Back to Journals » Open Access Rheumatology: Research and Reviews » Volume 13
Contentious Issues in Gout Management: The Story so Far
Authors Talaat M, Park K, Schlesinger N ![]()
Received 23 February 2021
Accepted for publication 25 March 2021
Published 12 May 2021 Volume 2021:13 Pages 111—122
DOI https://doi.org/10.2147/OARRR.S282631
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Chuan-Ju Liu
Mohamed Talaat,1 Kyle Park,1 Naomi Schlesinger2
1Rutgers-Robert Wood Johnson Medical School, New Brunswick, NJ, USA; 2Division of Rheumatology, Department of Medicine, Rutgers Robert Wood Johnson Medical School, New Brunswick, NJ, 08903-0019, USA
Correspondence: Naomi Schlesinger
Department of Medicine, Division of Rheumatology, Rutgers Robert Wood Johnson Medical School, Medical Education Building, Room 468, New Brunswick, NJ, 08903-0019, USA
Email [email protected]
Abstract: Gout is the most common inflammatory arthritis worldwide. Although gout has been known for antiquity, many challenges still exist in gout management. It is vital to view gout as a chronic disease and not just treat the acute flare. There is a perception of gout as an acute disease requiring treatment only for acute flares. However, to combat the disease, chronic urate-lowering therapy, reducing the serum urate levels to below the saturation threshold of 6.8 mg/dL, and chronic anti-inflammatory prophylaxis, especially during urate-lowering therapy initiation, are needed. In this manuscript, we discuss some of the contentious issues in gout management. These include the timing of urate-lowering therapy initiation, which urate-lowering therapy to chose, should comorbidities influence our treatment, using genetic determinants, and patient perspectives to drive treatment and differences between gout treatment the American College of Physicians and Rheumatology guidelines for gout management: driving care.
Keywords: gout, treatment, controversies
Introduction
Gout is the most common inflammatory arthritis worldwide. The incidence of gout is increasing and represents a major health burden. The disease is known from antiquity, however, there are many knowledge gaps despite years of clinical experience. Recently, after Mr. Paul Manafort, Donald Trump’s disgraced former chairman of the 2016 presidential campaign, was convicted in 2018 of financial fraud, he rolled into court in a wheelchair with his right foot wrapped in a bandage. He was not wearing a shoe. The Newspapers made the speculation that this was possibly from an acute gout flare. It was reported that his severe gout was caused by gluttony, anxiety, depression, and diabetes.1 However, Mr. Manafort’s gout is not necessarily caused by gluttony, as suggested by the Newspaper article. The idea that gout might be self-inflicted is a way to give the pain meaning, as a path to redemption, since for centuries, the sacrifice of earthly pleasures was the only relief for gout patients. The New York Times article stated that what holds his symptoms at bay in a gout patient is a daily dose of allopurinol, a urate-lowering drug.2 Is it that simple?
Although gout has been known for antiquity, many challenges still exist in gout management. In this manuscript, we will be discussing some of the contentious issues in gout management.
Acute Gout Flare Treatment
Acute gout flares are characterized by acute onset of severe pain, often occurring late at night or early morning. Early in the disease, the flares are usually monoarticular, especially in men, and as the disease progresses, flares often become polyarticular. Flares can involve any joint but most commonly involve the lower extremity joints. Treatment of acute flares should be initiated as early as possible. The earlier treatment is initiated, the more rapid the response. Treatment should be continued for the duration of the flare (days to weeks).3
Acute gout flares are caused by an inflammatory response to monosodium urate (MSU) crystals. This is mediated mainly by macrophages and neutrophils. The inflammatory response includes recognition of MSU crystals by Toll-like receptors (TLR) 2 and TLR 4. The TLR adaptor protein Myeloid differentiation primary response 88 (MyD88) promotes ingestion of the MSU crystals by phagocytes. MyD88 transduces activation of the transcription factor nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB) and the expression of other pro-inflammatory mediators.4 In addition, the intracellular NACHT-LRR-PYD-containing protein (NLRP3) inflammasome protein complex is activated by ingested MSU crystals in phagocytes leading to caspase-1 activation and the maturation and secretion of the active soluble interleukin (IL)-1β from macrophages.5 Il-1 has emerged as a pivotal cytokine in acute gout.
The main anti-inflammatory drugs used in the USA for gouty inflammation are NSAIDs, corticosteroids, colchicine, and IL-1 inhibitors.6
NSAIDs
Any NSAID can be used. NSAID selection should be based on the patient’s initial response, adverse events, and comorbidities, especially cardiovascular and renal. There is lower risk of bleeding with the cyclooxygenase (COX)-2 selective drugs, especially in patients with thrombocytopenia.
Corticosteroids
Acute flares usually require moderate doses of corticosteroids (20–40 mg daily for several days followed by a lower dose for several days). Corticosteroids and NSAIDs are comparable in regards to efficacy for treating acute gout flares.7 However, in monoarticular gout flares, intra-articular corticosteroids are frequently used as first line treatment.6
Colchicine
There are better ways than colchicine to treat gout flares in most patients. Colchicine should be administered in a total dose on day 1 not to exceed 1.8 mg, either taken as 0.6 mg three times on the first day or by taking 1.2 mg for the first dose followed by 0.6 mg an hour later; on subsequent days, colchicine is taken once or twice daily until flare resolution. In some countries, colchicine is available as a 0.5 mg rather than as a 0.6 mg pill. However, most patients treated with this dose, needed additional anti-inflammatory medications for pain relief.8
IL-1 Inhibitors
IL-1β, a proinflammatory cytokine, plays a key role in mediating gouty inflammation.9
Anakinra is a recombinant human IL-1 receptor antagonist (IL-1Ra). Due to its short plasma half-life of approximately 4–6 hours following subcutaneous administration, anakinra is administered daily. Anakinra anaGO Acute gout Phase 2 study compared intramuscular triamcinolone (TA) 40mg once versus subcutaneous (sc) Anakinra 100 or 200 mg once daily for 5 days. It resulted in pain reduction in most affected joints with anakinra by approximately 50%. However, no statistically significant difference was observed between TA and Anakinra.10 Canakinumab, on the other hand, a fully human anti-IL-1β monoclonal antibody with a long plasma half-life (3–4 weeks) provided potent and durable suppression of inflammation, with reduced clinical signs of inflammation by 3 days post-dose. Canakinumab was associated with significantly less pain from 24 hours post-dose (p<0.01).11
Although the manufacturer of anakinra has not sought FDA approval for a gout indication, the drug is utilized by rheumatologists, particularly in hospitalized patients with co-morbidities. Canakinumab, approved in Europe for acute gout was rejected by the FDA owing to concerns about the long half-life of the drug and adverse events. Thus, IL-1inhibitors have a role as anti-inflammatory drugs in refractory gout or for patients who are unable to tolerate conventional therapy, such as NSAIDs, colchicine, or corticosteroids, for acute flares.
Standard anti-inflammatory therapies are inappropriate for an increasing number of patients with gout due to underlying comorbidities. A reduced dose may be required in patients with chronic kidney disease (CKD), hepatic dysfunction, or potential drug interactions. Since colchicine is metabolized by cytochrome p450 3A4 (CYP3A4) and is a substrate for P glycoprotein, colchicine should be avoided, or dose decreased in patients with gout who are undergoing treatment with potent inhibitors of CYP3A4 or P glycoprotein, or drugs that inhibit the membrane P-glycoprotein (P-gp) drug efflux pump, including clarithromycin and ketoconazole, since this may result in dangerously increased colchicine drug levels.
Combination therapy such as colchicine plus either an NSAID or a corticosteroid is recommended in patients with severe gout, despite little or no evidence to support such treatment.
Based on the efficacy demonstrated in several randomized controlled trials, IL-1 inhibitors are recommended in patients with frequent flares who have contraindications to colchicine, NSAIDs, and corticosteroids. However, they are mainly indicated in patients who are refractory to standard treatment.
Urate-Lowering Therapy (ULT)
Serum urate (SU) levels of 6.8 mg/dL and higher exceed the saturation of urate in solution and promote MSU crystal deposition. To permanently resolve the underlying stimulus for acute flares and joint damage, the SU must be lowered below 6 mg/dl (or lower in some patients).12
Timing of ULT Initiation is Controversial
There is no consensus regarding the timing of ULT initiation.13–15 On one end of the spectrum, some physicians believe that the first gout flare is preceded by years of silent MSU crystal deposition and hence would be inclined to start ULT after the first flare. They suggest that delayed treatment might allow further MSU crystal deposition and thus promote inflammation and joint destruction. Early initiation of ULT in patients with underlying comorbidities has also been suggested, but further research is needed to provide supporting evidence. On the opposite side of the spectrum, some physicians believe that for a patient to develop tophi and severe symptomatic gout, it would usually be preceded by years of recurrent flares, since it has been well demonstrated that patients with asymptomatic hyperuricemia have MSU crystal deposits.16–19
The 2020 American College of Rheumatology (ACR) recommendations support starting ULT if there are two or more flares in the previous year, evidence of tophi, or evidence of radiographic damage attributed to gout and conditionally recommend starting ULT for CKD stage 3, SU > 9mg/dL, or urolithiasis.12 Will other societies support this?
Can We Start ULT During an Acute Flare?
It has been believed that initiating ULT during acute gout flare can worsen or prolong gout flares. In addition, patients starting ULT are at risk of developing further flares. Some suggest that ULT be started after an acute flare has completely subsided, usually 14 days after the start of a gout flare. Others suggest that initiating ULT during an acute flare may have the advantage of improved compliance, decreasing healthcare visits, and overutilization. A small randomized controlled trial (RCT) comparing initiating Allopurinol 100 mg for days 1–14 days followed by Allopurinol 200 mg days 15–28 versus placebo for acute flare concluded that allopurinol did not prolong or exacerbate the acute flares. Patients received colchicine or meloxicam for their flare.20 Another small RCT compared allopurinol 300 mg versus placebo for the first 10-days, followed by allopurinol 300 mg starting day 11 to day 30 for both groups concluded that in the 30 days of observation, allopurinol initiation caused no worsening in gout flares.13 Patients received colchicine and NSAIDs for prophylaxis. Yet another study, a retrospective study found that initiation of ULT during acute flares led to more frequent flares in the first 12-weeks following the initial flare.14 Thus, initiating ULT during acute flares needs further study.
What would the outcome be if patients received a different ULT such as Febuxostat? Would allopurinol prove superior when given during a flare due to its known anti-inflammatory and analgesic properties?15 It is worth noting that in the first RCT, patients received incremental doses of Allopurinol 100 mg daily for the first two weeks followed by 200 mg daily for the second two-weeks, which might be a safer approach with less likelihood for worsening or prolonging flare. Still, it might defeat the purpose of decreasing healthcare visits and cost. In the second RCT, patients received Allopurinol 300 mg daily, but they also received dual prophylaxis with Colchicine and NSAIDs.
Allopurinol versus Febuxostat: A Comparison
Since its Food and Drug Administration (FDA) approval in 1966, allopurinol has been the drug of choice for treating hyperuricemia in gout patients. It was not until 2009 that another ULT, Febuxostat, another xanthine oxidase inhibitor, was approved for use in the USA becoming a mainstay ULT alongside allopurinol.21 However, in 2019, the FDA issued a public safety alert due to a reported increased risk of death in febuxostat treated patients than allopurinol treated patients, leading to a Black Boxed Warning for febuxostat.22 In addition, lesinurad, a uricosuric drug, was taken off the US market in February 2019. One year later, in 2010, a pegylated recombinant uricase, pegloticase, was approved by the FDA for the treatment of hyperuricemia in patients with gout who have failed to normalize SU levels (<6 mg/dL) or continue to have signs and symptoms of gout on standard oral ULT.23 Unlike other available ULT, pegloticase is unique in that it catalyzes the oxidation of uric acid into the more water-soluble allantoin, allowing renal excretion.23 Thus, the options for urate-lowering in gout are limited.
Febuxostat is an inhibitor of xanthine oxidase (XO) but, unlike allopurinol and its metabolites, febuxostat is minimally excreted through the kidneys.22 The CARES trial enrolled only those with a significant history of cardiovascular disease (CVD). The Composite was not significantly different. However, the risk of death from CVD was 34% higher with febuxostat than allopurinol and 22% higher for deaths from any cause.22 Febuxostat increases death risk in people with preexisting major cardiovascular diseases, and should allopurinol remain the first choice ULT or not?
The Febuxostat versus Allopurinol Streamlined Trial (FAST) compared allopurinol and febuxostat’s cardiovascular safety in over 6000 European gout patients. Age ≥ 60.24 Enrolled gout patients were on 6-years of allopurinol (dose optimized in all patients to achieve a SU <6 mg/dL). Patients with ≥1 cardiovascular (CV) risk factor and/or severe heart failure were excluded. Patients were then randomized to- allopurinol versus febuxostat 80 mg/d (could be upped to 120 mg/(dose not approved by the FDA) if the SU was >6 mg/dL. The primary outcome was a composite of hospitalization for non-fatal MI or biomarker-positive acute coronary syndrome, non-fatal stroke, or CVS death. Only 33% of patients had established CVD and more patients in the febuxostat were on colchicine. Febuxostat was found non-inferior to allopurinol with respect to the primary outcome, and its long-term use is not associated with an increased risk of death. The FAST trial may provide for a higher comfort level for rheumatologists using febuxostat. However, only a third of patients in the FAST trial had CVD, whereas all the CARES trial patients had CVD. Will regulators review the febuxostat FDA the black-box warning?
Is the Use of Benzbromarone Indicated for the Treatment of Gout?
Benzbromarone, a powerful uricosuric drug, was first introduced to the market in the 1970s. Benzbromarone at standard daily doses of 100 mg was more efficacious than allopurinol 300 mg daily in lowering SU in multiple trials.25–27 Specifically, for uric acid underexcretors, benzbromarone was shown to be more efficacious than allopurinol.25,28 In patients with CKD where there is a question regarding allopurinol dose escalation and where probenecid’s uricosuric activity is reduced, benzbromarone retained its uricosuric activity and when did not a dose increase to 150–200 mg per day improved its hypouricemic effect.29–32
However, despite its efficacy, cases of hepatotoxicity have emerged. In 1994 a case report of a woman in the Netherlands, who developed acute hepatitis, was attributed to benzbromarone. This was confirmed when she was rechallenged with benzobramone two years later.33 In the late 1990s and early 2000s in Japan, several cases of fulminant liver failure leading to death were attributed to benzbromarone.34–36 Eventually, the drug was withdrawn from the market by Sanofi-Synthélabo in 2003 after reports of severe hepatotoxicity. The drug is still marketed in some European countries and is not available in the US.
It’s worth noting that only one case (the Dutch lady) showed clear causation between benzbromarone and hepatotoxicity. It is estimated that, in Europe, if all reported cases of hepatotoxicity were attributed to benzbromarone, then the risk would be 1 in 17,000. This risk is likely to be higher in Japan.
It was suggested that a slow dose increase with close monitoring of liver function could reduce the risk of hepatotoxicity. Given the paucity of ULT in our armamentarium and the fact that benzbromarone is an effective drug, it is possible that the decision to withdraw the drug from the market was not in the best interest of gout patients.37
What is the Most Appropriate Urate-Lowering Therapy in Patients with Chronic Kidney Disease?
For decades allopurinol has been recommended as a first-line ULT. However, the conventional dose of 300 mg per day is insufficient in over 50% of patients to achieve the target SU.38 The allopurinol dose can be gradually increased to above the conventional renal dose in people with CKD without allopurinol hypersensitivity syndrome.39
Several studies have been performed looking at ULT dosing in gout patients with CKD. In one study, patients with advanced CKD Estimated glomerular filtration rate (eGFR) < 30 mL/min/1.73 m2), refractory to allopurinol responded to febuxostat, indicated by reducing SU and a decrease in the decline in GFR.40 In another study, hyperuricemic patients with CKD stages 3–5 found febuxostat superior to allopurinol at Lowering SU. The decrement of SU was suspected of causing the slower progression of CKD.41 A randomized trial compared febuxostat and placebo effects on renal outcomes in patients with stage 3 CKD and asymptomatic hyperuricemia showed a significant benefit of febuxostat in patients without proteinuria and in those with higher baseline renal function.42 Thus, febuxostat may be superior to allopurinol in protecting renal function in patients with CKD.43
However, in yet another study, allopurinol was associated with a lower incidence of renal disease in older hyperuricemic patients than febuxostat.44 Further studies are needed to evaluate the best ULT in gout patients with CKD.
SU Levels Might Not Be Sufficient to Predict Flares
The literature on SU levels and the probability of flares in gout are inconsistent. On the one hand, SU level is a strong predictor of gout. The prevalence of gout flares correlated with an average SU but not the SU level at just one time in one study.45 SU levels measured at one time may not precisely reflect the urate load. A retrospective study found significantly fewer flares in patients on allopurinol with lower SU. Levels than with higher SU Levels.46 Aggregate clinical trial data did not confirm the association between SU and gout flares.47 Thus, SU levels might not be sufficient to predict flares. However, in some observational studies, with longer duration, the SU < 6mg/dL was associated with reduced gout flares.47
Use of Prophylaxis When Starting ULT
The flare risk is most significant when urate-lowering is rapid, independent of the ULT chosen. It has been suggested that a slow up-titration of ULT with anti-inflammatory prophylaxis is recommended.48 This approach may delay achieving the SU target of 6mg/dL, but the risk of flares is reduced and may lead to better patient compliance.49 On the other hand, the dramatic SU lowering by pegloticase is associated with a high flare rate due to a marked SU reduction.23 However, it is followed by the cessation of flares after several months of treatment.
The choice of anti-inflammatory prophylaxis should be based on patient factors. The most commonly used drugs are low-dose oral colchicine (0.5mg or 0.6mg once or twice daily), NSAIDs, and IL-1 inhibitors (second line).50–52 A study of 1167 gout patients found only 37% of patients on anti-inflammatory prophylaxis. Most were on colchicine.50 Another study, the administrative database (IQVIA™ Health Plan Claims Database), found that the proportion of patients receiving prophylaxis with ULT initiation is deficient (9.4%).52
How long should prophylaxis be prescribed? For at least 3–6 months, continued prevention as needed if the patient continues to experience flares. [12] Many patients were on prophylaxis for greater than one year.50 Further studies are required to assess the appropriate duration of the prophylaxis cohort (p < 0.001).52
Using Genetic Testing from Theory to Reality
An area of research with the potential to change the field of gout is understanding the underlying genetics. This may lead to personalized treatment in gout patients. However, the knowledge gap regarding the effect of genetic testing on clinical outcomes contributes to this approach not being part of the standard of care.
Numerous genetic markers associated with hyperuricemia and gout were identified in genome-wide association studies (GWAS). Many of those associated with gout are related to urate transporters and the NLRP3 inflammatory process.53,54
One of the most important susceptibility loci for hyperuricemia and gout is the adenosine triphosphate binding cassette subfamily G (ABCG2) located on chromosome 4q. ABCG2 is a urate-transporter gene involved mainly in urate excretion. ABCG2 variants have been associated with earlier onset of gout, development of tophi, and inadequate response to allopurinol.55 The predictive role of the ABCG2 variants on gout susceptibility varies with gender and ethnicity, as seen in a meta-analysis of 7 case-controlled studies.56 Identifying gene variants may be used in the future to counsel patients of their genetic risk, which may factor in the decision to treat a patient with ULT earlier. However, there is currently not enough data to support the clinical use of the ABCG2 gene variant.
One genetic marker currently used clinically is the human leukocyte antigen (HLA)-B*58:01. HLA-B*58:01 is associated with an increased risk of developing allopurinol hypersensitivity syndrome (AHS). The prevalence of HLA-B*58:01 varies with ethnicity and geographical location. The prevalence of HLA B*5801 in the US is 0.7% in Caucasians, 3.8% in African Americans, and 7.4% in Asians.57 This has led to studies evaluating HLA B*5801 testing’s cost-effectiveness before initiating allopurinol in different populations with varying results. In the US, a study found that HLA-B*58:01 testing was cost-effective in Asians and African Americans but not Caucasians or Hispanics.58 This led the ACR in 2020 to recommend screening for HLA-B*58:01 in the Southeast Asian and African American populations.12 In studies in non-American populations, including Taiwanese and South Koreans, genetic testing was cost-effective, while in Malaysians, Singaporeans, and British, the testing was not effective.59–63 However, in the UK study, the authors predict that the testing will become cost-effective when cheaper genotyping is available. Thus, the clinical utility of HLA-B*58:01 screening may be more expansive in the future. Large-scale prospective studies are needed to turn the use of genetics in gout treatment from theory to reality.
Patient Perspectives
Patient perspectives on clinical care of gout patients is a topic that requires more consideration. Treatment of patients is often seen as one-sided, with physicians deciding on the treatment plan. Patient adherence to the prescribed treatment is labeled as “compliant” or “non-compliant.” However, patient perspectives on gout diagnosis, efficacy and safety of gout medications, and nonpharmacological gout management can affect patients’ rapport with physicians, adherence to treatment, and patient outcomes.64
There are many aspects of gout that are underrecognized. One study found that the effect of gout on physical and emotional intimacy in relationships was a significant concern among patients.65 Another found that the impact of gout on quality of life differs among different races and genders.66 During the COVID-19 pandemic, up to 37% of gout patients reported difficulty in healthcare access, and 15% reported severe psychological distress.67
The awareness of the importance of patient perspectives on gout treatment may be growing. The 2020 ACR guidelines for gout treatment stemmed, in part, from gout patient perspectives.68 Patients placed a high value on reducing pain from gout flares and gout deformities due to tophi. This discussion led to the adaptation of more active and aggressive gout treatment, such as early initiation of ULT. The inclusion of patient perspectives on the treatment of gout in national guidelines is encouraging.
Choosing a Drug That is Good for Gout and Associated Comorbidities
Comorbidities are more common in gout patients than in the general population. Gout patients have an average of 4 four associated comorbidities. Addressing comorbidities in gout patients while treating their gout is greatly advantageous. This may help personalized treatments available to some our gout patients, as highlighted below.
Colchicine and Coronary Artery Disease (CAD)
Comorbidities are more common in gout patients than in the general population. Gout patients have an average of four associated comorbidities. Addressing comorbidities in gout patients while treating their gout is advantageous. This may help personalized treatments, as highlighted below.
Colchicine and Coronary Artery Disease (CAD)
Colchicine has been used in the treatment of gout for centuries.69 It blocks microtubule spindle formation, which leads to decreased cytokine production, downregulating neutrophil chemotaxis, and hinders the inflammasome function.
Inflammation-mediated activation of neutrophils plays a role in coronary artery disease (CAD). Given colchicine’s effects on neutrophils and their role in atherogenesis, several studies have looked at colchicine and its possible role in CAD. A retrospective, cross-sectional study of patients with gout compared those who received colchicine (n = 576) and those not on colchicine (n = 712) and evaluated the incidence of Myocardial infarction (MI).70 MIs occurred in 1.2% of patients in the colchicine arm and 2.6% in the arm, not on colchicine (p=0.03). Using data from EMR linked with a Medicare claims database, another cohort study compared gout patients who received colchicine versus those not on colchicine and followed patients for CV events.71 Colchicine use was associated with a 49% lower risk (0.30 to 0.88) in the primary CV outcome and a 73% reduction in all-cause mortality (0.35 to 0.85, p=0.007).
The LoDoCo (Low-Dose Colchicine) trial was a prospective, randomized, observer-blinded endpoint trial. It enrolled patients with stable CAD who were already on aspirin and/or clopidogrel and statins and randomized them to either receive colchicine 0.5 mg daily or no colchicine. CV events were followed in these patients for three years. The primary outcome (CV events) occurred in 5.3% of patients who received colchicine and in 16.0% of patients assigned no colchicine (p < 0.001).72 A recent large, randomized double-blinded placebo-controlled trial enrolled 4745 patients- the Colchicine Cardiovascular Outcomes Trial (COLCOT) enrolled patients with recent MIs (within 30 days) and randomized them to either receive colchicine 0.5 mg daily or placebo. Patients were followed for the occurrence of CV events for a median of 22.6 months. The primary efficacy endpoint occurred in 5.5% of the colchicine treated group versus 7.1% of those in the placebo group (p=0.02).73 Thus, low-dose colchicine (0.5 mg once daily) may play a role in decreasing CV events.
Sodium-Glucose Cotransporter-2 (SGLT-2) Inhibitors and Type 2 Diabetes
Sodium-glucose cotransporter-2 (SGLT-2) inhibitors are a class of medicine used to lower blood glucose levels in people with type 2 diabetes. SGLT-2 inhibitors increase uricosuria; however, their exact mechanism has not been fully understood. SGLT-2 inhibitors decrease SU by approximately (0.60–0.75 mg/dL) in people with normal u SU levels (3.3–6.7 mg/dl).74 In a large, propensity-matched study, using a nationwide commercial insurance database, adult patients with type 2 diabetes who were newly prescribed a sodium-glucose cotransporter-2 (SGLT-2) inhibitor had a lower rate of incident gout than those newly prescribed a glucagon-like peptide-1 (GLP-1) receptor agonist. SGLT2 inhibitors reduced by 36% the odds of developing gout. Future studies are needed to confirm these findings, and if replicated, SGLT2 inhibitors might be an effective class of medication for the prevention of gout for patients with diabetes.75
Differences Between the American College of Physicians (ACP) and Rheumatology Guidelines for Gout Management (Table 1)
Given the lack of good management of gout at the point of care,12,76,77 using gout treatment guidelines may help educate the community of Rheumatologists as well as non-Rheumatologists who are often the first medical contacts for gout patients. There is a disagreement between the ACP guidelines and the rheumatologic ACR and European League Against Rheumatism (EULAR) guidelines on gout treatment. Rheumatologists view gout as a chronic inflammatory, metabolic disease leading to acute flares, while the ACP guidelines suggest that treating the acute gout flare is most important. The Rheumatology associations recommend use of ULT and monitoring the SU, and lowering to a SU target of 6mg/dL while in contrast, the ACP does not provide a clear recommendation for (ULT for patients with frequent, recurrent flares or those with tophi, nor does it recommend monitoring SU levels of patients prescribed ULT. These different outlooks on the disease lead to different sets of recommendations (Table 1)
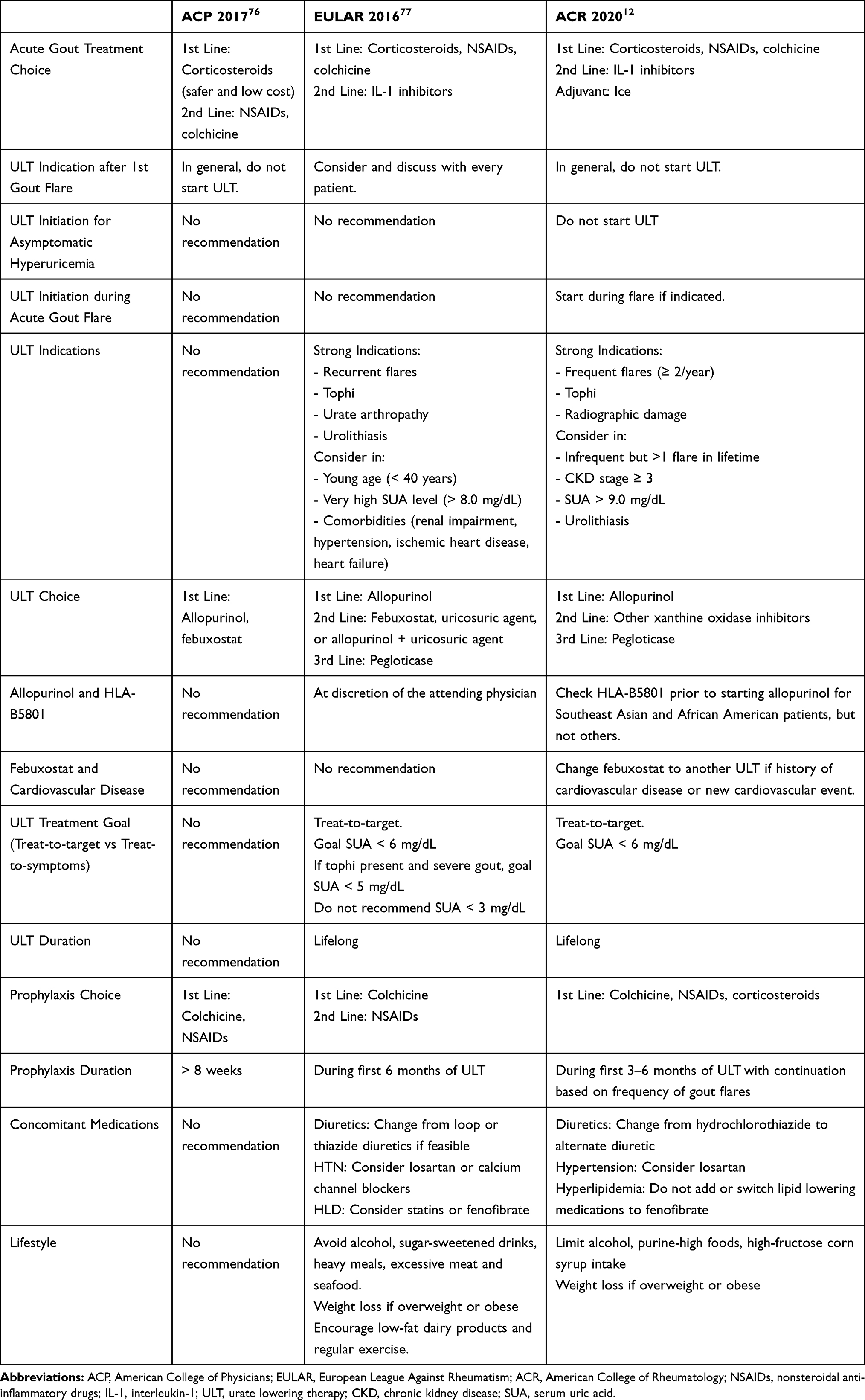 |
Table 1 Comparison of Rheumatology and Primary Care Recommendations/Guidelines |
Discussion
Gout continues to be commonly undertreated and mistreated. Lack of patient and provider education about gout management, the different outlooks of primary care publications, such as the ACP 2016 gout guidelines, which question the treat-to-target strategy advocated by rheumatology societies, failure to treat with ULT, failure to treat to target, underdosing, and contraindications (or perceived contraindications) to available therapies, all lead to a failure to achieve SU target and remission in many patients.
More therapeutic options are needed. The oral drugs currently used to treat acute gout flares may require caution in the setting of comorbidities commonly associated with gout. The amelioration of gouty inflammation using IL-1-inhibitors, and drugs directed at NLRP3 inflammasome activation or function, are an exciting example of biological understanding leading to targeted therapeutics. Therefore, more specific anti-inflammatory drugs may effectively treat and prevent acute flares without affecting co-existing comorbidities, such as diabetes, hypertension, and CKD.
In some patients, particularly in patients with more severe gout and/or higher SU levels—currently available treatments may be limited in their ability to achieve the SU target of 5–6mg/dL. More effective and rapidly acting ULT that would allow patients to achieve the SU target of 6mg/dL may decrease overall patient morbidity and healthcare costs. Dual ULT/anti-inflammatory drugs may simplify drug regimens and improve compliance.
It is vital to view gout as a chronic disease and not just treat the acute flare. There is a perception of gout as an acute disease requiring treatment only for acute flares. However, to combat the disease, chronic ULT, reducing SU levels to below the saturation threshold (6.8 mg/dL), and chronic anti-inflammatory prophylaxis, especially during ULT initiation, are needed.
In conclusion, the treatment of gout is riddled with contentious issues. Evidence-based research is needed to direct gout treatment. Studies need to compare the efficacy of anti-inflammatory treatment options for acute gout; develop personalized treatments based on the severity of flares and gout-associated comorbidities; explore combination treatments for acute and chronic gout; determine the optimal prophylaxis drugs; evaluate patient perspectives; investigate the use of genetic data, imaging modalities, and biomarkers to improve our understanding of gout and develop new treatment strategies.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
No funding was received for the writing of this manuscript.
Disclosure
MT: no conflicts of interest.
KP: no conflicts of interest.
NS: Research grant funding from AMGEN and consulting fees Horizon Therapeutics, IFM Therapeutics, Johnson and Johnson .
References
1. Brown R Manafort suffering depression, anxiety, gout in jail: lawyers. [cited February 17, 2021]. Available from: https://nypost.com/2019/01/08/manafort-suffering-depression-anxiety-gout-in-jail-lawyers/.
2. Mishan L Once the disease of gluttonous aristocrats, gout is now tormenting the masses; 2020 [cited February 17, 2021]. Available from: https://www.nytimes.com/2020/11/13/t-magazine/gout-tormenting-masses.html.
3. Schlesinger N. Treatment of acute gout. Rheum Dis Clin North Am. 2014;40(2):329–341. doi:10.1016/j.rdc.2014.01.008
4. Cronstein BN, Terkeltaub R. The inflammatory process of gout and its treatment. Arthritis Res Ther. 2006;8 Suppl 1(Suppl1):S3. doi:10.1186/ar1908
5. Martinon F, Pétrilli V, Mayor A, et al. Gout-associated uric acid crystals activate the NALP3 inflammasome. Nature. 2006;440(7081):237–241. doi:10.1038/nature04516
6. Schlesinger N. Difficult-to-treat gouty arthritis A disease warranting better management. Drugs. 2011;71(11):1413–1439. doi:10.2165/11592290-000000000-00000
7. Rainer TH, Cheng CH, Janssens HJEM, et al. Oral prednisolone in the treatment of acute Gout: a Pragmatic, Multicenter, Double-Blind, Randomized Trial. Ann Intern Med. 2016;164(7):464–471. doi:10.7326/M14-2070
8. Terkeltaub RA, Furst DE, Bennett K, et al. High versus low dosing of oral colchicine for early acute gout flare: twenty-four-hour outcome of the first multicenter, randomized, double-blind, placebo-controlled, parallel-group, dose-comparison colchicine study. Arthritis Rheum. 2010;62(4):1060–1068. doi:10.1002/art.27327
9. Schlesinger N. Anti-interleukin-1 therapy in the management of Gout. Curr Rheumatol Rep. 2014;16(2):398. doi:10.1007/s11926-013-0398-z
10. Saag K, So A, Khanna P, et al. THU0409 A randomized, Phase 2 study evaluating the efficacy and safety of ANAKINRA in difficult-to-treat acute Gouty Arthritis: THE Anago Study. Ann Rheum Dis. 2020;79(Suppl 1):442. doi:10.1136/annrheumdis-2020-eular.3766
11. Schlesinger N, Alten RE, Bardin T, et al. Canakinumab for acute gouty arthritis in patients with limited treatment options: results from two randomised, multicentre, active-controlled, double-blind trials and their initial extensions. Ann Rheum Dis. 2012;71(11):1839–1848. doi:10.1136/annrheumdis-2011-200908
12. FitzGerald JD, Dalbeth N, Mikuls T, et al. 2020 American College of Rheumatology Guideline for the Management of Gout. Arthritis Care Res (Hoboken). 2020;72(6):744–760. doi:10.1002/acr.24180
13. Taylor TH, Mecchella JN, Larson RJ, et al. Initiation of allopurinol at first medical contact for acute attacks of gout: a randomized clinical trial. Am J Med. 2012;125(11):1126–1134. e7. doi:10.1016/j.amjmed.2012.05.025
14. Feng X, Li Y, Gao W. Significance of the initiation time of urate-lowering therapy in gout patients: a retrospective research. Joint Bone Spine. 2015;82(6):428–431. doi:10.1016/j.jbspin.2015.02.021
15. Schlesinger N, Brunetti L. Beyond urate lowering: analgesic and anti-inflammatory properties of allopurinol. Semin Arthritis Rheum. 2020;50(3):444–450. doi:10.1016/j.semarthrit.2019.11.009
16. De Miguel E, Puig JG, Castillo C, et al. Diagnosis of gout in patients with asymptomatic hyperuricaemia: a pilot ultrasound study. Ann Rheum Dis. 2012;71(1):157–158. doi:10.1136/ard.2011.154997
17. Dalbeth N, House ME, Aati O, et al. Urate crystal deposition in asymptomatic hyperuricaemia and symptomatic gout: a dual energy CT study. Ann Rheum Dis. 2015;74(5):908–911. doi:10.1136/annrheumdis-2014-206397
18. Andrés M, Quintanilla M-A, Sivera F, et al. Silent monosodium urate crystal deposits are associated with severe coronary calcification in asymptomatic hyperuricemia: an Exploratory Study. Arthritis Rheumatol. 2016;68(6):1531–1539. doi:10.1002/art.39581
19. Abhishek A, Courtney P, Jenkins W, et al. Brief report: monosodium urate monohydrate crystal deposits are common in asymptomatic sons of patients with Gout: the Sons of Gout Study. Arthritis Rheumatol. 2018;70(11):1847–1852. doi:10.1002/art.40572
20. Hill EM, Sky K, Sit M, et al. Does starting allopurinol prolong acute treated gout? A randomized clinical trial. J Clin Rheumatol. 2015;21(3):120–125. doi:10.1097/RHU.0000000000000235
21. Becker MA, Schumacher HR, Wortmann RL, et al. Febuxostat compared with allopurinol in patients with hyperuricemia and gout. N Engl J Med. 2005;353(23):2450–2461. doi:10.1056/NEJMoa050373
22. White WB, Saag KG, Becker MA, et al. Cardiovascular safety of febuxostat or allopurinol in patients with Gout. N Engl J Med. 2018;378(13):1200–1210. doi:10.1056/NEJMoa1710895
23. Schlesinger N, Lipsky PE. Pegloticase treatment of chronic refractory gout: update on efficacy and safety. Semin Arthritis Rheum. 2020;50(3s):S31–S38. doi:10.1016/j.semarthrit.2020.04.011
24. Mackenzie IS, Ford I, Nuki G, et al. Long-term cardiovascular safety of febuxostat compared with allopurinol in patients with gout (FAST): a multicentre, prospective, randomised, open-label, non-inferiority trial. Lancet. 2020;396(10264):1745–1757. doi:10.1016/S0140-6736(20)32234-0
25. Perez-Ruiz F, Alonso-Ruiz A, Calabozo M, et al. Efficacy of allopurinol and benzbromarone for the control of hyperuricaemia. A pathogenic approach to the treatment of primary chronic gout. Ann Rheum Dis. 1998;57(9):545–549. doi:10.1136/ard.57.9.545
26. Perez-Ruiz F, Calabozo M, Fernandez-Lopez MJ, et al. Treatment of chronic gout in patients with renal function impairment: an open, randomized, Actively Controlled Study. J Clin Rheumatol. 1999;5(2):49–55. doi:10.1097/00124743-199904000-00003
27. Hanvivadhanakul P, Akkasilpa S, Deesomchok U. Efficacy of benzbromarone compared to allopurinol in lowering serum uric acid level in hyperuricemic patients. J Med Assoc Thai. 2002;85(Suppl 1):S40–7.
28. Boss GR, Seegmiller JE. Hyperuricemia and gout: Classification, complications and management. N Engl J Med. 1979;300(26):1459–1468. doi:10.1056/NEJM197906283002604
29. Ravera R. Il benbromarone nel trattamento delle iperuricemia. [Benzbromarone in the treatment of hyperuricemias]. Minerva Med. 1975;66(17):783–800. Italian.
30. Didier M, Olmer M. Effet hypo-uricémiant de la benzbromarone en particulier dans l'insuffisance rénale. [Hypouricemic effect of benzbromarone especially in kidney failure]. Sem Hop. 1978;54(9–12):463–465. French.
31. Kumar S, Ng J, Gow P. Benzbromarone therapy in management of refractory gout. N Z Med J. 2005;118(1217):U1528.
32. Masbernard A, Giudicelli CP. Ten years’ experience with benzbromarone in the management of gout and hyperuricaemia. S Afr Med J. 1981;59(20):701–706.
33. van der Klauw MM, Houtman PM, Stricker BHC, et al. Hepatic injury caused by benzbromarone. J Hepatol. 1994;20(3):376–379. doi:10.1016/S0168-8278(94)80011-1
34. Wagayama H, Shiraki K, Sugimoto K, et al. Fatal fulminant hepatic failure associated with benzbromarone. J Hepatol. 2000;32(5):874. doi:10.1016/S0168-8278(00)80263-9
35. Suzuki T, Suzuki T, Kimura M, et al. [A case of fulminant hepatitis, possibly caused by benzbromarone]. Nihon Shokakibyo Gakkai Zasshi. 2001;98(4):421–425. Japanese.
36. Arai M, Yokosuka O, Fujiwara K, et al. Fulminant hepatic failure associated with benzbromarone treatment: a case report. J Gastroenterol Hepatol. 2002;17(5):625–626. doi:10.1046/j.1440-1746.2002.02692.x
37. Lee MH, Graham GG, Williams KM, et al. A benefit-risk assessment of benzbromarone in the treatment of gout. Was its withdrawal from the market in the best interest of patients? Drug Saf. 2008;31(8):643–665. doi:10.2165/00002018-200831080-00002
38. Waller A, Jordan KM. Use of febuxostat in the management of gout in the United Kingdom. Ther Adv Musculoskelet Dis. 2017;9(2):55–64. doi:10.1177/1759720X16682010
39. Stamp LK, Chapman PT, Barclay M, et al. The effect of kidney function on the urate lowering effect and safety of increasing allopurinol above doses based on creatinine clearance: a post hoc analysis of a randomized controlled trial. Arthritis Res Ther. 2017;19(1):283. doi:10.1186/s13075-017-1491-x
40. Sakai Y, Otsuka T, Ohno D, et al. Febuxostat for treating allopurinol-resistant hyperuricemia in patients with chronic kidney disease. Ren Fail. 2014;36(2):225–231. doi:10.3109/0886022X.2013.844622
41. Liu X, Wang H, Ma R, et al. The urate-lowering efficacy and safety of febuxostat versus allopurinol in Chinese patients with asymptomatic hyperuricemia and with chronic kidney disease stages 3–5. Clin Exp Nephrol. 2019;23(3):362–370. doi:10.1007/s10157-018-1652-5
42. Kimura K, Hosoya T, Uchida S, et al. Febuxostat therapy for patients with stage 3 CKD and asymptomatic hyperuricemia: a Randomized Trial. Am J Kidney Dis. 2018;72(6):798–810. doi:10.1053/j.ajkd.2018.06.028
43. Kim S, Kim H-J, Ahn H-S, et al. Renoprotective effects of febuxostat compared with allopurinol in patients with hyperuricemia: a systematic review and meta-analysis. Kidney Res Clin Pract. 2017;36(3):274–281. doi:10.23876/j.krcp.2017.36.3.274
44. Singh JA, Cleveland JD. Comparative effectiveness of allopurinol versus febuxostat for preventing incident renal disease in older adults: an analysis of Medicare claims data. Ann Rheum Dis. 2017;76(10):1669–1678. doi:10.1136/annrheumdis-2017-211210
45. Shoji A, Yamanaka H, Kamatani N. A retrospective study of the relationship between serum urate level and recurrent attacks of gouty arthritis: evidence for reduction of recurrent gouty arthritis with antihyperuricemic therapy. Arthritis Rheum. 2004;51(3):321–325. doi:10.1002/art.20405
46. Sarawate CA, Patel PA, Schumacher HR, et al. Serum urate levels and gout flares: analysis from managed care data. J Clin Rheumatol. 2006;12(2):61–65. doi:10.1097/01.rhu.0000209882.50228.9f
47. Stamp L, Morillon MB, Taylor WJ, et al. Serum urate as surrogate endpoint for flares in people with gout: a systematic review and meta-regression analysis. Semin Arthritis Rheum. 2018;48(2):293–301. doi:10.1016/j.semarthrit.2018.02.009
48. Yamanaka H, Tamaki S, Ide Y, et al. Stepwise dose increase of febuxostat is comparable with colchicine prophylaxis for the prevention of gout flares during the initial phase of urate-lowering therapy: results from FORTUNE-1, a prospective, multicentre randomised study. Ann Rheum Dis. 2018;77(2):270–276. doi:10.1136/annrheumdis-2017-211574
49. Doherty M, Jenkins W, Richardson H, et al. Efficacy and cost-effectiveness of nurse-led care involving education and engagement of patients and a treat-to-target urate-lowering strategy versus usual care for gout: a randomised controlled trial. Lancet. 2018;392(10156):1403–1412. doi:10.1016/S0140-6736(18)32158-5
50. Schlesinger N, Etzel CJ, Greenberg J, et al. Gout prophylaxis evaluated according to the 2012 American College of Rheumatology Guidelines: analysis from the CORRONA Gout Registry. J Rheumatol. 2016;43(5):924–930. doi:10.3899/jrheum.150345
51. Schlesinger N. Treatment of chronic gouty arthritis: it is not just about urate-lowering therapy. Semin Arthritis Rheum. 2012;42(2):155–165. doi:10.1016/j.semarthrit.2012.03.010
52. Maes ML, Saseen, JJ, Wright G, et al. Utilization of acute gout prophylaxis in the real world: a retrospective database cohort analysis. Clin Rheumatol. 2021;40:1017–1026.
53. Tai V, Merriman TR, Dalbeth N. Genetic advances in gout: potential applications in clinical practice. Curr Opin Rheumatol. 2019;31(2):144–151. doi:10.1097/BOR.0000000000000571
54. Dehghan A, Köttgen A, Yang Q, et al. Association of three genetic loci with uric acid concentration and risk of gout: a genome-wide association study. Lancet. 2008;372(9654):1953–1961. doi:10.1016/S0140-6736(08)61343-4
55. Matsuo H, Yamamoto K, Nakaoka H, et al. Genome-wide association study of clinically defined gout identifies multiple risk loci and its association with clinical subtypes. Ann Rheum Dis. 2016;75(4):652–659. doi:10.1136/annrheumdis-2014-206191
56. Dong Z, Guo S, Yang Y, et al. Association between ABCG2 Q141K polymorphism and gout risk affected by ethnicity and gender: a systematic review and meta-analysis. Int J Rheum Dis. 2015;18(4):382–391. doi:10.1111/1756-185X.12519
57. González-Galarza FF, Takeshita LC, Santos EM, et al. Allele frequency net 2015 update: new features for HLA epitopes, KIR and disease and HLA adverse drug reaction associations. Nucleic Acids Res. 2015;43(D1):D784–8. doi:10.1093/nar/gku1166
58. Jutkowitz E, Dubreuil M, Lu N, et al. The cost-effectiveness of HLA-B*5801 screening to guide initial urate-lowering therapy for gout in the United States. Semin Arthritis Rheum. 2017;46(5):594–600. doi:10.1016/j.semarthrit.2016.10.009
59. Ke C-H, Chung W-H, Wen Y-H, et al. Cost-effectiveness analysis for genotyping before allopurinol treatment to prevent severe cutaneous adverse drug reactions. J Rheumatol. 2017;44(6):835–843. doi:10.3899/jrheum.151476
60. Park D-J, Kang J-H, Lee J-W, et al. Cost-effectiveness analysis of HLA-B5801 genotyping in the treatment of gout patients with chronic renal insufficiency in Korea. Arthritis Care Res (Hoboken). 2015;67(2):280–287. doi:10.1002/acr.22409
61. Chong HY, Lim YH, Prawjaeng J, et al. Cost-effectiveness analysis of HLA-B*58: 01 genetic testing before initiation of allopurinol therapy to prevent allopurinol-induced Stevens-Johnson syndrome/toxic epidermal necrolysis in a Malaysian population. Pharmacogenet Genomics. 2018;28(2):56–67. doi:10.1097/FPC.0000000000000319
62. Dong D, Tan-Koi W-C, Teng GG, et al. Cost–effectiveness analysis of genotyping for HLA-B*5801 and an enhanced safety program in gout patients starting allopurinol in Singapore. Pharmacogenomics. 2015;16(16):1781–1793. doi:10.2217/pgs.15.125
63. Plumpton CO, Alfirevic A, Pirmohamed M, et al. Cost effectiveness analysis of HLA-B*58:01 genotyping prior to initiation of allopurinol for gout. Rheumatology (Oxford). 2017;56(10):1729–1739. doi:10.1093/rheumatology/kex253
64. Singh JA. Patient perspectives in gout: a review. Curr Opin Rheumatol. 2019;31(2):159–166. doi:10.1097/BOR.0000000000000583
65. Singh JA. Gout and sexual function: patient perspective of how gout affects personal relationships and intimacy. BMC Rheumatol. 2019;3(1):8. doi:10.1186/s41927-019-0056-9
66. Singh JA. The impact of gout on patient’s lives: a study of African-American and Caucasian men and women with gout. Arthritis Res Ther. 2014;16(3):R132. doi:10.1186/ar4589
67. Singh JA, Edwards NL. Gout management and outcomes during the COVID-19 pandemic: a cross-sectional internet survey. Ther Adv Musculoskelet Dis. 2020;12:1759720x20966124. doi:10.1177/1759720X20966124
68. Singh JA, Neogi T, FitzGerald JD. Patient perspectives on gout and gout treatments: a patient panel discussion that informed the 2020 American College of Rheumatology Treatment Guideline. ACR Open Rheumatol. 2020;2(12):725–733. doi:10.1002/acr2.11199
69. Hartung EF. Colchicine and its analogs in gout: a brief review. Arthritis Rheum. 1961;4(1):18–26. doi:10.1002/art.1780040103
70. Crittenden DB, Lehmann RA, Schneck L, et al. Colchicine use is associated with decreased prevalence of myocardial infarction in patients with gout. J Rheumatol. 2012;39(7):1458–1464. doi:10.3899/jrheum.111533
71. Solomon DH, Liu -C-C, Kuo I-H, et al. Effects of colchicine on risk of cardiovascular events and mortality among patients with gout: a cohort study using electronic medical records linked with Medicare claims. Ann Rheum Dis. 2016;75(9):1674–1679. doi:10.1136/annrheumdis-2015-207984
72. Alayli G, Cengiz K, Cantürk F, et al. Acute myopathy in a patient with concomitant use of pravastatin and colchicine. Ann Pharmacother. 2005;39(7–8):1358–1361. doi:10.1345/aph.1E593
73. Tardif J-C, Kouz S, Waters DD, et al. Efficacy and safety of low-dose colchicine after myocardial infarction. N Engl J Med. 2019;381(26):2497–2505. doi:10.1056/NEJMoa1912388
74. Bailey CJ. Uric acid and the cardio-renal effects of SGLT2 inhibitors. Diabetes Obes Metab. 2019;21(6):1291–1298. doi:10.1111/dom.13670
75. Fralick M, Chen SK, Patorno E, et al. Assessing the risk for gout with sodium-glucose cotransporter-2 inhibitors in patients with Type 2 diabetes: a Population-Based Cohort Study. Ann Intern Med. 2020;172(3):186–194. doi:10.7326/M19-2610
76. Qaseem A, Harris RP, Forciea MA. Management of acute and recurrent Gout: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2017;166(1):58–68. doi:10.7326/M16-0570
77. Richette P, Doherty M, Pascual E, et al. 2016 updated EULAR evidence-based recommendations for the management of gout. Ann Rheum Dis. 2017;76(1):29–42. doi:10.1136/annrheumdis-2016-209707
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.