Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
Correlation Analyses Between Childhood Behavioral Disturbance and Maternal Alexithymia: An Observational Study
Received 16 May 2023
Accepted for publication 24 July 2023
Published 28 July 2023 Volume 2023:19 Pages 1665—1674
DOI https://doi.org/10.2147/NDT.S421458
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yu-Ping Ning
Yu-Chen Lin,1 Wei-Yang Lee2
1Department of Psychiatry, Veteran General Hospital-Taichung, Taichung, 407, Taiwan, Republic of China; 2Department of Psychiatry, Cheng Gung Memorial Hospital, Taoyuan City, 333, Taiwan, Republic of China
Correspondence: Wei-Yang Lee, Department of Psychiatry, Cheng Gung Memorial Hospital, Linkou, No. 5, Fuxing St., Guishan District, Taoyuan City, 333, Taiwan, Republic of China, Tel +886 988067722, Email [email protected]
Purpose: Caregivers’ responses have an impact on children’s emotional and behavioral development. The inability of caregivers to perceive their own emotions affects their responses to children. This study aims to examine the relationship between a mother’s difficulties in emotional expression and children’s emotional and behavioral disorders.
Patient and Methods: A total of 78 cases, aged between 3 and 15 years old, were included in this study. The mothers completed the Taiwan version of the “Toronto Alexithymia Scale” (TAS) and “Children’s Behavior Checklist” (CBCL) questionnaires, which served as research tools. TAS consists of three factors: difficulty in distinguishing emotions (Factor 1, F1), difficulty in expressing feelings (Factor 2, F2), and an externally oriented thinking style (Factor 3, F3). CBCL represents a child’s behavior profile. The Mann–Whitney test and correlation analyses were used for follow-up analysis.
Results: Our analysis revealed that F1, F2, F3, and total scores of TAS (TAS-Total) correlate positively with the somatic complaint subscale of CBCL (F1: p = 0.003; F2: p = 0.002; F3: p = 0.034, TAS-Total p=0.002). Additionally, TAS-F1 was positively correlated with the internalizing problems subscale of CBCL (p = 0.020) and the withdrawn (WD) subscale of CBCL (p = 0.044). We also found a significant association between TAS-F1 and WD of CBCL in boys alone (p = 0.022). However, we observed a negative association between TAS-F3 and the social problems subscale of CBCL in boys alone (p = 0.038).
Conclusion: Mothers with alexithymic features are more likely to have children who internalize emotions, leading to withdrawal and somatic expression. Boys tend to exhibit withdrawal traits associated with internalization. This study provides initial evidence of a partial correlation between maternal alexithymia and children’s emotional and behavioral disorders, emphasizing the importance of investigating caregivers’ emotional traits for a better understanding of children’s development in the future.
Keywords: maternal alexithymia, childhood behavioral disturbance, external and internal problem, children’s behavior checklist, Toronto alexithymia scale
Introduction
It is widely accepted that personality development gradually takes shape through long-term interactions between innate temperament and the acquired environment during the early years of life.1 Children’s behaviors are not only expressions of their innate temperaments but are also greatly influenced by their environment and family.2,3
According to the theories of object relations and self-psychology, the ability of the primary caregiver (usually the mother) to understand and respond to children’s emotions and behaviors significantly impacts healthy childhood development.4 Previous clinical studies and observations have revealed that the psychopathology of the primary caregiver can have lasting effects on the mental health of the children in their care, even into adulthood, and may even result in intergenerational transmission.5
Previous studies examining the influence of parental personality traits and psychopathology have rarely considered the impact of alexithymia. Alexithymia, which is characterized by difficulty recognizing and expressing emotions, has been linked to emotional dysregulation in individuals with psychosomatic disorders. Prior research has shown an inverse correlation between alexithymia and empathy.6 The nature of parent-child interaction has also been linked to alexithymia, which can impact children’s attachment and emotional bond with their parents. Individuals with an internally oriented thinking style are more likely to feel a stronger attachment and emotional bond with their primary caregiver, which acts as a buffer to developing an externally orientated cognitive style.7 The personality of parents has been identified as one of the key factors in children’s behavioral and emotional development.8 Maternal negative control has been found to mediate the connection between internalizing behaviors and emotional regulation in children.9 Additionally, shyness related to internalizing symptoms is mediated by different distraction regulation strategies such as redirecting one’s attention towards alternative activities instead of fixating on the source of delay, with mediations moderated by maternal negative control.10
Alexithymia
The alexithymia construct was initially defined in the early 1970s, and it encompasses several features, including (1) difficulty identifying and describing subjective feelings, (2) difficulty differentiating between feelings and bodily sensations, (3) a lack of imagination, and (4) an externally oriented cognitive style.11–15 This construct reflects deficits in the cognitive processing and regulation of emotions. An externally oriented cognitive style indicates a concrete thinking style that does not appear to significantly impact a person’s likelihood of experiencing positive or negative emotions.16
These deficits are considered important mechanisms that cause mood disorders and psychosomatic disorders. Previous studies have indicated that alexithymia is linked to many behavioral problems, both internalizing and externalizing.17,18
In the past, there have been few studies investigating the influence of a mother’s alexithymia on their children’s behavioral problems. Maternal alexithymia significantly predicts impaired emotional processing and increased risk of generalized anxiety in children and adolescents, particularly for internalizing behaviors.8,19 In this study, we collected comprehensive data from pediatric psychiatric outpatient clinics for children between the ages of 3 and 15. We hypothesized that caregivers who cannot empathize with others may have difficulty noticing and responding to the emotions of children under their care, which may result in emotional and behavioral disorders in the children. Currently, there is a lack of focused research on the specific subtypes of internal or external issues resulting from the influence of alexithymic mothers on their children. The current understanding implies that maternal alexithymia is associated with the development of internalizing problems in children, such as emotional difficulties, while there is no clear evidence of a similar relationship with externalizing problems.8 Another study showed that alexithymia is positively linked to internalizing behaviors in children, including symptoms like obsession, depression, anxiety, and negative thought patterns such as worry and rumination but it only focuses on children themself.20 Therefore, our study hopes to explore the correlation between children’s behavioral disturbances and the presence of alexithymia features in their mothers.
Materials and Methods
This research project is an observational study. The cases included in the psychological assessment referred from the Children and Adolescent Clinic at Taichung Veterans General Hospital in Taiwan primarily consisted of children presenting with issues related to hyperactivity, attention deficits, and intellectual and learning disabilities between 2008 and 2009. The diagnostic assessment process followed the criteria outlined in DSM-4, with exclusion criteria for organic brain injury. The cases included in the study encompassed individuals from the Han Chinese population residing in Taiwan, excluding indigenous populations. The study included a total of 78 participants (62 boys and 16 girls), with an age range from 3 to 15 years. In the subsequent diagnosis, the distribution revealed that the majority consisted of Attention Deficit Hyperactivity Disorder (ADHD) and learning disabilities (ID), which accounted for the highest (74%) and second highest (14%) proportions respectively. This was followed by Oppositional Defiant Disorder (8%), Autism Spectrum Disorders (6%), Obsessive-Compulsive Disorder (5%), and Trichotillomania (2%). The Taiwanese version of the TAS-20 questionnaire was used to evaluate alexithymia features in the mothers, while the CBCL questionnaire was used to assess emotional and behavioral disturbance in the children. The mothers completed both questionnaires independently without professional guidance.
Procedure and Data Analysis
This study was conducted by the principles outlined in the Declaration of Helsinki and was approved by the Institutional Review Board of Taichung Veterans General Hospital (approval code C07239). Informed consent was obtained from all parents or guardians of participants under the age of 15. Data analysis was conducted using a t-test and correlation analysis in SPSS.
Instruments
To evaluate the behavioral disturbance in children and the alexithymia features of their mothers in a pediatric psychiatric outpatient clinic, we administered the following items:
Toronto Alexithymia Scale(TAS)
In the past, there were few studies on Alexithymia due to the lack of quantitative research tools and rating scales. Among contemporary research tools for measuring alexithymia, the TAS developed in 1990 has been found to have optimal internal consistency and factor structure.11,21 Furthermore, the TAS was revised in 1994 and is currently the most widely used tool for studying alexithymia. The questionnaire consists of 20 narrative sentences and is divided into three factors: (1) difficulty identifying and distinguishing feelings from the bodily sensations of emotional arousal; (2) difficulty communicating feelings to others; and (3) an externally oriented thinking style. The original definition included a fourth factor, “lack of internal fantasy life”, but researchers found that it had a low correlation with the overall questionnaire and a high correlation with social needs during the questionnaire development process. Further factor analysis indicated that a 3-factor model had better validity than a 4-factor model.22,23 By the end of 2003, the TAS-20 had been translated into 18 languages and subjected to confirmatory factor analysis in 19 different cultural regions. The results showed goodness of fit index (GFI) of ≧0.85 for validity and Cronbach’s alpha of ≧0.70 for reliability, indicating optimal cross-language consistency and a stable 3-factor structure.24 The total score for alexithymia is obtained by summing the responses provided for all 20 items. In addition, the score for each subscale factor is calculated by summing the responses specifically related to that particular subscale.25
Dr. Yu-Chen Lin, MD, developed the Taiwanese version of the TAS in 2006 and named it the “Taiwanese version of the TAS” for studying the Taiwanese population.26 A total of 299 adult cases, comprising 117 males (mean age: 20 years) and 182 females (mean age: 19 years), were included in the study. There were no significant age differences observed between males and females. The collected data underwent confirmatory factor analysis with guidance from Dr. Bagby, the original author of TAS20. Following the recommended steps of back-translation and confirmatory factor analysis, based on Dr. Taylor’s advice, the Taiwanese version of the questionnaire demonstrated equivalent validity to the original instrument.27
In this study, we utilized the Taiwanese version of the TAS to assess primary caregivers of children with alexithymia features.
Child Behavior Checklist(CBCL)
The CBCL was developed by Professor Thomas M. Achenbach in the United States.28 It is often used as a screening instrument in standard child and adolescent psychiatric settings to provide valuable information for the diagnostic process. The CBCL is widely used to evaluate various aspects of children’s behavior as observed by their parents or primary caregivers.
The Taiwan version of the CBCL was standardized in 1994 and has well-established validity and reliability in Taiwan, with a 0.726 GFI for validity and a 0.9 Cronbach’s alpha for reliability.29 It consists of a 118-item parent-report questionnaire. The child’s score on the CBCL scale is based on age and sex norms for control. The scoring method is based on the frequency of behavior occurrence and follows a three-point scale: 0 points for “not applicable”, 1 point for “sometimes or somewhat applicable”, and 2 points for “quite or mostly applicable”.
The resulting data create a child’s behavior profile, including a Total Behavioral Problem score, two second-order factor scores (externalizing problems and internalizing problems), and 8 syndrome scale scores (somatic complaints (SC), anxious/depressed (AD), thought problems (TP), social problems (SP), withdrawn (WD), delinquent behavior (DB), aggressive behavior (AB), and attention problems (AP)). Externalizing behaviors, such as aggression, delinquency, and hyperactivity, refer to a group of behavioral problems that manifest in children’s outward behavior and reflect the child’s negative impact on the external environment.30 In contrast, internalizing behavioral problems such as withdrawal, somatic complaints, and anxiety and depression problems have a greater impact on the child’s internal psychological environment than on the external world.31 Each subscale score was converted to a t-score. Higher t-scores on each subscale indicate higher severity of problematic behaviors, with a clinical cutoff at t = 70. Scores between t = 65 and 70 fall within the borderline clinical range.
In this study, all mothers of each child in our outpatient clinic completed the Taiwan version of the CBCL. A trained research assistant, blind to the clinical history of the participants, rated the CBCL.
Statistical Analyses
First, we evaluated all items from TAS and CBCL and then performed all analyses using IBM SPSS Statistics 25. Correlation analyses were performed to investigate whether there was a correlation between children’s behavioral disturbances and their mothers’ alexithymic features.
Given the small sample size of 62 males and 16 females, as well as the presence of combined diagnoses such as ADHD and ID among different ethnic groups, it is uncertain whether the data will conform to a normal distribution. The modality of the association between the two variables was determined using the Spearman correlation test. The test was used to identify the type of association between the variables, and the statistical significance was determined based on a p-value of 0.05 or lower, using a two-tailed test. We used the Spearman correlation test to check the correlation between the three included alexithymia trait variables and the nine included Child Behavior trait variables. Besides, an analysis between age and TAS factors was conducted to examine any potential correlations. Furthermore, we use the Mann–Whitney U-test to assess the relationship between gender and TAS factors and the subscale of CBCL and determine if there are any significant associations.
Result
The study included a total of 78 participants, with a mean age of 8.9 years (SD=2.5). The age range of the participants was from 3 to 15 years, with the median age falling between 9 and 12 years. Among them, 62 were boys with a mean age of 8.9 years (SD=2.5), and 16 were girls with a mean age of 8.1 years (SD=2.9). There was no statistically significant difference in the mean age between boys and girls. Out of 78 individuals, 58 people, accounting for 74%, have ADHD, while 11 people, comprising 14%, have ID. (see Table 1) The mean TAS total score of the mothers was 46.4 (SD=10.2). The score was slightly higher in mothers with boys than in mothers with girls, but there was no significant difference found when analyzed between children’s sex and TAS-F1 (p=0.514), TAS-F2 (p=0.163), TAS-F3 (p=0.062) and TAS-total (p=0.151) (refer to Table 2). The mean CBCL total score of the children was 48.7 (SD=25). The score of the CBCL for girls was slightly higher than that of boys, but there was no significant difference found by children’s sex when analyzed (refer to Table 2). No statistical difference was observed between boys and girls in the mean score of individual subscales.
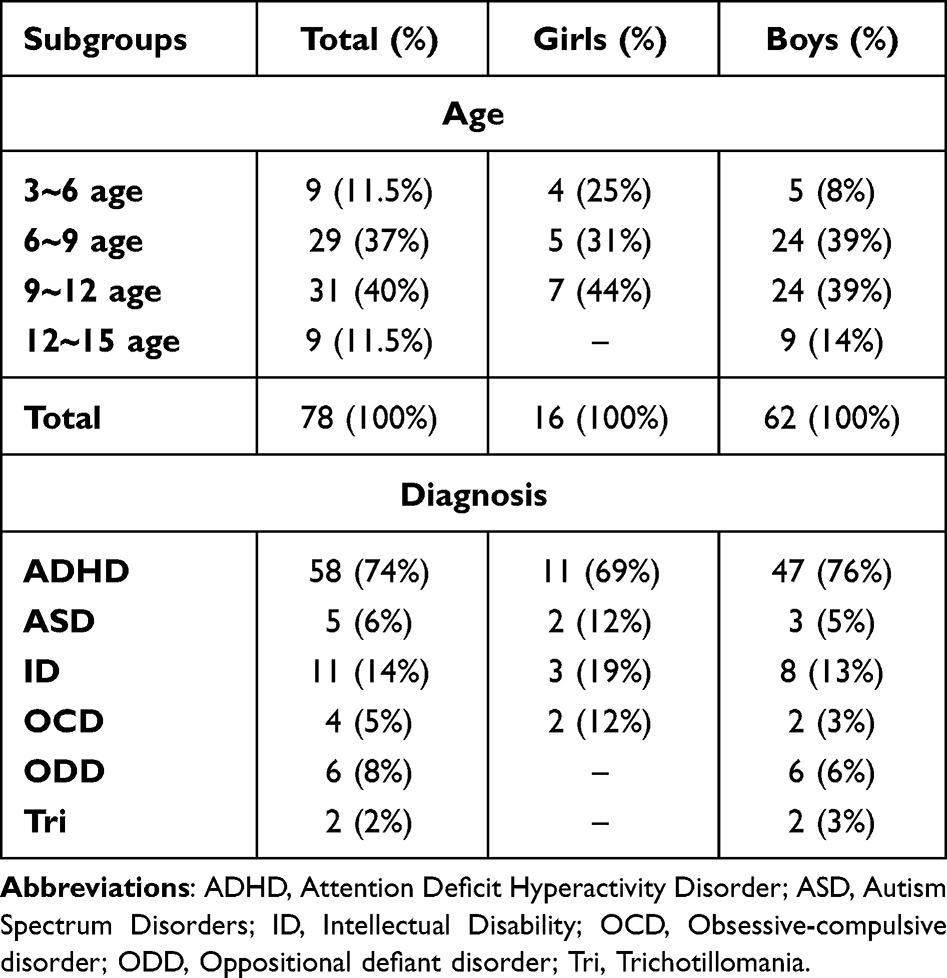 |
Table 1 Specific Subgroups of 78 Cases |
 |
Table 2 TAS Score of Caregivers and CBCL Score and 78 Cases |
Regarding the correlation between Mothers’ TAS and CBCL, there was no significant difference in total scores when analyzing the entire sample (n=78). However, all three factors (Factor 1, Factor 2, and Factor 3) as well as the total TAS score were positively correlated with the somatic complaint subscale of CBCL (F1 & SC: rs= 0.33, p =0.003; F2 & SC: rs = 0.342, p =0.002; F3 & SC: rs = 0.240, p =0.034; TAS-total and SC: rs = 0.353, p =0.002). Factor 1 of TAS was also positively correlated with the internalizing subscale (rs = 0.262, p =0.020) and the withdrawn subscale (rs = 0.228, p <0.044) of CBCL (see Table 3).
 |
Table 3 Correlation Analysis Between TAS Score and CBCL Score |
To examine the impact of caregiver alexithymia on behavioral problems in boys and girls, we conducted separate analyses due to previous evidence of higher rates of externalizing problems in boys compared to girls across cultures.32 When analyzing girls separately, only a positive correlation was found between TAS-F1 and the somatic complaint subscale (SC) of CBCL. In contrast, for boys, there was a positive correlation between Factor 1 of TAS and the withdrawn subscale (WD) of CBCL (rs = 0.25, p =0.022), as well as a positive correlation between TAS-Total and the SC subscale of CBCL (rs = 0.28, p =0.004). However, a negative correlation was observed between TAS-F3 and the social problems subscale (SP) of CBCL in a subgroup of boys (rs =−0.264, p =0.041) (see Table 4).
 |
Table 4 Correlation Analysis Between TAS Score and CBCL Score in Boys and Girls Separately |
Discussion
The results of this study suggest that there is no significant correlation between mothers’ TAS total score and children’s CBCL total score. This indicates that the mother’s inability to express emotional identification and expression does not have a significant impact on the overall range of children’s behavioral problems. However, TAS total score has a positive correlation with the SC subscale of CBCL, which suggests that the mother’s alexithymia may have an impact on the degree of children’s somatic complaints. This is consistent with previous studies indicating that alexithymia can cause somatization33,34 and may be transmitted across generations.35 Additionally, children with somatic complaints tend to have alexithymia.36 It would be worthwhile to further investigate whether children learn to use somatic complaints as a way of coping with stress through an emotional regulation model they acquire from caregivers who have difficulty identifying and expressing emotions, or if there is a biological hereditary tendency for this phenomenon to occur.5
To examine the correlation between the mothers’ TAS factors and the CBCL variables, we observed a statistically significant positive correlation between mothers’ TAS-factor 1 and the withdrawal and internalization dimensions of children’s CBCL scores. However, no correlation was found with the externalization dimensions. This result suggests that mothers’ difficulty in distinguishing their own emotions may result in their children having more internalizing behavioral problems, such as withdrawal, somatic complaints, and anxiety/depression, but not an increase in externalizing behavioral problems.8,26,36 Another possibility is that children with more internalization behavioral problems are more likely to have alexithymia and therefore have a decreased probability of externalizing their problems.37
There is a difference in the performance of CBCL scores between boys and girls in the general population.38 Previous studies have shown that boys have significantly higher rates of externalizing problems than girls in almost every culture.32 Based on this reasoning, we conducted separate analyses for boys and girls to examine if the presence of alexithymia in caregivers has a differential impact on behavioral problems in boys and girls. Mother’s difficulty distinguishing inner emotions (indicated by a high TAS-factor 1 score) impacts the child’s internalization dimension for both boys and girls. This finding aligns with the result that a mother’s alexithymia predicts internalizing problems in children.8 Additionally, it confirms that alexithymia in children is a strong risk factor for internalizing and externalizing behaviors.39 It also supports the association between maternal alexithymia, general psychopathology in the family during childhood, and the development of alexithymic features.40,41 Another finding was that boys tend to exhibit higher levels of withdrawal and somatic problems within the internalization dimension. This can provide evidence for a particular phenomenon that although internalizing problems are more prevalent among women than men in adolescence and later stages of life, this gender difference is usually not evident among children.42,43
The negative correlation between TAS factor 3 and CBCL SP subscale in boys is difficult to explain in terms of clinical significance. The study group mainly consisted of children with ADHD and ID, who typically have more social difficulties. This could result in the mother’s evaluation of the child’s social problems as being unstable or potentially affected by interference. While alexithymia is related to social problems in both autistic and non-autistic children,44 the family’s alexithymic status and social skill levels may also influence their children’s inclination towards physical activities such as sports, with a lower social problem-solving ability observed in terms of directing their children to participate in sports.41 Therefore, this may lead mothers to overestimate their children’s social adaptive abilities. Furthermore, maternal perceptions of their children’s behavioral problems can significantly impact the study’s results.45
In sum, given that our study primarily consisted of ADHD cases, existing evidence indicates that adolescents diagnosed with ADHD exhibit significantly higher scores in somatic complaints compared to control adolescents.46 The findings demonstrated a significant association between current somatic complaints and the reporting of previous negative events, such as loss and maltreatment.47 More specifically, among Chinese male adolescents, there was a significant correlation indicating that those who experienced childhood maltreatment or adversity were more likely to report somatic complaints.48 This association may be compatible with our study due to the presence of maternal alexithymia. However, it is still important for future research to broaden the investigation and include diverse ethnic subgroups to validate these findings. Additionally, expanding the sample size would further enhance the robustness and generalizability of the results.
Strengths and Limitations
This study has several limitations: (a) Due to the small sample size, we could not control for demographic variables among caregivers and children; (b) Further statistical analysis is needed to evaluate the quantitative and qualitative aspects of the interaction between caregivers and children, particularly when a mother with high TAS-20 (or its subscale) has a child with high CBCL (or its subscale); (c) Most of the children were diagnosed with ADHD, which may have influenced the CBCL results through biological factors rather than parent-child interaction;49 (d) The fact that both the TAS and CBCL scales were completed by the mother raises the possibility that a somatization-prone mother may pay more attention to her child’s somatic complaints, potentially influencing the results; (e) The sample size for girls was small (N=16), and there were insufficient numbers for meaningful statistical analysis.
These limitations need further clarification. Future research may need to sample from the community and use larger sample sizes to minimize the influence of intrinsic underlying psychopathology such as ADHD and to have better control over variables.
Conclusion
In this preliminary study, the results indicate a positive correlation between caregivers with alexithymia and children’s behavioral problems, particularly in internalization behavioral problems. Additionally, it appears that boys are more susceptible to this impact, particularly in somatic complaints. Factors such as temperament, maternal stress, and maternal somatic symptoms play a significant role in developing somatic complaints.50 These findings serve as a foundation for further research into the impact of caregivers’ emotional regulation characteristics on a child’s development.
Data Sharing Statement
The datasets utilized and/or examined in the present study can be obtained from the corresponding author upon a reasonable request.
Ethics Approval and Informed Consent
The study protocol and each study site (approved under code C07239) obtained approval from the Institutional Review Board of Taichung Veterans General Hospital. Informed consent was obtained from all parents or guardians of individuals under the age of 16, and written consent was obtained from each participant and their guardian. The study was conducted by the principles of the Helsinki Declaration and the committee’s regulations to ensure the subjects’ rights, health, personal privacy, and dignity.
Consent for Publication
The findings described in this document have not been previously published, and none of the authors are currently submitting them to another publisher for consideration.
Acknowledgments
In this study, special thanks to Professor Wei-Jen Chen for assistance with CBCL authorization and Mr. Hao-Ran Yang for his generous guidance in CBCL statistics.
Author Contributions
YCL collected and analyzed data, prepared tables, and wrote the manuscript. WYL was responsible for the supervision of this project. All authors made a significant contribution to the work reported whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare no competing interests.
References
1. Csathó Á, Birkás B. Early-life stressors, personality development, and fast life strategies: an evolutionary perspective on malevolent personality features. Front Psychol. 2018;9:305. doi:10.3389/fpsyg.2018.00305
2. Saudino KJ. Behavioral genetics, and child temperament. J Dev Behav Pediatr. 2005;26(3):214–223. doi:10.1097/00004703-200506000-00010
3. Hopwood CJ, Donnellan MB, Blonigen DM, et al. Genetic and environmental influences on personality trait stability and growth during the transition to adulthood: a three-wave longitudinal study. J Pers Soc Psychol. 2011;100(3):545–556. doi:10.1037/a0022409
4. Hong YR, Park JS. Impact of attachment, temperament, and parenting on human development. Korean J Pediatr. 2012;55(12):449–454. doi:10.3345/kjp.2012.55.12.449
5. Derks EM, Hudziak JJ, Beijsterveldt CEM, et al. A study of genetic and environmental influences on maternal and paternal CBCL syndrome scores in a large sample of 3-year-old Dutch twins. Behav Genet. 2004;34(6):571–583. doi:10.1007/s10519-004-5585-2
6. Goerlich KS. The multifaceted nature of alexithymia - a neuroscientific perspective. Front Psychol. 2018;9:1614. doi:10.3389/fpsyg.2018.01614
7. Oskis A, Clow A, Hucklebridge F, et al. Understanding alexithymia in female adolescents: the role of attachment style. Pers Individ Dif. 2013;54(1):97–102. doi:10.1016/j.paid.2012.08.023
8. Davodi-Boroujerd G, Abasi I, Arani AM, et al. The relation between maternal personality and internalizing/ externalizing behaviors: mediating role of maternal alexithymia, children’s alexithymia and emotional regulation. Iran J Psychiatry. 2022;17(1):61–71. doi:10.18502/ijps.v17i1.8050
9. Prinzie P, Stams GJ, Deković M, Reijntjes AH, Belsky J. The relations between parents’ Big Five personality factors and parenting: a meta-analytic review. J Pers Soc Psychol. 2009;97(2):351–362.
10. Feng X, Shaw DS, Moilanen KL. Parental negative control moderates the shyness-emotion regulation pathway to school-age internalizing symptoms. J Abnorm Child Psychol. 2011;39(3):425–436. doi:10.1007/s10802-010-9469-z
11. Taylor GJ, Bagby RM, Parker JD. The alexithymia construct. A potential paradigm for psychosomatic medicine. Psychosomatics. 1991;32(2):153–164. doi:10.1016/S0033-3182(91)72086-0
12. Zeitlin SB, McNally RJ. Alexithymia and anxiety sensitivity in panic disorder and obsessive-compulsive disorder. Am J Psychiatry. 1993;150(4):658–660.
13. Lesser IM. Current concepts in psychiatry. Alexithymia. N Engl J Med. 1985;312(11):690–692. doi:10.1056/NEJM198503143121105
14. Lanzara R, Conti C, Camelio M, et al. Alexithymia and somatization in chronic pain patients: a sequential mediation model. Front Psychol. 2020;11:545881. doi:10.3389/fpsyg.2020.545881
15. Sifneos PE. Alexithymia: past and present. Am J Psychiatry. 1996;153(7 Suppl):137–142.
16. Suslow T, Donges U-S. Alexithymia components are differentially related to explicit negative affect but not associated with explicit positive affect or implicit affectivity. Front Psychol. 2017;8:1758. doi:10.3389/fpsyg.2017.01758
17. Romano L, Buonomo I, Callea A, et al. Alexithymia in young people’s academic career: the mediating role of anxiety and resilience. J Genet Psychol. 2019;180(4–5):157–169. doi:10.1080/00221325.2019.1620675
18. Jellesma FC, Rieffe C, Terwogt MM, et al. Do I feel sadness, fear, or both? Comparing self-reported alexithymia and emotional task performance in children with many or few somatic complaints. Psychol Health. 2009;24(8):881–893. doi:10.1080/08870440801998970
19. Paniccia MF, Gaudio S, Puddu A, et al. Alexithymia in parents and adolescents with generalized anxiety disorder. Clin Psychol. 2018;22(3):336–343. doi:10.1111/cp.12134
20. Rieffe C, Oosterveld P, Terwogt MM. An alexithymia questionnaire for children: factorial and concurrent validation results. Pers Individ Dif. 2006;40(1):123–133. doi:10.1016/j.paid.2005.05.013
21. Taylor GJ, Ryan D, Bagby RM. Toward the development of a new self-report alexithymia scale. Psychother Psychosom. 1985;44(4):191–199. doi:10.1159/000287912
22. Bagby RM, Parker JD, Taylor GJ. The twenty-item Toronto alexithymia scale--I. Item selection and cross-validation of the factor structure. J Psychosom Res. 1994;38(1):23–32. doi:10.1016/0022-3999(94)90005-1
23. Bagby RM, Taylor GJ, Parker JD. The twenty-item Toronto alexithymia scale--II. Convergent, discriminant, and concurrent validity. J Psychosom Res. 1994;38(1):33–40. doi:10.1016/0022-3999(94)90006-X
24. Taylor GJ, Bagby RM, Parker JD. The 20-item Toronto alexithymia scale. IV. Reliability and factorial validity in different languages and cultures. J Psychosom Res. 2003;55(3):277–283. doi:10.1016/S0022-3999(02)00601-3
25. Pedersen G, Normann‐Eide E, Eikenæs IU-M, et al. Psychometric evaluation of the Norwegian Toronto Alexithymia Scale (Tas-20) in a multisite clinical sample of patients with personality disorders and personality problems. J Clin Psychol. 2022;78(6):1118–1136. doi:10.1002/jclp.23270
26. Yuchen L, Zhanhang C. Community residents and psychiatric outpatients cannot express emotions. Taiwan Psychiatry. 2006;20(1):44–52.
27. Yuchen L, Zhanhang C. Factor analysis of the Taiwanese version of the Toronto alexithymia scale. Taiwan Psychiatry. 2003;17(4):276–282.
28. Achenbach TM, Ruffle TM. The Child Behavior Checklist and related forms for assessing behavioral/emotional problems and competencies. Pediatr Rev. 2000;21(8):265–271. doi:10.1542/pir.21.8.265
29. Yang HJ, Soong W-T, Chiang C-N, et al. Competence and behavioral/emotional problems among Taiwanese adolescents as reported by parents and teachers. J Am Acad Child Adolesc Psychiatry. 2000;39(2):232–239. doi:10.1097/00004583-200002000-00024
30. Tremblay RE. Developmental origins of disruptive behavior problems: the ‘original sin’ hypothesis, epigenetics and their consequences for prevention. J Child Psychol Psychiatry. 2010;51(4):341–367. doi:10.1111/j.1469-7610.2010.02211.x
31. Shanahan L, Calkins SD, Keane SP, et al. Trajectories of internalizing symptoms across childhood: the roles of biological self-regulation and maternal psychopathology. Dev Psychopathol. 2014;26(4 Pt 2):1353–1368. doi:10.1017/S0954579414001072
32. Ara E. Internalising and externalizing problems in adolescents: analysing the gender difference. Int J Soc Sci. 2016;6:25.
33. Lundh LG, Simonsson-Sarnecki M. Alexithymia, emotion, and somatic complaints. J Pers. 2001;69(3):483–510. doi:10.1111/1467-6494.00153
34. Taylor GJ, Parker JDA, Michael Bagby R, et al. Alexithymia and somatic complaints in psychiatric out-patients. J Psychosom Res. 1992;36(5):417–424. doi:10.1016/0022-3999(92)90002-J
35. Fukunishi I, Paris W. Intergenerational association of alexithymic characteristics for college students and their mothers. Psychol Rep. 2001;89(1):77–84. doi:10.2466/pr0.2001.89.1.77
36. Rieffe C, Nasiri H, Latifian M. Alexithymia and its relationship with physical complaints and emotional competency in children and adolescents. Iran J Psychiatr Clin Psychol. 2009;15(3):248–257.
37. Sharp C, Vanwoerden S, Van Baardewijk Y, et al. Callous-unemotional traits are associated with deficits in recognizing complex emotions in preadolescent children. J Pers Disord. 2015;29(3):347–359. doi:10.1521/pedi_2014_28_161
38. Liu J, Cheng H, Leung PW. The application of the preschool Child Behavior Checklist and the caregiver-teacher report form to Mainland Chinese children: syndrome structure, gender differences, country effects, and inter-informant agreement. J Abnorm Child Psychol. 2011;39(2):251–264. doi:10.1007/s10802-010-9452-8
39. Manninen M, Therman S, Suvisaari J, et al. Alexithymia is common among adolescents with severe disruptive behavior. J Nerv Ment Dis. 2011;199(7):506–509. doi:10.1097/NMD.0b013e3182214281
40. Karukivi M, Saarijärvi S. Development of alexithymic personality features. World J Psychiatry. 2014;4(4):91–102. doi:10.5498/wjp.v4.i4.91
41. Top E, Akil M. The effect of families’ alexithymic status and social skill levels on directing their children with intellectual disabilities to sports. Int J Dev Disabil. 2019;67(1):37–43. doi:10.1080/20473869.2019.1591055
42. Ford T, Goodman R, Meltzer H. The British Child and Adolescent Mental Health Survey 1999: the prevalence of DSM-IV disorders. J Am Acad Child Adolesc Psychiatry. 2003;42(10):1203–1211. doi:10.1097/00004583-200310000-00011
43. Van de Velde S, Bracke P, Levecque K. Gender differences in depression in 23 European countries. Cross-national variation in the gender gap in depression. Soc Sci Med. 2010;71(2):305–313. doi:10.1016/j.socscimed.2010.03.035
44. Scheerer NE, Boucher TQ, Iarocci G. Alexithymia is related to poor social competence in autistic and nonautistic children. Autism Res. 2021;14(6):1252–1259. doi:10.1002/aur.2485
45. Cho J, Ha JH, Jue J. Influences of the differences between mothers’ and children’s perceptions of parenting styles. Front Psychol. 2020;11. doi:10.3389/fpsyg.2020.552585
46. Oncü B, Öner Ö, Öner P, et al. Symptoms defined by parents’ and teachers’ ratings in attention-deficit hyperactivity disorder: changes with age. Can J Psychiatry. 2004;49(7):487–491. doi:10.1177/070674370404900711
47. Garnefski N, van Rood Y, de Roos C, et al. Relationships between traumatic life events, cognitive emotion regulation strategies, and somatic complaints. J Clin Psychol Med Settings. 2017;24(2):144–151. doi:10.1007/s10880-017-9494-y
48. Wu S, Yang T, He Y, et al. Association between hyperactivity symptoms and somatic complaints: mediating and moderating mechanisms in childhood trauma and life events among Chinese male adolescents. Front Psychiatry. 2021;12. doi:10.3389/fpsyt.2021.630845
49. Harold GT, Leve LD, Barrett D, et al. Biological and rearing mother influences on child ADHD symptoms: revisiting the developmental interface between nature and nurture. J Child Psychol Psychiatry. 2013;54(10):1038–1046. doi:10.1111/jcpp.12100
50. Wolff N, Darlington A-S, Hunfeld J, et al. Determinants of somatic complaints in 18-month-old children: the generation R study. J Pediatr Psychol. 2009;35(3):306–316. doi:10.1093/jpepsy/jsp058
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.