Back to Journals » Clinical Ophthalmology » Volume 17
Contrast Sensitivity and Patient Reported Outcomes After Bilateral Implantation of a Bi-Aspheric Hydrophobic Trifocal Diffractive Intraocular Lens
Authors Tañá-Rivero P, Orts-Vila P, Aguilar-Córcoles S, Tañá-Sanz P, Tañá-Sanz S
Received 7 December 2022
Accepted for publication 30 December 2022
Published 19 January 2023 Volume 2023:17 Pages 247—258
DOI https://doi.org/10.2147/OPTH.S400136
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Pedro Tañá-Rivero, Paz Orts-Vila, Salvador Aguilar-Córcoles, Pedro Tañá-Sanz, Santiago Tañá-Sanz
Cataract Surgery Department, Oftalvist Alicante, Alicante, Spain
Correspondence: Pedro Tañá-Rivero, Cataract Surgery Department, Oftalvist Alicante, C/ Angel Lozano 11, Alicante, 03001, Spain, Tel +34 965 141 500, Email [email protected]
Purpose: To assess contrast sensitivity and patient reported outcomes after uncomplicated cataract surgery with a new bi-aspheric diffractive trifocal intraocular lens (IOL) implantation.
Methods: Twenty-five patients who underwent bilateral implantation with the Asqelio Trifocal TFLIO130C IOL (AST Products Inc., Billerica, MA, USA) were analyzed at 6 months post-surgery. Binocular contrast sensitivity with and without glare was measured under photopic conditions (85 cd/m2) and mesopic conditions (3 cd/m2). Patients were asked to complete the Catquest-9SF patient outcomes questionnaire and a visual symptoms questionnaire.
Results: Photopic contrast sensitivity values were either within or above normal levels without glare; when glare was induced, the mean sensitivity values dropped just below normal range. Mesopic contrast sensitivity values were above or within normal range both with and without glare, except for 12 cpd with glare, where the mean fell just below the normal range. Differences in binocular contrast sensitivity threshold values with and without glare were significant for all spatial frequencies tested under both photopic and mesopic conditions (p< 0.05). The Catquest-9SF questionnaire outcomes showed that 88% of patients were either satisfied or very satisfied with their sight after the surgery, and in all cases, the results indicated no difficulty in performing different daily activities. The visual symptoms questionnaire indicated no relevant visual symptoms regarding frequency, intensity, or bothersomeness after implantation of the trifocal IOL.
Conclusion: This novel bi-aspheric diffractive trifocal IOL provides good contrast sensitivity outcomes under bright and dim lighting conditions. Patients were satisfied with the surgery, with no relevant visual symptoms.
Keywords: multifocal intraocular lens, cataract surgery, contrast sensitivity, patient reported outcomes, visual symptoms
Introduction
Multifocal intraocular lenses (IOLs) have been designed to provide satisfactory vision at different distances to the pseudophakic patient without the use of additional correction with spectacles. To achieve this goal, it is necessary to create different foci, two or three depending on the IOL design. In bifocal or trifocal IOLs, these foci create different images superimposed on the retina. The undesired effect of light of the out-of-focus image (depending on the foci and where the object is located) is to reduce the contrast of the in-focus image. The different distribution of light may be the source of contrast sensitivity reduction.1 This reduction may be more evident under low lighting conditions since the light distribution may vary depending on the pupil aperture as a function of the IOL design, and can increase visual disturbances. However, despite several studies having shown a reduction in contrast sensitivity in patient implanted with multifocal IOLs compared to those implanted with monofocal IOLs, it has been suggested that the difference between IOL types was smaller than anticipated.2
A systematic review published in 2017 concluded that different studies have demonstrated that a reduced contrast sensitivity and a higher rate of dysphotopsia are risks associated with seeking spectacle independence by means of multifocal IOL implantation.3 In addition, the assessment of predictors of resulting postoperative quality of life satisfaction is increasingly important to help cataract surgeons perform adequate preoperative patient suitability assessment in order to choose the most appropriate option to optimize functional postoperative outcomes. Contrast sensitivity has been measured in trifocal IOLs, showing different outcomes taking into account the design of the IOL, conditions of measurement, and the instrument used.4–22
The benefit of spectacle independence could be achieved in multifocal IOL patients, at the cost of contrast sensitivity reduction and also increased photic phenomena, which correlates with patient satisfaction and visual symptoms. Thus, we consider that these metrics should be analyzed in patients implanted with any new design of multifocal IOL available on the market. The purpose of the current study was to evaluate the contrast sensitivity under different lighting conditions and patient reported outcomes following uncomplicated cataract surgery with implantation of the novel bi-aspheric Asqelio™ Trifocal TFLIO130C IOL (AST Products Inc, Billerica, MA, USA).
Methods
This was a prospective study that comprised patients submitted to bilateral lensectomy with implantation of the Asqelio trifocal IOL at the Oftalvist Clinic in Alicante, Spain. The research was carried out in accordance with the tenets of the Declaration of Helsinki and was approved by the Hospital Clínico San Carlos Ethics Committee (Code 21/592-O_P). Informed consent was obtained from all patients after a complete explanation of the nature and possible consequences of the study had been provided. The study was registered at www.clinicaltrials.gov (registration number: NCT05065749).
Inclusion criteria included being ≥50 years of age, bilateral IOL implantation, desire to achieve spectacle independence for any working distance, transparent ocular media other than crystalline lens, and potential postoperative visual acuity of 20/25 or better. Exclusion criteria included corneal astigmatism of 1.00 D or higher, previous corneal or intraocular surgery, corneal disease, abnormal iris or pupil deformation, macular degeneration or retinopathy, neuro-ophthalmic disease, history of glaucoma or retinal detachment, and history of ocular inflammation.
Intraocular Lens
Patients were implanted with the Asqelio Trifocal TFLIO130C IOL model (Figure 1). This C-loop haptic lens has a posterior diffractive optic design (15 rings within the central 4.5 mm, with the inner ring being 1.5 mm in diameter) within its 6.0 mm of optical zone diameter. It has a total diameter of 13.0 mm and provides additions of +2.20 and +3.30 D for intermediate and near distances, respectively. The lens is built with powers ranging from +5.00 to +34.00 D in 0.50 D increments, and has a light distribution between foci of 50% for distance, 24% for intermediate, and 26% for near. It has a bi-aspheric geometry with a spherical aberration of −0.27 microns, and is made of a soft hydrophobic acrylic material (glistening-free) with a refractive index of 1.50 and an Abbe number of 50.
 |
Figure 1 AsqelioTM Trifocal TFLIO130C intraocular lens. Courtesy of AST Products, Inc. |
Surgical Technique
A limbal incision of 2.2 mm was made, followed by the creation of a 5 mm centered manual curvilinear capsulorhexis. A standard phacoemulsification with the Centurion® Vision System (Alcon Labs Inc, Fort Worth, TX, USA) was carried out. The spherical IOL power was determined using the ORA system with Verifeye+ (Alcon, Fort Worth, TX, USA) in the aphakic condition, and the target refraction was emmetropia.
Measurements
The standard ophthalmologic examinations included visual performance, refraction, slit-lamp biomicroscopy, optical biometry Goldmann applanation tonometry, and binocular indirect ophthalmoscopy through dilated pupils. Binocular contrast sensitivity was determined with distance correction, both with and without glare, for spatial frequencies of 3, 6, 12, and 18 cycles per degree under photopic conditions (85 cd/m2), and 1.5, 3, 6, and 12 cycles per degree under mesopic conditions (3 cd/m2), using the Clinical Trial Suite (M&S Technologies, Inc, IL, USA) at least 6 months postoperatively (mean follow-up time 9.46±2.75 months). Absolute contrast threshold (log Contrast) values were determined for each combination of patient, spatial frequency, and luminance level, and mean values and standard deviations were then calculated. Corresponding contrast sensitivity values were computed from those thresholds as well (log CS), to plot the contrast sensitivity function. All examinations were carried out by the same optometrist, who was unaware of the objective of the study.
Patient Reported Outcomes
Patients were asked to complete two different questionnaires: the Catquest-9SF patient outcomes questionnaire and a visual symptoms questionnaire. The Catquest-9SF is a well-known nine-item questionnaire to determine patients’ limitations in daily life for carrying certain activities due to reduced vision, and its value in cataract surgery patients has been well reported.23,24 It has been translated into many languages, validated through Rasch analysis,25 and is recommended by the International Consortium of Health Outcomes Measurement26 and the European Registry of Quality Outcomes for Cataract and Refractive Surgery.27 The test comprises nine items with four response options, ranging from 4 for “very great difficulty/very dissatisfied” to 1 for “no difficulty/very satisfied”, and a “cannot decide” additional option, which is treated as missing data. Items A and C1–C7 are concerned with difficulty, while item B deals with satisfaction. The visual symptoms questionnaire explores the frequency, intensity, and bothersomeness of 10 different and common visual symptoms. These symptoms are: glare, halos, starbursts, foggy vision, blurred vision, distortion, double vision, fluctuation in vision, difficulty focusing, and difficulty judging distances or depth. A simulated image is shown to the patient to aid in the description of each of the symptoms, and they are asked to respond with four response options regarding the frequency of the symptom, from 1 for “Never” to 4 “Very often”, the intensity of the symptom, from 1 for “None” to 4 for “Severe”, and the level of bothersomeness of the symptom, from 1 for “None” to 4 for “A lot”.
Statistical Analysis
Data analysis was performed using IBM® SPSS® for Mac v.26.0.0 (SPSS Inc, Chicago, IL) and Microsoft Excel for Mac v.16.66.1 (Microsoft Inc, Redmont, WA). The normality of the data was checked by the Shapiro–Wilk test. Statistical differences in contrast sensitivity with and without glare were analyzed with either the paired t-test or the Mann–Whitney test when distributions were normal or not normal, respectively. Data were reported as mean ± SD. Differences were considered statistically significant when the p-value was lower than 0.05. Descriptive statistics and frequencies were used to analyze questionnaire outcomes.
Results
In total, 50 eyes of 25 consecutive patients were enrolled in this study. Table 1 shows the demographics of the patients included in the study. The mean age was 67.24±7.76 years (range 52 to 84 years), and 21 were female (84%) and four male (16%). No complications in any of the cases were reported during the surgery and follow-up.
 |
Table 1 Demographic Characteristics of Participants, Shown as Mean±SD and Range |
Contrast Sensitivity
Figure 2 shows the mean contrast sensitivity function determined under photopic conditions (85 cd/m2) with and without glare. Given that the CTS system does not provide a reference range of normality for healthy subjects under photopic and mesopic conditions with and without glare, the normal ranges for non-operated eyes above 60 years of age used by Escaf et al,28 using the Functional Acuity Contrast Test (FACT), were used as a reference here. The results show that while the values were either within or above normal levels without glare, when glare was induced the mean sensitivity values dropped just below the normal range. Under mesopic conditions (3 cd/m2) (see Figure 3), however, contrast sensitivity function values were above or within the normal range both with and without glare, except for 12 cpd with glare, where the mean fell just below the normal range. Differences in binocular contrast sensitivity threshold values with and without glare were significant for all spatial frequencies tested under both photopic and mesopic conditions (p<0.05) (Table 2).
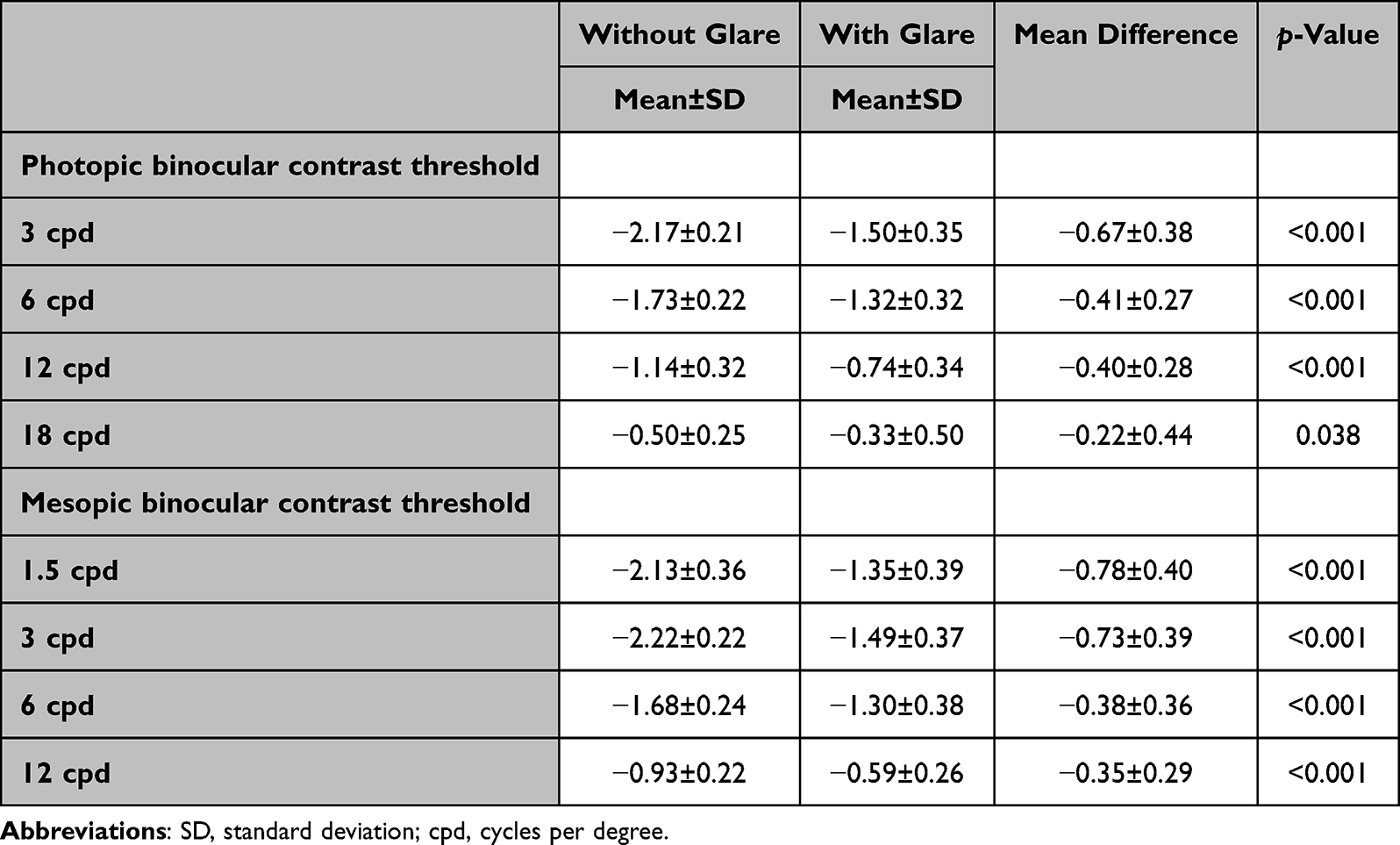 |
Table 2 Mean Binocular Photopic (85 cd/m2) and Mesopic (3 cd/m2) Contrast Threshold Values with and without Glare (Reported as log Contrast), Along with Mean Difference and Significance of the Difference |
 |
Figure 2 Contrast sensitivity function determined under photopic conditions (85 cd/m2) without (A) and with induced glare (B). Dotted lines delimit the normal range for non-operated eyes above 60 years of age using the Functional Acuity Contrast Test (FACT).28 Error bars represent the 95% confidence intervals. |
 |
Figure 3 Contrast sensitivity function determined under mesopic conditions (3 cd/m2) without (A) and with induced glare (B). Dotted lines delimit the normal range for non-operated eyes above 60 years of age using the Functional Acuity Contrast Test (FACT).28 Error bars represent the 95% confidence intervals. |
Patient Reported Outcomes
The results obtained from the Catquest-9SF questionnaire show that 88% of patients were either satisfied (8) or very satisfied (14) with their sight after the surgery, while one patient reported being very unsatisfied with the outcomes. Table 3 displays the average scoring and frequency of responses to the questions related to difficulty in performing daily activities as per the Catquest-9SF. In all cases, the results indicate no difficulty in performing any of these activities. Table 4 summarizes the outcomes of the visual symptoms questionnaire following the surgery. The mode indicates no relevant visual symptoms in frequency, intensity, or bothersomeness after implantation of the trifocal IOL. As expected, the frequency of halos was higher than that of the other visual symptoms, with 40% of patients reporting the presence of halos quite often (3) or very often (7), but 76% of patients reported either no bothersomeness (10) or a little (9).
 |
Table 3 Summary of Patient Reported Difficulties with Vision Determined by the Catquest-9SF Questionnaire |
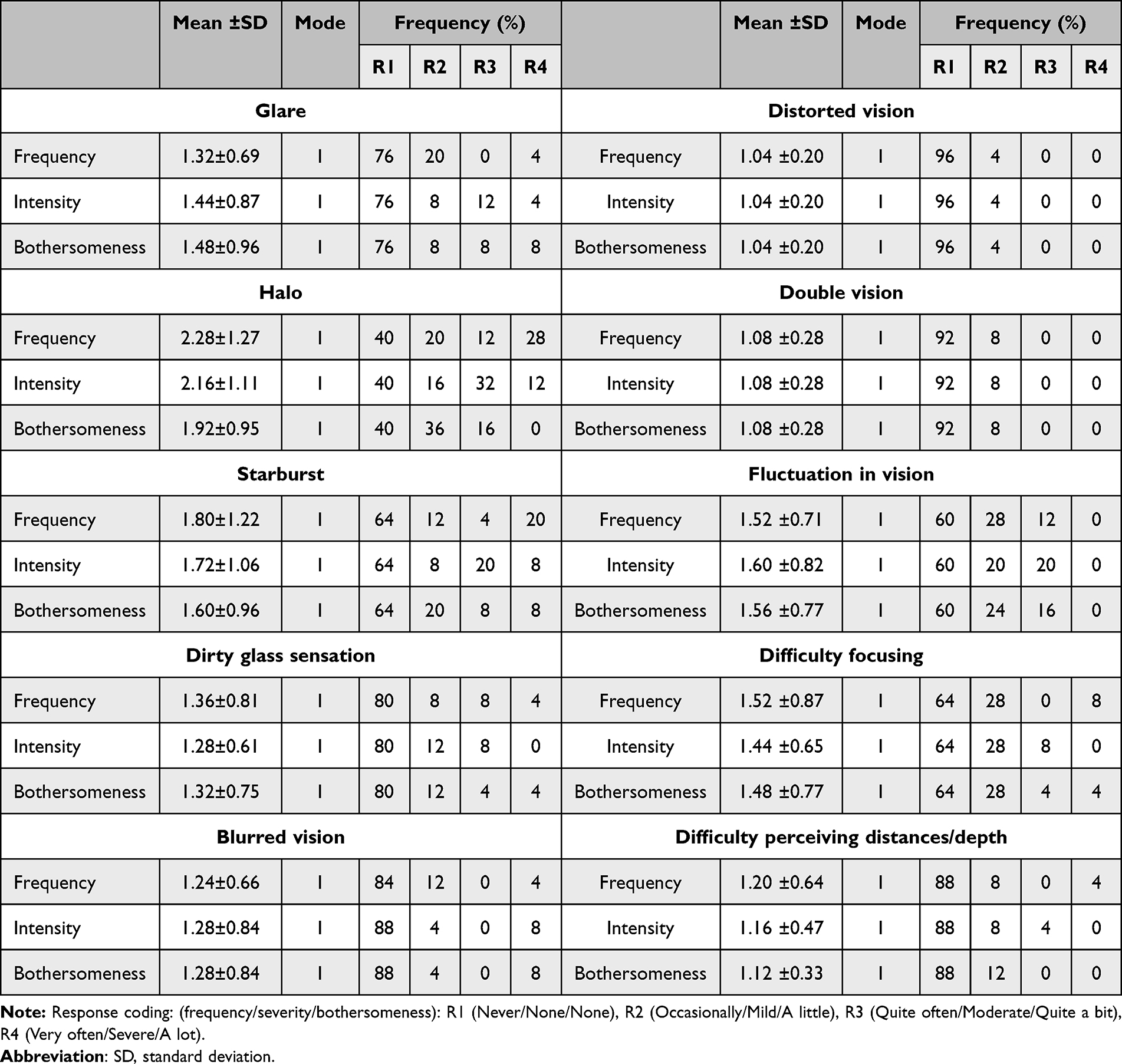 |
Table 4 Summary of Patient Reported Visual Symptoms (Mean Score, Mode, and Frequency of Responses) as per the Visual Quality Questionnaire |
Discussion
Contrast sensitivity measurement in clinical studies with multifocal IOLs helps us to gain a better understanding of the visual performance achieved postoperatively and the visual complaints that may arise from the correction using multifocality,29 since patients can refer to visual complaints due to a drop in contrast sensitivity even while maintaining good visual acuity. Dividing the incoming light into three foci for trifocal IOLs may decrease the amount of energy focused on each of these three foci, which inherently may affect the patient’s visual quality. Then, measurement under different lighting conditions and also with glare should be carried out to properly understand the visual performance of these patients and the effect of possible photic phenomena on their satisfaction after the surgery. In the present study, we aimed to measure these parameters to fully study the overall performance of patients implanted with a new bi-aspheric diffractive trifocal IOL.
The present results reveal that mean contrast sensitivity values under photopic conditions were above the normal range for low special frequencies and within the normal range for the rest of frequencies explored, but with glare the values fell just below the normal range for spatial frequencies, except for 18 cpd. Under mesopic conditions without glare, values were above the normal range for low spatial frequencies and over the upper limit of the normal range for the higher frequencies explored. With glare, these values were either within or above the normal range for all frequencies explored except for 12 cpd, where the value fell just below the normal range. It must be noted, however, that comparisons with normal ranges in the present analysis are limited by the fact that the normal ranges used correspond to a different CS determination method, owing to the lack of an age-matched reference range under the same conditions with the CTS system used in the present study, and therefore conclusions must take this into consideration. Despite this, the outcomes do show good contrast sensitivity overall under the different conditions measured.
Unfortunately, there are no previous publications reporting contrast sensitivity outcomes in patients implanted with the Asqelio Trifocal IOL to compare with the results reported herein. However, it is interesting to discuss the outcomes found in studies with other trifocal diffractive IOLs available on the market. Table 5 shows peer-reviewed publications reporting data on contrast sensitivity in patients implanted with non-toric trifocal IOLs with a minimum of 6 months of follow-up. It should be noted that the use of other trifocal lenses (with a different optical design: foci location and light percentage/focus), a different device to determine contrast sensitivity (sine-wave gratings or letters), different lighting conditions (cd/m2 value and with or without glare), and a different follow-up period (possible neuroadaptation with time) may produce different contrast sensitivity outcomes.
 |
Table 5 Peer-Reviewed Publications Reporting Data on Contrast Sensitivity in Patients Implanted with Non-Toric Trifocal Intraocular Lenses with a Minimum of 6 Months of Follow-Up |
The trifocal Finevision IOL (PhysIOL sa, Liege, Belgium) was assessed by several authors.4,9,12 Alió et al,4 in a sample of 20 patients, concluded that the monocular contrast sensitivity under scotopic conditions was within the normal range for a population aged >60 years. Cochener,9 in 15 patients, agreed with the previous authors and concluded that the contrast sensitivity results with the Finevision IOL were good and within normal limits under photopic conditions. They compared the outcomes with the bifocal Tecnis ZMB00 IOL and found that there were significant differences in contrast sensitivity between the two IOLs with and without glare at any spatial frequency (1.5, 3, 6, and 12 cpd, p>0.05). And, finally, Levinger et al,12 in 26 eyes of 26 patients (unilateral refractive lens exchange) concluded that at 6 (p=0.02), 12 (p=0.003), and 18 (p=0.04) cpd, the non-operated eyes showed better contrast sensitivity (about 0.2 log units) than the operated eyes.
Other authors evaluated the AT LISA tri 839MP (Carl Zeiss Meditec, Jena, Germany).5–8,10,11,17,21 Mojzis et al,5,7,11 in three studies with 6 and 12 months of follow-up, measured the photopic and mesopic contrast sensitivity. They reported high sensitivity to medium spatial frequencies at 6 months, although rapidly decreasing for higher frequencies, and roughly within the normal range for normal subjects aged between 50 and 60 years. At 12 months, they found good levels of contrast sensitivity.7 In their last study11 (comparing with the bifocal AT LISA 801), they found that the contrast sensitivity outcomes were somewhat more limited than those obtained with monofocal IOLs. They found minimal differences among the AT LISA tri and the AT LISA 801, only significant for some low to medium spatial frequencies 6 months postoperatively. Law et al,6 using the Pelli–Robson test for photopic and mesopic conditions, found mean values consistent with those reported using the same test in other modalities of multifocal IOLs. The same author group21 reported outcomes at 12 months post-surgery also using the CSV-1000 test compared with an extended depth of focus (EDOF), and concluded that the AT LISA and Symfony (Johnson&Johnson Vision) IOL cohorts achieved similar contrast sensitivity values in photopic conditions for 3, 6, and 12 cpd. Ganesh et al10 measured the binocular mesopic contrast sensitivity using the FACT chart at different times post-surgery, and found that the contrast sensitivity scores were comparable at 12 months and 1 month for all spatial frequencies.
Gyory et al13,20 assessed the Liberty Bi-Flex 677MY IOL (Medicontur Medical Engineering Ltd, Budapest, Hungary) in two studies with different follow-up durations using the CSV-1000. They reported that the mesopic and photopic contrast sensitivity values were within the upper normal range for age-matched values in the 24-month study (50 patients), and they were in the upper third range of the age-matched normal values in the 60-month study (37 patients).
The AcrySof IQ PanOptix TFNT00 IOL (Alcon Labs, Fort Worth, TX, USA) has also been analyzed in several clinical studies. Yesilirmak et al14 carried out a study comparing mix-and-match implanted bifocal AcrySof ReSTOR +2.50/+3.00 D (Alcon Labs, Fort Worth, TX, USA) IOLs with bilateral PanOptix IOLs. They concluded that PanOptix IOLs implanted bilaterally provided better contrast sensitivity than mix-and-match implanted AcrySof ReSTOR +2.50/+3.00 D IOLs. Alfonso et al,15 in a sample of 40 bilateral patients, concluded that values fell within the standard range for normal patients. Bissen-Miyajima et al16 measured distance and near photopic contrast sensitivity in 68 Japanese patients, with 6 months of follow-up. They concluded that contrast sensitivity was within the normal range for distance and near vision for all spatial frequencies measured under photopic conditions. In another study, Song et al,18 comparing mix-and-match implantation of the Tecnis ZLB00 IOL (Johnson&Johnson Vision) and Symfony EDOF IOL, concluded that contrast sensitivity was within the normal range. In addition, they found no statistically significant differences between bilateral implantation of PanOptix IOL and mix-and-match (Symfony and Tecnis ZLB00 IOL) under different light conditions for any spatial frequency. Modi et al19 compared the PanOptix IOL with the monofocal SN60AT IOL (Alcon Labs, Fort Worth, TX, USA) in a large sample study, and concluded that the mean contrast sensitivity was lower for higher spatial frequencies in patients implanted with PanOptix IOL compared to monofocal IOL recipients, under either photopic or mesopic conditions and regardless of the presence of glare. However, they concluded that these differences were lower than the levels required for clinical significance. Labiris et al22 compared the efficacy of premium monovision (trifocal PanOptix IOL implantation in the non-dominant eye and bifocal AcrySof ReSTOR +2.50 D IOL in the dominant eye) against myopic monovision (monofocal SN60WF IOL [Alcon Labs, Fort Worth, TX, USA] in both eyes) targeting −0.50 and −1.25 D in the dominant and non-dominant eye, respectively, hybrid monovision (trifocal PanOptix IOL in the non-dominant eye and SN60WF IOL in the dominant eye), and bilateral PanOptix IOL implantation. They found no significant differences in photopic contrast sensitivity among these groups of patients, using the Pelli–Robson test. And, finally, Lapid-Gortzak et al17 compared the PanOptix and the AT LISA tri in a large group of patients (86 versus 81) at 6 months post-surgery using the CSV-1000. They concluded that binocular contrast sensitivity showed similar results for both IOL models (within ±0.05 log units) for all spatial frequencies under both photopic and mesopic conditions, and both with and without glare.
With regard to the patient reported outcomes (Tables 3 and 4), the results are in agreement with those reported by Palomino-Bautista et al30 and Cano-Ortiz et al31 with the same IOL. In the Palomino-Bautista et al30 study, where patients were asked to score their satisfaction level, as well as the level of halo perception and bothersomeness, on a scale from 0 to 10, the average response was 8.32 (out of 10) with regard to overall satisfaction with vision after surgery, and 4.36 (out of 10) with regard to halo bothersomeness. In the Cano-Ortiz et al31 study, where the Catquest-9SF and visual symptoms questionnaires were used, all patients reported being satisfied with their vision at present (reporting a mean score of 3.60±0.50 out of 4), with 20% reporting some difficulties with vision in daily life and 80% no difficulty at all (mean score reported was 3.80±0.41 out of 4). In their study, halos were also the visual symptom most commonly referred to by patients, where more than 50% of the patients reported experiencing halos on a regular basis or constantly, but just 16% reported significant impairment as a result.
Our study assessed only subjective metrics through contrast sensitivity to assess the visual performance of the patient. Future studies should consider other metrics, such as the defocus curve, or specifically objective metrics, such as wavefront aberrometry, to fully describe the performance of the lens when implanted.
Conclusion
In conclusion, the novel bi-aspheric diffractive trifocal IOL provides good contrast sensitivity outcomes under both bright and dim lighting conditions, with and without glare, with patients reporting satisfaction with the visual outcomes and no relevant visual symptoms.
Data Sharing Statement
Data are not available for sharing.
Funding
This study was supported by a grant from AST Products Inc.
Disclosure
Dr Pedro Tañá-Rivero reports grants from AST Products Inc, during the conduct of the study; grants from Alcon Labs, grants from Carl Zeiss Meditec, grants from Hoya, grants from HumanOptics, grants from Johnson & Johnson, grants from Physiol sa, and grants from Staar Surgical, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Pieh S, Weghaupt H, Skorpik C. Contrast sensitivity and glare disability with diffractive and refractive multifocal intraocular lenses. J Cataract Refract Surg. 1998;24:659–662. doi:10.1016/S0886-3350(98)80261-7
2. de Silva SR, Evans JR, Kirthi V, Ziaei M, Leyland M. Multifocal versus monofocal intraocular lenses after cataract extraction. Cochrane Database Syst Rev. 2016;12:CD003169. doi:10.1002/14651858.CD003169.pub4
3. Wang SY, Stem MS, Oren G, et al. Patient-centered and visual quality outcomes of premium cataract surgery: a systematic review. Eur J Ophthalmol. 2017;27:387e401. doi:10.5301/ejo.5000978
4. Alió JL, Montalbán R, Peña-García P, Soria FA, Vega-Estrada A. Visual outcomes of a trifocal aspheric diffractive intraocular lens with microincision cataract surgery. J Refract Surg. 2013;29(11):756–761. doi:10.3928/1081597X-20131021-05
5. Mojzis P, Peña-García P, Liehneova I, Ziak P, Alió JL. Outcomes of a new diffractive trifocal intraocular lens. J Cataract Refract Surg. 2014;40(1):60–69.
6. Law EM, Aggarwal RK, Kasaby H. Clinical outcomes with a new trifocal intraocular lens. Eur J Ophthalmol. 2014;24(4):501–508. doi:10.5301/ejo.5000407
7. Mojzis P, Majerova K, Hrckova L, Piñero DP. Implantation of a diffractive trifocal intraocular lens: one-year follow-up. J Cataract Refract Surg. 2015;41(8):1623–1630. doi:10.1016/j.jcrs.2014.11.050
8. Alfonso JF, Fernández-Vega Cueto L, Belda-Salmerón L, Montés-Micó R, Fernández-Vega L. Visual function after implantation of a diffractive aspheric trifocal intraocular lens. Eur J Ophthalmol. 2016;26(5):405–411. doi:10.5301/ejo.5000741
9. Cochener B. Prospective clinical comparison of patient outcomes following implantation of trifocal or bifocal intraocular lenses. J Refract Surg. 2016;32(3):146–151. doi:10.3928/1081597X-20160114-01
10. Ganesh S, Brar S, Pawar A. Long-term visual outcomes and patient satisfaction following bilateral implantation of trifocal intraocular lenses. Clin Ophthalmol. 2017;11:1453–1459. doi:10.2147/OPTH.S125921
11. Mojzis P, Kukuckova L, Majerova K, Ziak P, Piñero DP. Postoperative visual performance with a bifocal and trifocal diffractive intraocular lens during a 1-year follow-up. Int J Ophthalmol. 2017;10(10):1528–1533. doi:10.18240/ijo.2017.10.08
12. Levinger E, Levinger S, Mimouni M, et al. Unilateral refractive lens exchange with a multifocal intraocular lens in emmetropic presbyopic patients. Curr Eye Res. 2019;44(7):726–732. doi:10.1080/02713683.2019.1591460
13. Gyory JF, Madár E, Srinivasan S. Implantation of a diffractive-refractive trifocal intraocular lens with centralized diffractive rings: two-year results. J Cataract Refract Surg. 2019;45(5):639–646. doi:10.1016/j.jcrs.2019.01.024
14. Yesilirmak N, Akova YA, Donmez O. Comparison of mix-and-match implanted bifocal iols and bilateral implanted trifocal IOLs after femtosecond laser-assisted cataract surgery. J Refract Surg. 2019;35(9):559–564. doi:10.3928/1081597X-20190806-01
15. Alfonso JF, Fernández-Vega-Cueto L, Fernández-Vega L, Montés-Micó R. Visual function after implantation of a presbyopia-correcting trifocal intraocular lens. Ophthalmic Res. 2020;63(2):152–164. doi:10.1159/000500834
16. Bissen-Miyajima H, Ota Y, Hayashi K, Igarashi C, Sasaki N. Results of a clinical evaluation of a trifocal intraocular lens in Japan. Jpn J Ophthalmol. 2020;64(2):140–149. doi:10.1007/s10384-019-00712-4
17. Lapid-Gortzak R, Bhatt U, Sanchez JG, et al. Multicenter visual outcomes comparison of 2 trifocal presbyopia-correcting IOLs: 6-month postoperative results. J Cataract Refract Surg. 2020;46(11):1534–1542. doi:10.1097/j.jcrs.0000000000000274
18. Song JE, Khoramnia R, Son HS, Knorz MC, Choi CY. Comparison between bilateral implantation of a trifocal IOL and mix-and-match implantation of a bifocal IOL and an extended depth of focus IOL. J Refract Surg. 2020;36(8):528–535. doi:10.3928/1081597X-20200616-01
19. Modi S, Lehmann R, Maxwell A, et al. Visual and patient-reported outcomes of a diffractive trifocal intraocular lens compared with those of a monofocal intraocular lens. Ophthalmology. 2021;128(2):197–207. doi:10.1016/j.ophtha.2020.07.015
20. Győry JF, Srinivasan S, Madár E, Balla L. Long-term performance of a diffractive-refractive trifocal IOL with centralized diffractive rings: 5-year prospective clinical trial. J Cataract Refract Surg. 2021;47(10):1258–1264. doi:10.1097/j.jcrs.0000000000000670
21. Law EM, Aggarwal RK, Buckhurst H, et al. One-year post-operative comparison of visual function and patient satisfaction with trifocal and extended depth of focus intraocular lenses. Eur J Ophthalmol. 2022;32(5):2967–2974. doi:10.1177/11206721211069737
22. Labiris G, Panagiotopoulou EK, Perente A, et al. Premium monovision versus bilateral myopic monovision, hybrid monovision and bilateral trifocal implantation: a comparative study. Clin Ophthalmol. 2022;16:619–629. doi:10.2147/OPTH.S351091
23. McAlinden C, Gothwal VK, Khadka J, Wright TA, Lamoureux EL, Pesudovs K. A head-to-head comparison of 16 cataract surgery outcome questionnaires. Ophthalmology. 2011;118(12):2374–2381. doi:10.1016/j.ophtha.2011.06.008
24. Khadka J, McAlinden C, Pesudovs K. Quality assessment of ophthalmic questionnaires: review and recommendations. Optom Vis Sci. 2013;90(8):720–744. doi:10.1097/OPX.0000000000000001
25. Kabanovski A, Hatch W, Chaudhary V, et al. Validation and application of Catquest-9SF in various populations: a systematic review. Surv Ophthalmol. 2020;65(3):348–360. doi:10.1016/j.survophthal.2019.12.002
26. Mahmud I, Kelley T, Stowell C, et al. A proposed minimum set of outcome measures for cataract surgery. JAMA Ophthalmol. 2015;133(11):1247–1252. doi:10.1001/jamaophthalmol.2015.2810
27. Lundström M, Barry P, Brocato L, et al. European registry for quality improvement in cataract surgery. Int J Health Care Qual Assur. 2014;27(2):140–151. doi:10.1108/IJHCQA-10-2012-0101
28. Escaf LJ, Escaf LC, Polo S, Rodríguez-Vallejo M, Fernández J. Standard results and contrast sensitivity reestablishment after implantation of a trifocal intraocular lens. Curr Eye Res. 2021;46(5):672–677. doi:10.1080/02713683.2020.1828486
29. ISO-11979-7: 2018. Ophthalmic implants - Intraocular lenses – part 7: clinical investigations; 2018.
30. Palomino-Bautista C, Cerviño A, Cuiña-Sardiña R, Carmona-Gonzalez D, Castillo-Gomez A, Sanchez-Jean R. Depth of field and visual performance after implantation of a new hydrophobic trifocal intraocular lens. BMC Ophthalmol. 2022;22(1):240. doi:10.1186/s12886-022-02462-3
31. Cano-Ortiz A, Sánchez-Ventosa Á, González-Cruces T, et al. Visual performance, satisfaction, and spectacle independence after implantation of a new hydrophobic trifocal intraocular lens. J Clin Med. 2022;11(19):5931. doi:10.3390/jcm11195931
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparison of Distance-Based Uncorrected Visual Acuity Based on the Optical Profile of Same Platform IOLs
Suzuki H, Nishiyama M
Clinical Ophthalmology 2024, 18:671-678
Published Date: 6 March 2024
Comparison of Visual Performance and Patient Satisfaction Between Two Trifocal Intraocular Lenses: A Prospective, Paired-Eye Comparative Study
Kang S, Arsenault SM, O’Brien RC, Chatzea MS, Zarei-Ghanavati S, Beniz LAF, Yoo SH
Clinical Ophthalmology 2026, 20:572237
Published Date: 17 January 2026