Back to Journals » Biologics: Targets and Therapy » Volume 16
Continuous Use of Etanercept During Pregnancy Does Not Affect TNF-Alpha Levels in Umbilical Cord Blood
Authors Nishide M ![]() , Yagita M, Kumanogoh A
, Yagita M, Kumanogoh A
Received 21 January 2022
Accepted for publication 2 March 2022
Published 31 March 2022 Volume 2022:16 Pages 17—19
DOI https://doi.org/10.2147/BTT.S358449
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Doris Benbrook
Masayuki Nishide,* Mayu Yagita,* Atsushi Kumanogoh
Department of Respiratory Medicine and Clinical Immunology, Graduate School of Medicine, Osaka University, Osaka, Japan
*These authors contributed equally to this work
Correspondence: Masayuki Nishide, Department of Respiratory Medicine and Clinical Immunology, Graduate School of Medicine, Osaka University, 2-2 Yamada-oka, Suita, Osaka, 565-0871, Japan, Tel +81-6-6879-3831, Fax +81-6-6879-3839, Email [email protected]
Abstract: TNF-alpha-targeted therapies during pregnancy is a topic of interest in rheumatology. Etanercept (ETN) is expected to have lower transplacental transfer, however, clinical evidence is lacking on the usefulness and safeness of continuing etanercept throughout pregnancy. We here described the first reported case of relapsing polychondritis where continuous use of ETN throughout pregnancy was required. The patient was a pregnant Japanese woman who presented with bilateral ear cartilage redness, swelling, saddle nose and severe subglottic oedema. Due to severe systemic and life-threatened disease, we decided to continue using ETN throughout pregnancy and resulted in successful vaginal delivery. The treatment with ETN was successful and TNF-alpha levels in umbilical cord blood were not affected. The infant did not have any signs of chondritis although levels of anti-type 2 collagen antibodies in maternal and umbilical cord blood were similar, suggesting that anti-type 2 collagen antibodies crossed the placenta. This case is an important clinical experience that strengthens the safety to continue ETN during the entire pregnancy if necessary.
Keywords: etanercept, relapsing polychondritis, pregnancy, TNF-alpha, anti-type 2 collagen antibody
Introduction
Treating autoimmune diseases during pregnancy with TNF-alpha inhibitors (TNFi) is a big topic of interest in rheumatology.1 There have been some important studies recently discussing when to stop TNFi therapy before childbirth.2 ETN is a dimeric fusion protein consisting of the ligand-binding domain of TNF-alpha receptor p75 with the Fc region of human IgG1. ETN is expected to have lower transplacental transfer3 and is approved to use during the gestation period.4 However, there are no published studies about the kinetics of TNF-alpha or autoantibody levels in maternal and cord blood when ETN was used continuously during pregnancy. In this report, we describe the first case of a pregnant woman with relapsing polychondritis where continuous ETN use was required due to severe systemic disease.
Case Presentation
The patient was a 39-year-old Japanese woman who presented at 27 weeks of gestation. She had been aware of nasal pain and wheezing for 3 months. She noticed swelling of her left ear at 3 weeks before hospitalization. On the day of admission, she was emergently transported to our hospital. She presented with bilateral ear cartilage redness, swelling, and a saddle nose (Figure 1A). Arterial oxygen saturation decreased to below 90%. Flexible fiberoptic laryngoscopy revealed severe subglottic oedema. Chest CT showed stenosis of the main bronchi (Figure 1B). Biopsy of auricular cartilage revealed inflammatory cells infiltrating the cartilage. Based on these clinical and histological findings, she was diagnosed with relapsing polychondritis.5 Foetal growth was consistent with expected growth for gestational age. After intubation, pulse methylprednisolone therapy (1 g/day for 3 days) was performed, followed by oral prednisolone therapy at 60 mg/day and subcutaneous injection of ETN (25 mg twice weekly). She was weaned off the ventilator on hospital day 17. During the prednisolone taper, azathioprine (50 mg/day) was started on hospital day 33. Ear cartilage redness and the saddle nose remained but did not worsen. During gestational week 36, a female infant was delivered vaginally. The infant was of appropriate size and development for gestational age (Apgar score, 9) and did not have any signs of chondritis. ETN was last given 2 days before delivery. Before ETN treatment, the maternal blood serum TNF-alpha concentration was 26.7 ng/mL. At delivery, it was 8.35 ng/mL. Umbilical cord blood TNF-alpha concentration was 60.2 ng/mL (Table 1). Levels of anti-type 2 collagen antibodies in maternal and umbilical cord blood were 25.3 EU/mL and 27.8 EU/mL, respectively (Table 1).
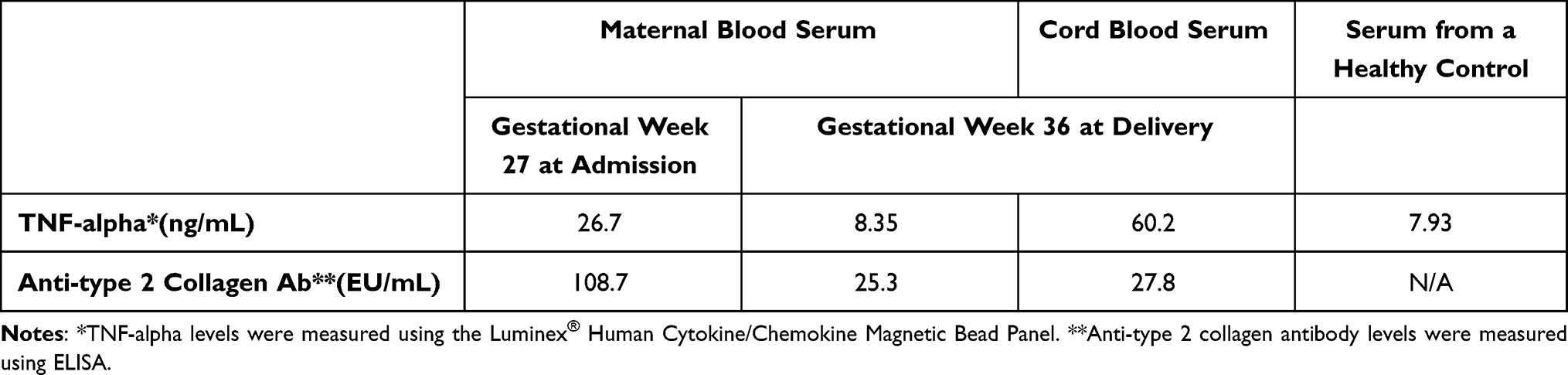 |
Table 1 Kinetics of TNF-Alpha and Anti-Type 2 Collagen Antibody Levels in Maternal Serum, Umbilical Cord Blood Serum, and Serum from a Healthy Control |
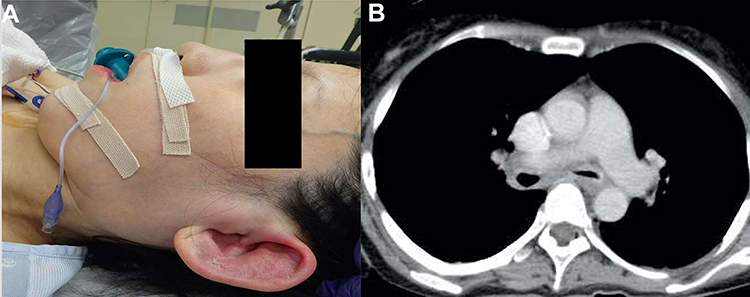 |
Figure 1 Clinical findings on the day of admission. (A) The patient presented with ear cartilage redness, swelling, and a saddle nose. (B) Chest CT on the day of admission. |
Discussion
Relapsing polychondritis is a systemic autoimmune disease that causes repeated inflammation of cartilage. Although swelling of the ear cartilage and saddle nose are the main symptoms, laryngotracheal bronchial disease occurs in approximately 26% of primary cases and 48% of all patients during the disease.6 In general, oral steroids and immunosuppressants such as methotrexate or azathioprine are used for treatment. However, in severe cases with airway complications, administration of biologics has been recently recommended.7 Pregnant women sometimes suffer from relapsing polychondritis. In a retrospective observational study of 25 pregnant women with relapsing polychondritis, pregnancy did not modify the course of the disease and no symptoms with chondritis were observed in neonates.8 However, this study did not include critically severe patients and no patients had airway complications. Therefore, there is little evidence available on how to care for pregnant women with life-threatening relapsing polychondritis. This is the first reported case of severe relapsing polychondritis treated with TNFi during pregnancy and resulted in successful vaginal delivery. Consistent with the previous study,8 chondritis was not observed in neonates.
Other unique aspects of this case are the duration of ETN usage and the kinetics of TNF-alpha and autoantibody levels. At delivery, the maternal blood serum TNF-alpha concentration was comparable to levels in healthy subjects, while umbilical cord blood TNF-alpha concentration was elevated. These data suggest that ETN was effective and TNF-alpha levels in maternal blood decreased accordingly but did not affect TNF-alpha levels in umbilical cord blood even though the drug was used throughout the pregnancy. Regarding the kinetics of anti-type 2 collagen antibodies, which are positive in approximately 33% of patients with relapsing polychondritis and correlate with disease activity,9 antibody titres were initially high but decreased after treatment. At delivery, levels of anti-type 2 collagen antibodies in maternal and umbilical cord blood were similar, suggesting that anti-type 2 collagen antibodies crossed the placenta.
EULAR published points to consider (PtC) that recommended discontinuation of ETN at gestational weeks 30–3210 and it can be used if indicated throughout pregnancy. However, more evidence is needed on the usefulness and safeness of continuing etanercept throughout pregnancy. In this case, the mother’s life was threatened; therefore, we decided to continue using ETN with the patient’s consent after a full explanation of the risks and benefits. This report helps to reinforce the theory that ETN is safe to give during pregnancy. Also, this is the first report about the kinetics of TNF-alpha and autoantibody levels in a pregnant woman who continuously received a TNFi during pregnancy. This case is an important clinical experience that strengthens the safety to continue ETN during the entire pregnancy if necessary.
Consent Statements
Patient samples were obtained after informed consent was provided by the subjects, in accordance with the Declaration of Helsinki and with approval from the ethical review board of the Graduate School of Medicine, Osaka University, Japan (no. 18370-3 and no. 11122-5). Consent of patient was obtained according to CARE guideline, using Patient Consent Form (provided by the Taylor & Francis group). Consent to publish the report is also obtained.
Funding
This study was funded by the Japan Society for the Promotion of Science (JSPS) KAKENHI (JP18H05282 to A.K.).
Disclosure
The authors have declared no conflicts of interest in this work.
References
1. Smeele HT, Roder E, Wintjes HM, Kranenburg-van Koppen LJ, Hazes JM, Dolhain RJ. Modern treatment approach results in low disease activity in 90% of pregnant rheumatoid arthritis patients: the PreCARA study.. Ann Rheum Dis. 2021;80(7):859–864. doi:10.1136/annrheumdis-2020-219547
2. Ghalandari N, Kemper E, Crijns IH, et al. Analysing cord blood levels of TNF inhibitors to validate the EULAR points to consider for TNF inhibitor use during pregnancy. Ann Rheum Dis. 2022;81(3):402–405.
3. Arora T, Padaki R, Liu L, et al. Differences in binding and effector functions between classes of TNF antagonists. Cytokine. 2009;45(2):124–131.
4. Murashima A, Watanabe N, Ozawa N, Saito H, Yamaguchi K. Etanercept during pregnancy and lactation in a patient with rheumatoid arthritis: drug levels in maternal serum, cord blood, breast milk and the infant’s serum. Ann Rheum Dis. 2009;68(11):1793–1794.
5. McAdam LP, O’Hanlan MA, Bluestone R, Pearson CM. Relapsing polychondritis: prospective study of 23 patients and a review of the literature. Medicine. 1976;55(3):193–215.
6. Michet CJ, McKenna CH, Luthra HS, O’Fallon WM. Relapsing polychondritis. Survival and predictive role of early disease manifestations. Ann Intern Med. 1986;104(1):74–78.
7. Kingdon J, Roscamp J, Sangle S, D’Cruz D. Relapsing polychondritis: a clinical review for rheumatologists. Rheumatology. 2018;57(9):1525–1532.
8. Papo T, Wechsler B, Bletry O, Piette AM, Godeau P, Piette JC. Pregnancy in relapsing polychondritis: twenty-five pregnancies in eleven patients. Arthritis Rheum. 1997;40(7):1245–1249.
9. Foidart JM, Abe S, Martin GR, et al. Antibodies to type II collagen in relapsing polychondritis. N Engl J Med. 1978;299(22):1203–1207.
10. Gotestam Skorpen C, Hoeltzenbein M, Tincani A, et al. The EULAR points to consider for use of antirheumatic drugs before pregnancy, and during pregnancy and lactation. Ann Rheum Dis. 2016;75(5):795–810.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.