Back to Journals » Risk Management and Healthcare Policy » Volume 19
Construction and Validation of a Nomogram Prediction Model for Recurrent Lumbar Disc Herniation After Percutaneous Endoscopic Lumbar Discectomy
Authors Jiang Z, Cui Z, Yang Y, Li H
Received 20 November 2025
Accepted for publication 4 March 2026
Published 13 March 2026 Volume 2026:19 578901
DOI https://doi.org/10.2147/RMHP.S578901
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Keon-Hyung Lee
Zeyu Jiang,1,* Ziying Cui,2,* Yiping Yang,1,* Haijun Li1
1Department of Orthopedics, The Affiliated Taizhou People’s Hospital of Nanjing Medical University, Taizhou School of Clinical Medicine, Nanjing Medical University, Taizhou, Jiangsu, People’s Republic of China; 2The Graduate School of Dalian Medical University, Dalian Medical University, Dalian, Liaoning, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Haijun Li, Department of Orthopedics, The Affiliated Taizhou People’s Hospital of Nanjing Medical University, Taizhou School of Clinical Medicine, Nanjing Medical University, No. 366 Taihu Road, Taizhou, Jiangsu, 225300, People’s Republic of China, Tel +86-13901436563, Fax +86-0523-86361510, Email [email protected]
Objective: To identify risk factors for recurrent lumbar disc herniation (rLDH) after percutaneous endoscopic lumbar discectomy (PELD) and to develop and internally validate a nomogram.
Methods: This retrospective, single-center study included 607 patients who underwent PELD between January 2018 and December 2023. Thirty candidate predictors were collected. Predictor selection was performed using least absolute shrinkage and selection operator (LASSO) regression, followed by multivariable logistic regression. A nomogram was constructed in accordance with the Transparent Reporting of a multivariable prediction model for Individual Prognosis Or Diagnosis (TRIPOD) recommendations. Discrimination was assessed using the area under the receiver operating characteristic curve (AUC); for a binary outcome, the concordance index (C-index) is numerically equivalent to the AUC and was therefore reported for internal validation. Calibration was evaluated using the Hosmer–Lemeshow test and calibration curves. Internal validation was conducted using bootstrap resampling (1,000 iterations) and 10-fold cross-validation. Decision curve analysis (DCA) was applied to evaluate clinical utility.
Results: During follow-up, 70 of 607 patients (11.5%) developed rLDH. Seven independent predictors were identified: postoperative activity, body mass index (BMI), smoking, ligamentum flavum (LF) thickness, sagittal range of motion (sROM), Modic change, and Pfirrmann grade. The nomogram achieved an AUC of 0.793 (95% CI: 0.736– 0.850) and good calibration (Hosmer–Lemeshow P = 0.668). Internal validation showed a C-index of 0.763 (95% CI: 0.682– 0.844) in bootstrap resampling and 0.775 in 10-fold cross-validation. The calibration curve showed close alignment with the ideal curve. DCA demonstrated favorable clinical utility of the model.
Conclusion: This internally validated nomogram integrates clinical and imaging predictors to provide individualized rLDH risk prediction after PELD. It may assist in identifying patients at higher risk of recurrence who could benefit from closer postoperative surveillance and individualized decision-making. External validation is warranted before broad clinical implementation.
Keywords: percutaneous endoscopic lumbar discectomy, recurrent lumbar disc herniation, nomogram prediction model, TRIPOD guideline, risk factor
Introduction
Lumbar disc herniation (LDH) is a common degenerative disorder of the lumbar spine. It usually causes low-back and leg pain, as well as sensorimotor deficits in the lower limbs. These symptoms can seriously affect daily activities and reduce the quality of life.1 When symptoms persist despite conservative management (eg, medication, rest, physical therapy/rehabilitation, and adjunct modalities such as laser therapy), surgical intervention is generally considered2,3 Compared with nonoperative care, surgical intervention can directly remove the extruded nucleus pulposus and markedly alleviate symptoms With advances in minimally invasive spine techniques, percutaneous endoscopic lumbar discectomy (PELD) has become increasingly established for the treatment of LDH. Relative to conventional open procedures, PELD offers shorter operative time, reduced intraoperative blood loss, and a shorter postoperative immobilization period.4
However, with the widespread adoption of PELD, postoperative recurrence has become a relatively common and challenging clinical complication, with an incidence ranging from approximately 3% to 18%.5,6 Recurrent lumbar disc herniation (rLDH) is defined as a reherniation at the same spinal level after lumbar discectomy that produces corresponding compressive symptoms following a pain-free interval, without a strict requirement for the duration of that interval.7,8 rLDH can exacerbate low-back and leg pain, and patients who do not respond well to conservative management may require revision surgery. Because the initial operation often induces local fibrosis and scar formation around the surgical site, revision surgery is typically more technically challenging than the primary procedure. This not only substantially elevates the risk of intraoperative complications, such as nerve injury, dural tears, and cerebrospinal fluid leakage, but also adds psychological and financial burdens to patients while consuming additional healthcare resources.8,9 Therefore, identifying and understanding the risk factors associated with rLDH has important clinical implications. Such knowledge may help reduce recurrence after PELD through risk-informed counseling and individualized perioperative management, and it can also support shared decision-making when discussing treatment strategies in selected patients, rather than prescribing a specific surgical approach.
Several prediction models and nomograms have been developed to estimate the risk of recurrent lumbar disc herniation after discectomy, with predictors commonly including demographic factors and baseline imaging markers of degeneration.10–13 However, these published models vary in candidate predictors and validation strategies, and few simultaneously integrate modifiable postoperative behavioral factors with dynamic instability and degenerative imaging parameters. In addition to regression-based nomograms, machine learning approaches have also been explored for LDH-related prediction tasks, reflecting growing interest in data-driven risk stratification.14 Accordingly, an additional comprehensively reported and internally validated model that integrates modifiable behavioral factors with degenerative and dynamic imaging features may further support individualized risk stratification, particularly in patients undergoing PELD.
Nomograms provide a user-friendly graphical representation of multivariable regression models and have been widely used for individualized risk prediction in clinical practice.15 Guided by the Transparent Reporting of a multivariable prediction model for Individual Prognosis Or Diagnosis (TRIPOD) recommendations for prediction model development and internal validation, we aimed to develop and internally validate an interpretable nomogram for rLDH after PELD by identifying independent clinical and imaging predictors and integrating multiple imaging parameters with modifiable clinical/behavioral factors. Dual internal validation (bootstrap resampling and 10-fold cross-validation) was performed to evaluate model stability and mitigate optimism bias in performance estimation.
Methods
Study Design and Participants
This retrospective observational study was conducted at a single tertiary center. Consecutive patients who underwent PELD for single-level LDH between January 2018 and December 2023 were screened. The minimum follow-up duration was 12 months. This study was developed and reported in accordance with the TRIPOD statement for prediction model development and internal validation; external validation was not performed.
Inclusion and Exclusion Criteria
Inclusion Criteria
(1) Clinical manifestations consistent with imaging findings supporting a diagnosis of LDH; (2) single-level LDH; (3) failure of standardized conservative treatment for at least 4 weeks; (4) complete clinical and imaging data.
Exclusion Criteria
(1) History of prior open lumbar surgery; (2) incomplete imaging data; (3) combined with significant spinal canal stenosis; (4) combined with lumbar spondylolisthesis; (5) far-lateral LDH; (6) sequestered LDH; (7) presence of definite surgical contraindications; (8) loss to follow-up or refusal to participate.
Data Collection
Demographic variables, comorbidities, perioperative parameters, postoperative activity level, and radiological characteristics were collected from medical records and follow-up evaluations. All surgeries were performed by the same spine surgery team to minimize surgeon-related variability. No missing data were observed for the outcome or included predictors; therefore, imputation was not performed.
The variables analyzed in this study included demographic characteristics, surgery-related data, and radiological factors. Demographic and surgical information comprised gender, age, course of disease, BMI, smoking, drinking, diabetes, hypertension, household registration type, high-risk occupation, postoperative activity, type of surgery, operation time, total protein, and albumin. Radiological factors included the level of herniated disc, herniation location, type of herniation, disc migration, Schmorl’s nodes, Modic change, Pfirrmann grade, lumbar lordosis angle (LL), intervertebral angle (IVA), disc height index (DHI), herniation base width, sagittal range of motion (sROM), scoliosis, ligamentum flavum (LF) thickness, and anterior vertebral osteophyte.
Imaging Assessment and Reliability
Radiological parameters were assessed using magnetic resonance imaging (MRI), computed tomography (CT) scans, and flexion–extension radiographs. Two spine surgeons independently assessed all imaging parameters and were blinded to recurrence status. Interobserver reliability was evaluated in a random subset of 60 patients. For continuous measurements (eg, LF thickness, sROM, LL, IVA, DHI, and herniation base width), intraclass correlation coefficients (ICC) were calculated using a two-way random-effects model with absolute agreement (ICC[2,1]) For categorical variables, Cohen’s κ was used for nominal variables and weighted κ for ordinal variables (eg, Modic type and Pfirrmann grade) Disagreements were resolved by consensus for the final dataset. Reliability was interpreted as poor (<0.50), moderate (0.50–0.75), good (0.75–0.90), or excellent (>0.90).
LF thickness and sROM were measured as illustrated in Figures 1 and 2; LF hypertrophy was defined as >4 mm and increased mobility as sROM ≥10°.16,17 Modic change and Pfirrmann grade were classified according to established criteria (Figures 3 and 4).
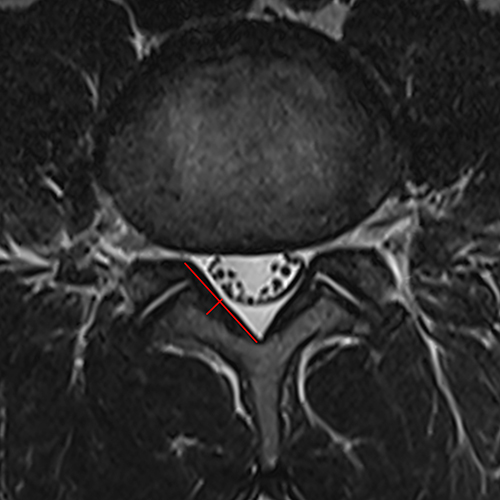 |
Figure 1 LF thickness was measured at the midpoint of the LF on axial MRI (red line indicates the measurement position). |
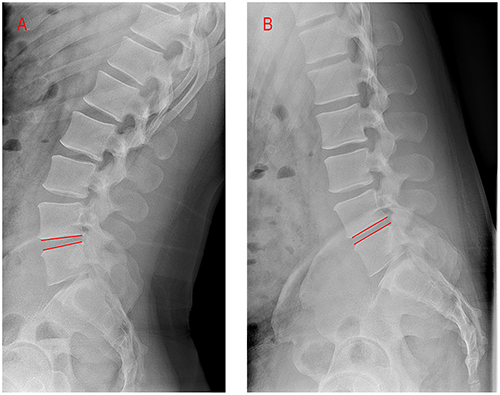 |
Figure 2 Measurement of the extension IVA (A) and flexion IVA (B); sROM was defined as the difference between the flexion and extension Cobb angles at the index level (red lines indicate the inferior endplate of the cranial vertebra and the superior endplate of the caudal vertebra used for Cobb angle calculation). |
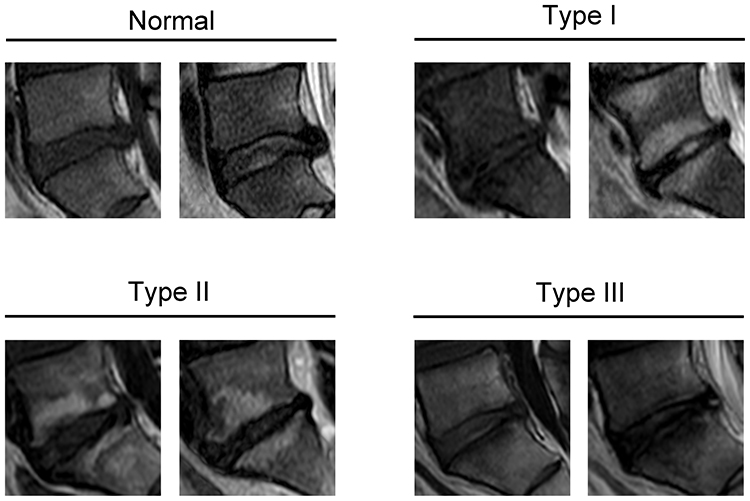 |
Figure 3 The classification of Modic change. On T1WI and T2WI images, normal: isointense on T1WI and T2WI. Type I, hypointense on T1WI and hyperintense on T2WI. Type II, hyperintense on T1WI and hyperintense or isointense on T2WI. Type III, hypointense on T1WI and T2WI. |
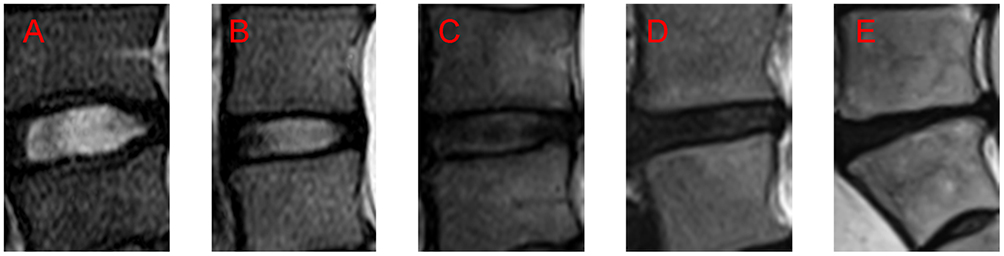 |
Figure 4 Pfirrmann grade classification on T2-weighted MRI. (A) Grade I normal disc structure and height with bright white, homogeneous high signal intensity. (B) Grade II: mildly inhomogeneous structure with normal disc height; white signal with a clear distinction between the nucleus and annulus. (C) Grade III: clearly inhomogeneous structure with normal or slightly decreased disc height; intermediate gray signal with an unclear nucleus–annulus distinction. (D) Grade IV: severely inhomogeneous structure with normal or moderately decreased disc height; dark gray, low signal intensity with loss of nucleus–annulus distinction. (E) Grade V severely disrupted disc with collapsed disc space; complete loss of the nucleus–annulus distinction. |
Postoperative Activity Assessment
Postoperative physical activity was assessed during the early postoperative period, defined as the first 3 months after surgery. Activity intensity was recorded at routine follow-up visits (or structured telephone follow-up when in-person visits were not feasible) at approximately 1 month and 3 months postoperatively. At the 1-month follow-up, patients reported their typical weekly activities during the preceding 4 weeks, including the type of activity, frequency, and duration. At the 3-month follow-up, patients reported activities during postoperative weeks 5–12. Each reported activity was assigned a metabolic equivalent of task (MET) value using the Compendium of Physical Activities described by Ainsworth et al18 For each patient, the highest-intensity activity performed regularly across the first 3 postoperative months was used to classify early postoperative activity intensity. Patients were dichotomized into two groups based on MET intensity: Low-intensity activity (< 6 METs), including light or moderate daily activities such as walking or light housework; High-intensity activity (≥ 6 METs), including vigorous activities such as brisk walking, running, or heavy manual labor. This threshold (6 METs) corresponds to the conventional boundary between moderate and vigorous activity as defined by the American College of Sports Medicine and has been applied in postoperative spine research.19,20
The study was approved by the Medical Ethics Committee of our hospital. Written informed consent was waived, and verbal informed consent was obtained as approved by the committee.
Statistical Analysis
Statistical analyses were performed using SPSS version 26.0 and R software version 4.5.1. Categorical variables were compared between groups using chi-square tests under the following conditions: the Pearson chi-square test was applied when the sample size was ≥40 and all expected frequencies were ≥5; the continuity-corrected chi-square test was used when the sample size was ≥40 but any expected frequency was <5; and Fisher’s exact test was adopted when the sample size was <40 or the minimum expected frequency was <1.
Model Development and Internal Validation (TRIPOD Workflow)
Step 1: Candidate predictors. Thirty candidate predictors were pre-specified based on clinical relevance and prior literature. No missing data were observed for the outcome or included predictors; therefore, imputation was not performed.
Step 2: Predictor selection. Least absolute shrinkage and selection operator (LASSO) logistic regression with 10-fold cross-validation was used for predictor selection. To obtain a more parsimonious model and reduce overfitting, the penalty parameter λ was selected using the 1-standard-error rule based on the cross-validated binomial deviance. Predictors with non-zero coefficients at the selected λ (λ_1se) were retained for subsequent multivariable logistic regression.
Overfitting control. Given the relatively limited number of recurrence events compared with the number of candidate predictors, penalization was used to limit model complexity. To mitigate optimism from fitting and evaluating the model in the same dataset, model performance was internally validated using bootstrap resampling (1,000 iterations) and 10-fold cross-validation, providing a more realistic assessment of model stability and generalizability.
Step 3: Final model and nomogram. Retained variables were entered into a multivariable logistic regression model to estimate odds ratios (ORs) with 95% confidence intervals (CIs). A nomogram was constructed based on the final regression coefficients to estimate the probability of recurrence.
Step 4: Model performance and validation. Discrimination was assessed using the area under the receiver operating characteristic curve (AUC). Model calibration was evaluated using calibration curves and the Hosmer–Lemeshow goodness-of-fit test. Internal validation was performed using bootstrap resampling (1,000 iterations) and 10-fold cross-validation. Clinical utility was assessed using decision curve analysis (DCA).
Results
Comparison of Clinical Characteristics Between the rLDH and Non-rLDH Groups
A total of 607 patients were included, with a follow-up duration ranging from 18 to 72 months. During follow-up, 70 patients developed rLDH, yielding a recurrence rate of 11.5%. Interobserver reliability was evaluated in a random subset of 60 patients and showed good agreement: for continuous imaging measurements, ICCs indicated good-to-excellent reliability, while for ordinal/categorical variables, Cohen’s κ/weighted κ also demonstrated good agreement (ICC range 0.81–0.93; κ/weighted κ range 0.83–0.87).
Significant differences between the rLDH and non-rLDH groups were observed for BMI, smoking status, postoperative activity level, Modic change, Pfirrmann grade, sROM, and LF thickness (all P < 0.05). All baseline characteristics are summarized in Table 1.
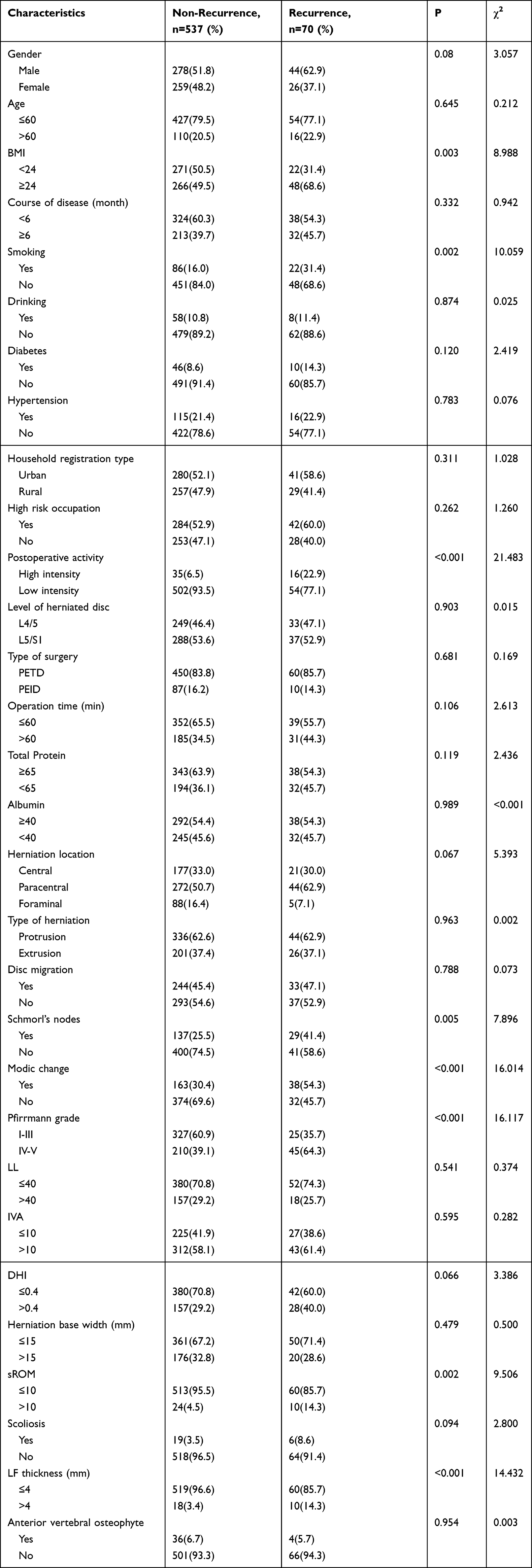 |
Table 1 Characteristics of Recurrence and Non-Recurrence Patients |
Construction of the Nomogram Prediction Model
Predictor selection was performed using LASSO logistic regression with 10-fold cross-validation. The penalty parameter was selected using the 1-standard-error rule based on the cross-validated binomial deviance (λ_1se = 0.0377), and predictors with non-zero coefficients at λ_1se were retained for multivariable logistic regression (Figure 5). Seven predictors with non-zero coefficients at λ_1se were retained, including postoperative activity level, BMI, smoking status, Modic change, Pfirrmann grade, sROM, and LF thickness. These variables were subsequently entered into a multivariable logistic regression model, and all seven remained independent predictors of rLDH (all P < 0.05). The corresponding ORs and CIs are presented in Table 2.
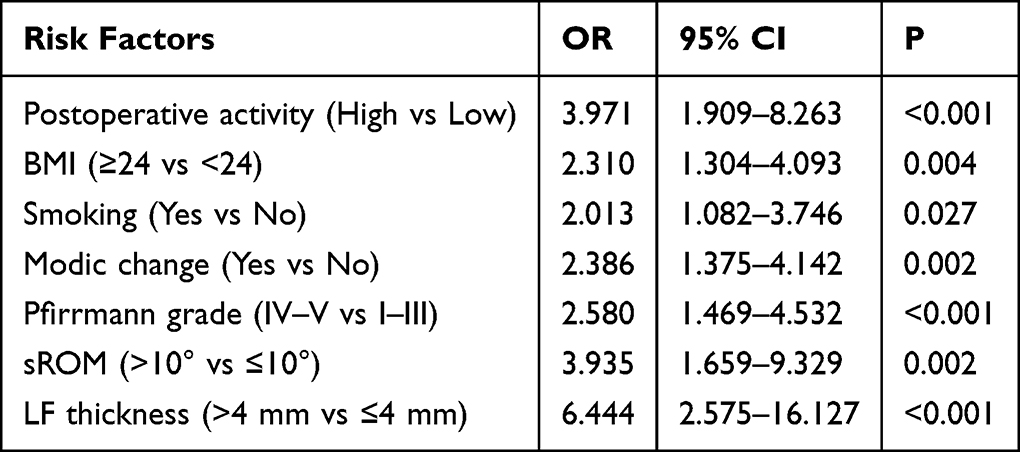 |
Table 2 Multivariate Logistic Regression Analysis of Risk Factors for rLDH After PELD |
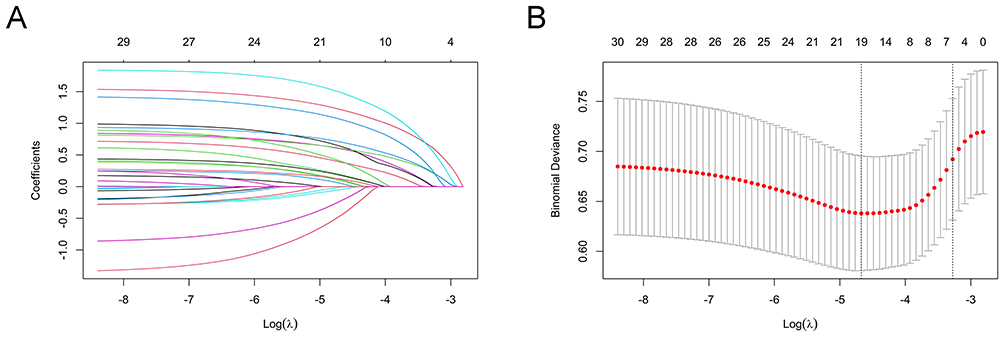 |
Figure 5 LASSO logistic regression for predictor selection. (A) Coefficient profiles of the 30 candidate predictors (each colored curve represents one predictor) plotted against log(λ). (B) 10-fold cross-validation curve of the binomial deviance. Red dots indicate the mean cross-validated deviance at each λ, and gray error bars represent ±1 standard error. The vertical dotted lines denote λ_min and λ_1se. Numbers above the plot indicate the number of predictors with non-zero coefficients at each λ. Predictors with non-zero coefficients at λ_1se were retained for subsequent multivariable logistic regression. |
From a clinical perspective, postoperative activity intensity, BMI, and smoking are modifiable predictors that can be targeted through risk-stratified rehabilitation guidance, weight management, and smoking cessation counseling. In contrast, LF thickness, sROM, Modic change, and Pfirrmann grade are objective imaging markers reflecting canal reserve, segmental stability, and degenerative burden, which may help identify patients who warrant closer surveillance and more individualized perioperative planning.
A nomogram model incorporating these seven risk factors was constructed to predict the probability of rLDH after PELD (Figure 6). In this model, each variable was assigned a specific score, and the sum of all scores yielded a total point value that corresponded to an individualized probability of recurrence.
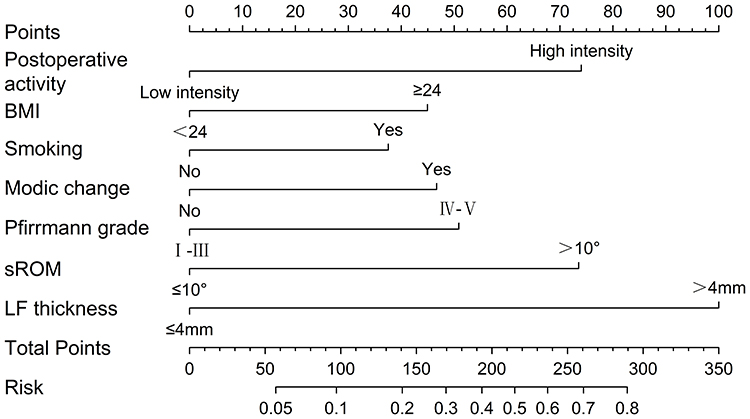 |
Figure 6 Nomogram to predict the risk of rLDH after PELD. |
Validation of the Nomogram Prediction Model
The AUC value was 0.793 (95% CI: 0.736–0.850), indicating that the model has good discriminatory ability (Figure 7). Bootstrap resampling (1,000 iterations) showed that the concordance index (C-index) was 0.763 (95% CI: 0.682–0.844), and the C-index obtained by 10-fold cross-validation was 0.775. These findings indicate stable discrimination in internal validation.
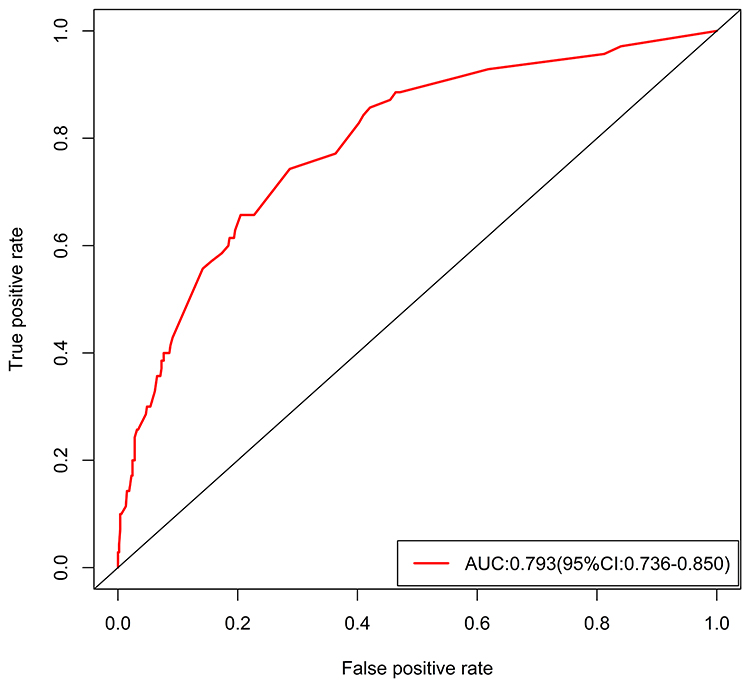 |
Figure 7 The ROC analysis for the nomogram. |
The Hosmer–Lemeshow goodness-of-fit test produced a P value of 0.668 (P > 0.05), suggesting satisfactory calibration of the model. The calibration curve closely overlapped with the observed outcomes, demonstrating strong agreement between the predicted and actual recurrence risks (Figure 8).
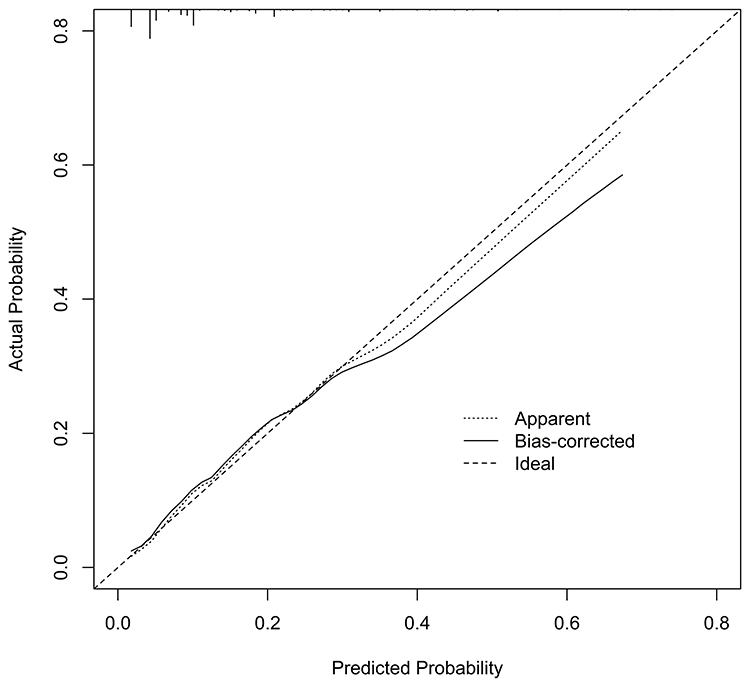 |
Figure 8 The calibration curves of the nomogram. |
DCA indicated that the nomogram model provided substantial clinical net benefit across a wide range of threshold probabilities, supporting its favorable clinical utility (Figure 9).
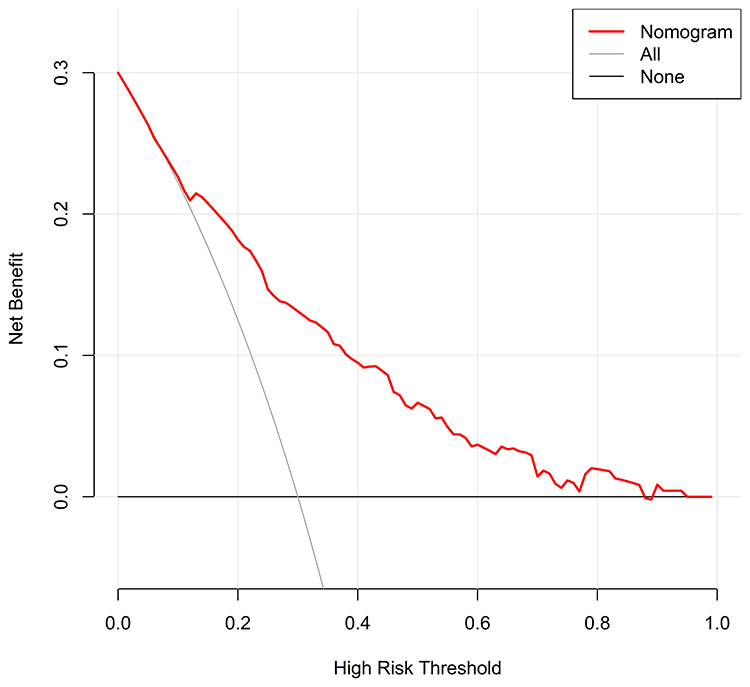 |
Figure 9 Decision curve for the risk of rLDH after PELD. |
Discussion
Owing to its advantages of minimal invasiveness, favorable clinical outcomes, and relatively low recurrence rate, PELD has become increasingly favored by spine surgeons. Nevertheless, postoperative recurrence remains a concern, with reported recurrence rates ranging from 3% to 18%; in the present study, the recurrence rate among patients with LDH was 11.5%, consistent with previous findings.5,6
As a widely applied visual predictive instrument in clinical medicine, the nomogram incorporates multiple independent risk factors and displays them graphically, allowing for the intuitive, individualized estimation of event probability to facilitate clinical decision-making.20,21 In the present retrospective study, 30 potential risk factors were initially included. Using LASSO regression and multivariate logistic regression analyses, seven independent risk factors were ultimately identified: postoperative activity level, BMI, smoking, Modic change, Pfirrmann grade, sROM, and LF thickness. A risk prediction model for rLDH was subsequently developed based on these seven variables. Multiple validation methods demonstrated good discrimination and calibration performance, indicating favorable clinical predictive value for estimating the risk of recurrence following PELD.
This study incorporated two complementary internal validation techniques—10-fold cross-validation and bootstrap method (1000 iterations)—to assess model stability and generalizability. These approaches are widely endorsed by the TRIPOD guideline when external data are unavailable, ensuring reliability without arbitrary data splitting.
Among the identified factors, postoperative activity, BMI, and smoking are modifiable clinical parameters, emphasizing the role of behavioral and perioperative management in reducing recurrence. From a risk-management perspective, the model enables individualized prediction of recurrence probability before and after PELD, thereby allowing surgeons to tailor rehabilitation intensity, weight-control interventions, and smoking cessation counseling according to predicted risk strata. Such stratified strategies may facilitate targeted perioperative counseling and more efficient follow-up planning.
High-intensity activity in the first 3 postoperative months was associated with rLDH, consistent with prior studies.11,22,23 In the early postoperative phase, the annular defect has not yet been fully repaired by mature fibrous scar. High-load physical activity at this stage can sharply increase intradiscal pressure, subjecting the disc to substantial biomechanical stress; when pressure is unevenly distributed, residual nucleus pulposus may reherniate through the disrupted annulus. Therefore, during the first 3 months after PELD, it may be advisable to implement a structured, staged rehabilitation program emphasizing activity modification and gradual functional exercises; thereafter, high-load activities should be reintroduced progressively rather than abruptly to help reduce recurrence risk.
Higher BMI (≥24) was also an independent predictor, consistent with previous findings.24 Excess body weight increases mechanical demands on the operated segment and may impair annular healing, thereby increasing susceptibility to reherniation, particularly during flexion/lifting.25,26 Therefore, for patients with higher BMI, weight-control counseling combined with avoidance of early high-load activities may be especially relevant.
Smoking emerged as another modifiable risk factor.27,28 As an avascular structure, the intervertebral disc relies primarily on diffusion through the capillary network at the endplate–disc interface for its nutrient supply. Smoking can induce arteriosclerosis of local arteries and arterioles, while nicotine acts on vascular smooth muscle to slow blood flow, thereby impairing disc perfusion.29,30 In addition, nicotine has been shown to inhibit cell proliferation and extracellular matrix synthesis and to accelerate nucleus pulposus cell senescence, further exacerbating disc degeneration.31,32 Therefore, smoking should be recognized as a modifiable risk factor in patients scheduled to undergo PELD. Comprehensive perioperative smoking cessation education and systematic interventions are recommended to improve the local microenvironment of the intervertebral disc, reduce postoperative recurrence risk, and enhance long-term outcomes.
Meanwhile, LF thickness, sROM, Modic change, and Pfirrmann grade are objective imaging indicators that capture complementary aspects of segmental vulnerability, including degenerative burden, canal reserve, endplate–disc health, and dynamic stability. Rather than providing redundant mechanistic explanations in isolation, these variables collectively describe a biomechanical and structural context in which recurrent herniation is more likely to become symptomatic and clinically relevant.
The results of this study indicate that LF thickness greater than 4 mm is an important risk factor for postoperative recurrence. Under the combined influence of repeated mechanical stress, inflammatory stimulation, and abnormal repair processes, pathological alterations such as disorganized collagen fiber arrangement, reduced elastic fibers, and fibrosis may occur, leading to LF proliferation and thickening.33,34 LF thickness >4 mm may reflect advanced degenerative remodeling and reduced canal/lateral recess reserve, such that even a small recurrent protrusion can precipitate nerve root compression and symptoms.
Kim et al reported that patients with sROM ≥ 10° had a postoperative recurrence rate as high as 26.5%, whereas those with sROM < 10° had a recurrence rate of only 4.1%, findings consistent with the present results.17 The underlying biomechanical mechanism may lie in the fact that increased sROM leads to reduced local stability of the operated segment. Such segmental instability can cause abnormal loading and uneven stress distribution on the residual nucleus pulposus, thereby increasing the risk of annular tear. A retrospective study on unilateral biportal endoscopic discectomy further quantified this risk by developing a dynamic nomogram, demonstrating that the probability of rLDH rises proportionally with increasing sROM.35
Modic change reflects endplate pathology and impaired disc–endplate function, which may compromise nutrient transport and reduce the disc’s ability to tolerate postoperative loading.36–38 Studies have shown that patients with concurrent Modic change have a higher risk of developing rLDH after PELD, which is consistent with the results of this study.39 Because the endplate structure is already compromised in such patients, and the interface between the cartilaginous endplate and vertebral body is relatively weak, the endplate may herniate together with the nucleus pulposus under load.40 Moreover, removal of the nucleus pulposus during surgery may further injure the endplate, thereby increasing the risk of rLDH after PELD.
Our findings indicate that Pfirrmann grade IV–V is a risk factor for rLDH. During disc degeneration, type I collagen increases while type II collagen decreases; concomitantly, intradiscal proteoglycan and elastin contents decline, reducing nucleus pulposus elasticity and leading to loss of disc height.41 Discs graded as Pfirrmann grade IV typically show heterogeneous signal intensity, an indistinct nucleus–annulus boundary, and mild loss of disc height, placing the lumbar segment in a biomechanically unstable state that predisposes to rLDH. Although patients with Pfirrmann grade V may exhibit reduced sROM due to disc collapse, the severe disc destruction and annular compromise still confer a high postoperative risk of rLDH.42 Prior studies likewise demonstrate that advanced lumbar disc degeneration is a risk factor for rLDH, consistent with our results.10
Taken together, these imaging parameters describe complementary aspects of segmental vulnerability and may help identify patients who warrant closer surveillance and more individualized perioperative counseling. Importantly, the nomogram is intended to support shared decision-making and follow-up planning rather than to mandate specific surgical strategies. For patients classified as high risk, closer follow-up and more individualized surgical decision-making may be considered; however, procedure selection should remain individualized and requires further external validation of the model.
Clinical Application Perspective
Because postoperative activity intensity is assessed during early follow-up, the proposed nomogram is best used as a dynamic risk-updating tool rather than a discharge-only predictor. At discharge, clinicians may estimate baseline risk using readily available clinical and imaging predictors (eg, BMI, smoking status, LF thickness, sROM, Modic change, and Pfirrmann grade) to guide counseling, prescribe an activity plan, and reinforce symptom monitoring At early follow-up (typically at 1 month and updated at 3 months), once early postoperative activity intensity has been ascertained, the nomogram can be recalculated using all predictors to provide an updated individualized rLDH risk and to support risk-stratified follow-up and rehabilitation planning.
Example 1 (low-risk profile). A patient with low-intensity activity during the first 3 postoperative months, BMI < 24, non-smoker, no Modic change, Pfirrmann I–III, sROM ≤ 10°, and LF thickness ≤ 4 mm would accumulate minimal points, corresponding to a low predicted recurrence risk (<0.10). In practice, standard rehabilitation and routine follow-up may be sufficient.
Example 2 (intermediate-risk profile). A patient with BMI ≥ 24 and smoking, combined with one unfavorable imaging marker (eg, Modic change present or Pfirrmann IV–V) but otherwise favorable parameters (eg, low-intensity activity and no marked instability), would yield a higher point total, mapping to an intermediate predicted risk (010–0.30) depending on the overall score. Clinically, this scenario supports intensified counseling on weight control/smoking cessation and a more structured, staged activity prescription, with earlier reassessment if symptoms recur.
Example 3 (high-risk profile). A patient with multiple adverse imaging markers (eg, sROM > 10°, Modic change, and Pfirrmann IV–V) together with at least one additional clinical risk factor (BMI ≥ 24 and/or current smoking) would accumulate a high point total, corresponding to a high predicted recurrence risk (>030) depending on the overall score. In practice, this profile supports a more conservative discharge plan, including stricter early activity restriction with a supervised, graded rehabilitation program, explicit avoidance of high-intensity loading and repetitive flexion/lifting, and closer follow-up with earlier reassessment if symptoms recur. Reinforcement of modifiable risk-reduction strategies (weight management and smoking cessation) should be prioritized during early recovery.
Importantly, the nomogram is intended to facilitate shared decision-making and follow-up planning, and it should not be used as the sole basis for procedure selection. Given the retrospective single-center design and the absence of external validation, any inference regarding alternative surgical strategies (eg, fusion) should be interpreted cautiously and considered hypothesis-generating To enhance usability and implementation, the model could be translated into an electronic calculator (web-based tool or mobile application) embedded into postoperative follow-up workflows. Prospective multicenter studies with external validation and impact analyses are warranted to determine whether nomogram-guided follow-up and rehabilitation strategies improve outcomes and optimize resource allocation.
This study has several limitations. First, its retrospective, single-center design may introduce selection bias (eg, referral patterns, local indications for PELD, and follow-up completeness), potentially inflating apparent model performance and limiting transportability to other settings Second, although all procedures were performed by the same surgical team, center-specific technical and perioperative practice patterns (eg, extent of nucleus removal, endplate handling, and rehabilitation advice) may influence recurrence risk and could affect calibration when the model is applied elsewhere Third, despite robust internal validation, external validation was not performed; therefore, the nomogram should be used as a decision-support tool rather than as a determinant of procedure selection. Prospective multicenter studies with standardized assessment of postoperative activity and independent external validation are warranted to confirm generalizability and refine the model.
Conclusion
Recurrent lumbar disc herniation after PELD remains clinically relevant, and existing prediction models vary in included predictors and validation strategies. We identified seven independent predictors (postoperative activity intensity, BMI, smoking, LF thickness, sROM, Modic change, and Pfirrmann grade) and developed an interpretable nomogram with good discrimination, calibration, and dual internal validation. This tool integrates modifiable behaviors with objective imaging markers to support individualized risk stratification and postoperative management; external validation is warranted before broad implementation.
Abbreviations
LDH, lumbar disc herniation; rLDH, recurrent lumbar disc herniation; PELD, percutaneous endoscopic lumbar discectomy; LASSO, least absolute shrinkage and selection operator; TRIPOD, Transparent Reporting of a multivariable prediction model for Individual Prognosis Or Diagnosis; ROC, receiver operating characteristic; AUC, area under the receiver operating characteristic curve; C-index, concordance index; DCA, decision curve analysis; BMI, body mass index; LF, ligamentum flavum; sROM, sagittal range of motion; LL, lumbar lordosis; IVA, intervertebral angle; DHI, disc height index; MRI, magnetic resonance imaging; CT, computed tomography; ICC, intraclass correlation coefficient; MET, metabolic equivalent of task; OR, odds ratio; CI, confidence interval; PEID, percutaneous endoscopic interlaminar discectomy; PETD, percutaneous endoscopic transforaminal discectomy.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This retrospective study was conducted in accordance with the Declaration of Helsinki. The study protocol was reviewed and approved by the Ethics Committee of The Affiliated Taizhou People’s Hospital of Nanjing Medical University (approval No. [LSKY 2025-135-01]). Because this was a minimal-risk study based on existing clinical data and follow-up assessments were conducted mainly by telephone and during routine outpatient visits, obtaining written informed consent from all participants was not feasible in practice, especially given that many eligible patients were older adults with limited mobility. All data were de-identified prior to analysis, and no directly identifying information was retained, resulting in a very low risk to participant privacy. In light of these considerations, the Ethics Committee waived the requirement for written informed consent and explicitly approved the use of verbal informed consent. Before each follow-up interview, trained investigators provided a standardized explanation of the study objectives, procedures, potential risks and benefits, and data confidentiality. Participants who agreed to take part provided verbal informed consent, which was documented in the study records by ticking a “verbal consent obtained” field together with the date and the interviewer’s identifier.
Consent for Publication
All authors have confirmed that the content can be published, and approved the submission of this manuscript.
Acknowledgments
All authors thank the hospital staff for their guidance, support, and collaboration.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funds were received in support of this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zhang AS, Xu A, Ansari K, et al. Lumbar Disc Herniation: diagnosis and Management. Am J Med. 2023;136(7):645–16. doi:10.1016/j.amjmed.2023.03.024
2. Thavarajasingam SG, Salih A, Arif A, et al. Indications for surgery versus conservative treatment in the management of lumbar disc herniations: a systematic review. Brain Spine. 2025;5:105619. doi:10.1016/j.bas.2025.105619
3. Kuzu Ş, Jawad SR, Canli M, et al. Investigation of Efficacy of High and Low Intensity Laser Therapy in Patients with Lumbar Disc Herniation: a Randomized Controlled Trial. J Med Biol Eng. 2025;45(5):738–744. doi:10.1007/s40846-025-00989-6
4. Pan M, Li Q, Li S, et al. Percutaneous Endoscopic Lumbar Discectomy: indications and Complications. Pain Physician. 2020;23(1):49–56.
5. Li X, Hu Z, Cui J, et al. Percutaneous endoscopic lumbar discectomy for recurrent lumbar disc herniation. Int J Surg. 2016;27:8–16. doi:10.1016/j.ijsu.2016.01.034
6. Yin S, Du H, Yang W, et al. Prevalence of Recurrent Herniation Following Percutaneous Endoscopic Lumbar Discectomy: a Meta-Analysis. Pain Physician. 2018;21(4):337–350.
7. Swartz KR, Trost GR. Recurrent lumbar disc herniation. Neurosurg Focus. 2003;15(3):E10. doi:10.3171/foc.2003.15.3.10
8. Zileli M, Oertel J, Sharif S, et al. Lumbar disc herniation: prevention and treatment of recurrence: WFNS spine committee recommendations. World Neurosurg X. 2024;22:100275. doi:10.1016/j.wnsx.2024.100275
9. Li Z, Yang H, Liu M, et al. Clinical Characteristics and Risk Factors of Recurrent Lumbar Disk Herniation: a Retrospective Analysis of Three Hundred Twenty-One Cases. Spine. 2018;43(21):1463–1469. doi:10.1097/brs.0000000000002655
10. He H, Ma J, Xiong C, et al. Development and Validation of a Nomogram to Predict the Risk of Lumbar Disk Reherniation within 2 Years After Percutaneous Endoscopic Lumbar Discectomy. World Neurosurg. 2023;172:e349–e56. doi:10.1016/j.wneu.2023.01.026
11. Zhou Y, Huang R-L, Liu Y, et al. Construction and validation: a nomogram model to predict recurrence after percutaneous endoscopic discectomy. Medicine. 2024;103(49):e40828. doi:10.1097/md.0000000000040828
12. Huang H, Yang M, Fu Z, et al. Predicting and analysing of the unfavourable outcomes of early applicated percutaneous endoscopic interlaminar discectomy for lumbar disc herniation: development and validation based nomogram. Eur Spine J. 2024;33(3):906–914. doi:10.1007/s00586-024-08141-9
13. Li ZP, Liu LL, Liu H, et al. Radiologic Analysis of Causes of Early Recurrence After Percutaneous Endoscopic Transforaminal Discectomy. Global Spine J. 2024;14(1):113–121. doi:10.1177/21925682221096061
14. Kocaman H, Yıldırım H, Gökşen A, et al. An investigation of machine learning algorithms for prediction of lumbar disc herniation. Med Biol Eng Comput. 2023;61(10):2785–2795. doi:10.1007/s11517-023-02888-x
15. Balachandran VP, Gonen M, Smith JJ, et al. Nomograms in oncology: more than meets the eye. Lancet Oncol. 2015;16(4):e173–80. doi:10.1016/s1470-2045(14)71116-7
16. Albishi W, Alhuqbani MN, Aldosar OA, et al. A decade-long trends in ligamentum flavum hypertrophy among spinal stenosis patients: a comparative analysis of incidence and patterns. J Orthop. 2025;68:171–174. doi:10.1016/j.jor.2025.05.056
17. Kim KT, Park SW, Kim YB. Disc height and segmental motion as risk factors for recurrent lumbar disc herniation. Spine. 2009;34(24):2674–2678. doi:10.1097/BRS.0b013e3181b4aaac
18. Ainsworth BE, Haskell WL, Whitt MC, et al. Compendium of physical activities: an update of activity codes and MET intensities. Med Sci Sports Exerc. 2000;32(9 Suppl):S498–504. doi:10.1097/00005768-200009001-00009
19. Garber CE, Blissmer B, Deschenes MR, et al. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med Sci Sports Exerc. 2011;43(7):1334–1359. doi:10.1249/MSS.0b013e318213fefb
20. Zhou LF, Jiang T, Zhang XQ, et al. Construction and validation of a nomogram prediction model for postoperative recurrence of lumbar disc herniation treated with percutaneous laminectomy. Medicine. 2024;103(46):e40626. doi:10.1097/md.0000000000040626
21. Rong Y, Wang K, Pan Y, et al. Nomogram for prediction of recurrence in patients with lumbar disc herniation after unilateral biportal endoscopy spinal surgery: a retrospective study. Front Surg. 2025;12:1564825. doi:10.3389/fsurg.2025.1564825
22. Wang F, Chen K, Lin Q, et al. Earlier or heavier spinal loading is more likely to lead to recurrent lumbar disc herniation after percutaneous endoscopic lumbar discectomy. J Orthop Surg Res. 2022;17(1):356. doi:10.1186/s13018-022-03242-x
23. Kong M, Xu D, Gao C, et al. Risk Factors for Recurrent L4-5 Disc Herniation After Percutaneous Endoscopic Transforaminal Discectomy: a Retrospective Analysis of 654 Cases. Risk Manag Healthc Policy. 2020;13:3051–3065. doi:10.2147/rmhp.S287976
24. Siccoli A, Staartjes VE, Klukowska AM, et al. Overweight and smoking promote recurrent lumbar disk herniation after discectomy. Eur Spine J. 2022;31(3):604–613. doi:10.1007/s00586-022-07116-y
25. Segar AH, Baroncini A, Urban JPG, et al. Obesity increases the odds of intervertebral disc herniation and spinal stenosis; an MRI study of 1634 low back pain patients. Eur Spine J. 2024;33(3):915–923. doi:10.1007/s00586-024-08154-4
26. Zhang X, Lin J, Liu C, et al. Biomechanical changes in lumbar intervertebral discs after percutaneous endoscopic transforaminal discectomy surgery at different Body Mass Index (BMI) categories. J Orthop Surg Res. 2024;19(1):875. doi:10.1186/s13018-024-05319-1
27. Jiang L, Xie X, He R, et al. Analysis of risk factors for post-operative recurrence after percutaneous endoscopic lumbar discectomy in patients with lumbar disc herniation: a meta-analysis. J Orthop Surg Res. 2023;18(1):935. doi:10.1186/s13018-023-04378-0
28. Pan YH, Wan D, Wang Q, et al. Association of spinal-pelvic parameters with recurrence of lumbar disc herniation after endoscopic surgery: a retrospective case-control study. Eur Spine J. 2024;33(2):444–452. doi:10.1007/s00586-023-08073-w
29. Andersen SB, Smith EC, Støttrup C, et al. Smoking Is an Independent Risk Factor of Reoperation Due to Recurrent Lumbar Disc Herniation. Global Spine J. 2018;8(4):378–381. doi:10.1177/2192568217730352
30. Khurana VG. Adverse impact of smoking on the spine and spinal surgery. Surg Neurol Int. 2021;12:118. doi:10.25259/sni_6_2021
31. Jiang C, Song C, Chen C, et al. Analysis of Nicotine Toxicity and Mechanisms of Senescence in Nucleus Pulposus Cells Using Network Toxicology and Molecular Docking Technique. JOR Spine. 2025;8(2):e70055. doi:10.1002/jsp2.70055
32. Lo WC, Chiou CS, Tsai FC, et al. Platelet-Derived Biomaterials Inhibit Nicotine-Induced Intervertebral Disc Degeneration Through Regulating IGF-1/AKT/IRS-1 Signaling Axis. Cell Transplant. 2021;30:9636897211045319. doi:10.1177/09636897211045319
33. Zhao R, Dong J, Liu C, et al. Thrombospondin-1 promotes mechanical stress-mediated ligamentum flavum hypertrophy through the TGFβ1/Smad3 signaling pathway. Matrix Biol. 2024;127:8–22. doi:10.1016/j.matbio.2024.01.005
34. Liu C, Li P, Ao X, et al. Clusterin negatively modulates mechanical stress-mediated ligamentum flavum hypertrophy through TGF-β1 signaling. Exp Mol Med. 2022;54(9):1549–1562. doi:10.1038/s12276-022-00849-2
35. Xing Z, Guo H, Song Y, et al. Development and validation of a nomogram for predicting postoperative recurrent lumbar disc herniation after unilateral biportal endoscopic discectomy. Sci Rep. 2025;15(1):26336. doi:10.1038/s41598-025-10943-w
36. Huang YC, Xiao J, Leung VY, et al. Lumbar intervertebral disc allograft transplantation: the revascularisation pattern. Eur Spine J. 2018;27(3):728–736. doi:10.1007/s00586-017-5419-6
37. Rajasekaran S, Tangavel C, Ss K, et al. Inflammaging determines health and disease in lumbar discs-evidence from differing proteomic signatures of healthy, aging, and degenerating discs. Spine J. 2020;20(1):48–59. doi:10.1016/j.spinee.2019.04.023
38. Sun Y, Li Z, Duan J, et al. From structure to therapy: the critical influence of cartilaginous endplates and microvascular network on intervertebral disc degeneration. Front Bioeng Biotechnol. 2024;12:1489420. doi:10.3389/fbioe.2024.1489420
39. Li X, Ren H, Peng L, et al. Association between Modic changes and recurrence of lumbar disc herniation after percutaneous endoscopic lumbar discectomy: a meta-analysis. Front Surg. 2025;12:1694557. doi:10.3389/fsurg.2025.1694557
40. Lama P, Zehra U, Balkovec C, et al. Significance of cartilage endplate within herniated disc tissue. Eur Spine J. 2014;23(9):1869–1877. doi:10.1007/s00586-014-3399-3
41. Taylor W, Erwin WM. Intervertebral Disc Degeneration and Regeneration: new Molecular Mechanisms and Therapeutics: obstacles and Potential Breakthrough Technologies. Cells. 2024;13(24):2103. doi:10.3390/cells13242103
42. Karadağ MK, Akıncı AT, Başak AT, et al. Preoperative Magnetic Resonance Imaging Abnormalities Predictive of Lumbar Herniation Recurrence After Surgical Repair. World Neurosurg. 2022;165:e750–e6. doi:10.1016/j.wneu.2022.06.143
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Endoscopic Revision Strategies and Outcomes for Recurrent L4/5 Disc Herniation After Percutaneous Endoscopic Transforaminal Discectomy
Lin A, Wang Y, Zhang H, Zhu K, Zhou D, Guo J, Zhao W, Zhou C, Ma X
Journal of Pain Research 2024, 17:761-770
Published Date: 23 February 2024