinical judgment of the doctor.37 Patients were assessed for disease severity on a scale from 1 (normal, disease-free) to 7 (very severe). The higher the score, the more severe the disease.
Insight and Treatment Attitude Questionnaire (ITAQ)
The ITAQ questionnaire consists of 11 items. It is mainly used to judge a patient’s understanding of the disease and attitude towards treatment.38 The scores range of ITAQ is 0 to 22. The higher a patient’s total score, the better their insight. Each item of the questionnaire is divided into three levels (0 = no knowledge, 1 = partial knowledge, 2 = full knowledge), with total scores categorized as follows: no self-awareness, 0; partial self-knowledge, 1–11; most self-knowledge, 12–21; and complete self-awareness, 22 points. Cronbach’s α for this test was 0.80, and the test-retest reliability was 0.869.
The above clinical symptoms were assessed by a uniformly trained group of ten attending clinicians. All physicians underwent rigorous training prior to participating in the evaluation and achieved good consistency (intraclass correlation coefficient = 0.85).
Statistical Analyses
EpiData 3.1 software was used for double data entry. Each statistical analysis in this study was conducted using Statistical Package for the Social Sciences (SPSS) software version 26.0 (IBM Corp.; Armonk, NY). Measurement data with a normal distribution was represented as (mean ± SD), and an independent-samples t-test was performed for inter-group comparison. Data with a non-normal distribution was represented as median (minimum and maximum), and a Mann–Whitney U-test was performed for inter-group comparison. Enumeration data were tested using a χ2 test (comparison of demographic characteristics). The test level α was 0.05. Logistic regression analysis was performed to assess the risk factors influencing aggressive behavior.
Results
Comparison of General Demographic Characteristics of Patients with or Without Aggressive Behavior
There were significant differences in age between the two groups, with the patients in the aggressive group being younger (p < 0.05) than those in the non-aggressive group. There were no significant differences in number of years of education, sex ratio, ethnic ratio, and occupational status between the aggressive and non-aggressive groups (p > 0.05; Table 1).
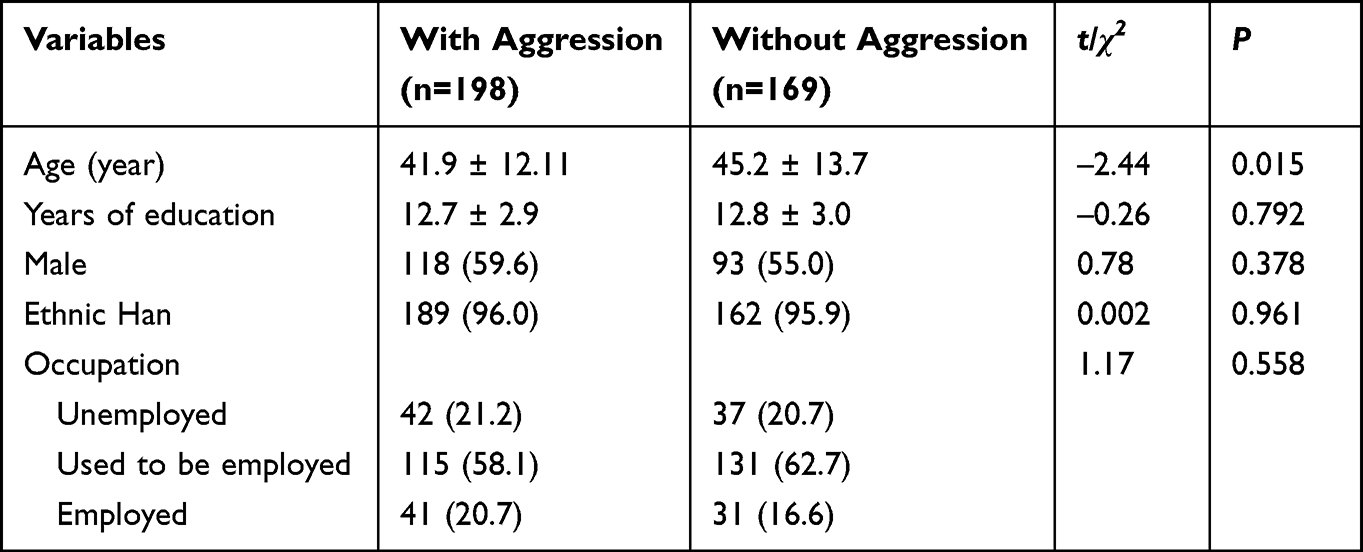 |
Table 1 Comparison of General Demographic Characteristics of Patients with or without Aggressive Behavior |
Comparison of Clinical Characteristics of Patients with or Without Aggressive Behavior
In terms of clinical characteristics, the disease severity, insight, total PANSS, positive factor, and general pathological factor scores of the patients in the aggressive group were higher than those of the patients in the non-aggressive group; the differences between the two groups were statistically significant (p < 0.01; Table 2 and Figure 1). The age of onset, course of disease, number of recurrences, negative factor score, family history, and schizophrenia classification did not differ between the groups (p > 0.05; Table 2).
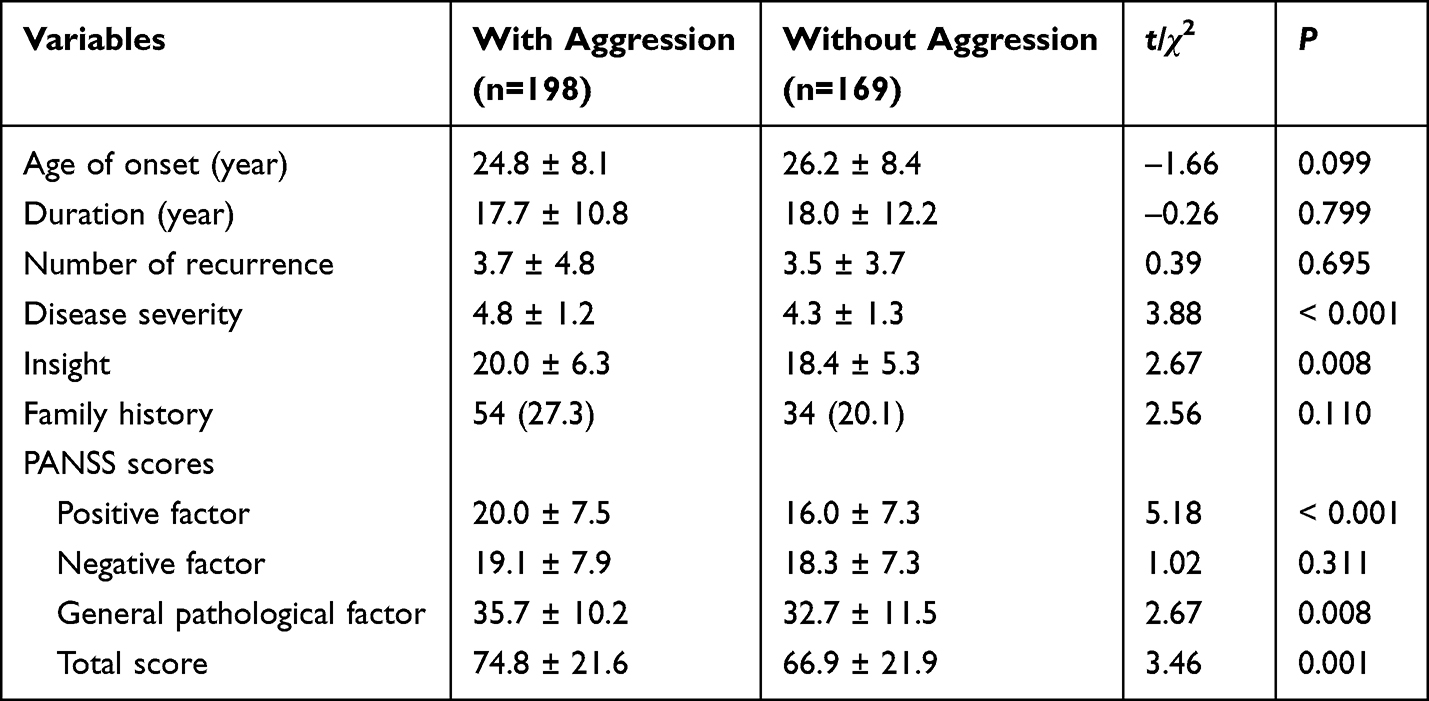 |
Table 2 Comparison of Clinical Characteristics of Patients with or without Aggressive Behavior |
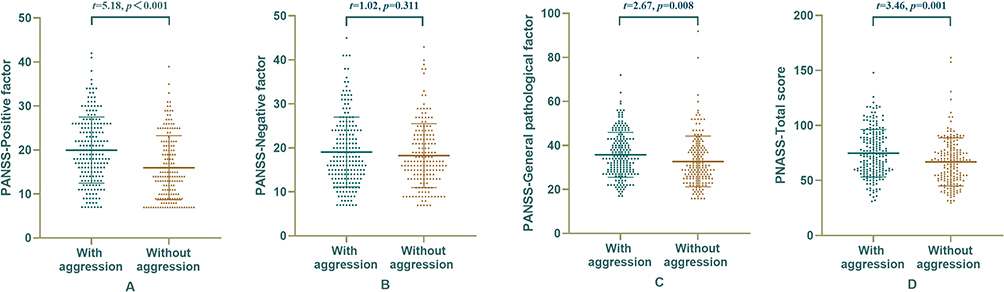 |
Figure 1 Comparison of PANSS score of patients with or without aggressive behavior. ((A) Comparison of PANSS positive factor; (B) Comparison of PANSS negative factor; (C) Comparison of general pathological factor; (D) Comparison of PANSS total score.). |
Comparison of Personality Traits of Patients with or Without Aggressive Behavior
Due to staff error, item 1 of the BIS-11 was not completely printed in the case report form, and the data for this item were missing for 110 patients recruited in the early stages of this study. Therefore, the non-planning factor and total BIS-11 scores were excluded from the statistical analyses. In terms of personality traits, only the behavioral factor score of the BIS-11 scale of the aggressive group was higher than that of the non-aggressive group, and the differences between the two groups were statistically significant (p < 0.05). The BPAQ total, physical aggression factor, verbal aggression factor, anger factor, hostility factor, and self-aggression factor scores of the aggressive group were remarkably higher than those of the non-aggressive group (p < 0.01; Figure 2).
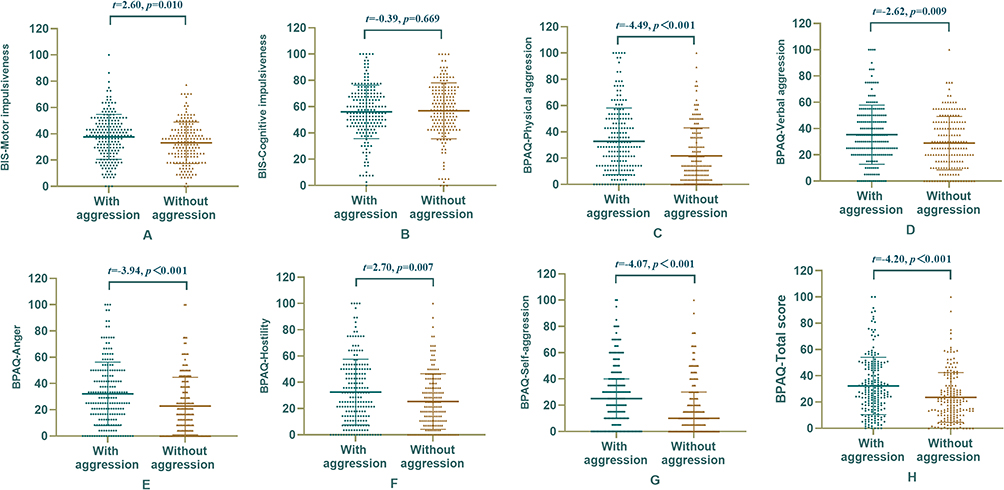 |
Figure 2 Comparison of BIS and BPAQ score of patients with or without aggressive behavior. ((A) Comparison of BIS motor impulsiveness; (B) Comparison of BIS cognitive impulsiveness; (C) Comparison of BPAQ physical aggression; (D) Comparison of BPAQ verbal aggression; (E) Comparison of BPAQ anger; (F) Comparison of BPAQ hostility; (G) Comparison of BPAQ self-aggression; (H) Comparison of BPAQ total score). |
Factors Influencing Aggressive Behavior in Patients with Schizophrenia
Variables with inter-group differences in Tables 1–3 (p < 0.1) were included in the regression equation, including age, disease severity, PANSS positive factor score, general pathological factor score, BIS-11 scale–behavior, BPAQ physical aggression score, verbal aggression factor score, anger factor score, hostility factor score, and self-aggression factor score. Age at onset and age were highly correlated and were not included in the model. The results showed that the PANSS positive factor score and BPAQ physical aggression score entered the equation, and the total accuracy of the classification was 62.0% (Table 3).
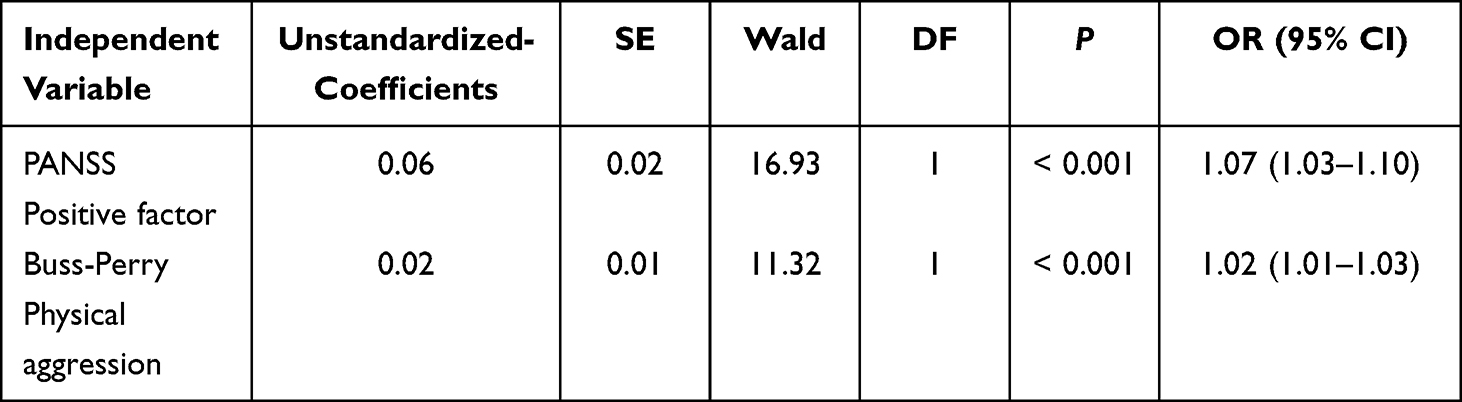 |
Table 3 Logistic Regression Analysis of Risk Factors for Aggressive Behavior in Patients |
Multistratified Exploration of Aggressive Behavior in Patients with Schizophrenia
The two groups were divided according to sex, number of years of education (high school and above, below high school), age of onset (25 years and above, 25 years), disease severity (PANSS ≤ 70, PANSS > 70), and family history (positive and negative) for the stratified statistical analysis, and there were no significant differences (p > 0.05).
Discussion
This study found that the age of the aggressive group was younger than that of the non-aggressive group, which is consistent with some of the previous research conducted in China.39 Likewise, in a sample of adults of 18–45 years, researchers found an inverse association between age and indicators of impulsive behavior.40 However, other research result3 have shown no correlation between the occurrence of aggressive behavior in patients with schizophrenia and age, sex, education level, occupational status, or other general demographic data. Similarly, in this study, no differences in general demographics other than age were found between the groups. The inconsistencies in the above conclusions may be related to regional and cultural differences, selection of included cases, and sample size.11,41
This study showed that the total PANSS, positive factors, general pathological factors, and disease severity scores were all higher in the aggressive group than in the non-aggressive group, which is similar to the result of research by van Dongen JD et al.42 Meanwhile, this study found that the group with aggressive behavior had better insight, which was contrary to the results of Witt et al,15 who found that violence is closely related to a lack of insight. However, our results were supported by Schandrin et al study,41 which speculated that insight may trigger the expression of an underlying hostile tendency, possibly via depression and self-stigmatization. Further logistic regression analysis showed that the PANSS positive factor score was a risk factor for aggressive behavior. This affirm that the more severe the positive symptoms of a patient with schizophrenia, the more likely they are to exhibit aggressive behavior. This aggressive behavior may be related to the patient’s cognitive deviation of reality, increased arousal, tendency to jump to conclusions43 and attribute hostile intentions to the actions of others, and use of aggressive behavior to try to maintain their “safety” or prevent risks.44,45 There are two different forms of aggression: predatory aggression and fear-induced aggression. Patients with schizophrenia with more positive symptoms and more severe illness are more prone to fear under the influence of hallucinations and delusions (especially delusions of victimization), so their aggressive behavior is usually fear-induced. Correspondingly, psychotic symptoms are less likely to be linked to planned/predatory aggression.46 Moreover, according to Hall’s proxemics theory, when other individuals infringe on our interpersonal space, feelings of discomfort and even fear may rise up.47 And studies have found that the personal space in these patients is often increased,48 so an ‘invasion’ could lead to an aggressive (fear-induced) behavior, especially if severe positive symptoms are predominant. Therefore, patients with schizophrenia should receive active treatment after admission to control positive symptoms as soon as possible, which may reduce the probability of them developing aggressive behavior.49
Impulsivity, as a personality trait, has always been a focus of researchers in the field and appears in the diagnostic criteria for some mental disorders. Excessive impulsivity has been considered to be a core feature of schizophrenia and psychotic disorders. Studies have shown that people with schizophrenia are more impulsive than healthy controls.50 Hoptman believed that impulsivity plays an important part in the aggressive behaviors of patients with severe psychosis.8 McDermott and Holoyda also showed that at least a plurality of inpatient aggression has an impulsive basis.46 Even in a recent study on a forensic sample, non-planning impulsiveness was found to be independent significant predictors of being in the homicidal group among patients with schizophrenia.21 The underlying pathways of psychosis-impulsiveness-violence nexus are likely attributable to Impaired executive functioning and disrupted top-down control in schizophrenia leading to inadequate behavioral control.51,52 Consistent with this, our study also showed that, compared to the non-aggressive group, the aggressive one had a higher BIS-11 behavior factor score, which manifested as thoughtless and reckless behavior, and a poor ability to control behaviors. However, regression analysis did not show that impulsivity was a risk factor for aggressive behavior, suggesting—as did the research of Sakanaka et al2 that the relationship between the two is not close. We used the BIS-11 to measure impulsivity in inpatients with schizophrenia, which does not evaluate emotional impulsivity; therefore, it is possible that we did not identify an impact of emotional impulsivity on aggression in these patients. Another possible reason is that our study participants were patients with schizophrenia without comorbid substance abuse, a factor known to be associated with increased impulsivity in schizophrenia.8 This also proves that, impulsivity is a multi-dimensional construct, not all impulsivity is the same. Future research is needed to refine our understanding of the relationship between aggressive behavior and impulsivity in schizophrenia.
Krakowski and Czobor found that individuals with aggressive behavior had more serious aggressive traits than those without aggressive behavior.28 There was also a consistent finding in this study, namely, the total score of the BPAQ and the scores of the five subscales in the aggressive group were distinctly higher than those in the non-aggressive group. Individuals with high-aggression traits are more likely to be induced to aggressive behavior, possibly because they have relatively larger aggression associative networks23 and more negative cognitive biases and poor cognitive attributions53 such as hostility; these can affect the individual’s assessment and decision-making abilities, preventing a thoughtful reassessment of the situation, which may lead to aggressive behavior. Further logistic regression analysis showed that the physical aggression score on the BPAQ was a risk factor for aggressive behavior in patients because this subscale was the most obvious report of real assault events, suggesting that patients with high scores on this subscale should pay more attention to early evaluation and the prevention of violent behavior.
There are several limitations to this study. This study used a self-rating scale, and the results may have been influenced by response bias. In addition, in this study, the influence of treatment drugs, hospitalization times, hospitalization time, and other factors on the aggressive behavior of patients with schizophrenia were not considered, and future research should address this.
Conclusion
In conclusion, our study has shown that hospitalized patients with schizophrenia with more severe positive symptoms and aggressive traits may be more prone to aggressive behavior. Further studies are required to elucidate on this.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Statement
Ethics Committee of Beijing HuiLongGuan Hospital approved the study. Signed informed consent forms were obtained from all participants. The study was conducted in accordance with the principles outlined in the Declaration of Helsinki.
Acknowledgment
We thank all of subjects who participated in this study. We would like to thank Editage (www.editage.cn) for English language editing.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. Chun-Ling Xiao conceived the original idea and has administrated the project. Shuang-Jiang Zhou conceived the original idea and writing-review & editing. Shu-Ping Tan has supervised the project. Material preparation and data collection were performed by Yan-Li Zhao. Data analysis was performed by Hong-Zhen Fan, Lei-Lei Wang. The first draft of the manuscript was written by Lan Gao and Rui Yang. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript. Lan Gao and Rui Yang share first authorship.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Darmedru C, Demily C, Franck N. Cognitive remediation and social cognitive training for violence in schizophrenia: a systematic review. Psychiatry Res. 2017;251:266–274. doi:10.1016/j.psychres.2016.12.062
2. Sakanaka S, Tsujii N, Morimoto H, Shirakawa O. Aggressiveness is associated with excitement on the five-factor model of the positive and negative syndrome scale and prefrontal function in patients with stable schizophrenia. Psychiatry Res. 2020;290:113054. doi:10.1016/j.psychres.2020.113054
3. Zhou JS, Zhong BL, Xiang YT, et al. Prevalence of aggression in hospitalized patients with schizophrenia in China: a meta-analysis. Asia Pac Psychiatry. 2016;8(1):60–69. doi:10.1111/appy.12209
4. Volavka J. Violence in schizophrenia and bipolar disorder. Psychiatr Danub. 2013;25(1):24–33.
5. de Bles NJ, Hazewinkel AWP, Bogers J, et al. The incidence and economic impact of aggression in closed long-stay psychiatric wards. Int J Psychiatry Clin Pract. 2021;25(4):430–436. doi:10.1080/13651501.2020.1821894
6. McEvoy J. The costs of schizophrenia. J Clin Psychiatry. 2007;14:4–7.
7. Taylor PJ, Kalebic N. Psychosis and homicide. Curr Opin Psychiatry. 2018;31(3):223–230. doi:10.1097/yco.0000000000000411
8. Hoptman MJ. Impulsivity and aggression in schizophrenia: a neural circuitry perspective with implications for treatment. CNS Spectr. 2015;20(3):280–286. doi:10.1017/S1092852915000206
9. Fjellvang M, Grøning L, Haukvik U. Imaging Violence in Schizophrenia: a Systematic Review and Critical Discussion of the MRI Literature. Front Psychiatry. 2018;9:333. doi:10.3389/fpsyt.2018.00333
10. Tang X, Jin J, Tang Y, Cao J, Huang J. Risk assessment of aggressive behavior in Chinese patients with schizophrenia by fMRI and COMT gene. Neuropsychiatr Dis Treat. 2017;13:387–395. doi:10.2147/ndt.S126356
11. Lau J, Jeyagurunathan A, Shafie S, et al. The factor structure of the Barratt Impulsiveness Scale (BIS-11) and correlates of impulsivity among outpatients with schizophrenia and other psychotic disorders in Singapore. BMC Psychiatry. 2022;22(1):226. doi:10.1186/s12888-022-03870-x
12. Araya T, Ebnemelek E, Getachew R. Prevalence and Associated Factors of Aggressive Behavior among Patients with Schizophrenia at Ayder Comprehensive Specialized Hospital, Ethiopia. Biomed Res Int. 2020;2020:7571939. doi:10.1155/2020/7571939
13. Jeyagurunathan A, Lau JH, Abdin E, et al. Aggression Amongst Outpatients With Schizophrenia and Related Psychoses in a Tertiary Mental Health Institution. Front Psychiatry. 2021;12:777388. doi:10.3389/fpsyt.2021.777388
14. Elbogen EB, Johnson SC. The Intricate Link Between Violence and Mental Disorder: results From the National Epidemiologic Survey on Alcohol and Related Conditions. Arch Gen Psychiatry. 2009;66(2):152–161. doi:10.1001/archgenpsychiatry.2008.537
15. Witt K, van Dorn R, Fazel S. Risk factors for violence in psychosis: systematic review and meta-regression analysis of 110 studies. PLoS One. 2013;8(2):e55942. doi:10.1371/journal.pone.0055942
16. Fazel S, Långström N, Hjern A, Grann M, Lichtenstein P. Schizophrenia, substance abuse, and violent crime. JAMA. 2009;301(19):2016–2023. doi:10.1001/jama.2009.675
17. Amr M, Elsayed H, Ibrahim IM. Impulsive behavior and its correlates among patients with schizophrenia in a tertiary care psychiatry setting in Mansoura. Asian J Psychiatr. 2016;22:111–115. doi:10.1016/j.ajp.2016.06.009
18. Trotta A, Murray R, Fisher H. The impact of childhood adversity on the persistence of psychotic symptoms: a systematic review and meta-analysis. Psychol Med. 2015;45(12):2481–2498. doi:10.1017/s0033291715000574
19. Černý M, Hodgins S, Kučíková R, et al. Violence in persons with and without psychosis in the Czech Republic: risk and protective factors. Neuropsychiatr Dis Treat. 2018;14:2793–2805. doi:10.2147/ndt.S167928
20. Roberts BW. Back to the Future: personality and Assessment and Personality Development. J Res Pers. 2009;43(2):137–145. doi:10.1016/j.jrp.2008.12.015
21. Balcioglub HBY. Impulsive and aggressive traits and increased peripheral inflammatory status as psychobiological substrates of homicide behavior in schizophrenia. Eur J Psychiatry. 2022;36(3):207–214.
22. Donnellan MB. Low self-esteem is related to aggression, antisocial behavior, and delinquency. Psychol Sci. 2005;1:5432.
23. Bushman BJ. Moderating role of trait aggressiveness in the effects of violent media on aggression. J Pers Soc Psychol. 1995;69(5):950–960. doi:10.1037//0022-3514.69.5.950
24. Bushman BJ. Individual differences in the extent and development of aggressive cognitive-associative networks. Pers Soc Psychol Bull. 1996;8:811–819.
25. Lemmens JS, Bushman BJ, Konijn EA. The appeal of violent video games to lower educated aggressive adolescent boys from two countries. Cyberpsychol Behav. 2006;9(5):638–641. doi:10.1089/cpb.2006.9.638
26. Moeller FG, Barratt ES, Dougherty DM, Schmitz JM, Swann AC. Psychiatric aspects of impulsivity. Am J Psychiatry. 2001;158(11):1783–1793. doi:10.1176/appi.ajp.158.11.1783
27. Moulin V, Golay P, Palix J, et al. Impulsivity in early psychosis: a complex link with violent behaviour and a target for intervention. Eur Psychiatry. 2018;49:30–36. doi:10.1016/j.eurpsy.2017.12.003
28. Krakowski MI, Czobor P. Distinctive profiles of traits predisposing to violence in schizophrenia and in the general population. Schizophr Res. 2018;202:267–273. doi:10.1016/j.schres.2018.07.008
29. Song CF, Huang SC, Zhu WL, Liang KM. Analysis of related factors of violence behavior in male schizophrenics. J Clin Psychiatry. 2020;30(6):408–410. doi:10.3969/j.issn.1005-3220.2020.06.009
30. Sun DP, Wang CD, Liang HB. Correlation between facial emotion recognition ability and impulsive aggressive behavior of patients with schizophrenia. Acta Acad Med Xuzhou. 2022;42(7):495–499. doi:10.3969/j.issn.2096-3882.2022.07.005
31. Pedersen S, Molina B, Belendiuk K, Donovan J. Racial differences in the development of impulsivity and sensation seeking from childhood into adolescence and their relation to alcohol use. Alcohol Clin Exp Res. 2012;36(10):1794–1802. doi:10.1111/j.1530-0277.2012.01797.x
32. Association AP. Diagnostic and Statistical Manual of Mental Disorders (DSM-IV). American Psychiatric Press; 1994.
33. Victoroff J, Coburn K, Reeve A, Sampson S, Shillcutt S. Pharmacological management of persistent hostility and aggression in persons with schizophrenia spectrum disorders: a systematic review. J Neuropsychiatry Clin Neurosci. 2014;26(4):283–312. doi:10.1176/appi.neuropsych.13110335
34. Si TM, Yang JZ, Shu L. The Reliability, Validity of PANSS and its Implication. Chine Mental Health J. 2004;18(1):45–47. doi:10.3321/j.issn:1000-6729.2004.01.016
35. Li XY, Fei LP, Xu D, et al. Reliability and validity of an adapted Chinese version of Barratt Impulsiveness Scale. Chine Mental Health J. 2011;25(8):610–615. doi:10.3969/j.issn.1000-6729.2011.08.013
36. Li XY, Fei LP, Zhang YL. Development, Reliability and Validity of the Chinese version of Buss & Perry Aggression Questionnaire. Chine J Nervous Mental Dis. 2011;37(10):607–613. doi:10.3969/j.issn.1002-0152.2011.10.010
37. TsTseng S. Psychiatry. People’s Medical Publishing House; 2001:356–357.
38. Gao H, Yu XJ, Lv F. Reliability and validity of insight and treatment attitude questionnaire. Chine Mental Health J. 1998;12(2):72–73.
39. Jiang J, Kang RY, Yan HF. Retrospective Analysis of Overt Aggressive Behavior and Associated Factors among Community-residing Patients with Schizophrenia from Beijing Fengtai District. Chine General Practice. 2017;20(25):3178–3183. doi:10.3969/j.issn.1007-9572.2017.25.024
40. Herman A, Critchley H, Duka T. Risk-Taking and Impulsivity: the Role of Mood States and Interoception. Front Psychol. 2018;9:1625. doi:10.3389/fpsyg.2018.01625
41. Schandrin A, Norton J, Raffard S, et al. A multi-dimensional approach to the relationship between insight and aggressiveness in schizophrenia: findings from the FACE-SZ cohort. Schizophr Res. 2019;204:38–45. doi:10.1016/j.schres.2018.07.029
42. van Dongen JDBN, van Marle HJ. Positive symptoms, substance use, and psychopathic traits as predictors of aggression in persons with a schizophrenia disorder. Psychiatry Res. 2016;1:654.
43. So S, Freeman D, Dunn G, et al. Jumping to conclusions, a lack of belief flexibility and delusional conviction in psychosis: a longitudinal investigation of the structure, frequency, and relatedness of reasoning biases. J Abnorm Psychol. 2012;121(1):129–139. doi:10.1037/a0025297
44. Freeman D. Suspicious minds: the psychology of persecutory delusions. Clin Psychol Rev. 2007;27(4):425–457. doi:10.1016/j.cpr.2006.10.004
45. Nederlof AF, Muris P, Hovens JE. Threat/control-override symptoms and emotional reactions to positive symptoms as correlates of aggressive behavior in psychotic patients. J Nerv Ment Dis. 2011;199(5):342–347. doi:10.1097/NMD.0b013e3182175167
46. McDermott B, Holoyda B. Assessment of aggression in inpatient settings. CNS Spectr. 2014;19(5):425–431. doi:10.1017/s1092852914000224
47. Perry A, Rubinsten O, Peled L, Shamay-Tsoory SG. Don’t stand so close to me: a behavioral and ERP study of preferred interpersonal distance. Neuroimage. 2013;83:761–769. doi:10.1016/j.neuroimage.2013.07.042
48. Deus V, Jokić-Begić N. Personal space in schizophrenic patients. Psychiatr Danub. 2006;18(3–4):150–158.
49. Mohr P, Knytl P, Vorackova V, Bravermanova A, Melicher T. Long-acting injectable antipsychotics for prevention and management of violent behaviour in psychotic patients. Int J Clin Pract. 2017;71(9):e12997. doi:10.1111/ijcp.12997
50. Nanda P, Tandon N, Mathew IT, et al. Impulsivity across the psychosis spectrum: correlates of cortical volume, suicidal history, and social and global function. Schizophr Res. 2016;170(1):80–86. doi:10.1016/j.schres.2015.11.030
51. Engelstad KN, Vaskinn A, Torgalsbøen AK, Mohn C, Lau B, Rund BR. Impaired neuropsychological profile in homicide offenders with schizophrenia. Compr Psychiatry. 2018;85:55–60. doi:10.1016/j.comppsych.2018.06.002
52. Yang Y, Raine A, Han CB, Schug RA, Toga AW, Narr KL. Reduced hippocampal and parahippocampal volumes in murderers with schizophrenia. Psychiatry Res. 2010;182(1):9–13. doi:10.1016/j.pscychresns.2009.10.013
53. Sani SRH, Tabibi Z, Fadardi JS, Stavrinos D. Aggression, emotional self-regulation, attentional bias, and cognitive inhibition predict risky driving behavior. Accid Anal Prev. 2017;109:78–88. doi:10.1016/j.aap.2017.10.006
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association Between Specific Insomnia Symptoms and Aggression in Chinese Patients with Chronic Schizophrenia: A Large-Scale Cross-Sectional Study
Wei L, Zhou Y, Peng P, Zhang X
Nature and Science of Sleep 2025, 17:2991-3002
Published Date: 19 November 2025