Back to Journals » International Journal of General Medicine » Volume 14
Correlation Between 25 Hydroxyvitamin D Levels and Nonalcoholic Fatty Liver Disease in Chinese Patients with Type 2 Diabetes Mellitus: A Cross-Sectional Study
Authors Xiu L, Jiang T ![]() , Yao XA, Wen Z
, Yao XA, Wen Z
Received 16 May 2021
Accepted for publication 15 June 2021
Published 1 July 2021 Volume 2021:14 Pages 3099—3107
DOI https://doi.org/10.2147/IJGM.S319449
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Lei Xiu, Tao Jiang, Xiao-ai Yao, Zhen Wen
Department of Endocrinology, Beijing Shijitan Hospital, Capital Medical University, Beijing, 100038, People’s Republic of China
Correspondence: Tao Jiang
Department of Endocrinology, Beijing Shijitan Hospital, Capital Medical University, Beijing, 100038, People’s Republic of China
Email [email protected]
Purpose: We aimed to analyze the serum vitamin D level in Chinese patients with type 2 diabetes mellitus (T2DM) and discuss its correlation with nonalcoholic fatty liver disease (NAFLD).
Patients and Methods: A total of 300 patients with T2DM (92 patients without NAFLD and 208 patients with NAFLD) were enrolled, and 25-hydroxyvitamin D [25-(OH)D] levels were compared between the two groups. Second, the NAFLD fibrosis score (NFS) and fatty liver index (FLI) were used to group patients with T2DM complicated by NAFLD, and the differences in serum 25-(OH)D in patients with different degrees of liver fibrosis were compared. Third, multiple regression analysis was used to analyze the independent predictors of liver fibrosis in patients with T2DM complicated by NAFLD.
Results: The level of 25-(OH)D in patients with T2DM complicated by NAFLD was significantly lower than that in patients with T2DM alone. Based on the NFS and FLI, the 25-(OH)D level of the hepatic fibrosis subgroup was significantly lower than that of the subgroup without liver fibrosis. 25-(OH)D was found to be an independent predictor of liver fibrosis in patients with T2DM complicated by NAFLD.
Conclusion: The serum 25-(OH)D level in patients with T2DM complicated by NAFLD was significantly reduced, and the 25-(OH)D level showed a gradual downward trend with the degree of liver fibrosis. Low concentrations of 25-(OH)D may be indicative of the degree of liver fibrosis in diabetic patients.
Keywords: type 2 diabetes mellitus, nonalcoholic fatty liver disease, 25-hydroxyvitamin D, liver fibrosis
Introduction
Globally, nonalcoholic fatty liver disease (NAFLD) is usually accompanied by insulin resistance. Unfortunately, a large number of type 2 diabetes mellitus (T2DM) patients subsequently develop NAFLD, and some develop nonalcoholic steatohepatitis (NASH); such patients may have further secondary liver cirrhosis or even develop liver cancer.1,2 The liver can produce, absorb, store and utilize glucose and is an important organ that maintains the homeostasis of blood glucose metabolism.3 Insulin inhibits hepatic gluconeogenesis and controls adipogenesis, so the rates of hepatic gluconeogenesis and lipid accumulation are closely related to insulin sensitivity.3 Liver insulin resistance leads to hyperglycemia, which can further aggravate insulin insensitivity. This negative cycle promotes the pathological state of liver dysfunction and ultimately develops into liver disease. NAFLD includes a series of clinicopathological conditions from simple steatosis to NASH. The prevalence of osteoporosis in patients with NAFLD is higher than that in normal people, and the risks of osteoporosis and osteoporotic fracture are increased.4,5 Increasing evidence shows interactions between glucose metabolism, the insulin signaling pathway and bone metabolism.6 Vitamin D is an important hormone that regulates calcium and phosphorus metabolism and bone homeostasis. In recent years, studies have shown that vitamin D receptor and 1α-(OH) vitamin D exist in extrarenal tissues such as the liver and islet cells.7 Animal experiments have shown that vitamin D may improve hepatic glucose and lipid metabolism in vivo and in vitro by activating the Ca2+/CaMKK β/AMPK signaling pathway and may also improve hepatic steatosis by upregulating ATG16L1-induced autophagy.8 However, the results of animal and human experiments can differ, suggesting that we cannot simply infer that the situation in humans is the same as that observed in animal experiments. At present, there are many ways to evaluate the degree of liver fibrosis in NAFLD patients, and the gold standard is still a pathological examination. However, the application of this method has some limitations due to invasive reasons. In addition, abdominal magnetic resonance imaging (MRI) can effectively evaluate liver fibrosis, but the application of this method is restricted by the economic situation. At present, the noninvasive assessment methods of liver fibrosis include the NAFLD fibrosis score (NFS)9,10 and fatty liver index (FLI).11 Bone homeostasis depends on the absorption of bone by osteoclasts and the formation of bone by osteoblasts. An imbalance in this tightly coupled process can lead to diseases such as osteoporosis.12 Bone turnover markers (BTMs) include both bone formation markers (eg, N-terminal collagen type I extension peptide (PINP), osteocalcin, and alkaline phosphatase (ALP)) and bone resorption markers (mainly degradation products of collagen I, such as the β-isomerized C-terminal peptide of type I collagen (β-CTX) and the N-terminal peptide of type I collagen) and reflect bone metabolism.13
Our previous studies showed that 25-hydroxyvitamin D [25-(OH)D] levels were associated with decreased diastolic function in Chinese adults with early-onset type 2 diabetes and that NFS and Fibrosis-4 (FIB-4), indicators of liver fibrosis, were associated with decreased diastolic function in adults with early-onset type 2 diabetes.14 Therefore, is there a correlation between 25-(OH)D and liver fibrosis in Chinese patients with type 2 diabetes? To address this question, our team conducted further research and investigation.
At present, few studies have been conducted to explore the relationship between 25-(OH)D levels and the degree of liver fibrosis in patients with type 2 diabetes mellitus complicated by NAFLD. In this study, serum 25-(OH)D and other bone metabolism indexes were observed in patients with different degrees of NAFLD, and their relationship with T2DM complicated by NAFLD was explored.
Materials and Methods
Patient Population
From July 2017 to October 2019, 300 patients with T2DM (178 males and 122 females) were diagnosed and treated at the Department of Endocrinology in our hospital. Among them, 208 were complicated by NAFLD; the mean patient age was 51.5 ± 15.2 years, and the course of diabetes was 8.3 ± 7.2 years. In total, 92 patients were not complicated by NAFLD; the mean patient age was 40.5 ± 15.0 years, and the course of diabetes was 6.9 ± 6.2 years. The inclusion criterion was as follows: patients with T2DM who met the diagnostic criteria and classification criteria of the World Health Organization for T2DM in 1999, that is, symptoms of diabetes plus random blood glucose concentration ≥ 11.1 mmol/L or fasting blood glucose (FPG) ≥ 7.0 mmol/L or 2 hPG ≥ 11.1 mmol/L after 75 g glucose load. If no symptoms of diabetes are observed, then the above three examinations need to be carried out on different dates, and if the criterion is met in two of these examinations, a diagnosis of diabetes can be made.15 Patients with other diseases, such as acute and chronic infection, other systemic diseases, immune system diseases, hyperparathyroidism, multiple myeloma, bone damage caused by malignant tumors, bone metastases and other diseases that significantly affect the metabolism of bone calcium and phosphorus, and liver and kidney diseases, were excluded. Patients who used drugs that affect bone metabolism, such as glucocorticoids, calcium, calcitonin, active vitamin D, common vitamin D, and bisphosphonates, were also excluded. The diagnosis of NAFLD was based on the following: 1) a negative history of alcohol abuse, with a weekly ethanol intake of <70 g for women and <140 g for men; 2) exclusion of ethanol-induced or drug-induced liver disease, autoimmune disease, viral hepatitis, cholestasis, metabolic liver disease and other liver diseases; 3) elevated levels of transaminase (alanine transaminase (ALT) and/or aspartate aminotransferase (AST)); and 4) confirmatory B-ultrasound results, as liver biopsy is difficult to promote clinically. The criteria for the diagnosis of fatty liver by ultrasound include an increase in liver echo, a difference in liver and kidney echo, and vascular blurring.16 Patients with variceal hemorrhage and decompensated cirrhosis were also excluded from the study.
Methods
All patient demographics were collected in detail. Their height, weight, and waist circumference (WC) were measured, and body mass index (BMI) was calculated. After 8 hours of fasting, blood samples were collected between 6:00 a.m. and 8:00 a.m. Serum ALT, AST, gamma-glutamyl transpeptidase (GGT), triglyceride (TG), albumin, platelet, 25-(OH)D, whole parathyroid hormone (PTH), N-terminal propeptide of type I procollagen (PINP) and C-terminal peptide of type I collagen (β CTX) were measured under fasting conditions. PTH was measured with a chemiluminescence immunoassay (CLIA) on a Beckman® automatic analyzer, and 25-(OH)D was measured with an automatic Roche® 601 analyzer. Bone mineral density was measured by dual energy X-ray absorptiometry.
The levels of 25-(OH)D in T2DM patients were divided into four grades: 10 ng/mL, 10–20 ng/mL, 20–30 ng/mL and > 30 ng/mL. The liver fibrosis grade of NAFLD patients (according to the NFS) was divided into the following subgroups: the < −1.455 subgroup (liver fibrosis exclusion subgroup), the −1.455~0.676 subgroup (uncertain subgroup), and the > 0.676 subgroup (liver fibrosis subgroup). Patients were divided into three subgroups according to the FLI: the < 30 subgroup (hepatic fibrosis exclusion subgroup), the 30~60 subgroup (uncertain subgroup), and the > 60 subgroup (hepatic fibrosis subgroup). The NFS was calculated as follows: NFS=1.675 + age (years) ×0.037 + BMI (kg/m2) × 0.094 + IFG/diabetes (yes=1, no=0) × 1.13 + AST/ALT ratio × 0.99 – platelet (×109/l) × 0.013 – albumin (g/dl) × 0.66.9 The FLI was calculated as follows: FLI = [e 0.953 ×loge (TG mg/dl)+0.139×(BMI kg/m2)+0.718×loge (GGT u/l)+0.053×(WC cm) – 15.745]/[1 + e0.953 ×loge (TG mg/dl)+0.139×(BMI kg/m2)+0.718×loge (GGT u/l)+0.053×(WC cm) - 15.745] × 100.11
Statistical Analysis
SPSS 25.0 software was used for the statistical analyses. The Kolmogorov–Smirnov test was used to verify whether the variables conformed to a normal distribution. Normally distributed measurement data are expressed as the mean ± standard deviation (χ ± s), and an independent sample t-test was used for comparisons between two groups. Gender comparisons between research groups were calculated and displayed by the chi-square test method. Abnormally distributed measurement data are expressed as the median and interquartile range [M (QL, QU)], and comparisons between two groups were conducted with the Mann–Whitney test. Binary logistic regression analysis was used to analyze the correlation. In the binary logistic regression, we transformed continuous variables into classified data according to certain rules: Age was divided into < 40 years old, 40–60 years old and > 60 years old. Waist circumference was divided into < 80 cm, 80–100 cm and > 100 cm. The course of disease was divided into < 5 years, 5–10 years, 10–20 years and > 20 years. Blood glucose levels were divided into < 5 mmol/L, 5–10 mmol/L and > 10 mmol/L. Similarly, other continuous variable data were converted into classified data according to a certain threshold.
This study was approved by the Ethics Committee of Beijing Shijitan Hospital, Capital Medical University and conducted according to the Declaration of Helsinki of the World Medical Association (ethical principles of medical research involving the human body).
Results
General Clinical Data and Biochemical Profiles
Our study included 300 T2DM patients (208 with NAFLD and 92 without NAFLD) diagnosed and treated at the Endocrinology Department in our hospital. The general condition and laboratory test results of the two groups are shown in Table 1. Patient age, waist circumference and HbA1c of the T2DM with NAFLD group were significantly higher than those of the T2DM without NAFLD group, and the albumin level was significantly lower than those of the T2DM without NAFLD group (P < 0.05). No other statistically significant difference was observed between groups (eg, duration, BMI, TG, glucose, insulin, HOMA-IR, calcium and phosphate).
 |
Table 1 Comparative Data of the Study Groups |
Levels of 25-(OH)D and Other Bone Metabolism Indexes in T2DM Patients with or without NAFLD
Experimental data have shown that interactions among the liver, adipose tissue and bone comprise a complex system to regulate each other’s functions. There may be a two-way relationship between liver metabolism and bone metabolism: liver metabolism may affect bone metabolism and vice versa. To investigate the effect of liver diseases on bone metabolism, we analyzed the changes in PINP, β-CTX, osteocalcin, ALP, PTH, 25-(OH)D and bone mineral density (BMD) levels in patients with T2DM complicated by NAFLD (Table 2). The results showed that the level of 25-(OH)D in patients with T2DM complicated by NAFLD was significantly lower than that in patients with T2DM only (P < 0.01). In addition, the levels of PINP, β-CTX, osteocalcin, vertebral bone density and hip bone density in patients with T2DM complicated by NAFLD were significantly lower than those in patients with T2DM only (P < 0.05). There was no significant difference in PTH or ALP between the two groups.
 |
Table 2 PINP, β-CTX, 25-(OH)D and Bone Mineral Density Levels Between T2DM Patients with or without NAFLD |
Binary Logistic Regression Analysis Reveals the Independent Predictors of NAFLD in Patients with T2DM
Binary logistic regression analysis was performed with NAFLD as the dependent variable and 25-(OH)D, waist circumference, TGs, albumin, insulin, fasting blood glucose (FBG), HOMA-IR, age, BMI, duration, ALT and AST as independent variables. The results showed that 25-(OH)D (OR = 1.084, P = 0.013) and age (OR = 0.954, P = 0.008) were independent predictors of NAFLD in patients with T2DM (Table 3).
 |
Table 3 Binary Logistic Regression Analysis of Factors Associated with NAFLD in T2DM Patients |
Correlation Analysis of the NFS, FLI and Various Indexes
The NFS and FLI are internationally recognized indicators that are used to evaluate the degree of liver fibrosis in patients with T2DM. All patients with T2DM complicated by NAFLD were divided into three groups according to the NFS and FLI: the liver fibrosis group, the uncertain subgroup and the hepatic fibrosis subgroup. The differences in PINP, β-CTX, osteocalcin, ALP, PTH and 25-(OH)D levels between the three groups were compared (Table 4). Our study showed that the 25-(OH)D level of the liver fibrosis subgroup was significantly lower than that of the liver fibrosis exclusion subgroup and the uncertain subgroup according to the NFS (P < 0.05). There was no significant difference in PINP, β-CTX, osteocalcin, ALP or PTH between the three groups. According to the FLI, the level of 25-(OH)D in the liver fibrosis subgroup was significantly lower than that in the liver fibrosis exclusion subgroup (P < 0.05). The level of osteocalcin was significantly lower in the liver fibrosis subgroup than in the uncertain subgroup (P < 0.01), and the level of osteocalcin was significantly lower in the uncertain subgroup than in the hepatic fibrosis exclusion subgroup (P < 0.05). There was no significant difference in PINP, β-CTX, ALP or PTH among the three groups.
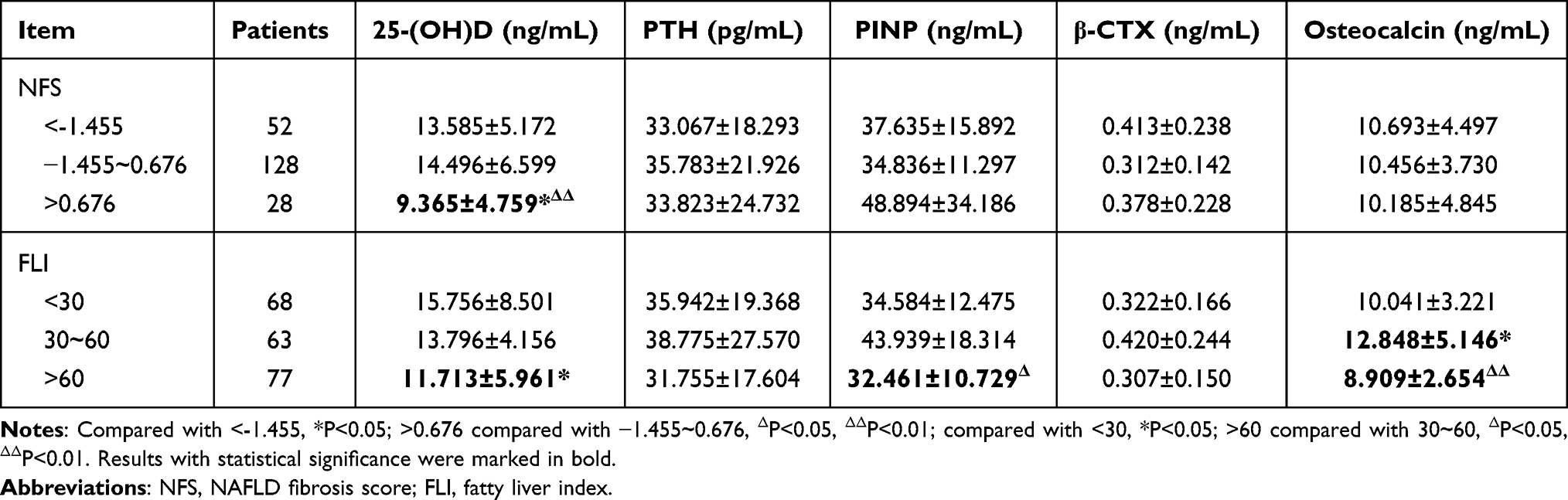 |
Table 4 Index Based on Different Degrees of Liver Fibrosis in T2DM Patients with NAFLD |
Discussion
The results of our study reveal a correlation between the serum vitamin D level and NAFLD in patients with T2DM. The vitamin D level in patients with T2DM complicated by NAFLD is significantly lower than that in patients with T2DM only. Vitamin D plays an important role in many pathophysiological processes. Studies in human and animal models have shown that vitamin D deficiency can promote oxidative stress, increase the systemic inflammatory response, reduce adiponectin levels, activate Toll-like receptors and promote the occurrence of NAFLD.17,18 Vitamin D and liver diseases have an interactive relationship. Vitamin D can prevent hepatic steatosis by stimulating autophagy.8 Vitamin D deficiency can cause insulin resistance, increase the expression of the liver resistin gene and upregulate the expression of hepatitis and oxidative stress genes, thus promoting the occurrence and development of NAFLD.17 In turn, NAFLD affects vitamin D levels. Vitamin D, which is found in some foods and produced by the skin through light, needs to be hydroxylated in the liver; thus, its synthesis can be affected by liver diseases.
Our study showed that the BMD of the vertebral body and hip joint in T2DM patients complicated by NAFLD was lower than that in T2DM patients without NAFLD. The serum levels of PINP and osteocalcin in T2DM patients complicated by NAFLD were lower than those in T2DM patients without NAFLD, and the levels of the osteoclast-derived molecule β-CTX were also lower in T2DM patients. This finding suggests that there may be bone-liver interactions, which are worthy of further study. Liver disease can affect bone metabolism in a variety of ways.19 Cytokines involved in chronic liver disease, such as IL-1, IL-6 and TNF-α, can activate the NF-κB ligand/osteoprotegerin receptor activator (RANKL/OPG) system. These cytokines increase osteoclast formation and activity and prevent osteoblast formation.20,21 In addition, TNF-α not only participates in the stimulation of osteoclasts but also inhibits the activation of osteoblasts in their progenitor cells.22 TNF-α stimulates the expression of genes related to osteoclast formation and suppresses the expression of genes related to osteogenesis.23 Similarly, TNF-α inhibits osteoclast apoptosis, and by binding to osteoblast receptors, TNF-α also inhibits osteoblast proliferation/differentiation and increases apoptosis in progenitor cells.24 Insulin-like growth factor-1 (IGF-1) is synthesized mainly by the liver and is a regulatory factor of bone formation. IGF-1 promotes the proliferation and differentiation of osteoblasts by autocrine and paracrine mechanisms and decreases with aging and liver diseases. Liver lesions can lead to abnormal IGF-1 synthesis and ultimately to bone loss and bone metabolism abnormalities.25,26 Both osteogenesis and osteoclast are affected.
The NFS and FLI are internationally recognized indicators that can reflect the degree of liver fibrosis in patients with diabetes mellitus. Because liver biopsy cannot be widely used in clinical practice, we used the above two indicators for the classification of liver fibrosis in patients with T2DM and NAFLD. With both methods, we found that serum vitamin D levels in patients with liver fibrosis were significantly lower than those in patients without liver fibrosis. This finding also suggests that the effect of liver disease on vitamin D levels is related to the severity of liver disease.
Vitamin D deficiency has also been linked with the development of cancer, particularly liver cancer.27 Maintaining normal levels of serum vitamin D is essential. Several supplements, such as omega-3 supplementation, can be used to increase vitamin D levels.28
Study Limitations
There are some limitations to this research that should be noted. First, although NFS and FLI are commonly recognized indicators to reflect the degree of liver fibrosis in NAFLD patients, pathological diagnosis is the gold standard to judge the degree of liver fibrosis. It is expected that more pathological diagnosis studies will further confirm our view in the future. Second, our results show that both bone osteogenesis and osteolysis are affected in T2DM patients with NAFLD. However, the sample size of our study was limited. In future studies, we will further clarify the change trend in bone formation markers and bone absorption markers in T2DM patients with NAFLD by increasing the sample size. The association of vitamin D deficiency with prognosis, such as progression to NASH, liver decompensation, and development of hepatocellular carcinoma (HCC), needs to be discussed in prospective studies. Third, our study is a retrospective study, and it is impossible to observe whether the degree of liver fibrosis is improved after vitamin D supplementation in patients with low vitamin D levels. In future prospective studies, we will carry out this part of the study to clarify the effect of low vitamin D levels on the degree of liver fibrosis in patients with diabetes.
Conclusion
Our study showed that there were differences in age, waist circumference and other factors between T2DM patients with NAFLD and those without NAFLD. To exclude their influence on the results, we included them in the binary logistic regression analysis for correction. After excluding these factors, 25-(OH)D was still associated with the occurrence of NAFLD in T2DM patients, which suggested that 25-(OH)D was a risk factor for NAFLD in T2DM patients or that a lower 25-(OH)D level may indicate an increased risk of NAFLD in patients with T2DM.
In conclusion, the results of this study showed that the serum 25-(OH)D level and BMD were significantly decreased in T2DM patients with NAFLD, and the level of 25-(OH)D gradually decreased with the aggravation of liver fibrosis. The 25-(OH)D level is an independent predictor of liver fibrosis in T2DM patients with NAFLD and may be used as a predictor of liver fibrosis in these patients.
Abbreviations
T2DM, type 2 diabetes mellitus; NAFLD, nonalcoholic fatty liver disease; NASH, nonalcoholic steatohepatitis; 25-(OH)D, 25-hydroxyvitamin D; NFS, NAFLD fibrosis score; FLI, fatty liver index; FIB-4, Fibrosis-4; BTMs, Bone turnover markers; PINP, N-terminal collagen type I extension peptide; ALP, alkaline phosphatase; β-CTX, β-isomerized C-terminal peptide of type I collagen; PTH, parathyroid hormone; ALT, alanine transaminase; AST, aspartate aminotransferase; GGT, amma-glutamyl transpeptidase; TG, triglyceride.
Data Sharing Statement
The main data analyzed in this study were included in the published article.
Ethics Approval and Informed Consent
The authors take responsibility for all aspects of the work and for ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. The study conformed to the provisions of the Declaration of Helsinki (as revised in 2013). The study was approved by the Scientific Research Ethics Committee of Beijing Shijitan Hospital affiliated with Capital Medical University (research ethics No. 37 in 2021), and informed consent was obtained from the research subjects.
Consent for Publication
All participants agreed to publication of the study.
Funding
This work was supported by the China Railway Corporation (grant number J2016Z029).
Disclosure
All authors have no conflicts of interest to declare.
References
1. Tilg H, Moschen AR, Roden M. NAFLD and diabetes mellitus. Nat Rev Gastroenterol Hepatol. 2017;14(1):32–42. doi:10.1038/nrgastro.2016.147
2. Dai W, Ye L, Liu A, et al. Prevalence of nonalcoholic fatty liver disease in patients with type 2 diabetes mellitus: a meta-analysis. Medicine (Baltimore). 2017;96(39):e8179. doi:10.1097/MD.0000000000008179
3. Bechmann LP, Hannivoort RA, Gerken G, Hotamisligil GS, Trauner M, Canbay A. The interaction of hepatic lipid and glucose metabolism in liver diseases. J Hepatol. 2012;56(4):952–964. doi:10.1016/j.jhep.2011.08.025
4. Chacko KR, Reinus J. Extrahepatic complications of nonalcoholic fatty liver disease. Clin Liver Dis. 2016;20(2):387–401. doi:10.1016/j.cld.2015.10.004
5. Adams LA, Anstee QM, Tilg H, Targher G. Non-alcoholic fatty liver disease and its relationship with cardiovascular disease and other extrahepatic diseases. Gut. 2017;66(6):1138–1153. doi:10.1136/gutjnl-2017-313884
6. Rathinavelu S, Guidry-Elizondo C, Banu J. Molecular modulation of osteoblasts and osteoclasts in type 2 diabetes. J Diabetes Res. 2018;2018:6354787. doi:10.1155/2018/6354787
7. Leung PS. The potential protective action of vitamin d in hepatic insulin resistance and pancreatic islet dysfunction in type 2 diabetes mellitus. Nutrients. 2016;8(3):147. doi:10.3390/nu8030147
8. Li R, Guo E, Yang J, et al. 1,25(OH)2D3 attenuates hepatic steatosis by inducing autophagy in mice. Obesity (Silver Spring). 2017;25(3):561–571. doi:10.1002/oby.21757
9. Angulo P, Hui JM, Marchesini G, et al. The NAFLD fibrosis score: a noninvasive system that identifies liver fibrosis in patients with NAFLD. Hepatology. 2007;45(4):846–854. doi:10.1002/hep.21496
10. Gheorghe G, Bungau S, Ceobanu G, et al. The non-invasive assessment of hepatic fibrosis. J Formos Med Assoc. 2021;120(2):794–803. doi:10.1016/j.jfma.2020.08.019
11. Bedogni G, Bellentani S, Miglioli L, et al. The Fatty Liver Index: a simple and accurate predictor of hepatic steatosis in the general population. BMC Gastroenterol. 2006;6(1):33. doi:10.1186/1471-230X-6-33
12. Chen X, Wang Z, Duan N, Zhu G, Schwarz EM, Xie C. Osteoblast-osteoclast interactions. Connect Tissue Res. 2018;59(2):99–107. doi:10.1080/03008207.2017.1290085
13. Szulc P, Naylor K, Hoyle NR, Eastell R, Leary ET. National bone health alliance bone turnover marker P: use of CTX-I and PINP as bone turnover markers: national bone health alliance recommendations to standardize sample handling and patient preparation to reduce pre-analytical variability. Osteoporos Int. 2017;28(9):2541–2556. doi:10.1007/s00198-017-4082-4
14. Xiu L, Yao XA, Jiang T. Correlation between 25-hydroxyvitamin d level and cardiac diastolic dysfunction in chinese adults with early-onset type 2 diabetes mellitus: a cross-sectional Study. Diabetes Metab Syndr Obes. 2021;14:1823–1831. doi:10.2147/DMSO.S299422
15. Mayfield J. Diagnosis and classification of diabetes mellitus: new criteria. Am Fam Physician. 1998;58(1355–62):69–70.
16. Saverymuttu SH, Joseph AE, Maxwell JD. Ultrasound scanning in the detection of hepatic fibrosis and steatosis. Br Med J (Clin Res Ed). 1986;292(6512):13–15. doi:10.1136/bmj.292.6512.13
17. Roth CL, Elfers CT, Figlewicz DP, et al. Vitamin D deficiency in obese rats exacerbates nonalcoholic fatty liver disease and increases hepatic resistin and Toll-like receptor activation. Hepatology. 2012;55(4):1103–1111. doi:10.1002/hep.24737
18. Nelson JE, Roth CL, Wilson LA, et al. Vitamin D deficiency is associated with increased risk of non-alcoholic steatohepatitis in adults with non-alcoholic fatty liver disease: possible role for MAPK and NF-kappaB? Am J Gastroenterol. 2016;111(6):852–863. doi:10.1038/ajg.2016.51
19. Targher G, Lonardo A, Rossini M. Nonalcoholic fatty liver disease and decreased bone mineral density: is there a link? J Endocrinol Invest. 2015;38(8):817–825. doi:10.1007/s40618-015-0315-6
20. Nakchbandi IA, van der Merwe SW. Current understanding of osteoporosis associated with liver disease. Nat Rev Gastroenterol Hepatol. 2009;6(11):660–670. doi:10.1038/nrgastro.2009.166
21. Mantovani A, Sani E, Fassio A, et al. Association between non-alcoholic fatty liver disease and bone turnover biomarkers in post-menopausal women with type 2 diabetes. Diabetes Metab. 2019;45(4):347–355. doi:10.1016/j.diabet.2018.10.001
22. Zou W, Hakim I, Tschoep K, Endres S, Bar-Shavit Z. Tumor necrosis factor-alpha mediates RANK ligand stimulation of osteoclast differentiation by an autocrine mechanism. J Cell Biochem. 2001;83(1):70–83. doi:10.1002/jcb.1202
23. Nanes MS. Tumor necrosis factor-alpha: molecular and cellular mechanisms in skeletal pathology. Gene. 2003;321:1–15. doi:10.1016/S0378-1119(03)00841-2
24. Lee HL, Yi T, Woo KM, Ryoo HM, Kim GS, Baek JH. Msx2 mediates the inhibitory action of TNF-alpha on osteoblast differentiation. Exp Mol Med. 2010;42(6):437–445. doi:10.3858/emm.2010.42.6.045
25. Novince CM, Whittow CR, Aartun JD, et al. Commensal gut microbiota immunomodulatory actions in bone marrow and liver have catabolic effects on skeletal homeostasis in health. Sci Rep. 2017;7(1):5747. doi:10.1038/s41598-017-06126-x
26. Ohlsson C, Mohan S, Sjogren K, et al. The role of liver-derived insulin-like growth factor-I. Endocr Rev. 2009;30:494–535.
27. Zhang Y, Jiang X, Li X, et al. Serum vitamin D levels and risk of liver cancer: a systematic review and dose-response meta-analysis of cohort Studies. Nutr Cancer. 2020;1–9.
28. Alhabeeb H, Kord-Varkaneh H, Tan SC, et al. The influence of omega-3 supplementation on vitamin D levels in humans: a systematic review and dose-response meta-analysis of randomized controlled trials. Crit Rev Food Sci Nutr. 2020;1–8.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.