Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Construction of a Multidisciplinary Follow-Up Indicator System Based on the ABC Pathway for Patients with Atrial Fibrillation After Ablation: A Delphi Study
Authors Shi X, Zhang J ![]() , Li B, Zheng Y, Liu M, Cui Y, Hao X
, Li B, Zheng Y, Liu M, Cui Y, Hao X
Received 22 December 2025
Accepted for publication 19 May 2026
Published 28 May 2026 Volume 2026:19 590772
DOI https://doi.org/10.2147/JMDH.S590772
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Tilakavati Karupaiah
Xiushan Shi,1 Jinyu Zhang,2 Bingjie Li,1 Ying Zheng,1 Mengting Liu,1 Yaya Cui,1 Xiaoyan Hao1
1Department of Nursing,Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Third Hospital of Shanxi Medical University, Tongji Shanxi Hospital, Taiyuan, 030032, People’s Republic of China; 2Department of Nursing,First Hospital of Shanxi Medical University, Taiyuan, 030001, People’s Republic of China
Correspondence: Jinyu Zhang, Email [email protected]
Background: Long-term follow-up is essential for patients with atrial fibrillation (AF) after ablation. Although the “Atrial Fibrillation Better Care” (ABC) pathway is widely recommended, a structured and operational follow-up indicator system tailored to post-ablation AF patients remains lacking. This study aimed to develop a multidisciplinary follow-up indicator system for post-ablation AF patients based on the ABC pathway.
Methods: A preliminary indicator pool was developed through a literature review guided by the ABC pathway and relevant guidelines, and further refined through semi-structured interviews with post-ablation AF patients. A two-round Delphi survey was then conducted among 23 multidisciplinary experts in cardiovascular care and nursing management. Indicators were screened, revised, and finalized according to prespecified consensus criteria and statistical analysis.
Results: A total of 23 experts completed two rounds of the Delphi survey. The response rates were 92.0% in round 1 and 100% in round 2. The authority coefficients were 0.892 and 0.914, respectively.Kendall’s W values ranged from 0.229 to 0.370 across indicator levels and rounds, respectively (P < 0.001).
Conclusion: This study developed a preliminary multidisciplinary follow-up indicator system for post-ablation AF patients based on the ABC pathway. The findings provide a consensus-based framework for structuring follow-up content and may inform future clinical application and empirical validation.
Keywords: atrial fibrillation, radiofrequency ablation, follow-up indicators, ABC pathway, multidisciplinary care, Delphi technique
Background
Atrial fibrillation (AF) has become an increasingly prevalent global health issue, with its burden intensifying in tandem with population ageing.1 Recent data indicates approximately 50 million individuals worldwide suffer from atrial fibrillation, with both incidence and associated mortality rates continuing to rise.2 This condition remains a significant independent risk factor for heart failure, stroke, and all-cause mortality, severely compromising patients’ quality of life while incurring substantial healthcare expenditures.3,4 Consequently, developing effective long-term management strategies remains crucial for alleviating the clinical and socio-economic burden associated with atrial fibrillation.
Radiofrequency ablation has become an established strategy for controlling atrial fibrillation rhythm. However, its long-term efficacy remains unsatisfactory: recurrence rates approximately 35% at 12 months post-procedure, rising to 50% within five years.5,6 Recurrence and poor outcomes are frequently influenced by modifiable factors, including inadequate anticoagulation therapy, poorly controlled comorbidities, and delayed detection of asymptomatic arrhythmic episodes.
Post-ablation care also presents numerous challenges, including poor patient compliance, low engagement with lifestyle interventions, and inadequate health literacy.7 Moreover, as ablation indications expand to include elderly patients and those with complex structural heart disease, clinical scenarios grow increasingly intricate.8 These populations require meticulous monitoring and personalised management to balance thromboembolic and haemorrhagic risks. These issues underscore the necessity for establishing a structured, comprehensive follow-up system integrating symptom monitoring, complication prevention, and long-term risk optimisation.9
Given the shift in treatment paradigms from isolated rhythm control towards comprehensive management, the European Society of Cardiology guidelines advocate for a holistic, multidisciplinary approach to atrial fibrillation management.10 Its core element is the “Atrial Fibrillation Better Care (ABC)” pathway: stroke prevention, optimised symptom management, and improved control of cardiovascular and comorbid conditions.11 While the ABC pathway provides a robust theoretical framework, its implementation in routine clinical practice remains inconsistent. During the post-ablation follow-up phase, anticoagulation monitoring and comorbidities management often remain fragmented and uncoordinated, leading to significant disparities in patient outcomes.12 Furthermore, existing research predominantly focuses on pharmacological interventions or the atrial fibrillation population as a whole, resulting in a critical gap in the post-ablation care domain: the absence of a specific, quantifiable, and actionable follow-up indicator system tailored to this patient cohort.
This study employed the Delphi method to construct a scientifically systematic follow-up indicator system for post-radiofrequency ablation atrial fibrillation patients based on the ABC clinical pathway. This system aims to support standardised multidisciplinary follow-up, promoting comprehensive, long-term integrated management in clinical practice.
Methods
Design
This study was conducted in two phases. First, a preliminary set of follow-up indicators for patients with AF after radiofrequency ablation was developed through a literature review and semi-structured patient interviews. Second, a modified Delphi process was undertaken to refine the indicator system and achieve expert consensus through two rounds of consultation.
Phase 1
Literature Review
A comprehensive literature search was performed from database inception to January 2024 in PubMed, MEDLINE, Web of Science, the Cochrane Library, CNKI, and the Wanfang Database. The search strategy combined Medical Subject Headings (MeSH) terms and free-text keywords. Key terms included “atrial fibrillation”, “radiofrequency ablation”, “catheter ablation”, “follow-up”, “continuity of care”, “outpatient follow-up”, “ABC pathway”, and “integrated care”.
Studies were included if they focused on post-ablation care, integrated management of atrial fibrillation, or follow-up strategies for patients with atrial fibrillation. Editorials, case reports, conference abstracts, and non-English/Chinese publications were excluded. Two reviewers independently screened titles and abstracts, followed by full-text review against the eligibility criteria. Disagreements were resolved through discussion or consultation with a third reviewer.
Semi-Structured Interviews
Semi-structured individual interviews were conducted with 12 post-ablation AF patients using purposive sampling combined with snowball recruitment. Each interview lasted approximately 30 minutes. An interview guide was used to explore patients’ perceived priorities and unmet needs during follow-up. The semi-structured interview guide is provided in Appendix 1. With participants’ consent, all interviews were audio-recorded and transcribed verbatim within 24 hours. The transcripts were analyzed using content analysis. Two researchers independently coded the transcripts, and themes were iteratively refined through repeated discussion. Data saturation was considered to have been achieved when no new codes or themes emerged in the final three consecutive interviews. Interview findings were used to refine the wording, relevance, and practicality of the draft indicators and to ensure that patient-centred concerns were adequately represented.
Phase 2
Delphi Questionnaire Development
Based on the literature review and qualitative findings, the research team developed the first-round Delphi questionnaire.Prior to formal distribution, the questionnaire was piloted with three experts who met the inclusion criteria but were not members of the final Delphi panel. Feedback from the pilot test was used to improve item clarity, wording, and response format.Following analysis of round-1 responses, indicators were revised and a second-round questionnaire was produced.The final questionnaires are provided in Appendix 2 and Appendix 3, respectively.Each questionnaire comprised three sections: (1) expert demographic and professional characteristics, (2) the indicator rating form, and (3) an expert self-assessment form.
Indicator importance was rated using a 5-point Likert scale, ranging from 1 (very unimportant) to 5 (very important). Free-text fields were provided to allow experts to propose modifications, deletions, additions, or merging of items, as well as to offer broader methodological suggestions. All expert feedback was documented, independently reviewed by two research team members, and discussed in team meetings before final decisions on indicator revisions were made.
Delphi Process
A modified Delphi technique was applied. Experts were invited to independently rate each indicator and provide written feedback. After round 1, responses were summarised and indicators were screened using predefined criteria established with reference to prior Delphi studies in healthcare quality indicator development. An indicator was considered for deletion when it simultaneously met all of the following conditions:a mean importance score <3.5, a full-score proportion (percentage of experts rating the indicator as 4 or 5) ≤60%, and a coefficient of variation(CV) ≥0.25.Indicators that partially met the deletion criteria were flagged for discussion and possible revision.The research team thoroughly discussed all expert feedback and revised the indicator set by removing, merging, rewording, or adding items, before distributing the round-2 questionnaire. The Delphi process was concluded after round 2, when ratings demonstrated adequate stability and no substantive new indicators were suggested, indicating that consensus had been achieved for the purposes of this exploratory framework development.
Expert Panel
Experts certified by the China Center for Atrial Fibrillation were recruited using convenience sampling. Inclusion criteria were: (1) a bachelor’s degree or above; (2) an associate senior title or above; (3) ≥10 years of experience in AF diagnosis and treatment or nursing management; (4) a master’s degree or above for medical experts and a bachelor’s degree or above for nursing experts; (5) familiarity with the Delphi method; and (6) willingness to participate. Ultimately, 23 experts from seven provinces/municipalities in China were included.
Data Collection
From June to December 2024, questionnaires were distributed electronically via Email or WeChat. Experts were asked to complete the questionnaires within the specified timeframe. All returned questionnaires were checked for completeness and validity prior to analysis.
Statistical Analysis
Statistical analyses were performed using SPSS version 25.0. Descriptive statistics were used to summarise indicator ratings, including means, standard deviations, coefficients of variation, and the proportion of high ratings. Expert engagement was assessed using the valid response rate. Expert authority was quantified using the authority coefficient (Cr), calculated as the average of the judgement coefficient (Ca) and familiarity coefficient (Cs): Cr = (Ca + Cs) / 2.
Results
Literature Search and Selection
A total of 1,247 records were retrieved from the six databases. After removing 326 duplicates, 921 records were screened by title and abstract, of which 34 were selected for full-text review. Following application of the inclusion and exclusion criteria, 10 studies were ultimately included in the analysis. The literature search and selection process is summarized in a flow diagram (Figure 1). The 10 included studies, together with the three predefined domains of the ABC pathway, informed the development of the initial indicator pool comprising 3 first-level, 9 second-level, and 44 third-level indicators.
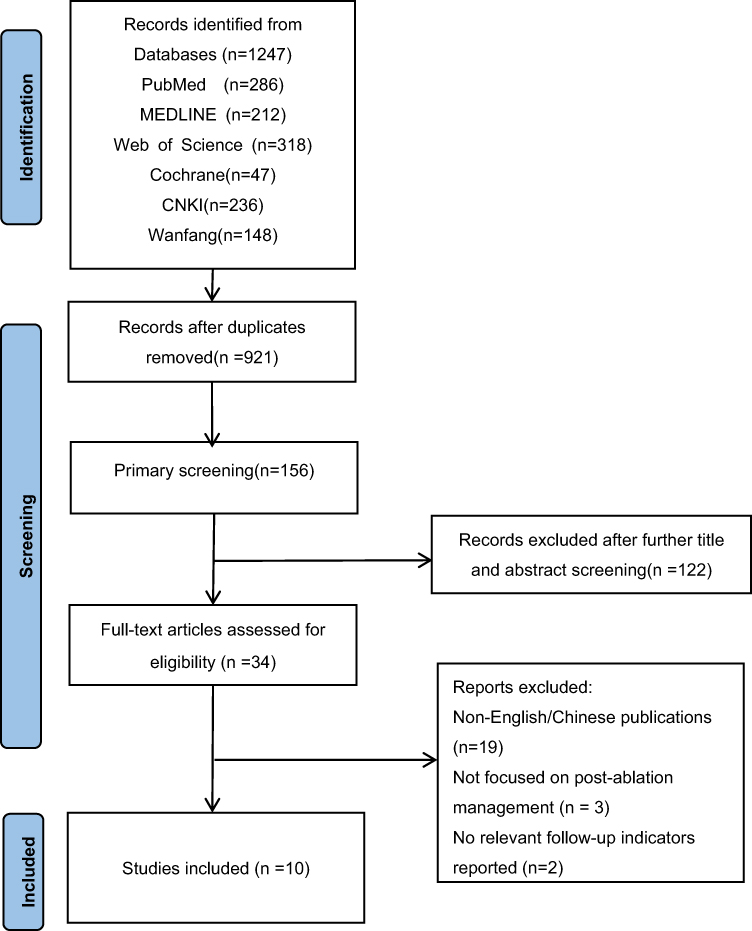 |
Figure 1 Flow diagram of literature search and selection. |
Integration of Qualitative Findings
Analysis of the semi-structured interviews with 12 post-ablation AF patients identified several patient-centred needs not adequately captured in the literature-derived indicator pool. Specifically, the following indicators were newly added based on the qualitative findings: (1) symptom coping style and ability (eg., self-measured pulse during sudden palpitations, and indications for seeking urgent medical care), reflecting patients’ expressed need for guidance on self-management during symptomatic episodes; (2) sleep quality, as sleep disturbances were frequently reported by interviewees as a concern after ablation; (3) mental status screening (SAS/SDS scales), corresponding to patients’ descriptions of anxiety and emotional distress related to possible recurrence; (4) assessment of family support (APGAR scale), reflecting the importance patients placed on their family’s understanding and assistance during recovery; and (5) the effect of financial burden on treatment (proportion of discontinuations of self-paid medication use), which emerged from patients’ concerns about the affordability of long-term medications. These patient-driven indicators were incorporated into the initial indicator pool prior to the Delphi consultation.
Characteristics of the Expert Panel
A total of 23 experts from seven provinces and municipalities across China (Beijing, Tianjin, Hubei, Shanxi, Hebei, Sichuan, and Heilongjiang) participated in the Delphi consultation. Among them, 16 (69.57%) were nursing management experts and 7 (30.43%) were clinicians specialising in cardiovascular care. The mean age of the panel was 47.65±7.50 years, and the mean length of professional experience was 27.39±7.92 years. Detailed demographic characteristics of the expert panel are presented in Table 1.
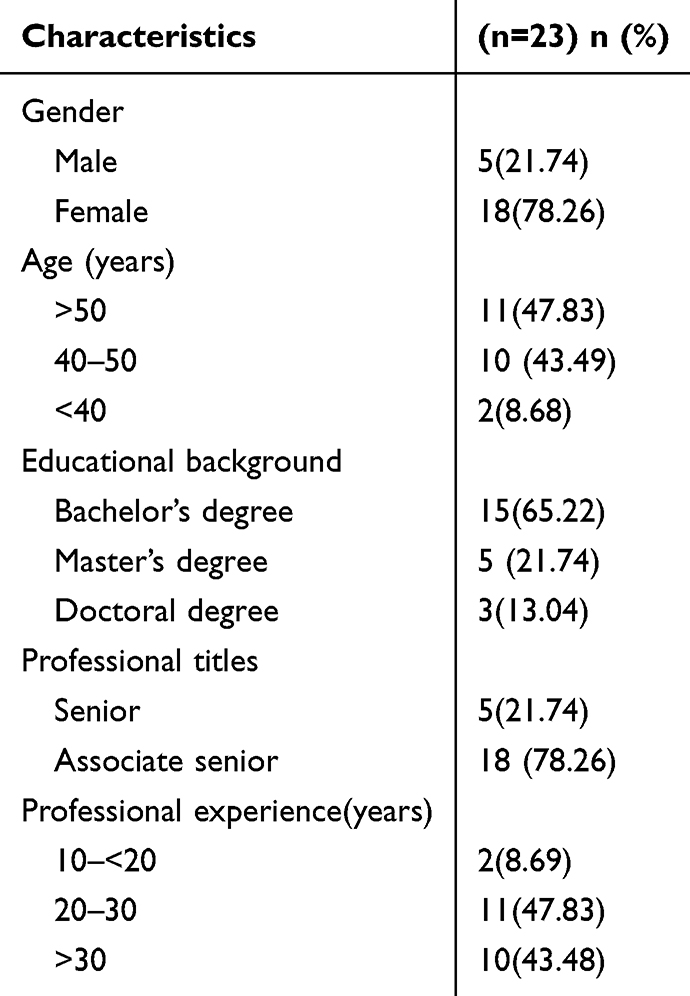 |
Table 1 Demographic Data of Expert Panel |
Level of Expert Activity
In round 1, 25 questionnaires were distributed and 23 valid responses were returned, yielding a response rate of 92%. In round 2, all 23 questionnaires were returned, corresponding to a response rate of 100%. In round 1, 20 experts (86.96%) provided written comments; in round 2, 10 experts (43.48%) provided comments, indicating sustained engagement across rounds.
Authority Coefficient of Experts
Expert authority was assessed using the authority coefficient (Cr), calculated from the judgement coefficient (Ca) and familiarity coefficient (Cs). In rounds 1 and 2, Ca values were 0.854 and 0.880, and Cs values were 0.930 and 0.948, respectively. The resulting Cr values were 0.892 in round 1 and 0.914 in round 2, suggesting that the participating experts were sufficiently familiar with the topic to provide informed judgments.
Consensus and Coordination of Expert Opinions
The degree of consensus among experts was evaluated using the coefficient of variation (CV) and Kendall’s coefficient of concordance (W). Across the two rounds, CV values ranged from 0.00 to 0.23 in round 1 and from 0.00 to 0.22 in round 2, indicating limited dispersion in expert ratings. Kendall’s W values for the first-, second-, and third-level indicators ranged from 0.305 to 0.370 in round 1 and from 0.229 to 0.306 in round 2. All Kendall’s W-tests were statistically significant (p < 0.001), indicating coordination in expert scoring across the panel. Given the magnitude of the W values, the degree of agreement is better interpreted as moderate rather than high.
Results of the Delphi Survey
Results of the First Round of the Delphi Survey
In round 1, experts evaluated the preliminary indicator set (Table 2). A total of 31 comments were received, primarily relating to the consolidation, refinement, addition, or removal of indicators. Based on expert feedback and group discussion, the research team implemented the following revisions: (1) Indicator merging: “Type of anticoagulant” and “dose of anticoagulant” were merged into “anticoagulant type and dose (medication verification)”. Similarly, “type of heart rate/rhythm control medication” and “dose of heart rate/rhythm control medication” were merged into “type and dosage of heart rate/rhythm control medication (medication verification)”.(2) Wording refinement: Several indicators were revised for clarity and operational feasibility, including the revision of “warning value of processing ability” to “symptom coping style and ability (eg., self-measured pulse during sudden palpitations, and indications for seeking urgent medical care)”. In addition, the quality-of-life indicator was revised from “SF-36” to “AF-QoL”, and “liver and kidney function” was expanded to “liver and kidney function and thyroid function indices”. “Diet” was refined to “diet management”, and “awareness of exercise plan” was revised to “exercise (exercise volume, contraindications, and indications for exercise termination, etc).”(3) Indicator retention and refinement: Under the domain of symptom identification, “symptoms of peripheral arterial embolism” was retained after discussion. “Sleep-disordered breathing screening” and “family support assessment (APGAR scale)” were also retained and refined based on expert feedback. (4) Indicator deletion: The following indicators were removed based on the predefined criteria and expert recommendations: “assessment of ablation line integrity”, “monitoring risk of conversion to atrial flutter/atrial tachycardia”, “screening risk of left atrio-oesophageal fistula”, and “assessment of anticoagulation continuity at 3 months after surgery”.
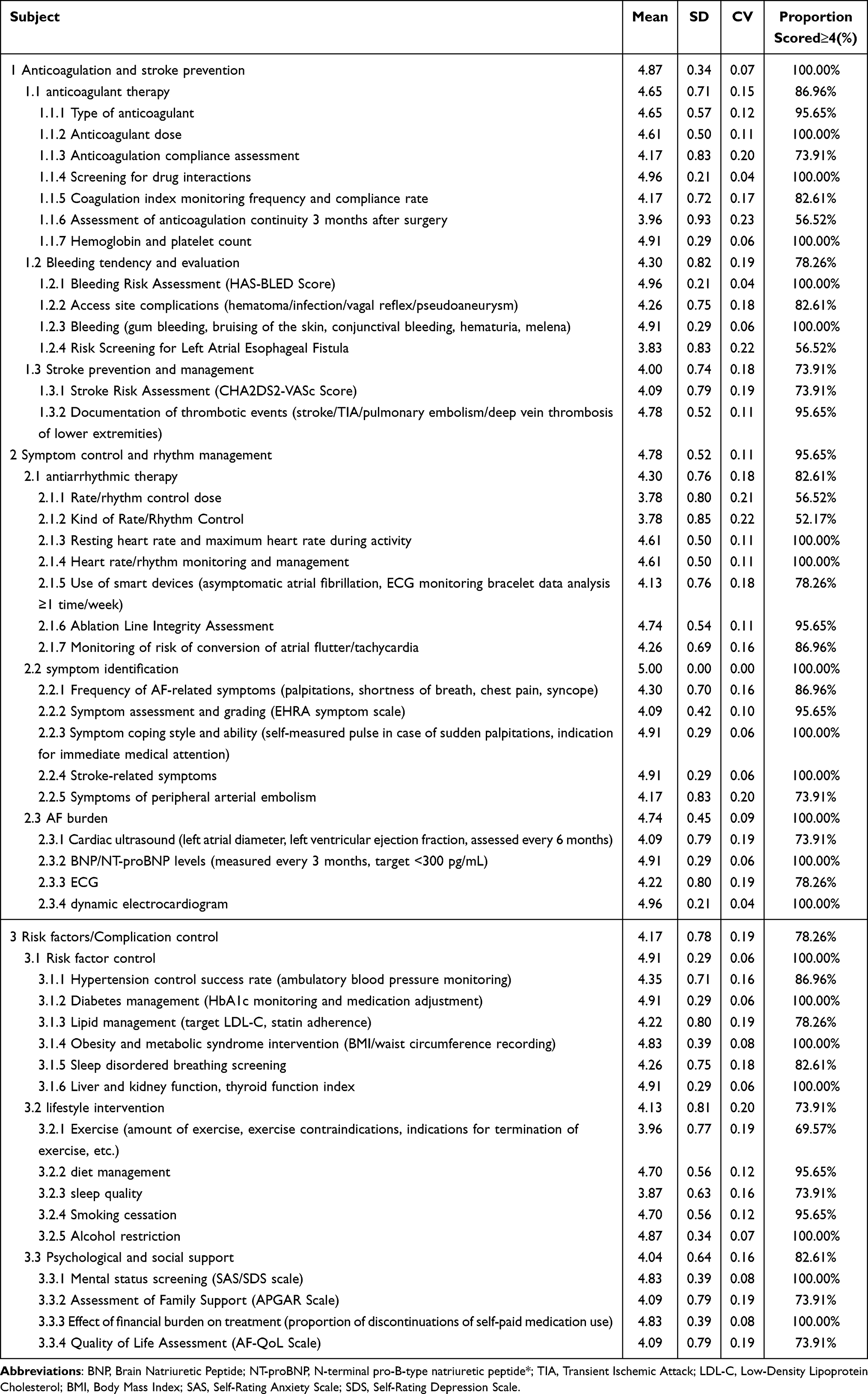 |
Table 2 Results of the First Round of the Delphi Survey |
Results of the Second Round of the Delphi Survey
In round 2, experts re-evaluated the revised indicator set. No additional indicators were proposed, and all remaining indicators met the predefined consensus criteria. The final follow-up indicator system comprised 3 first-level indicators, 9 second-level indicators, and 38 third-level indicators (Table 3).
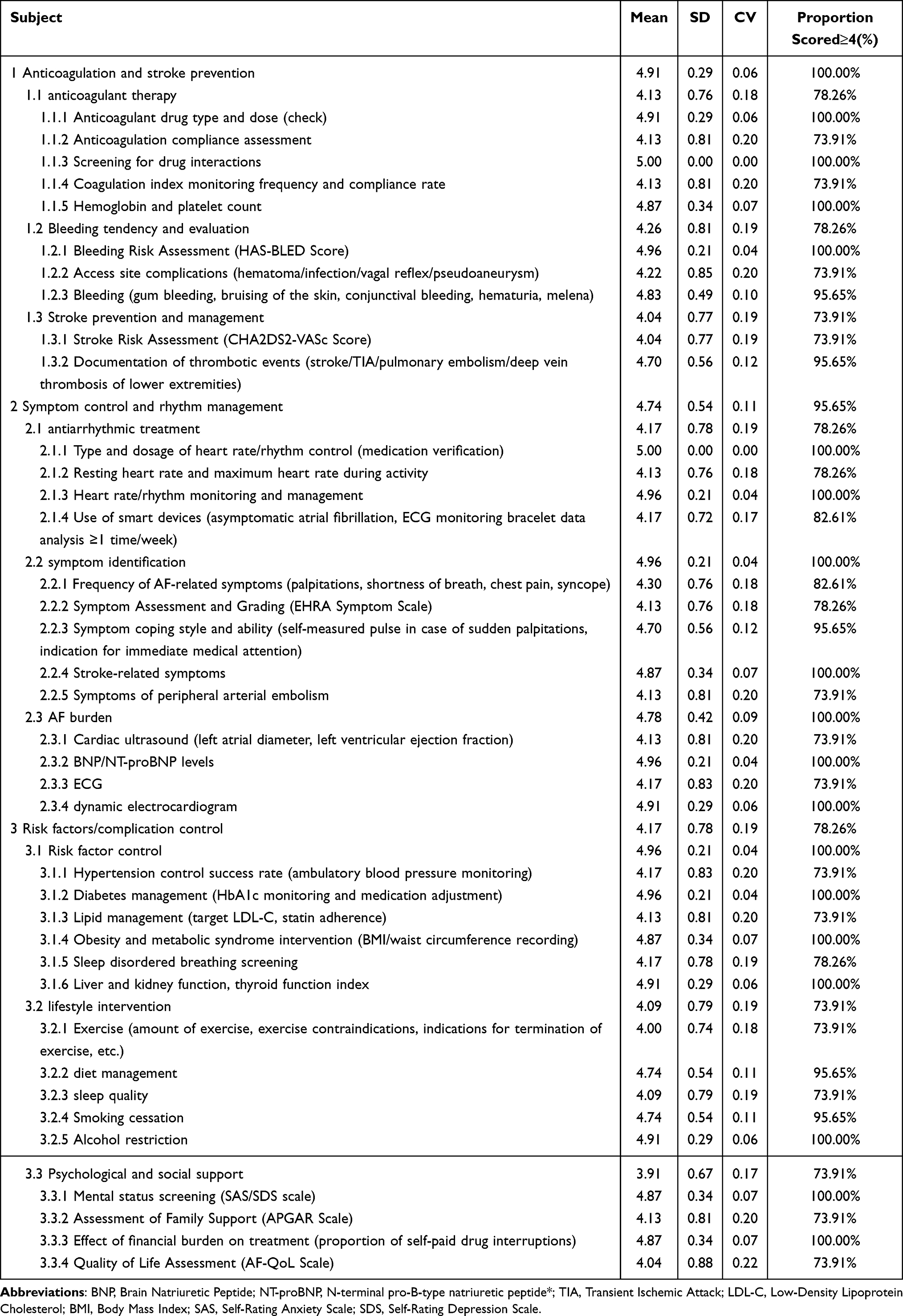 |
Table 3 Results of the Second Round of the Delphi Survey |
Discussion
Reliability of Research Results
The follow-up indicator system developed in this study was grounded in evidence from the literature on post-ablation management of atrial fibrillation (AF) and aligned with relevant guideline recommendations. The ABC pathway proposed in the 2020 European Society of Cardiology10 guidelines was adopted as the theoretical framework, which strengthened the scientific rationale of the initial indicator pool and ensured that the domains reflected contemporary principles of integrated AF care.
The Delphi panel comprised experts from seven provinces/municipalities in China, providing a degree of geographical diversity and multidisciplinary input. All experts had extensive experience in cardiovascular practice or nursing management and held senior or associate senior professional titles, supporting the credibility of the consultation process. In addition, the response rates in both Delphi rounds were high, indicating sustained expert participation throughout the consultation process. The authority coefficients (Cr) in rounds 1 and 2 were 0.892 and 0.914, respectively, suggesting that the participating experts were sufficiently familiar with the topic to provide informed judgments. Furthermore, Kendall’s coefficients of concordance (W) were statistically significant (p < 0.001), indicating coordination in expert scoring across the panel. However, given the magnitude of the W values, the degree of agreement is better interpreted as moderate rather than high.
The Comprehensiveness and Relevance of the ABC Pathway-Based Indicator System
The final indicator system is structured around the three core domains of the ABC pathway: Anticoagulation and stroke prevention,Symptom control and rhythm management,Risk factors/complication control. Previous studies indicate that adherence to the ABC pathway reduces all-cause mortality, cardiovascular mortality, and the incidence of thromboembolic events.13–15 Against this background, developing follow-up indicators within this framework may help translate the principles of integrated AF care into more structured and operational follow-up content for patients after ablation.Catheter ablation causes endothelial injury and transient inflammatory activation, potentially increasing the risk of early postoperative thromboembolism.16–18 It is therefore recommended that oral anticoagulation therapy be administered for at least three months post-ablation, with subsequent continuation determined by individual stroke risk rather than solely by cardiac rhythm status. Against this backdrop, structured follow-up is crucial to ensure appropriate anticoagulant selection, accurate dosing, and adequate adherence. Incorporating CHA2DS2-VASc and HAS-BLED assessments into follow-up provides standardised methods for evaluating thromboembolic and bleeding risks, respectively.18 Furthermore, monitoring for haemorrhagic symptoms and laboratory parameters (such as haemoglobin and platelet counts) facilitates early identification of adverse events. This is particularly important given that poor adherence to oral anticoagulation therapy is common, often due to treatment complexity, insufficient disease awareness, concerns about adverse effects, forgetfulness, and financial burdens.19,20 Given the short half-life of non-vitamin K antagonist oral anticoagulants (NOACs), missed doses may rapidly diminish anticoagulant protection, potentially increasing the risk of thromboembolism.Accordingly, the retention of indicators related to anticoagulant verification and adherence assessment suggests that medication safety and treatment continuity remain important components of post-ablation follow-up.21
Post-ablation cardiac rhythm monitoring remains the fundamental method for detecting atrial fibrillation recurrence. With the proliferation of digital health technologies, wearable devices and mobile monitoring tools have become widely adopted for rhythm surveillance.22 Many patients utilise smart devices to record cardiac rhythm data, aiding in the identification of recurrence and supporting clinical decision-making. The inclusion of smart-device-related monitoring reflects the increasing use of wearable and mobile technologies in contemporary AF follow-up and suggests that digital tools may become a more relevant component of post-ablation monitoring.
Recurrence of arrhythmias during the early’silent period’following ablation is relatively common and does not necessarily indicate procedural failure. The symptomatic burden remains clinically significant, with frequent occurrences of palpitations, chest tightness, and dyspnoea.23
Beyond symptom frequency and severity, patients’ ability to recognise and respond to symptoms appropriately may help reduce delays and support early detection of complications,24 although this requires prospective evaluation.
The long-term prognosis following atrial fibrillation ablation is significantly influenced by upstream risk factors and comorbidities. Studies indicate that conditions such as obesity, hypertension, diabetes, sleep-disordered breathing, impaired sleep quality, and psychological distress are associated with atrial fibrillation recurrence and poor outcomes.25 Optimizing these risk factors can slow atrial remodeling and contribute to improved rhythm control outcomes. The inclusion of weight management and metabolic syndrome-related indicators is justified by the finding that recurrence rates range from 35% to 37% in patients with a BMI < 35 kg/m2, while recurrence rates significantly increase in patients with a BMI ≥ 35 kg/m2.26 Psychological factors like anxiety and depression may worsen AF prognosis. A meta-analysis of five cohort studies found anxiety to be an independent factor increasing the risk of AF recurrence after catheter ablation by 2.36-fold.27 Recurrence occurring during the post-ablation window may further undermine patient confidence,28 exacerbate emotional distress, and reduce adherence to rehabilitation behaviors. The inclusion of mental health and social support indicators suggests that post-ablation follow-up may need to address psychosocial as well as physiological dimensions.Sleep disorders are common after ablation and may interact bidirectionally with AF. Sleep-disordered breathing has been identified as an intervenable risk factor for AF,29 with screening facilitating early detection and intervention. Exercise after catheter ablation has been associated with reduced AF recurrence and improved left atrial structure and function.30,31 However, adherence to post-ablation exercise rehabilitation has been reported to be as low as 51%, highlighting the need to monitor exercise-related indicators during follow-up.32
Implications for Multidisciplinary Follow-Up
The proposed indicator system may provide a preliminary structure for multidisciplinary follow-up after AF ablation. By clarifying follow-up content across different domains, it may support communication among electrophysiologists, cardiologists, nurses, general practitioners, and pharmacists. For nursing practice, the indicators may also offer a more structured basis for discharge education, medication review, symptom assessment, and counselling on modifiable risk factors. At the same time, the practical value of the system is likely to depend on staffing, workload, digital infrastructure, and the availability of multidisciplinary collaboration. Not all indicators may be equally feasible or necessary at every stage of follow-up, highlighting the need for further work on prioritisation and workflow integration.
Limitations
The indicator system developed in this study was primarily based on expert consensus and has not yet been empirically weighted or prioritised. In routine clinical practice, full implementation of all 38 third-level indicators may be challenging because of time constraints, limited healthcare resources, and differences in follow-up contexts across institutions. In the absence of a clearly defined core indicator set, the practical utility of the complete framework within busy clinical workflows remains to be established. In addition, this study did not assess the feasibility or acceptability of the indicator system from the perspective of frontline clinicians and nurses who would ultimately use it in practice. The expert panel, although geographically diverse, was relatively small (n = 23) and recruited via convenience sampling, which may have introduced selection bias. Moreover, nursing experts (n = 16, 69.6%) outnumbered cardiovascular clinicians (n = 7, 30.4%), which may have influenced the range of perspectives represented and may not fully reflect the priorities and implementation constraints encountered by frontline nurses and community-based practitioners.
Given these limitations, future research should focus on several areas. Methods such as the analytic hierarchy process may be used to assign weights to indicators and identify a more concise core indicator set, thereby improving the applicability of the system across different clinical settings. Prospective studies are also needed to evaluate the feasibility, acceptability, and degree of integration of the indicator system within routine post-ablation follow-up workflows. In addition, the reliability and validity of both individual indicators and the overall framework should be further examined. Future research may also explore whether implementation of the indicator system is associated with improvements in outcomes such as anticoagulation adherence, symptom control, risk-factor management, and quality of life. Continuous refinement through bidirectional feedback from healthcare professionals and patients will be important for enhancing the clinical relevance and practical applicability of the system.
Conclusion
This Delphi study resulted in a preliminary, consensus-based indicator system for post-ablation AF follow-up, systematically grounded in the ABC pathway. The final system comprises 3 first-level, 9 second-level, and 38 third-level indicators and reflects structured expert consensus on follow-up content. By integrating stroke prevention, symptom management, and risk factor optimization, the framework may provide a basis for more structured multidisciplinary follow-up. Its feasibility, acceptability, and impact on patient outcomes require further investigation in prospective implementation studies.
Data Sharing Statement
All data generated or analyzed during this study are included in this publication.
Ethical Approval and Consent for Participation
This study was approved by the Medical Ethical Committee of Shanxi Bethune Hospital (YXLL-2024-019) and informed consent was obtained from the participants. This study was conducted in accordance with the Declaration of Helsinki.
Funding
This study was supported by the Science Foundation of Shanxi Bethune Hospital (No.: 2023YH30).
Disclosure
The authors state that they have no conflicts of interest in this work.
References
1. Martin SS, Aday AW, Almarzooq ZI, et al. Heart disease and stroke statistics: a report of US and global data from the American heart association. Circulation. 2024;149(8):e347–12. doi:10.1161/CIR.0000000000001209
2. Center For Cardiovascular Diseases The Writing Committee Of The Report On Cardiovascular H, Diseases In China N. Report on cardiovascular health and diseases in China 2023: an updated summary. Biomed Environ Sci. 2024;37(9):949–992. doi:10.3967/bes2024.162
3. Joglar JA, Chung MK, Armbruster AL, et al. 2023 ACC/AHA/ACCP/HRS guideline for the diagnosis and management of atrial fibrillation: a report of the American college of cardiology/American heart association joint committee on clinical practice guidelines. Circulation. 2024;149(1):e1–e156. doi:10.1161/CIR.0000000000001193
4. Burdett P, Lip GYH. Atrial fibrillation in the UK: predicting costs of an emerging epidemic recognizing and forecasting the cost drivers of atrial fibrillation-related costs. Eur Heart J Qual Care Clin Outcomes. 2022;8(2):187–194. doi:10.1093/ehjqcco/qcaa093
5. Al-Kaisey AM, Parameswaran R, Bryant C, et al. Atrial fibrillation catheter ablation vs medical therapy and psychological distress: a randomized clinical trial. JAMA. 2023;330(10):925–933. doi:10.1001/jama.2023.14685
6. Ngo L, Lee XW, Elwashahy M, et al. Freedom from atrial arrhythmia and other clinical outcomes at 5 years and beyond after catheter ablation of atrial fibrillation: a systematic review and meta-analysis. Eur Heart J Qual Care Clin Outcomes. 2023;9(5):447–458. doi:10.1093/ehjqcco/qcad037
7. Vermeer J, Vinck T, de Louw B, et al. Improving outcomes of AF ablation by integrated personalized lifestyle interventions: rationale and design of the prevention to improve outcomes of PVI (POP) trial. Clin Res Cardiol. 2023;112(6):716–723. doi:10.1007/s00392-023-02185-5
8. Blandino A, Bianchi F, Frankel DS, et al. Safety and efficacy of catheter ablation for ventricular tachycardia in elderly patients with structural heart disease: a systematic review and meta-analysis. J Interv Card Electrophysiol. 2021;66(1):179–192. doi:10.1007/s10840-021-01007-w
9. Lucà F, Abrignani MG, Oliva F, et al. Multidisciplinary approach in atrial fibrillation: as good as gold. J Clin Med. 2024;13(16):4621. doi:10.3390/jcm13164621
10. Hindricks G, Potpara T, Dagres N, et al. 2020 ESC guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): the task force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J. 2021;42(5):373–498. doi:10.1093/eurheartj/ehaa612
11. Lip GYH, Gue Y, Zhang J, Chao T-F, Calkins H, Potpara T. Stroke prevention in atrial fibrillation. Trends Cardiovasc Med. 2022;32(8):501–510. doi:10.1016/j.tcm.2021.10.001
12. Romiti GF, Proietti M, Vitolo M, et al. Clinical complexity and impact of the ABC (Atrial fibrillation Better Care) pathway in patients with atrial fibrillation: a report from the ESC-EHRA EURObservational Research Programme in AF general long-term registry. BMC Med. 2022;20(1):326. doi:10.1186/s12916-022-02526-7
13. Chao T-F, Joung B, Takahashi Y, et al. 2021 focused update of the 2017 consensus guidelines of the Asia Pacific Heart Rhythm Society (APHRS) on stroke prevention in atrial fibrillation. J Arrhythmia. 2021;37(6):1389–1426. doi:10.1002/joa3.12652
14. Lip GYH, Banerjee A, Boriani G, et al. Antithrombotic therapy for atrial fibrillation: CHEST guideline and expert panel report. Chest. 2018;154(5):1121–1201. doi:10.1016/j.chest.2018.07.040
15. Lip GYH. The ABC pathway: an integrated approach to improve AF management. Nat Rev Cardiol. 2017;14(11):627–628. doi:10.1038/nrcardio.2017.153
16. Noseworthy PA, Yao X, Deshmukh AJ, et al. Patterns of anticoagulation use and cardioembolic risk after catheter ablation for atrial fibrillation. J Am Heart Assoc. 2015;4(11). doi:10.1161/JAHA.115.002597
17. Chew D, Piccini JP. Long-term oral anticoagulant after catheter ablation for atrial fibrillation. Europace. 2021;23(8):1157–1165. doi:10.1093/europace/euaa365
18. Karasoy D, Gislason GH, Hansen J, et al. Oral anticoagulation therapy after radiofrequency ablation of atrial fibrillation and the risk of thromboembolism and serious bleeding: long-term follow-up in nationwide cohort of denmark. Eur Heart J. 2015;36(5):307–14a. doi:10.1093/eurheartj/ehu421
19. Salmasi S, Loewen PS, Tandun R, Andrade JG, De Vera MA. Adherence to oral anticoagulants among patients with atrial fibrillation: a systematic review and meta-analysis of observational studies. BMJ Open. 2020;10(4):e034778. doi:10.1136/bmjopen-2019-034778
20. Pham PN, Brown JD. Real-world adherence for direct oral anticoagulants in a newly diagnosed atrial fibrillation cohort: does the dosing interval matter? BMC Cardiovasc Disord. 2019;19(1):64. doi:10.1186/s12872-019-1033-3
21. Van Gelder IC, Rienstra M, Bunting KV, et al. 2024 ESC Guidelines for the management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2024;45(36):3314–3414. doi:10.1093/eurheartj/ehae176
22. Ahmad OM, Ibrahim R, Odunsi DI, et al. Role of mobile health and wearable devices in cardiovascular disease prevention: a comprehensive review. Cureus. 2025;17(5):e83673. doi:10.7759/cureus.83673
23. Hobensack M, Zhao Y, Scharp D, Volodarskiy A, Slotwiner D, Reading Turchioe M. Characterising symptom clusters in patients with atrial fibrillation undergoing catheter ablation. Open Heart. 2023;10(2):e002385. doi:10.1136/openhrt-2023-002385
24. Giskes K, Lowres N, Orchard J, et al. Increasing screening for atrial fibrillation in general practice: the Atrial Fibrillation Self-Screening, Management And guideline-Recommended Therapy (AF Self-SMART) study. Med J Aust. 2023;218(1):27–32. doi:10.5694/mja2.51803
25. Shantsila E, Choi E-K, Lane DA, Joung B, Lip GYH. Atrial fibrillation: comorbidities, lifestyle, and patient factors. Lancet Regional Health Euro. 2024;37:100784. doi:10.1016/j.lanepe.2023.100784
26. Tabaja C, Younis A, Santageli P, et al. Impact of obesity on catheter ablation of atrial fibrillation: patient characteristics, procedural complications, outcomes, and quality of life. J Cardiovasc Electrophysiol. 2023;34(8):1648–1657. doi:10.1111/jce.15987
27. Du H, Yang L, Hu Z, Zhang H. Anxiety is associated with higher recurrence of atrial fibrillation after catheter ablation: a meta-analysis. Clin Cardiol. 2022;45(3):243–250. doi:10.1002/clc.23753
28. Risom SS, Fevejle Cromhout P, Overgaard D, Hastrup Svendsen J, Kikkenborg Berg S. Effect of rehabilitation on sleep quality after ablation for atrial fibrillation: data from a randomized trial. J Cardiovasc Nurs. 2018;33(3):261–268. doi:10.1097/JCN.0000000000000476
29. Deshmukh A, Covassin N, Dauvilliers Y, Somers VK. Sleep disruption and atrial fibrillation: evidence, mechanisms and clinical implications. Circ Res. 2025;137(5):788–808. doi:10.1161/CIRCRESAHA.125.325612
30. Buckley BJR, Risom SS, Boidin M, Lip GYH, Thijssen DHJ. Atrial fibrillation specific exercise rehabilitation: are we there yet? J Pers Med. 2022;12(4):610. doi:10.3390/jpm12040610
31. Elliott AD, Verdicchio CV, Mahajan R, et al. An exercise and physical activity program in patients with atrial fibrillation. JACC Clin Electrophysiol. 2023;9(4):455–465. doi:10.1016/j.jacep.2022.12.002
32. Risom SS, Zwisler A, Sibilitz KL, et al. Cardiac Rehabilitation for Patients Treated for Atrial Fibrillation With Ablation Has Long-Term Effects: 12-and 24-Month Follow-up Results From the Randomized CopenHeartRFA Trial. Arch Phys Med Rehabil. 2020;101(11):1877–1886. doi:10.1016/j.apmr.2020.06.026
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.