Back to Journals » Risk Management and Healthcare Policy » Volume 19
Consent Related Delay in Emergency Obstetric Care as a Sentinel Patient Safety Event: A Risk Governance Commentary from Somalia
Authors Salad YM ![]() , Mudei NM
, Mudei NM ![]() , Omar AA
, Omar AA ![]()
Received 1 March 2026
Accepted for publication 28 May 2026
Published 3 June 2026 Volume 2026:19 606125
DOI https://doi.org/10.2147/RMHP.S606125
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Keon-Hyung Lee
Yusuf Mohamed Salad,1 Nasteho Mohamud Mudei,2 Abdullahi Abdirahman Omar3
1Department of Nursing, Dr. Sumait Hospital, SIMAD University, Mogadishu, Somalia; 2Department of Obstetrics and Gynecology, Dr. Sumait Hospital, SIMAD University, Mogadishu, Somalia; 3Department of Research, Dr. Sumait Hospital, SIMAD University, Mogadishu, Somalia
Correspondence: Yusuf Mohamed Salad, Department of Nursing, Dr. Sumait Hospital, SIMAD University, Mogadishu, Somalia, Email [email protected]; [email protected]
Abstract: This evidence informed commentary addresses consent related delay in emergency obstetric care in Somalia, where clinician recommended escalation may be delayed by family mediated refusal, indecision, or uncertainty about emergency authority. The purpose is to strengthen the conceptual grounding and practical implementation of a risk governance response to this under recognized patient safety problem. The commentary draws on established patient safety concepts, maternal delay models, World Health Organization quality of care and near miss approaches, published evidence from Somali settings, and the Somali regulation on patient rights and responsibilities of healthcare workers. We propose an operational definition of consent related delay as a sentinel patient safety event when it contributes to serious maternal harm or creates substantial risk of such harm. The framework emphasizes timely recognition of contested consent, structured escalation, clear documentation, lawful emergency action, integration into maternal near miss and mortality review, and routine monitoring. This framing may support hospital managers, clinicians, and policymakers to convert a recurring source of avoidable delay into an auditable governance process while preserving respectful patient and family engagement.
Keywords: emergency consent, maternal health, clinical governance, obstetric delay, patient safety, low resource settings
Introduction
Emergency obstetric care is highly time sensitive. Delays occurring after a woman reaches a facility can be as dangerous as delays in deciding to seek care or reaching care, because the outcome of an obstetric emergency often depends on the interval between recognition of a complication and delivery of definitive treatment.1,2 The classic three delays model remains useful for understanding maternal mortality, but consent related obstruction after facility arrival should also be interpreted as a patient safety and clinical governance problem that requires a facility response.1,2
Established patient safety frameworks provide a rationale for this interpretation. The WHO Global Patient Safety Action Plan emphasizes policy action, safer systems, learning, and implementation at the point of care to reduce avoidable harm.3 The Institute of Medicine and Reason’s systems approach similarly encourages movement away from individual blame toward the identification of weak defenses, latent conditions, and preventable hazards in care delivery.4,5
Published evidence from Somali settings suggests that consent related delay is clinically and operationally relevant. A mixed methods study from Somaliland found that maternal near miss and death after emergency cesarean delivery were linked to the prerequisite for family consent, with healthcare providers sometimes prevented from proceeding until the family provided permission.6 A cohort study in Somaliland found that emergency cesarean section delayed by more than three hours was associated with higher odds of severe maternal outcomes.7 A recent study on family consent for cesarean section also showed that poor communication, delayed informed choice, disagreement between family members, and absence of the formal decision maker may delay consent.8
Somalia specific publications further strengthen the need for a governance response. A legal commentary argued for women’s surgical self consent and emergency presumed consent when delay threatens life.9 A qualitative study of doctors in Somalia reported that consent for life saving obstetric interventions may be controlled by paternal male relatives, that refusal or delay may occur for social and misconception related reasons, and that clinicians may fear consequences when acting without family approval.10 These sources should not be interpreted as proving that all families or communities behave similarly; rather, they indicate a recurring clinical governance risk that requires respectful, context informed management.
The Somali regulatory context also supports a more structured approach. The 2023 Regulation on the Rights of Patients and Responsibilities of Healthcare Workers defines consent, requires patient information in understandable language, recognizes emergency care obligations, describes substitute consent pathways when a patient lacks capacity, addresses responsibility for harmful delay, and establishes requirements related to patient records and confidentiality.11
The contribution of this commentary is to strengthen the conceptual and operational basis for reframing consent related delay as a sentinel patient safety event. Unlike prior discussions that primarily emphasize legal reform or moral autonomy, this article translates the problem into an implementation oriented governance framework for hospitals and health authorities. The framework is grounded in patient safety theory, WHO quality and near miss approaches, Somalia related evidence, and Somali patient rights regulation.2,3,6,8–12
Approach to Commentary and Framework Development
This article is a policy and patient safety commentary rather than an original empirical study. It does not report primary data, statistical analysis, recruitment, sample size, or new outcomes. The proposed framework was developed through narrative synthesis of relevant literature and policy documents, including the three delays model, WHO standards for maternal and newborn quality of care, the WHO Global Patient Safety Action Plan, the WHO near miss approach, the sentinel event concept, systems based patient safety literature, published Somalia related evidence on consent and obstetric emergencies, and the Somali patient rights and healthcare worker responsibilities regulation.1–12
The framework components were selected for practical relevance to facility level governance. Each component responds to an operational gap identified across the literature and regulatory context: unclear emergency authority, absence of a time recorded escalation process, inconsistent documentation, limited integration of consent delay into maternal near miss and mortality review, and weak routine measurement. The framework is therefore best understood as a conceptual and implementation oriented model that requires local adaptation and empirical evaluation before claims about outcome reduction can be made.
Conceptual Grounding in Patient Safety Frameworks
Patient safety frameworks emphasize that serious harm often results from system conditions rather than a single individual error. Reason described how latent conditions and weakened defenses can align to permit harm, while the broader patient safety movement emphasizes learning systems and prevention rather than blame.4,5 Consent related delay fits this logic. It may arise from family pressure, legal uncertainty, fear of retaliation, inadequate institutional policy, poor documentation, and lack of leadership support. These interacting conditions can weaken the defenses that should protect patients during time critical emergencies.
The WHO Global Patient Safety Action Plan calls for reducing avoidable harm through policy action, safer systems, and point of care implementation.3 WHO maternal and newborn quality standards emphasize timely, evidence based management of complications, effective communication, actionable information systems, and functioning governance structures.2 The WHO near miss approach supports systematic review of severe maternal outcomes and monitoring of critical interventions as a quality improvement process.12 Together, these frameworks justify treating contested emergency consent as a measurable safety risk rather than an informal interpersonal dispute.
The sentinel event concept is useful because it creates an organizational trigger for investigation and learning.13 In this commentary, a consent related sentinel patient safety event is operationally defined as a time critical obstetric situation in which a qualified clinician recommends urgent intervention, consent becomes contested or delayed, and the delay contributes to serious maternal harm or creates substantial risk of serious harm. This definition does not remove the importance of autonomy, culturally respectful communication, or legal safeguards. It clarifies that avoidable delay itself must be visible, documented, reviewed, and prevented.
Somali Legal and Policy Context
The Somali regulation provides several elements that can support facility level action. Article 3 states that health workers and health facilities cannot refuse emergency assistance and treatment to a patient needing urgent care without valid reason.11 Article 4 requires providers to inform patients about their condition, available investigations and treatments, benefits, risks, costs, consequences, and the right to refuse care in a language the patient understands.11 These provisions support early counseling, disclosure of risk, and respectful communication before refusal is documented.
Article 5 addresses consent and provider responsibility, including substitute consent when the patient lacks capacity and responsibility for delay that may cause death or irreversible injury.11 Article 7 describes procedures for health services provided without consent under applicable law, including written notification to district administration and police within specified circumstances.11 Articles 12 to 16 address record keeping, confidentiality, and access to patient records, which are important safeguards for any emergency consent pathway.11
These provisions should not be read as a simple permission to ignore consent. Rather, they support a more careful governance position. Facilities should develop internal policies that protect patient participation whenever possible, define substitute consent pathways when the patient lacks capacity, document the risk of delay, and specify when emergency action and notification procedures are required under applicable law. Such policies should be reviewed by local legal, clinical, ethics, and health authority stakeholders before implementation.
A Risk Governance Framework for Emergency Obstetric Consent Delay
The proposed framework has four linked functions: prevention, escalation, documentation, and learning. Prevention begins before crisis through antenatal counseling, community engagement, and communication about the risks of delaying emergency obstetric care. Escalation begins once a qualified clinician documents an emergency indication and the expected harm of delay. Documentation records patient capacity, patient preference or assent where possible, substitute consent, refusal, time points, second opinion, leadership involvement, and the final decision. Learning occurs when consent delay is included in maternal near miss and mortality review, with action plans monitored through quality improvement mechanisms.2,11,12
Table 1 summarizes the implementation package, including governance controls, operational steps, legal and policy alignment, and indicators that can be adapted for routine facility quality improvement.
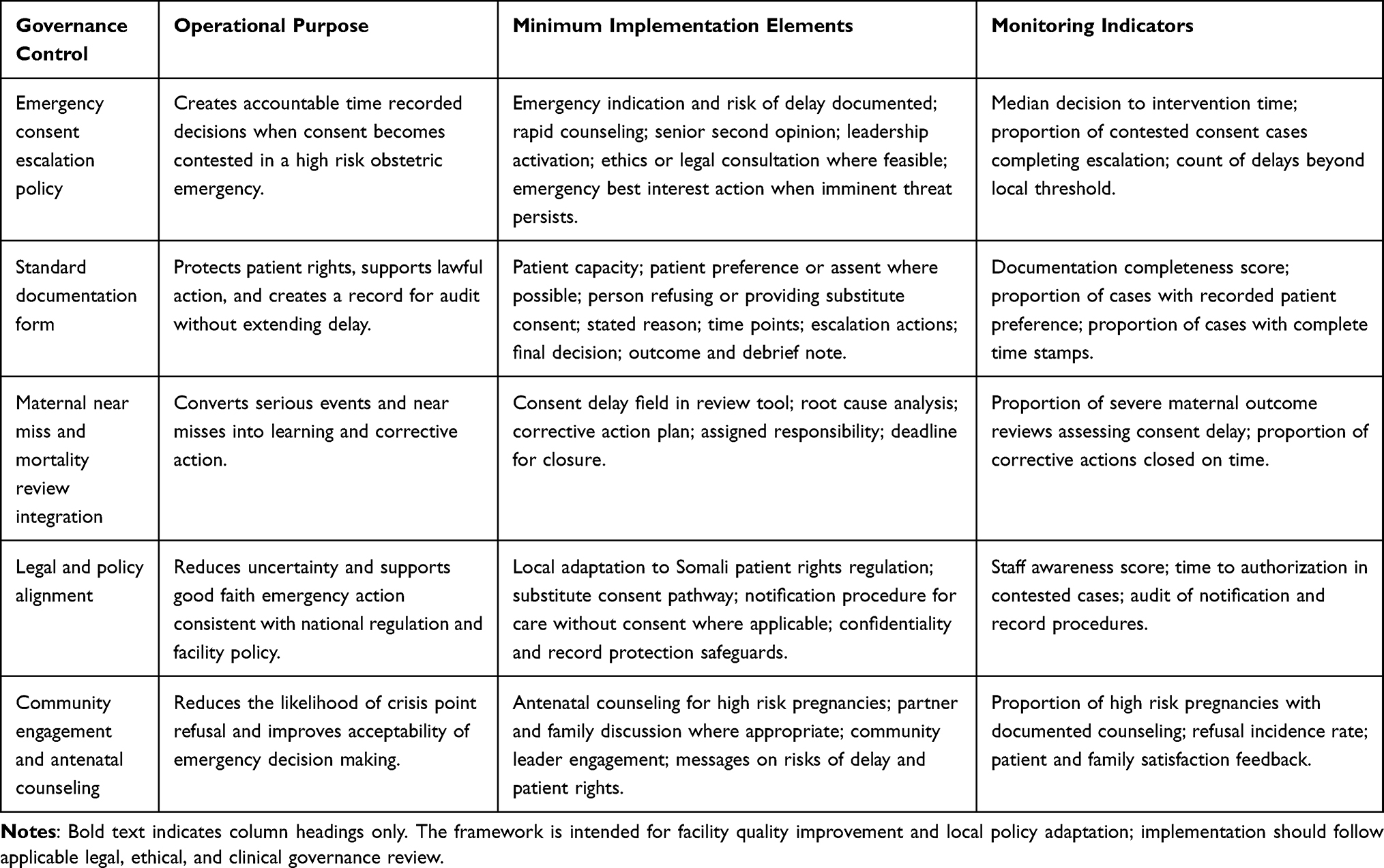 |
Table 1 Risk Governance Package for Preventing Consent Related Delays in Emergency Obstetric Care |
As shown in Figure 1, the escalation policy should define time recorded steps from clinical decision and rapid counseling to senior second opinion, leadership activation, ethics or legal consultation where feasible, and emergency best interest action when imminent threat persists. This pathway converts family mediated refusal or indecision into an accountable process that prioritizes safety while preserving respectful communication.
 |
Figure 1 Emergency consent delay escalation pathway and intervention points. The figure presents a conceptual escalation pathway with time recorded decision points from clinical decision and rapid counseling to senior second opinion, leadership activation, ethics or legal consultation where feasible, and emergency best interest action when imminent threat persists. |
The framework should be interpreted cautiously. It is not a substitute for national law, professional regulation, or hospital legal advice. It is a structured patient safety model that can help facilities align clinical urgency, patient rights, provider protection, and organizational accountability. Its effectiveness should be evaluated through implementation research, including measurement of decision to intervention intervals, completeness of documentation, staff understanding, patient and family acceptability, and severe maternal outcomes.2,3,12
Implementation Implications for Hospitals and Policymakers
For hospital managers, the practical implication is that emergency consent delay should be made visible in routine governance processes. A facility policy can define who initiates escalation, who provides a rapid second opinion, which administrator or medical leader is contacted, how ethics or legal advice is accessed when feasible, and what minimum documentation is required. The policy should also clarify that documentation must not become a new source of delay.
For clinicians, the framework supports earlier communication and safer escalation. The first communication should explain the emergency indication, expected harm of delay, available options, and likely consequences in language the patient and family can understand. When refusal or indecision persists, escalation should be framed as a safety process rather than an adversarial response. This may reduce hesitation and protect both the patient and the clinical team.
For policymakers and regulators, the framework identifies areas where national guidance may be useful. These include clarification of emergency authority, alignment of substitute consent rules with patient rights, standardized documentation requirements, and incorporation of consent related delay into maternal death surveillance, maternal near miss review, and quality improvement indicators. Such policy development should be culturally sensitive, legally reviewed, and informed by women, families, clinicians, hospital leaders, legal experts, and community representatives.
Limitations and Future Research
This commentary has limitations. It does not report primary data and cannot prove that the proposed framework reduces maternal morbidity or mortality. The framework is conceptually derived from patient safety literature, WHO guidance, Somalia related evidence, and national regulation, but it requires local validation. It should therefore be understood as a context informed proposal rather than a tested intervention.
Future research should assess acceptability, feasibility, legal interpretation, implementation fidelity, and unintended consequences in maternity units across public and private facilities. Studies could examine whether structured escalation improves documentation completeness, reduces decision to intervention intervals, improves staff confidence, and is acceptable to women and families. Qualitative research should also explore how emergency authority can be clarified without undermining respectful maternity care or community trust.
Conclusion
Consent related delay in emergency obstetric care can become a preventable pathway to severe maternal harm when clinical urgency is recognized but action is blocked by contested authority, fear, or weak institutional processes. Reframing this problem as a sentinel patient safety event strengthens the case for governance, documentation, review, and learning rather than blame. A Somalia adapted framework based on prevention, escalation, documentation, lawful emergency action, and maternal near miss review may help facilities respond more consistently while maintaining respect for patients, families, and healthcare workers.
Abbreviation
WHO, World Health Organization.
Ethics Approval and Informed Consent
This commentary does not report new research involving human participants or identifiable personal data. Formal ethics committee approval and informed consent were not required.
Acknowledgments
This research was supported by SIMAD University, Somalia.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Thaddeus S, Maine D. Too far to walk: maternal mortality in context. Soc Sci Med. 1994;38(8):1091–6. doi:10.1016/0277-9536(94)90226-7
2. World Health Organization. Standards for improving quality of maternal and newborn care in health facilities. World Health Organization; 2016. Available from: https://www.who.int/publications/i/item/9789241511216.
3. World Health Organization. Global patient safety action plan 2021-2030: towards eliminating avoidable harm in health care. World Health Organization; 2021. Available from: https://www.who.int/teams/integrated-health-services/patient-safety/policy/global-patient-safety-action-plan.
4. Institute of Medicine. To Err Is Human: Building a Safer Health System. National Academies Press; 2000.
5. Reason J. Human error: models and management. BMJ. 2000;320(7237):768–770. doi:10.1136/bmj.320.7237.768
6. Abdillahi HA, Hassan KA, Kiruja J, et al. A mixed-methods study of maternal near miss and death after emergency cesarean delivery at a referral hospital in Somaliland. Int J Gynecol Obstet. 2017;138(1):119–124. doi:10.1002/ijgo.12176
7. Kiruja J, Osman F, Egal JA, Erlandsson K, Klingberg-Allvin M. Association between delayed cesarean section and severe maternal and adverse newborn outcomes in the Somaliland context: a cohort study in a national referral hospital. Global Health Action. 2023;16(1):2207862. doi:10.1080/16549716.2023.2207862
8. Kiruja J, Osman F, Litorp H, Egal JA, Esse A, Klingberg-Allvin M. Barriers to and facilitators of timely family consent in caesarean sections: experiences, perspectives and associated factors: a mixed-methods study in Somaliland. PLoS One. 2026;21(3):e0342475. doi:10.1371/journal.pone.0342475
9. Ali RM. Women’s right to surgical self-consent: a legal and moral imperative for Somalia. Int J Women’s Health. 2025;17:1–6. doi:10.2147/IJWH.S563497
10. Aweis AA, Mauma M, Aweis A, Afrah A, Guled IA, Kulane A. Doctors’ experiences on dealing with informed consent required for lifesaving interventions for pregnant women in Somalia. Front Global Women’s Health. 2025;6:1584113. doi:10.3389/fgwh.2025.1584113
11. Jamhuuriyadda Federaalka Soomaaliya, Wasaaradda Caafimaadka iyo Daryeelka Bulshada. Xeer-Nidaamiyaha Xuquuqda Bukaanka iyo Waajibaadka Shaqaalaha Caafimaadka. Ministry of Health and Human Services; 2023.
12. World Health Organization. Evaluating the quality of care for severe pregnancy complications: the WHO near-miss approach for maternal health. World Health Organization; 2011. Available from: https://www.who.int/publications/i/item/9789241502221.
13. The Joint Commission. Sentinel event policy and procedures; 2026. Available from: https://www.jointcommission.org/en-us/knowledge-library/support-center/standards-interpretation/sentinel-event-policy-and-procedures/.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Audit of Documentation of Chest Drain Insertion Procedures Before and After Introduction of a Chest Drain Pro forma
Ahmed M, Malik S, Ng AYK, Tariq SM
Clinical Audit 2023, 15:1-5
Published Date: 21 April 2023
The State of Anesthesia and Critical Care Services in Somalia: Challenges and Opportunities
Mohamed IA, Garba B
Risk Management and Healthcare Policy 2026, 19:593539
Published Date: 15 April 2026
Closing the Referral Gap During Prolonged Labour in Somalia: From Traditional Birth Attendance to Emergency Obstetric Care
Sheik Yusuf LK
International Journal of Women's Health 2026, 18:596934
Published Date: 23 April 2026
Obstetric and Emergency Anesthesia in Somalia: Patient Safety Challenges in a Fragile Health System
Mohamed IA
International Journal of Women's Health 2026, 18:593204
Published Date: 8 May 2026