Back to Journals » Nature and Science of Sleep » Volume 15
Considering REM Sleep Behavior Disorder in the Management of Parkinson’s Disease
Authors Figorilli M ![]() , Meloni M, Lanza G
, Meloni M, Lanza G ![]() , Casaglia E, Lecca R
, Casaglia E, Lecca R ![]() , Saibene FL
, Saibene FL ![]() , Congiu P
, Congiu P ![]() , Puligheddu M
, Puligheddu M ![]()
Received 9 November 2022
Accepted for publication 25 April 2023
Published 5 May 2023 Volume 2023:15 Pages 333—352
DOI https://doi.org/10.2147/NSS.S266071
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Michela Figorilli,1 Mario Meloni,2 Giuseppe Lanza,3,4 Elisa Casaglia,1 Rosamaria Lecca,1 Francesca Lea Saibene,2 Patrizia Congiu,1 Monica Puligheddu1
1Sleep Disorder Research Center, Department of Medical Sciences and Public Health, University of Cagliari, Cagliari, Italy; 2IRCCS, Fondazione Don Carlo Gnocchi ONLUS, Milan, Italy; 3Department of Surgery and Medical-Surgical Specialties, University of Catania, Catania, Italy; 4Clinical Neurophysiology Research Unit, Oasi Research Institute-IRCCS, Troina, Italy
Correspondence: Monica Puligheddu, Sleep Disorder Research Center, Department of Medical Sciences and Public Health, SS 554 Km 4500, 09042 Monserrato CA, Cagliari, Italy, 09042, Tel +07051096001, Email [email protected]
Abstract: Rapid eye movement (REM) sleep behavior disorder (RBD) is the result of the loss of physiological inhibition of muscle tone during REM sleep, characterized by dream-enacting behavior and widely recognized as a prodromal manifestation of alpha-synucleinopathies. Indeed, patients with isolated RBD (iRBD) have an extremely high estimated risk to develop a neurodegenerative disease after a long follow up. Nevertheless, in comparison with PD patients without RBD (PDnoRBD), the occurrence of RBD in the context of PD (PDRBD) seems to identify a unique, more malignant phenotype, characterized by a more severe burden of disease in terms of both motor and non-motor symptoms and increased risk for cognitive decline. However, while some medications (eg, melatonin, clonazepam, etc.) and non-pharmacological options have been found to have some therapeutic benefits on RBD there is no available treatment able to modify the disease course or, at least, slow down the neurodegenerative process underlying phenoconversion. In this scenario, the long prodromal phase may allow an early therapeutic window and, therefore, the identification of multimodal biomarkers of disease onset and progression is becoming increasingly crucial. To date, several clinical (motor, cognitive, olfactory, visual, and autonomic features) neurophysiological, neuroimaging, biological (biofluids or tissue biopsy), and genetic biomarkers have been identified and proposed, also in combination, as possible diagnostic or prognostic markers, along with a potential role for some of them as outcome measures and index of treatment response. In this review, we provide an insight into the present knowledge on both existing and future biomarkers of iRBD and highlight the difference with PDRBD and PDnoRBD, including currently available treatment options.
Keywords: Parkinson’s disease, REM sleep behavior disorder, synucleinopathy, biomarkers, neurodegeneration
RBD in Neurodegenerative Disease, a Window into Prodromal Parkinson’s Disease
REM sleep behavior disorder (RBD) is a parasomnia characterized by dream-enacting behavior and loss of physiological muscle atonia during REM sleep (REM sleep without atonia, RSWA).1,2
Concerning RBD pathophysiology, studies mainly based on animal models seem to indicate the neurodegeneration of SLD glutamatergic and/or medullo-pontin GABA/glycinergic neurons as the cause of RBD.3
RBD may be isolated (iRBD) when non associated to other neurological diseases4 reaching a prevalence of about 0.5–1% in the general population over 60 years.5,6 RBD is also widely recognized as a prodromal manifestation of alpha-synucleinopathies, it is present when the neurodegeneration progress has already started but cardinal symptoms of the disease have not yet manifested.
In fact, about 90% of patients with iRBD at 15 years of follow-up receive a clinical diagnosis of alpha-synucleinopathy, namely Lewy Body Dementia (DLB) in about 45%, Parkinson’s disease (PD) in 45%, and multiple system atrophy (MSA) in 5%.7,8
Additionally, RBD associated with PD (PDRBD) seems to identify a malignant phenotype characterized with a more severe burden of disease in terms of motor and non-motor symptoms, and increased risk for cognitive decline, compared to PD patients without RBD (PDnoRBD).9
Managing of RBD includes pharmacological interventions (Clonazepam, Melatonin), bedroom interventions aimed to mitigate the risk of injuries improving the safety of both the patient and the bed-partner, in order to reduce dream-enacting behaviors, associated nightmares and consequent injuries, and to improve the quality of life. Moreover, in managing RBD it is important to inform the patient about the association between RBD and neurodegenerative disorders and scheduling follow-up neurological examinations in order to early recognize any sign of synucleinopathies.2,8
Up to now, neuroprotective and disease-modifying therapy are not available, in order to arrest or slow down the neurodegenerative process of alphasynucleinopathy. RBD population represents an ideal candidate to neuroprotective or disease-modifying clinical trial. Thus, the identification of multimodal biomarkers, both diagnostic and prognostic, of neurodegeneration is crucial. In this review, we provide an insight into the present knowledge on both existing and future biomarkers of iRBD and highlight the difference with PDRBD and PDnoRBD, including currently available treatment options.
Parkinson’s Disease Associated with RBD a New Phenotype Within the Spectrum of Alpha-Synucleinopathies
Although Parkinson’s disease was initially considered a single entity, soon biological and instrumental evidence reflecting the heterogeneity of possible clinical trajectories, allowed the delineation of phenotypes that not only are guiding the search for the underlying pathological mechanisms of the disease, but can predict its course and which will become increasingly crucial once targeted therapeutic options become available.10 The concept of RBD heralding synucleinopathies was introduced in 1996,11 but only in recent decades RBD and non-motor symptoms has been accorded the importance they deserve. Many years have elapsed since Braak postulated his famous hypothesis according to which the key lesions of the pathology begin to develop long before the onset of cardinal somato-motor symptoms of the disease, with an ascending and predictable topographical sequence.12,13 The first structures to be affected would be located in this model at the level of the medulla oblongata and pons, which may associate not only, as postulated by the author, with the onset of non-motor symptoms such as hyposmia and autonomic dysfunction, but structures critical for the preservation of physiological atonia during REM sleep.12 Subsequently, involvement of the substantia nigra and other nuclear grays of the midbrain and forebrain would occur and then end at stages 5–6 with involvement of the neocortex.14 Regarding pathogenesis of PD, one of the most famous theories is the dual-hit hypothesis: a pathogenic agent spreading in a prion-like manner, leading to the accumulation of misfolded alpha-synuclein aggregates, would have access to the brain through the olfactory bulb and the dorsal motor nucleus of the vagus (DMV).15,16 Although a large proportion of studies seem to confirm the validity of Braak’s model in most cases, it is also true that incidental PD may show pathological aggregates in substantia nigra or elsewhere in the brain with no implication of the dorsal motor nucleus of the vagus.17,18 These observations implying heterogeneity in the sites of origin from which alphasynucleinopathy progresses actually accord with the recent identification of two phenotypes, in contrast for their different spreading patterns: a brain-first (top-down) where the pathology originates in the central nervous system,9 and a body-first (bottom-up) type in which a-synuclein pathology initially arises in the enteric or peripheral autonomic nervous system.19 Premotor RBD is in this model a key clinical indicator of a body-first phenotype, in fact, the pons is involved before the substantia nigra in a bottom-up model; however, since late top-down involvement cannot be excluded, it is only iRBD that can be used as an early and distinctive biomarker of this phenotype.20,21 Moreover, the nigrostriatal dopamine system is widely preserved in many iRBD cases,19 whereas enteric phosphorylated α-synuclein histopathology (PASH) was found more frequent in a RBD subgroup of patients compared to PD patients without RBD.22 However, PDRBD patients also appear to display a more severe cerebral pathological involvement, reflecting a possible broader and heavier diffusion of alpha synucleinopathy in these subjects.19,23 To demonstrate the validity of the dichotomous brain first or gut first model, Horsager et al have investigated de novo PD patients with and without RBD through multimodal imaging studies and compared the results with those obtained in iRBD patients.20
Pre-motor RBD Parkinson’s disease and iRBD groups showed significantly reduced 11C-colonic donepezil and cardiac MIBG signal, mildly decreased locus coeruleus neuromelanin signal and colonic changes like an augmented colon volume and transit time, providing major support for the body-first disease subtype identification.20,24 The alpha-Synuclein Origin site and Connectome (SOC) model, proposed by Borghammer could be considered to some extent an evolution of the Brain-first/Body-first.25 According to this theory, the anatomical point of origin of alpha-synucleinopathy spread and the density of ipsilateral connections dominating intra-cerebral propagation appear to be a potential explanation for the asymmetric involvement at the hemispheric level in CNS-first patients, whereas in the bottom-up model the differences in neuropathological diffusion in the two hemispheres are more subtle.25 In addition to the asymmetry in motor symptoms it is also suggested by the author that the greater prevalence and severity in cognitive involvement in body-first patients is due to the fact that at the time of diagnosis of parkinsonism in this subgroup the alpha-synucleinopathy is already widely spread bilaterally in the brainstem and hemispheric regions, and presenting the aforementioned with a much more protracted prodromal phase.25 Indeed, brain atrophy seems to be already present in de novo PDRBD, which as we have seen appears to be a body-first type hallmark, and there seems to be a stronger correlation between volume reduction of thalamus, hippocampus, and putamen in particular and a severer cognitive impairment.26 Most early subtyping systems were based on age at onset and tremor versus akinetic-rigid predominance in general, on variables that were selected a priori, whereas, in order to improve the reliability and reproducibility of the identified phenotypes, more recent studies are adopting a hypothesis-free data-driven approach, giving increasing importance to non-motor symptoms such as RBD.9,10,27 Regardless, the dominant motor phenotype of tremor has always been found to have a more favorable prognosis than the postural instability and gait disturbance (PIGD) phenotype,9 and, in general, the dominant non-tremor subtypes have always been associated with a wider range of nonmotor symptoms, with early predominance of autonomics and later cognitive impairment as the most common nonmotor issues.
Fereshtehnejad et al, analyzing a comprehensive array of motor and nonmotor features in PD patients were able to identify three clinical subtypes: “mild motor-predominant”, “intermediate” and “diffuse malignant”.9,28 Interestingly, the most discriminating features were mild cognitive impairment, orthostatic hypotension, and RBD. Patients with the diffuse malignant subtype presented not only with a severer dopaminergic deficit on SPECT and atrophy in disease-specific brain networks29 but also displayed an Alzheimer’s disease-like CSF profile and faster progression of cognitive, motor, and other nonmotor domains.9
Finally, PDRBD may mark a unique, more malignant subtype of alphasynucleinopathy, with different neuropathological and genetic background and independent risk factor profile,30 which, however, given the long prodromal phase could ensure the identification of an early therapeutic window once disease-modifying treatments are identified.
REM Sleep Behavior Disorder and Biomarkers for Phenoconversion Prediction
Patients with iRBD have an estimated risk to develop a neurodegenerative disease (such as PD, MSA and LBD) up to 90% after a long follow up: 44.8% after 6 years, and from 67.5%30 to 81% after 10 years.31
This means that diagnosis of RBD offers a unique clue to individuate a cohort of patients that can be eligible for neuroprotective and disease modifying drug trials or therapy in the future.
In order to do so it is crucial to understand which features are associated with phenoconversion and with faster neurodegeneration, consequently during the last years, many longitudinal studies focused on the individuation of potential biomarkers of disease progression.32
Ideally, a good biomarker must have a good sensitivity and specificity, must be easily available and be useful both as a marker for progression and also as a marker for therapy response in neuroprotective therapy trials.33
To date, several clinical (motor symptoms, cognition, olfactive symptoms, visive function, autonomic function) neurophysiological, neuroimaging, biological (biofluids or tissue biopsy) and genetic biomarkers have been individuated. They can be classified accordingly to the purpose they serve as diagnostic biomarkers (to confirm diagnosis of alpha-synucleinopathy), prognostic biomarkers, (to predict phenoconversion), monitoring or therapy responsive (to monitor neurodegenerative progression and possible effect of therapies) and combined biomarkers.33
Table 1 summarizes the biomarkers of neurodegeneration in iRBD.
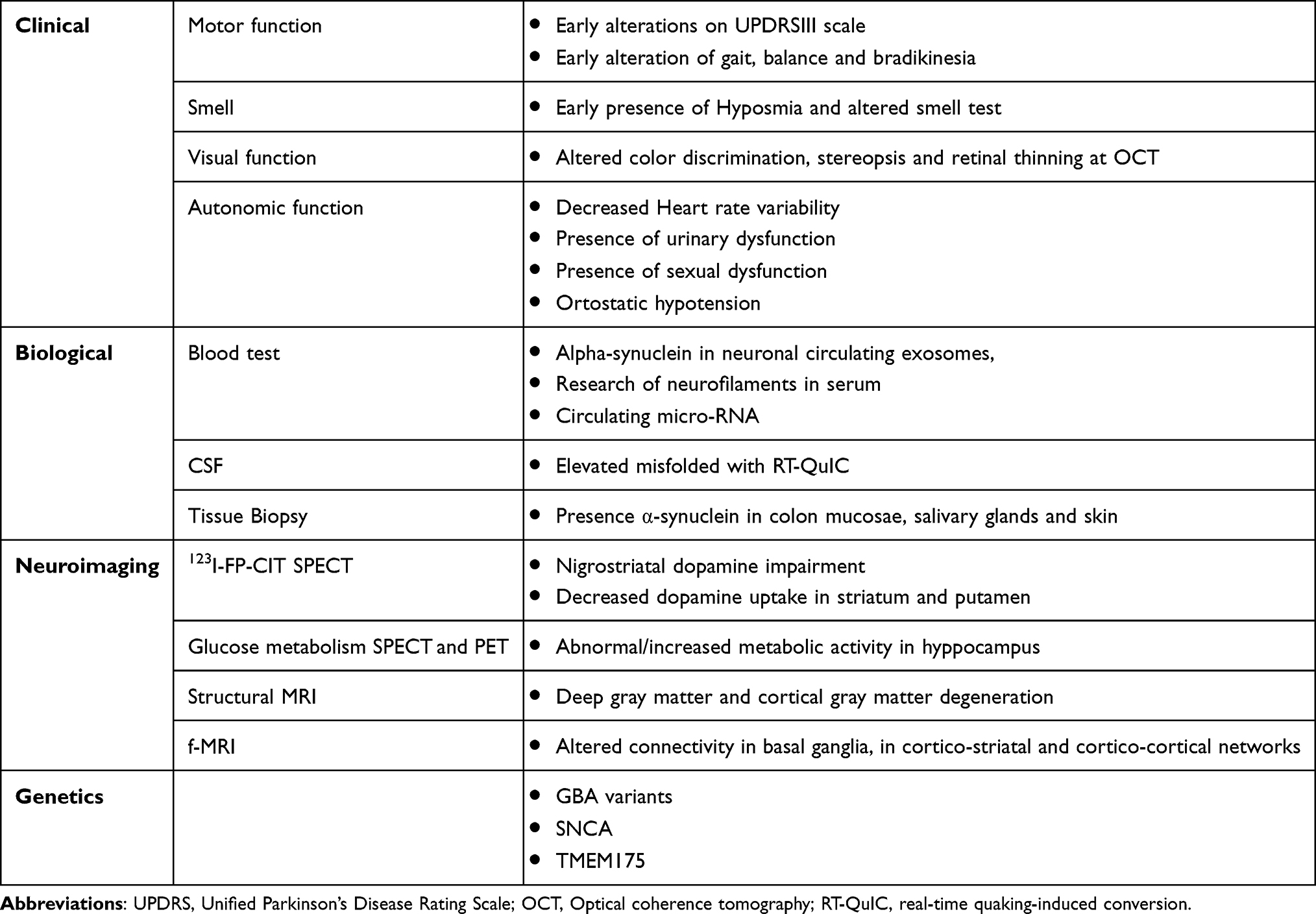 |
Table 1 Biomarkers of Neurodegeneration in Isolated REM Sleep Behavior Disorder (iRBD) |
Clinical Biomarkers
Motor function can be altered in iRBD patients, in a large multicenter study, Unified Parkinson’s disease Rating Scale (UPDRS) and quantitative motor test demonstrated to be powerful predictive factor of phenoconversion with an HR of 3.16 (95% CI 1.86–5.37),34 moreover, UPDRS-III motor score may be altered starting from 6.5 years before diagnosis.35
More recently assessment of motor function with wearable devices or computer detection algorithms was used in several studies, allowing an objective evaluation of gait,36 balance,37 eye movements,38 and bradykinesia.39
All these cross sectional studies showed promising results in the detection of alterations that can be used as biomarkers for phenoconversion, with sensitivity and specificity up to 80%;33 these systems are relatively easy to use and low cost and can be used at patient’s home,36,37 however further studies on larger population are needed for the validation of their use in clinical practice.
Hyposmia is recognized together with RBD a prodromal symptom of PD,40 with 67% of patients with RBD presenting with this symptom.34
The presence of hyposmia or anosmia is considered a low term risk factor for the development of alpha-synucleinopathy in iRBD patients,41,42 but smell test did not show any changes in time, therefore this symptom should be used as a prognostic marker at the moment of RBD diagnosis, but not as a monitoring biomarker in clinical intervention trials.41
Visual impairment, another common finding in alpha-synucleinopathies, can also be present in patients with iRBD in different forms, ranging from altered color discrimination,43 stereopsis44 and retinal thinning,45 suggesting that color vision test and optical coherence tomography (OCT) may be used as potential diagnostic and prognostic markers.33
Finally, another clinical feature that can be used as biomarker for phenoconversion is autonomic dysfunction, symptoms such as orthostatic hypotension, sexual and urinary dysfunction and constipation46 are present in up to 94% patients with RBD.47 Moreover, autonomic dysfunction is one of the cardinal nonmotor symptoms of PD and in patients with iRBD can appear several years before the diagnosis of alpha-synucleinopathy.47
Different studies reported a reduced heart rate variability (HRV) in iRBD patients,48 which also correlated with quantified tonic RSWA,49,50 however there is not a clear difference between patients who converted to a neurodegenerative disorder and those who did not.48
Even though longitudinal studies are still needed in order to have a standardization and clear cut-off values, performing a clinical assessment of motor, autonomic, olfactive and visual function is easy and low cost and is fundamental during baseline and follow-up visits of iRBD patients to predict and detect early signs of alfa-synucleinopathies
Neuroimaging
The use of neuroimaging in PD has greatly developed in the last decade, mostly with the purpose to detect early impairment of nigrostriatal dopaminergic circuit and dopamine transport alteration in the basal ganglia circuit with the use of PET and SPECT imaging.33
The most studied is 123I-FP-CIT SPECT for the assessment of dopamine transporter: many patients with iRBD have nigrostriatal dopamine impairment:51 decreased dopamine uptake in striatum and putamen demonstrated to predict phenoconversion with strong sensitivity and specificity,52–54 especially when combined to clinical biomarkers such as autonomic impairment.55
The use of 123I-FP-CIT SPECT is a powerful biomarker for phenoconversion and can also serve as a prognostic marker for neuroprotective therapy trials.56
Other PET and SPECT techniques for the study of glucose metabolism and perfusion demonstrated abnormal metabolic activity, especially in hippocampus,57 in RBD patients who converted to PD.58 Seriated follow up imaging demonstrated an increase in time of PD related pattern expression, making it a potential marker for prediction of short term phenoconversion.
Although these promising results, SPECT and PET are not available in all centers and expose the patient to radiation, therefore MRI has been considered as an alternative: structural studies demonstrated a reduction in deep gray matter and cortical gray matter degeneration in patients with RBD, along with changes in white matter typically found in neurodegenerative disorders.59
Functional MRI studies (f-MRI) showed altered connectivity not only within basal ganglia, but also in cortico-striatal and cortico-cortical networks.60
Biological
A more feasible and low cost alternative to imaging studies, may be biomarkers obtained from blood; however, research of alpha-synuclein in neuronal circulating exosomes, research of neurofilaments in serum and circulating micro RNA have only shown encouraging results and heir validity as biomarker is yet to be confirmed.33
A novel approach is the detection of alpha synuclein in neuronal extracellular vesicles, which are vesicles released from CNS cells that can transport and spread proteins, including pathological ones, they pass the blood brain barrier and spread the neuropathological proteins.61 Patological soluble alpha-synuclein in neuronal extracellular vesicles is significantly higher in patients with PD compared to controls, this novel approach is promising and will need further validation.62
In many patients with iRBD abnormal deposits of α-synuclein have been documented in olfactory mucosa,63 in peripheral organs (skin, colon and salivary glands)64 and misfolded α-synuclein has also been detected in the cerebral spinal fluid (CSF).65
Recently, detection in CSF of pathologically misfolded α-synuclein with the use of Real-time quaking-induced conversion (RT-QuIC) showed very promising results with a sensitivity and specificity of 90% in patients with iRBD, and its positivity was associated with an increased risk of phenoconversion.65 The same technique applied to swabs from olfactory mucosa, less invasive than lumbar puncture, showed a 90% specificity but lower sensitivity.63
Quantification of α-synuclein in tissue research has emerged as an interesting biomarker, also providing information on its deposition spread over time. Studies on samples from colon mucosae, salivary glands and skin using antibodies targeting phosphorylated α-syn showed good sensitivity and specificity in iRBD patients, with skin biopsy coming up as the most promising technique.64
Genetics
Several gene mutation related to Parkinson disease and other synucleinopathies have been discovered during the last 40 years, detection of gene mutations associated to PD in patients with RBD can represent a biomarker for phenoconversion prediction.
GBA, the gene encoding for Glucocerebrosidase, is more frequently mutated in patients with PDRBD than in patient with PDnoRBD.66 Frequency of GBA mutation in iRBD was higher than in control population and associated with a risk of conversion to PD and DLB,67,68 and was also more frequent in patients with iRBD compared to PD patients with unknown RBD status.
Other genes potentially involved in neurodegeneration progress are SNCA variants69 and TMEM175.70
RBD as a Cognitive Decline Risk Factor
Several studies have shown impairment in different cognitive domains, including memory, attention, executive functions and visuospatial abilities, in RBD patients, both idiopathic and associated with PD.71–73 Likewise, presence of mild cognitive impairment (MCI) and reduced cognitive performances seem to predict the phenoconversion of iRBD patients into a neurodegenerative disease.32,71 Moreover, MCI and/or impaired attention and executive functions might predict conversion to dementia prior to parkinsonism in iRBD patients.34,74
Up to 50% of iRBD and 73% of PDRBD show MCI, in particular, RBD in PD was associated with a more impaired cognitive performances compared to PDnoRBD patients and to healthy controls (HC).73,75 RSWA, the neurophysiological hallmark of RBD, have been correlated with reduced cognitive performances, namely attention, executive functions, episodic verbal and learning memory, verbal fluency and visuospatial abilities, in PDRBD compared to PDnoRBD and HC.73 Furthermore, higher RSWA can discriminate probable synucleinopathy from probable non-synucleinopathy in older adults with cognitive impairment, including in those with no clinical symptoms of dream enactment.76
MRI cortical thinning in the left anterior temporal cortex has been correlated with cognitive impairment in iRBD patients with MCI, and more precisely, reduced attention and executive function has been associated with thinning of the frontal cortex, reduced verbal learning with thinning in left temporal cortex and visuospatial abilities has been correlated with thinning of the fronto-temporal cortex in iRBD patients.33,77 Moreover, atrophy in the basal ganglia, thalamus, amygdala and frontotemporal grey and white matter might predict cognitive decline in both iRBD and PD, by means of MRI using partial least squares.78 More recently, iRBD patients with MCI have shown a widespread pattern of local alteration and volume atrophy in both cortical and subcortical regions compared to iRBD without MCI and controls.79
RBD is an heterogeneous clinical and neurophysiological entity, up to 50% of iRBD patients will develop DLB and the remainder will convert to a parkinsonism (PD>MSA).80,81 Thus, it is crucial to phenotype iRBD patients in dementia-first and parkinsonism-first converters. Presence of MCI, both amnestic and non-amnestic, in iRBD seems to be a key risk factor to dementia-first phenoconversion.82 Recently, cognitive impairment has been considered as a prodromal marker of alphasynucleinopathy and has been incorporated in the last updated research criteria for prodromal PD.83 Different evidences suggest that RBD together with hyposmia and reduced dopamine transporter binding, prodromal signs of PD, might be associated with worse cognitive performances compared with subjects without any or with only one of these prodromal signs.75,84 Moreover, PD associated with RBD has been identified as a diffuse-malignant phenotype characterized by a heavier burden of disease in terms of motor and non-motor symptoms, namely cognitive decline and dysautonomia and a more rapid progression compared to the other two PD phenotype, “mild motor predominant” and “intermediate”.9,29 Also, the diffuse-malignant PDRBD phenotype has shown more atrophy in substantia nigra-connected areas, more dopaminergic deficit on SPECT and reduced amyloid-b in CSF compared to the others.9 Thus, RBD might be associated with a more widespread neurodegenerative process involving cortical-subcortical-mesolimbic networks. Further longitudinal studies are needed in order to intercept iRBD patients at risk to develop cognitive decline, a specific population that might be included in future clinical trials for disease-modifying therapy for alpha-synucleinopathies and clinical trials for therapies targeting cognition in PD.
Neurophysiological Biomarkers of Neurodegeneration in RBD
Electroencephalography (EEG)
iRBD subjects showed some EEG changes which have been demonstrated also in those with PD and DLB, including diffuse slowing in wakefulness EEG recordings, though this was particularly evident on posterior brain regions.85 Notably, the cortical slowdown was related to cognitive impairment, thus hypothesizing a correlation between electrophysiological and neuropsychological features. Moreover, higher absolute delta and theta power from all cortical areas allowed to identify those patients at greater risk of short-term conversion into synucleinopathies.86
Both macro- and microstructure sleep alterations derived from EEG have been suggested as electrophysiological indexes, although prospective studies have not been performed yet. Only an earlier study found that quantification of RSWA, in particular the baseline high tonic chin EMG activity, may detect a greater risk of progression into PD.85 A more recent study with high-density EEG showed that, unlike RBD patients, good sleepers displayed a decreased beta power during phasic with respect to tonic REM sleep. Furthermore, RBD individuals showed a lower SWA decline from early to late non-REM sleep, as well as decreased overnight modifications in the slow-wave amplitude distribution.87 As such, because of the lack of suppression of the beta rhythms during phasic REM sleep, RBD subjects would show an increase in cortical arousal, thus likely favoring the presence of REM behavioral episodes.
A further report demonstrated, during REM sleep, the increase of instability of EEG microstructure in de novo iRBD subjects,88 with power EEG spectrum frequency lower than 15 Hz indicating a reduced REM-related decrease than in controls and an increased beta band, which might correlate with persistent muscular activation. Of note, clonazepam partially recovered the power of frequencies lower than 15 Hz; also, the increased EEG power instability was remarkably reduced by this treatment.
Based on the same rationale, clonazepam might be effective also for PDRBD, as clinically highlighted by recent randomized double-blind clinical trials and systematic reviews/meta-analysis.89–93 Considering these objective findings, indeed, clonazepam may act by reducing the negative effects from the supratentorial network rather than acting directly on the infratentorial pathology of RBD.88 However, its efficacy at EEG level has been demonstrated only in a mouse model of RBD, and not yet in patients with PDRBD.94 Therefore, we recommend continuing the studies to reveal whether there is not only a subjective but also an objective improvement in these patients as well.
The investigation on the cyclic alternating pattern (CAP) has been conducted as well.95 A previous study observed an increase of slow EEG transients (A1 CAP subtypes) and a decrease of fast EEG events (A2 and A3 CAP subtypes) in drug-naïve iRBD individuals.89 In this report, long-term intake of clonazepam improved the stability of non-REM sleep and EEG transients duration. Different results come from another study, ie, a global increased CAP, particularly due to the A2 and A3 subtypes; conversely, the A1 subtype decreased in RBD.96 Lastly, another investigation in iRBD showed a decrease of global CAP measures, mostly due to a decreased A1 CAP subtype.97 Taken together, the impact of non-REM sleep instability on RBD is still inconclusive.
In addition, the density of sleep spindles was found to be altered in RBD patients, with a decreased fast but increased slow spindles, that was viewed as a possible marker predictive of a neurodegenerative disorder.98 A further report revealed a diffuse decreased spindle density both in iRBD patients and in those with PDRBD, thus proposing it as a supportive diagnostic tool.99
Recently, it should be mentioned an advanced EEG-based study in which the analysis method reported theta-band bursts and decreased alpha-band burst during the eye-closed wakefulness, which may predict the progression into DLB or PD.100 Very recently, EEG power analyses showed a significant lower alpha and higher delta power in iRBD phenoconverters during the phasic REM state, which was more evident over the occipital and central cortical areas, with respect to those patients who remained disease-free.101 Significant higher slow-to-fast ratio during the phasic state was noted more diffusely in iRBD converters than in non-converters. The further analysis of slowing ratio during phasic REM sleep from occipital regions resulted in a remarkable area under the curve, whereas the subjective RBD severity did not have any predictive value. The authors concluded that EEG slowing (especially when generalized during the phasic period), rather than subjective RBD severity, may be promising in predicting phenoconversion.101
Motor Evoked Potentials (MEPs)
MEPs to transcranial magnetic stimulation (TMS) have been tested in sleep disorders to evaluate and non-invasively modulate cortical excitation, neuroplasticity, and brain connectivity.102–105
The first TMS study in RBD106 found an impaired short-latency afferent inhibition, which supported the cholinergic dysfunction in those patients developing cognitive decline; this was further supported in RBD patients in the context of PD.107 As such, cholinergic dysfunction may substantially contribute to non-motor aspects of PD as well, raising also the hypothesis that RBD increased the risk of cognitive changes in PD.
The second study found that iRBD patients exhibited an electrocortical profile similar to that observed in PD.108 Moreover, intracortical disinhibition was related to muscular tone change, which supports the model of retrograde influence of the brainstem to the cortex.109 Therefore, an altered control in RBD, which would arise from the brainstem and ascend to the cortex, may determine both a reduced atonia during REM sleep and an imbalanced cortical disinhibition and hypofacilitation, favoring the former.108
Recently, a direct comparison between iRBD and PDRBD revealed that both patient groups had a significantly decreased intracortical facilitation compared to healthy controls, thus sharing the involvement of glutamatergic transmission.110 Finally, another report has recently compared PD without and with RBD: an enhancement of GABA-mediated and a reduction of glutamine-mediated activity was found in PDRBD only, thus suggesting a distinctive physiopathological processes in these subjects.111
To date, no study has applied repetitive TMS in RBD or PDRBD.112
Vestibular Evoked Myogenic Potentials (VEMPs) and Other Brainstem Responses
Ocular (oVEMP), masseter (mVEMP), and cervical (cVEMP) VEMPs can provide an extensive evaluation of whole-length brainstem functioning, also allowing the detection of subtle changes in radiologically or clinically “mute” areas.113
De Natale et al114 reported for the first time a significant alteration of VEMPs in iRBD subjects, especially for oVEMP and mVEMP, thus suggesting that synaptic and neuronal derangement was particularly evident in the upper areas of the brainstem, a finding which is in accordance with current physiopathology of RBD in PD.115 Moreover, the correlation between VEMP and RSWA may precede the progression from iRBD to neurodegeneration, whereas changes at the dopamine transporter scan would indicated a later stage.116
Very recently, PD patients with RBD showed bilateral delays in cVEMP and oVEMP peak latencies with respect to PDnoRBD, whereas cVEMP features were also higher in PDRBD than in iRBD group.117 Although follow-up studies are needed, this indicates that brainstem neurophysiology might reflect different disease involvement and that VEMPs can vary based on the occurrence of RBD in PD, even in its early stages.
Both PD and RBD subjects exhibited altered blink and pupil behavior with respect to healthy controls.118 Notably, since measures of RBD saccade were similar to those found in normal individuals, blink and pupil brain regions might be affected before those underlying saccadic control, thus making them potential prodromal markers of PD.119 Moreover, blink reflex parameters in PD did not relate to cognition or RBD.120
Recently, the pedunculopontine nucleus in dream-enacting motor behavior has been assessed through the prepulse modulation (PPM). PPM was altered in both RSWA and iRBD patients, while auditory startle reflex was increased in iRBD only, suggesting the presence of both differences and similarities in RSWA and iRBD pathophysiology.121
Other Neurophysiological Investigations
Vegetative tests indicate that severity of autonomic dysfunction in iRBD seems to be intermediate between PD and normal values.122 Overall, orthostatic hypotension and RBD produced both combined and individual detrimental consequences on disability in alpha-synucleinopathy, possibly reflecting a “malignant subtype” of PD, along with postural instability and early cognitive decline. The involvement of selected noradrenergic and cholinergic brainstem nuclei may be among the proposed underlying pathomechanisms.123
Cortico-muscular coherence (CMC) is the functional correlate of connectivity between the primary motor cortex (as indexed by magnetoencephalography or EEG) and contralateral muscles during isometric activity.118 Under normal condition, CMC significantly lowers during REM sleep with respect to wakefulness; conversely, in RBD, CMC during the REM sleep was found to be higher than in controls, thus hypothesizing that cortical locomotor drive was enhanced during REM sleep in this disorder.124 These findings have been recently confirmed and extended by an independent study in which muscle atonia index, CMC, and cortico-cortical coherence revealed specific findings both in PDRBD and in iRBD groups.125
Lastly, some studies assessed psychophysiologic parameters, eg, through the active and passive oddball P300 paradigm.126 In iRBD, no difference was noted between patients and matched controls, at least at early-middle stages of the disease. Since cognitive alterations have been reported in RBD,127,128 event-related potentials using a cognitive task have been also tested. An occipital positive wave (P2) was found in PDRBD subjects, whereas it was nearly absent in healthy individuals. Of note, PDnoRBD were similar to controls, thus indicating that RBD may worsen the cortical dysfunction in PD.129
It should be acknowledged that, despite a number of available markers derived from different neurophysiological techniques, not all of them seem to have a diagnostic value or a clear prognostic role in the monitoring of disease progression or response to therapy. This may be due, at least in part, to the limited sample size included in most studies and some aspects of study design themselves (eg, drug-naïve vs de novo patients, adequate comparisons, technical/procedural variability, magnitude of the results, etc.).33 Therefore, a combined use of neurophysiological and other, multidimensional, biomarkers, will be needed, especially in the case of RBD subtyping and differential diagnosis.130,131 For instance, using solid neurophysiological features, such as RSWA, in combination with other types of biomarkers might have a relevant role in the identification and characterization of RBD as a prodromal form of PD.132 Nevertheless, longitudinal studies are required to verify whether the neurophysiological abnormalities detected at the early stages of RBD by EEG, TMS, VEMP, and other techniques correlate with clinical progression of RBD.
Table 2 summarizes main findings obtained from different neurophysiological techniques in patients with isolated REM sleep behavior disorder (iRBD), Parkinson’s disease with RBD (PDRBD), and Parkinson’s disease without RBD (PDnoRBD). Figure 1 summarizes the neurophysiological findings in iRBD, PDRBD and PDnoRBD population.
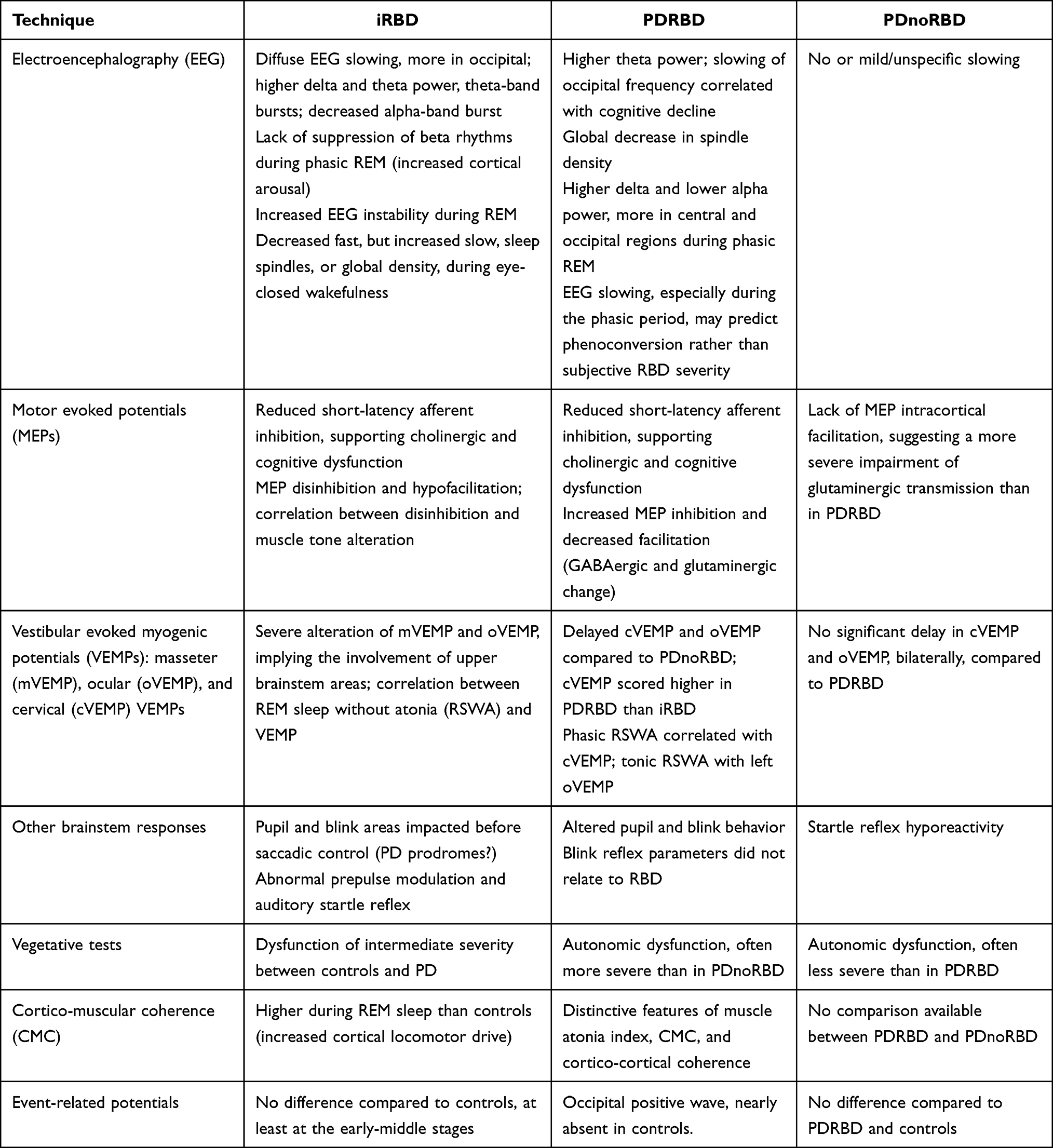 |
Table 2 Main Findings Obtained from Different Neurophysiological Techniques in Patients with Isolated REM Sleep Behavior Disorder (iRBD), Parkinson’s Disease with RBD (PDRBD), and Parkinson’s Disease Without RBD (PDnoRBD) |
 |
Figure 1 Neurophysiological findings in RBD population: Overview of the main electrophysiological techniques that have provided insights on the neurophysiological basis of RBD. Cortical activity is explored with conventional electroencephalography (EEG) and event-related potentials (ERPs). Cortico-muscular coherence (CMC) relates to the synchrony in the neural activity of brain’s cortical areas and muscles, thus allowing to study the neural control of movement. Motor evoked potentials (MEPs) to transcranial magnetic stimulation (TMS) specifically probe the excitation state of the primary motor cortex. Neurovegetative tests can be applied to functionally assess the hypothalamus, a key region for the central control of the autonomic nervous system. Finally, vestibular evoked myogenic potentials (VEMPs), as well as blink and startle reflexes, are suitable tools to evaluate the brainstem excitability. |
Parkinson’s Disease RBD Phenotype: Pharmacological Management
While many medications have been found to have some therapeutic effects on RBD, the overall effects of treatment are still unsatisfactory.
Clonazepam, a long-acting sedative benzodiazepine, is the first option to treat RBD,133 however, its mechanism of action is still unclear and the proof of its efficacy for RBD relies on many observational studies, mainly retrospective cohorts and case-series.134 Furthermore, most studies used small samples and did not contain quantitative measurements.
Clonazepam can dramatically decrease the phasic EMG activity on polysomnography, while there is insufficient evidence of reduction in the objective or subjective severity of RBD. It has been shown that Clonazepam can reduce phasic twitching in RBD without re-establish REM sleep muscle atonia.89
A recent randomized placebo-controlled trial was conducted in order to determine the efficacy and safety of clonazepam for the treatment of probable RBD (pRBD) in patients with PD.
The primary outcome was the Clinical Global Impressions Improvement score at week four. No significant difference in scores between the clonazepam and placebo groups was detected. The conclusions of this study must be interpreted cautiously. In fact, the authors recruited pRBD patients without VPSG confirmation.90
Very few studies have examined the effects of clonazepam on polysomnographic parameters. It has been previously reported in iRBD patients that 0.5 to 1 mg per day of clonazepam significantly improved the percentage of stage 2 sleep compared to baseline.135,136
However, clonazepam can worsen cognitive impairment and sleep apnea and it should be used cautiously in patients with these symptoms.11
Melatonin is recommended as a safe complementary treatment option for patients with RBD. Melatonin and clonazepam were found to be effective in reducing the symptoms of RBD, but melatonin was better tolerated with fewer adverse reactions and greater reduction in injury.137
Few studies are available on the therapeutic effects of melatonin on RBD. Melatonin is a hormone secreted by the pineal gland in a circadian pattern, influenced by dark environments with levels peaking during the middle of the night.134
Some studies have shown that 3 to 12 mg per day of melatonin can reduce RBD-related injuries with little side effects, though the numbers of RBD events has not decreased.134,137–140
Evidence suggests that melatonin improves RBD by reducing the tonic EMG activity during REM sleep, the inhibition of gamma-aminobutyric acid, the stabilization of the circadian rhythm, the increased striatal bioavailability of L-dopa and modulation of skeletal muscles.140
A recent randomized double-blind placebo-controlled trial was conducted to evaluate the efficacy of 4 mg slow-release melatonin in 30 patients with PD and RBD. The primary outcome was the difference in the total number of RBD events as assessed by the weekly CIRUS‐RBD Questionnaire (item - 4). The trial shows that melatonin 4 mg per day did not have a large effect on the reduction of RBD in PD patients, but it is still unknown if other doses are ineffective.141
Ramelteon is an agonist of melatonin receptors that has a positive impact on idiopathic and secondary RBD. Recently, two studies have shown that Ramelteon improve clinical RBD symptoms and decrease RWA in two patients for which conventional therapies were contraindicated.142,143 Kashihara et al showed that ramelteon improve nighttime sleep and PD motor performances according to UPDRS Part III scores.142
Randomized controlled studies of dopaminergic agonists for RBD in PD are still missing. Available uncontrolled studies, including those using newer dopaminergic agonists, are considered inconclusive.134
Dusek et al evaluated the impact of slow-release and immediate-release ropinirole on PD-related sleep disorders, including RBD. A total of 33 PD patients initially receiving immediate release ropinirole, followed by five to thirteen weeks of prolonged release ropinirole were investigated. The secondary outcome was to investigate the effects of slow-release versus immediate-release ropinirole on RBD symptoms assessed by RBDSQ. There was no statistically significant improvement in RBDSQ scores and RSWA.144
An open-label study was conducted to assess the effect of rotigotine on RBD in PD patients PDRBD patients. Subjects were treated for approximately 28 weeks at increasing doses from 2 to 16 mg/24 h according to parkinsonism response and tolerance. Patients were evaluated before and after treatment using the PSG, RBDSS, PDSS-2 and the REM sleep behavior disorder questionnaire-Hong Kong (RBDQ-HK) scales. At the end of the treatment, the PDSS-2, the overall RBDQ-HK scale scores decreased significantly. However, there were no objective changes in the motor variables assessed by PSG (percentage of RSWA) or RBDS.145
Pramipexole affects REM sleep by increasing REM sleep latency and reducing total REM sleep time.146 In patients with idiopathic RBD, pramipexole significantly decreased the frequency and severity of RBD symptoms and remained effective for 25 months.147 In contrast, PD patients with RBD did not have any benefit.148
In a prospective study, 11 PDRBD patients on levodopa monotherapy were treated with pramipexole. The effects on RBD were evaluated before and 3 months after stable pramipexole therapy through patient and bed partner interviews and blind assessment of video-polysomnography (VPSG) measures.134 Before and 3 months after stable pramipexole therapy, effects on RBD were assessed through patients and bed-partners interviews and VPSG measures.
No significant changes in severity and frequency of RBD related motor and vocal behavior as well as frequency of unpleasant dreams were reported by patients and bed-partners. The VPSG analyses showed no difference in sleep measures related to RBD and the severity of abnormal behavior revealed by the videotape.148
Currently rotigotine is the only dopaminergic agonist that has led to an improvement in the RBD symptoms in PD patients. That improvement appears to be due by improved nocturnal motor symptoms.149
Donepezil and rivastigmine can also be considered for treating patients with RBD, particularly in patients with cognitive impairment.150
The cholinesterase inhibitor rivastigmine has been used as a substitute treatment to melatonin and clonazepam. We found only one crossover double-blind study on the efficacy of rivastigmine in reducing the frequency of RBD episodes in PD.150
Rivastigmine was administered through a transdermal patch (4.6 mg/24 hours) for 3 weeks to non demented PDRBD patients that were refractory to melatonin and clonazepam.
Rivastigmine has demonstrated a beneficial effect on the reduction of RBD events and the improvement of subjective night sleep, proving to be a viable alternative in the control of RBD in patients resistant to conventional therapies. Unfortunately, the sample size was too small to reach definitive conclusions.
These preliminary data should be evaluated cautiously, as cases of RBD induced by acetylcholinesterase inhibitors have been reported.
Interestingly, a reduction in the frequency of refractory RBD episodes have been reported in subjects with mild cognitive impairment, who participated in a placebo-controlled, cross-over pilot trial of Rivastigmine.151
Moreover, the donepezil, another acetylcholinesterase inhibitor, has shown an effectiveness in improving RBD symptoms.152
Memantine may reduce the dream enactment frequency and the total REM sleep time.
A randomized controlled and multicenter study was conducted in order to assess the effectiveness of memantine on sleep disorders, including RBD in PD patients with dementia or DLB patients.134 After 24 weeks of treatment, subjects who received memantine significantly improved restlessness during sleep when compared to placebo. Nevertheless, the absence of PSG, both at the screening stage and at the follow-up, compromised the reliability of these results. Indeed, the RBD was assessed through a single question “Is the patient physically active during sleep?”.153
In a pilot study the use of cannabidiol (CBD) in PDRBD patients at doses ranging from 75 to 300 mg for six weeks, caused a reduction of up to 80% in the frequency of the nocturnal behaviors assessed through the sleep diary.154
Other drugs such as zopiclone (doses ranging from 3.75 to 7.5 mg) and sodium oxybate (doses ranging from 3 to 9 g) are also effective in RBD therapy, but their effectiveness has not been demonstrated in PD.155
Some case reports indicate that 10 mg daily of temazepam may be effective in treating RBD symptoms.155
There are also cases or small series that show the possible effectiveness of carbamazepine156 and gabapentin157 on RBD symptoms.
Antipsychotic drugs like quetiapine and clozapine have also been shown to be effective in patients with iRBD. However, there are no robust reports about their impact on RBD in PD.158
In a recent randomized, double-blind placebo-controlled crossover trial, the 5-hydroxytryptophan (a precursor of serotonin) increased the overall percentage of REM sleep stage without a related increase of RBD episodes. Moreover, the self-reported RBD frequency and severity were improved during 5-hydroxytryptophan treatment.159
The therapeutic effects of the Yi-Gan San, an herbal with gabaergic and serotonergic properties, has been described in iRBD.160
As evidenced by previous studies, there have been major limitations in subjective quantification of RBD symptoms. In a recent observational cohort study a newly developed RBD symptom severity scale (Ikelos-RS) has been used in a large group of patients with iRBD.161
Moreover, a self-administered modified RBDQ scale (the timeframe of the scale were modified into the past 3-month period) has proven to be a sensitive tool for monitoring treatment progress over a brief period of time.135 Table 3 summarizes the pharmacological treatment of RBD in PD patients.
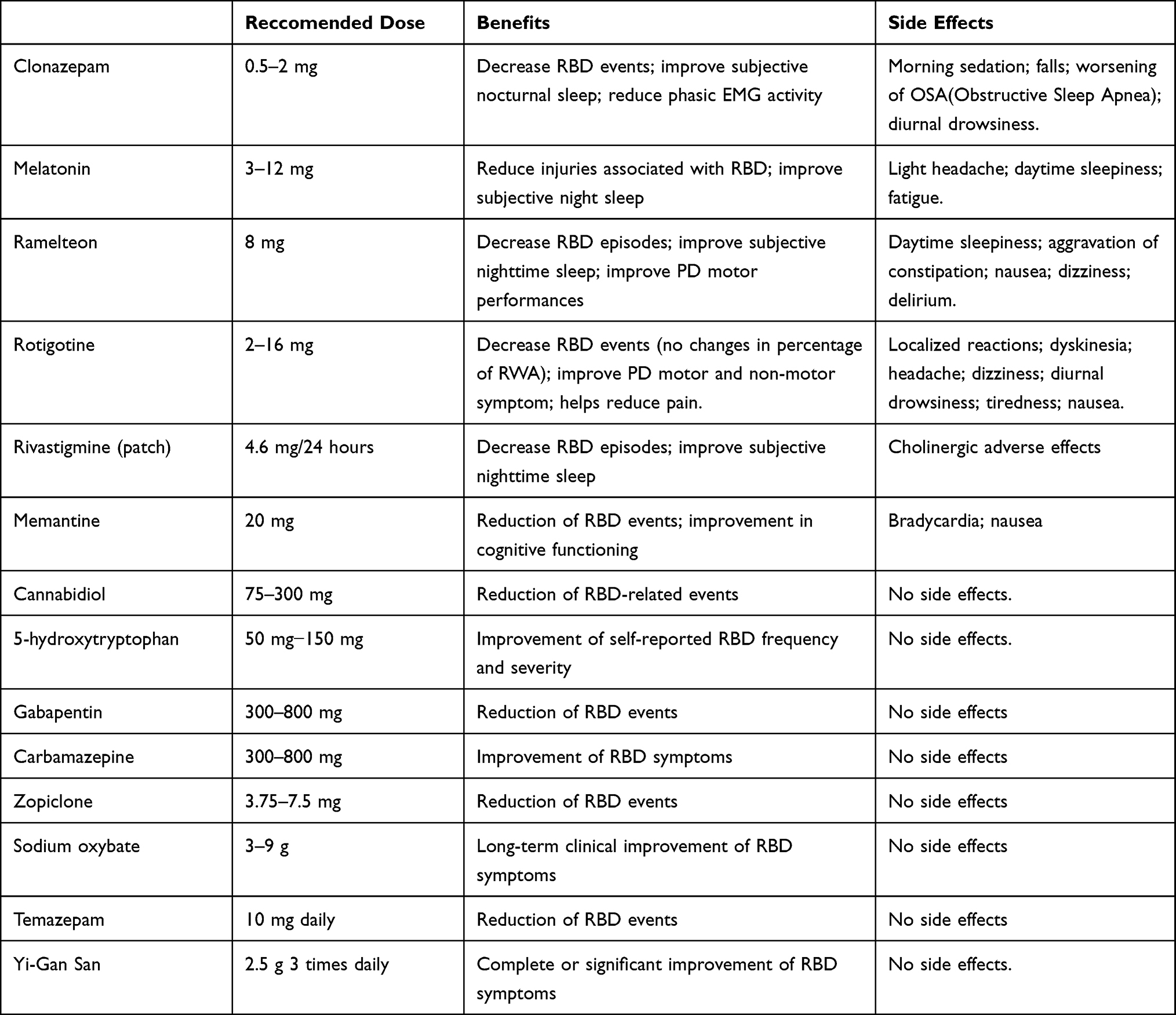 |
Table 3 Pharmacological Treatments of RBD in PD Patients |
Parkinson’s Disease RBD Phenotype: Non-Pharmacological Management
RBD patients, both isolated and associated with PD, are at risk of injuries, to themselves or to bedpartner, related to complex-motor dream-enacting behaviors.
Sleep protection measures are warranted to minimize the risk of injury to the patient and bedpartner. In order to improve the security of the bedroom, protective strategies such as the placement of mattresses on the ground or the securing of windows should be considered.162
Regular physical exercise is advisable in patients with PD and sleep disorders. In a recent meta-analysis has been found that exercise had a significant positive effect on subjective sleep quality in people with PD.163 Furthermore, it has been shown that intensive exercise may play a protective role through direct modulation of the accumulation of multiple proteins associated with neurodegenerative process. Since RBD is an early occurrence of a neurodegenerative disease caused by pathologic aggregates of α-synuclein, it would make sense to examine the potential neuroprotective effects of exercise with RBD patients.164
A reduced prevalence of prodromal features associated with PD in patients who were more physically active has been described in a recent study. PD subjects who maintained a high level of physical activity during follow-up were less susceptible to be affected by RBD symptoms.165
The benefits of multidisciplinary intensive rehabilitation treatment (MIRT) on sleep disorders in PD have been highlighted.140 Specifically, the rehabilitation treatment included a wide range of aerobic exercises combined with relaxation techniques, stretching exercises, stability exercises focused on balance and gait.166 However, research on exercise aimed at improving sleep disorders, including RBD, is still limited. Whereby the exercise modality, frequency, duration and intensity needed for sleep optimization are not known.167
Patients with RBD have a low arousal threshold of REM sleep. A reduction in RBD symptoms and sleep-related injuries was reported in four patients with RBD through the use of customized bed alarms with a familiar voice to deliver a soothing message at the beginning of dream enactment behaviors (level III of evidence).168
Many lines of evidence have demonstrated that deep brain stimulation (DBS) can ameliorate sleep quality in patients with PD.169 Some studies shown that DBS of the PPN may modulate some non-motor functions, including REM sleep, mood, arousal and sleep-wake cycle.170,171 However, some studies suggest that PPN-DBS could contribute to worsening RBD in PD patients.172
Conclusion
RBD offers a precious insight for the management of PD: not only its presence allows to individuate a population at risk of developing the disease, but also when the disease is conclamated it’s connected to a more aggressive phenotype for both motor and non-motor symptoms, especially cognitive impairment.
This can guide the physician to a more tailored treatment and follow up of PD patients, focusing on early intervention for the prevention and management of cognitive impairment.
Finally, iRBD is a unique cohort of patients ready to access to future trials of neuroprotective and disease modifying therapy.
Future research should focus on the creation of combination models and stratification of biomarkers in order to have easily accessible and reliable tools to select patients at risk of phenoconversion or to individuate early signs of cognitive impairment.
Final Remarks
- iRBD has an estimated risk to develop a neurodegenerative disease up to 90%, thus representing an ideal condition for testing new neuroprotective and disease-modifying drug.
- RBD seems to be a key clinical indicator of a body-first/diffuse-malignant phenotype, characterized by a more widespread neurodegenerative process and worse motor and non-motor symptoms of PD.
- RSWA, the neurophysiological hallmark of RBD, correlates with worse cognitive performances and MCI, and/or impaired attention and executive functions might predict early conversion to dementia.
- Some medications and non-pharmacological options have been found to have some therapeutic effects on RBD, although their overall impact is still unsatisfactory and, therefore, new evidence-based approaches are needed.
- Several clinical, neurophysiological, neuroimaging, biological, and genetic biomarkers have been individuated, although a consensus on the identification of one or more biomarkers to be translated in clinical practice is still lacking.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Matar E, McCarter SJ, St Louis EK, Lewis SJG. Current Concepts and Controversies in the Management of REM Sleep Behavior Disorder. Neurotherapeutics. 2021;18(1):107–123. doi:10.1007/s13311-020-00983-7
2. Dauvilliers Y, Schenck CH, Postuma RB, et al. REM sleep behaviour disorder. Nat Rev Dis Primers. 2018;4(1):19. doi:10.1038/s41572-018-0016-5
3. Iranzo A. The REM sleep circuit and how its impairment leads to REM sleep behavior disorder. Cell Tissue Res. 2018;373(1):245–266. doi:10.1007/s00441-018-2852-8
4. Iranzo A, Santamaria J, Tolosa E. The clinical and pathophysiological relevance of REM sleep behavior disorder in neurodegenerative diseases. Sleep Med Rev. 2009;13(6):385–401. doi:10.1016/j.smrv.2008.11.003
5. Haba-Rubio J, Marti-Soler H, Marques-Vidal P, et al. Prevalence and determinants of periodic limb movements in the general population: PLMS in the General Population. Ann Neurol. 2016;79(3):464–474. doi:10.1002/ana.24593
6. Pujol M, Pujol J, Alonso T, et al. Idiopathic REM sleep behavior disorder in the elderly Spanish community: a primary care center study with a two-stage design using video-polysomnography. Sleep Med. 2017;40:116–121. doi:10.1016/j.sleep.2017.07.021
7. Iranzo A, Santamaria J, Tolosa E. Idiopathic rapid eye movement sleep behaviour disorder: diagnosis, management, and the need for neuroprotective interventions. Lancet Neurol. 2016;15(4):405–419. doi:10.1016/S1474-4422(16)00057-0
8. Högl B, Arnulf I, Bergmann M, et al. Rapid eye movement sleep behaviour disorder: past, present, and future. J Sleep Res. 2022;31:4. doi:10.1111/jsr.13612
9. Fereshtehnejad SM, Zeighami Y, Dagher A, Postuma RB. Clinical criteria for subtyping Parkinson’s disease: biomarkers and longitudinal progression. Brain. 2017;140(7):1959–1976. doi:10.1093/brain/awx118
10. Marras C, Chaudhuri KR. Nonmotor features of ParkinsonParkinson’s disease subtypes. Mov Disord. 2016;31(8):1095–1102. doi:10.1002/mds.26510
11. Schenck CH, Bundlie SR, Mahowald MW. Delayed emergence of a parkinsonian disorder in 38% of 29 older men initially diagnosed with idiopathic rapid eye movement sleep behavior disorder. Neurology. 1996;46(2):388–393. doi:10.1212/wnl.46.2.388
12. Braak H, Del Tredici K, Rüb U, de Vos RAI, Jansen Steur ENH, Braak E. Staging of brain pathology related to sporadic Parkinson’s disease. Neurobiol Aging. 2003;24(2):197–211. doi:10.1016/s0197-4580(02
13. Valencia Garcia S, Brischoux F, Clément O, et al. Ventromedial medulla inhibitory neuron inactivation induces REM sleep without atonia and REM sleep behavior disorder. Nat Commun. 2018;9(1):504. doi:10.1038/s41467-017-02761-0
14. Braak H, Ghebremedhin E, Rüb U, Bratzke H, Del Tredici K. Stages in the development of Parkinson’s disease-related pathology. Cell Tissue Res. 2004;318(1):121–134. doi:10.1007/s00441-004-0956-9
15. Hawkes CH, Del Tredici K, Braak H. Parkinson’s disease: a dual-hit hypothesis. Neuropathol Appl Neurobiol. 2007;33(6):599–614. doi:10.1111/j.1365-2990.2007.00874.x
16. Van Den Berge N, Ulusoy A. Animal models of brain-first and body-first Parkinson’s disease. Neurobiol Dis. 2022;163:105599. doi:10.1016/j.nbd.2021.105599
17. Attems J, Jellinger KA. The dorsal motor nucleus of the vagus is not an obligatory trigger site of Parkinson’s disease. Neuropathol Appl Neurobiol. 2008;34(4):466–467. doi:10.1111/j.1365-2990.2008.00937.x
18. Jellinger KA. Is Braak staging valid for all types of Parkinson’s disease? J Neural Transm. 2019;126(4):423–431. doi:10.1007/s00702-018-1898-9
19. Borghammer P, Van Den Berge N. Brain-First versus Gut-First Parkinson’s Disease: a Hypothesis. JPD. 2019;9(s2):S281–S295. doi:10.3233/JPD-191721
20. Horsager J, Andersen KB, Knudsen K, et al. Brain-first versus body-first Parkinson’s disease: a multimodal imaging case-control study. Brain. 2020;143(10):3077–3088. doi:10.1093/brain/awaa238
21. McKenna D, Peever J. Degeneration of rapid eye movement sleep circuitry underlies rapid eye movement sleep behavior disorder. Mov Disord. 2017;32(5):636–644. doi:10.1002/mds.27003
22. Leclair-Visonneau L, Clairembault T, Coron E, et al. REM sleep behavior disorder is related to enteric neuropathology in Parkinson disease. Neurology. 2017;89(15):1612–1618. doi:10.1212/WNL.0000000000004496
23. Postuma RB, Adler CH, Dugger BN, et al. REM sleep behavior disorder and neuropathology in Parkinson’s disease: RBD in PD. Mov Disord. 2015;30(10):1413–1417. doi:10.1002/mds.26347
24. Bohnen NI, Postuma RB. Body-first versus brain-first biological subtyping of Parkinson’s disease. Brain. 2020;143(10):2871–2873. doi:10.1093/brain/awaa293
25. Borghammer P. The α-Synuclein Origin and Connectome Model (SOC Model) of Parkinson’s Disease: explaining Motor Asymmetry, Non-Motor Phenotypes, and Cognitive Decline. JPD. 2021;11(2):455–474. doi:10.3233/JPD-202481
26. Oltra J, Uribe C, Segura B, et al. Brain atrophy pattern in de novo Parkinson’s disease with probable RBD associated with cognitive impairment. npj Parkinsons Dis. 2022;8(1):60. doi:10.1038/s41531-022-00326-7
27. Riboldi GM, Russo MJ, Pan L, Watkins K, Kang UJ. Dysautonomia and REM sleep behavior disorder contributions to progression of Parkinson’s disease phenotypes. npj Parkinsons Dis. 2022;8(1):110. doi:10.1038/s41531-022-00373-0
28. Fereshtehnejad SM, Romenets SR, Anang JBM, Latreille V, Gagnon JF, Postuma RB. New Clinical Subtypes of Parkinson Disease and Their Longitudinal Progression: a Prospective Cohort Comparison With Other Phenotypes. JAMA Neurol. 2015;72(8):863. doi:10.1001/jamaneurol.2015.0703
29. Fereshtehnejad SM, Postuma RB. Subtypes of Parkinson’s Disease: what Do They Tell Us About Disease Progression? Curr Neurol Neurosci Rep. 2017;17(4). doi:10.1007/s11910-017-0738-x
30. Zhang H, Iranzo A, Högl B, et al. Risk Factors for Phenoconversion in Rapid Eye Movement Sleep Behavior Disorder. Ann Neurol. 2022;91(3):404–416. doi:10.1002/ana.26298
31. Schenck CH, Boeve BF, Mahowald MW. Delayed emergence of a parkinsonian disorder or dementia in 81% of older men initially diagnosed with idiopathic rapid eye movement sleep behavior disorder: a 16-year update on a previously reported series. Sleep Med. 2013;14(8):744–748. doi:10.1016/j.sleep.2012.10.009
32. de Natale ER, Wilson H, Politis M. Predictors of RBD progression and conversion to synucleinopathies. Curr Neurol Neurosci Rep. 2022;22(2):93–104. doi:10.1007/s11910-022-01171-0
33. Miglis MG, Adler CH, Antelmi E, et al. Biomarkers of conversion to α-synucleinopathy in isolated rapid-eye-movement sleep behaviour disorder. Lancet Neurol. 2021;20(8):671–684. doi:10.1016/S1474-4422(21)00176-9
34. Postuma RB, Iranzo A, Hu M, et al. Risk and predictors of dementia and parkinsonism in idiopathic REM sleep behaviour disorder: a multicentre study. Brain. 2019;142(3):744–759. doi:10.1093/brain/awz030
35. Fereshtehnejad SM, Yao C, Pelletier A, Montplaisir JY, Gagnon JF, Postuma RB. Evolution of prodromal Parkinson’s disease and dementia with Lewy bodies: a prospective study. Brain. 2019;142(7):2051–2067. doi:10.1093/brain/awz111
36. Del Din S, Yarnall AJ, Barber TR, et al. Continuous Real-World Gait Monitoring in Idiopathic REM Sleep Behavior Disorder. J Parkinsons Dis. 2020;10(1):283–299. doi:10.3233/JPD-191773
37. Arora S, Baig F, Lo C, et al. Smartphone motor testing to distinguish idiopathic REM sleep behavior disorder, controls, and PD. Neurology. 2018;91(16):e1528–e1538. doi:10.1212/WNL.0000000000006366
38. Hanuška J, Rusz J, Bezdicek O, et al. Eye movements in idiopathic rapid eye movement sleep behaviour disorder: high antisaccade error rate reflects prefrontal cortex dysfunction. J Sleep Res. 2019;28(5):e12742. doi:10.1111/jsr.12742
39. Krupička R, Krýže P, Neťuková S, et al. Instrumental analysis of finger tapping reveals a novel early biomarker of parkinsonism in idiopathic rapid eye movement sleep behaviour disorder. Sleep Med. 2020;75:45–49. doi:10.1016/j.sleep.2020.07.019
40. Berg D, Postuma RB, Adler CH, et al. MDS research criteria for prodromal Parkinson’s disease. Mov Disord. 2015;30(12):1600–1611. doi:10.1002/mds.26431
41. Iranzo A, Marrero-González P, Serradell M, Gaig C, Santamaria J, Vilaseca I. Significance of hyposmia in isolated REM sleep behavior disorder. J Neurol. 2021;268(3):963–966. doi:10.1007/s00415-020-10229-3
42. Miyamoto T, Miyamoto M. Odor identification predicts the transition of patients with isolated RBD: a retrospective study. Ann Clin Transl Neurol. 2022;9(8):1177–1185. doi:10.1002/acn3.51615
43. Postuma RB, Gagnon JF, Vendette M, Desjardins C, Montplaisir JY. Olfaction and color vision identify impending neurodegeneration in rapid eye movement sleep behavior disorder. Ann Neurol. 2011;69(5):811–818. doi:10.1002/ana.22282
44. Li Y, Zhang H, Mao W, et al. Visual dysfunction in patients with idiopathic rapid eye movement sleep behavior disorder. Neurosci Lett. 2019;709:134360. doi:10.1016/j.neulet.2019.134360
45. Yang ZJ, Wei J, Mao CJ, et al. Retinal nerve fiber layer thinning: a window into rapid eye movement sleep behavior disorders in Parkinson’s disease. Sleep Breath. 2016;20(4):1285–1292. doi:10.1007/s11325-016-1366-4
46. Ferini-Strambi L, Oertel W, Dauvilliers Y, et al. Autonomic symptoms in idiopathic REM behavior disorder: a multicentre case–control study. J Neurol. 2014;261(6):1112–1118. doi:10.1007/s00415-014-7317-8
47. Zitser J, During EH, Chiaro G, Miglis MG. Autonomic impairment as a potential biomarker in idiopathic REM-sleep-behavior disorder. Autonomic Neurosci. 2019;220:102553. doi:10.1016/j.autneu.2019.05.005
48. Postuma RB, Lanfranchi PA, Blais H, Gagnon JF, Montplaisir JY. Cardiac autonomic dysfunction in idiopathic REM sleep behavior disorder. Mov Disord. 2010;25(14):2304–2310. doi:10.1002/mds.23347
49. Yang JH, Choi SH, Lee MH, et al. Association of heart rate variability with REM sleep without atonia in idiopathic REM sleep behavior disorder. J Clin Sleep Med. 2021;17(3):461–469. doi:10.5664/JCSM.8934
50. McCarter SJ, Gehrking TL, St Louis EK, et al. Autonomic dysfunction and phenoconversion in idiopathic REM sleep behavior disorder. Clin Auton Res. 2020;30(3):207–213. doi:10.1007/s10286-020-00674-5
51. Bauckneht M, Chincarini A, De Carli F, et al. Presynaptic dopaminergic neuroimaging in REM sleep behavior disorder: a systematic review and meta-analysis. Sleep Med Rev. 2018;41:266–274. doi:10.1016/j.smrv.2018.04.001
52. Iranzo A, Santamaría J, Valldeoriola F, et al. Dopamine transporter imaging deficit predicts early transition to synucleinopathy in idiopathic rapid eye movement sleep behavior disorder. Ann Neurol. 2017;82(3):419–428. doi:10.1002/ana.25026
53. Li Y, Kang W, Yang Q, et al. Predictive markers for early conversion of iRBD to neurodegenerative synucleinopathy diseases. Neurology. 2017;88(16):1493–1500. doi:10.1212/WNL.0000000000003838
54. Chahine LM, Brumm MC, Caspell-Garcia C, et al. Dopamine transporter imaging predicts clinically-defined α-synucleinopathy in REM sleep behavior disorder. Ann Clin Transl Neurol. 2021;8(1):201–212. doi:10.1002/acn3.51269
55. Arnaldi D, Chincarini A, Hu MT, et al. Dopaminergic imaging and clinical predictors for phenoconversion of REM sleep behaviour disorder. Brain. 2021;144(1):278–287. doi:10.1093/brain/awaa365
56. Arnaldi D, Famà F, Girtler N, et al. Rapid eye movement sleep behavior disorder: a proof-of-concept neuroprotection study for prodromal synucleinopathies. Eur J Neurol. 2021;28(4):1210–1217. doi:10.1111/ene.14664
57. Dang-Vu TT, Gagnon JF, Vendette M, Soucy JP, Postuma RB, Montplaisir J. Hippocampal perfusion predicts impending neurodegeneration in REM sleep behavior disorder. Neurology. 2012;79(24):2302–2306. doi:10.1212/WNL.0b013e318278b658
58. Heller J, Brcina N, Dogan I, et al. Brain imaging findings in idiopathic REM sleep behavior disorder (RBD) – a systematic review on potential biomarkers for neurodegeneration. Sleep Med Rev. 2017;34:23–33. doi:10.1016/j.smrv.2016.06.006
59. Campabadal A, Segura B, Junque C, Iranzo A. Structural and functional magnetic resonance imaging in isolated REM sleep behavior disorder: a systematic review of studies using neuroimaging software. Sleep Med Rev. 2021;59:101495. doi:10.1016/j.smrv.2021.101495
60. Ota Y, Kanel P, Bohnen N. Imaging of sleep disorders in pre-Parkinsonian syndromes. Curr Opin Neurol. 2022;35(4):443–452. doi:10.1097/WCO.0000000000001084
61. Shi M, Sheng L, Stewart T, Zabetian CP, Zhang J. New windows into the brain: central nervous system-derived extracellular vesicles in blood. Prog Neurobiol. 2019;175:96–106. doi:10.1016/j.pneurobio.2019.01.005
62. Kluge A, Bunk J, Schaeffer E, et al. Detection of neuron-derived pathological α-synuclein in blood. Brain. 2022;145(9):3058–3071. doi:10.1093/brain/awac115
63. Stefani A, Iranzo A, Holzknecht E, et al. Alpha-synuclein seeds in olfactory mucosa of patients with isolated REM sleep behaviour disorder. Brain. 2021;144(4):1118–1126. doi:10.1093/brain/awab005
64. Zitser J, Gibbons C, Miglis MG. The role of tissue biopsy as a biomarker in REM sleep behavior disorder. Sleep Med Rev. 2020;51:101283. doi:10.1016/j.smrv.2020.101283
65. Iranzo A, Fairfoul G, Ayudhaya ACN, et al. Detection of α-synuclein in CSF by RT-QuIC in patients with isolated rapid-eye-movement sleep behaviour disorder: a longitudinal observational study. Lancet Neurol. 2021;20(3):203–212. doi:10.1016/S1474-4422(20)30449-X
66. Thaler A, Bregman N, Gurevich T, et al. Parkinson’s disease phenotype is influenced by the severity of the mutations in the GBA gene. Parkinsonism Relat Disord. 2018;55:45–49. doi:10.1016/j.parkreldis.2018.05.009
67. Krohn L, Ruskey JA, Rudakou U, et al. GBA variants in REM sleep behavior disorder: a multicenter study. Neurology. 2020;95(8):e1008–e1016. doi:10.1212/WNL.0000000000010042
68. Honeycutt L, Montplaisir JY, Gagnon JF, et al. Glucocerebrosidase mutations and phenoconversion of REM sleep behavior disorder to parkinsonism and dementia. Parkinsonism Relat Disord. 2019;65:230–233. doi:10.1016/j.parkreldis.2019.04.016
69. Krohn L, Wu RYJ, Heilbron K, et al. Fine‐Mapping of SNCA in Rapid Eye Movement Sleep Behavior Disorder and Overt Synucleinopathies. Ann Neurol. 2020;87(4):584–598. doi:10.1002/ana.25687
70. Ye G, Li Y, Zhou L, et al. Predictors of Conversion to α-Synucleinopathy Diseases in Idiopathic Rapid Eye Movement Sleep Behavior Disorder. J Parkinsons Dis. 2020;10(4):1443–1455. doi:10.3233/JPD-202243
71. Terzaghi M, Toscano G, Casoni F, et al. Assessment of cognitive profile as a prodromal marker of the evolution of REM sleep Behavior Disorder. Sleep. 2019. doi:10.1093/sleep/zsz103
72. Vendette M, Montplaisir J, Gosselin N, et al. Brain perfusion anomalies in rapid eye movement sleep behavior disorder with mild cognitive impairment. Mov Disord. 2012;27(10):1255–1261. doi:10.1002/mds.25034
73. Jozwiak N, Postuma RB, Montplaisir J, et al. REM Sleep Behavior Disorder and Cognitive Impairment in Parkinson’s Disease. Sleep. 2017;40:8. doi:10.1093/sleep/zsx101
74. Marchand DG, Montplaisir J, Postuma RB, Rahayel S, Gagnon JF. Detecting the Cognitive Prodrome of Dementia with Lewy Bodies: a Prospective Study of REM Sleep Behavior Disorder. Sleep. 2017;40:1. doi:10.1093/sleep/zsw014
75. Gagnon JF, Vendette M, Postuma RB, et al. Mild cognitive impairment in rapid eye movement sleep behavior disorder and Parkinson’s disease. Ann Neurol. 2009;66(1):39–47. doi:10.1002/ana.21680
76. McCarter SJ, Tabatabai GM, Jong HY, et al. REM sleep atonia loss distinguishes synucleinopathy in older adults with cognitive impairment. Neurology. 2020;94(1):e15–e29. doi:10.1212/WNL.0000000000008694
77. Rahayel S, Postuma RB, Montplaisir J, et al. Cortical and subcortical gray matter bases of cognitive deficits in REM sleep behavior disorder. Neurology. 2018;90(20):e1759–e1770. doi:10.1212/WNL.0000000000005523
78. Rahayel S, Postuma RB, Montplaisir J, et al. A Prodromal Brain-Clinical Pattern of Cognition in Synucleinopathies. Ann Neurol. 2021;89(2):341–357. doi:10.1002/ana.25962
79. Rémillard-Pelchat D, Rahayel S, Gaubert M, et al. Comprehensive Analysis of Brain Volume in REM Sleep Behavior Disorder with Mild Cognitive Impairment. J Parkinsons Dis. 2022;12(1):229–241. doi:10.3233/JPD-212691
80. Postuma RB, Iranzo A, Hogl B, et al. Risk factors for neurodegeneration in idiopathic rapid eye movement sleep behavior disorder: a multicenter study. Ann Neurol. 2015;77(5):830–839. doi:10.1002/ana.24385
81. Génier Marchand D, Postuma RB, Escudier F, et al. How does dementia with Lewy bodies start? Prodromal cognitive changes in REM sleep behavior disorder. Ann Neurol. 2018;83(5):1016–1026. doi:10.1002/ana.25239
82. Génier Marchand D, Montplaisir J, Postuma RB, Rahayel S, Gagnon JF. Detecting the Cognitive Prodrome of Dementia with Lewy Bodies: a Prospective Study of REM Sleep Behavior Disorder. Sleep. 2017;40:1. doi:10.1093/sleep/zsw014
83. Heinzel S, Berg D, Gasser T, et al. Update of the MDS research criteria for prodromal Parkinson’s disease. Mov Disord. 2019;34(10):1464–1470. doi:10.1002/mds.27802
84. Gagnon JF, Bertrand JA, Génier Marchand D. Cognition in rapid eye movement sleep behavior disorder. Front Neurol. 2012;3:82. doi:10.3389/fneur.2012.00082
85. Ferini-Strambi L, Fasiello E, Sforza M, Salsone M, Galbiati A. Neuropsychological, electrophysiological, and neuroimaging biomarkers for REM behavior disorder. Expert Rev Neurother. 2019;19(11):1069–1087. doi:10.1080/14737175.2019.1640603
86. Figorilli M, Lanza G, Congiu P, et al. Neurophysiological Aspects of REM Sleep Behavior Disorder (RBD): a Narrative Review. Brain Sci. 2021;11(12):1588. doi:10.3390/brainsci11121588
87. Valomon A, Riedner BA, Jones SG, et al. A high-density electroencephalography study reveals abnormal sleep homeostasis in patients with rapid eye movement sleep behavior disorder. Sci Rep. 2021;11(1):4758. doi:10.1038/s41598-021-83980-w
88. Ferri R, Rundo F, Silvani A, et al. REM Sleep EEG Instability in REM Sleep Behavior Disorder and Clonazepam Effects. Sleep. 2017;40:8. doi:10.1093/sleep/zsx080
89. Ferri R, Zucconi M, Marelli S, Plazzi G, Schenck CH, Ferini-Strambi L. Effects of long-term use of clonazepam on nonrapid eye movement sleep patterns in rapid eye movement sleep behavior disorder. Sleep Med. 2013;14(5):399–406. doi:10.1016/j.sleep.2013.01.007
90. Shin C, Park H, Lee WW, Kim HJ, Kim HJ, Jeon B. Clonazepam for probable REM sleep behavior disorder in Parkinson’s disease: a randomized placebo-controlled trial. J Neurol Sci. 2019;401:81–86. doi:10.1016/j.jns.2019.04.029
91. Hadi F, Agah E, Tavanbakhsh S, et al. Safety and efficacy of melatonin, clonazepam, and trazodone in patients with Parkinson’s disease and sleep disorders: a randomized, double-blind trial. Neurol Sci. 2022;43(10):6141–6148. doi:10.1007/s10072-022-06188-4
92. Yan J, Liu A, Huang J, et al. Pharmacological Interventions for REM Sleep Behavior Disorder in Parkinson’s Disease: a Systematic Review. Front Aging Neurosci. 2021;13:709878. doi:10.3389/fnagi.2021.709878
93. Que Z, Zheng C, Zhao Z, et al. The treatment efficacy of pharmacotherapies for rapid eye movement sleep behavior disorder with polysomnography evaluation: a systematic review and meta-analysis. Heliyon. 2022;8(11):e11425. doi:10.1016/j.heliyon.2022.e11425
94. Brooks PL, Peever JH. Impaired GABA and glycine transmission triggers cardinal features of rapid eye movement sleep behavior disorder in mice. J Neurosci. 2011;31(19):7111–7121. doi:10.1523/JNEUROSCI.0347-11.2011
95. Parrino L, Ferri R, Bruni O, Terzano MG. Cyclic alternating pattern (CAP): the marker of sleep instability. Sleep Med Rev. 2012;16(1):27–45. doi:10.1016/j.smrv.2011.02.003
96. Kutlu A, Işeri P, Selekler M, Benbir G, Karadeniz D. Cyclic alternating pattern analysis in REM sleep behavior disorder. Sleep and Breathing. 2013;17(1):209–215. doi:10.1007/s11325-012-0675-5
97. Melpignano A, Parrino L, Santamaria J, et al. Isolated rapid eye movement sleep behavior disorder and cyclic alternating pattern: is sleep microstructure a predictive parameter of neurodegeneration? Sleep. 2019;42(10):zsz142. doi:10.1093/sleep/zsz142
98. O’Reilly C, Godin I, Montplaisir J, Nielsen T. REM sleep behaviour disorder is associated with lower fast and higher slow sleep spindle densities. J Sleep Res. 2015;24(6):593–601. doi:10.1111/jsr.12309
99. Christensen JAE, Kempfner J, Zoetmulder M, et al. Decreased sleep spindle density in patients with idiopathic REM sleep behavior disorder and patients with Parkinson’s disease. Clin Neurophysiol. 2014;125(3):512–519. doi:10.1016/j.clinph.2013.08.013
100. Ruffini G, Ibañez D, Castellano M, et al. Deep Learning With EEG Spectrograms in Rapid Eye Movement Behavior Disorder. Front Neurol. 2019;10:806. doi:10.3389/fneur.2019.00806
101. Gong S-Y, Shen Y, Gu H-Y, et al. Generalized EEG Slowing Across Phasic REM Sleep, Not Subjective RBD Severity, Predicts Neurodegeneration in Idiopathic RBD. Nat Sci Sleep. 2022;14:407–418. doi:10.2147/NSS.S354063
102. Lanza G, DelRosso LM, Ferri R. Sleep and homeostatic control of plasticity. Handb Clin Neurol. 2022;184:53–72. doi:10.1016/B978-0-12-819410-2.00004-7
103. Fisicaro F, Lanza G, Cantone M, et al. Clinical and Electrophysiological Hints to TMS in De Novo Patients with Parkinson’s Disease and Progressive Supranuclear Palsy. J Pers Med. 2020;10(4):E274. doi:10.3390/jpm10040274
104. Cantone M, Lanza G, Ranieri F, Opie GM, Terranova C. Editorial: non-invasive Brain Stimulation in the Study and Modulation of Metaplasticity in Neurological Disorders. Front Neurol. 2021;12:721906. doi:10.3389/fneur.2021.721906
105. Di Lazzaro V, Bella R, Benussi A, et al. Diagnostic contribution and therapeutic perspectives of transcranial magnetic stimulation in dementia. Clin Neurophysiol. 2021;132(10):2568–2607. doi:10.1016/j.clinph.2021.05.035
106. Nardone R, Bergmann J, Kunz A, et al. Cortical afferent inhibition is reduced in patients with idiopathic REM sleep behavior disorder and cognitive impairment: a TMS study. Sleep Med. 2012;13(7):919–925. doi:10.1016/j.sleep.2012.03.009
107. Nardone R, Bergmann J, Brigo F, et al. Functional evaluation of central cholinergic circuits in patients with Parkinson’s disease and REM sleep behavior disorder: a TMS study. J Neural Transm. 2013;120(3):413–422. doi:10.1007/s00702-012-0888-6
108. Lanza G, Aricò D, Lanuzza B, et al. Facilitatory/inhibitory intracortical imbalance in REM sleep behavior disorder: early electrophysiological marker of neurodegeneration? Sleep. 2020;43(3):zsz242. doi:10.1093/sleep/zsz242
109. Peever J, Luppi PH, Montplaisir J. Breakdown in REM sleep circuitry underlies REM sleep behavior disorder. Trends Neurosci. 2014;37(5):279–288. doi:10.1016/j.tins.2014.02.009
110. Lanza G, Cosentino FII, Lanuzza B, et al. Reduced Intracortical Facilitation to TMS in Both Isolated REM Sleep Behavior Disorder (RBD) and Early Parkinson’s Disease with RBD. J Clin Med. 2022;11(9):2291. doi:10.3390/jcm11092291
111. Bhattacharya A, Kamble N, Yadav R, Stezin A, Pal PK. Abnormal Intracortical Functions in Parkinson’s Disease with Rapid Eye Movement Sleep Behaviour Disorder. Can J Neurol Sci. 2022;49(5):672–677. doi:10.1017/cjn.2021.206
112. Lanza G, Fisicaro F, Cantone M, et al. Repetitive transcranial magnetic stimulation in primary sleep disorders. Sleep Med Rev. 2023;67:101735. doi:10.1016/j.smrv.2022.101735
113. Magnano I, Pes GM, Cabboi MP, et al. Comparison of brainstem reflex recordings and evoked potentials with clinical and MRI data to assess brainstem dysfunction in multiple sclerosis: a short-term follow-up. Neurol Sci. 2016;37(9):1457–1465. doi:10.1007/s10072-016-2604-z
114. de Natale ER, Ginatempo F, Laccu I, et al. Vestibular Evoked Myogenic Potentials Are Abnormal in Idiopathic REM Sleep Behavior Disorder. Front Neurol. 2018;9:911. doi:10.3389/fneur.2018.00911
115. de Natale ER, Ginatempo F, Paulus KS, et al. Abnormalities of vestibular-evoked myogenic potentials in idiopathic Parkinson’s disease are associated with clinical evidence of brainstem involvement. Neurol Sci. 2015;36(6):995–1001. doi:10.1007/s10072-014-2054-4
116. Puligheddu M, Figorilli M, Serra A, et al. REM Sleep without atonia correlates with abnormal vestibular-evoked myogenic potentials in isolated REM sleep behavior disorder. Sleep. 2019;42(9):zsz128. doi:10.1093/sleep/zsz128
117. Xie WY, Shen Y, Chen Y, et al. REM sleep without atonia and vestibular-evoked myogenic potentials: clinical brainstem dysfunction in early-stage Parkinson’s disease and isolated REM sleep behavior disorder. Sleep Med. 2022;89:122–129. doi:10.1016/j.sleep.2021.12.004
118. Stefani A, Holzknecht E, Högl B. Clinical neurophysiology of REM parasomnias. Handb Clin Neurol. 2019;161:381–396. doi:10.1016/B978-0-444-64142-7.00062-X
119. Perkins JE, Janzen A, Bernhard FP, et al. Saccade, Pupil, and Blink Responses in Rapid Eye Movement Sleep Behavior Disorder. Mov Disord. 2021;36(7):1720–1726. doi:10.1002/mds.28585
120. Weise D, Pargac C, Pelz JO, Rumpf JJ, Fricke C, Classen J. Assessing blink reflex circuits by three different afferent routes in Parkinson’s disease. Clin Neurophysiol. 2019;130(4):582–587. doi:10.1016/j.clinph.2018.12.009
121. Aygün D, Ertaş Fİ, Gündüz A, Benbir Şenel G, Karadeniz D, Kızıltan M. The role of pedunculopontine nucleus in isolated REM sleep behavior disorder and REM sleep without atonia. Parkinsonism Relat Disord. 2021;84:68–73. doi:10.1016/j.parkreldis.2021.01.025
122. Frauscher B, Nomura T, Duerr S, et al. Investigation of autonomic function in idiopathic REM sleep behavior disorder. J Neurol. 2012;259(6):1056–1061. doi:10.1007/s00415-011-6298-0
123. Pilotto A, Romagnolo A, Tuazon JA, et al. Orthostatic hypotension and REM sleep behaviour disorder: impact on clinical outcomes in α-synucleinopathies. J Neurol Neurosurg Psychiatry. 2019;90(11):1257–1263. doi:10.1136/jnnp-2019-320846
124. Jung KY, Cho JH, Ko D, et al. Increased Corticomuscular Coherence in Idiopathic REM Sleep Behavior Disorder. Front Neurol. 2012;3:60. doi:10.3389/fneur.2012.00060
125. Choi GS, Yun JY, Hwang S, et al. Can Corticomuscular Coherence Differentiate between REM Sleep Behavior Disorder with or without Parkinsonism? J Clin Med. 2021;10(23):5585. doi:10.3390/jcm10235585
126. Raggi A, Manconi M, Consonni M, et al. Event-related potentials in idiopathic rapid eye movements sleep behaviour disorder. Clin Neurophysiol. 2007;118(3):669–675. doi:10.1016/j.clinph.2006.11.011
127. Raggi A, Lanza G, Ferri RA. Review on P300 in Obsessive-Compulsive Disorder. Front Psychiatry. 2021;12:751215. doi:10.3389/fpsyt.2021.751215
128. Raggi A, Lanza G, Ferri R. Auditory mismatch negativity in bipolar disorder: a focused review. Rev Neurosci. 2022;33(1):17–30. doi:10.1515/revneuro-2021-0010
129. Gaudreault PO, Gagnon JF, Montplaisir J, et al. Abnormal occipital event-related potentials in Parkinson’s disease with concomitant REM sleep behavior disorder. Parkinsonism Relat Disord. 2013;19(2):212–217. doi:10.1016/j.parkreldis.2012.10.006
130. Iranzo A, Santamaría J, Rye DB, et al. Characteristics of idiopathic REM sleep behavior disorder and that associated with MSA and PD. Neurology. 2005;65(2):247–252. doi:10.1212/01.wnl.0000168864.97813.e0
131. Antelmi E, Pizza F, Donadio V, et al. Biomarkers for REM sleep behavior disorder in idiopathic and narcoleptic patients. Ann Clin Transl Neurol. 2019;6(9):1872–1876. doi:10.1002/acn3.50833
132. Berg D, Borghammer P, Fereshtehnejad SM, et al. Prodromal Parkinson disease subtypes - key to understanding heterogeneity. Nat Rev Neurol. 2021;17(6):349–361. doi:10.1038/s41582-021-00486-9
133. Gilat M, Marshall NS, Testelmans D, Buyse B, Lewis SJG. A critical review of the pharmacological treatment of REM sleep behavior disorder in adults: time for more and larger randomized placebo-controlled trials. J Neurol. 2022;269(1):125–148. doi:10.1007/s00415-020-10353-0
134. de Almeida CMO, Pachito DV, Sobreira-Neto MA, Tumas V, Eckeli AL. Pharmacological treatment for REM sleep behavior disorder in Parkinson disease and related conditions: a scoping review. J Neurol Sci. 2018;393:63–68. doi:10.1016/j.jns.2018.08.008
135. Li SX, Lam SP, Zhang J, et al. A prospective, naturalistic follow-up study of treatment outcomes with clonazepam in rapid eye movement sleep behavior disorder. Sleep Med. 2016;21:114–120. doi:10.1016/j.sleep.2015.12.020
136. Ferri R, Marelli S, Ferini-Strambi L, et al. An observational clinical and video-polysomnographic study of the effects of clonazepam in REM sleep behavior disorder. Sleep Med. 2013;14(1):24–29. doi:10.1016/j.sleep.2012.09.009
137. McCarter SJ, Boswell CL, St Louis EK, et al. Treatment outcomes in REM sleep behavior disorder. Sleep Med. 2013;14(3):237–242. doi:10.1016/j.sleep.2012.09.018
138. Kunz D, Bes F. Melatonin as a therapy in rem sleep behavior disorder patients: an open-labeled pilot study on the possible influence of melatonin on rem-sleep regulation. Mov Disorders. 1999;14(3):507–511. doi:10.1002/1531-8257(199905)14:3<507::
139. Boeve B. Melatonin for treatment of REM sleep behavior disorder in neurologic disorders: results in 14 patients. Sleep Med. 2003;4(4):281–284. doi:10.1016/S1389-9457(03)00072-8
140. Taximaimaiti R, Luo X, Wang XP. Pharmacological and Non-pharmacological Treatments of Sleep Disorders in Parkinson’s Disease. Curr Neuropharmacol. 2021;19(12):2233–2249. doi:10.2174/1570159X19666210517115706
141. Gilat M, Coeytaux jackson A, Marshall NS, et al. Melatonin for Rapid Eye Movement Sleep Behavior Disorder in Parkinson’s disease: a Randomised Controlled Trial. Mov Disorders. 2020;35(2):344–349. doi:10.1002/mds.27886
142. Kashihara K, Nomura T, Maeda T, et al. Beneficial Effects of Ramelteon on Rapid Eye Movement Sleep Behavior Disorder Associated with Parkinson’s Disease - Results of a Multicenter Open Trial. Intern Med. 2016;55(3):231–236. doi:10.2169/internalmedicine.55.5464
143. Nomura T, Kawase S, Watanabe Y, Nakashima K. Use of ramelteon for the treatment of secondary REM sleep behavior disorder. Intern Med. 2013;52(18):2123–2126. doi:10.2169/internalmedicine.52.9179
144. Dusek P, Busková J, Růzicka E, et al. Effects of ropinirole prolonged-release on sleep disturbances and daytime sleepiness in Parkinson disease. Clin Neuropharmacol. 2010;33(4):186–190. doi:10.1097/WNF.0b013e3181e71166
145. Wang Y, Yang Y, Wu H, Lan D, Chen Y, Zhao Z. Effects of Rotigotine on REM Sleep Behavior Disorder in Parkinson Disease. J Clin Sleep Med. 2016;12(10):1403–1409. doi:10.5664/jcsm.6200
146. Wilson SM, Wurst MG, Whatley MF, Daniels RN. Classics in Chemical Neuroscience: pramipexole. ACS Chem Neurosci. 2020;11(17):2506–2512. doi:10.1021/acschemneuro.0c00332
147. Schmidt MH, Koshal VB, Schmidt HS. Use of pramipexole in REM sleep behavior disorder: results from a case series. Sleep Med. 2006;7(5):418–423. doi:10.1016/j.sleep.2006.03.018
148. Kumru H, Iranzo A, Carrasco E, et al. Lack of effects of pramipexole on REM sleep behavior disorder in Parkinson disease. Sleep. 2008;31(10):1418–1421.
149. Trenkwalder C, Kies B, Rudzinska M, et al. Rotigotine effects on early morning motor function and sleep in Parkinson’s disease: a double-blind, randomized, placebo-controlled study (RECOVER). Mov Disord. 2011;26(1):90–99. doi:10.1002/mds.23441
150. Di Giacopo R, Fasano A, Quaranta D, Della marca G, Bove F, Bentivoglio AR. Rivastigmine as alternative treatment for refractory REM behavior disorder in Parkinson’s disease. Mov Disord. 2012;27(4):559–561. doi:10.1002/mds.24909
151. Brunetti V, Losurdo A, Testani E, et al. Rivastigmine for refractory REM behavior disorder in mild cognitive impairment. Curr Alzheimer Res. 2014;11(3):267–273. doi:10.2174/1567205011666140302195648
152. Ringman JM, Simmons JH. Treatment of REM sleep behavior disorder with donepezil: a report of three cases. Neurology. 2000;55(6):870–871. doi:10.1212/wnl.55.6.870
153. Larsson V, Aarsland D, Ballard C, Minthon L, Londos E. The effect of memantine on sleep behaviour in dementia with Lewy bodies and Parkinson’s disease dementia. Int J Geriatr Psychiatry. 2010;25(10):1030–1038. doi:10.1002/gps.2506
154. Chagas MHN, Eckeli AL, Zuardi AW, et al. Cannabidiol can improve complex sleep-related behaviours associated with rapid eye movement sleep behaviour disorder in Parkinson’s disease patients: a case series. J Clin Pharm Ther. 2014;39(5):564–566. doi:10.1111/jcpt.12179
155. Anderson KN, Shneerson JM. Drug treatment of REM sleep behavior disorder: the use of drug therapies other than clonazepam. J Clin Sleep Med. 2009;5(3):235–239.
156. Bamford CR. Carbamazepine in REM sleep behavior disorder. Sleep. 1993;16(1):33–34.
157. Abenza Abildúa MJ, Miralles Martinez A, Arpa Gutiérrez FJ, et al. Conditions associated with REM sleep behaviour disorder: description of a hospital series. Neurologia. 2019;34(3):159–164. doi:10.1016/j.nrl.2016.11.011
158. Keir LHM, Breen DP. New awakenings: current understanding of sleep dysfunction and its treatment in Parkinson’s disease. J Neurol. 2020;267(1):288–294. doi:10.1007/s00415-019-09651-z
159. Meloni M, Figorilli M, Carta M, et al. Preliminary finding of a randomized, double-blind, placebo-controlled, crossover study to evaluate the safety and efficacy of 5-hydroxytryptophan on REM sleep behavior disorder in Parkinson’s disease. Sleep Breath. 2022;26(3):1023–1031. doi:10.1007/s11325-021-02417-w
160. Shinno H, Kamei M, Nakamura Y, Inami Y, Horiguchi J. Successful treatment with Yi-Gan San for rapid eye movement sleep behavior disorder. Prog Neuropsychopharmacol Biol Psychiatry. 2008;32(7):1749–1751. doi:10.1016/j.pnpbp.2008.06.015
161. Kunz D, Stotz S, Bes F. Treatment of isolated REM sleep behavior disorder using melatonin as a chronobiotic. J Pineal Res. 2021;71(2):e12759. doi:10.1111/jpi.12759
162. Cammisuli DM, Ceravolo R, Bonuccelli U. Non-pharmacological interventions for Parkinson’s disease mild cognitive impairment: future directions for research. Neural Regen Res. 2020;15(9):1650–1651. doi:10.4103/1673-5374.276329
163. Cristini J, Weiss M, De Las Heras B, et al. The effects of exercise on sleep quality in persons with Parkinson’s disease: a systematic review with meta-analysis. Sleep Med Rev. 2021;55:101384. doi:10.1016/j.smrv.2020.101384
164. McCarter SJ, Boeve BF, Graff-Radford NR, Silber MH, St Louis EK. Neuroprotection in idiopathic REM sleep behavior disorder: a role for exercise? Sleep. 2019;42(6):zsz064. doi:10.1093/sleep/zsz064
165. Hughes KC, Gao X, Molsberry S, Valeri L, Schwarzschild MA, Ascherio A. Physical activity and prodromal features of Parkinson disease. Neurology. 2019;93(23):e2157–e2169. doi:10.1212/WNL.0000000000008567
166. Frazzitta G, Maestri R, Ferrazzoli D, et al. Multidisciplinary intensive rehabilitation treatment improves sleep quality in Parkinson’s disease. J Clin Mov Disord. 2015;2:11. doi:10.1186/s40734-015-0020-9
167. Memon AA, Coleman JJ, Amara AW. Effects of exercise on sleep in neurodegenerative disease. Neurobiol Dis. 2020;140:104859. doi:10.1016/j.nbd.2020.104859
168. Howell MJ, Arneson PA, Schenck CH. A novel therapy for REM sleep behavior disorder (RBD). J Clin Sleep Med. 2011;7(6):639–644A. doi:10.5664/jcsm.1470
169. Zuzuárregui JRP, During EH. Sleep Issues in Parkinson’s Disease and Their Management. Neurotherapeutics. 2020;17(4):1480–1494. doi:10.1007/s13311-020-00938-y
170. Pereira EA, Muthusamy KA, De Pennington N, Joint CA, Aziz TZ. Deep brain stimulation of the pedunculopontine nucleus in Parkinson’s disease. Preliminary experience at Oxford. Br J Neurosurg. 2008;22:S41–44. doi:10.1080/02688690802448335
171. Stefani A, Lozano AM, Peppe A, et al. Bilateral deep brain stimulation of the pedunculopontine and subthalamic nuclei in severe Parkinson’s disease. Brain. 2007;130(Pt 6):1596–1607. doi:10.1093/brain/awl346
172. Chambers NE, Lanza K, Bishop C. Pedunculopontine Nucleus Degeneration Contributes to Both Motor and Non-Motor Symptoms of Parkinson’s Disease. Front Pharmacol. 2019;10:1494. doi:10.3389/fphar.2019.01494
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.