Back to Journals » Drug Design, Development and Therapy » Volume 16
Continuous Erector Spinae Plane Block Using Programmed Intermittent Bolus Regimen versus Intravenous Patient-Controlled Opioid Analgesia Within an Enhanced Recovery Program After Open Liver Resection in Patients with Coagulation Disorder: A Randomized, Controlled, Non-Inferiority Trial
Authors Wang J, Du F ![]() , Ma Y
, Ma Y ![]() , Shi Y
, Shi Y ![]() , Fang J, Xv J, Cang J, Miao C
, Fang J, Xv J, Cang J, Miao C ![]() , Zhang X
, Zhang X
Received 9 June 2022
Accepted for publication 19 September 2022
Published 30 September 2022 Volume 2022:16 Pages 3401—3412
DOI https://doi.org/10.2147/DDDT.S376632
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Georgios Panos
Jiali Wang1 *, Fang Du1 *, Yimei Ma,1 Yuncen Shi,1 Jie Fang,1 Jing Xv,1 Jing Cang,1 Changhong Miao,1 Xiaoguang Zhang1,2
1Department of Anesthesiology, Zhongshan Hospital, Fudan University, Shanghai, People’s Republic of China; 2Department of Anesthesiology, Jinshan Hospital, Fudan University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaoguang Zhang, Department of Anesthesiology, Zhongshan Hospital, Fudan University, 180 Fenglin Road, Shanghai, 200032, People’s Republic of China, Tel +86 13641995733, Fax +86 21-64041990, Email [email protected]
Purpose: Postoperative pain after open hepatectomy is significant. Preoperative coagulopathy limits the use of epidural analgesia, the gold standard for pain control in open abdominal surgery. Erector spinae plane block (ESPB) is a novel regional anesthesia technique that has been shown to provide effective analgesia in abdominal surgery. In this study, we compared the analgesic efficacy of patient-controlled continuous ESPB (CESPB) with hydromorphone patient-controlled intravenous analgesia (PCIA) after right subcostal incision hepatectomies in hepatocellular carcinoma patients with preoperative coagulopathy.
Patients and Methods: In this randomized, controlled, unblinded, and noninferiority trial, 120 patients were randomized to receive either CESPB or PCIA as primary postoperative analgesia together with parecoxib (40mg Q12 h IV) for 3 days after surgery. The primary outcome was the average cough-elicited pain numeric rating scales (NRS) recorded at the seven follow-up time points of 20:00 on the day of surgery and 9:00 and 15:00 on the postoperative day 1 to day 3 (POD1 to POD3).
Results: The average cough-elicited pain NRS score was 2.402 in the CESPB group and 2.676 in the PCIA group. The mean difference (95% CI) was − 0.274 (− 0.620 to 0.072), which demonstrated the noninferiority of CESPB to PCIA. Patients in the CESPB group had less intraoperative opioid consumption, a lower incidence of moderate-to-severe pain and PONV at POD3, and early resumption of oral intake.
Conclusion: CESPB provides analgesic efficacy noninferior to opioid PCIA in the context of multimodal analgesia after right subcostal incision open hepatectomy.
Keywords: acute pain, blood coagulation disorders, erector spinae plane block, hepatectomy, patient-controlled analgesia, ultrasonography
Plain Language Summary
Because the patients with hepatocellular carcinoma (HCC) often have preoperative or expected postoperative coagulopathy, thoracic epidural analgesia, although being considered as the golden standard for postoperative analgesia after open abdominal surgery, is sometimes a dilemma after open hepatectomy. There are only case reports and case series about the application of continuous erector spinae plane block (CESPB) as the primary analgesic therapy after open liver surgery, thus we aimed to perform a randomized controlled trial to investigate the feasibility, efficacy, and safety of CESPB block in HCC patients with preoperative coagulopathy receiving right subcostal incision hepatectomies. The primary outcome was average cough-elicited pain NRS scores recorded at the seven follow-up time points of 20:00 on the day of surgery, 9:00 and 15:00 on the postoperative day 1 to day 3 (POD1 to POD3), which was 2.402 in the CESPB group and 2.676 in the PCIA group. The 95% CI of the median treatment differences (CESPB-PCIA) successfully demonstrated the noninferiority (non-inferiority margin of 1, 95% CI, −0.620 to 0.072, p = 0.266).
In addition to the clinical meaningful analgesic effect, CESPB application was associated with lower intraoperative opioid consumption, lower incidence of moderate-to-severe pain at POD3, lower incidence of PONV at postoperative day 3 and early oral intake resumption after surgery.
There is still a lack of reliable regional block strategy for the patients contradicted to TEA after open liver surgery according to current evidence. Our study will augment the evidence showing CESPB, a less invasive and easily performed interfacial block is a possible choice. With the aid of further investigation on the benefits of CESPB to the patients receiving open hepatectomy, we might add a new choice for the anesthesiologists to control the pain after open liver resection.
Introduction
Open hepatectomy can be associated with significant postoperative pain. Adequate pain management is key to the success of an enhanced recovery after surgery (ERAS) program for liver resection.1–3 Thoracic epidural analgesia (TEA) is recommended for pain therapy after major open upper abdominal surgery. However, for liver cirrhosis patients with hepatocellular carcinoma (HCC), it is difficult to introduce TEA and determine the timing of catheter removal due to both the preoperative coagulopathy and concern of a prolonged change in platelet count and prothrombin time after liver resection.3,4 For these patients, opioid patient-controlled intravenous analgesia (PCIA) is the conventional postoperative pain therapy. Nonetheless, as the liver is primarily responsible for the metabolism of opioids, care must be taken to prescribe opioid-based analgesia for patients with liver dysfunction. Therefore, it is worth exploring an alternative regional technique for managing postoperative pain after open hepatectomy for patients with preoperative or highly expected postoperative coagulation dysfunction.
Erector spinae plane block (ESPB) is a novel fascial plane block (FPB) first described by Forero et al in 2016.5 Although the mechanism is still unclear, an increasing number of studies have been published describing the clinically meaningful analgesia of ESPB in various clinical scenarios.6,7 Single-shot ESPB possessed an opioid sparing effect in analgesia after open hepatectomy.8–10 Limited evidence from case reports or case series exists on the application of ESPB for postoperative analgesia in patients undergoing open liver surgery.11–13 There is still a lack of randomized controlled trials using continuous ESPB as the primary analgesic therapy after open liver resection.
We hypothesized that unilateral continuous ESPB after subcostal incision liver resection provided analgesia that was non-inferior to opioid PCIA in the context of multimodal analgesia and the ERAS pathway. The primary aim of our study was to compare the postoperative analgesic efficacy of continuous ESPB with that of hydromorphone PCIA in HCC patients with preoperative coagulopathy undergoing subcostal open liver resection. The secondary aim was to compare the effect of continuous ESPB and PCIA on the intraoperative clinical parameters and postoperative recovery profile.
Materials and Methods
Trial Design
This randomized controlled trial was approved by the Ethics Committee of Zhongshan Hospital, Fudan University (No. B2020-011R) and prospectively registered in the Chinese Clinical Trial Registry (Identifier: ChiCTR2000029998) on February 19, 2020. Written informed consent was obtained from all participants before enrolment. The study complied with the Declaration of Helsinki. It complied with the guidelines prescribed by the Consolidated Standards of Reporting Trials (CONSORT) checklist (Table S1).
Participants
We enrolled HCC patients scheduled for elective open liver resection with a right subcostal incision for HCC under general anesthesia between March 2020 and February 2021 at Zhongshan Hospital, Fudan University. The inclusion criteria included patients older than 18 years old and with American Society of Anesthesiologists Physical Status (ASA-PS) 1 or 2, complicated by one or more of the following abnormal preoperative coagulation parameters: international normalized ratio ≥1.4, platelet count <80×109/L, or partial thromboplastin time >38s.14 We also recruited the patients with abnormal coagulation parameters who did not meet the above criteria in whom the attending anesthesiologist decided that an epidural catheter should not be placed. In addition, the patients were required to have sufficient language skills to complete the postoperative follow-up. Patients were excluded if they had a history of being allergic to local anesthetics or chronic use of opioids for pain relief, or if they were being pregnant or lactating. The data were collected in the operating room and the surgical ward.
Interventions
After written informed consent was obtained, patients were randomized 1:1 to the CESPB group or PCIA group according to computer-generated random numbers sealed in opaque envelopes. All patients were transferred to the preoperative holding room and monitored with electrocardiography, pulse oximetry, and noninvasive blood pressure prior to surgery. All patients received peripheral intravenous line placement followed by midazolam 1 mg and fentanyl 50 μg IV. Parecoxib sodium 40 mg IV was given before the incision, and 40mg Q12 h IV was given within 3 days after the surgery in both groups.
Patients allocated to the CESPB group received a right-side ESP catheter inserted under ultrasound guidance by an experienced regional anesthesiologist while the patients were in a sitting position. The T7 transverse process was identified via a low frequency (5 MHz) convex transducer (Navi S, Wisonic company) by counting up from the transverse process of T12 to the T7 level and marked on the skin surface. After skin preparation using 10% povidone-iodine and local infiltration with 2% lidocaine 2 mL, a 9.84 cm 17-gauge Tuohy epidural needle was advanced in the caudal direction from the cephalad to approach the deep aspect of the erector spinae muscle towards the tip of the T7 transverse process using the in-plane technique. After contacting the T7 transverse process, 10% dextrose 10 mL was injected to confirm sufficient fluid spread and expand the plane. Then, a 90 cm 19-gauge epidural catheter (FlexTip Plus Epidural Catheterization Set, ARROW International, Inc.) was threaded 5 cm into the ESP. Next, 0.375% ropivacaine 30 mL was injected through the catheter. Continuous infusion of 0.2% ropivacaine with a programmed intermittent bolus pump (Apon ZZB-IV, Jiangsu Apon Medical Technology Co. Ltd.) was initiated after the ropivacaine bolus with a programmed bolus of 8 mL every hour, with the availability of 5 mL with a 15-min lockout time and background infusion of 3 mL/hr.
Postoperative pain intensity was measured using an 11-point (0 = no pain and 10 = worst pain) NRS. If the patients suffered from breakthrough pain (NRS≥4) that could not be relieved by the patient-controlled bolus, the research assistant first checked whether the catheter had been dislodged. If the catheter was in place, 10 mL 0.2% ropivacaine was administered through the catheter. After 15 minutes, if the pain was not relieved, 0.1 mg hydromorphone IV was titrated in 5-min intervals until NRS<4, and the analgesic method was switched to PCIA.
For the patients allocated to the PCIA group, a programmed infusion pump (Apon ZZBII, Jiangsu Apon Medical Technology Co., Ltd.) was set up to deliver a continuous infusion of PCIA with hydromorphone (0.05 mg/mL) at 0.4 mL/h, bolus 4 mL with a 10-min lockout interval at the first complaint of pain (NRS≥1) in the postoperative anesthesia care unit (PACU). The postoperative rescue analgesia for breakthrough pain was PCIA bolus administration.
Anesthesia Management
Patients in both groups received preoperative 200 mL oral 10% dextrose 2 h before entering the operating room and antibiotic prophylaxis 30 min before incision. Anesthesia was induced with propofol, remifentanil and rocuronium. After tracheal intubation, lung recruitment maneuvers were performed, and volume-controlled mechanical ventilation with a tidal volume of 6–8 mL/kg ideal body weight, and a respiratory rate of 10–12 bpm was initiated with 5 cmH2O PEEP. EtCO2 was maintained at 35 to 45 mmHg. A jugular central venous catheter and a radial arterial catheter were placed after anesthesia. Anesthesia was maintained with 1.0 MAC sevoflurane inhalation and intermittent rocuronium and opioid injection. The intraoperative opioid administration protocol included 0.1 mg/kg oxycodone administered 10 min before incision and titrated administration of 50 μg fentanyl intermittently based on the hemodynamic fluctuation during the surgery. If the surgery lasted over 2 h and was estimated to require more than 30 min to be completed, 0.05 mg/kg oxycodone was added. Central venous pressure (CVP) was maintained at less than 5 cmH2O during the transection phase through intravenous fluid restriction, reverse Trendelenburg position and dobutamine infusion when necessary. The core body temperature was maintained at 36–37°C through intravenous fluid warming and forced-air warming. A lower extremity intermittent compression device was used to prevent venous thrombosis of the lower extremities. The postoperative nausea and vomiting (PONV) prophylaxis strategy included 5 mg dexamethasone IV and 0.3 mg ramosetron IV. After surgery, the patients were extubated in the operating room and transferred to the PACU.
Outcomes
The primary outcome was the average postoperative cough-related NRS pain scores at the seven follow-up time points, which were 20:00 on the day of operation (NOS) and 9:00, and 15:00 on the postoperative days 1 to 3 (POD1 to POD3). Secondary outcomes included the incidence of moderate-to-severe pain (NRS≥4) as well as both rest- and cough-related pain scores at each follow-up time point; number of cutaneous sensory blocked dermatomes, intraoperative cumulative opioid consumption expressed as intravenous morphine milligram equivalent (IV MEQ); intraoperative amounts of crystalloid infusion, colloid infusion, and blood loss, number of patients requiring norepinephrine infusion during surgery; incidence of PONV and pruritus; time of mobilization; resumption of oral feeding; and the first anal exhaust (expressed as hours after surgery). One trained research nurse followed the patients after the surgery. The nurse tested anesthetized dermatomes at the anterior midline, right midclavicular line and right scapular line using a blunt 22-gauge needle applied to the skin at 9:00 AM on POD1. Anesthetized dermatomes were defined as areas with reduced or no sensation compared to the contralateral side. The nurse assessed and documented PONV using a verbal rating scale (VRS) from POD1 through POD3, with an objective measure of severity: 0 = no PONV, the patient reported no nausea and no emesis episodes; 1 = mild PONV, the patient reported nausea but no vomiting or dry-retching; 2 = moderate PONV, the patient reported nausea with dry-retching; and 3 = severe PONV, the patient reported nausea with vomiting episodes.
Sample Size Calculations
Based on the retrospective review of data from our institute, the standard deviation (sd) of the mean cough-related NRS score during 0–3 days after open liver resection was 2 in the patients receiving hydromorphone PCIA. According to our pilot study on the CESPB analgesia after open hepatectomy (n=10, unpublished data), we assumed the same standard deviation (sd) for the CESPB group. After consultation with the experts and review of the literature, we expected a difference in mean NRS score between the intervention groups of <1 on a scale from 0 to 10 as the clinical acceptable non-inferiority limit.15 Therefore, a mean score of 1.0 was assumed for the margin (Δ) in NRS score. With a power of 90% (β=0.10) for type 1 error and one-side α of 0.025, the minimum number of participants was 42 for each group by following formula:  (zα=1.96, zβ=1.28, sd=2, Δ=1).16 Considering a possible drop-out rate of 20%, we decided to include at least 50 patients per group.
(zα=1.96, zβ=1.28, sd=2, Δ=1).16 Considering a possible drop-out rate of 20%, we decided to include at least 50 patients per group.
Randomization
Patients were randomized 1:1 to the CESPB group or PCIA group according to computer-generated random number. The random number sequence was generated using the IBM SPSS Statistics V22.0 software (SPSS, Chicago, IL, USA) by a statistician (with random seed 20191230). The random numbers were sealed in opaque envelopes and opened by the attending anesthesiologist in charge of the case after written informed consent was obtained from the patients by the investigator (Fang Du and Jiali Wang). It was impossible to blind the study participants or outcome assessors to group allocation.
Statistical Analysis
Statistical analysis was performed using IBM SPSS Statistics V22.0 (SPSS, Chicago, IL, USA) and RStudio software version 1.3.1093 (Boston, MA, USA). The normality of the data was determined using the Shapiro–Wilk test. Data are presented as the mean (standard deviation [SD]), median (interquartile range [IQR]), or n (%). For continuous variables with equal variance, univariate analysis was performed using a 2-sample, independent t test. The Mann–Whitney U-test was used for data without normal distribution. The chi-squared test was used for frequency comparison. Categorical variables were compared using Fisher’s exact test. Bonferroni correction was used to analyze NRS scores, and statistical significance was adjusted to p < 0.01 because there were measurements from 7 time points. Repeated measures analysis of variance and simple effect analysis were used to verify whether the differences in the NRS scores between groups were statistically significant. A modified intention-to-treat (mITT) analysis was used for the primary analysis. Patients who did not receive an operation or did not provide any pain scores at the predefined follow-up points were excluded from the mITT analysis. The noninferiority analysis was conducted by comparing the 95% confidence interval (CI) of the pain score difference to the noninferiority margin.
Results
The CONSORT flow diagram is shown in Figure 1. Three hundred and one subjects were screened for eligibility from March 2020 to February 2021. One hundred eighty patients did not meet the inclusion criteria, and one patient declined to participate. After obtaining informed consent, 120 patients were enrolled and randomized to receive either postoperative analgesia with continuous ESPB (CESPB group, n=60) or PCIA (PCIA group, n=60). One patient in the CESPB group dropped out due to accidental ESPB catheter dislodgement before the surgery started. One patient in the PCIA group did not receive the intervention because the surgery was cancelled after randomization. Two patients experienced accidental catheter dislodgement at POD 3, and one patient’s catheter occluded at POD2. These three patients switched to PCIA and were analyzed with the CESPB group per intention-to-treat analysis. The baseline characteristics of patients are summarized in Table 1. All patient characteristics were balanced between groups.
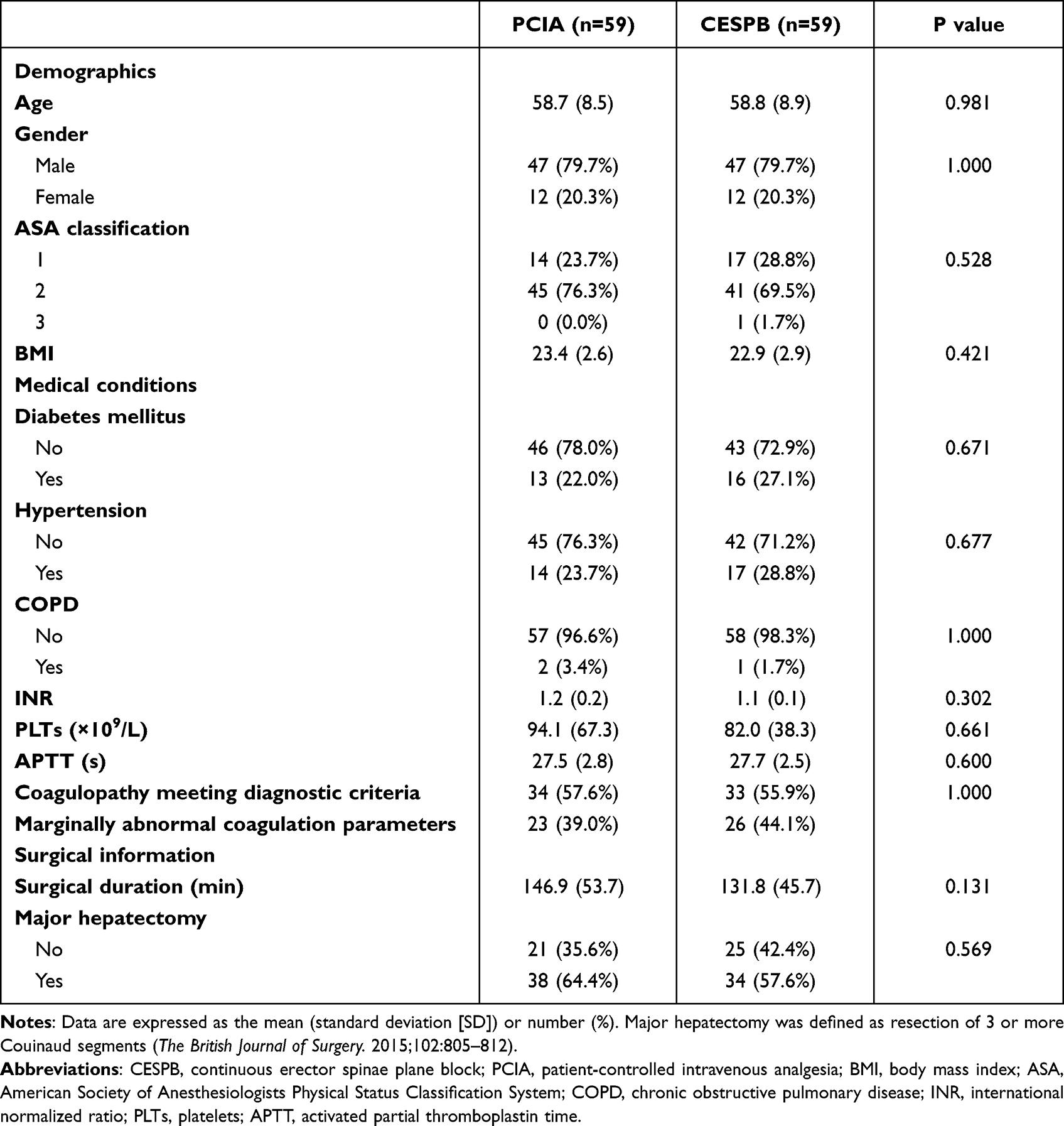 |
Table 1 Patient Characteristics and Surgical Data |
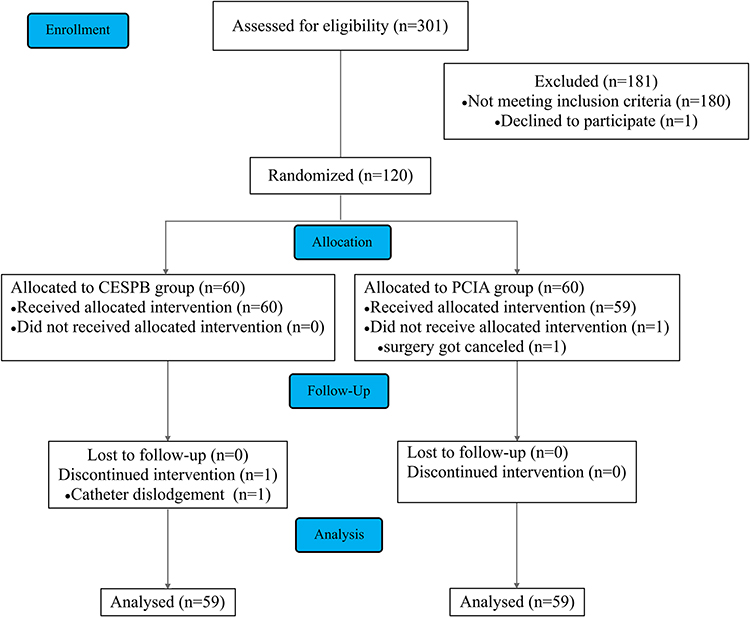 |
Figure 1 CONSORT flow diagram. Abbreviations: CONSORT, Consolidated Standards of Reporting Trials; CESPB, continuous erector spinae plane block; PCIA, patient-controlled intravenous analgesia. Notes: Adapted from: Schulz KF, Altman DG, Moher D, CONSORT Group. CONSORT 2010 Statement: Updated Guidelines for Reporting Parallel Group Randomised Trials. PLoS Med. 2010;7(3):e1000251.30 Copyright: © 2010 Schulz et al. Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0/legalcode). https://journals.plos.org/plosmedicine/article?id=10.1371/journal.pmed.1000251. |
Postoperative Pain Intensity and Trajectory
The primary outcome, the average cough-elicited pain NRS score of the seven follow-up time points, was 2.402 in the CESPB group and 2.676 in the PCIA group. The 95% CI of the median treatment differences (CESPB-PCIA) successfully demonstrated noninferiority, as shown in Figure 2A (noninferiority margin of 1, 95% CI, −0.620 to 0.072, p = 0.266).
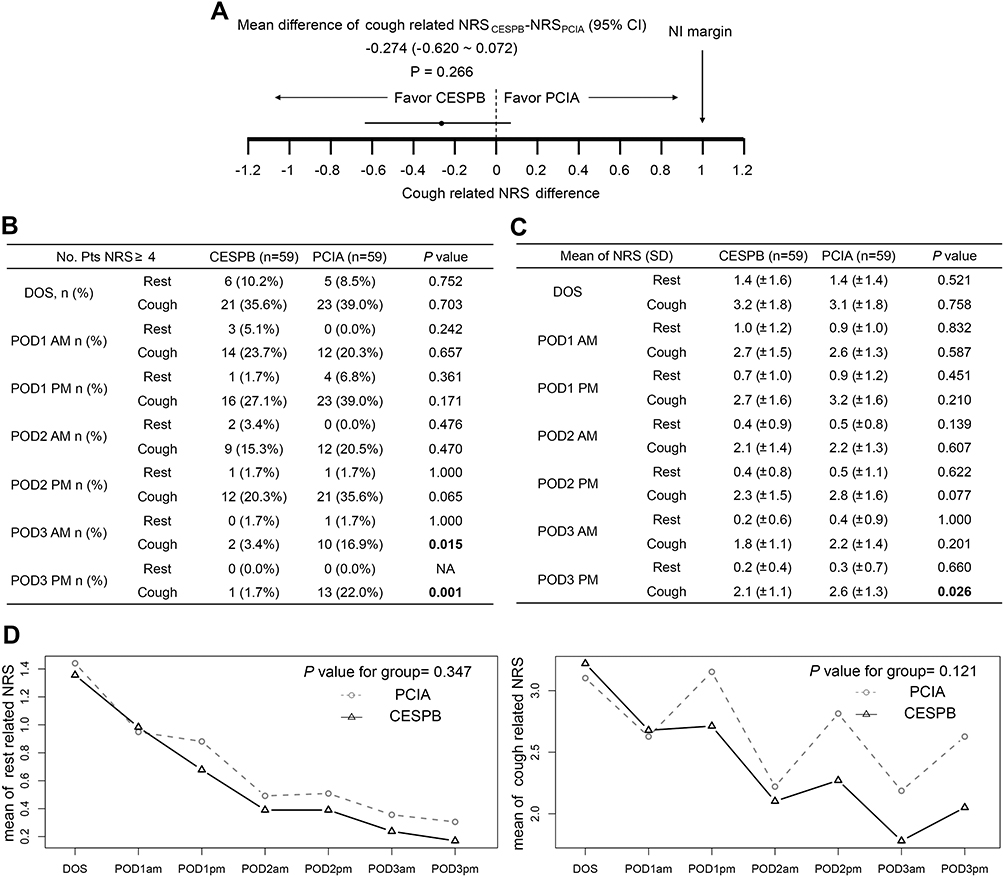 |
Figure 2 Comparison of numerical rating scale (NRS) scores between groups after surgery. (A) Mean differences (CESPB-PCIA) in the average cough-elicited pain NRS score from DOS to POD3. (B) Incidence of NRS scores ≥4 between groups. (C) NRS scores of both groups after surgery. (D) Interception plots illustrating repeated-measures ANOVA of rest-related and cough-related NRS scores between groups. Abbreviations: CESPB, continuous erector spinae plane block; PCIA, patient-controlled intravenous analgesia; NI, noninferiority; DOS, day of surgery; POD, postoperative day. |
The incidence of moderate-to-severe pain (NRS≥4) in the two groups at different time points is summarized in Figure 2B. The incidence of cough-elicited NRS≥4 was significantly lower in the CESPB group at POD3 AM and POD3 PM than that in the PCIA group (rate of cough-related NRS≥4; CESPB vs PCIA; POD3 AM, 3.4% vs 16.9%, p = 0.015; POD3 PM, 1.7% vs 22%, p = 0.001). Comparisons of day-to-day resting and cough-related NRS values were also conducted. Figure 2C shows a significantly lower cough-elicited pain NRS in the CESPB group during POD3 PM (cough-related NRS, CESPB vs PCIA, 2.1 vs 2.6, p = 0.026). Repeated-measures ANOVA of NRS was performed and is illustrated by an interception plot (Figure 2D). The effect of different treatments on the NRS value was not statistically significant (p value for intergroup, resting NRS, 0.347; cough NRS, 0.121).
The valid press ratio calculated as the valid press number divided by the total press number of the patient-controlled button was 0.67 (0.33,1.00) [median (interquartile)] in the CESPB group and 1 (0.90,1.00) in the PCIA group (p < 0.001). Two patients in the CESPB group reported breakthrough pain, which was relieved by administering 10 mL 0.2% ropivacaine through the catheter.
Anesthetized Dermatomes
The numbers of blocked dermatomes were 6 (0,8), 5 (0,7) and 0 (0,0) on the right scapular line, right midclavicular line and midline, respectively. Thirty-seven patients (62.7%) presented sensory loss covering T6 to T10 dermatomes on the right midclavicular line. Figure 3 shows the frequency of blockage at different dermatomes at the three anatomical lines.
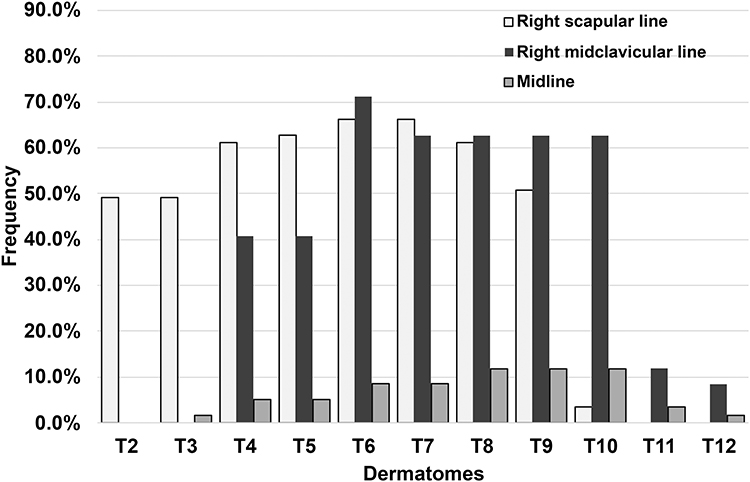 |
Figure 3 Frequency of blockages at different dermatomes at the right scapular line, right midclavicular line and midline. |
Intraoperative Data, Anesthesia-Related Complications and Postoperative Recovery
Opioid consumption expressed as IV MEQ (p = 0.013) was significantly lower in the CESPB group than in the PCIA group. There was no statistically significant difference in the intraoperative amounts of crystalloid infusion, colloid infusion, and estimated blood loss, or the number of patients requiring norepinephrine infusion between groups (Table 2).
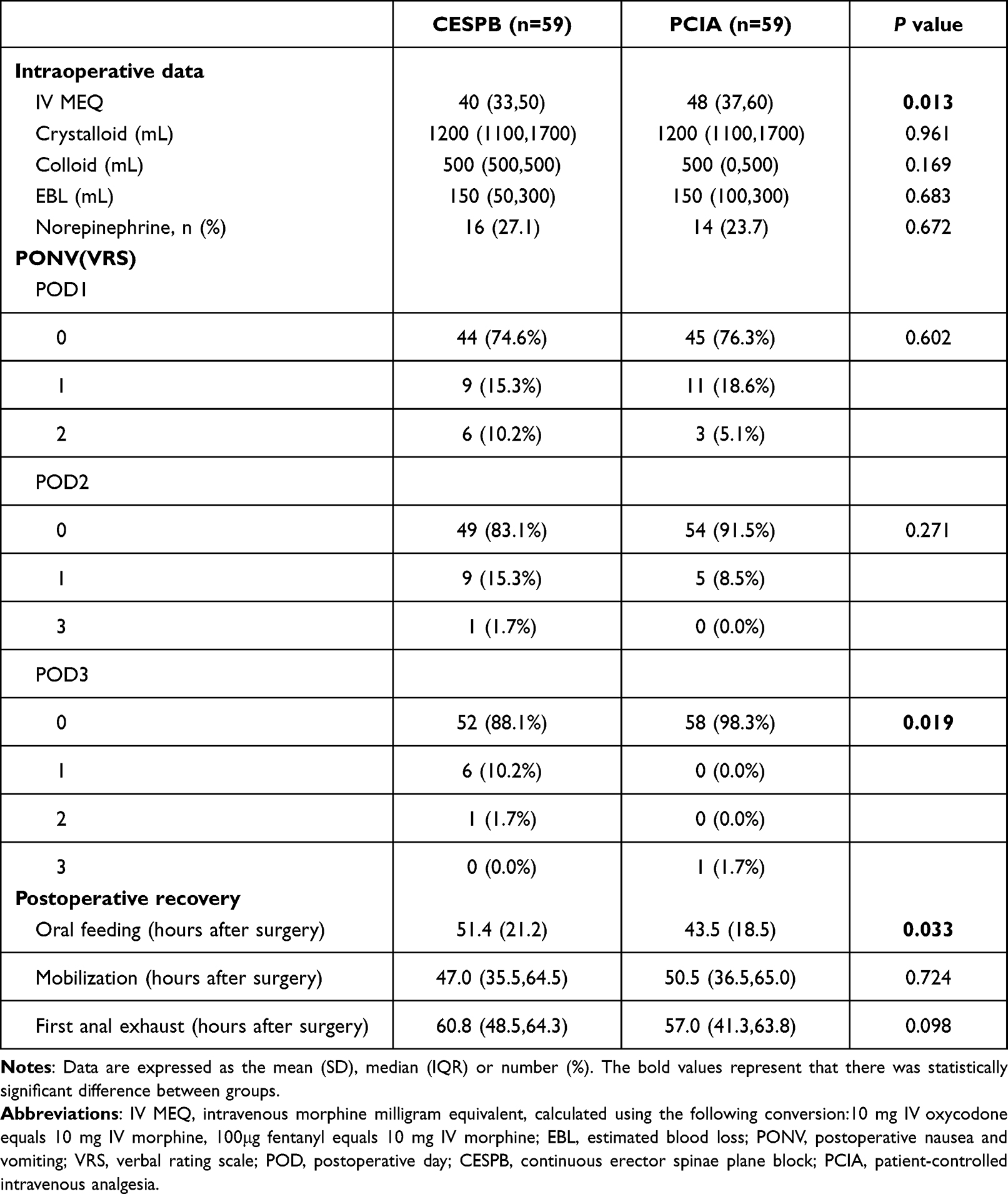 |
Table 2 Intraoperative Data, Anesthesia-Related Complications and Postoperative Recovery |
The incidence of PONV (VRS≥2) during the first 3 postoperative days was 17 (28.8%) in the CESPB group and 24 (40.7%) in the PCIA group (p = 0.176). The distribution of PONV severity differed between groups at POD3 as shown in Table 2. The incidence of PONV in the CESPB group was lower than that in the PCIA group on POD3 (rate of PONV, CESPB vs PCIA, 1.7% vs 11.9%, p = 0.019). The incidence of pruritus was similar between groups (CESPB vs PCIA, 4 [6.8%] vs 7[11.9%], p = 0.527).
Oral intake resumption occurred earlier in the CESPB group patients (CESPB vs PCIA, 43.5[18.5] vs 51.4[21.2], p = 0.033). There were no significant differences regarding the time of mobilization and first anal exhaust (p>0.05, Table 2).
Discussion
This randomized controlled study showed that the analgesic efficacy of unilateral continuous thoracic ESPB with ropivacaine using a programmed intermittent bolus regimen was noninferior to that of hydromorphone PCIA. In addition, continuous ESPB significantly reduced the intraoperative opioid consumption, decreased the incidence of moderate-to-severe pain and PONV on POD3 and led to early oral intake resumption.
Patient-controlled intravenous analgesia with opioids is a conventional acute pain therapy with established analgesic efficacy after open hepatectomy.17,18 We, therefore, performed a noninferiority trial to explore whether a safe and easily performed regional analgesia method, ie, continuous ESPB, would provide noninferior pain therapy to opioid PCIA after open liver resection.
Evidence regarding continuous ESPB for postoperative analgesia in patients undergoing open liver surgery comes from anecdotal experience, case series, or observational studies. Continuous ESPB as primary pain control following a major hepatectomy provided adequate postoperative analgesia in one patient with intrahepatic cholangiocarcinoma with preoperative coagulopathy.13 Nair et al described the successful utilization of an ESPB catheter inserted at the level of T7 as the primary postoperative pain therapy or rescue strategy in three individual cases after the Whipple procedure, major liver resection, and orthotopic liver transplantation respectively with satisfactory analgesic efficacy.11 A retrospective historical controlled cohort study in patients undergoing bilateral subcostal incision open right living donor hepatectomy found that continuous ESPB significantly reduced opioid consumption on the day of surgery and POD1.12 The results from our randomized controlled trial strengthen the evidence that continuous unilateral ESPB could be an alternative primary pain therapy after right subcostal incision open hepatectomy.
Pain control after hepatic resection presents unique challenges, as subcostal incisions, rib retraction, and diaphragmatic irritation can lead to significant somatic and visceral pain. The somatic pain caused by the subcostal incision is mainly transmitted via the intercostal nerves T6 to T10, while the visceral pain comes from the coeliac plexus.18 Although the mechanism of ESPB is controversial, anatomical and clinical studies have suggested that local anesthetic injected into the ESP could spread into the thoracic paravertebral space and proximal intercostal spaces where it acts on the ventral rami of the spinal nerves and intercostal nerves to provide both visceral and somatic analgesia.19,20 However, clinical evidence supports that the patterns of cutaneous sensory blockade often underrepresent the analgesia observed with FPB.21 In our study, despite the clinically meaningful analgesic efficacy, we did not obtain unanimous cutaneous sensory blockade patterns consistent with the clinical efficacy. Continuous ESPB produced a somatic sensory blockade covering the T6 to T10 intercostal nerve innervation area in 62.7% of our patients. The median blocked dermatomes were 6 and 5 on the right scapular and midclavicular lines, respectively. According to our search, there is no description of the sensory block pattern of continuous ESPB, and the results from the single-shot ESPB are inconsistent.22,23
Another critical theory advocated to reconcile the analgesia provided by FPB with the relative lack of consistent sensory neural blockade is the antinociceptive effect of systemically absorbed local anesthetic. This has been best characterized for intravenous lidocaine infusion (IVLI), which reduced early postoperative pain scores and opioid consumption.24,25 Intravenous regional anesthesia with ropivacaine provided sufficient levels of surgical anesthesia and a more prolonged analgesic effect than that of lidocaine without serious side effects26,27 and continuous infusion through an interfacial plane catheter prevented the decline in plasma concentration after a loading dose and caused a gradual increase over time.28 Although there was no clinical presentation of local anesthetic systemic toxicity in our patients, plasma concentration measurement is mandated in future studies to verify the role of systemic absorption of ropivacaine in the analgesic effect.
Although the continuous ESPB provided an analgesia effect that was noninferior to that of hydromorphone PCIA, it was inefficient in rescue therapy of breakthrough pain, as reflected by the lower ratio of the valid press of the patient-controlled button. Thus, appropriate rescue therapy requires more attention if continuous ESPB is planned as the primary postoperative analgesic method.
In addition to the analgesic efficacy, we also compared the intraoperative clinical parameters, anesthesia-related complications, and postoperative recovery. The absolute risk reduction of PONV incidence provided by CESPB analgesia was 11.9% without a statistically significant difference. However, the CESPB led to a lower PONV incidence at POD3. The patients in the CESPB group also reported earlier oral intake resumption than those in the PCIA group. These results suggested that the gastrointestinal function might recover earlier in patients who received CESPB analgesia. The reasons for PONV are multifarious.29 Because our study is not powered to detect the causal relationship between CESPB and the incidence of PONV, further study is required to investigate the effect of this opioid-sparing analgesic therapy on the incidence of PONV, especially in patients at high risk.
Limitations
An important limitation of this trial is that the patients, the caregivers and the outcome assessors were not blinded to the group allocation. Blinding was impossible to implement because of the catheter in the CESPB group and we considered it unethical to insert a sham catheter in the patients in the PCIA group. Another limitation was that through recruiting the patients with marginal coagulation disorder which did not meet the pre-defined criteria for coagulopathy,14 our study cohort might include those not absolutely contraindicated to TEA. Future study focuses on the safety of CESPB on the patients with severe coagulopathy is required. Nonetheless, because the patients with predefined coagulopathy or marginally abnormal coagulation parameters were well balanced between the two groups, it did not affect the outcome assessment.
Conclusion
We found that patient-controlled continuous ESPB through right side ESP catheter placed on the tip of the T7 transverse process was non-inferior to opioid PCIA in the context of multimodal analgesia within an enhanced recovery setting in the postoperative analgesia after right subcostal incision open hepatectomy.
Data Sharing Statement
The individual deidentified participant data that support the findings of this study are available from the corresponding author (Xiaoguang Zhang), under reasonable request upon publication. The study protocol, statistical analyses, and the case report forms will also be available.
Acknowledgments
We thank Hao Chen, Department of Preventive Medicine, School of Public Health, Fudan University, for assisting in the statistical analysis and Peixin Wang from Acute Pain Service of Zhongshan Hospital, Fudan University for assistance with the study.
Funding
This work was supported by the Shanghai Municipal Health Commission Clinical Research Program (202040177).
Disclosure
Xiaoguang Zhang reports grants from Shanghai Municipal Health Commission, during the conduct of the study. The authors report no other potential conflicts of interest in this work.
References
1. Melloul E, Hubner M, Scott M., et al. Guidelines for perioperative care for liver surgery: enhanced Recovery After Surgery (ERAS) society recommendations. World J Surg. 2016;40(10):2425–2440. doi:10.1007/s00268-016-3700-1
2. Noba L, Rodgers S, Chandler C, Balfour A, Hariharan D, Yip V. Enhanced Recovery After Surgery (ERAS) reduces hospital costs and improve clinical outcomes in liver surgery: a systematic review and meta-analysis. J Gastrointest Surg. 2020;24(4):918–932. doi:10.1007/s11605-019-04499-0
3. Agarwal V, Divatia J. Enhanced recovery after surgery in liver resection: current concepts and controversies. Korean J Anesthesiol. 2019;72(2):119–129. doi:10.4097/kja.d.19.00010
4. Dieu A, Huynen P, Lavand’homme P, et al. Pain management after open liver resection: procedure-specific postoperative pain management (PROSPECT) recommendations. Reg Anesth Pain Med. 2021;46(5):433–445. doi:10.1136/rapm-2020-101933
5. Forero M, Adhikary SD, Lopez H, Tsui C, Chin KJ. The erector spinae plane block: a novel analgesic technique in thoracic neuropathic pain. Reg Anesth Pain Med. 2016;41(5):621–627. doi:10.1097/AAP.0000000000000451
6. Saadawi M, Layera S, Aliste J, Bravo D, Leurcharusmee P, Tran Q. Erector spinae plane block: a narrative review with systematic analysis of the evidence pertaining to clinical indications and alternative truncal blocks. J Clin Anesth. 2021;68:110063. doi:10.1016/j.jclinane.2020.110063
7. Kot P, Rodriguez P, Granell M, et al. The erector spinae plane block: a narrative review. Korean J Anesthesiol. 2019;72(3):209–220. doi:10.4097/kja.d.19.00012
8. Daghmouri MA, Mesbahi M, Akremi S, et al. Efficacy of bilateral erector spinae block for post-operative analgesia in liver hydatid surgery. Br J Pain. 2021;15(4):376–379. doi:10.1177/2049463720966636
9. Hacibeyoglu G, Topal A, Arican S, Kilicaslan A, Tekin A, Uzun ST. USG guided bilateral erector spinae plane block is an effective and safe postoperative analgesia method for living donor liver transplantation. J Clin Anesth. 2018;49:36–37. doi:10.1016/j.jclinane.2018.06.003
10. Elshafie MA, Khalil MK, ElSheikh ML, Mowafy NI. Erector spinae block with opioid free anesthesia in cirrhotic patients undergoing hepatic resection: a randomized controlled trial. Local Reg Anesth. 2022;15:1–10. doi:10.2147/LRA.S343347
11. Nair S, McGuinness S, Masood F, Boylan JF, Conlon NP. Erector spinae plane blocks in major hepatopancreaticobiliary surgery: a case series. A a Pract. 2019;13(9):332–334. doi:10.1213/XAA.0000000000001069
12. Adelmann D, Khorashadi M, Zhou G, et al. The use of bilateral continuous erector spinae plane blocks for postoperative analgesia after right-sided living donor hepatectomy: a feasibility study. Clin Transplant. 2021;35(9):e14413.
13. Maddineni U, Maarouf R, Johnson C, Fernandez L, Kazior MR. Safe and effective use of bilateral erector spinae block in patient suffering from post-operative coagulopathy following hepatectomy. Am J Case Rep. 2020;21:e921123. doi:10.12659/AJCR.921123
14. Ramspoth T, Roehl AB, Macko S, et al. Risk factors for coagulopathy after liver resection. J Clin Anesth. 2014;26(8):654–662. doi:10.1016/j.jclinane.2014.08.002
15. Hausken J, Fretland AA, Edwin B, et al. Intravenous patient-controlled analgesia versus thoracic epidural analgesia after open liver surgery: a prospective, randomized, controlled, noninferiority trial. Ann Surg. 2019;270(2):193–199. doi:10.1097/SLA.0000000000003209
16. Xiao-hong Y. Sample size determination for comparison between two means in superiority/equivalence/non-inferiority trials. Chin J New Drugs. 2009;23:2205–2209.
17. Soliz JM, Gebhardt R, Feng L, Dong W, Reich M, Curley S. Comparing epidural analgesia and ON-Q infiltrating catheters for pain management after hepatic resection. Open J Anesthesiol. 2013;3(1):3–7. doi:10.4236/ojanes.2013.31002
18. Dudek P, Zawadka M, Andruszkiewicz P, Gelo R, Pugliese F, Bilotta F. Postoperative analgesia after open liver surgery: systematic review of clinical evidence. J Clin Med. 2021;10(16):3662. doi:10.3390/jcm10163662
19. Chin KJ, Malhas L, Perlas A. The erector spinae plane block provides visceral abdominal analgesia in bariatric surgery: a report of 3 cases. Reg Anesth Pain Med. 2017;42(3):372–376. doi:10.1097/AAP.0000000000000581
20. Chin KJ, El-Boghdadly K. Mechanisms of action of the erector spinae plane (ESP) block: a narrative review. Can J Anaesth. 2021;68(3):387–408. doi:10.1007/s12630-020-01875-2
21. Chin KJ, Lirk P, Hollmann MW, Schwarz SKW. Mechanisms of action of fascial plane blocks: a narrative review. Reg Anesth Pain Med. 2021;46(7):618–628. doi:10.1136/rapm-2020-102305
22. Zhang J, He Y, Wang S, et al. The erector spinae plane block causes only cutaneous sensory loss on ipsilateral posterior thorax: a prospective observational volunteer study. BMC Anesthesiol. 2020;20(1):88. doi:10.1186/s12871-020-01002-0
23. Barrios A, Camelo J, Gomez J, et al. Evaluation of sensory mapping of erector spinae plane block. Pain Phy. 2020;23(3):E289–E296.
24. Weibel S, Jelting Y, Pace NL, et al. Continuous intravenous perioperative lidocaine infusion for postoperative pain and recovery in adults. Cochrane Database Syst Rev. 2018;6:CD009642. doi:10.1002/14651858.CD009642.pub3
25. Masic D, Liang E, Long C, Sterk EJ, Barbas B, Rech MA. Intravenous lidocaine for acute pain: a systematic review. Pharmacotherapy. 2018;38(12):1250–1259. doi:10.1002/phar.2189
26. Atanassoff PG, Ocampo CA, Bande MC, Hartmannsgruber MW, Halaszynski TM. Ropivacaine 0.2% and lidocaine 0.5% for intravenous regional anesthesia in outpatient surgery. Anesthesiology. 2001;95(3):627–631. doi:10.1097/00000542-200109000-00013
27. Asik I, Kocum AI, Goktug A, Turhan KS, Alkis N. Comparison of ropivacaine 0.2% and 0.25% with lidocaine 0.5% for intravenous regional anesthesia. J Clin Anesth. 2009;21(6):401–407. doi:10.1016/j.jclinane.2008.10.011
28. Hessian EC, Evans BE, Woods JA, Taylor DJ, Kinkel E, Bjorksten AR. Plasma ropivacaine concentrations during bilateral transversus abdominis plane infusions. Br J Anaesth. 2013;111(3):488–495. doi:10.1093/bja/aet065
29. Horn CC, Wallisch WJ, Homanics GE, Williams JP. Pathophysiological and neurochemical mechanisms of postoperative nausea and vomiting. Eur J Pharmacol. 2014;722:55–66. doi:10.1016/j.ejphar.2013.10.037
30. Schulz KF, Altman DG, Moher D; CONSORT Group. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. PLoS Med. 2010;7(3):e1000251. doi:10.1371/journal.pmed.1000251
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.