Back to Journals » Patient Preference and Adherence » Volume 16
Consensus on the Objectives of an Educational Intervention for Patients with Oropharyngeal Dysphagia and Their Informal Caregivers: A Delphi Study
Authors Ghaddar Z ![]() , Matar N, Noujaim J, Diep AN, Tohmé A, Pétré B
, Matar N, Noujaim J, Diep AN, Tohmé A, Pétré B
Received 1 March 2022
Accepted for publication 27 May 2022
Published 23 June 2022 Volume 2022:16 Pages 1511—1524
DOI https://doi.org/10.2147/PPA.S364520
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Zahya Ghaddar,1– 3 Nayla Matar,3,4 Joyce Noujaim,3 Anh Nguyet Diep,1 Aline Tohmé,5 Benoit Pétré1
1Department of Public Health, University of Liège, Liege, Belgium; 2Doctoral School of Sciences and Health, Faculty of Medicine, Saint Joseph University of Beirut, Beirut, Lebanon; 3Department of Higher Institute of Speech and Language Therapy, Saint Joseph University of Beirut, Beirut, Lebanon; 4Department of Otolaryngology-Head and Neck Surgery, University Hospital Center Hotel-Dieu de France, Affiliated to Saint-Joseph University, Beirut, Lebanon; 5Department of Internal Medicine and Clinical Immunology, University Hospital Center Hotel-Dieu de France, Affiliated to Saint-Joseph University, Beirut, Lebanon
Correspondence: Zahya Ghaddar, Department of Public Health, University of Liège, Place du XX août 7, Liege, 4000, Belgium, Tel +961 3554813, Email [email protected]; [email protected]
Purpose: In the absence of literature allowing for an evidence-based approach to therapeutic patient education (TPE) in Oropharyngeal Dysphagia (OD), this study aims to reach a consensus of experts on the content of a competency framework of an educational program for OD patients and their informal caregivers (ICGs).
Methods: We used the Delphi consensus-building method. Four categories of experts were recruited: 12 patients, 17 ICGs, 46 healthcare professionals (HCP) (experienced in OD, not necessarily certified in TPE), and 19 experts in TPE (trained individuals to set up and run TPE programs not necessarily HCPs). The content of the questionnaire of the first round (R) was established according to the result of a scoping review and the opinion of an expert committee. We carried out three rounds. In R1 and R2, we collected the opinions on the relevance (7-point Likert-type scale) and on comprehensiveness (YES/No question and asking participants to propose additional content). Participants were also invited to leave comments on each objective. In R3, we asked the participants to give their opinion about the relevance of the objectives again and asked them to rank the themes from highest to lowest priority.
Results: Objectives were considered relevant for all participants if they reached consensus when the interquartile (IQR) ≤ 1, and if the median indicated agreement (Mdn ≥ 6) (6= appropriate, 7 = totally appropriate). Following three rounds, the final content of the educational program is composed of 23 educational objectives organized in 13 themes with an agreement about relevance amongst all participants (Mdn ≥ 6; IQR ≤ 1). The comprehensiveness criterion received also a consensus (IQR ≤ 1). The participants ranked the theme “normal swallowing vs difficulty swallowing” as the highest priority.
Conclusion: This Delphi study resulted in a consensus, on the content of a competency framework of an educational program for OD patients and their ICGs. Further steps are needed to construct learning activities based on these objectives before testing their feasibility and efficacy.
Keywords: deglutition disorders, Delphi method, educational program, swallowing disorders, patient and family education, recommendations
Introduction
Oropharyngeal Dysphagia (OD) is defined as a difficulty forming or moving the food bolus safely and/or efficiently from the oral cavity to the esophagus.1 Multiple etiologies can disrupt swallowing and have significant life-threatening implications.
The international and scientific societies recommend medically and socially supporting patients with dysphagia and their caregivers through a multidisciplinary team composed of physicians, therapists, dieticians, nurses, and caregivers.2–4 Within this support, Therapeutic Patient Education (TPE) appears as a central component. It is recognized as an approach that focuses to help patients and their caregivers acquire and maintain skills needed to manage the disorder and lead a dignified life.5 TPE is known as an effective way to enable patients with chronic conditions such as diabetes, asthma, and obesity to live better with their disease, adhere more to recommendations, and improve or maintain their quality of life.
The recognized effectiveness of TPE has led various scientific societies to propose TPE guidelines for specific diseases focusing on the competency framework pursued by the patient and their informal caregivers in diabetes,6 diabetes and obesity,7 and in psoriasis8 amongst others. However, such work has not been done in the field of OD. As mentioned by Daviet et al, there are a limited number of articles that have targeted TPE for OD patients, especially those with stroke.9 Another reason for this absence is that most of the studies targeted specific aims related to OD. There’s a lack of published studies of a transversal and fundamental TPE program specifically addressed to dysphagia adult patients and their informal caregivers. For example, Krajczy et al conducted in this population aimed to evaluate the effects of education on dysphagia patients in the early post-stroke period, it targeted only the education about safe food and liquid intake provided as an addition to classical rehabilitation which is a part of the compensatory strategies in OD management.10 Govender et al pointed only the education about the normal and abnormal mechanisms of swallowing.11 Furthermore, McKinstry et al targeted various educational objectives as the normal mechanism of swallowing, knowing the signs and symptoms of aspiration as well as the complications of aspiration and the importance of the application of specific rehabilitation exercises and compensatory strategies without taking into consideration the psychosocial skills.12 Wasserman et al aimed the education related only to the nutritional aspects and possible alternative feeding methods as well as the postoperative swallow safety.13 Although dysphagia appears in diversified contexts, hence, the establishment of a base of fundamental and transversal competencies for patients with OD and their informal caregivers seems essential to us to guide the development of relevant educational interventions for these patients.
However, the lack of evidence on what patients and their caregivers should be trained on led us to move towards consensus methods that seek to reach a consensus of the content of a competency framework.
There are published studies in other medical fields that have used the Delphi method to reach a consensus by questioning experts in a perspective of pedagogical development. This is exemplified in the results of a Delphi study conducted in France that showed agreement among experts around the decision-making skills that patients with cardiovascular disease and their families should acquire to manage heart attacks and the complex situations they might face.14 Globally, the Delphi method has been widely and successfully used for years to gather expert opinions on various topics and reach agreement or disagreement.15 It can be carried out anonymously via email, eliminating the bias that occurs in face-to-face meetings as in nominal group processes (expert panel method) or consensus development panels (consensus development conferences). Participants in a Delphi method can express their opinions freely without the fear of being reproached or losing their credibility, or being forced to have the majority opinion. In addition, the participants can avoid a compromised decision while answering multiple rounds because answering multiple rounds ensure thoughtful consideration by the entire response group which is more reliable than a single meeting. Furthermore, the multidisciplinary nature of the Delphi experts gives the chance to receive different perspectives and inputs.16 Lastly, a Delphi method does not require a specified meeting time therefore the participants can answer the different questionnaires when they are available17 and it can be carried out remotely by electronic exchange authorizing consultation of geographically dispersed experts.18,19
Therefore, this study aims to reach a consensus of experts on the content of a competency framework of a universal and transversal educational program for adult patients with OD and their informal caregivers.
Materials and Methods
Method
In this study, three rounds were planned to ensure the process did not become too repetitive20 since three rounds are sufficient to collect the needed information to reach a consensus21 and provide the participants the opportunity to reflect on their responses to statements in the previous rounds.22 Between the rounds, we provided controlled feedback to the participants and informed them of the opinions of their anonymous peers. We presented feedback as a simple statistical summary of the group response.23
The data collection period of this study was from November 2020 till March 2021.
Ethical Considerations
The study received the approval of the Research Ethics Committee (REC) of Saint Joseph University, Beirut, Lebanon, in June 2019, “CE-HDF: 1439”. The study was carried out in accordance with the principles of the Declaration of Helsinki.
We prepared a written informed consent form to obtain written consent online via a link on “Google Forms” and a formal letter of information to the experts together with an explanation letter concerning the information relating to the processing of personal data, following the General Data Protection Regulation (GDPR-EU 2016/679) and the Law of 30 July 2018 on the protection of individuals about the processing of personal data, that we sent alongside with the invitation letter for participation in the study. Therefore, when all participants provided written informed consent prior to participating in the Delphi study, they were provided with the link to the round one questionnaire.
Participants
According to the literature, participants in a Delphi study are considered eligible to be invited to participate if they have related backgrounds and experiences concerning the target issue.21 We considered the patients and their informal caregivers at an equal footing from the HCPs and the experts in TPE knowing their day-to-day challenges with OD. We reached out to four categories of participants: patients with OD and informal caregivers (known as family members, relatives, friends, and neighbors, with no training and providing care for free),24 to have feedback about the content of an educational program relying on their personal experience with OD to help us tailor the content to their day-to-day needs; healthcare professionals (HCPs) with experience with OD to benefit from their clinical expertise with OD patients and expert in TPE to cover properly the fundamentals of a TPE.
The inclusion and exclusion criteria of each category of participants are mentioned below:
- Patients: currently or formerly with OD, 18 years old or older, literate, without a cognitive impairment;
- Informal caregivers: currently or formerly taking care of patients with OD, 18 years old or older, literate;
- HCPs: neurologists, pulmonologists, gastroenterologists, ear, nose, and throat (ENT) specialists, geriatricians, internal medicine physicians, nurses, formal caregivers (formal caregivers are known as paid caregivers with training in the field but the depth of their training varies),24 speech-swallowing therapists, physical therapists, occupational therapists, nutritionists, psychotherapists …, with experience in OD in different settings;
- Experts in TPE: trained individuals to set up and run TPE programs.
Recruitment of Delphi Participants
Knowing there is little agreement on the size of expert panels,18,21 the panel of this Delphi study aimed to recruit a high number of participants to anticipate attrition. As recommended in the literature, we aimed to comprise at least 10 participants in each subcategory of experts at the end of the process.21
The recruitment of participants was made based on the network of HCPs and personal recommendations (snowball system) and through social media like LinkedIn, Facebook, and WhatsApp. An invitation letter, including information about the study, information relating to the processing of personal data (General Data Protection Regulation-GDPR), and a consent form were sent via email and phone message to 185 potential participants in September 2020 in French, English, or Arabic depending on the anticipated preferred language.
To confirm their consent, we asked the participants to sign the consent form and provide us with demographic characteristics: age, gender, the highest level of degree, professional activity, residency country. In addition, some specific information was stated for each subgroup of participants:
- For the patients: origin, date of onset and current status of the OD;
- For the informal caregivers: relationship status to the patient, specifying if they received a medical degree or special training, and years of experience in OD;
- For the HCP: workplace, training in TPE, participation in TPE activities, and years of experience in OD;
- For experts in TPE: workplace, TPE interest in which disorder/disease, years of experience in OD.
We also asked participants to specify their language preference between French, Arabic, or English to fill the questionnaire. After obtaining the participants’ consent, we sent a link to the Round 1 questionnaire, in November 2020.
Preparation of Delphi Rounds and Construction of Data Collection Tool
The first development of the content of the TPE objectives was based on a preliminary exploratory approach combining a scoping review and the opinion of an expert committee. Our scoping review summarized the modalities, the content of educational interventions for adult patients with OD,25 and their informal caregivers. We formed an expert committee of seven speech-swallowing therapists and one ICG to verify the content of the program. We conducted a telephone interview and asked the expert committee the same question: “What are the essential needs to be addressed in therapeutic education for patients with OD and their informal caregivers?”.
Therefore, this preliminary work resulted in an initial list of 21 objectives organized into 12 themes.
We built the electronic Delphi survey in three languages, using Limesurvey,26 an open source online survey application. For each round, we specified to the participants that they have 2 weeks to answer.
Before launching the first round of the Delphi study, we pilot tested the French version on two speech-swallowing therapists, the English version on a colleague expert in research methodology, and the Arabic version on two Lebanese patients with OD. Relying on the feedback of the participants to the pilot study, we added examples and/or explications for the different educational objectives to facilitate the intelligibility of the questionnaire and we added the “not concerned” option for each educational objective.
We created the main questionnaires and different study documents in French. Therefore, a group of HCPs verified the translation of the whole documents and a sworn translator ensured that the content of the invitation letter, consent form, information letter, the explanation letter concerning the Information relating to the processing of personal data, the General Data Protection Regulation (GDPR) were translated accurately to Arabic and English. This procedure was repeated for each of the three consecutive rounds.
Delphi Round One
For the first round, we collected the relevance and the comprehensiveness of the objectives chosen for the educational program. Relevance means that the chosen item addresses the need of patients or their informal caregivers to cope with the disorder in their daily life and help them maintain their quality of life. Comprehensiveness means that the proposed items are complete and cover the needs of the patients or their informal caregivers. For each objective, we asked the participant to determine relevance by expressing their opinion on a 7-point Likert scale (1: totally unsuitable, 2: unsuitable, 3: slightly unsuitable, 4: indecisive, 5: slightly suitable, 6: suitable, 7: totally suitable, and not concerned). We also asked the participants to comment on their answers, especially when they believed that the objective is unsuitable, unclear, or incomplete. Lastly, we asked participants to answer a YES/NO question about the comprehensiveness of the entire objectives, “Are the proposed objectives for the educational program for dysphagia patients and their caregiver complete? If not, please specify what may be the objectives of other educational activities”. We also included an explanation of the Delphi procedure with examples and instructions on how to complete the questionnaire.
The questionnaire of round one comprised 12 themes inclusive of 21 educational objectives. We distributed the link to the questionnaire via emails or via the WhatsApp application. The duration of the questionnaire of round one was around 12 minutes. Despite that participants were given two weeks for each Delphi round,21 due to the Covid19 pandemic, we extended the first round to one month. After the initial two weeks, we sent three reminders by emails and/or messages.
After receiving the answers, we gave each participant a name code [Abbreviation of each type of experts; the first letter of the name, first two letters of the family name] to allow the tracking of returned responses, to track the individual’s feedback, and to facilitate the data analysis afterward.
Delphi Round Two
For the second round, we first presented the results of the first round at the beginning of the questionnaire. Then, we followed the same steps as in round one so the participants can confirm or modify their answers. Thus, we collected also the relevance and the comprehensiveness of the chosen objectives for the educational program using the same evaluation parameters. We relied on the statistical calculations and the comments of the first round to obtain the second round. We reworded some items, clarified others with examples and/or explanations, we added a few objectives according to the participant’s comments. We sent the link for the questionnaire of round two by email and/or by message. The duration of the questionnaire was around 12 minutes.
Delphi Round Three
As for the third round, we divided it into two parts. In the first part, we asked the participants about the relevance of the objectives by also giving their opinion on a 7-point Likert-type scale as in the previous rounds. We omitted the Round 2 items that received stable responses and agreement among the participants from the Round 3 questionnaire to reduce its length. We asked the participants to judge the relevance of the items. We did not make any changes (rewording or adding examples) between round two and round three to ensure the stability of the responses to the remaining items. We specified that the “not concerned” answer is to be used only by patients, and informal caregivers to have complete feedback from HCPs and experts in TPE.
In this round, we added a second new part “ranking of themes for the educational program”. We asked participants to rank the proposed themes [from highest to lowest priority]. This prioritization aimed to establish a ranking for implementing an educational program for dysphagia patients and their informal caregivers. This information will be used to select the priority themes organized as educational activities. This prioritization took into account the perception of the patient’s needs and their experience as potential beneficiaries of the activities (patients – informal caregivers) or as observers of the priority educational needs to be covered (TPE experts and HCPs). We asked the participants to rank the themes from 1 to 13 (1 being the highest priority and 13 being the lowest priority). But before the ranking, we asked all participants to answer two closed-ended questions: “Have you ever had/been faced with a tracheostomy? Have you ever needed/been faced with enteral feeding?”. Depending on each participant’s answers to these questions, we included or excluded topic eight “tracheostomy cannula”, and topic nine “enteral feeding” from the ranking choices as these topics are relevant for some patients only.
The duration of the questionnaire was around 7 minutes.
Data Analysis
In the first round, we calculated the median (Mdn) of the relevance and the interquartile ranges (IQR) of the relevance and the comprehensiveness. Objectives were considered relevant and comprehensive for all participants if they reached consensus (IQR ≤ 1) with a smaller IQR indicating a higher consensus,1 and Mdn ≥ 6 on the 7-point Likert scale1 suggesting agreement.
During the second round, the stability, ie, the consistency of responses between successive rounds of the study, was examined by the non-parametric Wilcoxon test (Z). A non-significant Wilcoxon test at p>0.05 indicated no significant difference between the ratings of the same objectives in round 1 and round 2, hence, stability was considered confirmed. Furthermore, we verified if the choice of the list of objectives were comprehensive for all participants when it reached consensus (IQR ≤ 1).
In round 3, in addition to the stability and agreement calculations, we performed an Mdn calculation to obtain the final ranking of the objectives by priority.25 The theme with the lowest Mdn was considered the most important by the participants. When two themes acquired the same median, we referred to their means to decide concerning the ranking,27 the theme with the lowest mean was considered with a higher priority. The analysis was performed with IBM SPSS Statistics Base v21.0.
Results
A summary of the calculation of the Delphi results is presented in Figure 1.
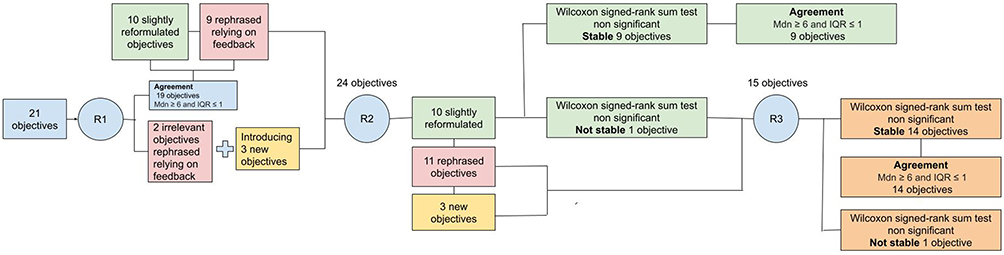 |
Figure 1 Summary of the calculation of the Delphi results. |
Profile of Participants
The 94 participants who agreed to participate in the study amongst 185 approached, filled in the first-round questionnaire, 78 filled the second-round questionnaire, and 70 filled out the third-round questionnaire. The number of participants of each subcategory and the reasons for attrition is presented in Figure 2.
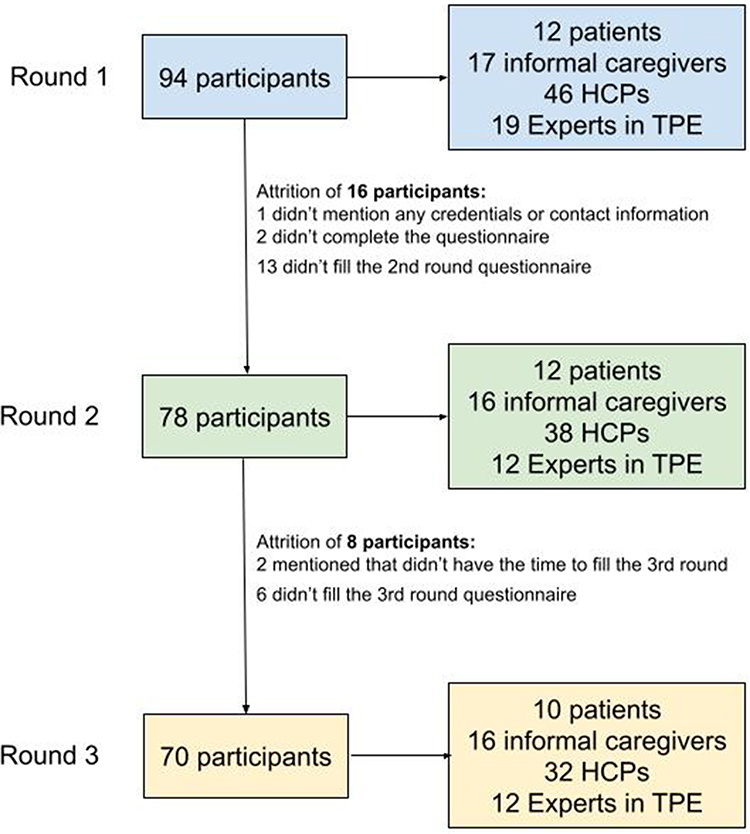 |
Figure 2 Participants of each subcategory and the reasons for attrition. |
The participants were located in six countries: Lebanon, Egypt, Belgium, France, Norway, and Spain. The mean age of participants was 39.18 years (SD=15.75). The participants were mostly female (71.28%). Stroke was the most frequent etiology of patients’ OD (58.33%). The status of the relationship of the informal caregiver to the patient was mostly daughter or son with 70.59%.
Results of Round 1
The Round 1 questionnaire included 12 themes broken down into 21 educational objectives. First, we calculated the median and interquartile range. The results indicated agreement by the 94 participants on the relevance of 19 of the 21 educational objectives initially proposed. Two objectives: “Explain the benefits of tracheostomy” and “Perform technical gestures related to tracheostomized patients during meals” belonging to theme 8 “Tracheostomy tube” did not obtain the agreement of the participants (MDN<6 and an IQR>1). The majority of the participants considered it necessary to specify for themes 8 “Tracheostomy tube” and 9 “Enteral feeding” that they are only relevant according to the situation of the patient. Table 1 shows, the calculation of the median and interquartile for the 21 objectives.
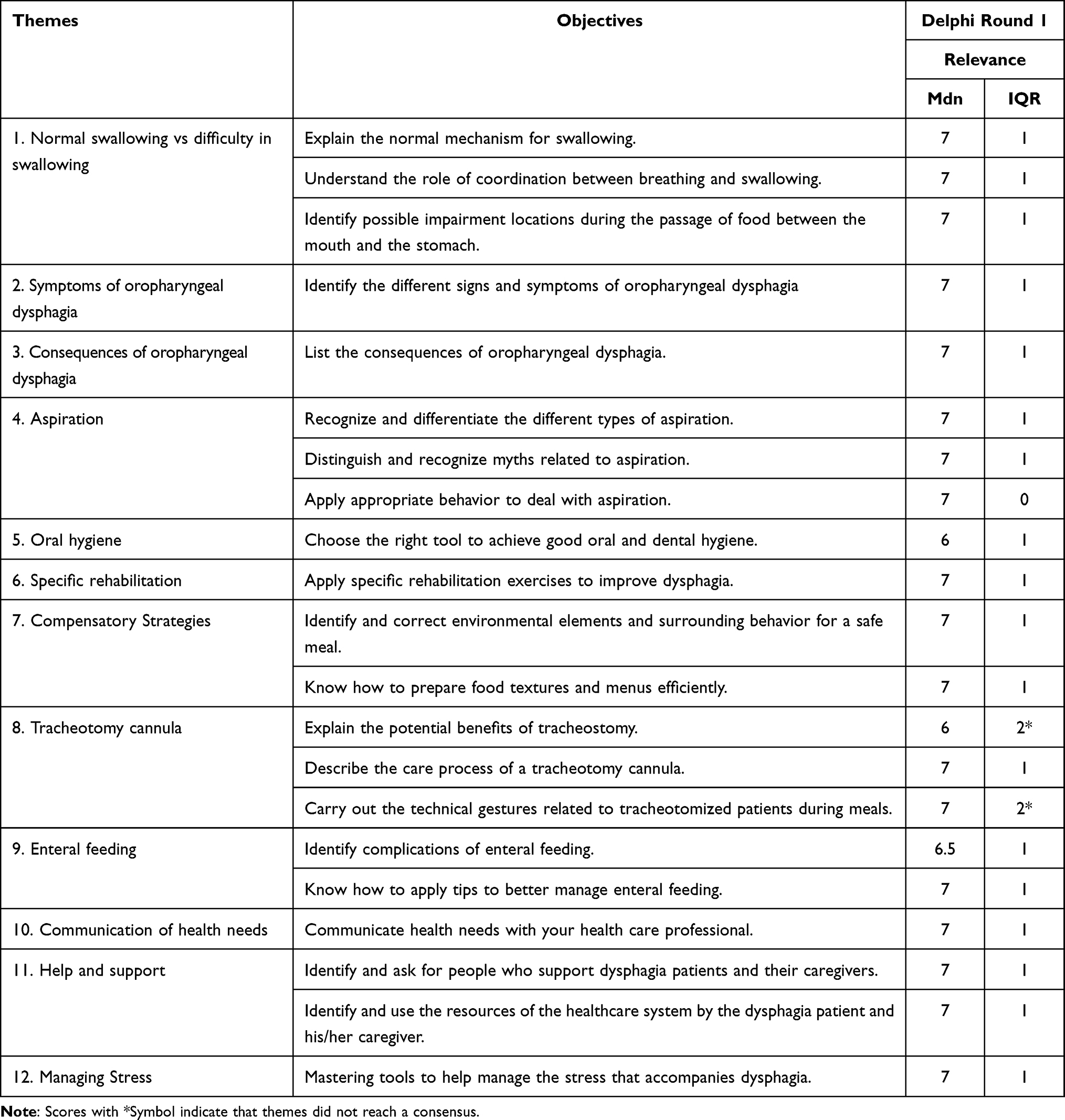 |
Table 1 Median and Interquartile Calculation of the Relevance of the Objectives of Round One |
Relying on the quantitative results, the majority of participants considered the suggested list of objectives as complete, the comprehensiveness criterion received consensus (IQR ≤ 1). But when we checked the qualitative feedback of the participants in the comments, we noticed the need to add objectives, and this was done in round two as explained below.
Results of Round 2
To constitute the second-round questionnaire, we added overall three objectives (Explain the link between good oral/dental hygiene and swallowing disorder of theme 5 “oral hygiene” and Choose foods and drink to get the recommended calorie and water intake of theme 7 “compensatory strategies”) and one new theme comprising one objective (theme 13 “appropriation of dysphagia”: Describe your story and experience from the onset of dysphagia and plan your life project) to round 2 to complete the list of objectives. We made modifications on the two objectives that were not considered relevant by the participants and we relied on the comments to rephrase or clarify several objectives by adding examples, explanations, or by adding precisions. For example, for theme 8 “Tracheostomy cannula” and theme 9 “Enteral feeding” we added the precision “The objectives are exclusively addressed according to the case and the needs of each patient and their caregiver” in red. Hence, the second round comprised 13 themes including 24 educational objectives.
The analysis of round 2 focused on determining the stability using the non-parametric Wilcoxon test. Between round 1 and round 2, we calculated the stability of the objectives that we did not change or were slightly rephrased from round 1. Subsequently, we calculated the stability of 10 objectives among the 24 (leaving aside the 11 objectives that were enormously changed and the 3 objectives that were added newly to round 2) using the non-parametric Wilcoxon test (Table 2). Among these 10 objectives, only one objective (Communicate health needs with your healthcare professional of theme 10 “Communication of health needs”) did not reach stability (Z=−2.182; p = 0.029). Therefore, we calculated the median and interquartile for the 9 stable remaining objectives. The results indicated participant agreement on these 9 objectives (Table 2). Lastly, the majority of participants considered the suggested list of objectives as complete, the comprehensiveness criterion received consensus (IQR ≤ 1). We sent the remaining 15 objectives in a third round.
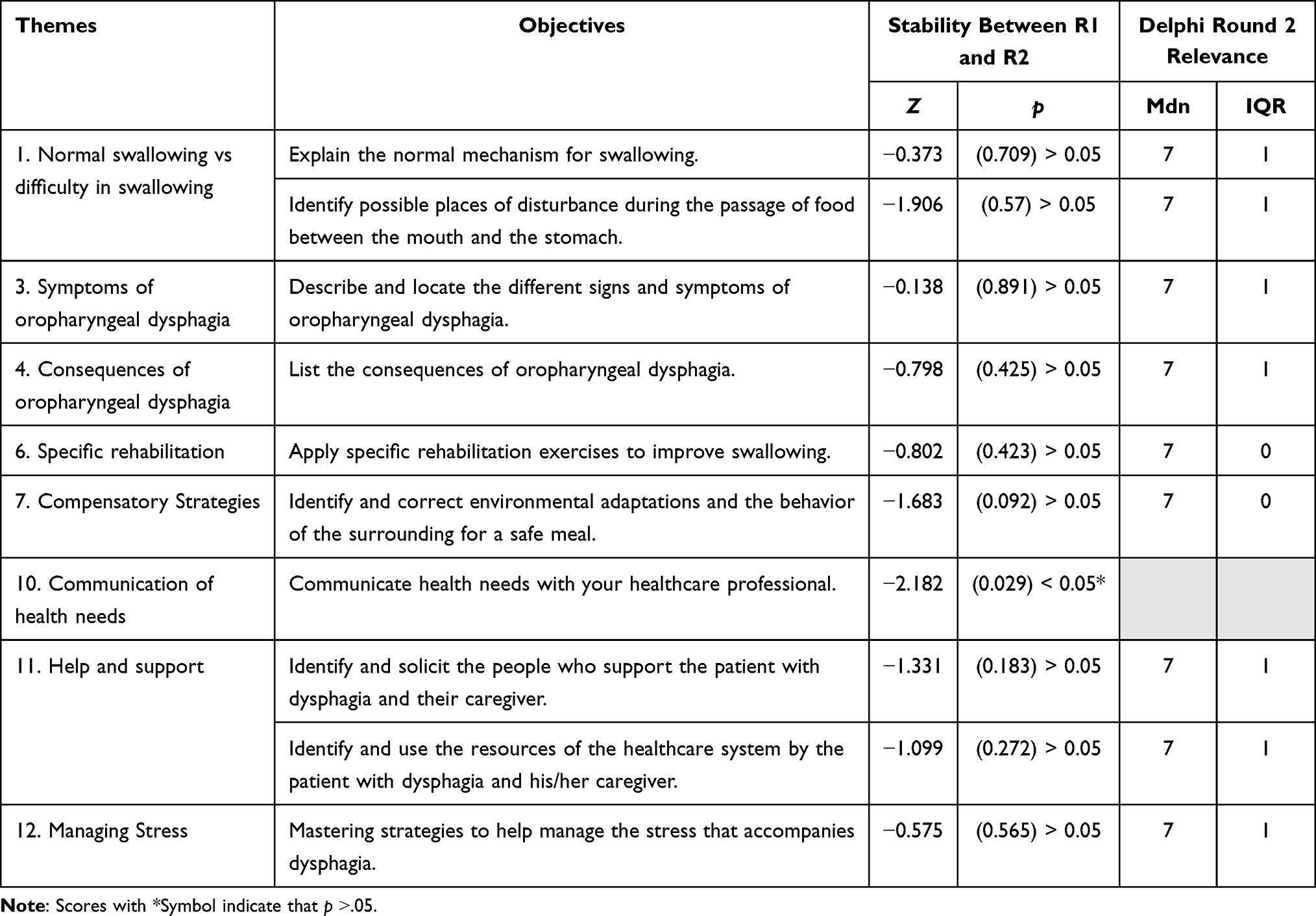 |
Table 2 Stability of the Responses Between Round 1 and Round 2 Using Wilcoxon Sign-Rank Test and Calculation of Median and Interquartile of the Relevance of the Stable Objectives of Round 2 |
Results of Round 3
The third and final round questionnaire was composed of 8 themes comprising 15 educational objectives.
Part 1
Similar to the two previous rounds, the analysis of the results of round 3 focused on calculating the stability and the degree of agreement. The results showed stability of response of the 70 participants on the 14 objectives amongst the 15. The responses to the objective “Recognize the different types of aspiration” of theme 2 “Aspiration” were not proven to be stable between round 2 and round 3 (Z = −2.396; p = 0.017) (Table 3). The 14 objectives with stable responses obtained an agreement on the relevance from the participants (Mdn ≥ 6; IQR ≤ 1) (Table 3). As a result, the transversal list of the educational program comprises 13 themes including 23 educational objectives.
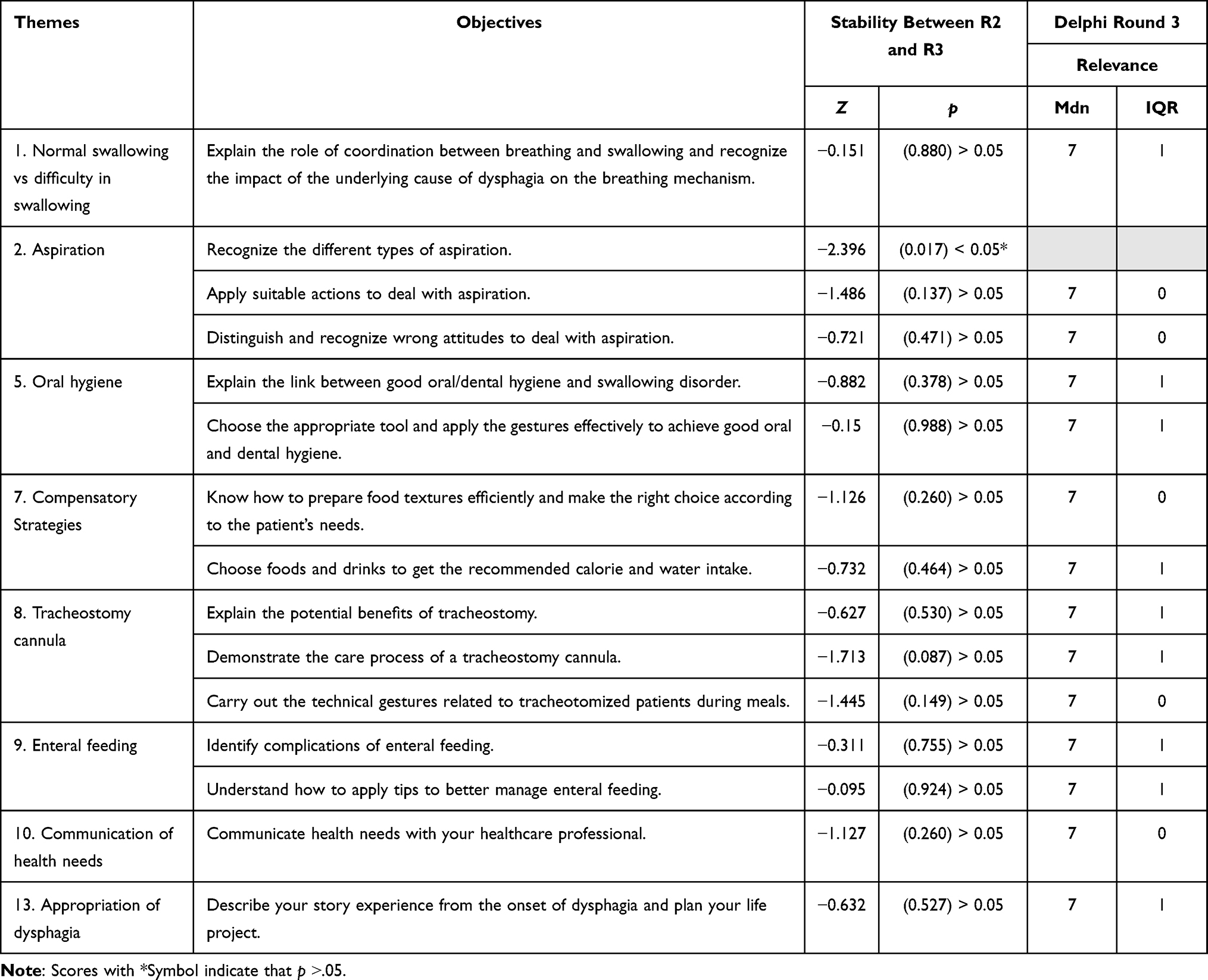 |
Table 3 Stability of the Responses Between Round 2 and Round 3 Using Wilcoxon Sign-Rank Test and Calculation of Median and Interquartile of the Relevance of the Stable Objectives of Round 3 |
Part 2
Figure 3 shows the results of ranking in which we calculated the medians for each of the 13 themes. The theme with the lowest median was considered with the highest rank. When having the same median, we calculated the mean to judge the rank of the theme, the theme with the lowest mean was considered with a higher priority. The participants ranked theme “normal swallowing vs difficulty swallowing”, “aspiration”, “symptoms of OD”, “consequences of OD” and “compensatory strategies” as the highest top five priority and theme “help and support” as the lowest priority.
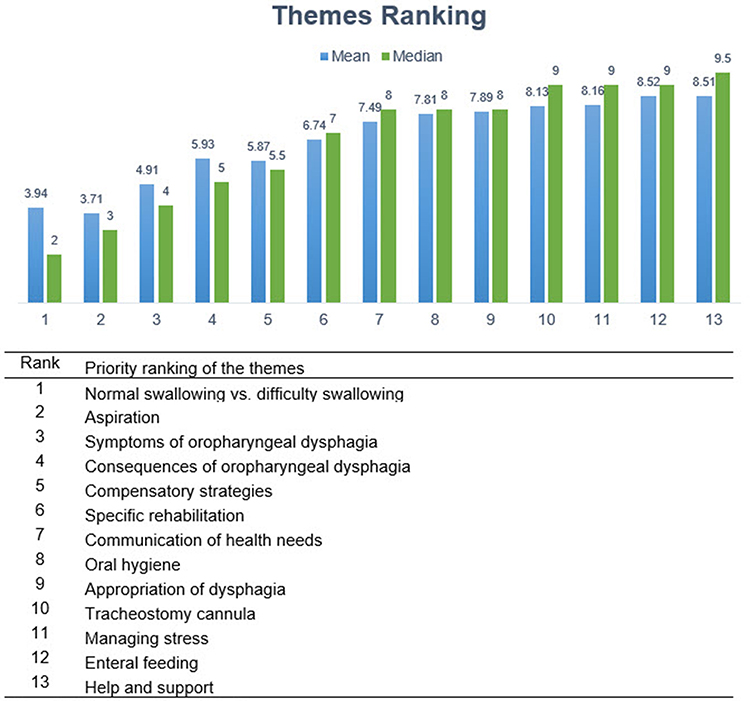 |
Figure 3 Priority ranking of the themes. |
Discussion
In the present study, we aimed to reach a consensus on the content of a competency framework of a universal and transversal educational program for adult patients with OD and their informal caregivers. Following the reviewed literature, we could not find clear benchmarks for determining the core competency framework of the TPE program for adult patients with OD and their informal caregivers. Therefore, the lack of evidence on what patients and their caregivers should be trained on led us to move towards consensus methods that seek to reach an agreement of the content by experts. The results obtained after the third and final round showed agreement from 70 participants on 13 themes comprising 23 educational objectives (Supplementary Table 1).
Knowing OD is a medical condition that affects the physical health matter and the social and psychological aspect of an individual life,28 we included themes comprising objectives targeting self-care and psychosocial skills as also recommended by the World Health Organization (WHO) considerations for TPE.29
Regarding the findings of the Delphi study, we note that the participants suggested the inclusion of one objective targeting self-care skills in the “Oral Hygiene” theme “Explain the link between good oral/dental hygiene and swallowing disorder”, the addition of this objective contributed to have a complete theme about “Oral Hygiene” while we educate the patient and their informal caregiver about the right tool to use to provide optimal oral hygiene and to understand the relationship between poor oral hygiene, a weak immune system, aspiration pneumonia and swallowing disorders.30,31 The participants also suggested the addition of another self-care objective “Choose foods and drinks to get the recommended calorie and water intake” in theme 7 “Compensatory strategies” which is also a very valuable addition that strengthen a multidisciplinary approach and teaches the patient and their caregiver about the proper food and liquid intake to avoid malnutrition and dehydration and therefore preserve a good quality of life. One last addition was an objective targeting psychosocial skills “Describe your story and experience from the onset of dysphagia and plan your life project” with a thirteenth theme “Appropriation of Dysphagia”. This addition is also imperative toward a global approach of TPE, especially since eating is a social behavior thus the onset of OD can influence the daily activities32 and the life plans of the patient and their family. Therefore, while working with patients with OD we need to think of the emotional, psychological, and behavioral well-being of the patient not only limiting the treatment to a precise symptom.
On the other hand, this Delphi study revealed areas of disagreement. The objective “Recognize the different types of aspiration” of theme 2 “Aspiration” did not reach a consensus. The participants did not agree with this objective because the wording of the example was not, in their opinion, clear and specific. However, it would be important to include this theme since it was ranked second in priority by the participants and that multiple published studies have shown the importance of knowing the relationship between inhalation lung disease, very often caused by aspiration, and oropharyngeal dysphagia.31 Clear and precise explanations to the patient and their family are important, due to the vital prognosis being at stake, especially in the case of silent aspiration. Therefore, healthcare professionals have to provide information and, this is not only through simple passive information but by including the knowledge to be acquired around the aspiration in specific workshops inserted in a therapeutic education program9 to help the patients and their caregivers acquire the required competencies to recognize and prevent aspiration, therefore, preserve their quality of life. Moreover, the participants did not agree on the objectives “Explain the potential benefits of tracheostomy” and “Carry out the technical gestures related to tracheostomized patients during meals” belonging to theme 8 “Tracheostomy cannula” in round one. The participants found that theme 8, as well as theme 9 “Enteral feeding”, are not relevant to all patients. Hence, they did not find it necessary to receive this information since not all patients would undergo a tracheostomy or enteral feeding. Even though we know that when swallowing disorders arise enteral feeding is not always recommended33 and not all dysphagia patients will necessarily need a tracheotomy or enteral feeding but we kept these two themes (8 and 9) and added a precision stating that “the objectives can be chosen to be used depending on the case and need of the patient and their caregiver”. Because it is really important to educate the patients and their caregivers about the objectives of these two themes when needed knowing the specificities of these two interventions and the psychological distress that can arise.34,35 Furthermore, we wanted to highlight that the multidisciplinary team must always discuss it with the patient and their family and must imperatively obtain the patient or the family’s consent.36
All the above mentioned, get us to an important recommendation which is to adapt the implementation of TPE following the needs of the patients and their families.29,37
Finally, the ranking by the participants of the 13 themes comprising the 23 educational objectives showed us that the highest priority objectives are related to self-care skills. Among these, the theme of oral hygiene was ranked 8th, showing the lack of knowledge of the importance of such skill as revealed amongst HCPs38 and patients.39 This finding encouraged us to include this theme as a priority knowing its enormous importance in the daily care of the patient with OD.30,40 As for the psychosocial skills, it was ranked 7th by the participants. The result of the ranking reveals that the psychosocial aspect of OD is less taken into consideration reflecting the reality of OD intervention where mostly the bioclinical aspects are considered. This could be due to the assumption that dealing with psychosocial consequences implicitly in clinical practices is enough. But when looking at OD from the lens of WHO’s International Classification of Functioning, Disability, and Health (ICF) framework, we have to look at the patient with OD holistically to help him acquire a better quality of life hence taking into consideration the social and psychological aspects of OD. Therefore, the inclusion of psychosocial skills is really important to decrease the common social and psychological consequences of OD such as the sense of isolation, avoidance of eating with others, and anxiety during mealtime28 amongst other consequences and treating the patient as a whole not only considering the physical impact.41
Limitations
Our Delphi study has some limitations. First, it was difficult to obtain the agreement of a larger number of patients and informal caregivers meeting the inclusion criteria and willing to participate in the study due to the Covid-19 pandemic. Because the health crisis has curtailed the majority of management of dysphagia patients and limited consultations and treatment at home.42 It prevented health professionals from being in direct and regular contact with their patients and, they were unable to involve them in the study. In addition, a potential bias in the perception of needs can be explained through the recruitment of some participants from the researcher’s network. Second, it was similarly difficult to recruit pulmonologists, even though it would have been interesting to collect the opinion of these health professionals who have an essential if not primary role in the follow-up of dysphagia patients.43 However, the items that are related to their specialization (aspiration, consequences of OD …) were still considered “totally appropriate” by all health professionals knowing their importance. Similarly, in Clayton’s 2006 study to identify core dermatologic content in the undergraduate medical curriculum, geriatricians and plastic surgeons did not participate. Nevertheless, items related to their specialties (pressure ulcers, cutaneous malignancies) were deemed “very important” following data collection from the questionnaires in the various rounds of the Delphi.44 An additional limitation is that from round to round, the attrition rate increased. The first round consisted of 94 participants, the second round of 78, and the third and final round of 70 participants. In each of the four categories, the number of participants decreased even though we tried to have a balance between them. We aimed to have at least 10 participants in each group at the end of the process as indicated in the literature to obtain reliable results.18
Conclusion
In conclusion, TPE is an important component in the management for dysphagia patients but lacks clear benchmarks on what should be the pursued skills. Therefore, we moved towards a Delphi method that seeks to reach a consensus on the content of a competency framework for OD patients and their informal caregivers. The results showed that the participants (HCPs, TPE experts, ICGs, and patients) agreed on 13 themes comprising 23 educational objectives, which are strong benchmarks for clinical practitioners who wish to implement TPE in OD. These help to offer comprehensive support and to maximize the possibilities of recovery to assist the patient and their family to cope with the disorder daily and thus benefit from a better quality of life. In future studies, it would be interesting to develop the objectives into learning activities and test their feasibility and acceptability amongst health professionals and OD patients, before checking at a later stage their efficacy with the patients and their informal caregivers.
Abbreviations
ENT, ear, nose, and throat specialist; HCP, healthcare professionals; ICF, International Classification of Functioning, Disability, and Health; ICG, informal caregivers; IQR, Interquartile; Mdn, Median; OD, oropharyngeal dysphagia; R, Round; REC, Research Ethics Committee; TPE, therapeutic patient education; WHO, World Health Organization.
Acknowledgments
We thank all of the experts who participated in this Delphi study for their time and for sharing their expertise.
Disclosure
The authors report no conflicts of interest in this work. The abstract of this paper was presented at the 11th European Society of Swallowing Disorders (ESSD) CONGRESS Conference “Optimizing management across the etiological spectrum – new tricks for an old problem” as a poster presentation with interim findings. The poster’s abstract is published in the Dysphagia Journal (11th ESSD Congress, 2021. Dysphagia. 2022. https://doi.org/10.1007/s00455-022-10456-y).
References
1. Ortega O, Martín A, Clavé P. Diagnosis and management of oropharyngeal dysphagia among older persons, state of the art. J Am Med Dir Assoc. 2017;18(7):576–582. doi:10.1016/j.jamda.2017.02.015
2. Cichero BS. Dysphagia clinical guidelines. The Speech Pathology Association of Australia Ltd; 2012:1–56. Available from: https://www.speechpathologyaustralia.org.au/SPAweb/Members/Clinical_Guidelines/spaweb/Members/Clinical_Guidelines/Clinical_Guidelines.aspx.
3. Royal College of Speech & Language Therapists. Royal College of Speech & Language Therapists Clinical Guidelines.
4. CASLPO. Practice standards and guidelines for dysphagia intervention by speech-language pathologists. College of Audiologists and Speech-Language Pathologists of Ontario (CASLPO); 2018. Available from: www.caslpo.com/practicestandards.com.
5. Brin-Henry F, Marchand C, Klein A, Diancourt S, Bernard E. L’Education Thérapeutique du Patient en orthophonie [Therapeutic Patient Education in speech therapy]. 2014:170. French.
6. The Diabetes Unit, Menzies Centre for Health Policy, The University of Sydney. National evidence based guideline for patient education in type 2 diabetes; 2009:190. Available from: http://www.nhmrc.gov.au/guidelines/publications/di16.
7. Pétré B, Guillaume M, Legrand C, et al. Un synoptique des co-compétences patients-soignants en éducation thérapeutique [An overview of therapeutic education skills for patients and healthcare professionals]. Educ Ther Patient. 2014;6(1):10202. French. doi:10.1051/tpe/2014003
8. Balica S, Bernier C, Mazereeuw-Hautier J, et al. Élaboration d’un référentiel d’éducation thérapeutique dans le psoriasis [Guide for therapeutic education program in psoriasis]. Annales de Dermatologie et de Vénéréologie. 2011;138(4):337–353. French. doi:10.1016/j.annder.2010.12.008
9. Daviet JC, Bonan I, Caire JM, et al. Therapeutic patient education for stroke survivors: non-pharmacological management. A literature review. Ann Phys Rehabil Med. 2012;55(9–10):641–656. doi:10.1016/j.rehab.2012.08.011
10. Krajczy E, Krajczy M, Luniewski J, Bogacz K, Szczegielniak J. Assessment of the effects of dysphagia therapy in patients in the early post-stroke period: a randomised controlled trial. Neurol Neurochir Pol. 2019;1. doi:10.5603/PJNNS.a2019.0053
11. Govender R, Taylor SA, Smith CH, Gardner B. Helping patients with head and neck cancer understand dysphagia: exploring the use of video-animation. Am J Speech Lang Pathol. 2019;28(2):697–705. doi:10.1044/2018_AJSLP-18-0184
12. McKinstry A, Tranter M, Sweeney J. Outcomes of dysphagia intervention in a pulmonary rehabilitation program. Dysphagia. 2010;25(2):104–111. doi:10.1007/s00455-009-9230-3
13. Wasserman T, Murry T, Johnson JT, Myers EN. Management of swallowing in supraglottic and extended supraglottic laryngectomy patients. Head Neck. 2001;23(12):1043–1048. doi:10.1002/hed.1149
14. Assez N, Gagnayre R. Consensus about cardiac patients and families’ competencies in emergency situations: use of a multi-partite Delphi method. Educ Ther Patient. 2016;8(2):20102. doi:10.1051/tpe/2016009
15. von der Gracht HA. Consensus measurement in Delphi studies. Technol Forecast Soc Change. 2012;79(8):1525–1536. doi:10.1016/j.techfore.2012.04.013
16. Jennings AA, Guerin N, Foley T. Development of a tool for monitoring the prescribing of antipsychotic medications to people with dementia in general practice: a modified eDelphi consensus study. CIA. 2018;13:2107–2117. doi:10.2147/CIA.S178216
17. Waggoner J, Carline JD, Durning SJ. Is there a consensus on consensus methodology? Descriptions and recommendations for future consensus research. Acad Med. 2016;91(5):663–668. doi:10.1097/ACM.0000000000001092
18. Coetzer A, Sitlington H. What knowledge, skills and attitudes should strategic HRM students acquire? A Delphi study. Asia Pacific J Human Resources. 2014;52(2):155–172. doi:10.1111/1744-7941.12008
19. de Villiers MR, de Villiers PJT, Kent AP. The Delphi technique in health sciences education research. Med Teach. 2005;27(7):639–643. doi:10.1080/13611260500069947
20. Halvorsrud K, Flynn D, Ford GA, et al. A Delphi study and ranking exercise to support commissioning services: future delivery of Thrombectomy services in England. BMC Health Serv Res. 2018;18(1):135. doi:10.1186/s12913-018-2922-3
21. Hsu CC, Sandford BA. The Delphi technique: making sense of consensus. Pract Assess Res Evaluation. 2007;12(10):8.
22. Blieck Y, Ooghe I, Zhu C, et al. Consensus among stakeholders about success factors and indicators for quality of online and blended learning in adult education: a Delphi study. Stud Continuing Educ. 2019;41(1):36–60. doi:10.1080/0158037X.2018.1457023
23. Rowe G, Wright G. The Delphi technique as a forecasting tool: issues and analysis. Int J Forecast. 1999;15(4):353–375. doi:10.1016/S0169-2070(99)00018-7
24. Li J, Song Y. Formal and informal care. In: Gu D, Dupre ME, editors. Encyclopedia of Gerontology and Population Aging. Springer International Publishing; 2019:1–8. doi:10.1007/978-3-319-69892-2_847-1
25. Ghaddar Z, Durieux N, Tohmé A, Pétré B, Matar N. Educational interventions for patients with oropharyngeal dysphagia and their informal caregivers: a scoping review. Educ Ther Patient. 2022. In press. doi:10.1051/tpe/2022002
26. Limesurvey GH. LimeSurvey: an open source survey tool. Available from: http://www.limesurvey.org.
27. Canter D, Hammond L. Prioritizing burglars: comparing the effectiveness of geographical profiling methods. Police Pract Res. 2007;8(4):371–384. doi:10.1080/15614260701615086
28. Ekberg O, Hamdy S, Woisard V, Wuttge-Hannig A, Ortega P. Social and psychological burden of dysphagia: its impact on diagnosis and treatment. Dysphagia. 2001;17(2):139–146. doi:10.1007/s00455-001-0113-5
29. World Health Organization. Therapeutic patient education: continuing education programmes for health care providers in the field of prevention of chronic diseases: report of a WHO working group; 1998. Available from: https://apps.who.int/iris/handle/10665/108151.
30. Ashford JR. Oral care across ages: a review. Perspect Swal Swal Dis. 2012;21(1):3–8. doi:10.1044/sasd21.1.3
31. Langmore SE, Terpenning MS, Schork A, et al. Predictors of aspiration pneumonia: how important is dysphagia? Dysphagia. 1998;13(2):69–81. doi:10.1007/PL00009559
32. Threats T. Use of the ICF in dysphagia management. Semin Speech Lang. 2007;28(4):323–333. doi:10.1055/s-2007-986529
33. JAGS. American Geriatrics Society feeding tubes in advanced dementia position statement. J Am Geriatr Soc. 2014;62(8):1590–1593. doi:10.1111/jgs.12924
34. Nakarada-Kordic I, Patterson N, Wrapson J, Reay SD. A systematic review of patient and caregiver experiences with a tracheostomy. Patient. 2018;11(2):175–191. doi:10.1007/s40271-017-0277-1
35. Vesey S. Dysphagia and quality of life. Br J Community Nurs. 2013;18(Sup5):S14–S19. doi:10.12968/bjcn.2013.18.Sup5.S14
36. Haute Autorité de Santé HAS. Place et gestion de la trachéotomie dans la prise en charge de la dépendance ventilatoire des patients atteints de maladies neuromusculaires lentement évolutives [Place and management of tracheostomy in the management of ventilatory dependence in patients with slowly progressive neuromuscular diseases]; 2020. Available from: https://www.has-sante.fr/jcms/p_3217806/fr/place-et-gestion-de-la-tracheotomie-dans-la-prise-en-charge-de-la-dependance-ventilatoire-des-patients-atteints-de-maladies-neuromusculaires-lentement-evolutives.
37. Martino R, McCulloch T. Therapeutic intervention in oropharyngeal dysphagia. Nat Rev Gastroenterol Hepatol. 2016;13(11):665–679. doi:10.1038/nrgastro.2016.127
38. Durgude Y, Cocks N. Nurses’ knowledge of the provision of oral care for patients with dysphagia. Br J Community Nurs. 2011;16(12):604–610. doi:10.12968/bjcn.2011.16.12.604
39. Ajwani S, Ferguson C, Kong AC, Villarosa AR, George A. Patient perceptions of oral health care following stroke: a qualitative study. BMC Oral Health. 2021;21(1):127. doi:10.1186/s12903-021-01501-7
40. Umay E, Eyigor S, Ertekin C, et al. Best practice recommendations for stroke patients with dysphagia: a Delphi-based consensus study of experts in Turkey-part II: rehabilitation. Dysphagia. 2021;36(5):800–820. doi:10.1007/s00455-020-10218-8
41. Ciucci M, Jones C, Malandraki G, Hutcheson K. Dysphagia practice in 2035: beyond fluorography, thickener, and electrical stimulation. Semin Speech Lang. 2016;37(03):201–218. doi:10.1055/s-0036-1584155
42. Fong R, Tsai KCF, Tong MCF, Lee KYS. Management of dysphagia in nursing homes during the COVID-19 pandemic: strategies and experiences. SN Compr Clin Med. 2020;2(9):1361–1365. doi:10.1007/s42399-020-00464-0
43. Mankekar G. Swallowing – Physiology, Disorders, Diagnosis and Therapy. Springer India; 2015. doi:10.1007/978-81-322-2419-8
44. Clayton R, Perera R, Burge S. Defining the dermatological content of the undergraduate medical curriculum: a modified Delphi study. Br J Dermatol. 2006;155(1):137–144. doi:10.1111/j.1365-2133.2006.07190.x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.