Back to Journals » International Journal of Women's Health » Volume 14
Contraception During Perimenopause: Practical Guidance
Authors Grandi G ![]() , Di Vinci P, Sgandurra A, Feliciello L, Monari F, Facchinetti F
, Di Vinci P, Sgandurra A, Feliciello L, Monari F, Facchinetti F
Received 6 February 2022
Accepted for publication 7 July 2022
Published 15 July 2022 Volume 2022:14 Pages 913—929
DOI https://doi.org/10.2147/IJWH.S288070
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Giovanni Grandi,1 Pierluigi Di Vinci,2 Alice Sgandurra,1 Lia Feliciello,1 Francesca Monari,1 Fabio Facchinetti1
1Department of Medical and Surgical Sciences for Mother, Child and Adult, University of Modena and Reggio Emilia, Azienda Ospedaliero Universitaria Policlinico, Modena, 41124, Italy; 2International Doctorate School in Clinical and Experimental Medicine, Department of Biomedical, Metabolic and Neural Sciences, University of Modena and Reggio Emilia, Modena, 41124, Italy
Correspondence: Giovanni Grandi, Department of Medical and Surgical Sciences for Mother, Child and Adult, University of Modena and Reggio Emilia, Azienda Ospedaliero Universitaria Policlinico, Via del Pozzo 71, Modena, 41124, Italy, Tel +39 059 422 2665, Email [email protected]
Abstract: Climacteric is by no means in itself a contraindication to safe contraception. On the contrary, there are several conditions related to the perimenopause that could benefit from the use of modern contraceptives, mainly hormonal, with the goals of avoiding unintended pregnancies and giving further possible benefits beyond contraception (menstrual cycle control, a reduction of vasomotor symptoms and menstrual migraines, a protection against bone loss, a positive oncological risk/benefit balance). This narrative review aims to provide practical guidance on their possible use in this particular life stage, both short- and long-acting reversible contraceptives, and to assist clinicians for women transitioning from contraception to their menopausal years, including the possible initiation of postmenopausal hormone therapy. Comprehensive contraceptive counselling is an essential aspect of the overall health and wellbeing of women and should be addressed with each such patient irrespective of age.
Keywords: contraception, perimenopause, SARCs, LARCs, oral contraceptives, combined oral contraceptives, vaginal rings, patch, intrauterine devices, implants, forties, metabolism
Contraception in Perimenopause: Is There Need or Not?
The perimenopause is the period that precedes the menopause and is roughly a synonym of “menopausal transition”. It corresponds to the stages −1 and −2 according to the STRAW+10 Staging System for Reproductive Aging in Women,1 beginning when there is a variable persistent length of ≥7-day difference of consecutive menstrual cycles plus supportive clinical and endocrinological criteria.1
It starts 5–10 years before the menopause, at approximately 40 years of age.2 Since the population is aging, the total number of women aged 40–49 years is increasing by 32% in Europe. As defined by the Stages of Reproductive Aging Workshop (STRAW) criteria, the term perimenopause or menopausal transition covers the transition from reproductive age through to menopause, ie, early perimenopause (stage −2), late perimenopause (stage −1), the last menstrual period (stage 0) and early post-menopause (stage +1).3 The principal criteria for entry into the early perimenopause include the onset of irregular or “variable length” cycles with at least 7-day differences in cycle length between consecutive cycles or a cycle length <25 days or >35 days. Late perimenopause starts once the cycles exceed 60 days in length.
This period is characterised by several changes in the hormonal milieu of a woman: a reduction in the number of primordial follicles is demonstrated due to the lower levels of inhibin B and Anti-Müllerian Hormone (AMH)4 and the ovaries begin to decrease in weight and size.5 This is associated with an increase in follicle stimulating hormone (FSH) levels due to the decrease in oestradiol (E2) and inhibin B in the serum, which are fundamental to its negative feedback, while progesterone levels control luteinising hormone (LH).5 Moreover, the low levels of E2 cannot induce the LH peak that is necessary for ovulation. Therefore, due to these hormonal changes, the occurrence of anovulatory cycles increases and the interval between two ovarian cycles tends to be variable in length.6 The result is that the fertility of a woman during the perimenopause is lower but, at the same time, there are higher rates of unintended pregnancies among these women.7 Women over 40 have lower fecundity (chance of a live birth per menstrual cycle) compared with their younger cohort. The annual risk of pregnancy is clearly lower than that in younger women: 10% at 40–44 years to only 2–3% at 45–49 years.8 Although the risk of pregnancy is lower in this age group, the acceptance of pregnancy is also reduced with more women having elective abortions, so there is an important need for contraception. In 2006, the overall rate of unintended pregnancy in the United States was 49%, of which 48% represents women aged 40–44.9
In Italy, the abortions in this lifestage (>40 years old) were 8140 out of 65,757 total abortions in 2020 (12%) (http://dati.istat.it/Index.aspx?DataSetCode=DCIS_IVG_CARATTDON). This is the only phase of life in which abortions are not significantly decreasing from 2010 to 2020 in our Italian region, Emilia-Romagna (Figure 1) (https://salute.regione.emilia-romagna.it/siseps/applicazioni/ig/documentazione). In addition, these “late” pregnancies can be complicated by several factors, such as higher risk of miscarriages, chromosomal abnormalities (due to the poorer quality of oocytes generated in metaphase over 40 years10), ectopic pregnancy, preeclampsia and post-partum haemorrhage risk.11 In 2011, women aged 40–44 experienced spontaneous abortion at a rate of 34%, while women aged 45 and older reported a rate of 53% for ongoing pregnancies. Moreover, the age-related issues associated with the use of hormonal therapies must be analysed.12 Importantly, among them is the increased risk of cancer, the possible occurrence of osteopenia and osteoporosis, the risk of thromboembolism, psychological changes and the possible sexual dysfunction associated with this peculiar late reproductive period.13 Regarding the thromboembolic risk, it is strictly related to hypertension and cardiovascular diseases in general, as well as obesity and metabolic syndrome, whose incidence rises with age.14
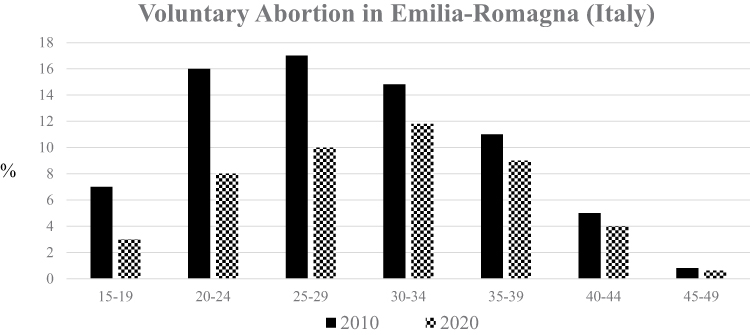 |
Figure 1 Comparisons between the percentage of voluntary abortions between 2010 and 2020 according to the different age groups in the Emilia-Romagna region (Italy). Notes: Data from: Regione Emilia-Romagna. Salute. Assessorato politiche per la salute; Relazione sull’interruzione volontaria digravidanza in Emilia-Romagna nel 2020 [Health Policy Department; Report on the voluntary termination of pregnancy in Emilia-Romagna in 2020]; 2021. Available from: https://salute.regione.emilia-romagna.it/siseps/applicazioni/ig/documentazione. Accessed February 1, 2022. Italian.101 |
Finally, another important problem often experienced during the climacteric period is represented by the abnormalities related to abnormal uterine bleeding (AUB), due to both organic and dysfunctional factors,15 which have a strong impact on the woman's life.16 Therefore, in the fourth and fifth decades of life in women there is a noticeable incidence of adenomyosis, polyps and fibroids, which are possible organic causes of AUB.17 Among the spectrum of perimenopausal uterine alterations, it is important to include endometrial hyperplasia, a condition that is characterised by morphological alterations in the ratio of endometrial glands/stroma.18 This disease frequently occurs after forties and the risks cannot be underestimated.
There are several conditions related to the perimenopause that could benefit from the use of modern contraceptives, mainly hormonal, with the goals of avoiding unintended pregnancies and providing further benefits beyond contraception. Fertility awareness-based methods are unreliable during the perimenopause because of unpredictable ovulation and cycles, as described above; therefore, they should not be utilised during this time. We will therefore detail the contraceptive options available to women over 40 and, also, the unique contraceptive and non-contraceptive benefits and health risks associated with different contraceptive methods in this population. Indeed, contraceptive use has recently been found to be relatively stable over time, with short-acting hormonal contraception and condoms being the most common contraceptive methods until women reach the age of 40–45 years when long-acting reversible contraceptives (LARCs) and permanent contraception become the most prevalent.19
In general, according to the International Medical Eligibility Criteria for Contraceptive Use, there is no single contraceptive choice contraindicated based on age alone20 because there is no evidence to suggest that age itself is a risk factor for contraceptive-related complications. However, with age comes an increased risk of some medical conditions, including obesity, hypertension, diabetes, hyperlipidaemia and cancer, which have to be considered as independent risk factors.
The aim of this narrative review is to give practical guidance on their possible use in this particular life stage, by separately describing Short- and Long-Acting Reversible Contraceptives (SARCs and LARCs, respectively) and to assist clinicians for women transitioning from contraception to their menopausal years, including the possible initiation of postmenopausal hormone therapy (HT). Comprehensive contraceptive counselling is an essential aspect of the overall health and wellbeing of women and should be addressed with each such patient irrespective of age. A practical guide to this particular medical counselling is reported in Box 1.
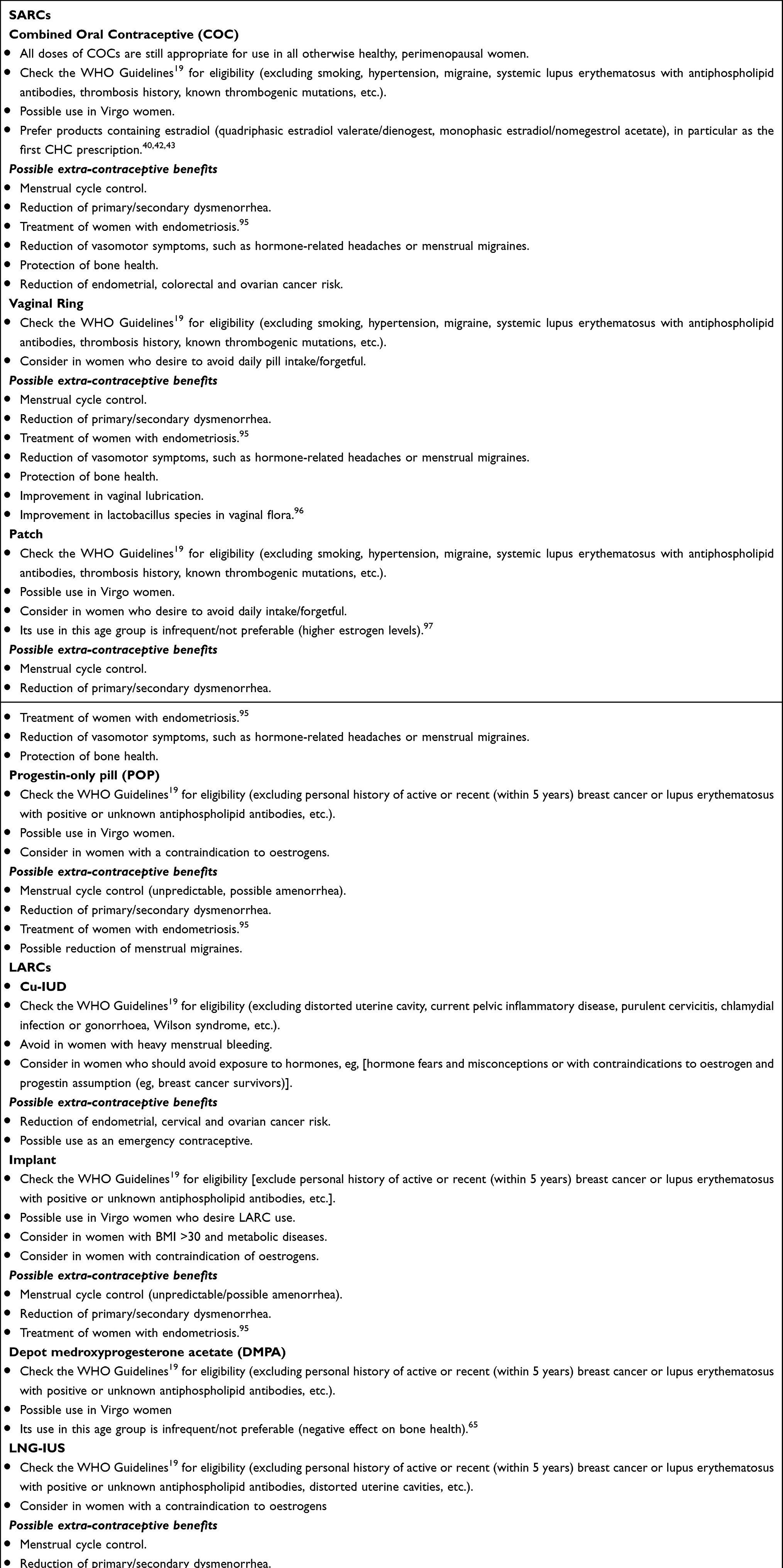 |
Box 1 Practical Guidance for Contraception Use in Perimenopause |
Short-Acting Reversible Contraceptives (SARCs)
Combined Hormonal Contraceptives (CHCs)
CHCs are available as a daily pill [combined oral contraceptives (COCs)], a weekly transdermal patch, a monthly vaginal ring (three weeks of use) and in few countries (US, Latin America) some monthly injectable combined contraceptives. These methods are made with an estrogenic component (“combined”), such as ethinyl-oestradiol (EE), E2, a natural oestrogen and, more recently, oestetrol (E4), in combination with many progestins, which can be derived from natural progesterone, from 19 nor-testosterone or by spironolactone.21
The general mechanism of action of these contraceptives is to inhibit ovulation, stabilise endometrial proliferation and modify the cervical mucus in order to make it inhospitable for the ascent of spermatozoa.22 CHCs are highly effective when correctly used, but they are prone to a higher risk of user failure due to the necessity of regular intake, so there is a significant difference between ideal use and typical use for contraceptive effectiveness. Perfect use failure rate is 0.3% and typical use failure rate is up to 7–9% in reproductive-age women. However, this difference is not as high in perimenopausal women compared to younger women due to the physiological decline of natural fertility.23 In the last 60 years, important developments in CHC technologies have been achieved, guaranteeing women more choices than in the past while maintaining/improving contraceptive efficacy: nowadays, new formulations of CHCs are available on the market with very low oestrogen doses as well as natural oestrogens (E2 and E4) and progestins without many of the androgenic side effects.21
A recent meta-analysis of 18 RCTs comparing the patch, ring and COCs found no significant differences in contraceptive effectiveness, indications and contraindications between the different SARCs.24
For women in perimenopause, CHC use offers, beyond a valid contraceptive method, potential additional benefits such as:
- satisfactory menstrual control, which avoids AUB, resulting in regular menstrual bleeds and further reducing dysmenorrhea and pelvic pain.25
- A reduction of vasomotor symptoms, such as hormone-related headaches or menstrual migraines, which occur in more than 60% of perimenopausal women, especially during a hormone-free interval (HFI).17,25,26
- Protection against bone loss via two mechanisms: preventing bone demineralisation, which is very important in this life-stage, and enhancing bone mineral density, even at low doses.27
- A reduction of endometrial, colorectal and ovarian cancer risk, close to their peak incidence.28
Overall, CHCs are still appropriate for use in all otherwise healthy, perimenopausal women.
The advantages of CHCs use in comparison to progestin-only contraceptives use are reported in Figure 2.
 |
Figure 2 Pros and cons of the use of combined hormonal contraceptives (CHCs) or progestin-only contraceptives in the perimenopause. |
COCs
COCs are the most commonly used hormonal contraceptives worldwide and remain a valid option thanks to their flexibility, convenience and well-known non-contraceptive benefits. COCs are available in:
- cyclic regimens, composed of 21 active pills and 7 inactive pills/no assumption
- a shortened HFI regimen, composed of 24–26 active pills and 2–4 inactive pills
- an extended regimen, which includes 84 active pills and 7 inactive pills
- a continuous regimen, which is made up of a 365 active pill regimen
The shorter the scheduled menstrual interval is, the less vasomotor effects, menstrual migraine and abnormal menstrual bleeding shall occur. Clinical experience shows that the continuous use of all types of COCs is effective in reducing blood loss.29 This reduction also seems to be influenced by the dosage of EE; in fact, it is greater with 30–35 µg compared to 20 µg30 and the type of oestrogen administered. Recent studies have demonstrated that even COCs with E2 seem to act very effectively in the management of heavy menstrual bleeding (HMB). In particular, it has been seen that the quadriphasic combination of oestradiol valerate (E2V) and dienogest has an important effect in reducing HMB, with a reduction of between 80 and 120 mL of blood per menstrual cycle.31
COCs, Vasomotor Symptoms and Menstrual Migraine
There is some evidence about the role of CHCs to also improve vasomotor symptoms: hot flushes could already appear in the premenopausal period and are effectively reduced by CHC use. For women who have already experienced the first symptoms of menopause during this period, COC therapy appears to be a more accepted option than postmenopausal hormone therapy (HT). One study evaluated COCs with an alternative option for oestrogen exposure during the usual placebo week: one group received 10 µg of EE for 5 days with 2 days of placebo and the other group received traditional placebo pills for 7 days. All women reported a decrease in somatic, anxiety and depression symptoms. In the group treated with additional oestrogen, there was an even larger decrease in vasomotor symptoms, depression, somatic symptoms and sexual dysfunction compared with those who received placebo during the hormone-free week.32
During perimenopause, migraine frequency and severity increase, particularly in women with menstrual migraine. This may partly be because menstruation and consequently menstrual migraine are more frequent as the cycle length shortens. Women with migraine also have a significantly increased risk of vasomotor symptoms, anxiety and depression, as well as sleep disturbance, further increasing morbidity. On the contrary, post-menopause, the prevalence of migraine without aura declines. In contrast, migraine with aura is not directly affected by menopause and headache becomes less of a feature of attacks with increasing age.33 In theory, continuous COC use, which suppresses ovarian activity as well as menstrual bleeding, should effectively manage hormonal migraine triggers. However, there are only limited clinical trial data regarding migraine. The European Headache Federation (EHF) and the European Society of Contraception and Reproductive Health (ESCRH) recommend COCs for women with migraine who require contraception, experience oestrogen-withdrawal headaches, or benefit from treatment with COCs for medical reasons.34 In all cases, continuous use is advised to prevent oestrogen-withdrawal migraine triggered during breaks. If breaks are necessary to control unscheduled bleeding, they should be shortened to four days. CHCs can be used by women with migraine without aura but are contraindicated for contraceptive use in women with migraine with aura since both COCs and aura are independent risk factors for ischemic stroke.
COCs and Bone Mineral Density
There are still no reliable data in the literature about the effect of COC on bone mineral density (BMD): in general, CHC use does not seem to exert any significant, nor detrimental or protective, effect on bone in the general population.35 While the strongest beneficial effect of CHCs on BMD was seen in perimenopausal women with low oestrogen levels, it is still not clear whether this effect might mitigate fracture risk.27
COCs and Cardiovascular Risk
The relative risk of thromboembolic diseases increases slightly in COC users, which is about two to three times higher than in non-users. However, the greatest risk occurs within the first 3 months of initiation (OR 12, 95% CI 7.1–22.4).36 The incidence of VTE sharply increases after age 40, thus demonstrating that age plays an important role. A meaningful Danish cohort study found that the incidence of VTE in COC users rose from 8.7 per 10000 women-years for women aged 30–34 to 20.8 per 10000 women-years for women aged 45–49.37 Another large case–control study found that the incidence rate of VTE in COC users increased by nearly 3-fold between the ages 20–29 and over 40.38 The risk of VTE in patients using COCs is influenced by both the type of progestin and the dose of oestrogen contained. A study performed by Sugiura et al shows that COCs with 20 µg of EE have a lower risk of pulmonary embolism and serious arterial thromboembolic events than COCs with 30–40 µg EE. In addition, using COC-containing levonorgestrel (LNG) is associated with a 50% lower risk of pulmonary embolism (PE) compared with using a COC with a third-generation progestin.39 The absolute risk of thrombotic stroke (TS) and myocardial infarction (MI) associated with COC is low in women of reproductive age but increases with age, EE dose and the presence of additional cardiovascular risk factors such as smoking, hypertension, diabetes, obesity and hyperlipidaemia.7 However, during counselling, the increased maternal morbidity and mortality of pregnancy related to older age should be addressed, including the fact that any particular contraindication of hormonal contraceptives also increases the risk of significant adverse events during pregnancy.
The incidence of TS and myocardial infarction (MI) was 20- and 100-times higher in an older cohort (aged 45–49 years) versus a younger cohort (aged 15–19 years) of Danish women, respectively; also, considering COC use, the overall risk of stroke increases by 2.2-times and that of MI by 2.3-times.37 A significantly increased risk of TS in women who use CHCs was also shown in a Cochrane review40 including 24 observational studies. The dose of EE seems to influence the risk of TS and MI. The Cochrane review found the relative risk of stroke and MI to increase from 1.6 (95% CI 1.4–1.8) for 20 μg EE to 2.0 (95% CI 1.4–3.0) for 30–50 μg EE; also, the Danish study had comparable, but non-significant findings, with an RR of 1.6–1.9 for current COC use depending on EE dose.37
In recent years, COCs containing E2 rather than EE have been developed.41 The most important exponents are a quadriphasic preparation containing E2V+dienogest (DNG) and a monophasic preparation containing micronised E2+nomegestrol acetate (NOMAc). Both have a short HFI, which results in better menstrual cycle control. It seems that using an estrogenic component identical to the natural one might offer a safer alternative to the traditional pill containing EE. These preparations share some similarities with postmenopausal HT preparations, rather than COCs, and so have theoretical safety benefits for women over 40. However, there is currently insufficient evidence to define a specific recommendation for the use of these preparations in women over 40. Preparations containing natural E2 seem to be more neutral than those with EE due to their theoretical safety benefits for women over 40 years of age; in the Expert Opinion of the authors, these are clearly the first-line choice between different CHCs in these women, especially if non-oral methods of E2 administration will be soon available.42
Noteworthy, WHO eligibility criteria do not report differences between E2 and EE-containing products,19 but, it is assumed that there could be a risk difference between diverse oestrogen components (EE versus E2). The INAS SCORE study by Dinger et al shows that COC containing E2V and DNG is associated with a similar or even lower cardiovascular risk compared to COCs containing LNG or other progestins.43 A similar recent large post-marketing study that includes a total of 101,498 women, with 49,598 using E2-NOMAc and 51,900 using EE-LNG for up to 2 years, has found a risk of VTE and PE in NOMAc-E2 which is similar to or even lower than that of LNG-based COCs users [HR adjusted of 0.59 (95% CI 0.25–1.35) (adjusted for age, BMI, family history of VTE and current duration of use)].44
COCs and Oncological Risk
The RR of both ovarian cancer and endometrial cancer is significantly reduced when using COCs; this protective effect increases with the duration of therapy and remains several decades after its interruption. A systematic review shows that the risk of ovarian cancer is reduced by at least 50% with COC use (<40 µg EE)45 and another collaborative reanalysis of 45 epidemiological studies found a 20% reduction in ovarian cancer risk for every 5 years of COC use.46 This effect was more evident if COCs have been used near the peak of incidence of ovarian cancer, precisely the perimenopause.45
For these reasons, COCs could be used as a chemoprophylactic strategy for younger women with a BRCA1 or BRCA2 gene mutation.47 Observational studies have also shown a reduction in functional ovarian cysts and benign ovarian tumours development in COC users,48 which are very common in this life stage.
The risk reduction for endometrial cancer is between 50% and 70%; in particular, the risk reduction in endometrial and serous serotypes is greater than in the mucinous one.49 In women using COCs for at least 12 months, the protection could last for at least 15 years after discontinuation.50
There is little evidence regarding CHC use and breast cancer risk, related specifically to women aged over 40. The increased risk is basically age-related: if the risk of developing breast cancer at 35 years is 1/500, it is 1/100 at 40.51 Studies with older COC formulations (higher-dose) found a slightly increased risk of breast cancer (with RR in the range 1.24–1.30) that declines gradually after cessation, with no significant risk of breast cancer after 10 years of non-use.28 However, nowadays, with the use of low-dose pills, this risk does not seem to exist or to be minimal at most: one meta-analysis of five cohort studies found a very small but significant increase in breast cancer risk for every 5 (RR 1.07, 95% CI 1.03–1.11) and 10 (RR 1.14, 95% CI 1.05–1.23) years of use.51
In the Danish study, the RR of developing breast cancer for recent and current users of any hormonal contraceptive (mostly utilising COCs) is 1.20 (95% CI 1.14–1.26, p = 0.002). This means one extra breast cancer per 7690 women using a CHC for one year.52 Importantly, the study has some limitations regarding other important confounding factors for breast cancer risk: in particular, the BMI is not known for all patients while breastfeeding, family history or other oncological risks were not included in the analysis.
For BRCA1/BRCA2 carriers, who themselves have an increased baseline risk, there does not appear to be an additional risk associated with COC use.53
It is important to take in mind that the specific benefits/risks ratio according to these specific topics (cardiovascular and oncological risk) can additionally change between different ages of reproductive years and between starters and long-term COC users:51 then, counselling should be personalised.11 Some risks differ if COC use begins in middle age or if use is continued from a young age. The thrombotic risk increases with age and is greatest in the first months of use. Additionally, the presence of other cardiovascular risk factors (eg, obesity, smoking, hypertension, and diabetes) highlights the importance of eligibility criteria and may even contraindicate the use of COC. On the other hand, the risk of cervical cancer should increase after continuous use for more than five years in women with human papillomavirus, while data about the cumulative risk of breast cancer data are conflicting.54
Vaginal Ring
The contraceptive ring is a type of CHC that does not involve a daily intake. It can be used cyclically (in for 3 weeks, out for 1 week) or continuously (in for four weeks, replaced immediately with a new ring) which is a way to avoid the oestrogen-withdrawal symptoms experienced by perimenopausal women while maintaining contraceptive efficacy.55,56
In the literature, studies comparing the ring and COCs showed fewer reports of nausea, acne, irritability and depression in ring users, but more complaints of vaginitis and genital itching.24 On the other hand, with regard to uterine bleeding patterns, there are conflicting data: some studies report less abundant cycles and spotting with the ring, while others do not. Concerning the cardiovascular risk, not enough events of TVE, stroke or MI have been found to assess the differential risk in comparison to COCs.57
This system has the important pros of a better vaginal lubrication thanks to local oestrogen which is very important in this life stage in which many women begin to suffer from vulvovaginal atrophy: 98% of women showed good lubrication after just 3 cycles of treatment. This is associated with a favourable impact on vaginal flora (increase in lactobacilli) and a perfect cycle control, superimposable/superior to that of a COC containing EE 30 µg.58
Transdermal Patch
The contraceptive patch is, like the vaginal ring, a type of CHC that does not demand daily attention: it is applied to the skin and worn for 7 days to suppress ovulation, after which the patch is replaced on a weekly basis for two further weeks. The fourth week is patch-free to allow a withdrawal bleeding.
Its use in this age group is infrequent, and there are no definite data on its continued use; as mentioned earlier in perimenopause, this is preferred to avoid the occurrence of symptoms in the window period. However, according to the International Medical Eligibility Criteria for Contraceptive Use, there are no contraindications on the use of transdermal patch in this life stage.19 However, few studies showed that patch users were less likely to experience bleeding and spotting than COC users but were more likely to report breast discomfort, nausea, vomiting and menstrual pain.24
With regard to cardiovascular risk, there seems to be an increased risk of VTE with the contraceptive patch compared to COCs in some studies. If we add to the aforementioned absence of long-term safety data, this contraceptive is definitely not the first line for the perimenopausal woman.59
Progestin-Only Pill (POP)
Progestin-only pills (POPs), are oestrogen-free oral contraceptives containing only synthetic progestins in low doses, even lower than those of combined pills. Most perimenopausal patients with contraindications to oestrogen-containing options, including tobacco use, obesity, migraines with aura, long-standing diabetes, hypertension, or a history of venous thromboembolism (VTE), can safely use POPs. Contraindications to POPs are limited to a personal history of active or recent (within 5 years) breast cancer. Their mechanism of action involves changes in cervical mucus, endometrial development, corpus luteum function and tubal motility and sometimes also prevention of ovulation.60,61 Administration is daily and continuous, without breaks. Most of the commonly used preparations contain LNG (30 µg), norethisterone (350 µg) and desogestrel (75 µg). The type of progestin that has the greatest efficacy on ovulation inhibition is desogestrel, which is comparable to that of CHCs.62 With the decline in fertility with age, the traditional POP becomes increasingly effective in older users.10 A new option for a POP was recently released with a product containing 4 mg of drospirenone (DRSP): it suppresses ovulation and thickens cervical mucus because of its higher doses of progestin. This allows more leeway in the dosing schedule and maintains effectiveness, even with a missed or late pill. DRSP has strong anti-mineralocorticoid and antiandrogenic properties. The anti-mineralocorticoid properties may lower blood pressure and reduce fluid retention, helping to combat bloating and some of the weight changes observed in perimenopause. The antiandrogenic properties have been shown to have a better impact on arterial cardiovascular risk.21
The use of DRSP-only pills showed higher rates of scheduled bleedings and amenorrhea rates and much lower rates of unscheduled intracyclic bleeding/spotting in comparison to continuous desogestrel regimen of POP.20
The use of POPs may be beneficial in this age group because of the lack of association they have with VTE, stroke, or MI.
The risk of breast cancer in users of POPs is controversial: in some studies, the risk appears to be the same as for CHCs, while there is no increased risk in others. Nevertheless, if there is also an increase in risk, it remains minimal and will continue to reduce after the cessation of POPs.61 On the other hand, with regard to its action on bone, there is no evidence in the literature of a negative effect on BMD.35
In contrast, the impact on bleeding patterns is important: they are altered in 50% of women using this type of contraceptive. The bleeding rates associated with DRSP-only pill are better than those for the DSG 75 µg POP, which are reported to be around 20% for scheduled withdrawal bleeding, 60% for unscheduled intracyclic bleeding/spotting and 15% for amenorrhoea.63 Thus, the DRSP-only pill shows higher rates of scheduled bleedings and much lower rates of unscheduled intracyclic bleeding/spotting. The improved predictability of bleeding with the DRSP-only pill is an important advantage of this new hormonal contraceptive.
Depot Medroxyprogesterone Acetate (DMPA)
DMPA is an injectable contraceptive whose effects last for three months, and which contains 104–400 mg of medroxyprogesterone acetate.5 There are not enough eligible data about its use during perimenopause due to its limited use in some countries. DMPA is related to a small loss in bone mineral density that is generally regained after cessation; however, it could reduce bone density that represents a critical factor that occurs physiologically during the climacteric period. Therefore, it is not a first-line contraceptive method after the age of 45 years, although there are no formal contraindications.64 The dose of DMPA is relatively high compared with the progestin doses in other progestin-only and oestrogen-containing contraceptive methods, with several unique implications for its use. Of the benefits, amenorrhea rates are higher than other methods – up to 50% at 1 year of use, with the prevalence of amenorrhea further increasing with ongoing use. The relatively higher dose of progestin prevents clinically significant interactions with medications that induce liver enzymes and can attenuate the contraceptive efficacy of the implant and COCs. However, a return to fertility can be delayed by up to an average of 10 months after the last injection in patients who want to become pregnant after use.
LARCs
LARCs can represent methods based on mechanical inflammatory effects or progestin-only administration, so that they do not provide any risk of cardiovascular disease or stroke and none of the other risks and contraindications related to oestrogen use or simple mechanical methods. These include levonorgestrel-releasing intrauterine systems (LNG-IUS), etonogestrel subdermal implants and copper intrauterine devices (Cu-IUDs).
Cu-IUDs
Cu-IUDs are a non-hormonal contraceptive method that creates an endometrial inflammatory response causing oedema, an increase in vascular permeability and macrophage infiltration that creates an unfavourable environment for the embryo implant. The copper ions released in utero are spermicidal. Thanks to its long action (between 5 and 12 years)65 it can be an ideal contraceptive method during the whole climacteric, especially in women with contraindications to hormone supplementation.49 No evidence that the Cu-IUDs lose its effectiveness after 10 years of use has been found at this life stage.66
Another advantage is that Cu-IUDs can provide emergency contraception if the insertion is within 5 days of unprotected sexual intercourse.67
Contraindications to IUD placement include the following: known or suspected pregnancy, known or suspected pelvic inflammatory disease, known or suspected pelvic malignancy, or anatomic conditions that prevent proper placement. IUDs can easily be placed in an office or clinical setting, without the need for anaesthesia in most instances. The cumulative risk of IUD expulsion is 10% over 3 years of use. Satisfaction and continuation rates associated with the use of IUDs are significantly higher than those associated with the use of SARCs such as COCs.
Additionally, Felix et al demonstrated a protective effect on the risk of endometrial cancer compared with women without these devices.68 However, their use is not recommended in women with heavy menstrual bleeding or dysmenorrhea, because copper intrauterine devices can accentuate these two problems; the bleeding patterns can also occur in women without abnormal endometrial bleeding, but these are not harmful and decrease overtime.7 As we can see, Cu-IUDs do not act on climacteric symptoms and cannot be used in women with a dysmorphic uterus or known pelvic inflammatory disease, or in women with submucous fibroids distorting the uterine cavity.7 Finally, when introducing a Cu-IUD, the woman has to be aware of the risks (very rare) of the procedure, including uterine perforation (2/1000), infections in the first 20 days (<1/300) and dislocation (5%).49
Implant
Various types of subdermal implants are available worldwide with the 68 mg etonogestrel (Nexplanon® or Implanon NXT®) being the most common. It is a subdermal implant which releases etonogestrel only and it has to be inserted and removed by trained operators and in a specific body area, which is 8–10 cm above the medial epicondyle of humerus. It has a contraceptive efficacy higher than tubal sterilisation with a Pearl index = 0.05/100 women-years. Its pharmacokinetics are such that there is a peak of 220 pg/mL of etonogestrel within the first 4 days after its implantation, which is greatly higher than the minimum dose needed to inhibit ovulation (90 pg/mL).69 By stopping the ovarian activity, ESI can act on endometriosis and other conditions affected by hormonal changes.70 The only real discomfort caused by ESI is the unpredictability of the bleeding pattern71: for this reason, 15% of women require its removal, as demonstrated by a US study;72 other reviews count prolonged/frequent bleeding in approximately one in five women.73 There are no associations with the loss of bone density or metabolic effect74, and it is recommended in obese women as well.75 To underline these data, women with BMI >30 kg/m2 generally do not require its removal72 and have an optimal hormonal distribution, unlike other contraceptive methods in which metabolism is highly influenced by weight. ESIs have to be replaced 3 years after implantation and, unlike IUDs, there are no recommendations to retain them for longer during the perimenopausal period.74 There is no specific action on the endometrium, so it appears that implants do not protect against endometrial hyperplasia and breast cancer is a contraindication to its use.49 Based on the aspects discussed here, the perfect phenotype for ESI in climacteric includes women with BMI > 30 kg/m2 and metabolic diseases or with a contraindication to oestrogen use.
LNG-IUS (Levonorgestrel-Releasing Intrauterine System)
This is an intrauterine device that releases levonorgestrel only; it is available in three different dosages (13.5 mg, 19.5 mg and 52 mg), all of them approved for contraceptive use throughout reproductive life. However, only the one which contains 52 mg of LNG has proven its effectiveness as an endometrial protection if estrogen replacement therapy is provided.76 LNG-IUS insertion has few contraindications and lots of benefits during climacteric and, if inserted after 45 years, it can be retained for up to seven years in women with menstrual disorders or until menopause if amenorrhoeic (off-label).49 Within those 7 years, LNG-IUS 52 mg safely prevents pregnancy (contraceptive failure rates are 0.1% per year in typical use): as a matter of fact, it causes endometrial suppression and increases cervical mucus.6 The IUS has one of the lowest failure rates of all contraceptive options (0.1% typical and perfect use failure rate).
LNG-IUS has been demonstrated to be the most effective method against abnormal uterine bleeding (AUB) thanks to its ability to decrease endometrial growth and prostaglandin ratio by promoting the formation of arachidonic acid in the endometrium.6 LNG-IUS is a safe and effective option in women in perimenopause suffering from heavy bleeding caused by benign lesions in the uterus or dysmenorrhea.77 In another study, the efficacy of LNG-IUS was compared with medroxyprogesterone acetate and continuous oral progestin assumption, with the evidence of the supremacy of the first method in reducing heavy menstrual bleeding in perimenopausal women.78 Therefore, LNG-IUS 52 mg has to be considered the first-line method in reducing excessive bleeding in women in their forties, considering that amenorrhoea is expected in up to 45% of women within 6 months of insertion and in up to 50% of women within one year.79 Perimenopausal patients with HMB experience reductions in menstrual bleeding similar to endometrial ablation, often precluding the need for surgery.80
As stated before, the risk of endometrial cancer increases during perimenopause and the rate of endometrial hyperplasia consequently rises. LNG-IUS has showed a concrete efficacy in reducing typical endometrial hyperplasia, so it is recommended in recent guidelines to be the first-line method in this treatment. A study conducted by Abu Hashim et al81 showed endometrial atrophy after 24 months of LNG-IUS insertion in 100% of women with a documented typical endometrial hyperplasia.6
The treatment with LNG-IUS 52 mg has also been used in the case of hyperplasia with atypia (endometrial intraepithelial neoplasia), and it has been associated with its significant regression (moderate-quality evidence) compared with no treatment.82
Moreover, few studies of its use also in the case of early-stage endometrial cancer stage I A1 in women who want to preserve fertility have been published, with or without an associated systemic progestin therapy, but its feasibility/effectiveness has to be clearly demonstrated.
LNG-IUS combined with progesterone ameliorates endometrial thickness and pregnancy outcomes of patients with early-stage endometrial cancer or atypical hyperplasia.83,84
Another indication to LNG-IUS 52 mg use is the presence of symptomatic fibroids, unless they are submucosal, because they could cause difficulties in the insertion of LNG-IUS due to endometrial inhomogeneity.6 Generally, myomas tends to reduce in menopause, but there are cases in which they provoke abnormal bleeding difficult to control; in addition, fibroids induce aromatase expression, determining the production of inflammatory markers in the endometrium.85 In those cases, the use of LNG-IUSs should be taken into account. In a study regarding the use of LNG-IUS in perimenopausal women with uterine fibroids, hysterectomy was avoided in 89.5% of women after 24 months of LNG-IUS 52 mg insertion.86 Finally, some oncologists consider the use of LNG-IUS in women using tamoxifen to prevent endometrial hyperplasia.87
Some authors have explored the association between an increase in body weight compared with other contraceptive methods. It turns out that the increase in body mass index (BMI) with LNG-IUS was higher than in the control group but lower than with the desogestrel-only pill.88 There is a concern that LNG-IUS can increase the risk of breast cancer: there are contrasting data regarding these topics, as some articles have proven the association between LNG-IUS and breast cancer, while others report the opposite.51 Thus, further research is needed to establish whether there is a real connection with breast cancer risk. Currently, UK Medical Eligibility Criteria for Contraceptive Use state that the risk of LNG-IUS use in women with active breast cancer is in category 4 (unacceptable risk), whereas the risk is in category 3 (risk outweigh benefits) for those women who have experienced breast cancer in the past 5 years with no active disease.49 There is no contraindication for patients considered to be at high-risk of breast cancer (eg, family history of breast cancer or BRCA1/2 mutation carriers).
Moreover, LNG-IUS 52 mg has been well studied in combination with oestrogens and is approved for use as HT outside of the United States.89,90,91 Although the IUS has contraceptive efficacy for longer than 5 years, it may not provide adequate endometrial protection from hyperplasia after this time, particularly the IUS with the lower doses IUS.76 Therefore, women using a lower dose of IUS should be counselled with regard to changing the device earlier to ensure adequate endometrial protection while using HT.
Ultimately, it seems that LNG-IUS can be associated with important mood changes in a smaller group of vulnerable women92 (made worse by the climacteric period itself), so that they require antidepressants and have a higher risk of hospitalisation for depression.93
Irreversible Contraception - Sterilisation
Permanent sterilisation, either via vasectomy of the patient’s partner or tubal ligation/salpingectomy (to further prevent ovarian cancer) is another possible option in this life stage. These are highly effective methods with 0.5% failure rates or lower. Patients should be counselled that these are not reversible and are considered permanent solutions. Since there are currently even more effective and long-acting reversible methods of contraception, the use of this contraceptive method should increasingly decrease and be selected only in particular situations because it still requires surgery with the associated recovery costs and risks and it is still associated with a possible negative long-term impact on the ovarian reserve.94
When to Stop Contraception?
Menopause is confirmed with 12 months of amenorrhea in women ages 40 and older according to The North American Menopause Society (NAMS), while guidelines from The Faculty of Sexual and Reproductive Healthcare (FSRH) recommend two years of amenorrhea for women between 40 and 50 years old and one year of amenorrhea for those aged 50 years old or above.7 Continue contraception therapy until menopause is recommended. NAMS further states that 90% of women will reach menopause by age 55 and recommends continuing contraception until mid-50s.95
If a nonhormonal contraceptive method (eg, Cu-IUD) is being used, the above amenorrhea criteria are applicable.
In the case of hormonal contraceptive use, assessing menopausal status is more challenging as amenorrhea may be artificial. Although hormonal testing is not definitive, Expert Opinion suggests that combining FSH levels with age can assist with assessing menopausal status in women using hormonal contraceptives between the ages of 50 and 55 years old.96 Most women (95.9%) are menopausal by the age of 55 years and virtually all are menopausal by the age of 59 years.
For women using POP, implant or LNG-IUS, clinicians can check FSH levels once; if it is more than 30 IU/l, the method can be continued for one more year and then stopped (Figure 1). If the level is less than 30 IU/l, the method should be continued for another year before rechecking FSH again.97,98 These methods can also be stopped at the age of 55 years without any hormonal evaluation (Figure 3A).96
 |
Figure 3 When to stop contraception? In the case of progestin-only pill, implant and levonorgestrel-realising intrauterine system use (A), depot medroxyprogesterone acetate use (B) and combined hormonal contraceptive (pill, vaginal ring and patch) use (C). |
For women using DMPA, FSH levels are not always impacted. In perimenopausal women, if FSH is suppressed, the levels generally return to the normal baseline prior to the next injection. For women aged 50–55 years, FSH can be checked on the day of injection and repeated 13 weeks later prior to the next injection. If both levels are more than 30 IU/l, contraception can be discontinued (Figure 3B).65,99
CHCs users have a more challenging scenario as FSH is more suppressed by the method. For FSRH, they should be switched to an alternative method at 50 years old (progestin-only, Cu-IUD, etc.) and then follow its specific recommendation. Another option for women aged 50 years and older is to stop their CHCs and use a non-hormonal method for a while. If they do not resume their menses after 6 weeks, they can check their FSH levels twice, 1–2 months apart; if the levels are more than 30 IU/l both times, the contraception can be stopped.100 A second option is to check FSH levels at the end of the 7-day placebo week twice, 6–8 weeks apart. If the FSH level is more than 30 IU/l both times, contraception can be discontinued (Figure 3C).
False-negative results can occur after 7 days and may require a full 14-day hormone-free interval or longer to repeat the testing if the woman is able to use a reliable back-up method. For women on CHC, NAMS state that they may continue CHC until 55 years old if no contraindications exist (Figure 1).95
Once a woman discontinues CHC, she may experience the onset of menopausal symptoms, including vasomotor symptoms, sleep disturbances, vaginal and urinary tract symptoms and changes in sexual function. At this time, postmenopausal HT may be considered on an individual basis.
Acknowledgment
No particular acknowledgments for this invited review.
Disclosure
Giovanni Grandi received honoraria for sponsored lectures and participation in advisory boards from Bayer AG, Italfarmaco, Theramex, Organon, Gedeon Richter and Exeltis, not related to this manuscript. Fabio Facchinetti reports personal fees from JnJ outside the submitted work. The authors report no other potential conflicts of interest in relation to this work.
References
1. Harlow SD, Gass M, Hall JE, et al. Executive summary of the stages of reproductive aging workshop 10: addressing the unfinished agenda of staging reproductive aging. Climacteric. 2012;15(2):105–114. doi:10.3109/13697137.2011.650656
2. John D. Obstetrics and Gynecology for Postgraduates.
3. Soules MR, Sherman S, Parrott E, et al. Stages of Reproductive Aging Workshop (STRAW). J Womens Health Gend Based Med. 2001;10(9):843–848. doi:10.1089/152460901753285732
4. Bacon JL. The menopausal transition. Obstet Gynecol Clin North Am. 2017;44(2):285–296. doi:10.1016/j.ogc.2017.02.008
5. Shaaban MM. The perimenopause and contraception. Maturitas. 1996;23(2):181–192. doi:10.1016/0378-5122(96)83915-6
6. Joo JK, Shin JH, Lee JR, Kim MR. Levonorgestrel-releasing intrauterine system use in perimenopausal women. J Menopausal Med. 2021;27(2):49–57. doi:10.6118/jmm.20038
7. FSRH Clinical Guideline: Contraception for Women Aged over 40 Years (August 2017, amended September 2019). Faculty of sexual and reproductive healthcare; 2018. Available from: https://www.fsrh.org/standards-and-guidance/documents/fsrh-guidance-contraception-for-women-aged-over-40-years-2017/.
8. Chandra A, Copen CE, Stephen EH. Infertility and impaired fecundity in the United States, 1982–2010: data from the National Survey Of Family Growth. Natl Health Stat Rep. 2013;67:1–18.
9. Finer LB, Zolna MR. Unintended pregnancy in the United States: incidence and disparities, 2006. Contraception. 2011;84(5):478–485. doi:10.1016/j.contraception.2011.07.013
10. Navot D, Bergh PA, Williams MA, et al. Poor oocyte quality rather than implantation failure as a cause of age-related decline in female fertility. Lancet Lond Engl. 1991;337(8754):1375–1377. doi:10.1016/0140-6736(91)93060-M
11. Antinori S, Gholami GH, Versaci C, et al. Obstetric and prenatal outcome in menopausal women: a 12-year clinical study. Reprod Biomed Online. 2003;6(2):257–261. doi:10.1016/S1472-6483(10)61718-X
12. Grandi G, Del Savio MC, Boggio Sola V, Monari F, Melotti C, Facchinetti F. Attitudes of women towards products containing hormones (hormonal contraceptives or hormone therapy): what changes from pre to postmenopause? Ann Med. 2021;53(1):908–915. doi:10.1080/07853890.2021.1938662
13. Bitzer J, Platano G, Tschudin S, Alder J. Sexual counseling in elderly couples. J Sex Med. 2008;5(9):2027–2043. doi:10.1111/j.1743-6109.2008.00926.x
14. Speroff L, Darney PD. A Clinical Guide for Contraception. Lippincott Williams & Wilkins; 2011:464.
15. Munro MG, Critchley HOD, Fraser IS, FIGO Menstrual Disorders Committee; The two FIGO systems for normal and abnormal uterine bleeding symptoms and classification of causes of abnormal uterine bleeding in the reproductive years: 2018 revisions. Int J Gynaecol Obstet off Organ Int Fed Gynaecol Obstet. 2018;143(3):393–408. doi:10.1002/ijgo.12666
16. Davies J, Kadir RA. Heavy menstrual bleeding: an update on management. Thromb Res. 2017;151(Suppl 1):S70–7. doi:10.1016/S0049-3848(17)30072-5
17. Di Bella ZIK, de J Bianchi AMH, de M Araujo FF, De, Sartori MGF, Girão MJBC. Contraception and family planning at the extreme of reproductive life - climacteric. Rev Assoc Medica Bras. 2016;62(5):454–457. doi:10.1590/1806-9282.62.05.454
18. Sanderson PA, Critchley HOD, Williams ARW, Arends MJ, Saunders PTK. New concepts for an old problem: the diagnosis of endometrial hyperplasia. Hum Reprod Update. 2017;23(2):232–254. doi:10.1093/humupd/dmw042
19. Harris ML, Egan N, Forder PM, Coombe J, Loxton D. Contraceptive use among women through their later reproductive years: findings from an Australian prospective cohort study. PLoS One. 2021;16(8):e0255913. doi:10.1371/journal.pone.0255913
20. World Health Organization. Medical eligibility criteria for contraceptive use; 2022. Available from: https://www.who.int/publications-detail-redirect/9789241549158.
21. Chiara Del Savio M, De FR, Facchinetti F, Grandi G. Drospirenone 4 mg-only pill (DOP) in 24+4 regimen: a new option for oral contraception. Expert Rev Clin Pharmacol. 2020;13(7):685–694. doi:10.1080/17512433.2020.1783247
22. Rice C, Killick S, Hickling D, Coelingh Bennink H. Ovarian activity and vaginal bleeding patterns with a desogestrel-only preparation at three different doses. Hum Reprod Oxf Engl. 1996;11(4):737–740. doi:10.1093/oxfordjournals.humrep.a019245
23. Bitzer J. Overview of perimenopausal contraception. Climacteric J Int Menopause Soc. 2019;22(1):44–50. doi:10.1080/13697137.2018.1540566
24. Lopez LM, Grimes DA, Gallo MF, Stockton LL, Schulz KF. Skin patch and vaginal ring versus combined oral contraceptives for contraception. Cochrane Database Syst Rev. 2013;30(4):CD003552.
25. Marret H, Fauconnier A, Chabbert-Buffet N, et al. Clinical practice guidelines on menorrhagia: management of abnormal uterine bleeding before menopause. Eur J Obstet Gynecol Reprod Biol. 2010;152(2):133–137. doi:10.1016/j.ejogrb.2010.07.016
26. MacGregor EA. Menstrual and perimenopausal migraine: a narrative review. Maturitas. 2020;142:24–30. doi:10.1016/j.maturitas.2020.07.005
27. Gambacciani M, Monteleone P, Ciaponi M, Sacco A, Genazzani AR. Effects of oral contraceptives on bone mineral density. Treat Endocrinol. 2004;3(3):191–196. doi:10.2165/00024677-200403030-00006
28. Cibula D, Gompel A, Mueck AO, et al. Hormonal contraception and risk of cancer. Hum Reprod Update. 2010;16(6):631–650. doi:10.1093/humupd/dmq022
29. Long ME, Faubion SS, MacLaughlin KL, Pruthi S, Casey PM. Contraception and hormonal management in the perimenopause. J Womens Health. 2015;24(1):3–10. doi:10.1089/jwh.2013.4544
30. Gallo MF, Nanda K, Grimes DA, Schulz KF. 20 mcg versus >20 mcg estrogen combined oral contraceptives for contraception. Cochrane Database Syst Rev. 2005;18(2):CD003989.
31. Fraser IS, Parked S, Mellinger U, Machlitt A, Serrani M, Jensen J. Effective treatment of heavy and/or prolonged menstrual bleeding without organic cause: pooled analysis of two multinational, randomised, double-blind, placebo-controlled trials of oestradiol valerate and dienogest. Eur J Contracept Reprod Health Care. 2011;16(4):258–269. doi:10.3109/13625187.2011.591456
32. Blümel JE, Castelo-Branco C, Binfa L, Aparicio R, Mamani L. A scheme of combined oral contraceptives for women more than 40 years old. Menopause N Y N. 2001;8(4):286–289. doi:10.1097/00042192-200107000-00011
33. Grandi G, Imbrogno MG, Cainazzo MM, et al. Easy tools to screen Italian women suffering from migraine with and without aura in early reproductive age. Eur J Obstet Gynecol Reprod Biol. 2019;242:63–67. doi:10.1016/j.ejogrb.2019.09.012
34. Sacco S, Merki-Feld GS, Ægidius KL, et al. Effect of exogenous estrogens and progestogens on the course of migraine during reproductive age: a consensus statement by the European Headache Federation (EHF) and the European Society of Contraception and Reproductive Health (ESCRH). J Headache Pain. 2018;19(1):76. doi:10.1186/s10194-018-0896-5
35. Nappi C, Bifulco G, Tommaselli GA, Gargano V, Di Carlo C. Hormonal contraception and bone metabolism: a systematic review. Contraception. 2012;86(6):606–621. doi:10.1016/j.contraception.2012.04.009
36. Allen RH, Cwiak CA, Kaunitz AM. Contraception in women over 40 years of age. CMAJ Can Med Assoc J. 2013;185(7):565–573. doi:10.1503/cmaj.121280
37. Ø L, Nielsen LH, Skovlund CW, Skjeldestad FE, Løkkegaard E. Risk of venous thromboembolism from use of oral contraceptives containing different progestogens and oestrogen doses: Danish cohort study, 2001–2009. BMJ. 2011;25(343):d6423.
38. Weill A, Dalichampt M, Raguideau F, et al. Low dose oestrogen combined oral contraception and risk of pulmonary embolism, stroke, and myocardial infarction in five million French women: cohort study. BMJ. 2016;10(353):i2002. doi:10.1136/bmj.i2002
39. Sugiura K, Kobayashi T, Ojima T. Risks of thromboembolism associated with hormonal contraceptives related to body mass index and aging in Japanese women. Thromb Res. 2016;137:11–16. doi:10.1016/j.thromres.2015.11.038
40. Roach REJ, Helmerhorst FM, Lijfering WM, Stijnen T, Algra A, Dekkers OM. Combined oral contraceptives: the risk of myocardial infarction and ischemic stroke. Cochrane Database Syst Rev. 2015;27(8):CD011054.
41. Grandi G, Napolitano A, Cagnacci A. Metabolic impact of combined hormonal contraceptives containing estradiol. Expert Opin Drug Metab Toxicol. 2016;12(7):779–787. doi:10.1080/17425255.2016.1190832
42. Grandi G, Barra F, Ferrero S, Facchinetti F. Estradiol in non-oral hormonal contraception: a ‘long and winding road’. Expert Rev Endocrinol Metab. 2019;14(3):153–155. doi:10.1080/17446651.2019.1604217
43. Dinger J, Möhner S, Heinemann K. Combined oral contraceptives containing dienogest and estradiol valerate may carry a lower risk of venous and arterial thromboembolism compared to conventional preparations: results from the extended INAS-SCORE study. Front Womens Health. 2020;5(1). doi:10.15761/FWH.1000178
44. Reed S, Koro C, DiBello J, et al. Prospective controlled cohort study on the safety of a monophasic oral contraceptive containing nomegestrol acetate (2.5mg) and 17β-oestradiol (1.5mg) (PRO-E2 study): risk of venous and arterial thromboembolism. Eur J Contracept Reprod Health Care. 2021;26(6):439–446. doi:10.1080/13625187.2021.1987410
45. Havrilesky LJ, Moorman PG, Lowery WJ, et al. Oral contraceptive pills as primary prevention for ovarian cancer: a systematic review and meta-analysis. Obstet Gynecol. 2013;122(1):139–147. doi:10.1097/AOG.0b013e318291c235
46. Collaborative Group on Epidemiological Studies of Ovarian Cancer. Ovarian cancer and oral contraceptives: collaborative reanalysis of data from 45 epidemiological studies including 23 257 women with ovarian cancer and 87 303 controls. Lancet. 2008;371(9609):303–314. doi:10.1016/S0140-6736(08)60167-1
47. Grandi G, Sammarini M, Del Savio MC, Toss A, Facchinetti F. Combined hormonal contraceptives in BRCA gene mutation carriers: why not? Eur J Contracept Reprod Health Care off J Eur Soc Contracept. 2019;24(6):417–419. doi:10.1080/13625187.2019.1647335
48. Westhoff C, Britton JA, Gammon MD, Wright T, Kelsey JL. Oral contraceptive and benign ovarian tumors. Am J Epidemiol. 2000;152(3):242–246. doi:10.1093/aje/152.3.242
49. UK Medical Eligibility Criteria for Contraceptive Use (UKMEC). Faculty of sexual and reproductive healthcare; 2022. Available from: https://www.fsrh.org/standards-and-guidance/uk-medical-eligibility-criteria-for-contraceptive-use-ukmec/.
50. Weiderpass E, Adami HO, Baron JA, Magnusson C, Lindgren A, Persson I. Use of oral contraceptives and endometrial cancer risk (Sweden). Cancer Causes Control CCC. 1999;10(4):277–284. doi:10.1023/A:1008945721786
51. Zhu H, Lei X, Feng J, Wang Y. Oral contraceptive use and risk of breast cancer: a meta-analysis of prospective cohort studies. Eur J Contracept Reprod Health Care off J Eur Soc Contracept. 2012;17(6):402–414. doi:10.3109/13625187.2012.715357
52. Mørch LS, Skovlund CW, Hannaford PC, Iversen L, Fielding S, Lidegaard Ø. Contemporary hormonal contraception and the risk of breast cancer. N Engl J Med. 2017;377(23):2228–2239. doi:10.1056/NEJMoa1700732
53. Moorman PG, Havrilesky LJ, Gierisch JM, et al. Oral contraceptives and risk of ovarian cancer and breast cancer among high-risk women: a systematic review and meta-analysis. J Clin Oncol off J Am Soc Clin Oncol. 2013;31(33):4188–4198. doi:10.1200/JCO.2013.48.9021
54. Mendoza N, Soto E, Sánchez-Borrego R. Do women aged over 40 need different counseling on combined hormonal contraception? Maturitas. 2016;87:79–83. doi:10.1016/j.maturitas.2016.02.008
55. Timmer CJ, Mulders TM. Pharmacokinetics of etonogestrel and ethinylestradiol released from a combined contraceptive vaginal ring. Clin Pharmacokinet. 2000;39(3):233–242. doi:10.2165/00003088-200039030-00005
56. Algorta J, Diaz M, de Benito R, et al. Pharmacokinetic bioequivalence, safety and acceptability of Ornibel®, a new polymer composition contraceptive vaginal ring (etonogestrel/ethinylestradiol 11.00/3.474 mg) compared with Nuvaring® (etonogestrel/ethinylestradiol 11.7/2.7 mg). Eur J Contracept Reprod Health Care off J Eur Soc Contracept. 2017;22(6):429–438. doi:10.1080/13625187.2017.1413179
57. Dinger J, Möhner S, Heinemann K. Cardiovascular risk associated with the use of an etonogestrel-containing vaginal ring. Obstet Gynecol. 2013;122(4):800–808. doi:10.1097/AOG.0b013e3182a5ec6b
58. Fruzzetti F, Perini D, Fornaciari L, Russo M, Bucci F, Gadducci A. Discontinuation of modern hormonal contraceptives: an Italian survey. Eur J Contracept Reprod Health Care off J Eur Soc Contracept. 2016;21(6):449–454. doi:10.1080/13625187.2016.1234598
59. Cole JA, Norman H, Doherty M, Walker AM. Venous thromboembolism, myocardial infarction, and stroke among transdermal contraceptive system users. Obstet Gynecol. 2007;109(2 Pt 1):339–346. doi:10.1097/01.AOG.0000250968.82370.04
60. Tepper NK, Whiteman MK, Marchbanks PA, James AH, Curtis KM. Progestin-only contraception and thromboembolism: a systematic review. Contraception. 2016;94(6):678–700. doi:10.1016/j.contraception.2016.04.014
61. Samson M, Porter N, Orekoya O, et al. Progestin and breast cancer risk: a systematic review. Breast Cancer Res Treat. 2016;155(1):3–12. doi:10.1007/s10549-015-3663-1
62. Endrikat J, Gerlinger C, Richard S, Rosenbaum P, Düsterberg B. Ovulation inhibition doses of progestins: a systematic review of the available literature and of marketed preparations worldwide. Contraception. 2011;84(6):549–557. doi:10.1016/j.contraception.2011.04.009
63. Collaborative Study Group on the Desogestrel-containing Progestogen-only Pill. A double-blind study comparing the contraceptive efficacy, acceptability and safety of two progestogen-only pills containing desogestrel 75 micrograms/day or levonorgestrel 30 micrograms/day. Eur J Contracept Reprod Health Care off J Eur Soc Contracept. 1998;3(4):169–178. doi:10.3109/13625189809167250
64. Petitti DB, Piaggio G, Mehta S, Cravioto MC, Meirik O, The WHO Study of Hormonal Contraception and Bone Health; Steroid hormone contraception and bone mineral density: a cross-sectional study in an international population. Obstet Gynecol. 2000;95(5):736–744. doi:10.1016/s0029-7844(00)00782-1
65. Miller TA, Allen RH, Kaunitz AM, Cwiak CA. Contraception for midlife women: a review. Menopause N Y N. 2018;25(7):817–827. doi:10.1097/GME.0000000000001073
66. Bahamondes L, Faundes A, Sobreira-Lima B, Lui-Filho JF, Pecci P, Matera S. TCu 380A IUD: a reversible permanent contraceptive method in women over 35 years of age. Contraception. 2005;72(5):337–341. doi:10.1016/j.contraception.2004.12.026
67. Cleland K, Zhu H, Goldstuck N, Cheng L, Trussell J. The efficacy of intrauterine devices for emergency contraception: a systematic review of 35 years of experience. Hum Reprod Oxf Engl. 2012;27(7):1994–2000. doi:10.1093/humrep/des140
68. Felix AS, Gaudet MM, La Vecchia C, et al. Intrauterine devices and endometrial cancer risk: a pooled analysis of the epidemiology of endometrial cancer consortium. Int J Cancer J Int Cancer. 2015;136(5):E410–E422. doi:10.1002/ijc.29229
69. Grandi G, Cagnacci A, Volpe A. Pharmacokinetic evaluation of desogestrel as a female contraceptive. Expert Opin Drug Metab Toxicol. 2014;10(1):1–10. doi:10.1517/17425255.2013.844229
70. Walch K, Unfried G, Huber J, et al. Implanon versus medroxyprogesterone acetate: effects on pain scores in patients with symptomatic endometriosis–a pilot study. Contraception. 2009;79(1):29–34. doi:10.1016/j.contraception.2008.07.017
71. Mansour D, Korver T, Marintcheva-Petrova M, Fraser IS. The effects of Implanon on menstrual bleeding patterns. Eur J Contracept Reprod Health Care off J Eur Soc Contracept. 2008;13(Suppl 1):13–28. doi:10.1080/13625180801959931
72. Casey PM, Long ME, Marnach ML, Bury JE. Bleeding related to etonogestrel subdermal implant in a US population. Contraception. 2011;83(5):426–430. doi:10.1016/j.contraception.2010.09.012
73. Bateson D, McNamee K. Perimenopausal contraception: a practice-based approach. Aust Fam Physician. 2017;46(6):372–377.
74. Lopez LM, Grimes DA, Schulz KF, Curtis KM, Chen M. Steroidal contraceptives: effect on bone fractures in women. Cochrane Database Syst Rev. 2014;24(6):CD006033.
75. Xu H, Wade JA, Peipert JF, Zhao Q, Madden T, Secura GM. Contraceptive failure rates of etonogestrel subdermal implants in overweight and obese women. Obstet Gynecol. 2012;120(1):21–26. doi:10.1097/AOG.0b013e318259565a
76. Grandi G, Farulla A, Sileo FG, Facchinetti F. Levonorgestrel-releasing intra-uterine systems as female contraceptives. Expert Opin Pharmacother. 2018;19(7):677–686. doi:10.1080/14656566.2018.1462337
77. Yoo HJ, Lee MA, Ko YB, Yang JB, Kang BH, Lee KH. The efficacy of the levonorgestrel-releasing intrauterine system in perimenopausal women with menorrhagia or dysmenorrhea. Arch Gynecol Obstet. 2012;285(1):161–166. doi:10.1007/s00404-011-1937-3
78. Küçük T, Ertan K. Continuous oral or intramuscular medroxyprogesterone acetate versus the levonorgestrel releasing intrauterine system in the treatment of perimenopausal menorrhagia: a randomized, prospective, controlled clinical trial in female smokers. Clin Exp Obstet Gynecol. 2008;35(1):57–60.
79. Sangi-Haghpeykar H, Poindexter AN, Bateman L, Ditmore JR. Experiences of injectable contraceptive users in an urban setting. Obstet Gynecol. 1996;88(2):227–233. doi:10.1016/0029-7844(96)00194-9
80. Kaunitz AM, Meredith S, Inki P, Kubba A, Sanchez-Ramos L. Levonorgestrel-releasing intrauterine system and endometrial ablation in heavy menstrual bleeding: a systematic review and meta-analysis. Obstet Gynecol. 2009;113(5):1104–1116. doi:10.1097/AOG.0b013e3181a1d3ce
81. Abu Hashim H, Zayed A, Ghayaty E, El Rakhawy M. LNG-IUS treatment of non-atypical endometrial hyperplasia in perimenopausal women: a randomized controlled trial. J Gynecol Oncol. 2013;24(2):128–134. doi:10.3802/jgo.2013.24.2.128
82. Mittermeier T, Farrant C, Wise MR. Levonorgestrel-releasing intrauterine system for endometrial hyperplasia. Cochrane Database Syst Rev. 2020;9(9):CD012658. doi:10.1002/14651858.CD012658.pub2
83. Fang F, Xu H, Wu L, et al. LNG-IUS combined with progesterone ameliorates endometrial thickness and pregnancy outcomes of patients with early-stage endometrial cancer or atypical hyperplasia. Am J Transl Res. 2021;13(5):5412–5419.
84. Leone Roberti Maggiore U, Martinelli F, Dondi G, et al. Efficacy and fertility outcomes of levonorgestrel-releasing intra-uterine system treatment for patients with atypical complex hyperplasia or endometrial cancer: a retrospective study. J Gynecol Oncol. 2019;30(4):e57. doi:10.3802/jgo.2019.30.e57
85. Maia H, Pimentel K, Casoy J, et al. Aromatase expression in the eutopic endometrium of myomatous uteri: the influence of the menstrual cycle and oral contraceptive use. Gynecol Endocrinol off J Int Soc Gynecol Endocrinol. 2007;23(6):320–324. doi:10.1080/09513590701321565
86. Machado RB, de Souza IM, Beltrame A, Bernardes CR, Morimoto MS, Santana N. The levonorgestrel-releasing intrauterine system: its effect on the number of hysterectomies performed in perimenopausal women with uterine fibroids. Gynecol Endocrinol off J Int Soc Gynecol Endocrinol. 2013;29(5):492–495. doi:10.3109/09513590.2013.769517
87. Dominick S, Hickey M, Chin J, Su HI. Levonorgestrel intrauterine system for endometrial protection in women with breast cancer on adjuvant tamoxifen. Cochrane Database Syst Rev. 2015;2015(12):CD007245.
88. Napolitano A, Zanin R, Palma F, et al. Body composition and resting metabolic rate of perimenopausal women using continuous progestogen contraception. Eur J Contracept Reprod Health Care off J Eur Soc Contracept. 2016;21(2):168–175. doi:10.3109/13625187.2015.1079610
89. Varila E, Wahlström T, Rauramo I. A 5-year follow-up study on the use of a levonorgestrel intrauterine system in women receiving hormone replacement therapy. Fertil Steril. 2001;76(5):969–973. doi:10.1016/S0015-0282(01)02846-1
90. Suvanto-Luukkonen E, Kauppila A. The levonorgestrel intrauterine system in menopausal hormone replacement therapy: five-year experience. Fertil Steril. 1999;72(1):161–163. doi:10.1016/S0015-0282(99)00162-4
91. Depypere H, Inki P. The levonorgestrel-releasing intrauterine system for endometrial protection during estrogen replacement therapy: a clinical review. Climacteric J Int Menopause Soc. 2015;18(4):470–482. doi:10.3109/13697137.2014.991302
92. Bitzer J. Hormonal contraception and depression: another Pill scandal? Eur J Contracept Reprod Health Care off J Eur Soc Contracept. 2017;22(1):1–2. doi:10.1080/13625187.2016.1269163
93. Skovlund CW, Mørch LS, Kessing LV, Lidegaard Ø. Association of hormonal contraception with depression. JAMA Psychiatry. 2016;73(11):1154–1162. doi:10.1001/jamapsychiatry.2016.2387
94. Qin F, Du DF, Li XL. The effect of salpingectomy on ovarian reserve and ovarian function. Obstet Gynecol Surv. 2016;71(6):369–376. doi:10.1097/OGX.0000000000000323
95. North American Menopause Society. Menopause Practice: a Clinician’s Guide; 2022. Available from: https://www.menopause.org/publications/professional-publications/em-menopause-practice-em-textbook.
96. Baldwin MK, Jensen JT. Contraception during the perimenopause. Maturitas. 2013;76(3):235–242. doi:10.1016/j.maturitas.2013.07.009
97. Inal MM, Yildirim Y, Ertopcu K, Avci ME, Ozelmas I, Tinar S. Effect of the subdermal contraceptive etonogestrel implant (Implanon) on biochemical and hormonal parameters (three years follow-up). Eur J Contracept Reprod Health Care off J Eur Soc Contracept. 2008;13(3):238–242. doi:10.1080/13625180802075315
98. Halmesmäki K, Hurskainen R, Tiitinen A, et al. A randomized controlled trial of hysterectomy or levonorgestrel-releasing intrauterine system in the treatment of menorrhagia-effect on FSH levels and menopausal symptoms. Hum Reprod Oxf Engl. 2004;19(2):378–382. doi:10.1093/humrep/deh055
99. Juliato CT, Fernandes A, Marchi NM, Castro S, Olivotti B, Bahamondes L. Usefulness of FSH measurements for determining menopause in long-term users of depot medroxyprogesterone acetate over 40 years of age. Contraception. 2007;76(4):282–286. doi:10.1016/j.contraception.2007.06.005
100. Faculty of Family Planning and Reproductive Health Care Clinical Effectiveness Unit. FFPRHC guidance (January 2005) contraception for women aged over 40 years. J Fam Plann Reprod Health Care. 2005;31(1):51–63. doi:10.1783/0000000052973086
101. Regione Emilia-Romagna. Salute.Assessorato politiche per la salute; Relazione sull’interruzione volontaria digravidanza in Emilia-Romagna nel 2020 [Health Policy Department; Report on the voluntary termination of pregnancy in Emilia-Romagna in 2020]; 2021. Available from: https://salute.regione.emilia-romagna.it/siseps/applicazioni/ig/documentazione. Accessed February 1, 2022. Italian
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.