Back to Journals » Journal of Pain Research » Volume 14
Continuous Erector Spinae Plane Block as Postoperative Analgesic Technique for Robotic-Assisted Thoracic Surgery: A Case Series
Authors Cavaleri M, Tigano S ![]() , Nicoletti R, La Rosa V, Terminella A, Cusumano G, Sanfilippo F
, Nicoletti R, La Rosa V, Terminella A, Cusumano G, Sanfilippo F ![]() , Astuto M
, Astuto M
Received 5 May 2021
Accepted for publication 22 July 2021
Published 2 October 2021 Volume 2021:14 Pages 3067—3072
DOI https://doi.org/10.2147/JPR.S308027
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Ellen Soffin
Marco Cavaleri,1 Stefano Tigano,1,2 Roberta Nicoletti,1,2 Valeria La Rosa,1,2 Alberto Terminella,3 Giacomo Cusumano,3 Filippo Sanfilippo,1 Marinella Astuto1,2
1Department of General Surgery and Medical-Surgical Specialties, Section of Anaesthesia and Intensive Care, University Hospital “G. Rodolico”, University of Catania, Catania, 95123, Italy; 2School of Anaesthesia and Intensive Care, University Hospital “G. Rodolico”, University of Catania, Catania, 95123, Italy; 3Thoracic Surgery Unit, Department of General Surgery and Medical-Surgical Specialties, University Hospital “G. Rodolico” - San Marco Hospital, Catania, 95121, Italy
Correspondence: Marco Cavaleri
Department of General Surgery and Medical-Surgical Specialties, Section of Anaesthesia and Intensive Care, University Hospital “G. Rodolico”, University of Catania, Via Santa Sofia 78, Catania, 95123, Italy
Tel +393339369927
Email [email protected]
Introduction: The erector spinae plane block (ESPB) is a recently implemented analgesic technique initially reported for thoracic analgesia and subsequently adopted for both intra- and postoperative pain management. Thoracic surgery is among the most painful surgical procedures, even when conducted with minimally invasive approach. Robotic-assisted thoracic surgery (RATS) challenges the traditional analgesic regimens as one of its aims is to decrease the patient’s length of stay (LOS) whilst achieving optimal postoperative pain management. Furthermore, there is lots of growing evidence on the impact of poorly controlled postoperative pain (PP) on the development of chronic post-surgical pain (CPSP). In these case series, we aim to describe our preliminary experience of postoperative pain management with continuous ESPB in the field of RATS.
Case Series Presentation: In eight consecutive patients undergoing elective RATS procedure, we performed the ESPB after surgery with an initial bolus of local anesthetic followed by catheter insertion for continuous infusion. The infusion of local anesthetic lasted for the first two postoperative days. The effectiveness of the ESPB was evaluated through serial pain assessment with numeric rate scale (NRS) score, both at rest and during movement every 6 hours. Any analgesic rescue drug prescription was reported. We noted that the ESPB strongly reduced the prescription of opioids and of rescue analgesic. In our series, only one patient needed opioids during the first two postoperative days, and no rescue analgesic administration was noted in the remaining cases.
Conclusion: We report a small but promising experience regarding postoperative pain management with continuous ESPB performed after RATS. We implemented the ESPB before surgery. Larger studies on postoperative pain management with continuous regional blocks in thoracic surgery are warranted.
Keywords: pain management, regional block, thoracic surgery, postoperative care
Introduction
Video-assisted thoracoscopic surgery (VATS) has been used for several decades in the treatment of lung and thoracic diseases and offers several advantages over thoracotomies.1,2 In the last decade, robotic-assisted thoracoscopic surgery (RATS) has emerged as a further development of minimally invasive surgery, offering even better visualization with an improved three-dimensional depth perception, thus allowing fine movements and significant freedom of robotic instruments as compared to VATS. Additionally, robotic technique allows precise assessment of lymph node involvement and disease staging.3 RATS procedures challenge the traditional perioperative pain-relieving regimens since one of its goals is to reduce the patient’s length of stay (LOS). Therefore, an optimal pain control should be achieved early in the postoperative period in order to boost recovery and deambulation. Minimally invasive thoracic surgery reduces postoperative pain (PP) as compared to thoracotomies, but patients can still experience significant PP.4 For decades opioids have been the mainstay of pain management in patients undergoing thoracic surgery, recently with the implementation of patient-controlled analgesia (PCA) systems. The enhanced recovery after surgery (ERAS) programs raised concerns about PP management achieved mainly with intravenous medications, both in thoracic and general surgery, highlighting the therapeutic limits and side effects of such a strategy.4 In order to improve the pain management, intravenous and oral pain medications have been combined with regional analgesic techniques such as thoracic epidural blockade and perineural blocks.5 In this context suboptimal pain management and residual PP are associated with worse respiratory dynamics effort and decreased functional residual capacity, thus reducing the ability to cough and clear secretions. Indeed, these PP-related pulmonary complications could result in airway closure, atelectasis, shunting and tissue hypoxemia.4,5 Thoracic surgery, both conducted with open and minimally invasive approach, is considered to be at high risk for development of chronic post-surgical pain (CPSP) which is defined as
Pain persisting for at least 3 months after surgery, different from preoperative pain or pain caused by other conditions such as continuing malignancy or chronic infection should be excluded.6
Regional analgesic blocks (paravertebral, intercostal or erector spinae plane [ESP]) have been increasingly used for multimodal pain management within the last decades and are currently strongly advocated within pain management for thoracic surgery. The implementation of regional nerve block with injection of local anesthetic (LA) greatly improves analgesia and decreases postoperative requirements for opioid medications.5–9 Among the regional analgesic blocks the ESP block (ESPB) is a novel interfascial plane block where LA is injected preferably below the erector spinae muscle. The first description of ESPB dates from the 2016 paper by Forero et al,10 describing it as an innovative analgesic technique for the acute and chronic thoracic pain. Recent studies have shown that this analgesic block can be safely and effectively used both in cardio-thoracic and in spine and chest trauma surgery.11–13 The ESPB is technically simpler as compared to thoracic epidural anesthesia or paravertebral block, and a significant cranial-caudal spread occurs from a single injection point, which is an additional advantage.
Case Series Presentation
We report our case series, enlisted retrospectively and consisting of eight cases who have undergone RATS at our institution (5 atypical pulmonary resection, 2 lobectomy and 1 pleurectomy). The preoperative evaluation of patients scheduled for robotic surgery was similar to those undergoing VATS or open thoracic surgery. All procedures have been performed in lateral decubitus position with axillary rolls and arm boards. All cases were conducted with Xi DaVinci robotic model and approached in a similar way with full robotic technique (without any thoracotomy or divarication of intercostal spaces). Port placement was similar in all procedures and basically placed along the 7th intercostal space.
We standardized the anesthesia protocol for all lung and pleural RATS procedures, given the same anesthesiologist was in charge during all the procedures. General anesthesia was delivered with full monitoring as per European and American guidelines:15 non-invasive blood pressure monitoring until radial artery cannulation was performed for invasive blood pressure monitoring and arterial blood gas sampling; SpO2; ECG; bi-spectral index (BIS) monitoring; TOF (train of four); urinary output; EtCO2; FiO2; peak and plateau pressure; positive end-expiratory pressure. Induction was performed with propofol 2 mg/kg, remifentanil 2.0–4.5 ng/mL (Target Controlled Infusion-Minto model-Plasma Concentration-Alaris Asena Pump®), rocuronium 1.2 mg/kg after confirming the patient could be bag-mask-ventilated. After confirmation from appropriate TOF value, a left-sided double lumen tube was positioned with direct laryngoscopy, and sevoflurane was administered throughout the procedure targeting BIS values of 30–50. Fiberoptic bronchoscopy check was made for the correct positioning of the tube in the left bronchus. All patients received continuous monolateral ESPB and catheter insertion for postoperative analgesia. Before this case series we used a single-shot ESPB for PP management during lung and pleural surgery in a cohort of 5 patients. Although we did not store data for comparison, the overall impression was that single-shot ESPB improved postoperative analgesia during the first 12 to 24 hours. However, PP recurred after this interval of time, despite the use of adjuvant drugs (dexamethasone) with long-acting LA (ropivacaine). In accordance with previous reports of ESPB in rib fractures by Eng and colleagues,16,17 we hypothesized that systemic absorption of LA might be a contributing factor limiting the effectiveness of the ESPB to a shorter than expected duration. Therefore, we changed our practice, adopting the positioning of an ESP catheter in all patients scheduled for lung RATS, allowing us a continuous postoperative administration of LA and thus longer duration of analgesia. The ESPB with catheter insertion was performed immediately at the end of surgery with the patient still in lateral position. Before the anesthesiological preparation an informed consent to ESPB and data collection for research purposes was obtained in all the patients included in our case series; they also consented for the anonymous reporting of this preliminary experience. Ethics approval was provided from the ethical committee Catania 1, “Policlinico ‘G. Rodolico’-San Marco University Hospital” n.106/2021-PO, and the present manuscript complies with the Declaration of Helsinki.
Block Equipment
The ESPB with catheter insertion was performed in all the cases in full asepsis and ultrasound-guided using a high-frequency (10–16 MHz) linear array transducer as it provides a higher-resolution image. The selected transverse processes (TP) were usually detected within 3–4 cm of depth. We adopted an epidural set (Arrow® Epidural Catheterization – FlexTip Plus) with Tuohy needle 19 G because of the high resistance to kinking of its catheter and the high echogenicity of the needle. The selected thoracic level, basically between the T5 and T6, was identified along with the target TP. Given that LA spreads cranially and caudally from the point of injection, those thoracic levels are usually deemed appropriate to cover the surgical dermatomes involved during thoracic surgery. The ultrasound transducer was placed in a longitudinal parasagittal orientation, about 3 cm lateral to the spinous processes, allowing for visualization of adjacent TP in an in-plane approach. After correct TP identification, the echogenic Tuohy needle was inserted with cranial-to-caudal approach to contact the bone shadow of the TP with the tip directed deep to the fascial plane of the erector spinae muscle. The correct location of the needle tip was confirmed by injecting 0.5–1 mL of normal saline 0.9% and observing linear fluid spread lifting the erector spinae muscle from the TP. Once the fascial plane was recognized, a standardized solution of LA, 15 mL of ropivacaine 0.5% + 10 mL of mepivacaine 1% used to hasten the onset, was administered whilst visualizing cranial–caudal spread of the LA. Once the LA administration was accomplished, the catheter was inserted through the Tuohy needle itself and secured with proper dressing. Correct catheter location was confirmed through ultrasound identification below the erector spinae sheet above the TP line. The catheter was dressed with plasters on the skin, and no cases of accidental displacement or removal happened in our case series. The ESP catheter was removed 48 hours after the positioning.
Postoperative Assessment
Before extubation all the patients received an intravenous analgesic dose of morphine (0.15 mg/kg) together with ketorolac (0.5 mg/kg) unless contraindicated; all the patients were positioned in supine decubitus before being awakened in the operatory room according to the early extubation policy for thoracic surgical patients. The ESP catheter was connected to an elastomeric infusion pump (Accufuser® Elastomeric Vygon) set at 5 mL/h and containing a solution of ropivacaine 0.2%. No patients experienced early complications related to the ESPB, and no drug reactions were noted. Our multimodal approach for postoperative analgesia during the first 48 hours included regular paracetamol (1 g IV every 8 hours) with continuous ESP catheter infusion with ropivacaine 0.2%; rescue analgesia was planned with ketorolac 30 mg IV unless contraindicated, otherwise tramadol 100 mg IV was considered. In all the patients our analgesic approach did not include postoperative intravenous opioids in the attempt to boost as much as possible the postoperative recovery and to avoid opioid-related side effects. During the first two postoperative days the effectiveness of the ESPB was evaluated through serial pain assessment with numeric rate scale (NRS) score, both at rest and during movement every 6 hours. Patient characteristics, data on analgesic management and PP are shown in Table 1. Three patients required rescue analgesic doses within the first 24 hours with ketorolac IV. Another patient who underwent a lobectomy required a low dose of morphine infusion, 0.75 mg/h, during the first 12 h of postoperative care in addiction to the LA infusion through ESP catheter. Furthermore no surgical and cardiovascular complications were detected during the whole postoperative stay in this cohort of patients. No postoperative nausea and vomiting (PONV) or any kind of dizziness was reported. All patients were able to complete their postoperative pulmonary rehabilitation on the following day after surgery, being also able to provide their own care (eating, personal cleaning, etc) from postoperative day 2 (Table 1).
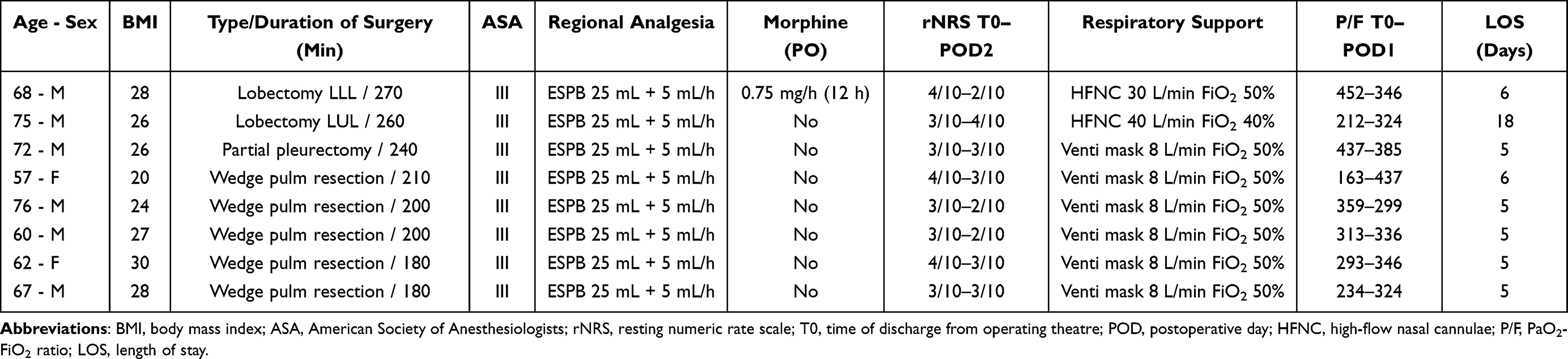 |
Table 1 Characteristics of the Cohort of Patients Undergoing Robotic-Assisted Thoracic Surgery with Postoperative Analgesia Managed with the Erector Spinae Plane Block (ESPB) and Catheter for Continuous Infusion |
Discussion
We report a preliminary experience with the use of continuous postoperative ESPB through LA infusion via catheter positioned at the end of RATS procedures. To the best of our knowledge only one case report of continuous ESPB in RATS has been reported in the literature,18 thus our study represents the first case series data reporting on eight consecutive patients managed with continuous ESPB as analgesic technique in different RATS procedures.
Although the ESPB has been only recently described as an analgesic technique after thoracic surgery and chronic thoracic neuropathic pain,7 it must be considered that it has been used for several other surgical procedures, ranging from thoracic and cardiac surgery, to orthopedic procedures and cesarean section. The ESPB had also been used at different vertebral levels.10–22 A recent trial has proved that the analgesic effect of ESPB after VATS was non-inferior to that of thoracic paravertebral block in the first 24 postoperative hours.19 As compared to this previous work, our RATS case series with ESPB has provided effective postoperative analgesia, longer than 48 hours, within a multimodal pain-relieving program with few opioid needs, thus showing a promising opioid-sparing effect and faster patient recovery, in line with a recent meta-analysis reported by Kendall et al.20 Although originating from a retrospective data collection, our experience with ESPB seems promising, as demonstrated also by overall results of the NRS scores and the good gas exchange profiles as shown in Table 1. Even when an intravenous administration of morphine 0.75 mg/h in addition to ESP catheter infusion was prescribed in a case undergoing RATS lobectomy, the overall patient’s NRS scores were promising. This positive analgesic effect of ESPB technique was positively noted by the surgical équipe. This allowed to path a further step on the performance of ESPB before surgery, thus enabling better intraoperative pain control and potentially reducing the doses of intraoperative opioids.
We believe that this new protocol may also optimize the preemptive effects of regional analgesia on neuropathic components of PP, potentially decreasing the impact of PP on CPSP occurrence. Taking into account the influence of regional analgesic blocks on potential prevention of CPSP occurrence, an increasing emphasis has been recently focused on the mechanisms underlying the transition from acute pain to chronic pain, as well as aggressive prevention and management of PP following thoracic surgery. It is reasonable as well as demonstrated that regional analgesic blocks, and especially the continuous techniques like catheter ESPB, may improve PP management probably reducing those factors, such as overuse of postoperative narcotics or the intensity of acute PP, both factors related to a potential increase of CPSP incidence rate.7,8 However, such a hypothesis is not yet validated, and the lack of well-designed prospective studies on this specific clinical outcome means that no recommendations for its use for this strategy have been made yet.
In recent years fascial plane blocks, with ESPB above all, are increasingly used in many surgical fields as compared to the central neuraxial blocks (ie, epidural analgesia), both as single shot or as catheter for continuous infusion. Such evolution is supported by several advantages offered by this fascial block (ease of performing, analgesic efficacy, low risk of complications). According to cadaveric and contrast studies, it seems that the ESPB anesthetizes the lateral origins of the spinal nerves, including both the dorsal and ventral branches. The mechanism of such combined parietal-visceral analgesic effect is believed to result from the diffusion of the LA anteriorly to the paravertebral ganglions or sympathetic trunks as is the case with the paravertebral block.10–12 Moreover ERAS programs strongly advocate the implementation of loco-regional blocks aiming at reducing the surgical stress response and organ dysfunction, therefore promoting patients’ postoperative recovery. As an emerging and promising technique, the ESPB block has all the aforementioned advantages of the fascial plane blocks suitable for thoracic surgery. Thoracic ESPB has increased acceptance because it is safer than thoracic paravertebral block, with lower complication rates, and it is less difficult to perform relative to thoracic epidural analgesia or thoracic paravertebral block itself, as long as there is adequate ultrasound-guided regional anesthesia training. The block has an excellent safety profile since the local anesthetic injection is distant from the pleura, major blood vessels and spinal cord. While thoracic regional blocks, particularly the ESPB, are increasingly used worldwide, some reports of adequate PP control achieved with the intercostal block using liposomal bupivacaine after VATS thymectomy are coming up, although no further validation of this technique has been provided in other thoracic surgery procedures.23 In this context, it would be interesting to study the effectiveness and replicability of single-shot ESPB using liposomal bupivacaine.
In conclusion, we report a promising preliminary experience regarding PP management after RATS through the positioning of an ESP catheter for continuous LA infusion. Our planned development is the early positioning of ESP catheter before surgery for its intraoperative use in order to reduce also the intraoperative opioid administration.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, agreed to the submitted journal, and agree to be accountable for all aspects of the work.
Funding
The authors declare that this study has received no financial support.
Disclosure
Authors have no conflicts of interest to declare.
References
1. Heller JA, Bhora FY, Heller BJ, Cohen E. Robotic-assisted thoracoscopic lung surgery: anesthetic impact and perioperative experience. Minerva Anestesiol. 2018;84:108–114.
2. Pauli H, Eladawy M, Park J, et al. Anesthesia for robotic thoracic surgery. Ann Cardiothorac Surg. 2019;8(2):263–268. doi:10.21037/acs.2018.12.06
3. Jablons DM. Robot Thoracic Surgery Program. UCSF; 2019.
4. Thompson C, French DG, Costache I. Pain management within an enhanced recovery programs after thoracic surgery. J Thorac Dis. 2018;10(32):3773–3780.
5. Adhikary SD, Pruett A, Forero M, et al. Erector spinae plane block as an alternative to epidural analgesia for post-operative analgesia following video-assisted thoracoscopic surgery: a case study and a literature review on the spread of local anaesthetic in the erector spinae plane. Indian J Anaesth. 2018;62(1):75–78. doi:10.4103/ija.IJA_693_17
6. Macrae WA. Chronic postsurgical pain. In: Crombie IK, editor. Epidemiology of Pain. Seattle: IASP Press; 1999:125–142.
7. Peng Z, Li H, Zhang C, et al. A Retrospective Study of chronic post-surgical pain following thoracic surgery: prevalence, risk factors, incidence of neuropathic component, and impact on quality of life. PLoS One. 2014;9(2):90014. doi:10.1371/journal.pone.0090014
8. Homma T, Doki Y, Yamamoto Y, et al. Risk factors of neuropathic pain after thoracic surgery. J Thorac Dis. 2018;10(5):2898–2907. doi:10.21037/jtd.2018.05.25
9. Butterworth JF, Mackey DC, Wasnick JD. Anesthesia for thoracic surgery. In: Morgan & Mikhail’s Clinical Anesthesiology.
10. Forero M, Adhikary SD, Lopez H, Tsui C, Chin KJ. The erector spinae plane block: a novel analgesic technique in thoracic neuropathic pain. Reg Anesth Pain Med. 2016;41(5):621–627. doi:10.1097/AAP.0000000000000451
11. Jain K, Jaiswal V, Puri A. Erector spinae plane block: relatively new block on horizon with a wide spectrum of application – a case series. Indian J Anaesth. 2018;62(10):809–813.
12. Kot P, Rodriguez P, Granell M, et al. Erector spinae plane block: a narrative review. Korean J Anesthesiol. 2019;72(3):209–220. doi:10.4097/kja.d.19.00012
13. Hamilton DL, Manickam B. Erector spinae plane block for pain relief in rib fractures. Br J Anaesth. 2017;118(3):474–475. doi:10.1093/bja/aex013
14. Standards for Basic Anesthetic Monitoring [webpage on the Internet]. Schaumburg, IL: American Society of Anesthesiologists; 2020. Available from: https://www.asahq.org/standards-and-guidelines/standards-for-basic-anesthetic-monitoring. Accessed September 30, 2021.
15. Hinkelbein J, Lamperti M, Akeson J, et al. ESA and EBA guidelines for procedural sedation and analgesia in adults. Eur J Anaesthesiol. 2018;35(1):6–24. doi:10.1097/EJA.0000000000000683
16. Thiruvenkatarajan V, Cruz Eng H, Adhikary SD, et al. An update on regional analgesia for rib fractures. Curr Opin Anaesthesiol. 2018;31(5):601–607. doi:10.1097/ACO.0000000000000637
17. Eng HC, Chin KJ, Adhikary SD. How I do it: erector spinae block for rib fractures: the Penn state health experience. ASRA News. 2018;18:116–120
18. Ceraolo E, Balzani E, Rosboch GL, et al. Continuous erector spinae plane block for postoperative analgesia in robotic lung lobectomy: a case report. Tumori. 2021:030089162110058. doi:10.1177/03008916211005839
19. Pinto C. Comparison of ultrasound-guided erector spinae plane block and thoracic paravertebral block for postoperative analgesia after video-assisted thoracic surgery: a randomized controlled non-inferiority clinical trial. Reg Anesth Pain Med. 2020;45(1):10–15. doi:10.1136/rapm-2019-100827
20. Kendall M, Alves L, Traill LL, et al. The effect of ultrasound-guided erector spinae plane block on postsurgical pain: a meta-analysis of randomized controlled trials. BMC Anesthesiol. 2020;20(1):99. doi:10.1186/s12871-020-01016-8
21. Tulgar S, Senturk O. Ultrasound guided erector spinae plane block at L-4 transverse process level provides effective postoperative analgesia for total hip arthroplasty. J Clin Anesth. 2018;44:68.
22. Altinpulluk EY, Simón DG, Fajardo-Pérez M. Erector spinae plane block for analgesia after lower segment caesarean section: case report. Rev Esp Anestesiol Reanim. 2018;65:284–286.
23. Jackson AS, Devulapalli C, Lowe A, et al. Left video-assisted thoracic surgery thymectomy. J Vis Surg. 2017;3:47. doi:10.21037/jovs.2017.02.13
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.