Back to Journals » Journal of Pain Research » Volume 19
Continuous Erector Spinae Plane Block versus Thoracic Epidural Analgesia After Thoracotomy: A Randomized Controlled Assessor-Blinded Non-Inferiority Trial
Authors Cho S, Lee HJ ![]() , Yoon SH
, Yoon SH ![]() , Park SY, Park S, Lee HJ, Park IK, Kang CH, Na KJ, Yoon S
, Park SY, Park S, Lee HJ, Park IK, Kang CH, Na KJ, Yoon S ![]() , Kim YT, Bahk JH
, Kim YT, Bahk JH
Received 30 November 2025
Accepted for publication 12 April 2026
Published 22 April 2026 Volume 2026:19 585519
DOI https://doi.org/10.2147/JPR.S585519
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Andrea Tinnirello
Sooah Cho,1 Ho-Jin Lee,1,2 Soo-Hyuk Yoon,1,2 Sang-Youn Park,1 Samina Park,3,4 Hyun Joo Lee,3,4 In Kyu Park,3,4 Chang Hyun Kang,3,4 Kwon Joong Na,3– 5 Susie Yoon,1,2 Young Tae Kim,3– 5 Jae-Hyon Bahk1,2
1Department of Anesthesiology and Pain Medicine, Seoul National University Hospital, Seoul, Republic of Korea; 2Department of Anesthesiology and Pain Medicine, Seoul National University College of Medicine, Seoul, Republic of Korea; 3Department of Thoracic and Cardiovascular Surgery, Seoul National University Hospital, Seoul, Republic of Korea; 4Department of Thoracic and Cardiovascular Surgery, Seoul National University College of Medicine, Seoul, Republic of Korea; 5Cancer Research Institute, Seoul National University College of Medicine, Seoul, Republic of Korea
Correspondence: Kwon Joong Na, Department of Thoracic and Cardiovascular Surgery, Seoul National University College of Medicine, 101 Daehak-ro, Jongno-gu, Seoul, 03080, Republic of Korea, Tel +82-2-2072-2347, Email [email protected] Susie Yoon, Department of Anesthesiology and Pain Medicine, Seoul National University College of Medicine, 101 Daehak-ro, Jongno-gu, Seoul, 03080, Republic of Korea, Tel +82 2 2072 7361, Email [email protected]
Purpose: Thoracic epidural analgesia (TEA) remains the current gold standard for postoperative pain control after thoracotomy, but is associated with significant complications and contraindications. This study evaluated whether continuous erector spinae plane block (ESPB) provides non-inferior analgesia to TEA.
Patients and Methods: Adult patients scheduled for elective thoracotomy were randomized 1:1 to receive continuous TEA or ESPB. Outcome assessors were blinded to group allocation. In the TEA group, an epidural catheter was inserted at T6– 7 under fluoroscopic guidance with tip confirmation at T5. In the ESPB group, a catheter was placed under ultrasound guidance at the T5 transverse process. Both groups received 0.2% ropivacaine boluses before incision, followed by patient-controlled analgesia for three days. The primary endpoint was resting numeric rating scale pain score on postoperative day 1 with a 2-point non-inferiority margin. Secondary endpoints included pain scores on days 2– 3, opioid consumption, QoR-15K scores, and chronic pain assessments at 3 and 6 months.
Results: Fifty-three patients were enrolled; 44 were included in the modified intention-to-treat analysis (ESPB n=23; TEA n=21). Mean resting NRS scores on postoperative day 1 were 4.22± 1.93 (ESPB) versus 4.81± 1.78 (TEA). The between-group difference was − 0.59 (95% CI, − 1.72– 0.54; P=0.296), meeting the predefined non-inferiority margin. Secondary outcomes, including pain scores, opioid consumption, Quality of Recovery-15 scores, and chronic pain assessments at 3 and 6 months, were comparable between groups. No major complications occurred.
Conclusion: Continuous ESPB demonstrated analgesic efficacy comparable to TEA for postoperative pain control after thoracotomy. Combined with its superior safety profile and technical simplicity, ESPB may serve as an effective alternative to TEA in thoracic surgery.
Keywords: postoperative pain management, multimodal analgesia, thoracic anesthesia, regional anesthesia, quality of recovery
A Letter to the Editor has been published for this article.
A Response to Letter by Ms Liu has been published for this article.
Introduction
Thoracotomy is widely recognized as one of the most painful surgical procedures, and inadequate postoperative pain control has been associated with increased pulmonary complications, delayed recovery, and higher mortality.1,2 Because intravenous opioids often fail to provide adequate analgesia after thoracotomy, thoracic epidural analgesia (TEA) has been established as the gold standard for postoperative pain control.3
Despite its effectiveness, TEA is associated with several complications. Sympathetic blockade can reduce systemic vascular resistance and cardiac output, leading to hypotension, particularly when upper thoracic levels are involved.4 It may also cause orthostatic hypotension, which can delay postoperative ambulation.5 Although rare, serious complications such as epidural hematoma have been reported, limiting its use in patients with coagulopathy or recent anticoagulant therapy.6,7 Additionally, TEA has a reported failure rate of up to 15%, often due to technical difficulties or inaccurate catheter placement.8
The erector spinae plane block (ESPB), first introduced by Forero et al in 2016, represents a promising alternative regional analgesic technique9 This interfascial plane block involves injection of local anesthetic deep to the erector spinae muscle, with the injectate hypothesized to spread through connective tissues to reach spinal nerve rami and potentially diffuse into paravertebral and epidural spaces. ESPB offers several advantages, including technical simplicity, improved safety profile, and no neuraxial contraindications.10 Since its introduction, studies have reported variable analgesic efficacy of ESPB across surgical procedures,11–13 and its clinical effectiveness remains controversial. Notably, healthy volunteer studies have demonstrated limited or absent sensory changes over the anterior thorax.14 Nevertheless, case reports have described continuous ESPB as a rescue technique in thoracotomy patients with failed epidural analgesia.15,16
While a recent randomized controlled trial reported similar analgesic efficacy between ESPB and TEA in thoracotomy patients, methodological limitations, including small sample size and lack of a non-inferiority design, warrant further investigation.17 Therefore, this study was designed as a randomized, assessor-blinded non-inferiority trial to determine whether continuous ESPB provides comparable analgesic effectiveness and safety to TEA, and whether ESPB could serve as a viable alternative to TEA in patients undergoing thoracotomy.
Materials and Methods
Study Design and Participants
This single-center, prospective, randomized, assessor-blinded, non-inferiority trial was approved by the Institutional Review Board (No. 2104–142-1214, 05/17/2021) and registered at ClinicalTrials.gov (ID: NCT05008614, 08/03/2021). Written informed consent was obtained from all participants before enrollment.
Adult patients scheduled for elective thoracotomy with unilateral pulmonary resection were enrolled and randomized in a 1:1 ratio to receive either continuous TEA or continuous ESPB for postoperative analgesia. Randomization was performed using a computer-generated sequence with allocation concealed in sealed opaque envelopes. Anesthesiologists performing the procedures were necessarily unblinded, but postoperative outcome assessment was conducted by a dedicated research nurse who was not involved in block placement or postoperative analgesia management. The assessor did not access procedural details or inspect catheter sites or pump settings during assessments. PCA pump screens were covered, and dosage data were retrieved from the devices after catheter removal for separate analysis.
Inclusion criteria were as follows: age ≥18 years; Eastern Cooperative Oncology Group (ECOG) performance status of 0 or 1; American Society of Anesthesiologists (ASA) physical status classification I to III; and ability to understand study procedures, complete patient-reported outcome questionnaires, and provide written informed consent. We excluded patients with a history of thoracic surgery with persistent postoperative pain, planned chest wall resection, contraindications to neuraxial or interfascial plane blocks (including coagulopathy, ongoing anticoagulant therapy, or known hypersensitivity to fentanyl or ropivacaine), significant renal or hepatic dysfunction, inability to operate a patient-controlled analgesia (PCA) device, cognitive or language barriers precluding questionnaire completion, chronic opioid use for more than three months before surgery, and pregnancy.
Sample Size Calculation
The sample size was calculated using the SampleSize4ClinicalTrials package in R software (version 3.5.1; R Foundation for Statistical Computing, Vienna, Austria). The non-inferiority margin (Δ) was set at 2 points on the 0–10 numeric rating scale (NRS) pain scores, based on Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials (IMMPACT) recommendations indicating that an approximately 2-point reduction represents a moderate clinically important improvement and supported by more recent psychometric evidence suggesting that 2 points may be considered an upper bound for a clinically meaningful difference on 0–10 pain scales.18,19 Based on previous literature20,21 and institutional clinical experience, the standard deviation of NRS pain scores was assumed to be 3.
Assuming 80% power and a one-sided type I error of 0.05, the minimum required sample size was 56 patients (28 per group). To account for an anticipated dropout rate of approximately 24%, the target enrollment was set at 74 patients (37 per group).
Intervention
All patients received their assigned regional analgesia before surgery. All procedures were conducted at the pain clinic by anesthesiologists experienced in thoracic regional anesthesia.
In the TEA group, a thoracic epidural catheter was inserted at the T6–7 interspace under fluoroscopic guidance using a 17-gauge Tuohy needle. The catheter tip was positioned at the mid-body level of T5, and correct placement was confirmed with up to 2 mL of contrast agent. In the operating room, 10 mL of 0.2% ropivacaine was administered before skin incision with hemodynamic monitoring. One hour before the end of surgery, a patient-controlled epidural analgesia pump (0.2% ropivacaine; 3 mL/h basal, 1 mL bolus, 20-min lockout) was initiated with an additional 4 mL loading dose. Epidural analgesia was continued through postoperative day 3.
In the ESPB group, continuous ESPB was performed under ultrasound guidance at the T5 level. An 18-gauge echogenic needle was advanced in a caudocranial direction to the transverse process, followed by minimal hydrodissecion using approximately 3–5 mL of saline to open the fascial plane. The catheter was then advanced 5 cm beyond the needle tip. In the operating room, 20 mL of 0.2% ropivacaine was administered before skin incision with vital sign monitoring. One hour before the end of surgery, an additional 10 mL was injected, and a PCA pump was initiated (0.2% ropivacaine; basal rate 10 mL/h, bolus 5 mL, lockout 20 min). ESPB was continued until postoperative day 3.
Catheter failure was predefined as catheter dislodgement, occlusion, leakage, or suspected malposition requiring catheter replacement or removal. Catheter-related complications and any catheter replacement or removal were recorded.
Perioperative Management
All patients underwent open posterolateral thoracotomy through the fifth intercostal space. General anesthesia was induced with propofol, remifentanil, and rocuronium, and maintained with total intravenous anesthesia using target-controlled infusion of propofol and remifentanil with bispectral index monitoring (target 40–60). Intraoperative monitoring included invasive arterial pressure monitoring, urine output, and esophageal temperature monitoring, and lung-protective ventilation strategies were applied. Detailed protocols are provided in Supplementary Methods 1.
Postoperative Pain Management Protocol
All patients received standardized multimodal analgesia in addition to their assigned regional technique. Intravenous acetaminophen 1000 mg was administered every 8 hours for the first three postoperative days as baseline analgesia. Rescue analgesics were administered when NRS pain scores exceeded 5, following a standardized protocol. First-line rescue agents included ketorolac 15 mg IV every 6 hours as needed (maximum 60 mg/day, limited to 2 days) and tramadol 50 mg IV every 6 hours as needed (maximum 400 mg/day). For patients with contraindications to nonsteroidal anti-inflammatory drugs or inadequate response to first-line agents, morphine 2–4 mg or fentanyl 50 μg IV was administered every 6 hours as needed. Rescue medication selection was individualized based on clinical judgment and patient-specific factors.
Outcome Measures
The primary outcome was the resting NRS pain score on postoperative day 1, defined as the higher of the morning and afternoon measurements. Secondary pain-related outcomes included resting NRS pain scores on postoperative days 2 and 3, movement-associated NRS scores during the same periods, and the maximum NRS score recorded within each 24-hour postoperative period. Additional secondary outcomes included total rescue opioid consumption during the first three postoperative days, converted to oral morphine equivalents (OME).22 Non-opioid analgesics were not included in OME calculations. The proportion of patients requiring any rescue analgesia, opioid rescue, and non-opioid rescue were also recorded. Recovery-related outcomes included Quality of Recovery-15K (QoR-15K) scores measured on postoperative day 3, duration of urinary catheter placement, intensive care unit and hospital length of stay, and chest tube drainage duration. Chronic pain was evaluated at 3 and 6 months postoperatively using the painDETECT questionnaire.
Safety outcomes included adverse events such as hypotension, nausea, vomiting, sedation, respiratory depression, and urinary retention. Technical complications, including catheter dislodgement, migration, or infection, were recorded. Postoperative complications were classified according to the revised Clavien–Dindo classification.
Statistical Analysis
Efficacy and safety analyses were performed on both the modified intention-to-treat (mITT) and per-protocol (PP) populations. The mITT population included all randomized patients who received the allocated intervention and had at least one postoperative pain assessment. The PP population excluded patients with major protocol violations or missing primary endpoint data.
Continuous variables were assessed for normality using the Shapiro–Wilk test. Normally distributed data were presented as mean ± standard deviation and compared using Student’s t-test. Non-normally distributed data were presented as median [interquartile range] and analyzed using the Mann–Whitney U-test. Categorical variables were expressed as frequencies and percentages and analyzed using the chi-square test or Fisher’s exact test as appropriate. The primary analysis assessed non-inferiority by comparing the mean resting NRS pain score on postoperative day 1 between groups. Based on previous studies and clinical judgment, the non-inferiority margin was set at 2 points. Non-inferiority was concluded if the upper bound of the 95% confidence interval for the between-group difference did not exceed 2 points. Secondary endpoints were analyzed using appropriate statistical tests without adjustment for multiple comparisons, as they were considered exploratory. Missing data were handled using available case analysis without imputation. To assess the robustness of 3- and 6-month chronic pain outcomes to loss to follow-up, attrition sensitivity analyses were performed using three approaches: complete-case analysis, best-case/worst-case scenario analysis, and group-specific mean imputation. Baseline characteristics were compared between completers and non-completers to evaluate potential attrition bias.
Post-hoc power analysis was performed using the observed variability from the study data. Bayesian analysis was conducted using the brms package (version 2.20.1) in R with Markov Chain Monte Carlo (MCMC) sampling to provide probabilistic inference complementary to the frequentist non-inferiority test. Weakly informative priors were specified: Normal (0, 5) for the treatment effect, Half-Cauchy (0, 5) for residual standard deviation, and Normal (5, 5) for the intercept. Four parallel MCMC chains were run with 4000 iterations each (2000 warmup, 2000 sampling). Convergence was assessed using  statistics and effective sample sizes. Detailed methodology is provided in Supplementary Methods 2 and 3.
statistics and effective sample sizes. Detailed methodology is provided in Supplementary Methods 2 and 3.
The primary non-inferiority test used a one-sided significance level of 0.05; the 95% confidence interval reported above provides a more conservative criterion. A two-sided P-value of <0.05 was considered statistically significant for all other analyses. The full statistical analysis plan is provided in Supplementary Methods 4. All analyses were performed using R software (version 4.3.0; R Foundation for Statistical Computing, Vienna, Austria) and SPSS (version 25.0; IBM Corp., Armonk, NY, USA).
Results
Between July 2021 and May 2024, 56 patients were assessed for eligibility, of whom 53 were randomized to receive either continuous ESPB (n=26) or TEA (n=27) (Figure 1). Although the initial target enrollment was 74 patients to account for anticipated dropouts, recruitment was stopped at 53 patients due to external circumstances, including a nationwide healthcare workforce disruption and a subsequent decrease in thoracotomy case volume. Of 53 randomized patients, 44 (83.0%) were included in the mITT analysis (ESPB: 23/26 [88.5%]; TEA: 21/27 [77.8%]); 9 patients were excluded due to changes in surgical procedure (n=8) or the need for postoperative mechanical ventilation (n=1). The PP population comprised 40/53 patients (75.5%; ESPB: 20/26 [76.9%]; TEA: 20/27 [74.1%]), with 4 additional patients excluded for catheter-related protocol deviations. At 6 months, follow-up was completed by 37/44 mITT patients (84.1%; ESPB: 18/23 [78.3%]; TEA: 19/21 [90.5%]), with 7 patients lost due to death (n=3), refused survey (n=3), and postoperative complications (n=1). Baseline characteristics were well balanced between groups in both mITT and PP populations (Table 1 and Supplementary Table S1).
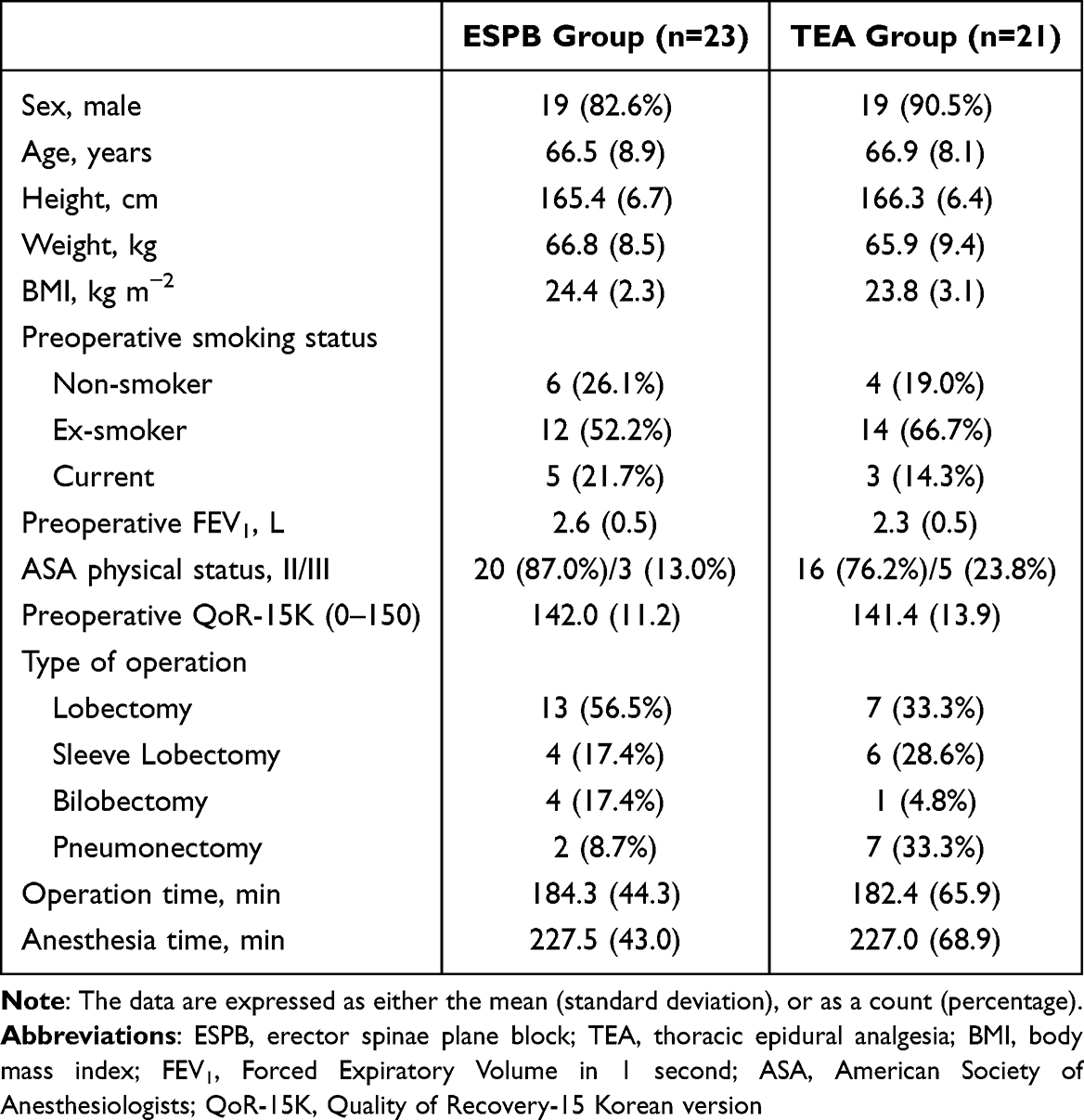 |
Table 1 Baseline Characteristics |
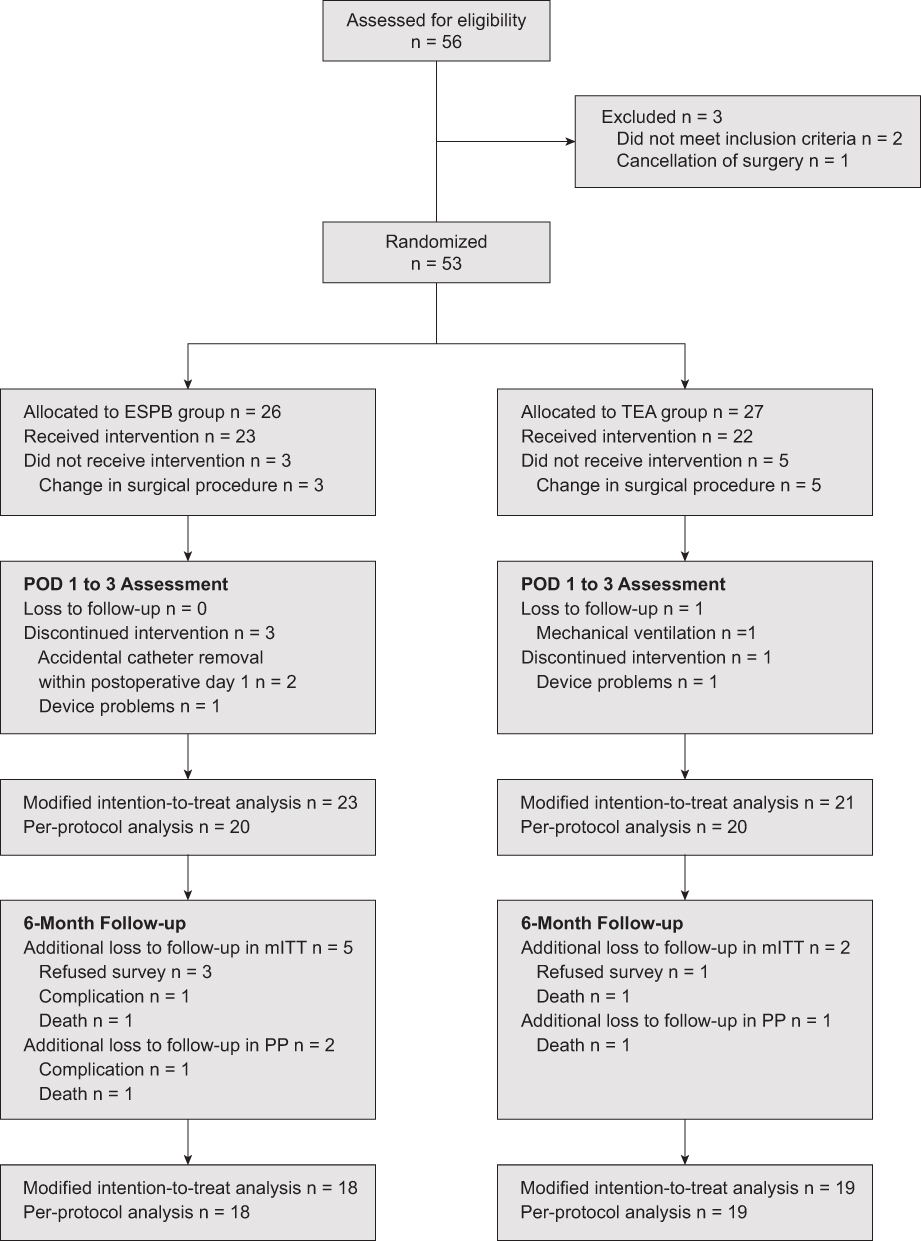 |
Figure 1 CONSORT flow diagram of patient recruitment and analysis. Abbreviations: ESPB, erector spinae plane block; TEA, thoracic epidural analgesia; POD, postoperative day. |
ESPB was non-inferior to TEA for the resting NRS pain score on postoperative day 1. In the mITT analysis, the mean (SD) score was 4.22 (1.93) in the ESPB group and 4.81 (1.78) in the TEA group (mean difference −0.59, 95% CI −1.72 to 0.54, P=0.296). In the PP analysis, corresponding values were 4.10 (1.94) vs 4.65 (1.66) (mean difference −0.55, 95% CI −1.71 to 0.61, P=0.343). Non-inferiority was concluded as the upper bound of the 95% confidence interval did not exceed the predefined margin of 2 points in both analyses (Figure 2).
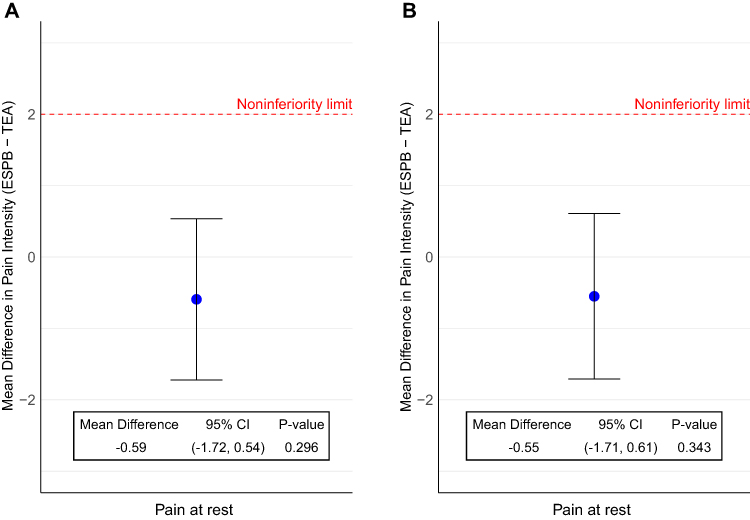 |
Figure 2 Non-inferiority analysis of resting pain scores on postoperative day 1. Forest plots showing the mean difference in numeric rating scale (NRS) pain scores between continuous erector spinae plane block (ESPB) and thoracic epidural analgesia (TEA) groups. (A) Modified intention-to-treat analysis (n=44; ESPB n=23, TEA n=21). (B) Per-protocol analysis (n=40; ESPB n=20, TEA n=20). The vertical dashed line represents no difference between groups. The non-inferiority margin was predefined as 2 points. Non-inferiority is demonstrated when the upper bound of the 95% confidence interval does not exceed the non-inferiority margin of 2 points. Abbreviation: CI, confidence interval. |
No significant differences were observed between groups for any secondary pain outcomes (Table 2, Supplementary Tables S2 and S3). The mean (SD) movement-associated NRS scores on POD 1 were 6.10 (2.13) vs 6.90 (1.58) (P=0.179), and maximum NRS scores were 6.80 (1.40) vs 7.38 (1.47) (P=0.202) for ESPB and TEA groups, respectively. Pain scores progressively decreased over the 3-day observation period in both groups, with no significant between-group differences at any time point in the mITT population (Figure 3), with consistent findings observed in the per-protocol analysis (Supplementary Figure S1). By POD 3, resting pain scores had decreased to 2.96 (1.77) in the ESPB group and 2.95 (1.28) in the TEA group (P=0.993). Total rescue opioid consumption during the first 3 postoperative days, expressed as OME, did not differ significantly between groups (ESPB: 14.6 ± 19.9 mg vs TEA: 10.6 ± 15.8 mg; mean difference 4.0 mg, 95% CI −6.9 to 14.9; P=0.564, mITT population, Table 2). The proportion of patients requiring any rescue analgesia was also comparable (ESPB: 73.9% [17/23] vs TEA: 81.0% [17/21]; P=0.724 Supplementary Table S4).
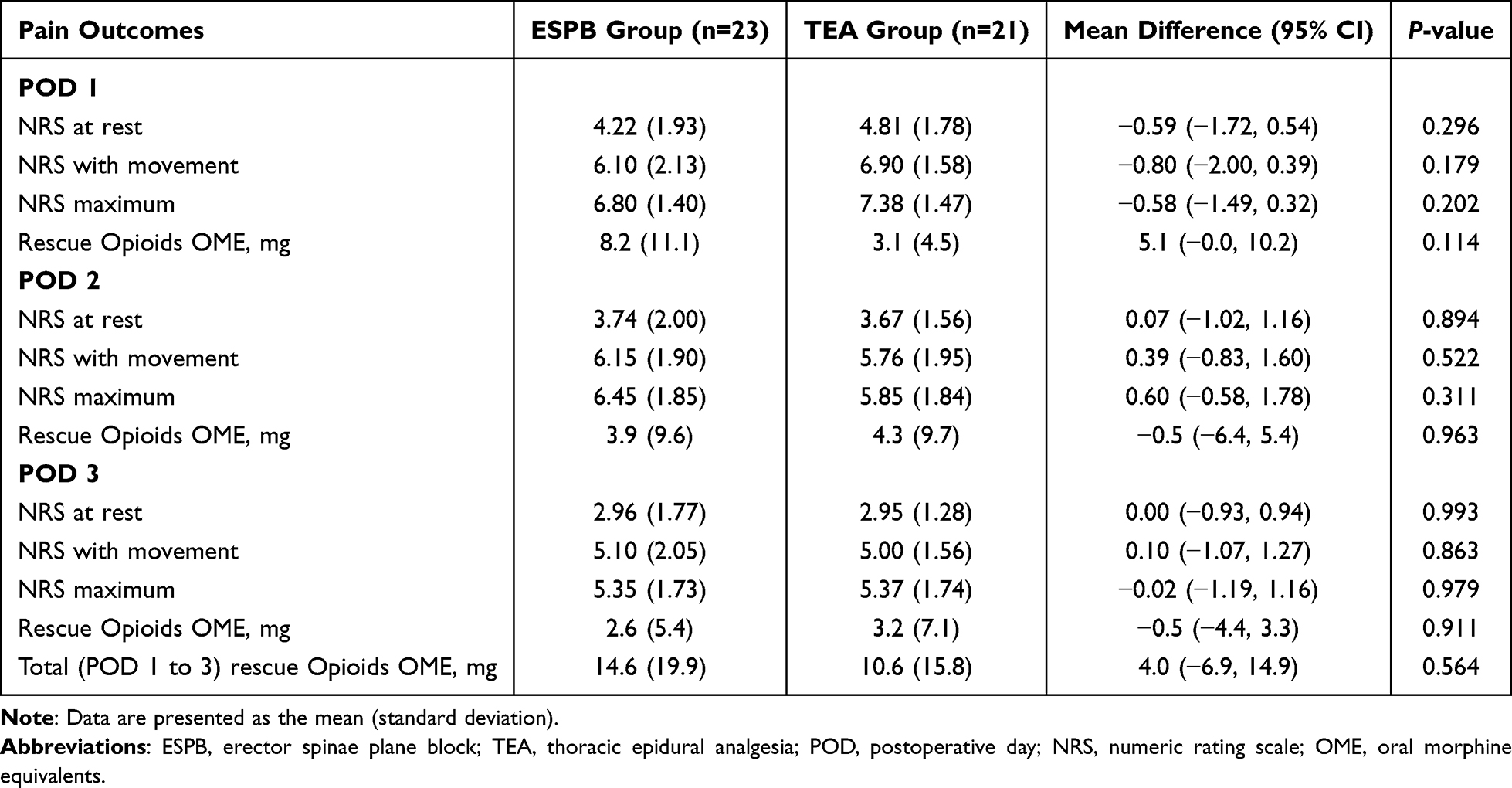 |
Table 2 Comparison of Postoperative Pain Score and Need of Rescue Analgesics at Each Time Point |
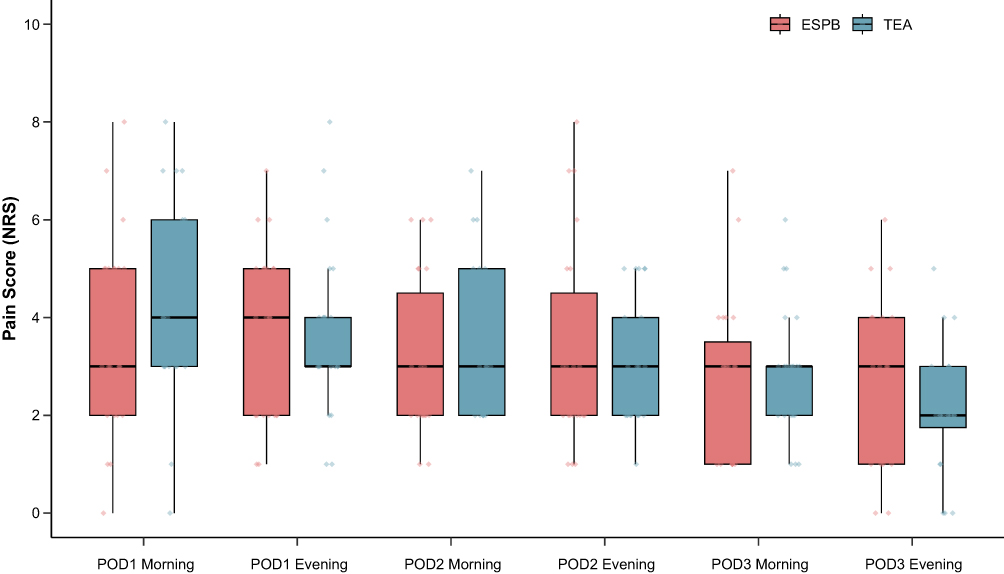 |
Figure 3 Resting pain scores over time. Box plots showing numeric rating scale (NRS) pain scores at rest from postoperative day (POD) 1 morning through POD 3 evening. Box plots display the median (center line), interquartile range (box), and maximum and minimum values (upper and lower whiskers, respectively). Dots show the individual data points. Abbreviations: ESPB, erector spinae plane block; TEA, thoracic epidural analgesia. |
Postoperative recovery quality as measured by the QoR-15K on POD3 was similar (mean (SD), ESPB group 104.0 (25.0) vs TEA group 105.4 (18.6), P=0.85). The total dose of intraoperative remifentanil, duration of chest tube drainage, urinary catheterization, length of ICU or hospital stay, and postoperative 3-month FEV1 were comparable across groups (Table 3 and Supplementary Table S5). Chronic pain assessments using the painDETECT questionnaire at 3 and 6 months postoperatively showed no significant group differences (Table 4). The incidence of adverse events, including hypotension, sedation, respiratory depression, and urinary retention, was low and not statistically different between groups (Table 3 and Supplementary Table S5). No catheter-related complications, such as hematoma or infection, were reported in either group. Attrition sensitivity analyses for the 3- and 6-month outcomes, including best-case/worst-case scenarios and mean imputation, yielded results consistent with the complete-case analysis, indicating that loss to follow-up did not meaningfully alter the chronic pain findings (Supplementary Table S6).
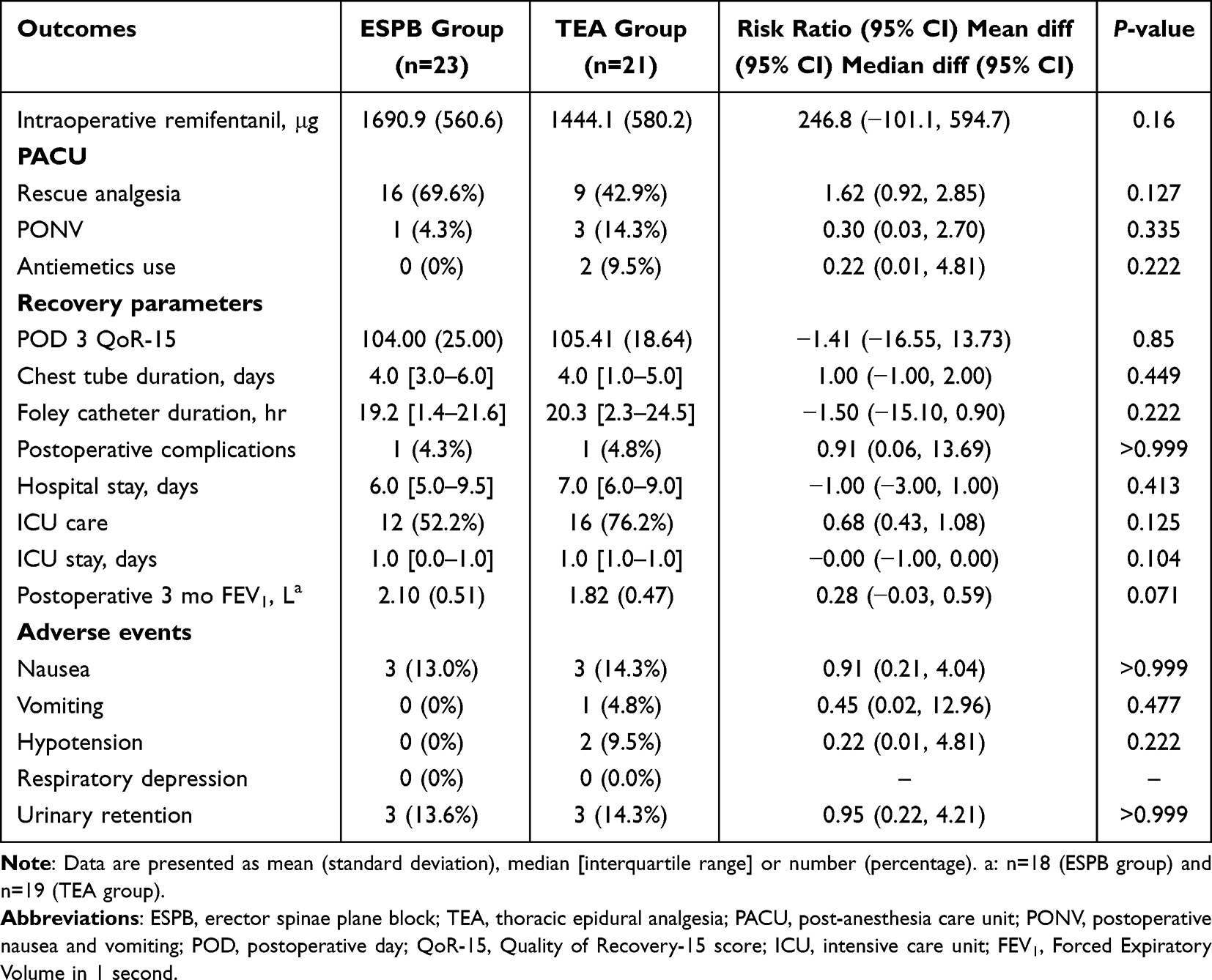 |
Table 3 Postoperative Secondary Outcomes and Recovery Parameters |
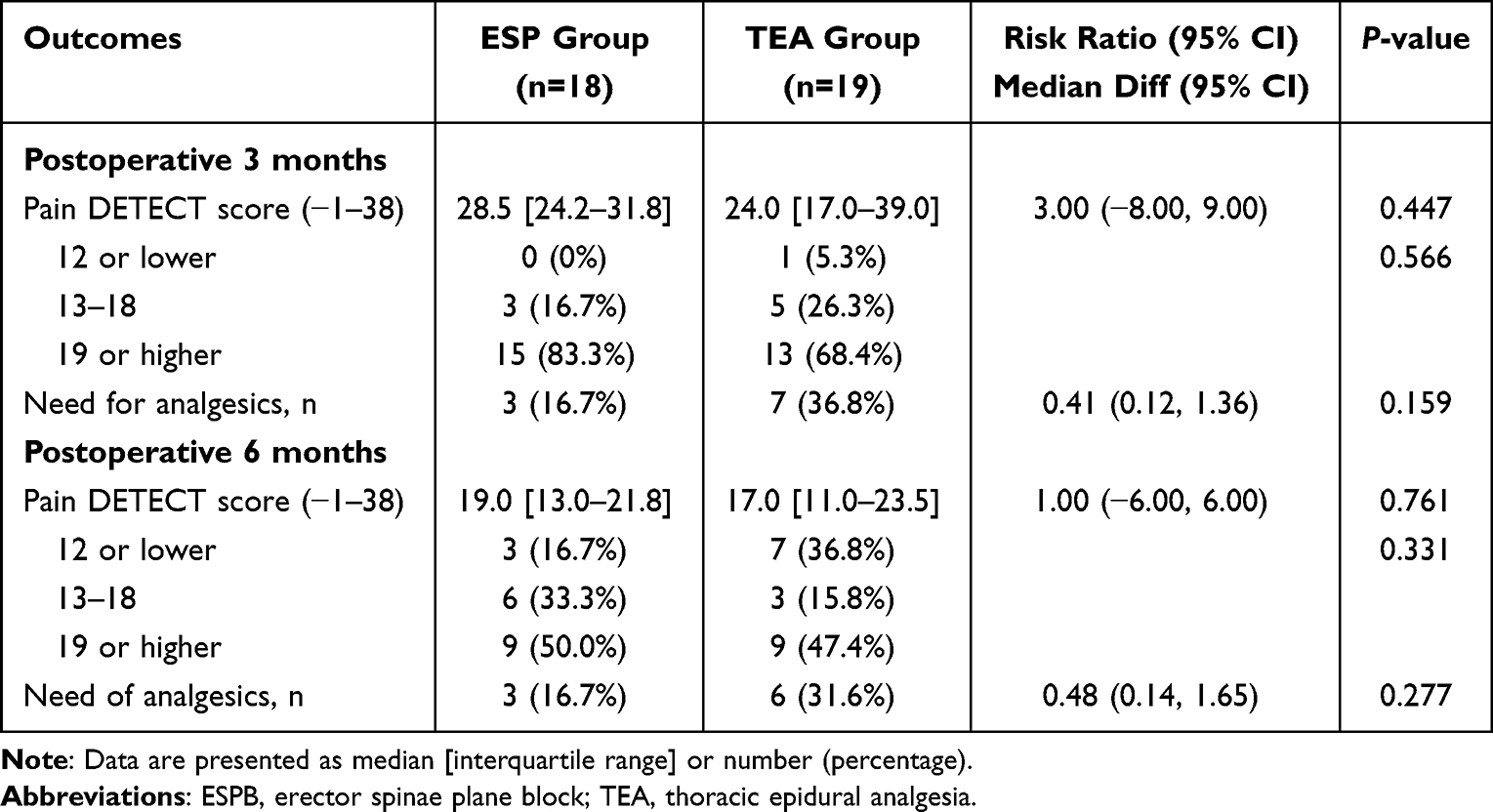 |
Table 4 Chronic Pain Assessment |
Post-hoc power analysis using the observed pooled standard deviation (1.86 points) showed that the achieved sample size of 44 patients provided approximately 65% power to detect the predefined non-inferiority margin of 2.0 points with a one-sided alpha of 0.05, substantially below the target 80% power (Supplementary Table S7).
Bayesian analysis with weakly informative priors yielded a posterior mean treatment difference of −0.58 points (95% credible interval: −1.69 to 0.52), consistent with the frequentist analysis. The posterior probability that the true difference is within the non-inferiority margin of 2.0 points was >99.9%, providing strong probabilistic evidence for non-inferiority. Model convergence was excellent with all  values = 1.00 and effective sample sizes >3500. Detailed Bayesian results are presented in Supplementary Table S8.
values = 1.00 and effective sample sizes >3500. Detailed Bayesian results are presented in Supplementary Table S8.
Discussion
In this randomized, assessor-blinded non-inferiority trial, continuous ESPB was non-inferior to TEA for postoperative pain control after thoracotomy. The between-group difference in NRS scores was −0.59 points (95% CI −1.72 to 0.54) in the modified intention-to-treat analysis and −0.55 points (95% CI −1.71 to 0.61) in the per-protocol analysis, both meeting the predefined non-inferiority criterion of 2 points with a substantial margin. This clinically negligible difference demonstrates that ESPB provides equivalent analgesic efficacy to the current gold standard while offering potential advantages in safety and applicability.
Establishing non-inferiority between ESPB and TEA extends beyond simple pain control, validating ESPB as a viable first-line option for thoracotomy analgesia, particularly when TEA may be contraindicated or technically challenging. This represents a meaningful advancement in perioperative pain management, potentially expanding high-quality analgesia to a broader patient population.
Although the secondary outcomes and chronic pain assessments did not show statistically significant between-group differences, several endpoints demonstrated numerically meaningful differences that may be clinically important. These included rescue analgesia use (69.6% vs 42.9%), hospital length of stay (6 vs 7 days), ICU admission (52.2% vs 76.2%), and the need for analgesics at 3 months and 6 months (16.7% vs 36.8% and 16.7% vs 31.6%) in the ESPB and TEA groups, respectively. Given the reduced sample size and the exploratory nature of these comparisons, the corresponding estimates are imprecise and should be interpreted cautiously. These findings are preliminary, suggest possible differences, and should be confirmed in larger, adequately powered trials.
Recent meta-analyses have consistently demonstrated ESPB’s analgesic efficacy across multiple surgical specialties, with significant reductions in postoperative opioid consumption and pain scores.23–25 Systematic reviews including thoracic surgery have reported that ESPB is associated with significant reductions in postoperative pain compared with non-block care (standard systemic analgesia without a regional block) and, in some studies, thoracic paravertebral block (TPVB).12 Our findings support this evidence base while extending it to the most challenging thoracic procedure in terms of postoperative pain. However, recent network meta-analyses comparing regional analgesic techniques for thoracic surgery have generally ranked TEA and/or TPVB highly for early postoperative pain outcomes, while suggesting that ESPB may offer a more favorable adverse-event profile in some analyses.26–28 Importantly, relative performance appears to vary by surgical approach and outcome domain. Thus, while analgesic superiority may be procedure- and endpoint-dependent, beyond analgesic efficacy, ESPB offers distinct safety advantages as a superficial interfascial block outside the neuraxis, classified as low risk for bleeding complications by major international guidelines.29–31 Comprehensive systematic reviews analyzing nearly 2000 patients reported no cases of pneumothorax, motor blockade, or local anesthetic systemic toxicity.32 In our study, no hypotension events occurred in the ESPB group compared to 9.5% (2/21 patients) in the TEA group, with comparable rescue analgesic requirements (73.9% vs 81.0%).
Our findings align with studies demonstrating comparable efficacy between ESPB and TEA, though with variations. Van den Broek et al found that while TEA provided superior dermatomal spread in video-assisted thoracoscopic surgery, ESPB offered tolerable analgesia with fewer adverse events.33 A pediatric randomized controlled trial by Singh et al comparing ESPB with TEA for thoracotomy reported hypotension in 40% of TEA patients but none receiving ESPB.34 However, not all studies demonstrated equivalent efficacy. Van den Broek et al concluded that ESPB may be inferior to TEA, with higher morphine consumption despite similar recovery scores.33 Zapletal et al reported higher opioid requirements with ESPB compared to TEA.35 Additionally, ESPB success rates of 83–85% indicate block failure in 15–17% of cases,10,36 and the mechanism of action remains incompletely understood with variable sensory spread.37,38
Our use of continuous infusion protocols for both techniques contrasts with studies employing single-bolus ESPB that reported inferior outcomes. The timing of block placement and delivery method may significantly impact efficacy, particularly given the importance of establishing adequate neural blockade before surgical stimulation. Image-guided techniques—fluoroscopy for TEA and ultrasound for ESPB—likely contributed to our consistent results by minimizing technical failures.39 This dual approach to precision placement minimized technical failures and enhanced the internal validity of our comparison, representing current best practices for both techniques.
The complementary Bayesian analysis provides additional insights beyond the frequentist framework. While frequentist non-inferiority testing evaluates whether the upper confidence bound exceeds a pre-specified margin, Bayesian analysis directly quantifies the probability that ESPB is non-inferior given the observed data. The >99.9% posterior probability of non-inferiority represents strong evidence supporting comparable efficacy, even in the context of an underpowered study design. This probabilistic interpretation may be more intuitive for clinicians than traditional P-values and provides a continuous measure of evidence strength rather than a binary reject/fail-to-reject decision. The consistency between Bayesian credible intervals and frequentist confidence intervals further supports the robustness of our findings.
Our study has several important limitations that warrant consideration. First, patient enrollment was prematurely terminated due to external circumstances, resulting in a final sample size of 44 patients that fell short of the calculated requirement of 56 patients, which may have reduced statistical power. Second, complete blinding cannot be guaranteed because catheter insertion sites and infusion devices could have been visible during routine postoperative care. However, practical measures were implemented to minimize assessment bias: PCA pump screens were covered, dosage data were collected separately after device retrieval, and outcome assessment was performed by a research nurse who was limited to pain score recording and patient interviews without access to procedural or analgesic management details. Third, our single-center design at a high-volume academic institution may limit generalizability to centers with different patient populations or levels of regional anesthesia expertise. Fourth, the non-inferiority margin of 2-point, while clinically justified based on previous literature, may be considered generous by some standards, though our actual difference was substantially smaller. Moreover, the minimal clinically important difference is primarily defined at the individual level and may not directly translate to between-group differences in trial design.40 Notably, the observed upper bound of the 95% confidence interval (0.54 points) was well below the pre-specified margin, and Bayesian analysis demonstrated posterior probabilities of non-inferiority exceeding 98% even at a more stringent margin of 1.5 points. Although a predefined non-inferiority margin for opioid consumption would have provided a more comprehensive assessment of analgesic efficacy, opioid consumption was included as a secondary outcome rather than a co-primary endpoint in the present study and should be considered in future non-inferiority designs.
Future research should prioritize large-scale, multicenter trials and standardization of continuous ESPB protocols. Significant heterogeneity exists regarding optimal local anesthetic concentration, infusion rates, bolus volumes, and therapy duration. Our protocol (0.2% ropivacaine, 10 mL/h basal rate, 5 mL bolus every 20 minutes) was based on institutional experience rather than evidence-based guidelines. This lack of standardization represents a barrier to widespread adoption and may contribute to variable efficacy across studies. Dose-finding studies should establish optimal concentration-volume relationships, appropriate infusion rates for different procedures, and minimum effective therapy duration while minimizing local anesthetic exposure. Economic analyses, investigations into enhanced recovery protocols, and research identifying patient-specific predictors of ESPB success would further advance clinical application.
Conclusion
In conclusion, continuous ESPB met the pre-specified non-inferiority criterion compared with TEA for controlling postoperative pain after thoracotomy, as the upper bound of the 95% confidence interval for the between-group difference (0.54 points) was below the non-inferiority margin (Δ=2). The comparable analgesic efficacy, combined with ESPB’s favorable safety profile, technical simplicity, and broad applicability, suggests that it may be a practical alternative to TEA. However, given the reduced sample size, these findings should be interpreted cautiously and warrant confirmation in adequately powered trials. Taken together, these findings represent a step toward expanding access to postoperative analgesia options and support further evaluation of ESPB within thoracic surgery analgesic pathways.
Data Sharing Statement
The datasets are available from the two corresponding authors upon reasonable request.
Ethics Approval and Informed Consent
This study was approved by the Institutional Review Board of Seoul National University Hospital (IRB No. 2104-142-1214; approved on 17 May 2021). The trial was registered at ClinicalTrials.gov (Identifier: NCT05008614) prior to patient enrollment. Written informed consent was obtained from all participants before inclusion in the study, in accordance with the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by a grant from the Seoul National University College of Medicine Research Foundation (800-20210480).
Disclosure
Kwon Joong Na reports cofounder and stakeholder of Portrai, grants from Inocras, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Liu S, Carpenter RL, Neal JM. Epidural anesthesia and analgesia: their role in postoperative outcome. Anesthesiology. 1995;82(6):1474–13. doi:10.1097/00000542-199506000-00019
2. Wu CL, Fleisher LA. Outcomes research in regional anesthesia and analgesia. Anesth Analg. 2000;91(5):1232–1242. doi:10.1097/00000539-200011000-00035
3. Ng A, Swanevelder J. Pain relief after thoracotomy: is epidural analgesia the optimal technique? Br J Anaesth. 2007;98(2):159–162. doi:10.1093/bja/ael360
4. Holte K, Foss NB, Svensén C, Lund C, Madsen JL, Kehlet H. Epidural anesthesia, hypotension, and changes in intravascular volume. Anesthesiology. 2004;100(2):281–286. doi:10.1097/00000542-200402000-00016
5. Gramigni E, Bracco D, Carli F. Epidural analgesia and postoperative orthostatic haemodynamic changes: observational study. Eur J Anaesthesiol. 2013;30(7):398–404. doi:10.1097/EJA.0b013e32835b162c
6. Rawal N. Current issues in postoperative pain management. Eur J Anaesthesiol. 2016;33(3):160–171. doi:10.1097/EJA.0000000000000366
7. Ruppen W, Derry S, McQuay H, Moore RA. Incidence of epidural hematoma, infection, and neurologic injury in obstetric patients with epidural analgesia/anesthesia. Anesthesiology. 2006;105(2):394–399. doi:10.1097/00000542-200608000-00023
8. Romero A, Garcia JEL, Joshi GP. The state of the art in preventing postthoracotomy pain. Semin Thorac Cardiovasc Surg. 2013;25(2):116–124. doi:10.1053/j.semtcvs.2013.04.002
9. Forero M, Adhikary SD, Lopez H, Tsui C, Chin KJ. The erector spinae plane block: a novel analgesic technique in thoracic neuropathic pain. Reg Anesth Pain Med. 2016;41(5):621–627. doi:10.1097/AAP.0000000000000451
10. Pawa A, King C, Thang C, White L. Erector spinae plane block: the ultimate ‘plan A’ block? Br J Anaesth. 2023;130(5):497–502. doi:10.1016/j.bja.2023.01.012
11. Altiparmak B, Toker MK, Uysal AI, Kuscu Y, Demirbilek SG. Ultrasound-guided erector spinae plane block versus oblique subcostal transversus abdominis plane block for postoperative analgesia of adult patients undergoing laparoscopic cholecystectomy: randomized, controlled trial. J Clin Anesth. 2019;57:31–36. doi:10.1016/j.jclinane.2019.03.012
12. Huang W, Wang W, Xie W, Chen Z, Liu Y. Erector spinae plane block for postoperative analgesia in breast and thoracic surgery: a systematic review and meta-analysis. J Clin Anesth. 2020;66:109900. doi:10.1016/j.jclinane.2020.109900
13. Taketa Y, Irisawa Y, Fujitani T. Comparison of ultrasound-guided erector spinae plane block and thoracic paravertebral block for postoperative analgesia after video-assisted thoracic surgery: a randomized controlled non-inferiority clinical trial. Reg Anesth Pain Med. 2020;45(1):10–15. doi:10.1136/rapm-2019-100827
14. Zhang J, He Y, Wang S, et al. The erector spinae plane block causes only cutaneous sensory loss on ipsilateral posterior thorax: a prospective observational volunteer study. BMC Anesthesiol. 2020;20(1):88. doi:10.1186/s12871-020-01002-0
15. Forero M, Rajarathinam M, Adhikary S, Chin KJ. Continuous erector spinae plane block for rescue analgesia in thoracotomy after epidural failure: a case report. A a Case Rep. 2017;8(10):254–256. doi:10.1213/XAA.0000000000000478
16. Adler AC, Yim MM, Chandrakantan A. Erector spinae plane catheter for neonatal thoracotomy: a potentially safer alternative to a thoracic epidural. Can J Anaesth. 2019;66(5):607–608. doi:10.1007/s12630-019-01296-w
17. Elsabeeny WY, Ibrahim MA, Shehab NN, Mohamed A, Wadod MA. Serratus anterior plane block and erector spinae plane block versus thoracic epidural analgesia for perioperative thoracotomy pain control: a randomized controlled study. J Cardiothorac Vasc Anesth. 2021;35(10):2928–2936. doi:10.1053/j.jvca.2020.12.047
18. Dworkin RH, Turk DC, Wyrwich KW, et al. Interpreting the clinical importance of treatment outcomes in chronic pain clinical trials: IMMPACT recommendations. J Pain. 2008;9(2):105–121. doi:10.1016/j.jpain.2007.09.005
19. Reed DE, Stump TE, Monahan PO, Kroenke K. Comparable minimally important differences and responsiveness of brief pain inventory and PEG pain scales across 6 trials. J Pain. 2024;25(1):142–152. doi:10.1016/j.jpain.2023.07.028
20. Liu SS, Richman JM, Thirlby RC, Wu CL. Efficacy of continuous wound catheters delivering local anesthetic for postoperative analgesia: a quantitative and qualitative systematic review of randomized controlled trials. J Am Coll Surg. 2006;203(6):914–932. doi:10.1016/j.jamcollsurg.2006.08.007
21. Mungroop TH, Veelo DP, Busch OR, et al. Continuous wound infiltration versus epidural analgesia after hepato-pancreato-biliary surgery (POP-UP): a randomised controlled, open-label, non-inferiority trial. Lancet Gastroenterol Hepatol. 2016;1(2):105–113. doi:10.1016/S2468-1253(16)30012-7
22. Dowell D, Ragan KR, Jones CM, Baldwin GT, Chou R. CDC clinical practice guideline for prescribing opioids for pain — United States, 2022. MMWR Recomm Rep. 2022;71(No. RR–3):1–95. doi:10.15585/mmwr.rr7103a1
23. Cai Q, Liu GQ, Huang LS, Zhang Y, Dai Z, Xu R. Effects of erector spinae plane block on postoperative pain and side-effects in adult patients underwent surgery: a systematic review and meta-analysis of randomized controlled trials. Int J Surg. 2020;80:107–116. doi:10.1016/j.ijsu.2020.05.038
24. Kendall MC, Alves L, Traill LL, De Oliveira GS. The effect of ultrasound-guided erector spinae plane block on postsurgical pain: a meta-analysis of randomized controlled trials. BMC Anesthesiol. 2020;20(1):99. doi:10.1186/s12871-020-01016-8
25. Leong RW, Tan ESJ, Wong SN, Tan YL, Loo CC, Tan G. Efficacy of erector spinae plane block for analgesia in breast surgery: a systematic review and meta-analysis. Anaesthesia. 2021;76(3):404–413. doi:10.1111/anae.15164
26. Yue F, Xie Y, Chen X, et al. Bayesian network meta-analysis of postoperative analgesic techniques in thoracoscopic lung resection patients. Pain Ther. 2025;14(2):617–637. doi:10.1007/s40122-025-00712-y
27. Zeng J, Tang ZH, Liang JQ, et al. Comparison of various regional analgesia methods for postoperative analgesic effects in video-assisted thoracoscopic surgery: a systematic review and network meta-analysis. Pain Physician. 2022;25(7):E917–E930.
28. Li J, Sun Q, Zong L, Li D, Jin X, Zhang L. Relative efficacy and safety of several regional analgesic techniques following thoracic surgery: a network meta-analysis of randomized controlled trials. Int J Surg. 2023;109(8):2404–2413. doi:10.1097/JS9.0000000000000167
29. Kietaibl S, Ferrandis R, Godier A, et al. Regional anaesthesia in patients on antithrombotic drugs: joint ESAIC/ESRA guidelines. Eur J Anaesthesiol. 2022;39(2):100–132. doi:10.1097/EJA.0000000000001600
30. Horlocker TT, Vandermeulen E, Kopp SL, et al. Regional anesthesia in the patient receiving antithrombotic or thrombolytic therapy: American society of regional anesthesia and pain medicine evidence-based guidelines (fourth edition). Reg Anesth Pain Med. 2018;43(3):263–309. doi:10.1097/AAP.0000000000000763
31. Tsui BCH, Kirkham K, Kwofie MK, et al. Practice advisory on the bleeding risks for peripheral nerve and interfascial plane blockade: evidence review and expert consensus. Can J Anesth. 2019;66(11):1356–1384. doi:10.1007/s12630-019-01466-w
32. De Cassai A, Geraldini F, Carere A, Sergi M, Munari M. Complications rate estimation after thoracic erector spinae plane block. J Cardiothorac Vasc Anesth. 2021;35(10):3142–3143. doi:10.1053/j.jvca.2021.02.043
33. van den Broek RJC, Postema JMC, Koopman JSHA, et al. Continuous erector spinae plane block versus thoracic epidural analgesia in video-assisted thoracoscopic surgery: a prospective randomized open-label non-inferiority trial. Reg Anesth Pain Med. 2025;50(1):11–19. doi:10.1136/rapm-2023-105047
34. Singh S, Andaleeb R, Lalin D. Can ultrasound-guided erector spinae plane block replace thoracic epidural analgesia for postoperative analgesia in pediatric patients undergoing thoracotomy? A prospective randomized controlled trial. Ann Card Anaesth. 2022;25(4):453–459. doi:10.4103/aca.aca_269_20
35. Zapletal B, Bsuchner P, Begic M, et al. Effectiveness and safety of erector spinae plane block vs. conventional pain treatment strategies in thoracic surgery. J Clin Med. 2025;14(9):2870. doi:10.3390/jcm14092870
36. Cassai AD, Bonvicini D, Correale C, Sandei L, Tulgar S, Tonetti T. Erector spinae plane block: a systematic qualitative review. Minerva Anestesiologica. 2019;85(3):308–319. doi:10.23736/S0375-9393.18.13341-4
37. De Cassai A, Andreatta G, Bonvicini D, et al. Injectate spread in ESP block: a review of anatomical investigations. J Clin Anesth. 2020;61:109669. doi:10.1016/j.jclinane.2019.109669
38. Tulgar S, Balaban O. Local anaesthetic injection point of erector spinae plane block. Indian J Anaesth. 2018;62(5):403–404. doi:10.4103/ija.IJA_200_18
39. Parra MC, Washburn K, Brown JR, et al. Fluoroscopic guidance increases the incidence of thoracic epidural catheter placement within the epidural space: a randomized trial. Reg Anesth Pain Med. 2017;42(1):17–24. doi:10.1097/AAP.0000000000000519
40. Muñoz-Leyva F, El-Boghdadly K, Chan V. Is the minimal clinically important difference (MCID) in acute pain a good measure of analgesic efficacy in regional anesthesia? Reg Anesth Pain Med. 2020;45(12):1000–1005. doi:10.1136/rapm-2020-101670
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.