Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Construction of a Management Plan for Physical Activity Symptom Clusters in Hospitalized Stroke Patients
Received 6 November 2025
Accepted for publication 3 February 2026
Published 11 February 2026 Volume 2026:19 579511
DOI https://doi.org/10.2147/JMDH.S579511
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Veronica Swallow
Jialing Zhou,1 Jinxiu Li,1 Jianghong Tan2
1School of Medicine, Jishou University, Jishou, Hunan, People’s Republic of China; 2Department of Medical Education, Zhuzhou Central Hospital, Zhuzhou, Hunan, People’s Republic of China
Correspondence: Jianghong Tan, Email [email protected]
Objective: To construct a scientifically sound and reliable management protocol for the physical activity symptom clusters in hospitalized stroke patients, based on the Symptom Management Theory (SMT).
Methods: This methodological study employed a multi-step approach. First, a preliminary protocol was drafted based on a systematic literature review and best evidence summary. Second, a two-round Delphi expert consultation process was conducted to refine and validate the protocol. Statistical analysis included calculating the positive coefficient, authority coefficient (Cr), coefficient of variation (CV), and Kendall’s coefficient of concordance (W).
Results: Fifteen experts completed both consultation rounds. The expert positivity rates were 83.33% and 100%, respectively. The authority coefficients (Cr) were 0.89 and 0.91. The first round yielded a CV of 0.00– 0.14 and a Kendall’s W of 0.195 (P < 0.05). The second round yielded a CV of 0.00– 0.11 and a Kendall’s W of 0.160 (P < 0.05). The final protocol comprised 3 first-level domains, 14 second-level domains, and 31 third-level items, organized within the SMT framework of symptom experience, management strategies, and outcomes.
Conclusion: The developed management protocol for the management protocol demonstrates strong scientific validity, reliability, and practical applicability. It serves as a valuable tool for healthcare professionals to develop personalized care plans, potentially enhancing rehabilitation outcomes and quality of life for stroke patients. Future studies are required to test its efficacy in multi-center trials.
Keywords: stroke, symptom clusters, symptom management, Delphi
Introduction
Stroke, a prevalent central nervous system injury, is characterized by high incidence, disability, mortality, recurrence rates, and substantial economic burden.1 In China, epidemiological data report approximately 3.9 million prevalent cases, with an age-standardized incidence rate of 200 per 100,000 and a prevalence of 1468.9 per 100,000.2 Stroke survivors frequently endure multiple co-occurring symptoms across the disease trajectory (acute, recovery, and chronic phases), with an average of over ten concurrent physical, cognitive, and psychological symptoms.3,4 These symptoms often interact synergistically, amplifying the overall disease burden.5–7 Common consequences include diminished activities of daily living (ADL), reduced quality of life, and plateaued functional recovery during later stages. Consequently, accurate symptom identification and optimized management during hospitalization are critical for precise symptom cluster intervention.Current symptom management practices for hospitalized stroke patients often focus on isolated symptoms or rely predominantly on patients’ immediate subjective complaints, lacking systematic strategies informed by the inherent interrelationships among symptoms. While contemporary approaches like network analysis offer novel pathways for identifying core symptom clusters,8 few studies have progressed to developing comprehensive management protocols based on these insights. Our preceding symptom network analysis identified a distinct Physical Activity Symptom Clusters, encompassing paralysis, imbalance, hand dysfunction, and ambulation difficulties. This study aims to construct a standardized management protocol targeting this symptom cluster based on the Symptom Management Theory (SMT).9 This theoretical framework emphasizes holism, dynamism, and contextualization. Its core principle lies in not treating symptoms as isolated issues but rather focusing on the complex interactions among symptoms themselves, as well as between symptoms and the individual and their environment. This aligns closely with the intrinsic characteristics of the identified physical activity symptom cluster in this study. Applying SMT will ensure the scientific rigor and structural integrity of the intervention measures, providing a solid theoretical foundation for achieving precise and efficient management of stroke symptom clusters.
Methods
Study Design
1) establishment of a research team, 2) development of a preliminary protocol via evidence synthesis evidence synthesis, and 3) refinement and validation through a two-round Delphi expert consultation expert consultation.
Research Team
Formation An 8-member research team was established, comprising 2 master’s supervisors, 2 associate chief nurses from neurology, 1 rehabilitation therapist, and 2 postgraduate nursing students. Responsibilities included literature retrieval, screening, data extraction, and evidence summarization. The study received approval from the institutional Medical Ethics Committee.
Preliminary Protocol Development
Theoretical Framework
The Symptom Management Theory (SMT) served as the foundational framework.9 The SMT model conceptualizes symptom management through management through three interconnected components: Symptom Experience, Management Strategies, and Outcomes.
Literature Search and Evidence Synthesis
A systematic literature search was conducted from the inception of relevant databases up until March 2025, spanning multiple databases such as PubMed, CINAHL, Web of Science, Embase, CNKI, Wanfang, and VIP, along with guideline repositories including UpToDate, BMJ Best Practice, NICE, SIGN, and Yimaitong. To ensure comprehensive coverage of the research topic, the search strings were meticulously constructed by combining Medical Subject Headings (MeSH) terms with free-text words. The exact search terms used were (“Stroke” OR “Cerebrovascular Apoplexy” OR “Cerebrovascular Accident” OR “Brain Vascular Accident” OR “Cerebrovascular Stroke” OR “Apoplexy” OR “Cerebral Stroke”) AND (“Paralysis” OR “Hemiplegia” OR “Hemiparesis” OR “Hand Dysfunction” OR “Hand Function” OR “Walking Ability” OR “Gait Disorder” OR “Balance” OR “Postural Control”) AND (“management” OR “intervention” OR “rehabilitation”) AND (“guideline” OR “systematic review” OR “recommendation” OR “evidence summar*” OR “randomized controlled trial*”). Initially, a total of 5,598 records were identified through these database searches. Following a rigorous screening process based on predefined inclusion criteria, 17 publications were deemed eligible and subsequently utilized for evidence extraction and summary. (The evidence summary can be found in Supplementary Material 1).
Drafting the Initial Protocol
Integrating the SMT framework with synthesized best evidence, a preliminary draft protocol was created. The initial draft encompassed 3 first-level, 13 second-level, and 30 third-level indicators. Functional activity management was stratified according to BrunnstromI-V.10
Delphi Expert Consultation Expert Consultation
Expert Selection
The Delphi method requires that the selected expert panel possesses both authority and representativeness, with rich theoretical knowledge and clinical practical experience in the research field. Generally, the number of experts selected ranges from 15 to 50 individuals.11 The criteria were as follows: 1) Professional engagement in stroke diagnosis, treatment, neurological nursing, or nursing management; 2) Bachelor’s degree or higher; 3) Intermediate professional title or above; 4) ≥10 years of relevant experience; 5) Willingness to participate. Eighteen experts were initially invited.
Consultation Procedure
Two rounds of Delphi consultation were conducted between June and September 2025 via online and paper-based questionnaires. The first-round questionnaire included the draft protocol, with experts rating the importance of each item on a 5-point Likert scale. Feedback and statistical analysis from the first round informed revisions and the creation of the second-round questionnaire. Consensus was achieved after two rounds (A portion of the survey questionnaires used in this study is provided in Supplementary Material 2).
Data Analysis Statistical analyses were performed using SPSS 26.0. Descriptive statistics summarized expert demographics. The positivity coefficient was measured by the effective questionnaire return rate. The authority coefficient (Cr) was calculated as (Ca + Cs)/2, where Ca represents the judgment basis and Cs signifies familiarity with the topic. Cr ≥ 0.7 indicated acceptable authority. The degree of consensus was assessed using the Coefficient of Variation (CV = SD/Mean) and Kendall’s W.12 Lower CV and higher Kendall’s W values indicated stronger consensus. Item retention criteria were: mean importance score > 3.5, CV < 0.25, and full score ratio > 20%. Qualitative suggestions were reviewed thematically.
Quality Control Measures included evidence-based draft development, strict adherence to expert selection criteria, pre-consultation communication, and dual independent data entry.
Results
Expert Demographics
Fifteen experts participated in both rounds. They represented five provinces across China, specializing in clinical medicine, rehabilitation therapy, and nursing management. Details are presented in Table 1.
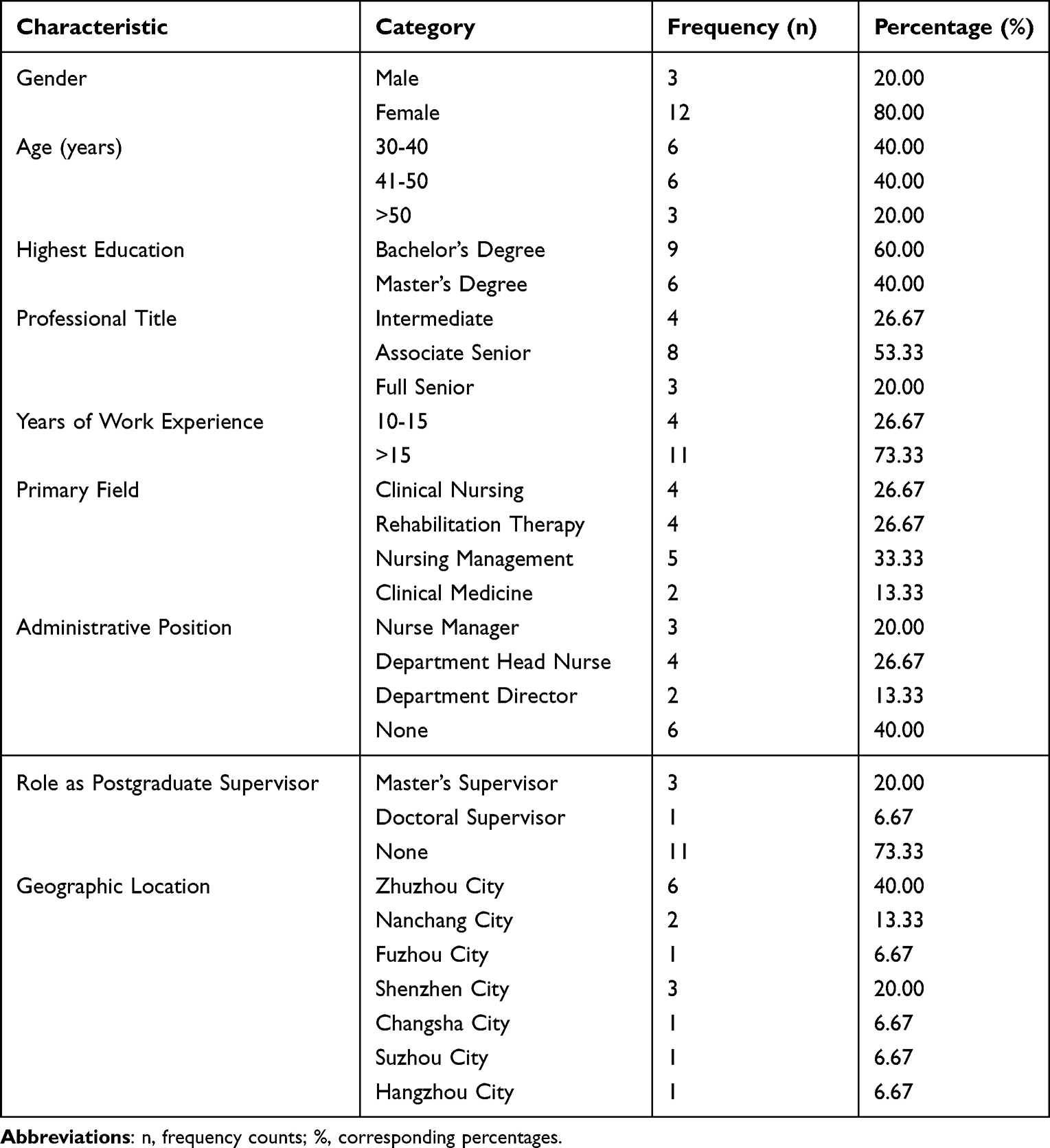 |
Table 1 Demographic Characteristics of the Expert Panel (n=15) |
Expert Positivity and Authority
The effective questionnaire return rates were 83.33% (Round 1) and 100% (Round 2). Eleven (73.33%) and three (20.00%) experts provided written suggestions in Rounds 1 and 2, respectively, indicating high engagement.(See Supplementary Material 3 for expert opinions). The authority coefficients (Cr) were 0.89 (Round 1) and 0.91 (Round 2), demonstrating high expertise. See Tables 2 and 3.
 |
Table 2 Expert Positivity and Response Rates |
 |
Table 3 Expert Authority Coefficients |
Expert Consensus Level
All Kendall’s W values in both rounds were statistically significant (P < 0.05), and all CVs were below 0.25, confirming good coordination and reliability of the results. See Table 4. (Detailed item-level data can be found in Supplementary Material 4) The observable declining trend of Kendall’s W values across the rounds in the table may stem from a gradual reduction in the level of agreement or consensus among raters or participants as the assessment or decision-making process unfolds, or from participant fatigue that affects the consistency of their judgments.
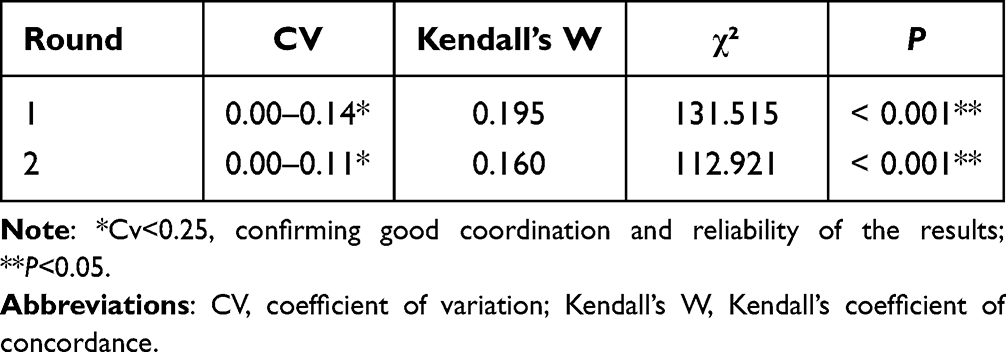 |
Table 4 Degree of Expert Consensus |
Final Protocol
After two rounds of revision, the final management protocol was established, see Table 5. Consisting of 3 first-level domains, 14 second-level domains, and 31 third-level items. The core structure aligns with SMT:
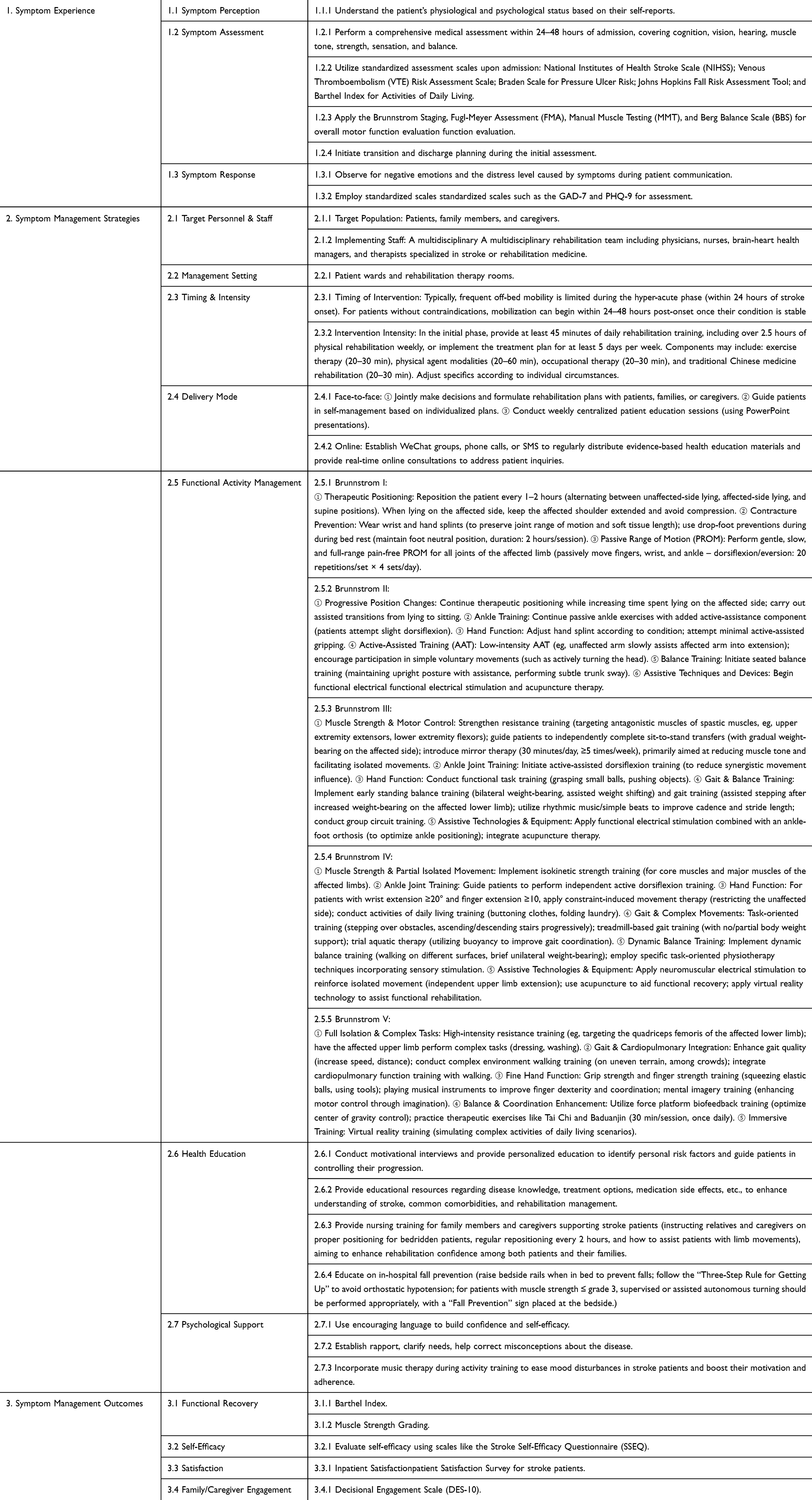 |
Table 5 Management Protocol for the Physical Activity Symptom Cluster in Hospitalized Stroke Patients |
Domain 1: Symptom Experience (Perception, Assessment, Response).
Domain 2: Symptom Management Strategies (Personnel, Setting, Timing/Intensity, Delivery Mode, Functional Activity Management by Brunnstrom Stage, Health Education, Psychological Support).
Domain 3: Symptom Management Outcomes (Functional Recovery, Self-Efficacy, Satisfaction, Family Engagement).
Discussion
Scientific Rigor of the Protocol
During the evidence-based research phase, the research team used the PIPOST framework to define relevant research questions and systematically searched domestic and international literature databases (including PubMed, CINAHL, Web of Science, Embase, CNKI, Wanfang, VIP), guideline repositories (such as UpToDate, BMJ Best Practice, NICE, SIGN, Yimaitong) and professional websites related to the topic to gather literature evidence addressing the research problems, ensuring comprehensiveness and timeliness of evidence sources. Each piece of evidence, its grading level, and corresponding recommendations were determined through thorough discussions among project team members, strictly following the JBI Evidence Pre-Grading System, recommendation hierarchy, and principles for rating evidence strength. The findings were ultimately summarized into three aspects: symptom experience, symptom management strategies, and symptom management outcomes. A total of 41 best-practice recommendationsractice recommendations were identified. These pieces of evidence are comprehensive and substantial, providing a scientific basis for developing a core symptom cluster management protocol for hospitalized stroke patients. In the protocol development phase, the study adopted the Symptom Management Theory as its theoretical foundation. This theory focuses on key elements encapsulated elements encapsulated in the 5W2H approach, enabling a holistic understanding of patients’ physiological and psychological conditions associated with symptoms, as well as areas requiring intervention. Building on prior literature review, identification of core symptom clusters, and synthesis of best evidence, the research team conducted multiple internal discussions and utilized the Delphi expert consultation method. Experts from various fields—including neurology, rehabilitation medicine, and nursing science—were invited to review and refine the initially proposed indicators. This process not only validated the feasibility and appropriateness of the evidence in clinical contexts but also integrated cutting-edge evidence with practical experience from senior specialists, thereby establishing a rational and scientifically sound management protocol for the physical activity symptom cluster in hospitalized stroke patients.
Reliability and Validity
This study focused on developing a management protocol for the physical activity symptom cluster in hospitalized stroke patients, strictly adhering to the standardized procedures of the Delphi expert consultation method. While ensuring scientific validity and rationality, it also fully considered clinical practicality. The reliability of this method primarily depends on the expertise, knowledge base, and practical experience of the involved panelists. A total of 15 experts from seven cities across five provinces in China were invited to participate in the consultation. Their specialties covered neurology, rehabilitation medicine, and nursing management. All experts had over ten years of relevant work experience and possessed substantial expertise in stroke clinical diagnosis and treatment, rehabilitation intervention, and care management, enabling them to provide feasible practical recommendations for the protocol content. Moreover, these experts have long been engaged in research and clinical practice related to stroke, equipping them with solid theoretical foundations that strongly supported the content validity and scientific rigor of the protocol. During the consultation process, the effective response rates for the two rounds were 83.33% and 100%, respectively, reflecting strong expert engagement and cooperation. The proportions of experts providing suggestions providing suggestions were 73.33% and 20%, indicating active feedback in the first round and convergence of opinions toward consensus in the second. Additionally, the expert authority coefficients were 0.89 and 0.91 for the respective rounds, demonstrating high academic influence and judgment credibility in the field. In the first round, the coefficient of variation (CV) for all items ranged from 0.00 to 0.14, and Kendall’s W was 0.195 (P < 0.001). By the second round, the CV narrowed to a range of 0.00–0.11, and Kendall’s W was 0.160 (P < 0.001). These data indicate satisfactory concentration and coordination of expert opinions, with further improved consensus and enhanced stability and consistency of the results after two iterative rounds.Therefore, through a rigorous Delphi process, a high-caliber expert panel, robust participation and authority, along with highly consistent opinion integration, the management protocol developed in this study demonstrates strong methodological scientificity and reliability, laying a solid foundation for subsequent clinical practice and application.
Implications for Clinical Practice
Physical activity impairment represents one of the central challenges in the rehabilitation of stroke patients. Such symptoms frequently manifest in clusters and interact with one another.13 A significant positive correlation between symptom clusters such as limb deformity and pain and patients’ illness uncertainty: the greater the number and severity of symptoms, the stronger the patients’ uncertainties tend to be regarding disease progression, treatment efficacy, and prognosis.14 This sense of uncertainty not only increases psychological burden psychological burden but may also translate into notable healthcare-seeking pressure, potentially leading to reduced compliance, interruption of the rehabilitation process, and compromised overall recovery outcomes.15 To alleviate functional limitations and physical and emotional distress in stroke patients, researchers globally continue to explore scientifically sound and effective symptom management strategies. Substantial evidence supports that implementing individualized and comprehensive interventions for functional deficits effectively alleviates suffering, promotes restoration of physical and psychological functions, and significantly enhances quality of life.16,17 In the field of stroke rehabilitation, existing studies have confirmed the effectiveness of various single or combined interventions (such as music therapy and Tai Chi,virtual reality technology) in improving overall or specific functions.18–20 However, these studies generally follow a “method-to-outcome” paradigm, often treating patient symptoms as homogeneous wholes or isolated items, rather than using the actual interrelated symptom clusters experienced by patients as the analytical unit and starting point for intervention. This “method-driven” approach tends to lead to a mismatch between interventions and the complex, heterogeneous clinical phenotypes of patients. Therefore, this study emphasizes the need for a paradigm shift in symptom management—from focusing on diseases or methods to targeting patient symptom clusters. The new strategy advocates assessment-first, systematically evaluating and precisely identifying individualized symptom clusters structures, and then dynamically integrating and matching intervention modules accordingly. This model enhances the targeting of assessments by accurately identifying core sources of distress, improves the precision of interventions by selecting synergistic measures based on common mechanisms of symptom clusters—achieving multiple targets with one integrated plan—and promotes dynamic management by allowing continuous adjustments according to the evolution of symptom clusters throughout the rehabilitation process. Particularly during hospitalization, there is no standardized, structured clinical pathway for managing core symptom clusters in stroke patients, nor is there a dynamic adjustment mechanism based on both symptom-clusters characteristics and individual patient differences. Therefore, developing a systematic and precise management protocol management protocol for core symptom clusters in hospitalized stroke patients has become a crucial direction in contemporary clinical rehabilitation and research.Within this context, the present study employed the Symptom Management Theory as a framework and integrated evidence‐based medical findings to construct a structured, scientific, and clinically applicable management protocol for core symptom clusters in this population. The protocol comprises three core components: symptom experience assessment, symptom management strategies, and outcome evaluation. During the assessment stage, the protocol specifies critical symptomatic manifestations and introduces concise yet valid standardized assessment tools to enable rapid identification and quantification of symptom-clusters profiles. Regarding management strategies, the program specifically targets the physical activity symptom clusters. It stratifies functional activity into stages and defines corresponding activity training methods for each stage, thereby strengthening the relevance and operability of the measures implemented measures implemented. The outcome evaluation module is designed for ongoing monitoring of effectiveness, forming a closed-loop management system. With its coherent architecture and emphasis on key issues, the overall protocol aims to offer healthcare professionals a practical and standardized operational guide. Ultimately, it seeks to enhance motor function, relieve symptom burden, and further improve patients’ quality of life and rehabilitation prognosis.
Conclusion
Based on preliminary work and grounded in the Symptom Management Theory, this study constructed a symptom clusters management protocol for stroke patients. The protocol demonstrates sound scientific validity, reliability, and practicability, which can effectively elevate rehabilitation standards and ameliorate the quality of life among individuals with stroke. It offers theoretical support and practical guidance for healthcare providers in formulating individualized health management plans. But this study involved only Chinese experts in the two-round Delphi consultation process. Although these experts possess considerable authority in the relevant field, their perspectives may not fully represent the breadth of views and experiences regarding the management of physical activity symptom clusters in hospitalized stroke patients across the broader healthcare landscape. Differences in clinical practices and conceptual approaches may exist among experts from diverse regions and healthcare institutions. Future research could benefit from including a more diverse panel of experts from various geographical areas and hospital tiers. Additionally, exploring international expert collaboration could help integrate advanced management experiences and techniques from other countries, thereby further refining the management protocol. Moreover, although the developed management protocol has undergone expert consultation and theoretical validation, it has not yet been subjected to large-scale practical verification in real-world clinical settings. Given the significant individual variability among patients and the complex, dynamic nature of clinical practice, unforeseen challenges may arise during the protocol’s implementation. Its effectiveness and feasibility require further validation through clinical application. Future efforts should involve multi-center, large-sample clinical studies to comprehensively evaluate the efficacy and feasibility of the protocol. By implementing it in actual clinical environments, collecting patient feedback, promptly identifying existing issues, and making necessary adjustments and optimizations, a solid practical foundation can be established for its broader promotion and application.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tu WJ, Wang LD. Special Writing Group of China Stroke Surveillance Report. China stroke surveillance report 2021. Mil Med Rese. 2023;10(1):33. doi:10.1186/s40779-023-00463-x
2. The WCOTROCHADIC. The WCOTROCHADIC. Report on Cardiovascular Health and Diseases in China 2022: an Updated Summary. Biomed Environ Sci. 2023;36(8):669–11. doi:10.3967/bes2023.106
3. Ashaie SA, Funkhouser CJ, Jabbarinejad R, Cherney LR, Shankman SA. Longitudinal trajectories of post-stroke depression symptom subgroups. Neurorehabil Neural Repair. 2023;37(1):46–52. doi:10.1177/15459683221143464
4. Oestreich LKL, Lo JW, Di Biase MA, et al. Network analysis of neuropsychiatric, cognitive, and functional complications of stroke: implications for novel treatment targets. Psychiatry Clin Neurosci. 2024;78(4):229–236. doi:10.1111/pcn.13633
5. Krick S, Koob JL, Latarnik S, et al. Neuroanatomy of post-stroke depression: the association between symptom clusters and lesion location. Brain Commun. 2023;5(5):fcad275. doi:10.1093/braincomms/fcad275
6. Weaver NA, Kuijf HJ, Aben HP, et al. Strategic infarct locations for post-stroke cognitive impairment: a pooled analysis of individual patient data from 12 acute ischaemic stroke cohorts. Lancet Neurol. 2021;20(6):448–459. doi:10.1016/S1474-4422(21)00060-0
7. Wong A, Lau AY, Yang J, et al. Neuropsychiatric symptom clusters in stroke and transient ischemic attack by cognitive status and stroke subtype: frequency and relationships with vascular lesions, brain atrophy and amyloid. PLoS One. 2016;11(9):e0162846. doi:10.1371/journal.pone.0162846
8. Fried EI, Boschloo L, Van Borkulo CD, et al. Symptomics as a new research paradigm for psychiatry. Front Psychiatry. 2015;6:1–3. doi:10.3389/fpsyt.2015.00117
9. Humphreys JLK, Carrieri-Kohlman V, Puntillo K, et al.Theory of symptom management.Middle Range Theory for Nursing.
10. Huang CY, Lin GH, Huang YJ, et al. Improving the utility of the Brunnstrom recovery stages in patients with stroke: validation and quantification. Medicine. 2016;95(31):e4508. doi:10.1097/MD.0000000000004508
11. Keeney S, Hasson F, McKenna H. The Delphi Technique in Nursing and Health Research. Wiley-Blackwell; 2011; doi:10.1002/9781444392029
12. Boulkedid R, Abdoul H, Loustau M, Sibony O, Alberti C. Using and reporting the Delphi method for selecting healthcare quality indicators: a systematic review. PLoS One. 2011;6(6):e20476. doi:10.1371/journal.pone.0020476
13. Shi D, Li Z, Yang J, Liu BZ, Xia H. Symptom experience and symptom burden of patients following first-ever stroke within 1 year: a cross-sectional study. Neural Regen Res. 2018;13(11):1907–1912. doi:10.4103/1673-5374.239440
14. Dong X, Yang S, Guo Y, Lv P, Liu Y. Exploring psychoneurological symptom clusters in acute stroke patients: a latent class analysis. J Pain Res. 2022;15:789–799. doi:10.2147/JPR.S350727
15. Katzan IL, Schuster A, Daboul L, et al. Changes in health-related quality of life after transient ischemic attack. JAMA Netw Open. 2021;4(7):e2117403. doi:10.1001/jamanetworkopen.2021.17403
16. Song R, Park M, Jang T, Oh J, Sohn MK. Effects of a tai chi-based stroke rehabilitation program on symptom clusters, physical and cognitive functions, and quality of life: a randomized feasibility study. Int J Environ Res Public Health. 2021;18(10):5453. doi:10.3390/ijerph18105453
17. Kankam K, Murray L. Rehabilitation of post-stroke aphasia in Ghana. Int J Lang Commun Disord. 2024;59(4):1308–1321. doi:10.1111/1460-6984.13000
18. Raglio A, Zaliani A, Baiardi P, et al. Active music therapy approach for stroke patients in the post-acute rehabilitation. Neurol Sci. 2017;38(5):893–897. doi:10.1007/s10072-017-2827-7
19. Lyu D, Lyu X, Zhang Y, et al. Tai chi for stroke rehabilitation: a systematic review and meta-analysis of randomized controlled trials. Front Physiol. 2018;9:983. doi:10.3389/fphys.2018.00983
20. Prajjwal P, Chandrasekar KK, Battula P, et al. The efficacy of virtual reality-based rehabilitation in improving motor function in patients with stroke: a systematic review and meta-analysis. Ann Med Surg. 2024;86(9):5425–5438. doi:10.1097/MS9.0000000000002403
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.