")
Back to Journals » International Journal of General Medicine » Volume 16
Correlating Salivary Levels of Immunoglobin E and Human Eosinophil Cationic Protein in the Aseer Cohort with Recurrent Apthous Stomatitis
Authors Assiri K, Hosmani J, Chalikkandy SN, Alkahtani AM , Alhanif RM, Alsarh SA, Patil S , Reda R , Testarelli L
Received 8 March 2023
Accepted for publication 23 June 2023
Published 10 July 2023 Volume 2023:16 Pages 2923—2931
DOI https://doi.org/10.2147/IJGM.S410061
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Khalil Assiri,1 Jagadish Hosmani,1 Sandeepa Nuchilakath Chalikkandy,1 Abdullah M Alkahtani,2 Raghad Mohammed Alhanif,3 Sarah Ahmed Alsarh,3 Shankargouda Patil,4 Rodolfo Reda,5 Luca Testarelli5
1Department of Diagnostic Dental Sciences, College of Dentistry, King Khalid University, Abha, 62529, Saudi Arabia; 2Department of Microbiology and Clinical Parasitology, College of Medicine, King Khalid University, Abha, Saudi Arabia; 3College of Dentistry, King Khalid University, Abha, Saudi Arabia; 4College of Dental Medicine, Roseman University of Health Sciences, South Jordan, UT, 84095, USA; 5Department of Oral and Maxillofacial Sciences, Sapienza University of Rome, Rome, 00161, Italy
Correspondence: Jagadish Hosmani, Department of Diagnostic Dental Sciences, College of Dentistry, King Khalid University, Abha, 62529, Saudi Arabia, Tel +966532529838, Email [email protected] Rodolfo Reda, Department of Oral and Maxillo-Facial Science, Sapienza University of Rome, Via Caserta 06, Rome, 00161, Italy, Email [email protected]
Background: Repeated Aphthous Stomatitis (RAS) is the most prevalent inflammatory disorder of the oral mucosa, characterized by recurrent emergence of single or numerous painful ulcers. RAS usually affects healthy people without systemic illnesses. There is evidence linking atopy to the progression of this illness. Immunoglobulin E (IgE) and human eosinophil cationic protein (HECP) levels in the saliva of individuals with aphthous stomatitis were assessed as allergy-related indicators.
Materials and Methods: Sixty people were assessed for this study. 30 patients with RAS were included in the patient group, while 30 healthy individuals made up for the control group. Sixty participants’ non-stimulated saliva was taken and IgE and HECP were evaluated using enzyme-linked immunosorbent assay (ELISA). Data were analyzed in SPSS 20 through the Mann–Whitney test and p< 0.05 was considered significant.
Results: The salivary level of HECP was significantly (p 0.05) higher among cases (0.83 0.70) compared to controls (0.170 0.15), whereas the salivary level of IgE was not significantly (p = 0.41) higher among cases (35.60 11.19) compared to controls (67.42 18.34).
Conclusion: Even though this study found a positive correlation between elevated HECP levels and RAS, additional research with larger sample sizes is required to identify the biological mechanisms responsible for the observed associations and to include salivary HECP levels in the RAS patient’s evaluation.
Keywords: recurrent aphthous stomatitis, saliva, immunoglobulin E, human eosinophil cationic protein
Introduction
Recurrent intraoral ulcers of the non-keratinized mucosa are the hallmark of recurrent aphthous stomatitis (RAS). Ulcers often manifest themselves first with a painful, searing feeling. Although some studies have shown a female preponderance, most agree that RAS starts in infancy and affects both sexes equally. Minor RAS is the most frequent clinical manifestation of the illness; however, there are also major and herpetiform subtypes. These ulcers are excruciatingly painful and disrupt normal oral behaviors like eating, speaking, and swallowing, hence lowering quality of life.1,2 Multiple local, systemic, immunologic, genetic, allergy, dietary, and microbiological variables have been hypothesized to contribute to the development of RAS lesions, but the exact cause of these abnormalities remains unclear.3,4 Additionally, a correlation has been postulated between RAS and psychological stress and anxiety.5 Hypersensitivity to certain dietary ingredients, oral microorganisms like Streptococcus sanguis, and microbial heat-shock proteins have been postulated as probable causal reasons, and it has been hypothesized that allergy is a contributing element in the development of RAS.3
IgE, also known as immunoglobulin E, is one of the five isotypes of human immunoglobulins, along with IgG, IgA, IgM, and IgD.6 It has a pivotal role in the development of several allergy illnesses and is crucial in the fight against parasitic infections.7 Although immunoglobulin E (IgE) was originally recognized for its role in allergic diseases, newer studies have shown that it may also play a role in the pathogenesis of auto-immune diseases.8
Serum and salivary IgA and IgG, as well as IgD and IgE, have all been shown to be altered in RAS patients, whereas higher serum IgE levels have been seen in Behcet’s illness.9
An analysis of the correlation between IgE levels and clinical and demographic parameters associated with disease severity in patients with RAS is necessary because of the growing body of evidence linking elevated serum IgE levels to dermatologic and immune-mediated conditions, as well as stress and anxiety.9
The eosinophil granulocyte helps the body fight parasites and inflammatory illnesses, including asthma and gastro-intestinal problems. Once drawn to an inflamed region, an eosinophil activates and secretes tissue-toxic mediators.10 These are basic and granule-stored proteins (eosinophil cationic protein (HECP), eosinophil peroxidase (EPO), and eosinophil protein/eosinophil-derived neurotoxin) or reactive oxygen-free radicals. HECP is found in eosinophil secretory granules. HECP is a member of the RNase A superfamily that goes by the name of RNase-3. Mature HECP is a 133-residue cationic polypeptide that resides in the matrix of the particular granule of the eosinophil and has a much higher pI of 10.8. 5.3 g of HECP is present per 106 eosinophils. The neurotoxic Gordon phenomenon is induced by HECP. HECP is toxic to several helminth parasites, hemoflagellates, bacteria, single-stranded RNA viruses, and host tissue types. Serum HECP levels may be used as a clinical tool to assess eosinophil inflammatory activity in asthma and other allergic illnesses, and levels correlate with disease severity. In vitro, HECP may operate as an antiviral agent and may contribute to the host’s defense against the respiratory syncytial virus with single-stranded RNA.11,12
Almoznino et al reviewed the relationship between serum IgE levels and demographic, clinical, and serological parameters of patients with aphthous stomatitis. They found a statistically significant relationship between mean IgE levels and female gender; age less than 12 years, onset and frequency of aphthous episodes, and C-reactive protein level (CRP).9 Jang et al found that HECP was greater in patients with allergic illnesses than in those with non-allergic inflammatory disorders. Serum levels of HECP were shown to be higher in patients with atopic dermatitis during the acute phase compared to those in the control group.11
Saliva is the consequence of serum outflow from salivary glands feeding blood vessels, and disease-induced changes in the serum are reflected in the saliva; consequently, the use of saliva appears reasonable due to its greater convenience, reduced danger of HIV and hepatitis transmission, and cheaper cost.
Due to the possibility of a link between allergy and RAS and the paucity of research on the salivary levels of IgE and HECP in Aseer province RAS patients, the current study sought to examine IgE and HECP in the saliva of minor RAS patients.
Materials and Methods
The procedures and standards of the Institutional Review Board of the College of Dentistry, King Khalid University (IRB/KKUCOD/ETH/2020-21/026 approved on 12/12/2020) were followed while using data on human subjects. The trial was authorized by the Institutional Review Board, and all patients were informed of and consented to their participation. The medical records of 30 RAS patients who satisfied the inclusion criteria and were referred to the Department of Oral Medicine in the College of Dentistry, King Khalid University, between December 24, 2020, and March 31, 2021, were analyzed.
Inclusion criteria comprised individuals between the ages of 18 and 60 with a history of at least two episodes of RAS in the previous six months and the presence of RAS ulcers at the visit. Patients with HIV, Hepatitis B or C, oral mucosal illnesses such as lichen planus, pemphigus vulgaris, and mucous membrane pemphigoid, patients who persistently take drugs linked with oral ulcerations, patients with allergic conditions like atopic dermatitis, allergic rhinitis, bronchial asthma and pregnant patients were excluded from the study.
The evaluation of recurrent aphthous stomatitis consisted of a comprehensive questionnaire followed by pertinent laboratory testing. At the first appointment, patients were interrogated in Arabic before any drugs were prescribed. The resulting information was entered into a typical intake form. The questionnaire covered demographic information (age, gender, education, and area of residence in the Aseer region), smoking habits, family history of RAS (at least one first-degree relative), and onset age of RAS.
A disposable mirror was used to inspect the oral mucosa under the dental unit light. The diagnosis of RAS was based on the following criteria: Round or ovoid oral ulcers with circumscribed margins and a white or yellow pseudo-membrane surrounded by a red halo.
The patient’s whole medical history and demographic data were also documented in a questionnaire. Saliva from 30 subjects with apparently normal oral mucosa, no drug history, and no systemic illness was collected as a control group to determine the difference in the values of IgE and HECP. All participants in the case and control groups received an explanation of the study’s objectives, and their signed consent was obtained.
The method used for saliva collection: non-stimulated saliva was collected from study subjects through the spitting method. All patients were asked to avoid eating, drinking, and brushing for 90 minutes before sampling. All saliva samples were collected between 9:00 and 12:00 AM. Every 1–2 minutes, saliva was spit into sterilized test tubes for 10 minutes. The test tubes were sealed with a screw cap and parafilm after the saliva collection, encoded, and immediately sent in a cooled container to the microbiology laboratory. In the laboratory, the saliva was centrifuged in a refrigerated centrifuge for 20 min at 1000 g to remove cellular debris. The clear saliva supernatant was transferred to a microtube using a micropipette, coded according to the test tube code, and kept at −80°C for future testing.13 In the biochemistry laboratory, we used ELISA kits to determine the concentrations of IgE and HECP in the saliva of study participants.
Determination of Total IgE Levels
Total IgE levels in saliva were determined using a commercially available sandwich ELISA kit (My Biosource, CA, USA). In brief, 100 ul of undiluted saliva samples and standards were added to ELISA plate coated wells, leaving one well blank, and incubated for 1 hour at 37C. The contents of the plates were decanted, and 100 ul of diluted detection reagent A (biotinylated anti IgE antibody) was added to all wells and incubated for 1 hour at 37 °C.
Then plates were washed manually three times, and 100 ul of diluted reagent B (Streptavidin-HRP conjugate) was added to all wells and incubated for 30 minutes at 37 °C.After washing the plates five times, 90 ul of substrate was added to all wells and incubated for 20 minutes at 37C. The reaction was stopped by the addition of 50 ul of stop solution, and the optical densities were measured at 450nm using an ELISA reader (Humareader, Human, Germany). IgE levels were determined using an ELISA plate generated regression analysis standard curve. The sensitivity of the test is 3.3 ng/mL.
Determination of Human Eosinophil Cationic Protein
Human eosinophil cationic protein (HECP) levels in saliva were determined using a commercially available sandwich ELISA kit (Genochem, Valencia, Spain). For the brief experiment, 50 ul of undiluted saliva samples and standards were added to ELISA plate coated wells, leaving one well blank, and incubated for 30 minutes at 37C. The plates were washed five times, and 50 ul of HRP-conjugate was added to all wells and incubated for 30 minutes at 37C. The plates were washed five times, and 100 ul of substrate mixture was added to all wells and incubated for 15 minutes at 37C. The reaction was stopped by the addition of 50 ul of stop solution, and the optical densities were measured at 450nm using an ELISA reader (Humareader, Human, Germany). HECP levels were determined using an ELISA plate-generated point-to-point standard curve. The sensitivity of the test is.05 ng/mL.
Statistical Analyses
The Mann–Whitney test was used for data analysis in SPSS 20. The cut-off for significance was set at a P value of 0.05.
Results
There were a total of 30 patients and 30 controls that participated in the research, with 34 (56.7%) of the participants being female and 26 (43.3%) of the participants being male. According to the findings, 44 (73.3% of participants) were not married, while 16 (26.7% of participants) were married. The overall mean age of all 60 subjects included in the study was found to be 27.76 years, with a standard deviation (SD) of 10.67 years. Table 1 shows the distribution of patients and controls according to gender and marital status. Regarding age, gender, and marital status, there was not a discernible difference between the two groups at all.
 |
Table 1 Distribution of Patients and Controls According to Gender and Marital Status |
In an intergroup comparison using the Mann Whitney U-test, it was discovered that there was no significant difference between patients and controls in terms of IgE ng/mL (p = 0.416). However, there was a statistically significant difference between the two groups in terms of HECP ng/mL (p 0.05) (Table 2).
 |
Table 2 Intergroup Comparison Using Mann Whitney U-Test Showed No Significant Difference Between Patients and Controls with Respect to IgE Ng/Ml (p=0.416). However, HECP Ng/Ml Differed Significantly Between the Two Groups (P<0.05) |
Discussion
Most people have experienced the anguish of repeated episodes of recurrent aphthous stomatitis (RAS), an inflammatory illness of the oral mucosa characterized by the recurrence of one or more painful ulcers. People who are otherwise healthy and have no other systemic disorders are more likely to get RAS. The incidence of RAS varies from 2% to 50% of the general population, depending on the population studied, environmental factors, and diagnostic criteria.14–16
RAS is more frequent among women over 40, whites, nonsmokers, and those with a high socioeconomic standing, according to studies. In most cases, the disorder manifests in infancy and progresses with age. Despite much research and therapeutic focus, RAS’s genesis and pathology remain a mystery.17
Aphthous ulcers may be caused by a number of factors, including heredity, viral and bacterial infections, stress, food allergies, and trauma to the area. Homocysteine, iron, vitamin B12, vitamin D, folic acid, and heme are all associated with the RAS. An impaired immune response and inflammation may lead to the development of an apthous ulcer in RAS in those who are genetically susceptible.18,19
In contrast to other biological substances, collecting saliva poses little risk to the subject. Approximately 0.5% of the fluid is made up of secretory immunoglobulin A, lysozyme, electrolytes, mucus, glycoproteins, enzymes, and peptide hormones. Saliva usually reflects the concentration of peptides in the blood and plays a crucial function in oral health by preserving the integrity of the oral mucosal membrane. Unlike serum and biopsies, people are more likely to accept a saliva sample.20,21
In light of the hypothesis that allergic reactions may play a role in the development of these ulcers, the present work sought to compare the salivary levels of IgE and HECP in a cohort from the Aseer region with active apthous ulcers and healthy controls. Eosinophils are responsible for the production of HECP, which is then triggered by immunoglobulin E (IgE). HECP is a mediator of allergic inflammation. This leukocytic protein is toxic to neurons as well as the membrane of epithelial cells; nevertheless, the levels of this protein do not exactly correlate with the number of eosinophils in the peripheral blood.22
Multiple studies have shown a connection between HECP and a number of allergy diseases and illnesses. Researchers Keles et al23 discovered persistently elevated levels of HECP in the serum of asthmatic patients. In their investigation of allergic illnesses, Jang et al concluded that HECP may serve as biomarkers of allergic disorders.11
Acute and chronic stages of atopic dermatitis in 21 patients were investigated by Angelova-Fischer et al. When compared to other factors, HECP levels in the blood were analyzed. Acute atopic dermatitis was associated with significantly elevated levels of these parameters in the blood compared to healthy controls. As the patient’s condition improved, so did the levels.12
According to the findings of a study carried out by Lee et al, children suffering from atopic dermatitis who reduced the number of ready-made meals they consumed had an improvement in both their blood HECP levels and their clinical symptoms.24
Schmekel et al observed that detrimental eosinophilic activity or increased HECP levels in the peripheral circulation enhance HECP levels in asthmatic patients’ saliva, which increases oral mucosa permeability.25
An investigation along the same lines as ours conducted by Mollashahi et al found a significant difference (p = 0.001) in the salivary HECP levels of apthous stomatitis patients (26.936.95 ng/mL) in comparison to the control group (21.976.72 ng/mL).26 The findings of our study echoed the similar findings of a significant difference in salivary HECP levels when compared between Aphthous and the control group presented in Figure 1.
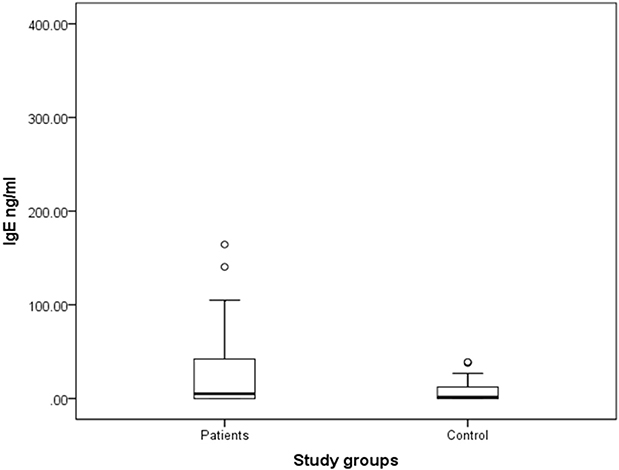 |
Figure 1 Boxplot for salivary level of HECP (ng/mL) in patients with recurrent aphthous stomatitis and controls. The salivary level of HECP was significantly (p<0.05) higher among cases (0.83 ± 0.70) compared to controls (0.170 ± 0.15). |
There have only been a small number of studies that have been reported in the scientific literature; however, the ones that have been carried out have demonstrated that the levels of HECP in saliva and serum do not reflect the disease process and that there is no significant difference between the group that is affected and the group that serves as a control.
By comparing the levels of salivary and serum HECP, Krgezen et al sought to determine if there may be a connection between the levels of salivary HECP and the diagnosis of allergic rhinitis. Despite finding higher levels of HECP in the study group’s saliva and serum, it was concluded that there was no discernible difference in these levels between the control and study groups. It was hypothesized that this could be due to the influence of numerous factors, including age, the seasons, and circadian rhythm, on HECP levels. Additionally, they discovered no connection between the research group’s serum IgE level and the amounts of HECP in the serum and saliva.27
In juvenile asthmatics, Koh et al assessed whole saliva and serum HECP, asthma severity, cockroach and dust mite sensitivity, and concurrent allergic rhinitis and atopic dermatitis. Salivary HECP was unaffected by asthma severity or asthma medications. The presences of atopic diseases, skin prick test positivity, or wheal size were unrelated to serum and salivary HECP. Salivary HECP is unrelated to serum HECP.28
Human immunoglobulin E, often known as IgE, is one of the five isotypes that has been shown to play a significant role in the development of a variety of allergic conditions. Since IgE-coated lymphocytes and mast cells have been found in biopsies taken from RAS ulcers as well as peripheral blood, it may be concluded that they play a role in the pathogenesis of RAS ulcers.9,26
According to Almoznino et al, RAS patients had higher serum IgE levels. Additionally, there was a strong correlation between serum IgE levels and female sex, younger age, and an earlier beginning of RAS episodes.9 In 27 of the 39 patients with RAS that were studied by Fornasa and Gallina, clinical and laboratory evidence of atopy was found. Fornasa and Gallina looked at factors such as personal and family history of atopy, serum IgE levels, skin prick test, skin patch test, and specific IgE Ab to determine the relationship between RAS and atopy [29]. In addition to revealing a connection between RAS and atopy, Ruan et al found that individuals with RAS had significantly higher blood levels of IgE compared to controls in their study.29
Analysis carried out by Mollashahi et al uncovered a disparity in the levels of salivary IgE that was statistically significant (p = 0.001) between the Aphthous group (1.110.65 Iu/mL) and the control group (0.730/39 Iu/mL).26 In contrast, the present investigation did not find any statistically significant differences in the levels of salivary IgE between the test group and the control group, even though there was a clear distinction between the two groups depicted in Figure 2.
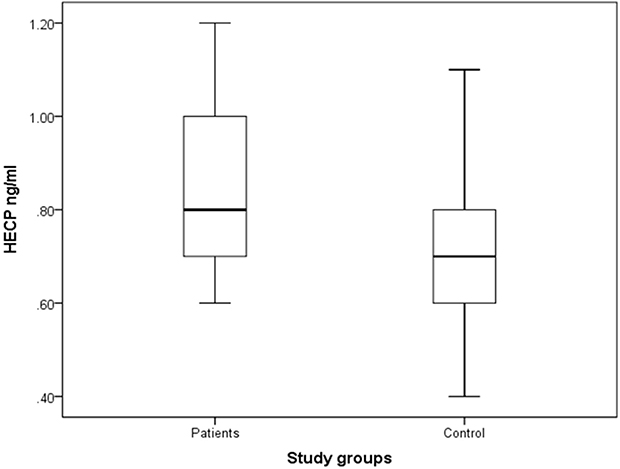 |
Figure 2 Boxplot for salivary level of IgE (ng/mL) in patients with recurrent aphthous stomatitis and controls. The salivary level of IgE was not significantly (p=0.41) higher among cases (35.60 ± 11.19) compared to controls (67.42 ± 18.34). |
It should be noted that HECP and IgE expression is tightly regulated in the absence of disease. The positive correlation between elevated HECP levels and RAS, in our opinion, was the most fascinating result of our investigation. According to our knowledge, this research is the first to examine links between high salivary HECP and RAS disease features in the Aseer community. The findings of this study indicate that salivary HECP levels can be used as a biomarker to monitor the clinical course of Aphthous ulcers in affected individuals and can even potentially be used as a yardstick to assess the efficacy of the treatment modality used to treat these lesions. Differences in salivary HECP levels were statistically significant between the Aphthous ulcer patient group and the control group. However, the salivary IgE levels were not statistically significant between the two studied groups.
The study’s limitations were a smaller sample size and the absence of measurements of salivary HECP and IgE levels at various phases (initial, intermediate, and terminal) of Aphthous lesions. Also, the different salivary flow rates between the diseased group and the control group can have a bearing on the outcome. The present study’s results have prompted further, more extensive monitoring of salivary HECP and IgE levels among members of the native Aseer tribe. Comparative evaluation of serum and salivary HECP and IgE levels will be essential to establishing the sensitivity and specificity of these biomarkers in the saliva of RAS patients. Evaluation of salivary HECP and IgE at the different stages of RAS will also be considered in the future.
Conclusion
Saudi Arabia’s Aseer area has never researched salivary HECP and IgE levels. RAS patients have higher HECP than controls. This research found that Aseer oral RAS patients had greater salivary HECP than controls. However, salivary IgE levels did not differ significantly between RAS patients and controls. We would like to add a caveat that, though the HECP levels were significantly higher in RAS patients than in controls and the salivary IgE levels did not differ significantly between the RAS and control groups, sequential saliva sampling is needed to correlate concentrations to the disease course to affirmatively state that salivary HECP levels can be used as a biomarker to monitor the clinical course of aphthous ulcers in affected individuals.
The relationship between clinical features and higher HECP and IgE levels needs further investigation into the molecular causes. The small size of our study’s sample is its principal limitation. Financial constraints meant that only saliva samples could be tested for HECP and IgE. Problematically, saliva samples from individuals with RAS were only taken during the ulcer’s active phase. Inequalities are highest during the early stage of ulcer development, when inflammation is expected to be at its worst.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The study was approved by the Institutional Review Board of the College of Dentistry, King Khalid University (IRB/KKUCOD/ETH/2020-21/026 approved on 12/12/2020. All participants signed informed consent in accordance with the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was not supported by any external funding.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Giannetti L, Murri Dello Diago A, Lo Muzio L. Recurrent aphtous stomatitis. Minerva Dent Oral Sci. 2018;67(3). doi:10.23736/s0026-4970.18.04137-7
2. Chattopadhyay A, Shetty KV. Recurrent aphthous stomatitis. Otolaryngol Clin North Am. 2011;44(1):79–88. doi:10.1016/j.otc.2010.09.003
3. Chavan M, Jain H, Diwan N, Khedkar S, Shete A, Durkar S. Recurrent aphthous stomatitis: a review. J Oral Pathol Med. 2012;41(8):577–583. doi:10.1111/j.1600-0714.2012.01134.x
4. Akintoye SO, Greenberg MS. Recurrent aphthous stomatitis. Dent Clin North Am. 2014;58(2):281–297. doi:10.1016/j.cden.2013.12.002
5. Huling LB, Baccaglini L, Choquette L, Feinn RS, Lalla RV. Effect of stressful life events on the onset and duration of recurrent aphthous stomatitis. J Oral Pathol Med. 2011;41(2):149–152. doi:10.1111/j.1600-0714.2011.01102.x
6. Schroeder HW, Cavacini L. Structure and function of immunoglobulins. J Allergy Clin Immunol. 2010;125(2):S41–S52. doi:10.1016/j.jaci.2009.09.046
7. Stone KD, Prussin C, Metcalfe DD. IgE, mast cells, basophils, and eosinophils. J Allergy Clin Immunol. 2010;125(2):S73–S80. doi:10.1016/j.jaci.2009.11.017
8. Anand P, Singh B, Jaggi AS, Singh N. Mast cells: an expanding pathophysiological role from allergy to other disorders. Naunyn-Schmiedeb Arch Pharmacol. 2012;385(7):657–670. doi:10.1007/s00210-012-0757-8
9. Almoznino G, Zini A, Mizrahi Y, Aframian D. Elevated serum I g E in recurrent aphthous stomatitis and associations with disease characteristics. Oral Dis. 2013;20(4):386–394. doi:10.1111/odi.12131
10. Kita H. Eosinophils: multifaceted biological properties and roles in health and disease. Immunol Rev. 2011;242(1):161–177. doi:10.1111/j.1600-065x.2011.01026.x
11. Jang WR, Choi JW, Nahm CH, et al. Significance of serum eosinophil cationic protein and high-sensitivity C-reactive protein levels in patients with allergic and non-allergic inflammatory diseases. Lab Med. 2012;2(1):20. doi:10.3343/lmo.2012.2.1.4
12. Angelova-Fischer I, Hipler UC, Bauer A, et al. Significance of interleukin-16, macrophage-derived chemokine, eosinophil cationic protein and soluble E-selectin in reflecting disease activity of atopic dermatitis-from laboratory parameters to clinical scores. Br J Dermatol. 2006;154(6):1112–1117. doi:10.1111/j.1365-2133.2006.07201.x
13. Mohamed R, Campbell J, Cooper‐White J, Dimeski G, Punyadeera C. The impact of saliva collection and processing methods on CRP, IgE, and Myoglobin immunoassays. Clin Transl Med. 2012;1(1). doi:10.1186/2001-1326-1-19
14. Cui RZ, Bruce AJ, Rogers RS. Recurrent aphthous stomatitis. Clin Dermatol. 2016;34(4):475–481. doi:10.1016/j.clindermatol.2016.02.020
15. Tuzun B, Wolf R, Tuzun Y, Serdaroglu S. Recurrent aphthous stomatitis and smoking. Int J Dermatol. 2000;39(5):358–360. doi:10.1046/j.1365-4362.2000.00963.x
16. Rivera-Hidalgo F, Shulman J, Beach M. The association of tobacco and other factors with recurrent aphthous stomatitis in an US adult population. Oral Dis. 2004;10(6):335–345. doi:10.1111/j.1601-0825.2004.01049.x
17. Crivelli MR, Aguas S, Adler I, Quarracino C, Bazerque P. Influence of socioeconomic status on oral mucosa lesion prevalence in schoolchildren. Community Dent Oral Epidemiol. 1988;16(1):58–60. doi:10.1111/j.1600-0528.1988.tb00556.x
18. Sun A, Chen HM, Cheng SJ, et al. Significant association of deficiencies of hemoglobin, iron, vitamin B12, and folic acid and high homocysteine level with recurrent aphthous stomatitis. J Oral Pathol Med. 2014;44(4):300–305. doi:10.1111/jop.12241
19. Compilato D, Carroccio A, Calvino F, Di Fede G, Campisi G. Haematological deficiencies in patients with recurrent aphthosis. J Eur Acad Dermatol Venereol. 2009;24(6):667–673. doi:10.1111/j.1468-3083.2009.03482.x
20. Hegde S, Ajila V, Babu S, Kumari S, Ullal H, Madiyal A. Evaluation of salivary tumour necrosis factor–alpha in patients with recurrent aphthous stomatitis. Eur Oral Res. 2019;52(3):157–161. doi:10.26650/eor.2018.543
21. Jose M, Dadhich M, Prabhu V, Pai V, D′Souza J, Harish S. Serum and salivary sialic acid as a biomarker in oral potentially malignant disorders and oral cancer. Indian J Cancer. 2014;51(3):214. doi:10.4103/0019-509x.146720
22. McBrien CN, Menzies-Gow A, Ducceschi M. The biology of eosinophils and their role in asthma. Front Med. 2017;4:4. doi:10.3389/fmed.2017.00093
23. Keleş E, Yazgan H, Gebeşçe A. To evaluate serum eosinophil cationic protein and total IgE concomitantly may predict the persistence of wheezing in young children. ISRN Pediatr. 2012;2012:1–4. doi:10.5402/2012/168379
24. Lee JM, Jin HJ, Noh G, Lee SS. Effect of processed foods on serum levels of eosinophil cationic protein among children with atopic dermatitis. Nutr Res Pract. 2011;5(3):224. doi:10.4162/nrp.2011.5.3.224
25. Schmekel B, Ahlner J, Malmström M, Venge P. Eosinophil cationic protein (ECP) in saliva: a new marker of disease activity in bronchial asthma. Respir Med. 2001;95(8):670–675. doi:10.1053/rmed.2001.1123
26. Farhad-Mollashahi L, Honarmand M, Nakhaee A, Kamalzadeh S, Amini S. Salivary levels of IgE and ECP in patients with recurrent aphthous stomatitis. J Clin Exp Dent. 2020;e9–e12. doi:10.4317/jced.56254
27. Kirgezen T, Araz Server E, Savran Turanoglu F, Yigit O, Uzun H, Durmus S. Salivary eosinophil cationic protein in allergic rhinitis. Turk Arch Otorhinolaryngol. 2019;57(2):91–94. doi:10.5152/tao.2019.4127
28. Koh GCH, Pei-Chi Shek L, Kee J, Wee A, Ng V, Koh D. Saliva and serum eosinophil cationic protein in asthmatic children and adolescents with and without allergic sensitization. J Asthma. 2010;47(1):61–65. doi:10.3109/02770900903350499
29. Ruan HH, Li GY, Duan N, et al. Frequencies of abnormal humoral and cellular immune component levels in peripheral blood of patients with recurrent aphthous ulceration. J Dent Sci. 2018;13(2):124–130. doi:10.1016/j.jds.2017.09.003
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.