Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
COPD Exacerbations, Air Pollutant Fluctuations, and Individual-Level Factors in the Pandemic Era
Authors Mikaeeli S, Doiron D, Bourbeau J, Li PZ, Aaron SD ![]() , Chapman KR, Hernandez P
, Chapman KR, Hernandez P ![]() , Maltais F
, Maltais F ![]() , Marciniuk DD
, Marciniuk DD ![]() , O'Donnell DE, Sin DD
, O'Donnell DE, Sin DD ![]() , Walker BL, Tan WC
, Walker BL, Tan WC ![]() , Rousseau S
, Rousseau S ![]() , Ross BA
, Ross BA ![]()
Received 29 September 2024
Accepted for publication 23 February 2025
Published 17 March 2025 Volume 2025:20 Pages 735—751
DOI https://doi.org/10.2147/COPD.S498088
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Sahar Mikaeeli,1– 3 Dany Doiron,1 Jean Bourbeau,1,4,5 Pei Zhi Li,1 Shawn D Aaron,6 Kenneth R Chapman,7 Paul Hernandez,8 François Maltais,9 Darcy D Marciniuk,10 Denis E O’Donnell,11 Don D Sin,12 Brandie L Walker,13 Wan C Tan,12 Simon Rousseau,3 Bryan A Ross1,4,5 On behalf of the CanCOLD Collaborative Research Group and the Canadian Respiratory Research Network
1Respiratory Epidemiology and Clinical Research Unit, Centre for Outcomes Research and Evaluation, Research Institute of the McGill University Health Centre (RI-MUHC), Montreal, Quebec, Canada; 2Division of Experimental Medicine, Department of Medicine, McGill University Health Centre, Montreal, Quebec, Canada; 3Meakins-Christie Laboratories, Research Institute at McGill University Health Centre, Montreal, Canada; 4Division of Respiratory Medicine, Department of Medicine, McGill University Health Centre, Montreal, Quebec, Canada; 5Montreal Chest Institute, McGill University Health Centre, Montreal, QC, Canada; 6The Ottawa Hospital Research Institute, University of Ottawa, Ottawa, Ontario, Canada; 7Toronto General Hospital Research Institute, University of Toronto, Toronto, Ontario, Canada; 8Department of Medicine, Faculty of Medicine, Dalhousie University, Halifax, Nova Scotia, Canada; 9Institut Universitaire de Cardiologie et de Pneumologie de Québec, Université Laval, Québec, Québec, Canada; 10Respiratory Research Centre and Division of Respirology, Critical Care and Sleep Medicine; University of Saskatchewan, Saskatoon, Saskatchewan, Canada; 11Department of Medicine, Queen’s University, Kingston, Ontario, Canada; 12Centre for Heart Lung Innovation, St. Paul’s Hospital, University of British Columbia, Vancouver, British Columbia, Canada; 13Department of Medicine, University of Calgary, Calgary, Alberta, Canada
Correspondence: Bryan A Ross, Respiratory Epidemiology and Clinical Research Unit (RECRU), Research Institute of the McGill University Health Centre (RI-MUHC), 5252 De Maisonneuve, Room 3D.57, Montreal, QC, H4A 3S5, Canada, Tel +1-514-843-1465, Email [email protected]
Purpose: Pandemic-era associations between air pollutant exposures and exacerbations of chronic obstructive pulmonary disease (COPD) are under-explored. Given the considerable observed pandemic-era pollutant fluctuations, these associations were investigated along with possible individual-level risk factors.
Patients and Methods: Participants with spirometry-confirmed COPD from Canadian Cohort Obstructive Lung Disease (CanCOLD) were included, with data collected before (“pre-pandemic”) and during (“pandemic”) the COVID-19 pandemic. Nitrogen dioxide (NO2), fine particulate matter (PM2.5), ground-level ozone (O3), total oxidant (Ox) and weather data were obtained from national databases. Associations between each air pollutant and “symptom-based” exacerbations (increased dyspnea or sputum volume/purulence ≥ 48hrs) and “event-based” exacerbations (“symptom-based” plus requiring antibiotics, corticosteroids, or unscheduled healthcare use) were estimated in separate models. Generalized estimating equations (GEE) models were reported as rate ratios (RRs) per interquartile range (IQR) increment in pollutant concentration with 95% confidence intervals (95% CIs).
Results: NO2, PM2.5, and Ox (NO2+O3) concentrations (but not O3) fell significantly during the pandemic. In the 673 participants with COPD included, both symptom-based and event-based exacerbation rates were likewise significantly higher during the pre-pandemic period. During the pre-pandemic period, Ox was positively associated with symptom-based exacerbations (RR: 1.21 [1.08,1.36]). During the pandemic period, Ox was positively associated with symptom-based (1.46 [1.13,1.89]) and event-based (1.43 [1.00,2.05]) exacerbations. Fewer self-reported pandemic protective behaviors, and higher viral infectious symptoms, were also associated with exacerbations. In stepwise multivariable risk-factor analyses, female gender (1.23 [1.04,1.45] and 1.41 [1.13,1.76]) and co-morbid asthma (1.65 [1.34,2.03] and 1.54 [1.19,2.00]) were associated with symptom-based and event-based exacerbations, respectively, blood eosinophils (1.42 [1.10,1.84]) were associated with event-based exacerbations, and each IQR increment in Ox was associated with symptom-based exacerbations (1.31 [1.06,1.61]).
Conclusion: Ox exposure was consistently associated with symptom-based COPD exacerbations, and female gender, co-morbid asthma, and blood eosinophilia were found to be relevant risk factors.
Plain Language Summary: Previous research has identified air pollution as a relevant non-infectious trigger for episodic ‘lung attacks’, referred to as exacerbations, in patients living with chronic obstructive pulmonary disease (COPD). Very few studies, however, have studied this relationship during the COVID-19 pandemic. During that time, there were large fluctuations in key forms of air pollution (air pollutants). The few studies available used population-level approaches and relied on hospital administrative coding of visits to classify the disease and to identify exacerbation events. This approach may lead to potentially missing clinically important non-severe events and may limit individual-level risk factor assessment around this period.
This study was conducted in participants with COPD as confirmed by the gold-standard test, spirometry, who were living in 9 Canadian cities across 6 provinces. The results showed that while the air pollutants nitrogen dioxide (NO2), fine particulate matter (PM2.5), and total oxidant (Ox) concentrations were all notably higher before the pandemic (pre-pandemic), only ambient Ox concentration was consistently associated with exacerbations. This relationship was seen across both pre-pandemic and pandemic periods. Female gender, co-morbid asthma, and eosinophilia were identified as notable risk factors for exacerbations and were effect modifiers for the association between Ox exposure and exacerbations. This study adds to a very limited existing literature on the relationship between air pollutant fluctuations and exacerbations of COPD around the pandemic era and highlights important risk factors to guide targeted public health and exposure response interventions.
Keywords: Chronic obstructive pulmonary disease, acute exacerbations of chronic obstructive pulmonary disease, ambient air pollution, COVID-19 pandemic, total oxidant concentration
Introduction
Chronic obstructive pulmonary disease (COPD) is the third-leading cause of global morbidity and mortality worldwide,1,2 and exacerbations of COPD (ECOPDs) represent a major burden to patients and health systems. The modern exacerbation framework recognizes air pollution as a relevant non-infectious precipitant.3
The COVID-19 pandemic resulted in considerable global fluctuations in air pollutant concentrations. During recurrent lockdowns across Europe, North America, and Asia,4,5 the ambient concentrations of most air pollutants including nitrogen dioxide (NO2) and fine particulate matter (PM2.5) decreased, while an increase in ozone (O3) concentrations was observed.6,7 Total oxidant (Ox), the arithmetic sum of NO2 and O3 concentrations and an indicator of ambient oxidative capacity,8 varied regionally during the pandemic, increasing in some areas due to elevated O3 despite reduced NO2, and were influenced by complex atmospheric dynamics and regional factors that were not uniform across various geographic regions.9–14
Within the limited literature focused strictly on these pandemic-era phenomena and associations, some reported an observed reduction in COPD exacerbation rates and COPD-related admissions,15–18 though few actually explored air pollution-ECOPD associations.18 Studies that did estimate these pandemic era associations mainly pursued an ecological approach, with reliance on International Classification of Disease (ICD) codes for disease diagnosis,16–19 which may risk disease and outcome misclassification and tend to neglect non-severe events that are still clinically relevant.20,21 More detailed information of study participants, had they been available in those ecological studies, may have allowed for investigation into individual-level risk factors in the observed pandemic-era “pollutant-exacerbation” associations.
The present study sought first to characterize the fluctuations in ambient air pollution during and preceding the COVID-19 pandemic in 9 Canadian cities, and to determine COPD exacerbation rates over these same periods. The main objective was to determine the relationship between each air pollutant and COPD exacerbation rates with consideration of relevant confounders. The secondary objective was to identify individual-level risk factors in relation to these associations. We hypothesized a positive association between ambient air pollutant concentration fluctuations and COPD exacerbation rates, and that certain risk factors may emerge in these relationships. Some of the results of this study have been previously reported in the form of an abstract.22
Material and Methods
Population and Study Periods
Data from Canadian Cohort Obstructive Lung Disease (CanCOLD), a prospective longitudinal cohort study described previously (see online data Supplement), were utilized. The present study included participants diagnosed with COPD by spirometry (post-bronchodilator FEV1/FVC<0.7) with telephone interview exacerbation data available. Two distinct periods of observation were included: the “pre-pandemic” period (July 2012-December 2019, inclusive) and the “COVID-19 pandemic” period (January 2020-December 2022, inclusive). Institutional review board approval was obtained, and all participants provided written informed consent.
Study Outcomes, Air Pollution Exposure, and Covariates
Exacerbations were collected prospectively via structured telephone interview at three-month intervals throughout both study periods. Exacerbations were defined as either “symptom-based” (increase in dyspnea, sputum volume or sputum purulence lasting ≥48 hours) or “event-based” (meeting “symptom-based” criteria plus requiring either antibiotic or systemic corticosteroid treatment or unscheduled visit/hospitalization).20,21,23,24 Exacerbation rates were calculated for each of the two study periods.
Collection and aggregation of daily air pollutant concentrations and weather covariates were performed as reported previously25 (see Supplement). Air pollution exposure data were obtained from the federal National Air Pollution Surveillance (NAPS) monitoring network using fixed-location monitoring stations within each of the nine CanCOLD cities.
Additional Pandemic-Specific Covariates
From May 2020 onwards, a monthly “COVID-19 Questionnaire” was administered to collect relevant behaviors, symptoms, and events directly or indirectly related to the COVID-19 pandemic (see Supplement text, and Supplement Figure S1, for details).
Statistical Analysis
Differences between the pre-pandemic and COVID-19 pandemic periods were compared using generalized estimating equations (GEE) with normal distribution, adjusted for season and for temperature and humidity (restricted cubic splines). Differences in symptom-based and event-based exacerbation rates between the two study periods were compared using unadjusted and adjusted GEE models with negative binomial distribution (see Supplement).
The association between air pollutant concentrations and exacerbation rates across both study periods were estimated by fitting GEE models, first by period only and secondly following adjustment for period as well as age, gender, season, and temperature and humidity (spline terms). Within-period models were also fitted. Offset was used to account for differing period follow-up durations.
Sensitivity analyses were conducted in the subgroup of participants with COVID-19 Questionnaire responses available, in order to estimate the association between behavioral “protective” measures and markers of viral infection status with exacerbations. These two variables were inserted into the within-COVID-19 pandemic period models, to retest the associations between each air pollutant and exacerbation rates within this period.
Finally, the determination of relevant individual-level susceptibilities or ‘risk factors’ was investigated using multivariable analyses with a stepwise approach (see Supplement). Subgroup differences by self-reported gender, self-reported presence or absence of physician-diagnosed co-morbid asthma, and blood eosinophil count (Eos: <300 versus ≥300 counts/microliter and <3% versus ≥3%) were analyzed using of the Wald test for effect modification.
All GEE models used an exchangeable correlation structure. Results are presented as point estimates, or as rate ratios (RRs), as appropriate, with 95% confidence intervals (95% CIs). Adjustments for multiple comparisons were not made. All statistical analyses were conducted using SAS statistical software, version 9.4 (SAS Institute, Cary, North Carolina, USA).
Results
Study Population and Baseline Characteristics
In total, 673 of 1,561 CanCOLD study participants met all eligibility criteria and were included (Figure 1). Of these, 413 participants had COVID-19 Questionnaire data available for inclusion in within-COVID-19 pandemic period sub-analyses with behavioral and viral infection factors.
 |
Figure 1 Flow diagram of study participants. Abbreviations: COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in one second; FVC, forced vital capacity. Symbols: n, number. |
Baseline characteristics and missingness by variable are presented in Table 1. Participants were older adults with a slight preponderance of males, and just over half with mild (GOLD 1) COPD. Co-morbid self-reported physician-diagnosed asthma was present in 32.1% of participants, and among participants with blood eosinophil data available, 151 (25.5%) had Eos ≥300 counts/microliter.
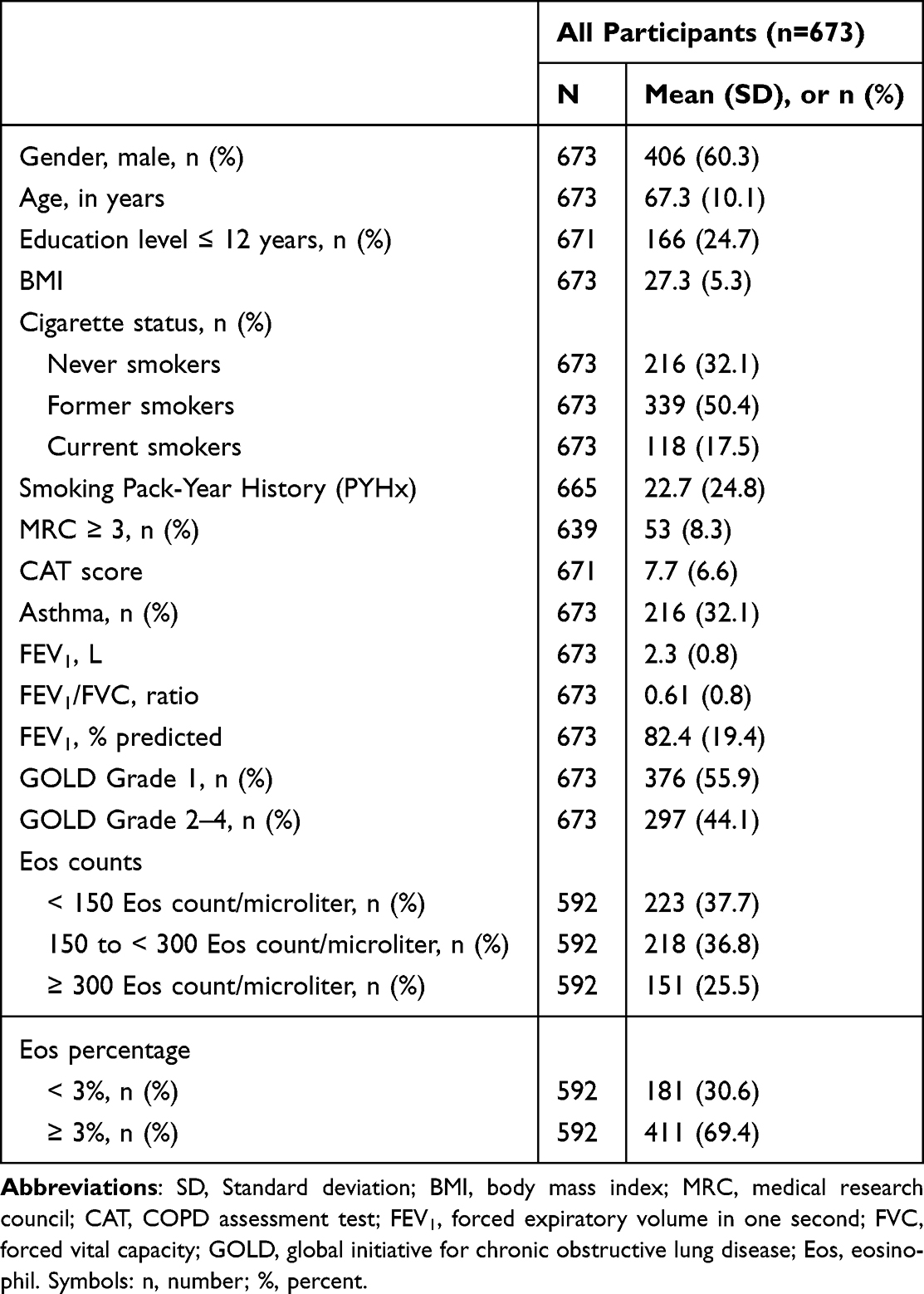 |
Table 1 Characteristics of Study Participants |
In the pre-pandemic period, the median follow-up duration was 77.3 months (IQR: 59.2–83.9). During this time, the symptom-based exacerbation rate was 0.41 events per person-year (95% CI: 0.37–0.45), and the event-based exacerbation rate was 0.22 events per person-year (95% CI: 0.19–0.25). In the COVID-19 pandemic period, the median follow-up duration was 33.8 months (IQR: 29.5–35.1). The symptom-based exacerbation rate decreased to 0.25 events per person-year (95% CI: 0.21–0.29), while the event-based exacerbation rate dropped to 0.15 events per person-year (95% CI: 0.12–0.18).
Air Pollutant Concentrations, Exacerbation Rates, and Air Pollutant-Exacerbation Associations
Median and IQR air pollutant concentrations, by both study city and study period, are shown in Table 2, and are presented by both season and study period in Figure 2. While seasonal variations were observed within both periods, compared with the pre-pandemic period the COVID-19 pandemic period was associated with lower NO2 (−1.97 [−2.08, −1.86] ppb), PM2.5 (−0.53 [−0.59, −0.47] μg/m3), and Ox (−1.44 [−1.61, −1.27] ppb) concentrations. As previously reported,6,7 O3 concentrations were significantly higher during the COVID-19 pandemic period (0.36 [0.18, 0.55] ppb). Heterogeneity was observed across study sites.
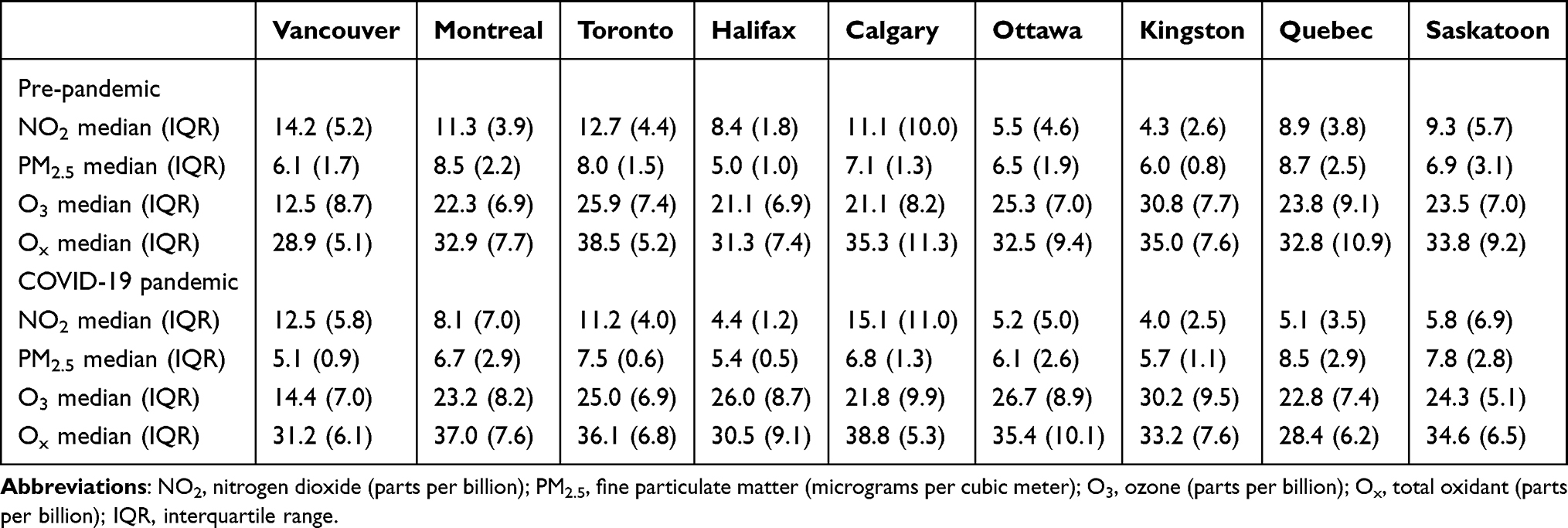 |
Table 2 Distribution of Median Air Pollutant Concentrations Stratified by the Two Periods and the Nine Study Centers |
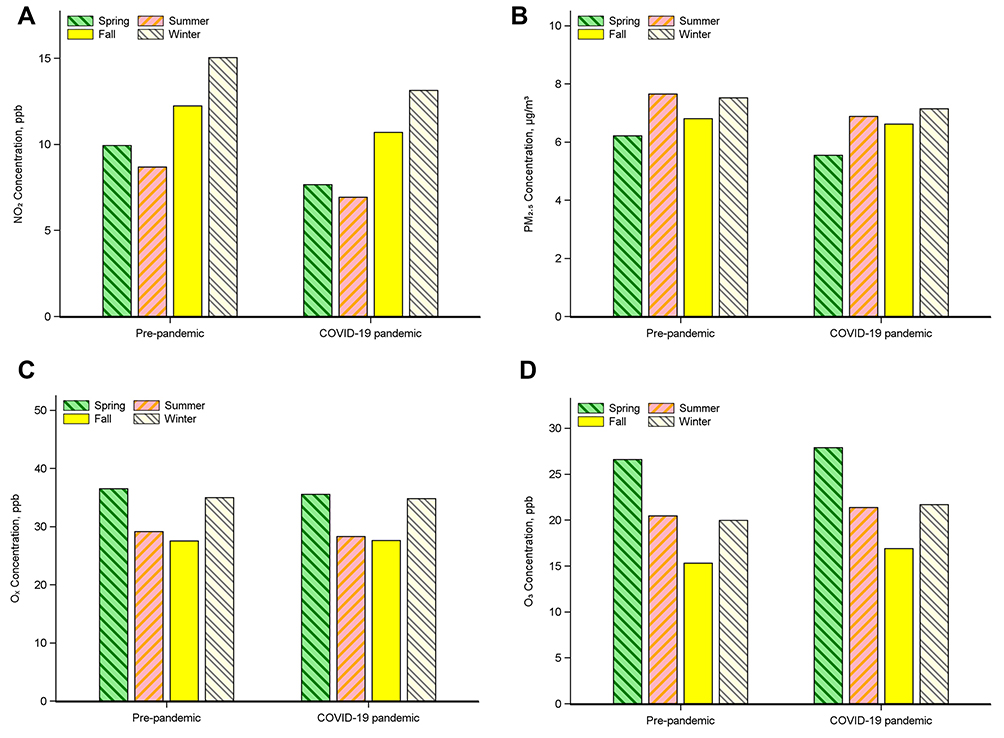 |
Figure 2 Air pollutant concentration in each study period for (A) nitrogen dioxide (NO2), parts per billion (ppb); (B) fine particulate matter (PM2.5), micrograms per cubic meter (μg/m3); (C) total oxidant (Ox), parts per billion (ppb); and (D) ozone (O3), parts per billion (ppb). |
Compared with the pre-pandemic period, significant reductions were observed in unadjusted symptom-based (RR: 0.58 [0.50, 0.68]) and event-based (0.66 [0.55, 0.80]) exacerbation rates, as well as in adjusted rates (Figure 3).
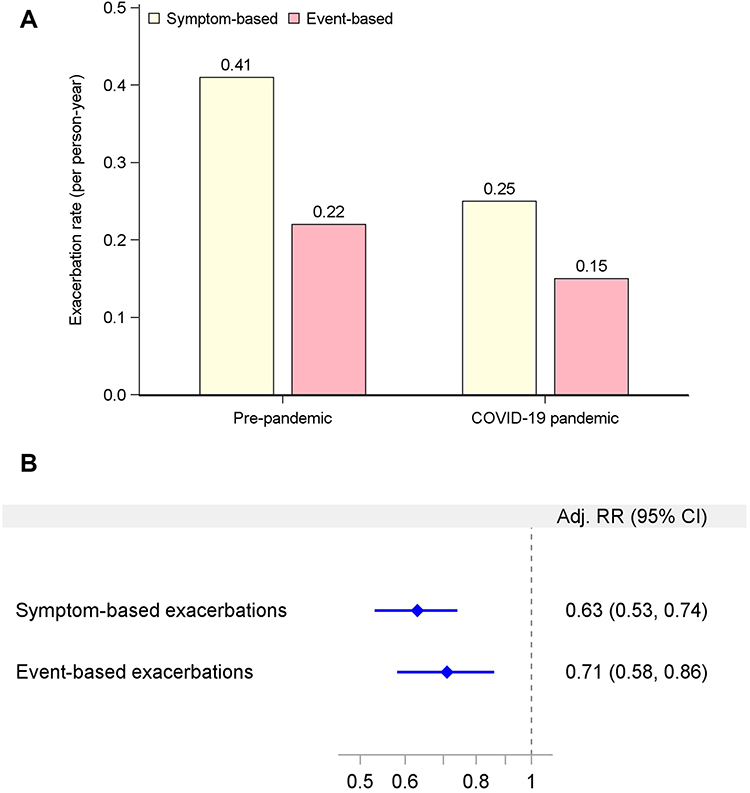 |
Figure 3 Comparison of symptom-based and event-based exacerbations between the two study periods, presented as rates in person-years (A) and as rate ratios (RR) and corresponding 95% confidence intervals (CI) estimated using Generalized Estimating Equation (GEE) models (B), adjusted (Adj) for baseline age, gender, season, and the spline terms for temperature and humidity. Symbols: %, percent. |
Regarding the association between each air pollutant and exacerbations across both periods, an IQR increment in NO2 and in Ox were each associated with an increase in symptom-based and event-based exacerbation rates, while no associations were observed with each IQR increment in PM2.5 or O3 exposure (see Supplement Table S1). In adjusted models, each IQR increment in Ox concentration alone was associated with an increase in symptom-based exacerbation rates, with no associations observed with the other air pollutants (Table 3).
 |
Table 3 Adjusted Associations Between Each Air Pollutant and Exacerbation Rates Across Both Study Periods |
In within-period analyses, during the pre-pandemic period unadjusted models demonstrated that each IQR increment in NO2 and Ox were again associated with an increase in symptom-based exacerbations (1.30 [1.16, 1.45]; and 1.21 [1.08, 1.36], respectively), and event-based exacerbations for NO2 alone (1.16 [1.02, 1.33]), with a trend for Ox that did not reach statistical significance (1.13 [0.96, 1.33], P=0.136). In adjusted models, no associations were observed, though a trend with each IQR increment for Ox alone with symptom-based exacerbations was observed (1.25 [0.99, 1.59], P=0.064). During the COVID-19 pandemic period, unadjusted models demonstrated that each IQR increment in NO2 was associated with an increase in symptom-based exacerbations (1.24 [1.01, 1.54]), while in adjusted models, NO2 was associated with a decrease in event-based exacerbations (0.69 [0.49, 0.97]). Each Ox increment was associated with an increase in both symptom-based (1.46 [1.13, 1.89]) and event-based (1.43 [1.00, 2.05]) exacerbations in unadjusted, but not adjusted, models.
Each additional listed behavior (action taken) to reduce the risk of COVID-19 infection/transmission as captured in the COVID-19 Questionnaire data (n=413; see Supplement Figure S1) was associated with a reduction in event-based exacerbation rates (0.59 [0.43, 0.82]). Likewise, participants who reported <4 listed behaviors to reduce infection/transmission risk had a higher rate of symptom-based exacerbations (1.52 [1.02, 2.27]) compared with those who reported ≥4 behaviors. Regarding viral infectious symptoms, scoring>1 compared with scoring=1 (FLU-PRO questionnaire; see Supplement) was associated with an increased rate of symptom-based (2.96 [2.10, 4.18]) and event-based (2.72 [1.66, 4.46]) exacerbations. When both behaviors and viral infectious symptoms were inserted into each air pollutant-exacerbation adjusted model, the only association observed was a decrease in the rate of event-based exacerbations with each NO2 increment (0.65 [0.46, 0.91]).
Pollutant-Exacerbation Associations and Individual-Level Risk Factors
Female gender, co-morbid asthma, and Eos ≥3% were each associated with increased rates of both symptom-based and event-based exacerbations, respectively, in univariable analyses (see Supplement Table S1). Eos ≥300 was associated with event-based exacerbations alone. Cumulative cigarette smoking history (in pack-years) and FEV1 (percent predicted) were also associated with both symptom-based and event-based exacerbations. Smoking history, FEV1, female gender, co-morbid asthma, and Eos ≥3% were associated with an increase in both symptom-based and event-based exacerbations, while each IQR increment in Ox (and no other air pollutants) was associated with increased rates of symptom-based exacerbations, in stepwise adjusted multivariable analyses (Table 4).
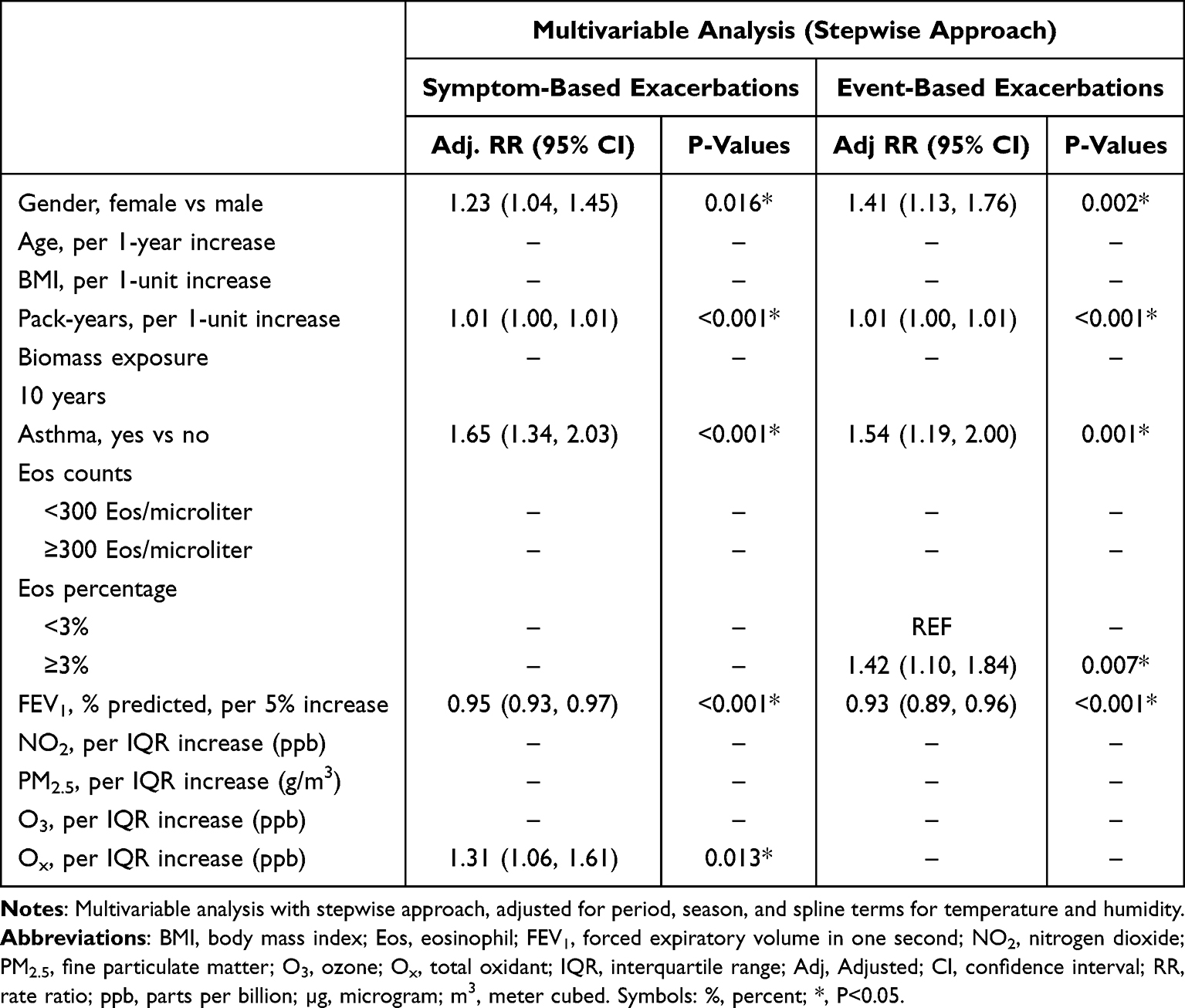 |
Table 4 Associations Between Individual-Level Factors and Exacerbation Rates |
In risk factor subgroup (effect modification) analyses, each IQR increment of Ox was associated with an increase in symptom-based exacerbation rates in females whereas in males, each IQR increment in PM2.5 was associated with a decrease in symptom-based exacerbations (Figure 4). In the non-asthma subgroup, each IQR increment in PM2.5 was associated with a decrease in symptom-based exacerbations (Figure 5). Finally, in the Eos <300 subgroup, each IQR increment in both NO2, and Ox were associated with a decrease in event-based exacerbations, whereas in the Eos ≥300 subgroup, each Ox increment alone was associated with an increase in symptom-based exacerbations (Figure 6). Evidence of effect modification was observed for gender (both NO2 and O3 with event-based exacerbations) and for co-morbid asthma status (PM2.5 with both symptom-based and event-based exacerbations).
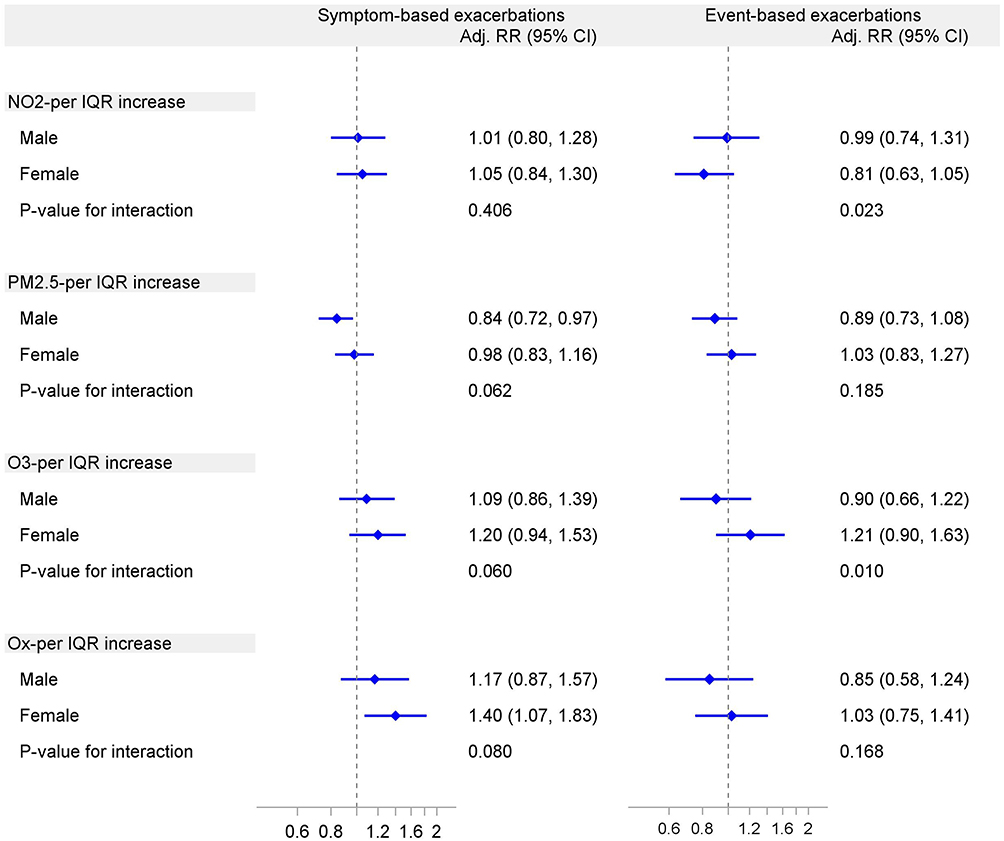 |
Figure 4 Forest plot of the association between air pollutant concentration and exacerbation rates stratified by gender across both pre-pandemic and COVID-19 pandemic periods. Rate ratios (RR) and 95% confidence intervals (CI) were estimated using Generalized Estimating Equation (GEE) models with a negative binomial distribution and exchangeable correlation, with time included as the offset term. Adjusted (Adj) for age, period, season, and spline terms for temperature and humidity. NO2, nitrogen dioxide (parts per billion); PM2.5, fine particulate matter (microgram per cubic meter); O3, ozone (parts per billion); Ox, total oxidant (parts per billion); IQR, interquartile range. Symbols: %, percent. |
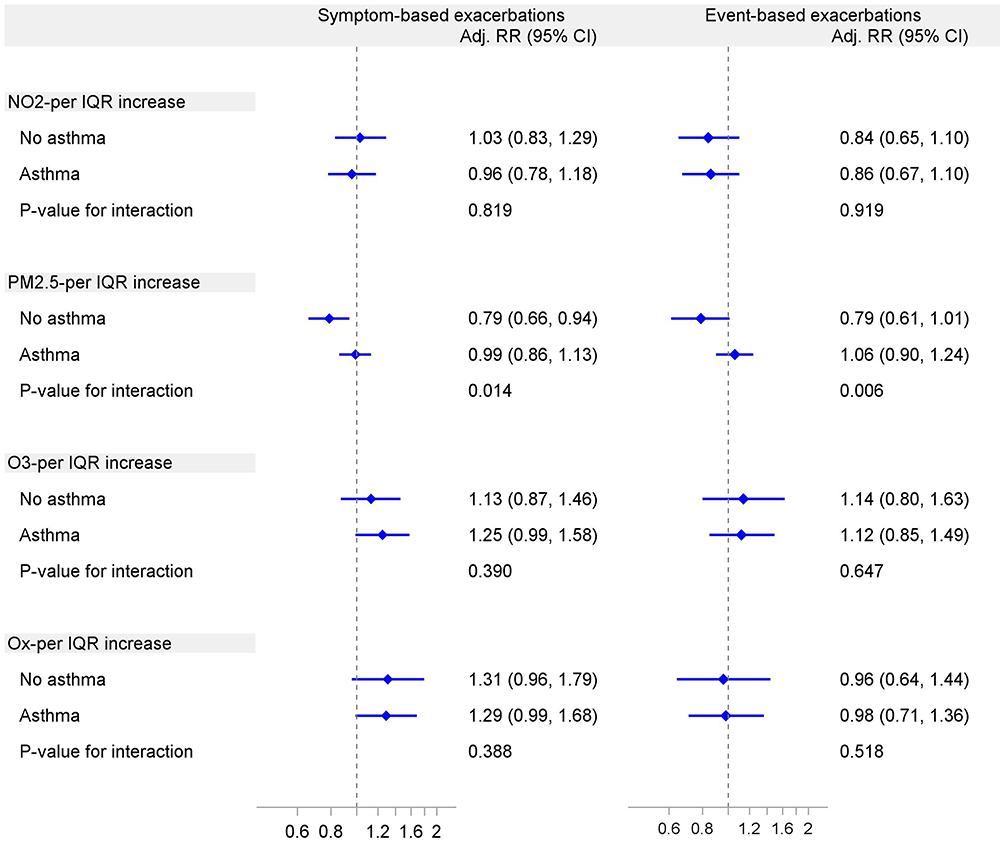 |
Figure 5 Forest plot of the association between air pollutant concentration and exacerbation rates stratified by asthma status across both pre-pandemic and COVID-19 pandemic periods. Rate ratios (RR) and 95% confidence intervals (CI) were estimated using Generalized Estimating Equation (GEE) models with a negative binomial distribution and exchangeable correlation, with time included as the offset term. Adjusted (Adj) for age, gender, period, season, and spline terms for temperature and humidity. NO2, nitrogen dioxide (parts per billion); PM2.5, fine particulate matter (microgram per cubic meter); O3, ozone (parts per billion); Ox, total oxidant (parts per billion); IQR, interquartile range. Symbols: %, percent. |
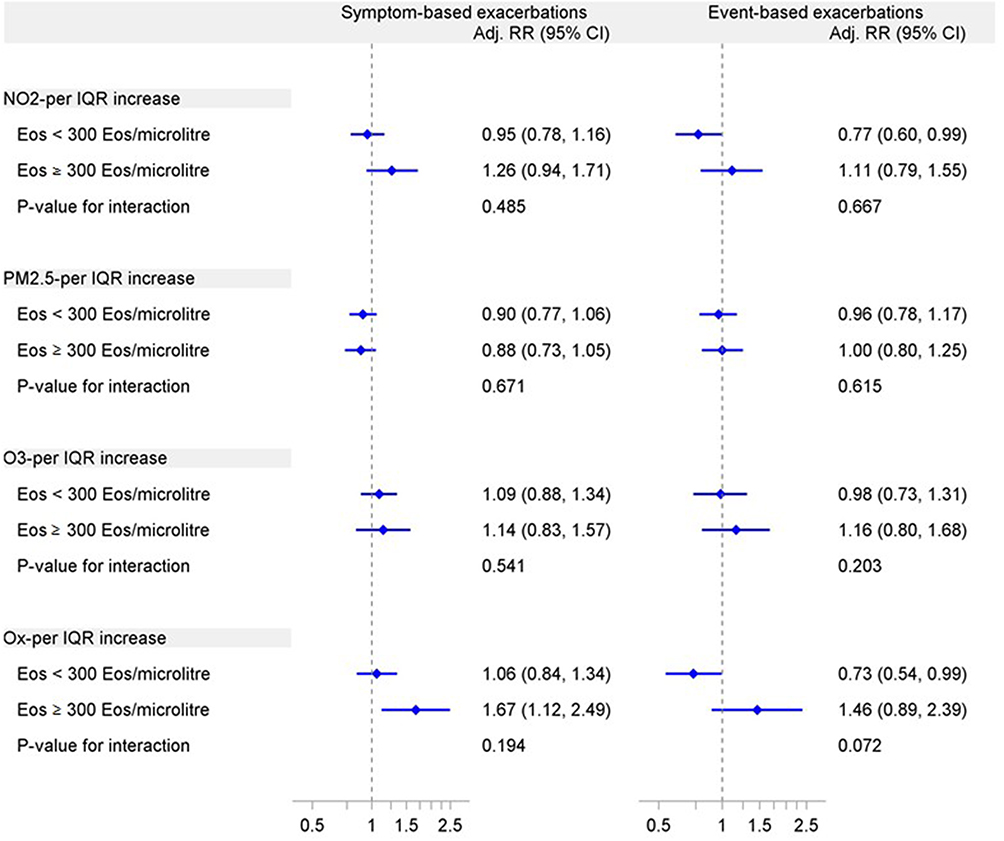 |
Figure 6 Forest plot of the association between air pollutant concentration and exacerbation rates stratified by blood eosinophil count across both pre-pandemic and COVID-19 pandemic periods. Rate ratios (RR) and 95% confidence intervals (CI) were estimated using Generalized Estimating Equation (GEE) models with a negative binomial distribution and exchangeable correlation, with time included as the offset term. Adjusted (Adj) for age, gender, period, season, and spline terms for temperature and humidity. NO2, nitrogen dioxide (parts per billion); PM2.5, fine particulate matter (microgram per cubic meter); O3, ozone (parts per billion); Ox, total oxidant (parts per billion); IQR, interquartile range. Symbols: %, percent. |
Discussion
The present study investigated the associations between air pollutant concentrations and exacerbations of COPD in the global COVID-19 pandemic era, across which there was a substantial fluctuation in ambient air pollution, and additionally investigated relevant individual-level risk factors in these associations in a prospective cohort of participants with COPD. While a significant decrease in NO2, PM2.5, and Ox concentrations was observed during the COVID-19 pandemic period, O3 concentration on average increased. We also observed a decrease in the rate of both symptom-based and event-based exacerbations during the pandemic. The most consistent association across both periods, in both unadjusted and adjusted models, was observed between ambient Ox exposure and COPD exacerbations. NO2 exposure was associated with both an increase, decrease, or no association with exacerbations across the different models, and likewise, some unexpected associations were observed with PM2.5, such that PM2.5 exposure in some models was associated with a decrease in exacerbations. When investigating behaviors and events during the COVID-19 pandemic period, interestingly, fewer self-reported health-protective behaviors were associated with an increase in exacerbations and higher self-reported symptoms of viral infection were associated with an increase in exacerbations. Including both of these variables into adjusted models led to a loss of the association between Ox and exacerbations that was observed consistently across the other models. Finally, beyond typical markers of disease severity including cumulative smoking history and lung function, female gender, co-morbid asthma, and high blood eosinophil count were each positively associated with exacerbations, and in stepwise multivariable modeling with air pollutants, these were relevant risk factors in the significant association between Ox concentration and exacerbations.
The significant reductions in NO2, PM2.5, and Ox concentrations, the increase in O3 levels, and the reduction in both symptom-based and event-based exacerbation rates during the COVID-19 pandemic period are all consistent findings with the existing available literature. The same directionality of air pollutant fluctuations was reported during regional and pan-national lockdowns,4,5 as were the observed reductions in COPD exacerbations, COPD-related hospitalizations,4,9,26–29 and mortality.30 PM2.5 and NO2 changes during lockdowns have been attributed to industrial and economic slowdowns and reduced human transportation and traffic;6 meteorological factors were also considered to be, at least in part, contributory.5 Another study during COVID-19 lockdowns in Europe demonstrated that, while Ox levels decreased slightly at “traffic” sites due to reduced primary NO2 emissions, they remained nearly constant in “urban background” locations.14
The most consistent association observed in the present study was between ambient Ox exposure and symptom-based COPD exacerbations, while the associations between NO2 and PM2.5 exposure and exacerbations varied considerably. The strong association between Ox and symptom-based exacerbations, despite NO2 and O3 individually not being associated, may relate to their differing spatial distribution. NO2 is typically higher in urban areas, while O3 is higher in rural areas, and Ox captures the overall oxidative potential across different geographic areas.31 Recent studies suggest that gaseous and particulate pollutants contribute to exacerbations of COPD through different proposed mechanisms. While gaseous pollutants may trigger bronchoconstriction, particulate pollutants may promote airway inflammation and increased mucus production.32–34 O3 and NO2 are gaseous pollutants with strong oxidative potential, with Ox representing the sum of their oxidative capacities.35–37 One study in the UK investigated the impact of O3, NO2, and Ox on mortality and found that 24-hour mean concentrations of Ox were associated with greater increases in mortality compared to O3 and NO2 individually.38 When analyzed together in two-pollutant modeling, the associations for O3 and NO2 were similar in magnitude to those for Ox.38 The association between gaseous pollutants, in particular Ox, with respiratory exacerbations have been observed in Germany,9 Greece,18 and China.35,39 Thus, considering the combined oxidative potential of gaseous pollutants, as encapsulated by Ox, this ambient air pollutant may be of particular value in future epidemiological studies in the investigation of the associations between air pollution exposure and exacerbations of COPD.
Interesting additional findings in the present study were that adopting health protective behaviors and practices during the COVID-19 pandemic period was associated with a reduction in exacerbations, while experiencing viral infection symptoms was associated with an increase in exacerbations. In the subgroup with this data available, integrating both terms into the COVID-19 pandemic period adjusted models attenuated the observed association between Ox and exacerbations to the null. While this could be due to the reduced sample size (from 673 to 413, potentially leading to loss of associations), alternatively these findings may indicate that respiratory viral infection and health protective behaviors are associated with exacerbations and that exposure to Ox may be a potential modifier of these known associations. Previous studies demonstrated that COVID-19 pandemic-specific preventive interventions, such as lockdowns themselves but also behaviors such as hand hygiene, face coverings and physical distancing played a role in lowering the risk of infectious exacerbations.15,26,40–42 These findings emphasize the impact of individual behaviors on exacerbation risk and indicate the need for tailored interventions to promote health-protective actions, especially during pandemic periods and/or periods of high respiratory viral infection. The consistency of the association between Ox in particular with symptom-based exacerbations across several different models (unadjusted and adjusted) and periods (pre-pandemic and COVID-19 pandemic), however, support this interesting relationship and its relevance beyond just viral transmission as contributory in the COPD patient population. A study from Germany supports this plausibility, wherein gaseous pollutants (NO2) were found to have the highest risk ratios for hospital admissions of COPD and asthma, surpassing those of particulate matter pollutants, and moreover smoking and influenza infection were found to be minimally influential in those associations.9 Finally, ambient air pollution and respiratory viruses may not actually be distinct and separate triggers per se but may instead interact in complex ways to precipitate exacerbations of COPD. In a notable study focused on a period preceding the COVID-19 pandemic era (1996–2015) in the East London Cohort, daily diary cards were used as a sensitive patient-reported outcome to identify exacerbations in order to examine the mechanistic relationship between air pollutant exposure, viruses, and exacerbations.43 The authors of this study observed an association between elevated gaseous pollutants (oxides of nitrogen) and, specifically, viral-type exacerbations of COPD.43
Female gender, comorbid self-reported physician-diagnosed asthma, and elevated blood eosinophils were each associated with increased exacerbation rates, and in stepwise multivariable modeling with air pollutants, these factors emerged as relevant in the significant association between Ox concentration and exacerbations. In females, each IQR increase in Ox alone was associated with higher rates of event-based exacerbations, while in males, each increase in PM2.5 was associated with lower rates of symptom-based exacerbations. Evidence of effect modification based on gender for both NO2 and O3 and event-based exacerbations was also observed. Gender-specific disparities in the health impact of air pollution have been highlighted across several previous studies, including from our own group,25 in other Canadian studies outside of the COPD patient population,44 and in COPD populations outside of North America and Europe.29 Asthma status also appears to be a relevant modifier in the association between Ox and exacerbations. Previous findings in patients with asthma and COPD identified various indoor and outdoor factors including air pollutants, allergens, and climate conditions, that can provoke respiratory symptoms and exacerbations.45 Specifically, exposure to air pollutants such as particulate matter, O3, NO2, sulfur dioxide and carbon monoxide were associated with increased exacerbations and hospitalizations in these individuals. Studies show that O3 exposure increases the odds of the development of COPD in individuals with asthma, indicating that O3 may be an important risk factor in progression to irreversible airflow obstruction.46 Finally, among participants in the present study with Eos ≥300, Ox was associated with increased symptom-based exacerbations. Reduced air pollution levels and fewer in-hospital admissions were observed in recent COVID-19 era research in patients with asthma and/or COPD during lockdown periods, and elevated blood eosinophils were observed in those patients with COPD who were ultimately admitted to hospital during those periods.18 More recent work has found that the association between short-term air pollution and day-to-day lung function (FEV1) in COPD may be influenced by blood eosinophil levels.47 Our findings align with these emerging studies and further support the important role of eosinophilia in the COPD patient population and in particular, their mechanistic interaction with air pollution exposure in the occurrence of exacerbations.
This study has important and notable strengths. The inclusion of participants and prospectively collected data from a comprehensive multi-site and multi-regional national cohort, confirmation of disease status in each participant, the inclusion of data both preceding and during the COVID-19 pandemic, the inclusion of clinically important acute respiratory events that did not necessitate hospital admission or ICD code reliance,20,21,23,24 and the collection of self-reported potential confounding (behavioral and infectious status) variables are noteworthy strengths of the present study. There are also, however, important limitations that mandate consideration in the interpretation of these study findings. Firstly, the reliance on self-reported participant behaviors during the pandemic introduces the potential for recall bias, as individuals may not accurately remember or report their actions, particularly given this unprecedented period. Secondly, the study’s focus on a specific geographic and temporal context may limit the generalizability of our findings to other settings and populations.48 Thirdly, the consistent association between Ox and exacerbations were no longer observed following adjustment for COVID-19 pandemic period confounders, which may or may not have been limited by the smaller size of this subgroup as mentioned, and even by the reliability in estimating behavior or viral infection status during this unprecedented period. Fourthly, adjustments for multiple comparisons were not performed despite the large number of associations tested. Fifthly, the consistent associations between certain variables and exacerbations observed in our models may be attributed to unmeasured or unadjusted confounders, which is an important consideration and limitation in all observational studies. Lastly, air pollution exposure data from fixed-location monitoring stations was used rather than from satellite-based data due to the duration and frequency of sampling needed to conduct the present study.
Conclusion
In summary, the COVID-19 pandemic era was a monumental and unique period that has served to provide valuable lessons and information regarding the associations between ambient air pollution and exacerbations of COPD. Important findings include the reduction in some but not all air pollutants during the COVID-19 pandemic, largely consistent associations between Ox exposure and exacerbations of COPD, an influence of the effect of protective behaviors and self-reported viral infection on these associations, and the role of female gender, co-morbid asthma, and blood eosinophilia as individual-level risk factors on these associations. These findings emphasize the need for targeting more at-risk populations and for targeted interventions to reduce the impact of air pollution on exacerbations of COPD during crisis periods.
Abbreviations
CanCOLD, Canadian Cohort Obstructive Lung Disease; COPD, Chronic Obstructive Pulmonary Disease; COVID-19, Coronavirus Disease 2019; ECOPDs, Exacerbations of Chronic Obstructive Pulmonary Disease; FEV1, Forced Expiratory Volume in 1 second; FVC, Forced Vital Capacity; FLU-PRO, Flu Patient Reported Outcome; GEE, Generalized Estimating Equations; GOLD, Global Initiative for Chronic Obstructive Lung Disease; ICD, International Classification of Diseases; IQR, Interquartile Range; NO2, Nitrogen Dioxide; Ox, Total Oxidant (NO2 + O3); O3, Ground-Level Ozone; PM2.5, Fine Particulate Matter (particles smaller than 2.5 micrometers); RR, Rate Ratio; RRs, Rate Ratios; SAS, Statistical Analysis System; 95% CIs, 95% Confidence Intervals; Eos, Eosinophils.
Data Sharing Statement
Due to data privacy regulations, individual participant data collected during this study is not publicly accessible. However, access to anonymized data may be granted upon evaluation. Additional documents will also be available upon inquiry. All requests should be directed to the corresponding author (BAR).
Ethics Approval and Informed Consent
Written informed consent was obtained from all participants, and the study received institutional review board approval at each site (BMC09-025), coordinated through the McGill University Health Centre (MUHC) Research Ethics Board (REB).
Acknowledgments
We thank all CanCOLD participants, the CanCOLD collaborative research group, the open-access Government of Canada databases and the grant foundations of this research for making this work possible. Researchers at RI-McGill University Health Centre Montreal and iCAPTURE Centre Vancouver lead the project. Executive Committee: Jean Bourbeau (McGill University, Montreal, QC, Canada); Wan C Tan, J Mark FitzGerald, Don D Sin (UBC, Vancouver, BC, Canada); Darcy D Marciniuk (University of Saskatoon, Saskatoon, SK, Canada); Denis E O’Donnell (Queen’s University, Kingston, ON, Canada); Paul Hernandez (Dalhousie University, Halifax, NS, Canada); Kenneth R Chapman (University of Toronto, Toronto, ON, Canada); Brandie Walker (University of Calgary, Calgary, AB, Canada); Shawn Aaron (University of Ottawa, Ottawa, ON, Canada); François Maltais (University of Laval, Quebec City, QC, Canada). International Advisory Board: Jonathon Samet (the Keck School of Medicine of USC, California, USA); Milo Puhan (John Hopkins School of Public Health, Baltimore, USA); Qutayba Hamid (McGill University, Montreal, QC, Canada); James C Hogg (University of British Columbia, James Hogg Research Centre, Vancouver, BC, Canada). Operations Centre: Jean Bourbeau (PI), Dany Doiron, Palmina Mancino, Pei Zhi Li, Dennis Jensen, Carolyn Baglole (University of McGill, Montreal, QC, Canada), Yvan Fortier (Laboratoire telematique Respiratory Health Network, FRQS); Wan C Tan (co-PI), Don Sin, Julia Yang, Jeremy Road, Joe Comeau, Adrian Png, Kyle Johnson, Harvey Coxson, Miranda Kirby, Jonathon Leipsic, Cameron Hague (University of British Columbia, James Hogg Research Centre, Vancouver, BC, Canada). Economic Core: Mohsen Sadatsafavi (University of British Columbia, Vancouver, BC). Public Health Core: Teresa To, Andrea Gershon (University of Toronto). Data management and Quality Control: Wan C Tan, Harvey Coxson (UBC, Vancouver, BC, Canada); Jean Bourbeau, Pei-Zhi Li, Zhi Song, Andrea Benedetti, Dennis Jensen (McGill University, Montreal, QC, Canada); Yvan Fortier (Laboratoire telematique Respiratory Health Network, FRQS). Field Centres: Wan C Tan (PI), Christine Lo, Sarah Cheng, Elena Un, Cynthia Fung, Wen Tiang Wang, Liyun Zheng, Faize Faroon, Olga Radivojevic, Sally Chung, Carl Zou (UBC James Hogg Research Centre, Vancouver, BC, Canada); Jean Bourbeau (PI), Palmina Mancino, Jacinthe Baril, Laura Labonté (McGill University, Montreal, QC, Canada); Kenneth Chapman (PI), Patricia McClean, Nadeen Audisho (University of Toronto, Toronto, ON, Canada); Brandie Walker, (PI), Curtis Dumonceaux, Lisette Machado (University of Calgary, Calgary, AB, Canada); Paul Hernandez (PI), Scott Fulton, Kristen Osterling, Denise Wigerius (Dalhousie University and Queen Elizabeth II Health Sciences Centre, Halifax, NS, Canada); Shawn Aaron (PI), Kathy Vandemheen, Gay Pratt, Amanda Bergeron (University of Ottawa, Ottawa, ON, Canada); Denis O’Donnell (PI), Matthew McNeil, Kate Whelan (Queen’s University, Kingston, ON, Canada); François Maltais (PI), Cynthia Brouillard (University of Laval, Quebec City, QC, Canada); Darcy Marciniuk (PI), Ron Clemens, Janet Baran, Candice Leuschen (University of Saskatchewan, Saskatoon, SK, Canada). The Canadian Cohort Obstructive Lung Disease (CanCOLD) study makes de-identified data available for research on respiratory health. Information on how to submit a data access application can be found on the CanCOLD website at: www.cancold.ca.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the Canadian Institutes of Health Research (CIHR: #447731), the McGill University Health Centre (MUHC) Department of Medicine Contract Academic Staff (CAS) Research Award, and the Fonds de la Recherche en Santé du Québec (FRQS). Additionally, the Canadian Cohort Obstructive Lung Disease (CanCOLD; NCT00920348) study is currently funded by the Canadian Respiratory Research Network and the industry partners AstraZeneca Canada Ltd, Boehringer Ingelheim Canada Ltd, GlaxoSmithKline (GSK) Canada Ltd, and Novartis. Previous funding partners were the Canadian Institutes of Health Research (CIHR; CIHR/Rx&D Collaborative Research Program Operating Grants- 93326), the Respiratory Health Network of the Fonds de la Recherche en Santé du Québec (FRQS), and industry partners: Almirall; Merck Nycomed; Pfizer Canada Ltd; and Theratechnologies.
Disclosure
Dr Jean Bourbeau reports grants from the Canadian Institute of Health Research (CIHR), Réseau en santé respiratoire du FRQS, McGill University, McGill University Health Centre Foundation, AstraZeneca Canada Ltd, Boehringer Ingelheim Canada Ltd, GlaxoSmithKline Canada Ltd, Grifols, Novartis, Sanofi, and Trudell Canada Ltd, and payment or honoraria for lectures, presentations, speakers bureaus, and educational events from AstraZeneca Canada Ltd, Boehringer Ingelheim Canada Ltd, GlaxoSmithKline Canada Ltd, Trudell Canada Ltd, Pfizer Canada Ltd, and COVIS Pharma Canada Ltd. Dr Shawn D. Aaron reports consulting fees from AstraZeneca, GlaxoSmithKline, Sanofi, and Methapharm. Dr Kenneth Chapman reports grants from BMS, Bellus, AstraZeneca, GlaxoSmithKline, Sanofi, Regeneron, Takeda, and Novartis, consulting fees from AstraZeneca, GlaxoSmithKline, Inhibrix, Mereo, Regeneron, Sanofi, and Takeda, and payment or honoraria for lectures, presentations, speaker bureaus, manuscript writing, or educational events from Valeo, Sanofi, Novartis, and GlaxoSmithKline. He serves on the Board of Directors of AlphaNet Canada. Dr Paul Hernandez reports grants from Grifols, support for the present manuscript from CIHR, and payment or honoraria from the Canadian Thoracic Society and GlaxoSmithKline. He has participated on advisory boards for AstraZeneca, GlaxoSmithKline, and Takeda, and holds leadership role with the Canadian Thoracic Society. Dr François Maltais reports grants from GlaxoSmithKline, AstraZeneca, Sanofi, Novartis, Boehringer Ingelheim, and Grifols, and consulting fees from AstraZeneca and payment or honoraria from GlaxoSmithKline, Boehringer Ingelheim, Grifols, and AstraZeneca. He holds stock or stock options in Oxynov. Dr Simon Rousseau reports support for the present manuscript from FRQ-S and holds a leadership role as director of the Canadian Respiratory Research Network. Dr Bryan A. Ross reports funding as Principal Investigator from QHRN, MUHC-CAS, MUHC-Foundation, MGH-Foundation, Innovation-Partnership Grant (I+&P: McGill & Thorasys), Trudell Medical International Unrestricted Investigator-Initiated Operating Grant, AstraZeneca Unrestricted Investigator-Initiated Operating Grant, and MI-4. He has received of in-kind support (placebo and intervention) for research from Amazentis and received in-kind support (diagnostic device(s)) for research from Thorasys Inc. and Restech. He has participated in COPD educational speakerships/moderatorships for GSK, AstraZeneca, Covis, the Canadian Thoracic Society (CTS), CHEST, APPQ, AKA, Respiplus, and McGill CPD. Brandie Walker reports personal fees from AstraZeneca, personal fees from GSK, personal fees from Sanofi, outside the submitted work; Wan Tan reports grants from Canadian Institute of Health Research (CIHR/Rx&D Collaborative Research Program Operating Grants- 93326) with industry partners Astra Zeneca Canada Ltd., Boehringer-Ingelheim Canada Ltd, GlaxoSmithKline Canada Ltd, Merck, Novartis Pharma Canada Inc., Nycomed Canada Inc., Pfizer Canada Ltd., during the conduct of the study. The authors report no other conflicts of interest.
References
1. Leung C, Bourbeau J, Sin DD, et al. The prevalence of chronic obstructive pulmonary disease (COPD) and the heterogeneity of risk factors in the Canadian population: results from the Canadian Obstructive Lung Disease (COLD) study. Int J Chron Obstruct Pulmon Dis. 2021;16:305–320. doi:10.2147/copd.S285338
2. Global strategy for the diagnosis, management, and prevention of COPD (2024 report). 2024. Available from: https://goldcopd.org/2024-gold-report/.
3. Celli BR, Fabbri LM, Aaron SD, et al. An updated definition and severity classification of chronic obstructive pulmonary disease exacerbations: the Rome proposal. Am J Respir Crit Care Med. 2021;204(11):1251–1258. doi:10.1164/rccm.202108-1819PP
4. Sarmadi M, Rahimi S, Rezaei M, Sanaei D, Dianatinasab M. Air quality index variation before and after the onset of COVID-19 pandemic: a comprehensive study on 87 capital, industrial and polluted cities of the world. Environ Sci Eur. 2021;33(1):134. doi:10.1186/s12302-021-00575-y
5. He C, Hong S, Zhang L, et al. Global, continental, and national variation in PM2.5, O3, and NO2 concentrations during the early 2020 COVID-19 lockdown. Atmos Pollut Res. 2021;12(3):136–145. doi:10.1016/j.apr.2021.02.002
6. Venter ZS, Aunan K, Chowdhury S, Lelieveld J. COVID-19 lockdowns cause global air pollution declines. Proc Natl Acad Sci USA. 2020;117(32):18984–18990. doi:10.1073/pnas.2006853117
7. Mashayekhi R, Pavlovic R, Racine J, et al. Isolating the impact of COVID-19 lockdown measures on urban air quality in Canada. Air Qual Atmos Health. 2021;14(10):1549–1570. doi:10.1007/s11869-021-01039-1
8. Carslaw DC, Beevers SD. Estimations of road vehicle primary NO2 exhaust emission fractions using monitoring data in London. Atmos Environ. 2005;39(1):167–177. doi:10.1016/j.atmosenv.2004.08.053
9. Hoffmann C, Maglakelidze M, von Schneidemesser E, Witt C, Hoffmann P, Butler T. Asthma and COPD exacerbation in relation to outdoor air pollution in the metropolitan area of Berlin, Germany. Respir Res. 2022;23(1):64. doi:10.1186/s12931-022-01983-1
10. Brancher M. Increased ozone pollution alongside reduced nitrogen dioxide concentrations during Vienna’s first COVID-19 lockdown: significance for air quality management. Environ Pollut. 2021;284:117153. doi:10.1016/j.envpol.2021.117153
11. Gaubert B, Bouarar I, Doumbia T, et al. Global changes in secondary atmospheric pollutants during the 2020 COVID-19 pandemic. J Geophys Res Atmos. 2021;126(8):e2020JD034213. doi:10.1029/2020JD034213
12. Lovric M, Pavlovic K, Vukovic M, Grange SK, Haberl M, Kern R. Understanding the true effects of the COVID-19 lockdown on air pollution by means of machine learning. Environ Pollut. 2021;274:115900. doi:10.1016/j.envpol.2020.115900
13. Itahashi S. Severe level of photochemical oxidants (Ox) over the western coast of Japan during autumn after typhoon passing. Sci Rep. 2023;13(1):16369. doi:10.1038/s41598-023-43485-0
14. Grange SK, Lee JD, Drysdale WS, et al. COVID-19 lockdowns highlight a risk of increasing ozone pollution in European urban areas. ACP. 2021;21(5):4169–4185. doi:10.5194/acp-21-4169-2021
15. Alqahtani JS, Oyelade T, Aldhahir AM, et al. Reduction in hospitalised COPD exacerbations during COVID-19: a systematic review and meta-analysis. PLoS One. 2021;16(8):e0255659. doi:10.1371/journal.pone.0255659
16. Alsallakh MA, Sivakumaran S, Kennedy S, et al. Impact of COVID-19 lockdown on the incidence and mortality of acute exacerbations of chronic obstructive pulmonary disease: national interrupted time series analyses for Scotland and Wales. BMC Med. 2021;19(1):124. doi:10.1186/s12916-021-02000-w
17. Montiel-Lopez F, Rodriguez-Ramirez D, Cassou-Martinez M, et al. Air quality in Mexico City during the COVID-19 lockdown possibly decreased COPD exacerbations. ERJ Open Res. 2022;8(4):00183–2022. doi:10.1183/23120541.00183-2022
18. Sigala I, Giannakas T, Giannakoulis VG, et al. Effect of COVID-19-related lockdown on hospital admissions for asthma and COPD exacerbations: associations with air pollution and patient characteristics. J Pers Med. 2021;11(9):867. doi:10.3390/jpm11090867
19. Hazan G, Fox C, Mok H, Haspel J. Age-dependent rebound in asthma exacerbations after COVID-19 lockdown. J Allergy Clin Immunol Glob. 2022;1(4):314–318. doi:10.1016/j.jacig.2022.06.001
20. Langsetmo L, Platt RW, Ernst P, Bourbeau J. Underreporting exacerbation of chronic obstructive pulmonary disease in a longitudinal cohort. Am J Respir Crit Care Med. 2008;177(4):396–401. doi:10.1164/rccm.200708-1290OC
21. Xu W, Collet JP, Shapiro S, et al. Negative impacts of unreported COPD exacerbations on health-related quality of life at 1 year. Eur Respir J. 2010;35(5):1022–1030. doi:10.1183/09031936.00079409
22. Mikaeeli SDD, Bourbeau J, Rousseau S, Zhi Li P, Ross B. Exacerbations of COPD (ECOPDs) in CanCOLD cohort participants during the pandemic era: air pollution fluctuations and individual-level risk factors [abstract]. 2024.
23. Bourbeau J, Ford G, Zackon H, Pinsky N, Lee J, Ruberto G. Impact on patients’ health status following early identification of a COPD exacerbation. Eur Respir J. 2007;30(5):907–913. doi:10.1183/09031936.00166606
24. Labonte LE, Tan WC, Li PZ, et al. Undiagnosed chronic obstructive pulmonary disease contributes to the burden of health care use. Data from the CanCOLD study. Am J Respir Crit Care Med. 2016;194(3):285–298. doi:10.1164/rccm.201509-1795OC
25. Ross BA, Doiron D, Benedetti A, et al. Short-term air pollution exposure and exacerbation events in mild to moderate COPD: a case-crossover study within the CanCOLD cohort. Thorax. 2023;78(10):974–982. doi:10.1136/thorax-2022-219619
26. Ko FWS, Lau LHS, Ng SS, et al. Respiratory admissions before and during the COVID-19 pandemic with mediation analysis of air pollutants, mask-wearing and influenza rates. Respirol. 2023;28(1):47–55. doi:10.1111/resp.14345
27. Bhattacharyya P, Mukherjee S, Chatterjee M, Saha D, Sengupta S, Dey D. The impact of lockdown on symptoms and health status of patients with chronic airway diseases: an appraisal of patient perceived impressions. Lung India. 2023;40(2):128–133. doi:10.4103/lungindia.lungindia_278_22
28. Dabrowiecki P, Chcialowski A, Dabrowiecka A, Piorkowska A, Badyda A. Air pollution and long-term risk of hospital admission due to chronic obstructive pulmonary disease exacerbations in Poland: a time-stratified, case-crossover study. Pol Arch Intern Med. 2023;133(7–8). doi:10.20452/pamw.16444
29. Liang L, Cai Y, Barratt B, et al. Associations between daily air quality and hospitalisations for acute exacerbation of chronic obstructive pulmonary disease in Beijing, 2013-17: an ecological analysis. Lancet Planet Health. 2019;3(6):e270–e279. doi:10.1016/S2542-5196(19)30085-3
30. Ghobakhloo S, Khoshakhlagh AH, Mostafaii GR, Chuang KJ, Gruszecka-Kosowska A, Hosseinnia P. Critical air pollutant assessments and health effects attributed to PM2.5 during and after COVID-19 lockdowns in Iran: application of air(Q+) models. Front Public Health. 2023;11:1120694. doi:10.3389/fpubh.2023.1120694
31. Lu M, Soenario I, Helbich M, et al. Land use regression models revealing spatiotemporal co-variation in NO2, NO, and O3 in the Netherlands. Atmos Environ. 2020;223:117238. doi:10.1016/j.atmosenv.2019.117238
32. Lin AH, Hsu CC, Lin YS, Lin RL, Lee LY. Mechanisms underlying the stimulatory effect of inhaled sulfur dioxide on vagal bronchopulmonary C-fibres. J Physiol. 2020;598(5):1093–1108. doi:10.1113/JP279152
33. Petit PC, Fine DH, Vasquez GB, Gamero L, Slaughter MS, Dasse KA. The pathophysiology of nitrogen dioxide during inhaled nitric oxide therapy. ASAIO J. 2017;63(1):7–13. doi:10.1097/MAT.0000000000000425
34. Arias-Perez RD, Taborda NA, Gomez DM, Narvaez JF, Porras J, Hernandez JC. Inflammatory effects of particulate matter air pollution. Environ Sci Pollut Res Int. 2020;27(34):42390–42404. doi:10.1007/s11356-020-10574-w
35. Guo H. Comparisons of combined oxidant capacity and redox-weighted oxidant capacity in their association with increasing levels of FeNO. Chemosphere. 2018;211:584–590. doi:10.1016/j.chemosphere.2018.07.191
36. Yuan Z, Chen P, Yang L, et al. Combined oxidant capacity, redox-weighted oxidant capacity and elevated blood pressure: a panel study. Ecotoxicol Environ Saf. 2022;234:113364. doi:10.1016/j.ecoenv.2022.113364
37. Weichenthal S, Lavigne E, Evans G, Pollitt K, Burnett RT. Ambient PM2.5 and risk of emergency room visits for myocardial infarction: impact of regional PM2.5 oxidative potential: a case-crossover study. Environ Health. 2016;15(1):46. doi:10.1186/s12940-016-0129-9
38. Williams ML, Atkinson RW, Anderson HR, Kelly FJ. Associations between daily mortality in London and combined oxidant capacity, ozone and nitrogen dioxide. Air Qual Atmos Health. 2014;7(4):407–414. doi:10.1007/s11869-014-0249-8
39. Fu Y, Zhang W, Li Y, Li H, Deng F, Ma Q. Association and interaction of O3 and NO2 with emergency room visits for respiratory diseases in Beijing, China: a time-series study. BMC Public Health. 2022;22(1):2265. doi:10.1186/s12889-022-14473-2
40. Farrugia Y, Spiteri Meilak BP, Grech N, et al. The impact of COVID-19 on hospitalised COPD exacerbations in Malta. Pulm Med. 2021;2021:5533123. doi:10.1155/2021/5533123
41. Chan KPF, Ma TF, Kwok WC, et al. Significant reduction in hospital admissions for acute exacerbation of chronic obstructive pulmonary disease in Hong Kong during coronavirus disease 2019 pandemic. Respir Med. 2020;171:106085. doi:10.1016/j.rmed.2020.106085
42. Acharya VK, Sharma DK, Kamath SK, et al. Impact of COVID-19 pandemic on the exacerbation rates in COPD patients in southern India - a potential role for community mitigations measures. Int J Chron Obstruct Pulmon Dis. 2023;18:1909–1917. doi:10.2147/COPD.S412268
43. Pfeffer PE, Donaldson GC, Mackay AJ, Wedzicha JA. Increased chronic obstructive pulmonary disease exacerbations of likely viral etiology follow elevated ambient nitrogen oxides. Am J Respir Crit Care Med. 2019;199(5):581–591. doi:10.1164/rccm.201712-2506OC
44. Shin HH, Maquiling A, Thomson EM, Park IW, Stieb DM, Dehghani P. Sex-difference in air pollution-related acute circulatory and respiratory mortality and hospitalization. Sci Total Environ. 2022;806(Pt 3):150515. doi:10.1016/j.scitotenv.2021.150515
45. Sebastiao BF, Hortelao RM, Granadas SS, Faria JM, Pinto JR, Henriques HR. Air quality self-management in asthmatic patients with COPD: an integrative review for developing nursing interventions to prevent exacerbations. Int J Nurs Sci. 2024;11(1):46–56. doi:10.1016/j.ijnss.2023.12.003
46. To T, Zhu J, Larsen K, et al. Progression from asthma to chronic obstructive pulmonary disease. Is air pollution a risk factor? Am J Respir Crit Care Med. 2016;194(4):429–438. doi:10.1164/rccm.201510-1932OC
47. Nurhussien L, Kang CM, Koutrakis P, Coull BA, Rice MB. Air pollution exposure and daily lung function in chronic obstructive pulmonary disease: effect modification by eosinophil level. Ann Am Thorac Soc. 2022;19(5):728–736. doi:10.1513/AnnalsATS.202107-846OC
48. Bourbeau J, Doiron D, Biswas S, et al. Ambient air pollution and dysanapsis: associations with lung function and chronic obstructive pulmonary disease in the Canadian cohort obstructive lung disease study. Am J Respir Crit Care Med. 2022;206(1):44–55. doi:10.1164/rccm.202106-1439OC
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.