")
Back to Journals » OncoTargets and Therapy » Volume 9
Consolidation chemotherapy improves progression-free survival in stage III small-cell lung cancer following concurrent chemoradiotherapy: a retrospective study
Authors Chen X, liang J, Ma S, Fang W, Zhou N, Liao H, Li D, Chen L
Received 22 May 2016
Accepted for publication 25 July 2016
Published 19 September 2016 Volume 2016:9 Pages 5729—5736
DOI https://doi.org/10.2147/OTT.S113340
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr William C. Cho
Xin-Ru Chen,1,* Jian-Zhong Liang,2,* Shu-Xiang Ma,1 Wen-Feng Fang,1 Ning-Ning Zhou,1 Hai Liao,1 De-Lan Li,1 Li-Kun Chen1
1Department of Medical Oncology, 2Department of Pathology, State Key Laboratory of Oncology in South China, Collaborative Innovation Center for Cancer Medicine, Sun Yat-sen University Cancer Center, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Background: Concurrent chemoradiotherapy (CCRT) is the standard treatment for limited-stage small-cell lung cancer (LD-SCLC). However, the efficacy of consolidation chemotherapy (CCT) in LD-SCLC remains controversial despite several studies that were performed in the early years of CCT use. The aim of this study was to reevaluate the effectiveness and toxicities associated with CCT.
Methods: This retrospective analysis evaluated 177 patients with stage IIIA and IIIB small-cell lung cancer (SCLC) who underwent CCRT from January 2001 to December 2013 at Sun Yat-Sen University Cancer Center (SYSUCC). Overall survival (OS) and progression-free survival (PFS) were analyzed using Kaplan–Meier methods. Univariate and multivariate analyses were performed to analyze patient prognosis factors.
Results: Among the 177 patients, 72 (41%) received CCT and 105 (59%) did not receive CCT. PFS was significantly better for patients in the CCT group compared to that for patients in the non-CCT group (median PFS: 17.0 vs 12.9 months, respectively, P=0.031), whereas the differences in OS were not statistically significant (median OS: 31.6 vs 24.8 months, respectively, P=0.118). The 3- and 5-year OS rates were 33.3% and 20.8% for patients in the CCT group and 27.6% and 6.7% for patients in the non-CCT group, respectively. Multivariate analysis revealed that having a pretreatment carcinoembryonic antigen level <5 ng/mL (P=0.035), having undergone prophylactic cranial irradiation (P<0.001), and having received CCT (P=0.002) could serve as favorable independent prognostic factors for PFS. Multivariate analysis for OS also showed that having undergone PCI (P<0.001) and having received CCT (P=0.006) were independent significant prognostic factors.
Conclusion: CCT can improve PFS for patients with stage IIIA and IIIB SCLC following CCRT without significantly increasing treatment-related toxicities.
Keywords: stage III, small-cell lung cancer, consolidation chemotherapy, survival analysis, prognosis, toxicities
Introduction
Small-cell lung cancer (SCLC) accounts for ~15% of all lung cancer cases. Approximately, 30%–40% of the patients with SCLC are initially diagnosed in limited stage; among them, stage III accounted for ~75% of the cases.1–3 The current standard treatment for limited-stage small-cell lung cancer (LD-SCLC) is systemic chemotherapy combined with concurrent thoracic radiotherapy.4 According to the previous reports, the complete remission (CR) rate after concurrent chemoradiotherapy (CCRT) reached 80% and higher. However, the median overall survival (OS) was 16–24 months, and the 5-year survival rate was found to be only12%–26%.5–7 A large portion of patients died due to recurrence and distant metastasis.
To further improve the therapeutic efficacy of treatments, a number of studies have focused on consolidation chemotherapy (CCT) in LD-SCLC. A meta-analysis that included eleven earlier randomized clinical trials (RCTs) showed that both maintenance and CCT slightly improved the OS of SCLC patients. However, the OS increased by only 2 weeks, and CCT also resulted in some inevitable toxicities; therefore, positive results should be treated with caution.8 Over the past decade, with the emergence of new active drugs, such as topoisomerase I inhibitors and paclitaxel, several studies have incorporated these new drugs into CCT. In two similar Phase II studies conducted in Japanese patients, concurrent etoposide and cisplatin (EP) plus accelerated hyperfractionated thoracic radiotherapy followed by three cycles of irinotecan and cisplatin (IP) showed promising OS and were well tolerated.9,10 In another two Phase II studies conducted in Western patients,11,12 EP and CCRT followed by three cycles of paclitaxel and cisplatin (TP) consolidation for LD-SCLC were also well tolerated, although the OS failed to surpass the OS of the two studies mentioned earlier (Kubota et al and Saito et al9,10).
In recent years, less attention has been focused on CCT for SCLC, and no large prospective randomized study has been performed; thus, the definitive role of CCT is still controversial. However, new active agents for CCT have shown the potential and advantages of this approach based on the aforementioned studies.9–12 The purpose of this study was to retrospectively analyze the effectiveness and toxicity of CCT in patients with stage III SCLC at Sun Yat-Sen University Cancer Center (SYSUCC).
Patients and methods
Patients and eligibility criteria
This retrospective study was approved by the Institutional Review Board of SYSUCC. Because this is a retrospective study the Institutional Review Board of SYSUCC deemed patient consent unnecessary. In this study, 177 patients who were initially diagnosed with stage IIIA and IIIB SCLC between January 2001 and December 2013 were retrospectively analyzed. Patients were included in the study according to the following inclusion criteria: 1) SCLC was histologically or cytologically confirmed; 2) the disease was clinically diagnosed as stage III (American Joint Committee on Cancer, 7th edition);13 3) completion of 4–6 cycles of EP-based chemotherapy and concurrent thoracic radiotherapy, and the chemotherapeutic regimen during CCRT was kept consistent with induction chemotherapy; and 4) no disease progression at 1 month after CCRT.
Treatment assessments and follow-up
Evaluations during treatment, including physical examinations, complete blood cell counts (CBCs), serum biochemistry, tumor marker, and electrocardiogram were performed before each cycle. In addition, imaging examinations, including chest and upper abdomen computed tomography (CT) scans, were performed after every two cycles of chemotherapy. Imaging examinations and physical examinations were necessary for the follow-up evaluations and were performed at intervals of 3 months for the first year followed by every 6 months for the second and third years and each later year. Treatment responses were evaluated by Response Evaluation Criteria for Solid Tumors (RECIST)14 version 1.1 as CR, partial response (PR), stable disease (SD), and progressive disease (PD). Toxicity was graded according to the Common Terminology Criteria (CTC) for Adverse Events version 3.0.
Data analysis
All data were processed using SPSS version 22.0 software (SPSS Inc., Chicago, IL, USA). OS was defined as the time from the initiation of treatment to death due to any cause. PFS was defined as the time from start of treatment to the first documented tumor progression or death due to any cause. The Pearson’s χ2 test was used to compare patient baseline characteristics and the incidence of toxicities between two treatment groups. OS and PFS were analyzed using the Kaplan–Meier method and log-rank test. Univariate and multivariate analyses of risk factors of OS and PFS were performed using the log-rank test and Cox proportional hazards regression model, respectively. Variables with P<0.2 in univariate analyses were entered in multivariate analyses. A two-sided P-value ≤0.05 was considered statistically significant.
Results
Baseline characteristics
In total, 177 patients with stage IIIA and IIIB SCLC between January 2001 and December 2013 who had received 4–6 cycles of chemotherapy and concurrent thoracic radiotherapy as the first-line treatment were included. Seventy-two patients were in the CCT group, and 105 patients were in the non-CCT group. Patient characteristics are shown in Table 1. The median patient age was 58 (age range 33–78) years, 47.5% of the patients were younger than 60 years, and a large number of patients were male (87.6%) and had a smoking history (80.8%). Only a few patients had weight loss (15.8%), and most patients (97.7%) had a good Karnofsky Performance Status (KPS ≥80). Patients with stage IIIA and IIIB accounted for 65.5% and 34.5%, respectively.
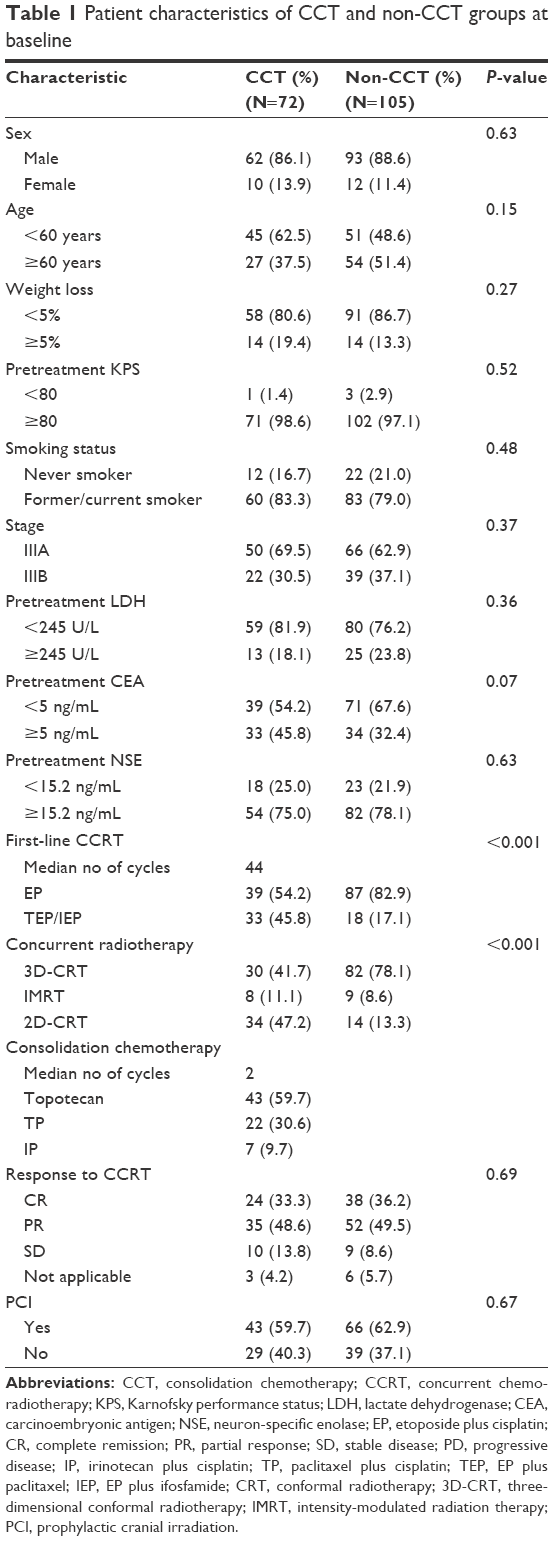 | Table 1 Patient characteristics of CCT and non-CCT groups at baseline |
Most of the patients (71.2%) received 4–6 cycles of EP as first-line chemotherapy, and the rest of the patients received EP plus ifosfamide (IEP: 19.8%) or EP plus paclitaxel (TEP: 9%). The majority of patients received three-dimensional conformal radiotherapy (3D-CRT: 63.8%), while the rest received two-dimensional conformal radiotherapy (2D-CRT: 26.6%) or intensity-modulated radiation therapy (IMRT: 9.6%). All patients received radiation doses of no less than 45 Gy. The responses to CCRT were 35.0, 49.2, 10.7, and 5.1%, respectively, for CR, PR, SD, and not applicable patients. The regimen of CCT differed from that of induction chemotherapy; the median number of cycles was two (range 1–4), and topotecan (59.7%) and TP (30.6%) were the primarily used consolidation regimens. Of all the 177 patients, 109 (75.1%) were treated with prophylactic cranial irradiation (PCI).
Survival
All patients were followed up until October 2015, and 118 (66.1%) patients had died by the end of the follow-up period (CCT: 63.9%; non-CCT: 68.6%). For the entire study population, the median follow-up time was 24 months (range 3–131 months), and the median PFS and OS were 13.6 and 23.5 months, respectively. There was a significant difference in the median PFS between the CCT and non-CCT groups (median PFS: 17.0 vs 12.9 months, respectively, P=0.031; Figure 1A). The median OS was 31.6 months in the CCT group compared with 24.8 months in the non-CCT group (P=0.118; Figure 1B). The 3- and 5-year OS rates were 33.3% and 20.8% in the CCT group and 27.6% and 6.7% in the non-CCT group, respectively.
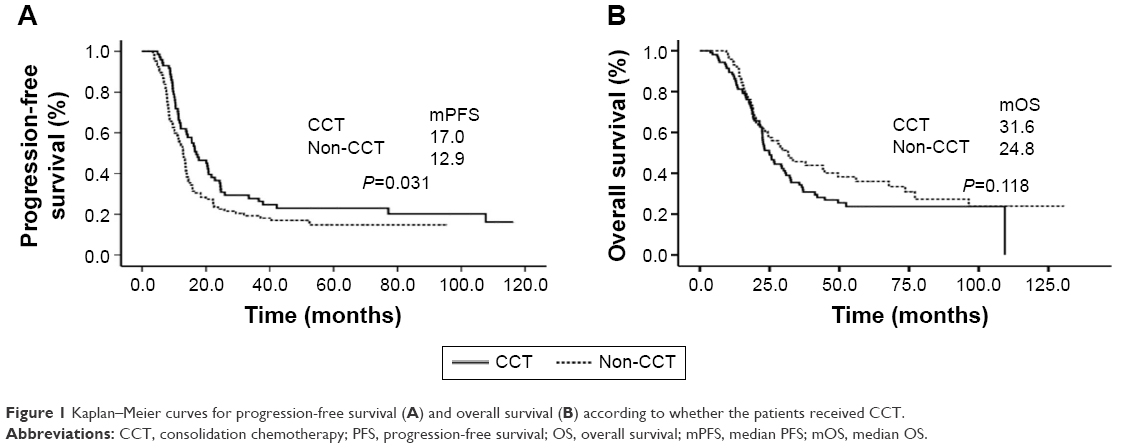 | Figure 1 Kaplan–Meier curves for progression-free survival (A) and overall survival (B) according to whether the patients received CCT. |
In the CCT group, the median PFS and OS for patients with stage IIIA did not significantly differ from those of patients with stage IIIB (median PFS: 15.5 vs 20.5 months, respectively, P=0.56; median OS: 31.6 vs 37.9 months, respectively, P=0.99). The 5-year OS rates for patients with stage IIIA and patients with stage IIIB were 24.0% and 13.6%, respectively. The median PFS and OS for patients receiving topoisomerase inhibitor CCT (topotecan + IP) were longer than those for patients receiving paclitaxel CCT (median PFS: 20.5 vs 16.5 months, respectively, P=0.35; median OS: 31.8 vs 28.9 months, respectively, P=0.85). Patients receiving ≤2 cycles of CCT showed better median PFS (17.3 vs 13.8 months, respectively, P=0.589) and OS (median OS: 31.6 vs 28.9 months, respectively, P=0.589) than those receiving >2 cycles of CCT.
Prognostic factors
Univariate and multivariate analyses for PFS and OS are shown in Tables 2 and 3, respectively. Univariate analysis showed that having a pretreatment lactate dehydrogenase level <245 U/L (P=0.05), having undergone PCI (P<0.001), and having received CCT (P=0.03) were significantly favorable prognostic factors for PFS; sex (P=0.06) and pretreatment carcinoembryonic antigen (CEA) level (P=0.09) could then be entered in multivariate analyses. Multivariate analysis showed that having a pretreatment CEA level <5 ng/mL (P=0.04), having undergone PCI (P<0.001), and having received CCT (P=0.002) could serve as independent prognostic factors for PFS. Univariate analysis for OS revealed that having a pretreatment neuron-specific enolase level <12.5 ng/mL (P=0.05) and having undergone PCI (P<0.001) presented statistically significant differences; treatment modality (P=0.12) could be entered in multivariate analyses. Multivariate analysis showed that OS was significantly associated with the following factors: having undergone PCI (P<0.001) and having received CCT (P=0.002).
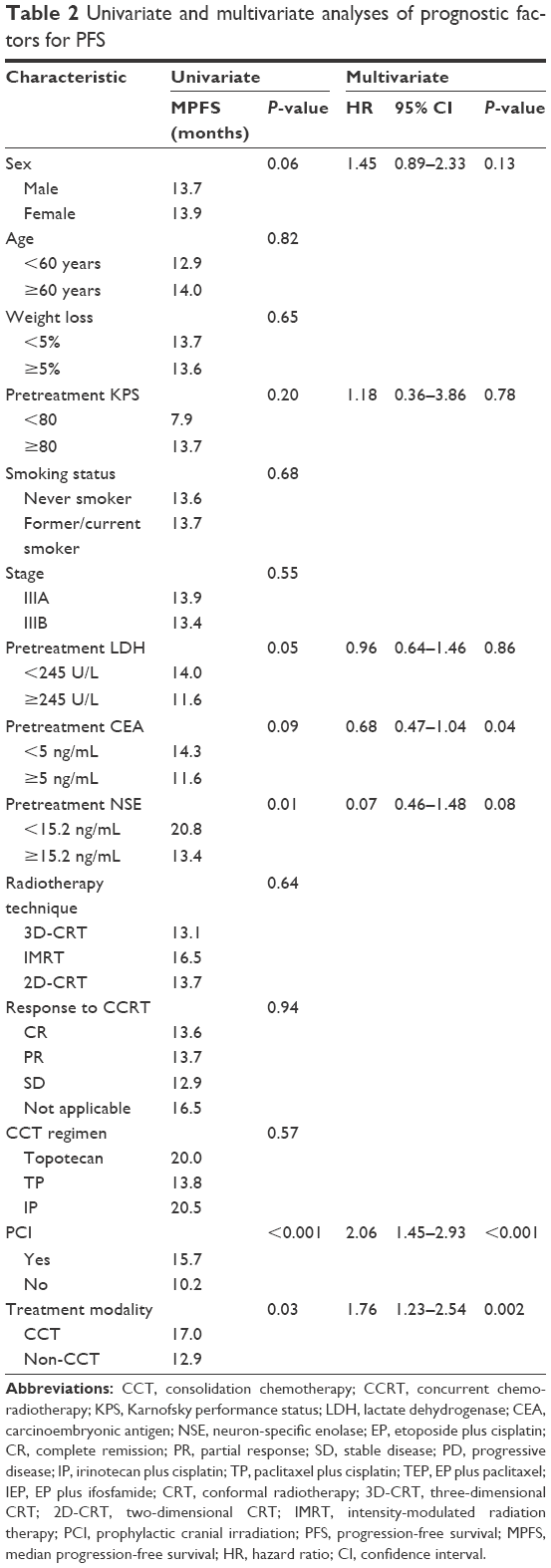 | Table 2 Univariate and multivariate analyses of prognostic factors for PFS |
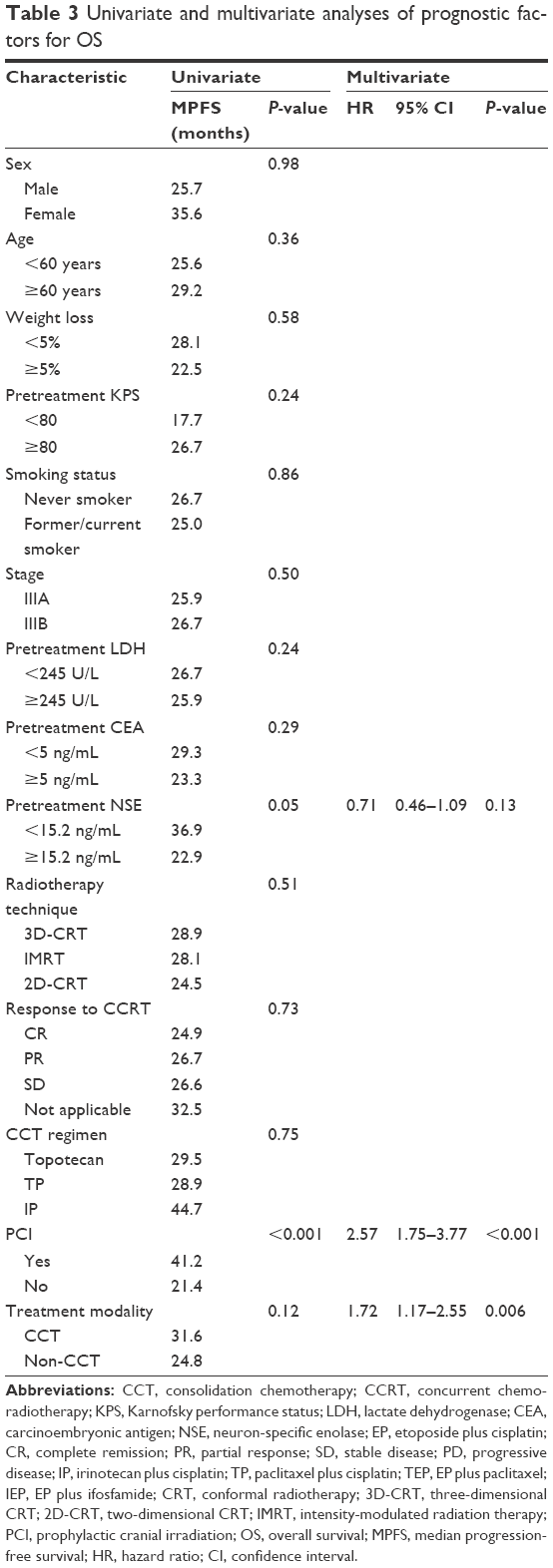 | Table 3 Univariate and multivariate analyses of prognostic factors for OS |
Toxicity
Table 4 summarizes the major treatment-related toxicities. Hematological grade 3/4 toxicity did not significantly differ between the CCT and non-CCT groups (38.9% vs 34.3%, respectively, P=0.53) during the CCRT phase. Among the patients receiving CCT, 23% experienced grade 3/4 hematological toxicities, and no patient had febrile neutropenia-related hospitalization. No grade 3/4 acute radiation pneumonitis occurred in the non-CCT group but did occur in one patient in the CCT group during the CCRT phase (P=0.406). During the CCT phase, the incidence rates of grade 3/4 radiation-related pneumonitis were comparable between the two groups (P=0.20). The incidence rates of grade 3/4 esophagitis were 8 (11.0%) and 7 (6.7%) during the CCRT phase for the CCT group and the non-CCT group, respectively (P=0.30). Irinotecan-related diarrhea and paclitaxel-related allergy did not occur during the CCT phase.
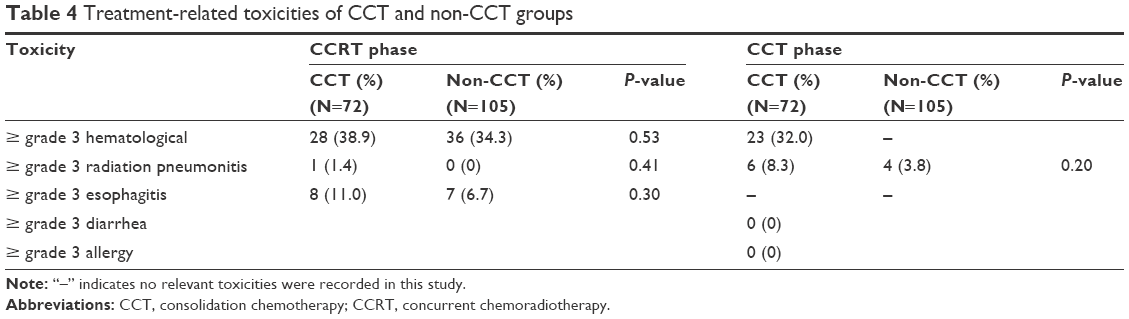 | Table 4 Treatment-related toxicities of CCT and non-CCT groups |
Discussion
SCLC is an aggressive tumor with poor long-term prognosis. Although LD-SCLC is potentially curable, a majority of patients die due to recurrence or distant metastasis. Thus far, four major prospective RCTs have been conducted to explore the efficacy of CCT in LD-SCLC. Cullen et al, who performed the first randomized controlled study, showed that eight cycles of vincristine, doxorubicin, and cyclophosphamide (CAV) consolidation after six cycles of CAV plus thoracic radiotherapy failed to provide a survival benefit for patients undergoing CCT (P=0.13).15 Einhorn et al reported that six cycles of EP consolidation after CAV plus concurrent thoracic radiotherapy improved OS (median OS: 24.4 vs 17 months, P=0.0008).16
Johnson et al conducted a study similar to that of Einhorn et al and achieved a promising median OS value in the CCT group (median OS: 21.1 vs 13.2 months, P=0.028).17 Bryne et al demonstrated that six cycles of cyclophosphamide, vincristine, and methotrexate (CVM) consolidation after induction therapy showed a trend toward inferior OS (median OS: 14.1 months vs 19.2 months, P=0.05).18 In addition to the four studies previously mentioned, other studies also explored the role of CCT in SCLC; however, those studies randomized both limited and extensive stages and came to different conclusions. All of these RCTs were performed in the early 1990s and produced conflicting results. In recent decades, some new drugs, such as topoisomerase I inhibitors and paclitaxel, showed an active property in SCLC, and several small Phase II studies have shown encouraging outcomes in CCT.9–12 In clinical practice, CCT is still used after CCRT by some oncologists. This retrospective study has focused on the efficacy of new drugs as consolidation regimens for stage III SCLC in recent years at SUSUCC.
In our study, the 5-year PFS and OS rates were 16.2% and 20.8% in the CCT group and 2.9% and 6.7% in the non-CCT group, respectively. The CCT group demonstrated a longer PFS of 17.0 months and showed a tendency to prolong survival. The longer PFS may be due to several of the following reasons. The first reason is the application of new agents in CCT. Using three cycles of IP consolidation, JCOG9903 and WJTOG9902 showed promising outcomes, with median OS and PFS of 20 and 23 months and 9 and 11.8 months and with 3-year survival rates of 38% and 29.7% in the CCT and non-CCT groups, respectively.11,12 Jiang et al reported that topotecan could improve the efficacy of first-line CCRT in LD-SCLC, with a 5-year survival rate of 21%.19 Edelman et al demonstrated that consolidation TP resulted in a median PFS of 9 months and a median OS of 17 months.11 All the results showed the high efficiency of the new agents in CCT for LD-SCLC. In our CCT group, the median PFS (a CCT regimen of topotecan [20.0 months] vs IP [20.5 months] vs TP [13.8 months]) and OS (a CCT regimen of topotecan [29.5 months] vs IP [44.7 months] vs TP [28.9 months]) were superior to those of the aforementioned studies. From the former studies, it is of interest that topoisomerase I inhibitors seemed more effective than paclitaxel in CCT, consistent with our study. We yielded median PFS values of 20.5 and 16.5 months and median OS values of 31.8 and 28.9 months for topoisomerase I inhibitors and paclitaxel as consolidation regimens, respectively. Previous outcomes combined with our data suggest that CCT in LD-SCLC is feasible and that further studies regarding CCT in LD-SCLC, particularly topoisomerase I inhibitor consolidation, will be of value. Second, more cycles (ranging from two to eight) were delivered as CCT in most studies compared to the number of cycles in our study (the median number of cycles was 2). It has yet to be proven whether the use of two cycles is the best approach; our study may provide indications for future studies. However, the negative results for OS may be associated with the relatively small numbers of cases and with the bias existing in this retrospective study. Future large trials should continue to verify the role of CCT and investigate the optimal regimen. We believe that CCT may be beneficial at least for a subset of patients with LD-SCLC.
The prognosis of patients with stage III SCLC was even worse than that of patients with stage I–II SCLC. According to the previous records, the 5-year OS rates for patients with stage IIIA and IIIB were 13% and 9% respectively,3 whereas in our study, for the CCT group, the 5-year OS rates for patients with stage IIIA and stage IIIB were as promising as 24.0% and 13.6%, respectively. Notably, 11.1% of patients lived for more than 8 years in the CCT group compared to 0.01% of patients in the non-CCT group. In addition, one patient in the CCT group has lived for 10 years and is still alive at present. These results may be attributed to the inclusion of new agents in the CCT regimen, which could improve the long-term survival rates of patients.
There is a good consensus that poor PFS (<80), weight loss, and markers associated with most diseases (such as lactate dehydrogenase) are the most important adverse prognostic factors in SCLC.20,21 In our study, multivariate analysis showed that having undergone PCI, having received CCT, and having a pretreatment CEA level <5 ng/mL could serve as independent prognostic factors for PFS. The prognostic factors having undergone PCI and having received CCT showed statistically significant differences in predicting good OS. However, the widely recognized prognostic factors mentioned earlier did not show a significant association between PFS and OS in our study. This result may be attributed to the small sample size and to a large portion of patients who had pretreatment KPS ≥80 (97.7%). Several studies have shown that CEA is a useful indicator of OS and PFS in non-small-cell lung cancer (NSCLC), especially for adenocarcinoma.22–24 However, the prognostic value of CEA in SCLC remains controversial.20,25 Few studies link CEA to SCLC, which means that CEA is not specific for SCLC. Recently, one study reported that serum CEA level was an independent prognostic factor for OS in LD-SCLC.26 However, our results suggest that CEA could serve as an independent prognostic factor for PFS but not for OS; thus, further studies are needed.
The major toxicity during CCT was grade 3/4 myelosuppression, which was comparable to the reported studies; however, no toxicity or death resulting from neutropenia was observed.9–12 Additionally, no irinotecan-related diarrhea or paclitaxel-related allergy occurred in the CCT phase, which may due to the small numbers of patients enrolled. However, slightly higher grade 3/4 radiation pneumonitis and esophagitis were seen in the CCT group, possibly in association with a large proportion of patients using 2D-CRT instead of 3D-CRT or IMRT (2D-CRT: 45.8% vs 13.3%, 3D-CRT or IMRT: 54.3% vs 86.7%, P<0.001); 3D-CRT and IMRT may decrease the rate of pneumonitis and esophagitis.27 In general, the addition of CCT is a feasible regimen with acceptable toxicities.
Conclusion
In summary, CCT could improve patient PFS for stage III SCLC with acceptable toxicities. In the future, additional prospective, RCTs are needed to further explore the effectiveness and toxicities of CCT in localized advanced SCLC. Simultaneously, more drugs with high efficiency and low toxicity should also be considered for CCT.
Acknowledgment
We thank Yin-duo Zeng, Xiao-Xiao Ding Lin, and Tao Qin for assistance with the data analysis. This work was supported by the Natural Science Foundation of Guangdong Province (2015A030313040).
Disclosure
The authors report no conflicts of interest in this work.
References
Govindan R, Page N, Morgensztern D, et al. Changing epidemiology of small-cell lung cancer in the United States over the last 30 years: analysis of the surveillance, epidemiologic, and end results database. J Clin Oncol. 2006;24:4539–4544. | ||
Riaz SP, Luchtenborg M, Coupland VH, Spicer J, Peake MD, Moller H. Trends in incidence of small cell lung cancer and all lung cancer. Lung Cancer. 2012;75:280–284. | ||
Shepherd FA, Crowley J, Van Houtte P, et al. The International Association for the Study of Lung Cancer lung cancer staging project: proposals regarding the clinical staging of small cell lung cancer in the forthcoming (seventh) edition of the tumor, node, metastasis classification for lung cancer. J Thorac Oncol. 2007;2:1067–1077. | ||
Janne PA, Freidlin B, Saxman S, et al. Twenty-five years of clinical research for patients with limited-stage small cell lung carcinoma in North America. Cancer. 2001;95:1528–1538. | ||
Johnson BE, Bridges JD, Sobczeck M, et al. Patients with limited-stage small-cell lung cancer treated with concurrent twice-daily chest radiotherapy and etoposide/cisplatin followed by cyclophosphamide, doxorubicin, and vincristine. J Clin Oncol. 1996;14:806–813. | ||
Turrisi AT 3rd, Kim K, Blum R, et al. Twice-daily compared with once-daily thoracic radiotherapy in limited small-cell lung cancer treated concurrently with cisplatin and etoposide. N Engl J Med. 1999;340: 265–271. | ||
Samson DJ, Seidenfeld J, Simon GR, et al. Evidence for management of small cell lung cancer: ACCP evidence-based clinical practice guidelines (2nd edition). Chest. 2007;132:314S–323S. | ||
Rossi A, Garassino MC, Cinquini M, et al. Maintenance or consolidation therapy in small-cell lung cancer: a systematic review and meta-analysis. Lung Cancer. 2010;70:119–128. | ||
Kubota K, Nishiwaki Y, Sugiura T, et al. Pilot study of concurrent etoposide and cisplatin plus accelerated hyperfractionated thoracic radiotherapy followed by irinotecan and cisplatin for limited-stage small cell lung cancer: Japan Clinical Oncology Group 9903. Clin Cancer Res. 2005;11:5534–5538. | ||
Saito H, Takada Y, Ichinose Y, et al. Phase II study of etoposide and cisplatin with concurrent twice-daily thoracic radiotherapy followed by irinotecan and cisplatin in patients with limited-disease small-cell lung cancer: West Japan Thoracic Oncology Group 9902. J Clin Oncol. 2006;24:5247–5252. | ||
Edelman MJ, Chansky K, Gaspar LE, et al. Phase II trial of cisplatin/etoposide and concurrent radiotherapy followed by paclitaxel/carboplatin consolidation for limited small-cell lung cancer: Southwest Oncology Group 9713. J Clin Oncol. 2004;22:127–132. | ||
Kakolyris S, Agelidou A, Androulakis N, et al. Cisplatin plus etoposide chemotherapy followed by thoracic irradiation and paclitaxel plus cisplatin consolidation therapy for patients with limited stage small cell lung carcinoma. Lung Cancer. 2006;53:59–65. | ||
Goldstraw P, Crowley J, Chansky K, et al. The IASLC Lung Cancer Staging Project: proposals for the revision of the TNM stage groupings in the forthcoming (seventh) edition of the TNM classification of malignant tumours. J Thorac Oncol. 2007;2(8):706–714. | ||
Therasse P, Arbuck SG, Eisenhauer EA, et al. New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J Natl Cancer Inst. 2000;92(3):205–216. | ||
Cullen M, Morgan D, Gregory W, et al. Maintenance chemotherapy for anaplastic small cell carcinoma of the bronchus: a randomised, controlled trial. Cancer Chemother Pharmacol. 1986;17:157–160. | ||
Einhorn LH, Crawford J, Birch R, Omura G, Johnson DH, Greco FA. Cisplatin plus etoposide consolidation following cyclophosphamide, doxorubicin, and vincristine in limited small-cell lung cancer. J Clin Oncol. 1988;6:451–456. | ||
Johnson DH, Bass D, Einhorn LH, et al. Combination chemotherapy with or without thoracic radiotherapy in limited-stage small-cell lung cancer: a randomized trial of the Southeastern Cancer Study Group. J Clin Oncol. 1993;11:1223–1229. | ||
Byrne MJ, van Hazel G, Trotter J, et al. Maintenance chemotherapy in limited small cell lung cancer: a randomised controlled clinical trial. Br J Cancer. 1989;60:413–418. | ||
Jiang W, Zhang Y, Zhao H, et al. [Immediate versus delayed topotecan after first-line therapy in small cell lung cancer]. Zhongguo Fei Ai Za Zhi. 2010;13:211–215. Chinese. | ||
Bremnes RM, Sundstrom S, Aasebo U, Kaasa S, Hatlevoll R, Aamdal S. The value of prognostic factors in small cell lung cancer: results from a randomised multicenter study with minimum 5 year follow-up. Lung Cancer. 2003;39:303–313. | ||
Foster NR, Mandrekar SJ, Schild SE, et al. Prognostic factors differ by tumor stage for small cell lung cancer: a pooled analysis of North Central Cancer Treatment Group trials. Cancer. 2009;115:2721–2731. | ||
Arrieta O, Saavedra-Perez D, Kuri R, et al. Brain metastasis development and poor survival associated with carcinoembryonic antigen (CEA) level in advanced non-small cell lung cancer: a prospective analysis. BMC Cancer. 2009;9:119. | ||
Matsuoka K, Sumitomo S, Misaki N. Prognostic factors in patients with pathologic T1-2N1M0 disease in non-small cell carcinoma of the lung. J Thorac Oncol. 2007;2:1098–1102. | ||
Blankenburg F, Hatz R, Nagel D, et al. Preoperative CYFRA 21-1 and CEA as prognostic factors in patients with stage I non-small cell lung cancer: external validation of a prognostic score. Tumour Biol. 2008;9:272–277. | ||
Zhu H, Guo H, Li M, et al. Increased serum carcinoembryonic antigen level can predict poor survival of patients with small cell lung cancer. Transl Res. 2015;166:355–365. | ||
Tsujino K, Hirota S, Kotani Y, et al. Radiation pneumonitis following concurrent accelerated hyperfractionated radiotherapy and chemotherapy for limited-stage small-cell lung cancer: Dose-volume histogram analysis and comparison with conventional chemoradiation. Int J Radiat Oncol Biol Phys. 2006;64:1100–1105. | ||
Paesmans M, Sculier JP, Lecomte J, et al. Prognostic factors for patients with small cell lung carcinoma: analysis of a series of 763 patients included in 4 consecutive prospective trials with a minimum follow-up of 5 years. Cancer. 2000;89:523–533. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.