Back to Journals » Advances in Medical Education and Practice » Volume 16
Continuous Flipped Classroom in Anesthesiology: Enhancing Learning Outcomes and Anesthesiology Major Selection in Eight-Year Program Students
Authors Hu ZL ![]() , Hu YZ, Gao ZJ, Luo YW, Ou P, Luo C, Cui YH, Luo RY
, Hu YZ, Gao ZJ, Luo YW, Ou P, Luo C, Cui YH, Luo RY ![]()
Received 23 September 2025
Accepted for publication 13 December 2025
Published 20 December 2025 Volume 2025:16 Pages 2349—2358
DOI https://doi.org/10.2147/AMEP.S569669
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Balakrishnan Nair
Zhao-Lan Hu,1,2 Yue-Zi Hu,3 Zi-Jing Gao,1,2 Yan-Wei Luo,4 Peng Ou,1,2 Cong Luo,1,2 Yan-Hui Cui,5 Ru-Yi Luo1,2
1Department of Anesthesiology, The Second Xiangya Hospital, Central South University, Changsha, Hunan, 410011, People’s Republic of China; 2Anesthesia Medical Research Center, Central South University, Changsha, Hunan, 410011, People’s Republic of China; 3Clinical Laboratory, The Second Hospital of Hunan University of Chinese Medicine, Changsha, People’s Republic of China; 4Department of Blood Transfusion, The Third Xiangya Hospital of Central South University, Changsha, People’s Republic of China; 5Department of Anatomy and Neurobiology, Xiangya School of Basic Medical Science, Central South University, Changsha, Hunan, 410013, People’s Republic of China
Correspondence: Yan-Hui Cui, Email [email protected] Ru-Yi Luo, Email [email protected]
Background: The flipped classroom (FC) is increasingly used in medical education, but the impact of a continuous FC strategy on anesthesiology learning and career choice in eight-year medical program students remains unclear.
Methods: In a randomized trial, 200 students received either continuous FC (n=100) or traditional (n=100) anesthesiology instruction. Outcomes included final exam scores, survey-assessed satisfaction, active learning, critical thinking, and post-course specialty selection. Mediation analysis evaluated how a weighted composite of these scores influenced anesthesiology major selection.
Results: The continuous FC group demonstrated significantly higher final exam scores, satisfaction, and active learning levels (all P < 0.05). Most importantly, students in the FC group were 21.77 times more likely to choose anesthesiology as their specialty than those in the control group (OR = 21.77, 95% CI: 1.79– 264.83, P = 0.016). Mediation analysis indicated that 44.13% of the total effect of the FC intervention on specialty choice was mediated by improvements in the weighted composite score (indirect effect: β = 0.059, 95% CI: 0.024– 0.102, P = 0.005).
Conclusion: The continuous FC approach enhances learning outcomes, fosters essential skills, and significantly increases the selection of anesthesiology as a specialty. This demonstrates its substantial positive impact and potential value in addressing specialty shortages in medical education.
Keywords: flipped classroom, anesthesiology, major choice, teaching quality, eight-year program students
Introduction
In China, medical students participate in either a five-year or eight-year clinical program, with anesthesiology instruction occurring in the fall semester of the fourth and fifth years, respectively, a pivotal time for career specialization.1,2 An eight-year program designed to train highly skilled healthcare professionals has been introduced at 18 leading medical colleges in China since 2001.3 Eight-year medical program students typically complete pre-clinical coursework and core medical training during the first five years, self-select specialized clinical disciplines starting in the sixth year, and undertake research training culminating in a doctoral dissertation during the final three years. This pivotal decision determines their subsequent residency training focus and primary career track. However, a study found that only 2.3% of eight-year program students chose an anesthesiology specialty.4
China’s critical deficiency of anesthesiologists (6.7 per 100,000 population) highlights systemic obstacles in specialized medical recruitment, particularly within the eight-year training program.4 To address this gap, this study advocates for reforming the anesthesiology curriculum in the fifth year of the eight-year program to enhance educational quality and student involvement before specialization selection at the beginning of the sixth year.
The flipped classroom (FC) model reverses traditional teaching by assigning pre-class materials for self-study and dedicating classroom time to interactive problem-solving and addressing knowledge gaps.5 This approach fosters proactive learning, enhances engagement, and improves educational outcomes, particularly in medical fields like anesthesiology, where it has gained traction among residents and pediatric anesthesiology graduate students.6,7 Studies have highlighted benefits such as increased teaching efficiency, improved work-life balance, and stronger motivation for a clinical career.5,8 Unlike problem-based learning (PBL) or team-based learning (TBL), the FC model shifts knowledge acquisition to the pre-class phase.9,10 This is critical for a dense subject like anesthesiology, as it reserves classroom time for expert-guided, higher-order activities like case simulations and hands-on problem-solving.
However, current research primarily focuses on evaluating its short-term implementation within courses.11 This limited emphasis constitutes a significant constraint, as prolonged application is crucial for the development of effective instructional tactics.12 Anesthesiology is often perceived as a “behind-the-scenes” specialty, affording students limited early clinical exposure. Consequently, traditional didactic teaching often fails to convey the field’s intellectual dynamism, decision-making complexity, and clinical satisfaction—a visibility gap that creates a pronounced barrier to entry compared to more patient-facing disciplines. We therefore selected anesthesiology as a critical test case to examine whether pedagogical reform can influence career decisions in a high-need field plagued by practitioner shortages and low appeal among top students. We introduced a semester-long FC model, hypothesizing that its emphasis on active problem-solving and clinical scenario simulation would provide a continuous, immersive experience. This, in turn, was expected to improve knowledge retention, foster a deeper understanding of anesthesiology’s clinical reasoning, and ultimately transform students’ perceptions of the specialty by engaging them directly with an anesthesiologist’s cognitive processes.
This study evaluated a continuous FC teaching paradigm in anesthesiology education by comparing students’ specialty choices, academic performance, and educational assessment scores between experimental and control groups. We hypothesized that: (1) The pedagogical intervention would significantly increase rates of selecting anesthesiology as a specialty, and (2) choosing anesthesiology would correlate with higher academic achievement and more positive survey responses regarding perceptions of the specialty.
Participants and Methods
Basic Information of Research Participants and Ethics Approval
The study comprised 200 undergraduate students enrolled in the eight-year program at the Xiangya School of Medicine, Central South University. Inclusion criteria: (1) The students are in their fifth year of the program (2) The subjects were informed and agreed. Exclusion criteria: (1) The subject refuses to participate in the study. (2) The subject withdraws from the study midway. We enrolled a total of 202 participants, excluding two students who refused to participate. Using a random number table, 200 participants (age range: 22 ~ 24 years) were randomized to either the research group (n = 100; female = 48, male = 52) or the control group (n = 100; female = 46, male = 54). Participants were assigned to either traditional classroom (control group) or continuous FC (research group) instruction for the Anesthesiology course throughout the entire fall semester. Both groups were instructed by teachers with over 5 years of professional experience. To address equity concerns, we provided all FC materials to the control group after completion of the study.
This study complied with the Declaration of Helsinki (1989) and obtained approval from the Ethics Committee of our institution.The Second Xiangya Hospital, with the research trial registration number LYF20240281. Following a comprehensive verbal elucidation of the experimental protocols, each participant furnished written consent for the investigation. Trained researchers distributed the surveys, guaranteeing voluntary and anonymous participation while alerting participants of the study’s goal.
Study Design and Setting
The research group implemented a continuous FC learning approach, which systematically combined pre-class preparation with interactive in-class sessions. To this end, the cohort of 100 students was subdivided into four fixed sub-groups of 25 students each. Within each sub-group, one student was randomly designated as the team leader, tasked with coordinating pre-class learning activities, facilitating intra-team discussions and compiling a summary report of their team’s discussion for formal submission to the instructor prior to the in-class session. The learning cycle commenced one week before each session, with the distribution of curated digital materials (including instructional video and PowerPoint (PPT) presentations) via a WeChat group. During the in-class session, after the instructor’s lecture, time was dedicated to discussing the reports submitted by each team. The instructor provided overall feedback and clarified questions based on the reports, with the aim of reinforcing key concepts and resolving challenging topics. This process also incorporated active learning strategies, including structured group discussions centered on the pre-class materials, as well as interactive Q&A sessions to deepen students’ understanding of the video-based content.
The control group adopted traditional PPT-based concentrated teaching, in which teachers explained relevant knowledge points based on actual cases and addressed any student concerns.
The reformed anesthesiology curriculum includes fundamental theories and techniques (such as organ function monitoring/support, anesthesia risk assessment, and airway management), perioperative complication management, pain management, drug dependence, and anesthesiology therapeutics, incorporating clinical cases to improve practical skills. The flow diagram for developing and analyzing the data model was illustrated in Figure 1.
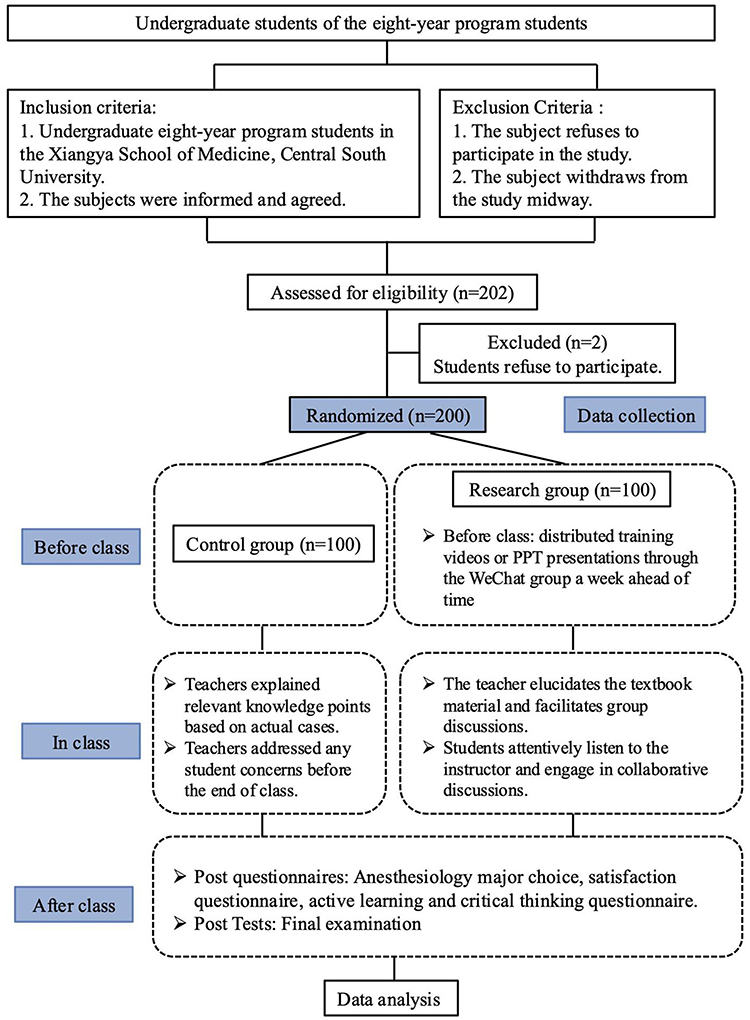 |
Figure 1 The study design flowchart. |
Data Collection and Measurement
We collected demographic characteristics (sex and age), as well as the following information:
Final Test
Following the theoretical lectures, the teaching team organizes the students for the final examination. The final test grade was scored on a scale of 0 ~ 100 points.
Students’ Major Choice, Satisfaction, Active Learning and Critical Thinking
An anonymous survey was conducted to gather data on the intended graduate majors of students at the end of their fifth year of academic study. The number of eight-year program students who selected anesthesiology as their specialty was recorded for both groups. Besides, the students’ satisfaction comprised five items, active learning comprised six items, and critical thinking comprised eight items, as shown in Table 1.9,13,14 Students were assessed using a five-point Likert scale questionnaire, with responses ranging from 1 (strongly disagree) to 5 (strongly agree). The composite scores for students’ satisfaction, active learning, and critical thinking were 0 ~ 25 points, 0 ~ 30 points, and 0 ~ 40 points, respectively. The Likert scale used in this study was adapted from previously validated standardized instruments.9 Minor semantic adjustments were made to tailor the item to the context of anesthesiology education while maintaining the original structure of the scale. In the present study, the instrument demonstrated excellent internal consistency, with a Cronbach’s α coefficient of 0.91.
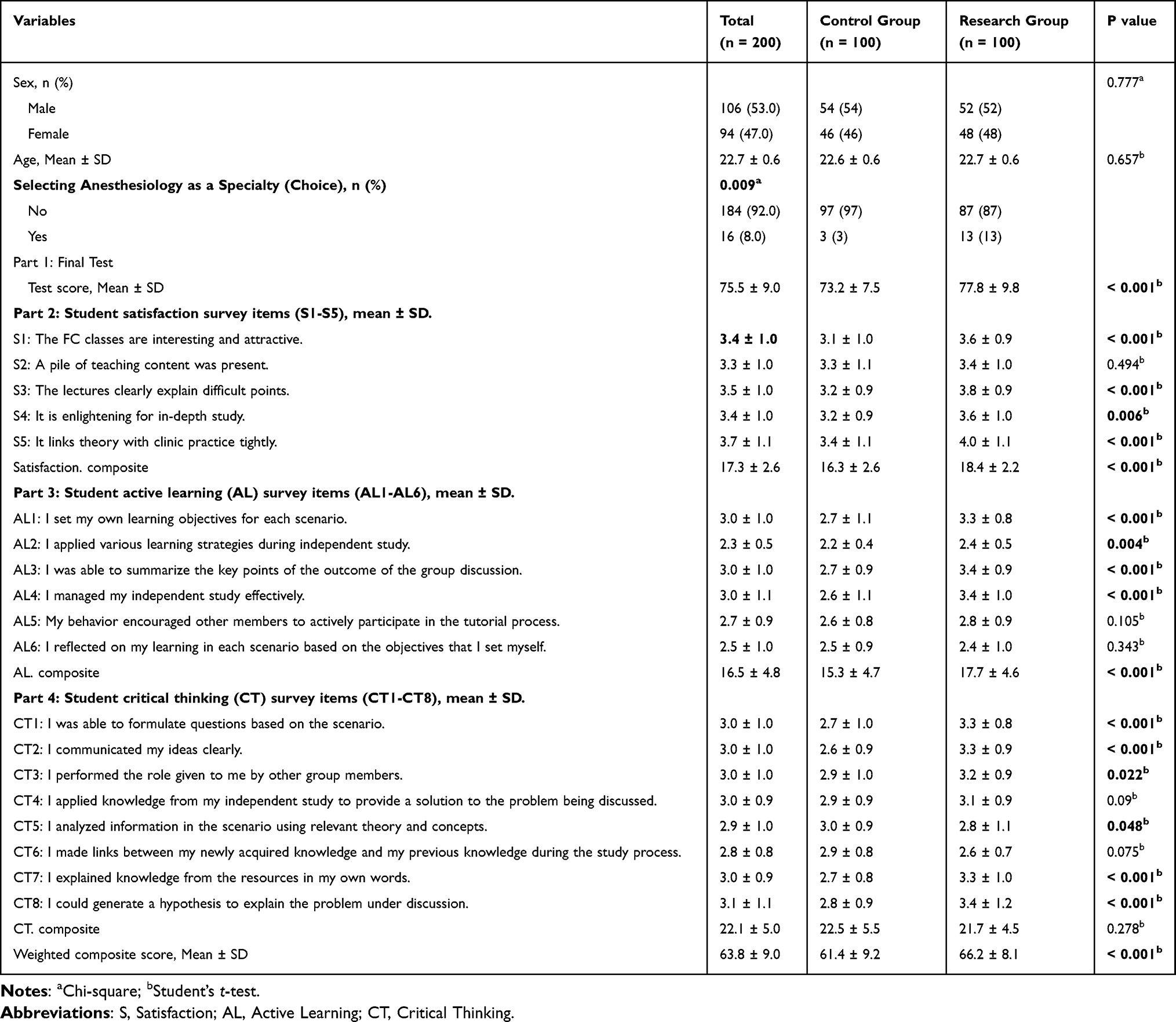 |
Table 1 Descriptive Statistics of Basic Information and Survey |
Weighted Composite Score
The weighted composite score was computed by standardizing each component to a 100-point scale, then applying 25% weights:
Composite = 0.25 * [Final test + (Satisfaction / 25 * 100) + (Active Learning / 30 * 100) + (Critical Thinking / 40 * 100)].
Definition of Exposure, Covariates and Outcome
The research group implemented the continuous FC learning approach whereas the control group implemented the traditional teaching method. Covariates included sex, age, final test score, satisfaction score (five items), active learning score (six items), critical thinking score (eight items) and weighted composite score. The outcome of the present study was selecting anesthesiology as a Specialty (choice).
Statistical Analysis
Continuous variables with normal distribution (confirmed by Shapiro–Wilk test) are presented with mean ± standard deviation (SD), and categorical variables are reported with numbers (percentages) (Table 1). Differences were assessed using the Student’s t-test for continuous data, and the Chi-square test for categorical data. We conducted univariable and multivariable logistic regression analyses to calculate odds ratios (OR) and corresponding 95% confidence intervals (CI), with selection of anesthesiology specialty as the dependent variable (Tables 2 and 3). Univariable logistic regression was used to examine the association between each independent variable and specialty selection. Multivariable logistic regression enabled simultaneous adjustment for demographic and educational assessment covariates, allowing evaluation of the independent effect of continuous FC exposure on specialty choice.
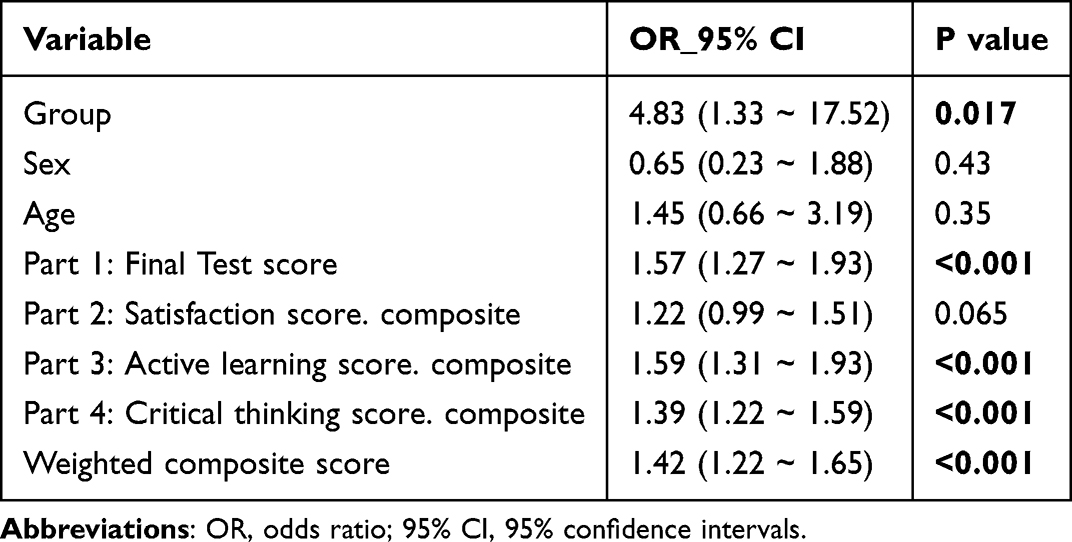 |
Table 2 Univariate Logistic Regression Analyses to Investigate the Factors Associated with the Choice of Anesthesiology as a Major |
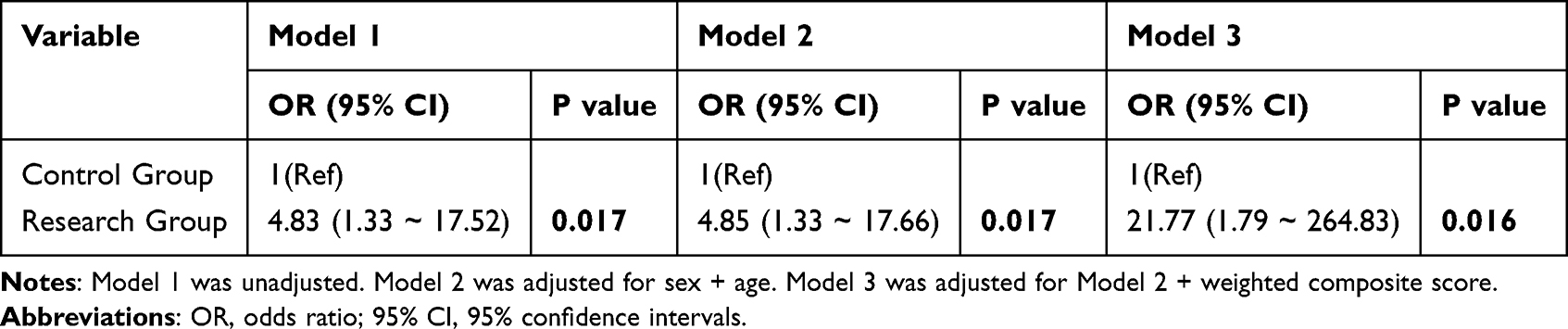 |
Table 3 Multivariable Logistic Regression to Assess the Continuous FC Factor Associated with the Choice of Anesthesiology as a Major |
To mitigated potential confounding effects, we conducted four hierarchically adjusted multivariable regression models: an unadjusted crude model (Model 1), a model adjusted for baseline demographics (sex and age; Model 2), and a model additionally incorporating the weighted composite score (Model 3). To address potential bias from small size and sparse events, we performed sensitivity analyses using Firth’s penalized likelihood logistic regression, which reduces finite-sample bias by introducing a Jeffreys prior penalty term.15 Results were compared with conventional maximum likelihood estimates (Table 4).
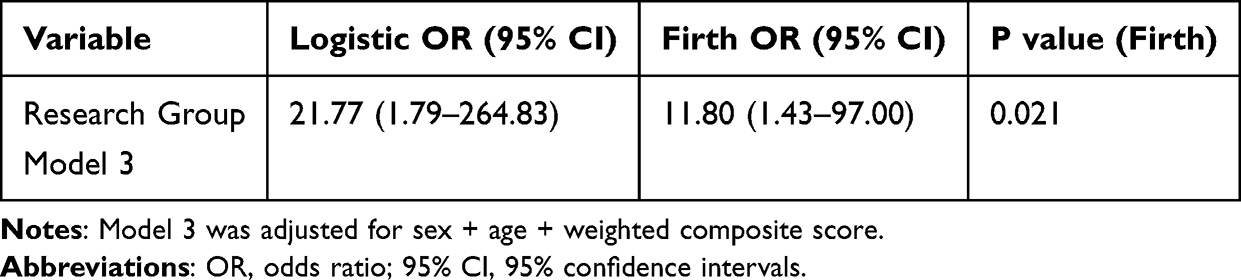 |
Table 4 Sensitivity Analysis Using Firth’s Penalized Likelihood Regression to Address Finite-Sample Bias |
Furthermore, mediation analysis was employed to explore the contribution of the weighted composite score to the influence of the FC on the choice of anesthesiology as a specialty. This approach aligns with the conceptual framework proposed by Baron & Kenny16 and modern causal mediation methods.17 We included all participants (intervention and control groups) to ensure comprehensive estimation of mediator-outcome relationships across the full observational spectrum. Using 5,000 bootstrap iterations, we quantified both the existence and magnitude of this indirect pathway, reporting 95% bias-corrected confidence intervals to provide robust effect estimates. This approach allowed us to rigorously evaluate the temporal sequence of the proposed mediation process while accounting for sampling variability.
All the statistical analyses were performed using R Statistical software (Version 4.2.2, The R Foundation) and the Free Statistics analysis platform (Version 1.9.2). We employed a two-tailed test, and a result was considered statistically significant when the P value was less than 0.05.
Results
Comparison of Basic Information and Survey Results
There was no disparity in sex and age between the two groups of students (Table 1). Thirteen students from the eight-year program in the research group chose anesthesiology as their primary research focus in postgraduate study (P = 0.009), whereas just three students were in the control group (Table 1). The final test composite score (P < 0.001) in the research group was significantly higher than that of the control group (Table 1).
Student satisfaction with the ongoing FC classes was higher in the research group compared to the control group (Table 1). The FC lessons were engaging and appealing (P < 0.001). The lectures elucidated difficult points (P < 0.001), were enlightening for in-depth content (P = 0.006), and closely integrated theory with clinical practice (P < 0.001).
In comparison to their control group peers, students in the research group demonstrated a significantly greater level of enthusiasm for active learning (Table 1). This passion was especially evident in their ability to set learning objectives (P < 0.001), apply learning strategies during independent study (P = 0.004), summarize key points from group discussions (P < 0.001), and manage their independent study (P < 0.001).
Moreover, students in the research group perceived superior critical thinking skills compared to those in the control group (Table 1). They showed excellent proficiency in formulating questions based on the scenarios (P < 0.001), expressing ideas clearly (P < 0.001), coordinating with others (P = 0.022), enhancing problem-solving (P = 0.048), acquiring knowledge from resources (P < 0.001), and developing hypotheses to explain problems (P < 0.001).
Associations Between Continuous FC and the Choice of Anesthesiology as a Major Among Eight-Year Program Students
We conducted univariate logistic regression analyses to investigate the factors associated with the choice of anesthesiology as a major (Table 2). Univariate logistic regression analyses revealed that factors such as sex, age, and satisfaction were not significantly associated with the choice of anesthesiology as a major for eight-year program students. On the other hand, the group (continuous FC vs traditional method), final test score, composite score from active learning, composite score from critical thinking, and overall weighted score showed a positive relationship with the choice of anesthesiology as a major.
Then, multivariable logistic regression models were constructed to examine the relationship between continuous FC teaching exposure (primary predictor) and anesthesiology specialty selection (outcome variable), with adjustment for demographic characteristics, academic performance and educational assessment scores (Table 3). The crude model (Model 1) revealed a significant positive association between FC teaching and anesthesiology specialty selection (OR = 4.83, 95% CI: 2.1 ~ 11.2, P < 0.001). Through progressively adjusted models, the association remained significant with incremental covariate adjustment: Model 2 (adjusted for demographic factors as sex and age) yielded an OR of 4.85 (95% CI: 1.33 ~ 17.66, P = 0.017); Model 3 (fully adjusted for all covariates) demonstrated a substantially increased OR of 21.77 (95% CI: 1.79 ~ 264.83, P = 0.016).
Given the wide confidence intervals observed in Model 3 of our multivariable logistic regression analysis (OR = 21.77, 95% CI: 1.79 ~ 264.83), suggesting potential small-sample bias due to low event rates. To address this limitation, we employed Firth’s penalized likelihood logistics regression as a sensitivity analysis which provides finite and less biased estimates when traditional maximum likelihood estimation fails,15 particularly valuable when complete or quasi-complete separation occurs. As shown in Table 4, while both methods demonstrated statistically significant intervention effects (conventional logistic regression: P = 0.016; Firth’s correction: P = 0.021), Firth’s correction yielded a more precise and clinically plausible estimate (OR = 11.80, 95% CI: 1.43 ~ 97.00) representing a 45.8% reduction in effect size magnitude compared to the conventional approach. This finding underscores the importance of using bias-reduced estimation methods when analyzing studies with limited event rates.
These findings exhibit a consistent and statistically significant association between the continuous FC model and the choice of anesthesiology as a major in the eight-year program for students.
Mediation Analyses
We further conducted mediation analysis to examine the hypothesized pathway whereby the continuous FC intervention enhances the likelihood of choosing anesthesiology as a specialty through improving the weighted composite score (academic performance, satisfaction, active learning, and critical thinking), thereby strengthening students’ interest and confidence in this specialty (Figure 2). Mediation analysis revealed significant impacts of continuous FC intervention on anesthesiology specialty selection: direct effect: β = 0.074 (95% CI: 0.024 ~ 0.139, P = 0.012); indirect effect via composite score: β = 0.059 (95% CI: 0.024 ~ 0.102, P = 0.005); total effect: β = 0.133 (95% CI: 0.060 ~ 0.224, P = 0.001). The indirect pathway mediated 44.13% of the total effect, indicating substantial mediation through academic performance and educational assessment scores (satisfaction, active learning and critical thinking). This finding indicates that improvements in the composite academic and educational assessment metrics partially mediate the relationship between the continuous FC intervention and specialty choice.
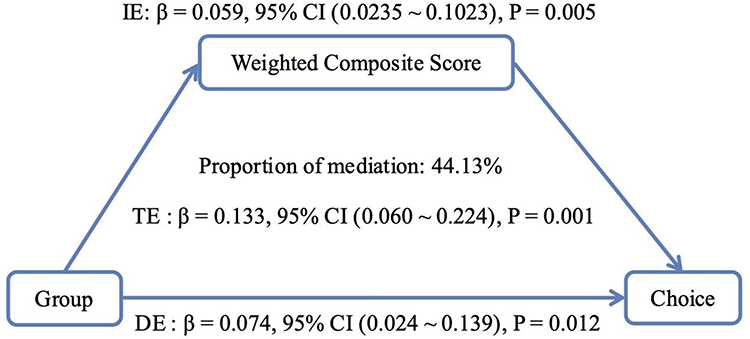 |
Figure 2 Mediation analysis of weighted composite score factor influencing anesthesiology specialty selection among eight-year program students. Abbreviations: IE, Indirect effect; DE, Direct effect; TE, Total effect; 95% CI, 95% confidence intervals. |
Discussion
Our research indicates that the continuous FC model significantly enhances student satisfaction, and students reported higher levels of self-perceived active learning engagement and critical-thinking-related behaviors. These perceived improvements were accompanied by better academic performance and a higher likelihood of selecting anesthesiology as a postgraduate specially. On the other hand, these findings highlight a significant deficiency in current medical education, as conventional teaching methods have not motivated students in the eight-year program, of whom only 2.3% have traditionally selected anesthesiology, despite China’s acute shortage of anesthesiologists.
FC Enhances Satisfaction Through Interactive, Clinically Integrated Learning
The higher satisfaction scores reported by the research group support previous evidence indicating that FC enhances engagement through personalized and interactive learning.18,19 Unlike traditional lectures, our continuous FC model combines pre-class materials with in-class simulations, case discussions, and real-world clinical applications. This approach not only clarified complex concepts but also bridged theory and practice, resonating with students’ expectations for dynamic, relevant education.20 The magnificent improvement in satisfaction underscores FC’s advantage to transform perceptions of anesthesiology from a challenging specialty to an appealing career choice.
FC Cultivates Active Learning and Critical Thinking
Learning enthusiasm can be evaluated via active learning and critical thinking ability.21,22 Instructional strategies that actively involve students in their education are known as active learning. Critical thinking is a comprehensive and extensive process in identifying and tackling problems. Active learning and critical thinking are fundamental competencies throughout all professional disciplines, and they are considered one of the primary skills in the twenty-first century.23
Active learning and critical thinking are pivotal for medical professionals, yet traditional curricula often neglect their development.24 The FC group demonstrated significantly higher scores in both domains. Students in this group reported a greater self-perceived ability to set learning goals, solve problems, and collaborate effectively—skills directly linked to clinical competence. The mediation analysis revealed that active learning is the indirect mediation factor influencing the choice of anesthesiology, indicating that the continuous FC approach, which emphasizes independent study and collaboration with teammates, fosters a greater commitment to the field.
Weighted Composite Score as a Gateway to Specialty Choice
Participants in the FC group selected anesthesiology as their specialty at a rate 21.77 times higher than that of the control group (OR = 21.77; 95% CI: 1.79 ~ 264.83), as confirmed by multivariable logistic regression, indicating a significant independent effect of the FC intervention. However, the exceptionally wide confidence interval suggests considerable imprecision in the point estimate, likely attributable to the limited sample size and low number of observed events. To address this methodological concern and obtain a more reliable effect estimate, we performed a sensitivity analysis using Firth’s penalized-likelihood logistic regression. This bias-reducing approach yielded a more precise and conservative estimate (OR = 11.80; 95% CI: 1.43 ~ 97.00), while still confirming a statistically significant and independent association between FC exposure and specialty choice.
The mediation analysis revealed that 44.13% of the total effect of the continuous FC intervention on specialty selection was mediated through the weighted composite score – comprising academic performance, satisfaction, active learning, and critical thinking. This substantial indirect effect suggests that weighted composite score represent a key mechanistic pathway partially underlying the influence of continuous FC on career choice.
This aligns with the implementation of the FC teaching model in the surgery clerkship, which is feasible and yields high learner satisfaction, effective knowledge acquisition, and increased career interest in surgery.25 By breaking down barriers to comprehension, FC may help dispel misconceptions about the difficulty of anesthesiology, making it a more accessible and attractive option.
Implications for Addressing China’s Anesthesiologist Shortage
China’s shortfall of anesthesiologists (6.7 per 100,000 population) necessitates new solutions.26 This study suggests that prolonged exposure to FC pedagogy, particularly in the fifth year when specialization choices are solidified, can influence career paths. The model’s effectiveness likely arises from its dual emphasis: (1) enhancing core knowledge through iterative learning and (2) cultivating positive attitudes through practical clinical integration. Our findings, while obtained in an anesthesiology context, suggest a broader implication: that FC and similar active learning strategies may help mitigate workforce shortages in medical specialties perceived as “less visible” or particularly challenging by students. Future research should explore the transferability of this approach to other disciplines facing recruitment challenges.
Limitations
Although encouraging, our findings provoke validation in larger, long-term research. The single-institution design and brief follow-up period limit generalizability. The study did not employ a crossover design, which limits within-student comparisons between teaching models. To address these limitations, future studies will incorporate a crossover design or adopt a multi-institutional framework to enhance comparability and generalizability. The resource-intensive nature of the FC model may present practical issues. Subsequent studies should investigate economic adjustments and assess retention rates in anesthesiology programs.
Conclusion
The continuous FC approach significantly enhances learning outcomes, fosters self-reported essential skills, and increases the selection of anesthesiology as a specialty, demonstrating high effectiveness in medical education.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This project is supported by the Research Project of Teaching Reform in Colleges and Universities of Hunan Province (2024JGYB028 to ZLH, 2024JGYB029 to RYL), and the Central South University Postgraduate Education and Teaching Reform Research Project (2024JGB007 to ZLH, 2024JGB009 to RYL, 2024YJSKS033 to PO, 2025JGB110 to YWL, 2025JGB083 and 2025jy052-3 to YHC).
Disclosure
All authors report no conflicts.
References
1. Tie H, Luo Y, Chen D. Thinkings on the reform of medical education system in China. Med Educ Online. 2024;29(1):2302677. doi:10.1080/10872981.2024.2302677
2. Tianlong L, Yuguang S, Yuanruohan Z, Jian T, Enhao Z. Medical education reform in China in the 21st century: a literature review. Adv Med Educ Pract. 2024;15:1313–1324. doi:10.2147/amep.S489903
3. Zhao W, Zhuo Y, Yong-Bao W, Long-Fei L, Jin-Rui Y. The expansion of 8-year medical training programs in China: a status report. Med Educ Online. 2015;20:25890. doi:10.3402/meo.v20.25890
4. Yixin Y, Yi D, Yannis MP, Haibo J. Attitudes toward ophthalmology as a prospective career among pre-clinical medical students in China. BMC Med Educ. 2023;23(1):539. doi:10.1186/s12909-023-04518-4
5. Priti L, Eiman M, Abdel M, Ihsan M, A E, Mohammed KK. The application of flipped classroom strategies in medical education: a review and recommendations. Med Sci Educ. 2025;35(1):531–540. doi:10.1007/s40670-024-02166-x
6. Yu W, Wen-Jie S, Jia-Cen L, Meng-Chang Y. Flipped classroom model in the standardized training of anesthesiology residents. Asian J Surg. 2023;46(11):4899–4900. doi:10.1016/j.asjsur.2023.05.177
7. Rachel M, Megan D, Ashley W, Ottavia G, Anna Rebecca Y. The flipped classroom approach in a pediatric anesthesiology fellowship curriculum. Cureus. 2023;15(8):e43979. doi:10.7759/cureus.43979
8. Michelle H, Rishi A, Diana L, et al. Flipping the script: a multiyear assessment and comparison of flipped classroom versus traditional didactic teaching at two academic institutions. Curr Probl Diagn Radiol. 2024;54(2):238–241. doi:10.1067/j.cpradiol.2024.07.008
9. Khoiriyah U, Roberts C, Jorm C, Van der Vleuten CP. Enhancing students’ learning in problem based learning: validation of a self-assessment scale for active learning and critical thinking. BMC Med Educ. 2015;15:140. doi:10.1186/s12909-015-0422-2
10. Xie ZB, Cheng XY, Li XY, Zhang YF. Team based learning pedagogy enhances the education quality: a systematic review and meta-analysis. BMC Med Educ. 2025;25(1):580. doi:10.1186/s12909-025-07175-x
11. Ziqi L, Yangting X, Yicheng L, Pei Y, Ming J, Ziqiang L. A partially flipped physiology classroom improves the deep learning approach of medical students. Adv Physiol Educ. 2024;48(3). doi:10.1152/advan.00196.2023
12. Junhua X. Improving student learning and performance through a continuous flipped anatomy teaching model. Anat Sci Educ. 2023;17(2):219–226. doi:10.1002/ase.2351
13. Yun H, Jiaying W, Jie W, et al. Semi-flipped classroom-based learning interventions in a traditional curriculum of oral medicine: students’ perceptions and teaching achievements. BMC Med Educ. 2023;23(1):44. doi:10.1186/s12909-023-04017-6
14. Wanjing Y, Xiaoyan Z, Xinhuan C, Jing L, Fang T. Based case based learning and flipped classroom as a means to improve international students’ active learning and critical thinking ability. BMC Med Educ. 2024;24(1):759. doi:10.1186/s12909-024-05758-8
15. Heinze G, Schemper M. A solution to the problem of separation in logistic regression. Stat Med. 2002;21(16):2409–2419. doi:10.1002/sim.1047
16. Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J Pers Soc Psychol. 1986;51(6):1173–1182. doi:10.1037//0022-3514.51.6.1173
17. Nguyen TQ, Ogburn EL, Schmid I, et al. Causal mediation analysis: from simple to more robust strategies for estimation of marginal natural (in)direct effects. Stat Surv. 2023;17:1–41. doi:10.1214/22-ss140
18. Su Jin C. Medical students’ satisfaction on online flipped learning by learning styles. Korean J Med Educ. 2021;33(4):405–409. doi:10.3946/kjme.2021.208
19. Jarina B, Syed Irfan A, Manasee P. Introduction of interactive teaching for undergraduate students in community medicine. Indian J Community Med. 2020;45(1):72–76. doi:10.4103/ijcm.IJCM_232_19
20. Javeed S, Cha-Chi F, Arianne T, Tasha RW, Daniel JS, Andrea NLH. What are we made for? Mobilizing medical education research for impact. Acad Med. 2024;99(11):1177–1180. doi:10.1097/acm.0000000000005850
21. Özkan Ö, Sevil Ç. Effectiveness of flipped classroom teaching models in nursing education: a systematic review. Nurse Educ Today. 2021;102:104922. doi:10.1016/j.nedt.2021.104922
22. Punithalingam Y, Yan C, Mataroria L, Marcus AH. Exploring the pedagogical design features of the flipped classroom in undergraduate nursing education: a systematic review. BMC Nurs. 2021;20(1):50. doi:10.1186/s12912-021-00555-w
23. Mohammad A, Ahmad K, Reza C, Zakieh S, Mehdi R. Creativity and its determinants among medical students. J Educ Health Promot. 2021;9:320. doi:10.4103/jehp.jehp_279_20
24. Najafi M, Motlagh MK, Najafi M, et al. Trend of tendency to critical thinking among medical students in Tehran University of Medical Sciences, 2010-2015: a longitudinal study. J Educ Health Promot. 2022;11:29. doi:10.4103/jehp.jehp_1373_20
25. Cara AL, Dana TL, Laura MM, Sylvia B, James NL. Effectiveness of the surgery core clerkship flipped classroom: a prospective cohort trial. Am J Surg. 2015;211(2):451–457. doi:10.1016/j.amjsurg.2015.10.004
26. Changsheng Z, Shengshu W, Hange L, Fan S, Yuguang H, Weidong M. Anaesthesiology in China: a cross-sectional survey of the current status of anaesthesiology departments. Lancet Reg Health West Pac. 2021;12:100166. doi:10.1016/j.lanwpc.2021.100166
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.