Back to Journals » Journal of Pain Research » Volume 18
Consensus Guidelines for the Use of Peripheral Nerve Stimulation in the Treatment of Chronic Pain and Neurological Diseases: A Neuron Project from the American Society of Pain and Neuroscience
Authors Latif U, Moghim R, Valimahomed A, Lam CM ![]() , Abd-Elsayed A, Gulati A
, Abd-Elsayed A, Gulati A ![]() , Aman MM
, Aman MM ![]() , Desai MJ
, Desai MJ ![]() , Dickerson DM
, Dickerson DM ![]() , Tieppo Francio V
, Tieppo Francio V ![]() , Gilmore C, Gish B
, Gilmore C, Gish B ![]() , Hah JM
, Hah JM ![]() , Hunter C, Ilfeld BM, Kalia H
, Hunter C, Ilfeld BM, Kalia H ![]() , Lester D, Li S
, Lester D, Li S ![]() , Mata R
, Mata R ![]() , Naidu R
, Naidu R ![]() , Ottestad E, Pritzlaff SG
, Ottestad E, Pritzlaff SG ![]() , Schatman ME
, Schatman ME ![]() , Sheth SJ, Slavin KV
, Sheth SJ, Slavin KV ![]() , Suvar T, Yalamuru B, Staats PS
, Suvar T, Yalamuru B, Staats PS ![]() , Sayed D
, Sayed D ![]() , Deer TR
, Deer TR ![]()
Received 28 April 2025
Accepted for publication 24 September 2025
Published 7 November 2025 Volume 2025:18 Pages 5949—5990
DOI https://doi.org/10.2147/JPR.S537222
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Andrea Tinnirello
Usman Latif,1 Robert Moghim,2 Ali Valimahomed,3 Christopher M Lam,1 Alaa Abd-Elsayed,4 Amitabh Gulati,5 Mansoor M Aman,6 Mehul J Desai,7,8 David M Dickerson,9 Vinicius Tieppo Francio,10 Christopher Gilmore,11 Brandon Gish,12 Jennifer M Hah,13 Corey Hunter,14,15 Brian M Ilfeld,16 Hemant Kalia,17 Denise Lester,18 Sean Li,19 Robin Mata,20 Ramana Naidu,21 Einar Ottestad,22 Scott G Pritzlaff,23 Michael E Schatman,24 Samir J Sheth,25 Konstantin V Slavin,26 Tolga Suvar,27 Bhavana Yalamuru,28 Peter S Staats,29 Dawood Sayed,1 Timothy R Deer30
1Department of Anesthesiology and Interventional Pain, The University of Kansas Health System, Kansas, KS, USA; 2Interventional Spine and Pain, Colorado Pain Care, Denver, CO, USA; 3Interventional Pain Medicine, Advanced Orthopedics Sports Medicine Institute, Freehold, NJ, USA; 4Department of Anesthesiology, University of Wisconsin, Madison, WI, USA; 5Department of Anesthesiology, Memorial Sloan Kettering Cancer Center, New York, NY, USA; 6Alleviate Pain & Spine, De Pere, WI, USA; 7International Spine, Pain and Performance Center, Washington, DC, USA; 8Monument Research Institute, Washington, DC, USA; 9Department of Anesthesiology, Critical Care and Pain Medicine, Endeavor Health, Evanston, IL, USA; 10Department of Anesthesiology, Washington University School of Medicine, St. Louis, MO, USA; 11Queen City Clinical Research, Charlotte, NC, USA; 12Department of Interventional Pain, Lexington Clinic, Lexington, KY, USA; 13Department of Anesthesiology, Perioperative, and Pain Medicine, Stanford University, Stanford, CA, USA; 14Ainsworth Institute of Pain Management, New York, NY, USA; 15Department of Rehabilitation & Human Performance, Icahn School of Medicine at Mount Sinai, New York, NY, USA; 16Department of Anesthesiology, University of California San Diego, La Jolla, CA, USA; 17C.R.I.S.P Center for Research & Innovation in Spine & Pain, Rochester, NY, USA; 18Department of Physical Medicine & Rehabilitation, Richmond VA Medical Center, Virginia Commonwealth University, Richmond, VA, USA; 19National Spine and Pain Centers, Shrewsbury, NJ, USA; 20Department of Physical Medicine and Rehabilitation, University of Miami/Jackson Health System, Miami, FL, USA; 21MarinHealth Spine Institute, UCSF Affiliate, Larkspur, CA, USA; 22Department of Anesthesiology, Perioperative and Pain Medicine, Stanford University School of Medicine, Stanford, CA, USA; 23Department of Anesthesiology and Pain Medicine; University of California - Davis, Sacramento, CA, USA; 24Department of Anesthesiology, Perioperative Care and Pain Medicine, Department of Population Health - Division of Medical Ethics, NYU Grossman School of Medicine, New York, NY, USA; 25Sutter Health System, Roseville, CA, USA; 26Department of Neurosurgery, University of Illinois at Chicago, Chicago, IL, USA; 27Department of Anesthesiology and Pain Medicine, Rush University, Chicago, IL, USA; 28Department of Anesthesiology, University of Virginia, Charlottesville, VA, USA; 29National Spine and Pain Centers, Atlantic Beach, FL, USA; 30The Spine and Nerve Center of the Virginias, Charleston, West Virginia, USA
Correspondence: Usman Latif, Department of Anesthesiology and Interventional Pain, The University of Kansas Health System, Kansas, KS, USA, Email [email protected]
Abstract: Peripheral nerve stimulation (PNS) has evolved substantially over recent decades in terms of hardware and evidence supporting efficacy. Treatment targets continue to expand and address both pain and functional applications. The American Society of Pain and Neuroscience (ASPN) seeks to substantially update and expand upon a review of the evidence supporting PNS as well as provide guidelines for clinical practice. A diverse multidisciplinary panel of experts was selected to provide opinions and guidance based on evidence-graded assessment and clinical knowledge. This document aims to serve as a resource for clinicians and payors in the interest of expanding awareness of the breadth of research in the field of PNS and expanding access to therapy.
Keywords: peripheral nerve stimulation, neuromodulation, pain, technique, evidence, nerve injury, review, guideline
Introduction
Peripheral nerve stimulation (PNS) is an essential category of neuromodulation, allowing for a targeted approach to focal pain coverage via a peripheral axon. Early use of devices for this indication involved cuffed electrodes and paddle leads originally designed for spinal use. Significant technological advances have resulted in hardware customized for this application with implantable electrodes and decoupled internal pulse generators that operate in concert with external power sources. This is a shift from repurposing spinal cord stimulator (SCS) systems for this application.1 Expanding payor coverage, growing research demonstrating efficacy, and proliferating descriptions of procedural techniques for burgeoning indications have increased the prevalence and accessibility of PNS for the benefit of patients.2 The initial description of this therapy was by Sweet and Wall in 1967 via an open neurosurgical method. Weiner and Reed described a percutaneous lead placement technique that accelerated the procedure’s adoption and ease.3 Current work is focused on expanding indications, targets, and payor coverage while advancing the technology and design of leads and implantable and wearable hardware.
Methods
The American Society of Pain and Neuroscience (ASPN) is committed to increasing evidence-based access to treatment. In furtherance of that mission, ASPN created a multidisciplinary panel of authors consisting of anesthesiologists, pain medicine physicians, physical medicine and rehabilitation physicians, and neurosurgeons who are experts and leaders in PNS. This panel was supplemented with residents and fellow physicians demonstrating significant potential in the field. Critical focus areas were developed into an outline and refined by the lead author, senior authors, and a small group of section editors. The authors then worked in teams and undertook a search of global English-language literature from multiple databases, including Medline, EMBASE, and PubMed. Specific search terms, including MESH terms, were chosen to identify relevant peer-reviewed articles, such as meta-analyses, systematic reviews, and randomized controlled trials. The identified literature was then critically evaluated and graded using the United States Preventive Services Task Force (USPSTF) criteria for evidence level (Table 1) and degree of recommendation (Table 2). Following evidence-based analysis, each team formulated initial consensus points, which were then submitted to the entire author group for review. Through an iterative process of consolidation and refinement, the statements were developed until final consensus was achieved among all authors.
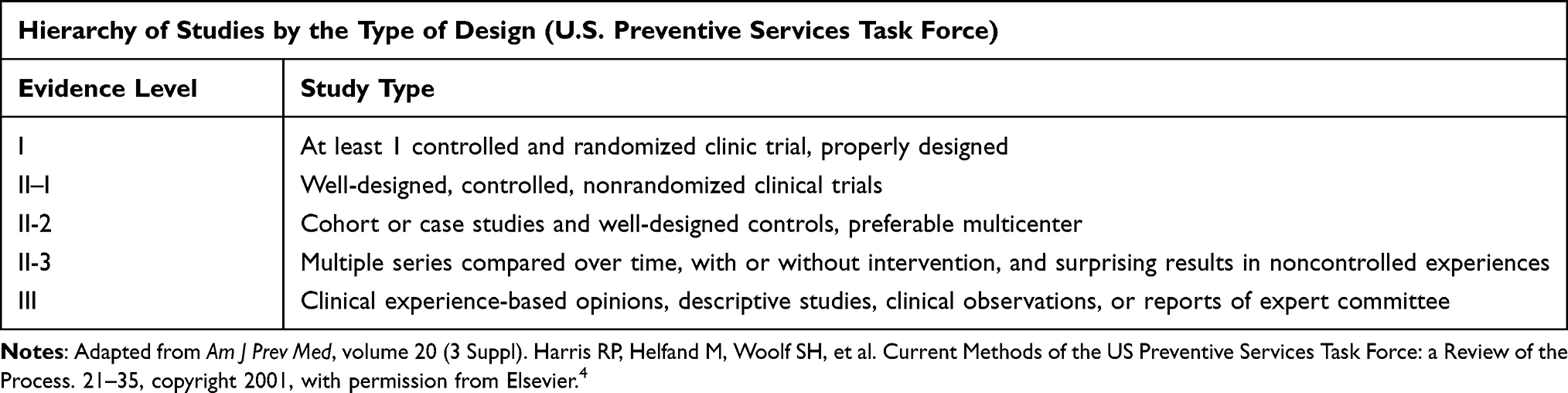 |
Table 1 Hierarchy of Studies by the Type of Design (U.S. Preventive Services Task Force) |
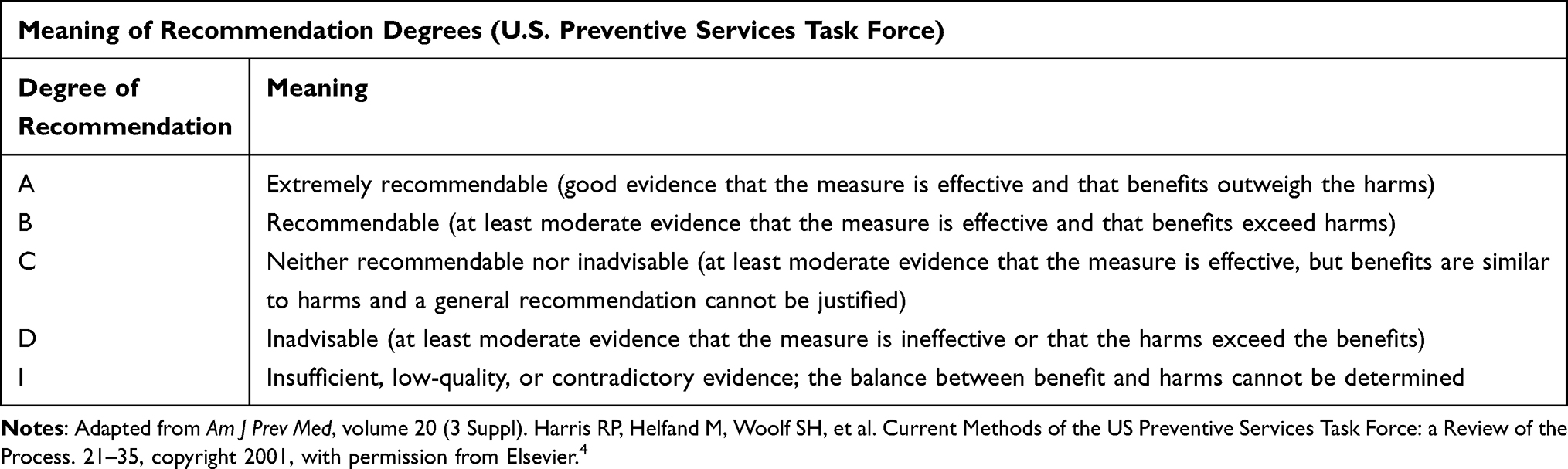 |
Table 2 Meaning of Recommendation Degrees (U.S. Preventive Services Task Force) |
All authors disclosed financial conflicts of interest and were asked to recuse themselves on any issue with which they have a relationship and competing interests. In cases where conflicted authors were the authority in an area, a nonconflicted author served as the ultimate editor of any submitted material. The purpose and scope of this paper are to serve as a resource for clinicians and payors in the interest of expanding awareness of the breadth of research in the field of PNS and expanding access to therapy for patients suffering from chronic pain, post-operative pain, or functional issues. The goal is to provide comprehensive, evidence-based recommendations on the appropriateness, efficacy, and safety of the reviewed treatments to guide clinical practice as well as practical guidance on billing and payor coverage.
Physiology
Neuromodulation systems, such as peripheral nerve stimulation (PNS), utilize electricity to modulate nerves, altering the transmission of pain signals to the brain. In the case of PNS, a peripheral nerve is targeted to alleviate peripheral neuropathic pain. Following injury, an inflammatory cascade activates pro-inflammatory cytokines and neuropeptides that heighten nociceptive afferents’ excitability, sensitizing dorsal horn neurons and diminishing inhibitory transmission. This exacerbates pain transmission to the sensory cortex, altering pain representation and sensory processing.5,6 Abnormal glial activation, ectopic firing, and interneuron excitation contribute to persistent neural hyper-excitability across peripheral, spinal, and cranial levels. Chemical and environmental shifts can induce prolonged nociception, triggering chemical and structural transformations at the spinal and supraspinal levels, culminating in a chronic neuropathic pain state.7 Thus, peripheral and central sensitization are likely involved in the development of chronic neuropathic pain syndromes post-nerve dysfunction.8
The exact mechanism of action for PNS is uncertain. Several theories implicate central nervous system involvement, while others propose peripheral mechanisms, including stimulation conduction block in afferent fibers. Understanding neuropathic pathophysiologic mechanisms involving inflammatory cascades, changes in neural transmission, and cerebral vascular changes is crucial for effective pain management.9 Ongoing research into peripheral nerve stimulation mechanisms holds promise to improve peripheral neuropathic pain relief and expand upon indications for use.
Mechanism of Action
Gate Control Theory
The process of electrical nerve modulation, rooted in the “gate control theory”, remains incompletely understood.10 Proposed by Melzack and Wall in 1965, this theory suggests that the analgesic effects of PNS may arise from both central and peripheral mechanisms.10 Stimulating low-threshold, large-diameter A-beta fibers with non-painful stimuli activates inhibitory interneurons, suppressing conduction and discharge in nociceptive A-delta and C nerve fibers within the dorsal horn, impeding their transmission to the central cortex.11 By stimulating A-beta fibers near C fibers, the “gate” in the dorsal horn of the spinal cord can be closed, halting the transmission of painful signals.11 However, alternative theories propose various mechanisms for PNS-induced pain relief, including membrane depolarization blockade, reduced excitation of nociceptors, and suppression of dorsal horn activity.12
Local Chemical and Neurotransmitter Effects
Animal studies suggest the involvement of serotonergic, GABAergic, and glycinergic pathways in the analgesic effects of PNS.13,14 PNS regulates the local neural environment by affecting endogenous opioid activity, glutamate, and aspartate signaling pathways, as well as decreasing neurotransmitters, endorphins, and inflammatory mediators, impacting their concentrations and efficacy.15,16 It is important to note that these mechanisms depend on the type of nerve, type of stimulation, and type of condition being treated.17
Opioid responses via the enkephalin-delta opioid receptor pathway have been identified in transcutaneous electrical nerve stimulation (TENS) and may be implicated in PNS as well.18,19 Anti-inflammatory effects of PNS have also been proposed.20 In human studies, excitation failure of A and C fibers occurs through repeated electrical stimulation.21
Peripherally Induced Reconditioning of CNS
PNS may alleviate central sensitization and hyperalgesia by diminishing excessive peripheral nociceptive activity, inhibiting wide dynamic range neurons, and decreasing Aβ fiber-induced activity.13 GABAergic and glycinergic activity augmentation, along with serotonin and dopamine metabolite alterations, may subsequently occur at the spinal level.12,14 Substance P and CGRP level variations might alter central pain signaling.22 Additionally, it has been proposed that peripheral reconditioning of the central nervous system can occur through prolonged alterations in central plasticity in neuropathic pain states.22
Consensus Guideline 1: The mechanism of action (MOA) of Peripheral Nerve Stimulation (PNS) is complex. It includes modulation of local transmission of pain signals, inhibition of local A and C fibers with repeated stimulation, impact on local inflammatory mediators, endogenous opioids and neurotransmitters, gate control theory, and peripherally induced reconditioning of the central nervous system. Future research will help further describe the MOA of PNS.
PNS Device
PNS is an established treatment approach that has been successfully used for the management of a wide variety of disease states, including motor dysfunction and chronic pain. Although the first series of patients with neuropathic pain treated with PNS was published by Wall and Sweet in early 1967,23 the first documented use of this approach was even earlier, when C.H. Shelden used high-frequency PNS (14 kHz) for treatment of neuropathic facial pain in 196224 (Figure 1). Since that time, PNS has been utilized all over the world as a unique modality for the treatment of various neuropathic pain conditions, with complex regional pain syndromes (CRPS) initially being the most prevalent condition.25 For the first three decades of PNS clinical use, the application of PNS electrodes required surgical exposure of the stimulated nerves, limiting access to this modality only to those who possessed significant surgical expertise.26–28 The situation changed dramatically after the percutaneous PNS technique was introduced by Weiner and Reed in 1999,29 making it available to pain specialists from non-surgical backgrounds and significantly increasing the utilization of this therapy.
 |
Figure 1 History of PNS The history of PNS from inception to advancements to coding. |
The lack of percutaneous, FDA-approved PNS devices hampered the widespread acceptance of PNS as a pain-relieving treatment modality.29 Over the last decade, a multitude of well-designed clinical studies with the use of novel dedicated devices30–32 paved the way for multiple FDA approvals. The recent surge of technological advances and regulatory approvals marked a new era of PNS in the treatment of pain, where it quickly became a globally accepted part of the mainstream neuromodulation armamentarium.32–34 PNS is a recognized component of the educational neuromodulation curriculum endorsed by professional pain societies.35 In 2024, the American Medical Association (AMA) revised CPT codes to address industry confusion regarding the distinction between systems and physician work performed.
Mechanisms of Stimulation
Waveform Background
Stimulation waveforms are a pattern of delivery of electrical energy with the goal of excitation or inhibition of Aα/β afferent fibers to modulate pain. Nociceptive A and C fibers exhibit varying responses to electrical stimulation based on their diameters. Larger diameter fibers require lower intensity stimulation for activation than smaller diameter fibers. This phenomenon suggests using titrated stimulation intensities to primarily activate large diameter Aα/β fibers while avoiding the activation of small-diameter nociceptive fibers through a gating mechanism.36,37 One of the challenges of PNS is that leads are often placed adjacent to mixed motor-sensory nerves, so fiber selectivity is paramount.
In many cases, sensory afferents are the primary targets for sensory stimulation. In certain instances, the emphasis is placed on targeting motor efferent nerves to elicit muscular contraction. The treatment strategy for core muscle atrophy, which centers on stimulating the multifidus muscle in the lumbar spine, has consistently reflected this approach.38 Understanding the stimulation and waveform characteristics of each commercially available PNS device is vital due to their complex programming parameters and nuances.
Low-Frequency Stimulation
Low-frequency stimulation (20 Hz) has been employed in PNS for multiple conditions, including hemiplegic shoulder (HSP) and low back pain. When preferentially applied to mixed motor-sensory nerves, low-frequency stimulation stimulates motor efferent nerves, causing muscular contraction. When applied to the axillary nerve in the shoulder, resulting deltoid muscle contraction may help decrease pain in patients with HSP.39 Although this form of stimulation has shown to have durable pain relief even with temporary therapy courses, subluxation of the glenohumeral joint is not reduced long-term.40 Similarly, low-frequency stimulation of the medial branch nerves in the lumbar spine has decreased low back pain in patients who have failed conservative therapies.41,42 Increasingly, there is an understanding that the multifidus muscle plays a vital role in lumbar stability, and restoring function and decreasing inhibition of this muscle in chronic pain states can be achieved with motor stimulation.43 In a recent randomized, sham-controlled, double-blinded trial, patients in the treatment group received a stimulation frequency of 20 Hz, a pulse width of 214 µs, with participant-specific pulse amplitudes to elicit multifidus contractions for 10 seconds twice per minute during the stimulation session.
Mid-Range Stimulation
Mid-range stimulation (20–100 Hz) has traditionally been the therapy window for PNS devices, as this range preferentially targets afferent fibers, giving the patient a perception of paresthesia or vibration. This stimulation range primarily activates large diameter Aα/β fibers while avoiding activating small-diameter nociceptive fibers (C and Ad).36 Recent studies on paresthesia-based, sensory peripheral stimulation have explored waveform parameters. In 2016, Deer et al conducted a prospective, multicenter, randomized, double-blinded, partial crossover study on a permanent PNS system. The typical settings used in this study included a pulse width of 200 µs, a pulse frequency of 100 Hz, and an amplitude set to induce paresthesia.31 A prospective precursor study by Wilson et al involving eight patients examined PNS targeting the median nerve. The study used lower frequency settings, including amplitude (≤ 80 mA), pulse width (100 to 300 µs), and pulse frequency (20 to 45 Hz). Patients in this study reported experiencing paresthesia in the hand or distribution of the median nerve during the stimulation.44
High-Frequency and Ultra High-Frequency Stimulation
High-frequency (>1500 Hz) and ultra-high-frequency (>500,000 Hz) therapies are still under investigation. Because of their association with pain relief and the absence of paresthesia, it is of great interest to some investigators. Early data on high-frequency stimulation (5000–1000 Hz) in lower extremity amputees has been promising.45,46 Additionally, a recent study by Abd-Elsayed and Moghim demonstrated the effectiveness of high-frequency peripheral nerve stimulation (PNS) in treating chronic pain.34 The study involved 57 patients who received PNS treatment across various nerve targets. The results indicated successful pain management even 24 months post-procedure, in addition to a reduction in opioid medication. The treatment parameters included a pulse width of 32 us and a frequency of 1499 kHz, with varying amplitudes in on/off patterns. However, further research is needed to compare the benefits of these waveforms against other options.
Advanced Programming and Evolving Technologies
An analysis of nearly 84,000 PNS programs for over 5,300 patients from one device company indicates that lower frequencies (<100Hz) may not be typical for most patients using their device. Like SCS systems, complex programming was deemed correlated with long-term PNS success in this analysis, with parameters including pulse widths of ≥500 µs and frequencies ≥500 Hz. Over 96% of the analysis’s commercial and ongoing RCT PNS programs utilized this approach. Notably, 58% utilized multi-area programming, and 39% employed frequencies ≥1,000 Hz. These findings highlight the need for PNS devices to offer diverse programming options to accommodate patient and nerve target variations. (Data Source: Nalu Medical). While this analysis was not designed to evaluate the efficacy of lower frequency parameters, it does indicate an ongoing reevaluation and evolution of advanced programming parameters and waveforms for PNS.
Consensus Guideline 2: Low and mid-range frequency settings can be utilized for motor, sensory, parasympathetic, and sympathetic stimulation, respectively, and are well-studied in the literature. High and ultra-high frequency and high pulse width stimulation have each been shown to be associated with promising outcomes and should be the focus of further research.
Definition: Peripheral Nerve Stimulation
It is crucial to differentiate direct Peripheral Nerve Stimulation (PNS), the focus of this paper, from the starkly different indirect Peripheral Nerve Field Stimulation (PNfS), indirect Percutaneous Electrical Nerve Stimulation (PENS), and Transcutaneous Electrical Nerve Stimulation (TENS) for clarity in clinical practice, alignment of understanding, and interpretation of evolving research.33 PNS directly stimulates specific nerves and requires specialized knowledge of peripheral nervous system anatomy for successful lead placement using image guidance (fluoroscopy or ultrasound) and advanced procedural, often surgical, skills to avoid lead fracture and migration.
PNfS involves placing leads in subcutaneous tissues to diffuse stimulation across the painful loci, enhancing blood flow, blocking cell depolarization, and raising the nociceptive threshold.47 PENS temporarily stimulates subcutaneous nerves. TENS relieves pain through skin electrodes without specific nerve stimulation.48 Payors must differentiate PNS as a unique modality from these other nonspecific stimulation treatments, as this is delineated in the existing peer-reviewed evidence base.
Consensus Guideline 3: PNS should be clearly differentiated in payor policies from the divergent and unrelated therapies of peripheral nerve field stimulation (PNfS), indirect percutaneous electrical stimulation (PENS), and transcutaneous electrical nerve stimulation (TENS). Peer-reviewed literature has extensively differentiated PNS from these treatments.
Magnetic Nerve Stimulation
Magnetic fields (MFs) have been suggested as a potential treatment option for generalized myofascial pain syndromes and rheumatoid arthritis.49 In their review, Fan et al examined 28 studies exploring the analgesic effects of static magnetic fields (SMFs) on humans and mice.50 Findings indicate that 64% of human and all mice studies reported positive effects of SMFs on pain relief, with factors such as SMF intensity, treatment duration, and pain type influencing outcomes. SMFs are not considered a form of PNS.
Magnetic peripheral nerve stimulation (mPNS), on the other hand, is FDA-approved to treat chronic and intractable post-traumatic and post-surgical pain.51 mPNS consists of applying biphasic, time-varying magnetic pulses at a frequency of 0.5 Hz to induce electrical fields in the nerve bundles in the center of the waveform. These pulses generate action potentials in the ascending and descending pathways of the peripheral and central nervous systems.36 The recruitment ratio of A-beta (sensory) to A-delta (pain fibers) is 3:1 with traditional PNS, whereas it is 9:1 with mPNS.51 Kapural et al randomized 65 subjects to mPNS vs conventional medical management (CMM) and observed that 71% of subjects had at least 50% pain relief in the mPNS as opposed to 13% in the CMM arm.
Strategies for Peripheral Nerve Stimulation
Nerve Blocks
A single shot low volume (3–5 mL) local anesthetic nerve block using 2% lidocaine or 0.5% bupivacaine before PNS may be used to isolate a neural target. It may also help to assess patient anatomy and identify the optimal stimulation target nerve if multiple nerves are innervating the dermatome. For example, the scrotum or testicular region is innervated by pudendal, ilioinguinal, genitofemoral, and posterior femoral cutaneous nerves. If a block is not performed, the dermatomal innervation is determined via clinical evaluation, specifically history and physical examination, when selecting a nerve target for PNS. A recent review evaluating diagnostic blocks and PNS outcomes at 3 and 6 months found no outcome difference when nerve blocks were performed before the PNS implant.52 This may be due to the differences in mechanism of action as local anesthetic reversibly binds to Na+ channels while stimulation activates motor or sensory fibers.53,54 However, no definitive mechanistic evidence exists to explain the lack of predictive value of nerve blocks for PNS.
Consensus Guideline 4: While nerve blocks may be utilized in the early diagnostic and therapeutic phases of patient care, the literature does not support their prognostic value in predicting response to a PNS trial.
Short Term PNS
In 2018, a single and dual lead peripheral nerve stimulation system was FDA-approved as indwelling therapy for up to 60 days for pain control. The system consists of a percutaneous electrode (micro lead- flexible, helically coiled) placed in proximity to the target peripheral nerve and connected to a wearable external pulse generator (www.accessdata.fda.gov/cdrh_docs/pdf18/K181422.pdf). This 60-day therapy is intended to supplant the “conventional trial followed by permanent implantation” approach. Many studies demonstrate continued pain reduction and clinical improvement beyond the 60 days of percutaneous stimulation treatment.55,56
Trial and Permanent Implantation of PNS
Permanent PNS systems are similar to SCS in that patients undergo a temporary trial, typically about one week, followed by a permanent implant if the trial is successful. Patients with chronic pain due to peripheral neuropathies often undergo targeted peripheral nerve blocks to help identify the stimulation target before a temporary PNS trial is performed, whereby a percutaneous lead is placed near the targeted nerve. A permanent system is implanted after a trial period of device utilization if the patient experiences satisfactory relief (>50% improvement in pain). Various nuances between device manufacturers dictate modifications to device placement for permanent implantation.
Technology and Device Design
Lead Design
The design of peripheral nerve stimulation (PNS) leads has evolved to optimize efficacy, durability, and patient comfort. Modern PNS leads encompass several key design elements to enhance performance and patient outcomes. A few crucial aspects are lead size, shape, and profile. Traditional designs often featured cylindrical leads with multiple contacts incorporated into the body of the lead. Still, newer iterations employ innovations such as open helical-coil designs with barbed singular contacts at the end of the lead. This has offered the advantage of lower infection rates (0.03 vs 0.83 per 1000 indwelling days for coiled vs non-coiled leads),57 due to several factors including a small skin-to-lead interface (0.3mm diameter), the ability of the lead to expand and compress in response to movement of the body part in which it is implanted, and fibrotic ingrowth into the coil potentially creating a bacteriostatic seal albeit with the qualifier that these coiled leads are intended for 60-day placement, not permanent implantation.58
These monopolar leads differ significantly from traditional multiple-contact arrays. When combined with a relatively narrow pulse width, the former allows for remote placement of the stimulating contact away from the target nerve to better select for A-beta fiber activation.59 The latter allows for more complex stimulation patterns using bipoles and guarded cathode configurations. This has implications for the placement of the lead relative to the target nerve, accommodating both perpendicular and parallel implant orientations.
Lead anchoring mechanisms are pivotal in maintaining lead stability and minimizing migration, one of the most common complications of early peripheral nerve stimulator implants. Recent innovations include anchoring sleeves or cuffs designed to secure the lead within surrounding tissues, reducing the likelihood of displacement.60 Additionally, lead fixation techniques utilizing barbs or tines enhance anchoring for permanently implanted devices without compromising flexibility or patient comfort.61 These features reduce or eliminate the need for separate anchors in many instances. However, granulation around the tines makes removal difficult in some cases and may lend toward lead fracture during explant. Non-tined leads are invariably used for peripheral nerve stimulation trials due to their ease of withdrawal. New technology allows for injectable electrodes composed of an in-body curing polymer/metal composite, though still in the early stages of human testing.62 Newer revisions of the technology utilize a platinum-iridium microwire rather than a curing polymer to facilitate explantation.63
Integration of wireless communication capabilities represents a cutting-edge innovation in PNS lead design. By incorporating a receiver into the body of the stimulator array, wireless-enabled leads eliminate the need for percutaneous extensions and physically connected external pulse generators, offering flexibility and convenience for patients in respect to implant burden. Uncoupled external batteries with internally implanted generators are another strategy (See Figure 2).
 |
Figure 2 Commercially Available PNS Systems Examples of commercially available PNS leads and associated hardware. |
Commercially available, permanent systems include Nalu Medical (Carlsbad, CA), StimRouter (Bioventus, Durham, NC), and Curonix (Pompano, FL). These systems have FDA approval for pain management in adults with severe, intractable chronic pain of peripheral nerve origin.33 The StimRouter system has a receiver, electrodes, and anchoring mechanism (in the form of tines), which is implanted via a test probe using image guidance. The lead is 15 cm long, 1.2 mm in diameter, and has three stimulating electrodes. The lead is powered by an external pulse transmitter and controlled by a patient programmer (a handheld remote-control device).31
The Nalu system consists of a lead with electrodes (4 or 8 contacts, tined or untined) and a battery-free miniaturized implantable pulse generator (micro-IPG) that can accommodate one or two leads. It is powered wirelessly by an external therapy disc and controlled with a smartphone app (Nalu-Product-Catalog-MKT-400005-Rev-A.pdf). An advantage of the Nalu system is the implantation of a micro internal pulse generator and the ability to communicate bi-directionally with the internal device. The Curonix Freedom® Peripheral Nerve Stimulator (PNS) System (curonix.com) has an implanted electrode array (4 or 8 contacts), an implanted receiver, an external transmitter assembly, and a wearable accessory. The system is comprised of a two-component implant that the physician connects during the procedure. As with other implanted PNS, the physician must also create a pocket for the Curonix system. The Curonix implanted receiver is a coiled wire that is connected to the implanted lead. The system is fully programmable and powered by high-frequency electromagnetic coupling (HF-EMC). The HF-EMC technology delivers power and data at significant range and depth into the body. HF-EMC also accommodates individual patient wearable needs by maintaining power to the system through clothing without jeopardizing connectivity. StimRouter lacks a trial option among these systems, whereas Nalu Medical and Curonix offer trial capability. A trial can assist in appropriately selecting patients and introducing them to the therapy’s process. A permanent implant can be considered if patients experience satisfactory pain relief during the trial period.33 Additionally, many payors mandate a trial before permanent implantation.
Pulse Generation
Generator technology has evolved significantly in the past decade. Several generator options are now specific to PNS, including traditional implantable, external, and hybrid decoupled systems. Traditional implantable internal pulse generators (IPGs) rely on a hardwired connection between lead(s) and IPG through a ported interface and historically represent the majority of PNS use. Previously, spinal cord stimulator (SCS) IPGs were adapted for use with PNS; however, due to their large size, they were not ideally suited to the periphery. More recently, externally powered and hybrid decoupled systems were introduced, thus decreasing the size of surgical implants. There are three types of externally powered systems that are commercially available. One, the first described by Yu et al,64 consists of partially implanted leads ported to an external generator.
In contrast, the second, as described by Abd-Elsayed and Moghim,34 is composed of a fully implanted lead with a receiver wire that communicates with a rechargeable generator attached to a transmitting antenna via high-frequency electromagnetic coupling technology. The third of these systems features a fully implanted lead with an integrated receiver that communicates via elective field conduction with an external generator, as described by Deer and colleagues in 2010.44 Finally, a hybrid system featuring fully implanted lead arrays directly ported to a micro-IPG decoupled from an external battery, as detailed by Kalia et al,65 features near-field magnetic induction delivering power from the external battery to the IPG.
Consensus Guideline 5: Given the wide variability between implantable, external, and hybrid decoupled PNS systems, as well as the rapid pace of innovation in the field, payor policies should defer to shared medical decision making by the treating physician and patient to maximize patient satisfaction, safety and efficacy across diverse clinical scenarios when selecting a PNS platform.
MRI Conditionality
Patients with chronic pain may require advanced imaging for a multitude of reasons. Magnetic resonance imaging (MRI) is limited due to foreign ferromagnetic materials in the body of PNS components. The current PNS landscape is rich with various device options, each with its limitations regarding MRI. These limitations can be summarized here but may depend on specific details such as lead location, number of leads, and IPG type, given the extensive testing required to deem each configuration MRI conditional (Table 3). MRI conditionality of PNS components is rapidly evolving, and clinicians are encouraged to regularly review updates from device manufacturers to determine the exact compatibility of particular device components.
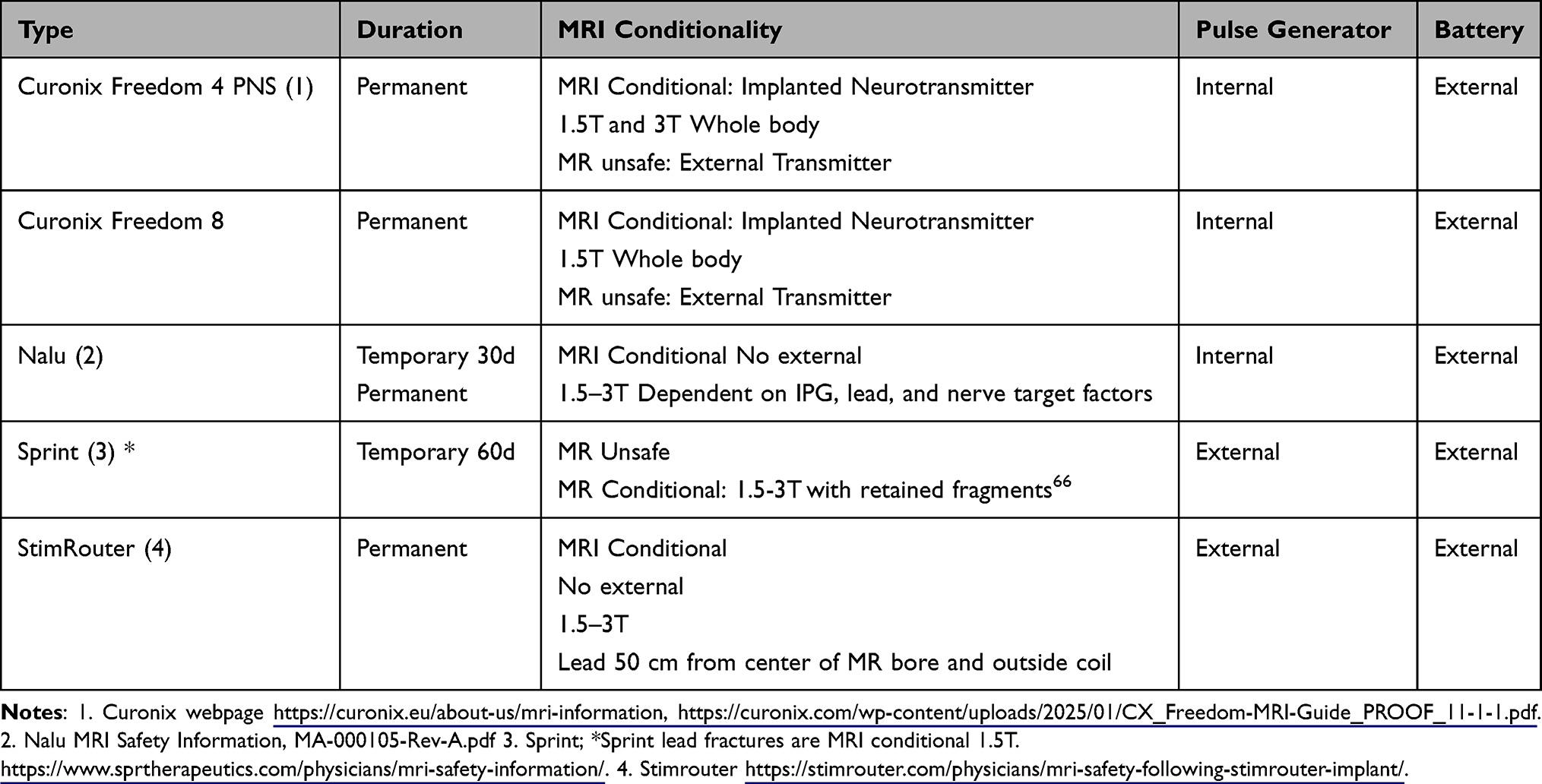 |
Table 3 MRI Conditionality |
Consensus Guideline 6: MRI conditionality, and the variability and complexity of determining MRI implications in the setting of various devices, lead targets, orientation and patient factors, results in the requirement for physicians to consider MRI implications in partnership with the patient when selecting a PNS platform.
Technique Overview
Peripheral nerve stimulator (PNS) lead placement may be performed under ultrasound,67–69 or fluoroscopic guidance.70–73 Ultrasound offers the advantage of directly visualizing the neural target and surrounding vasculature using an in-plane needle technique. However, the operator must be proficient in the basic principles of ultrasound, including velocity of propagation, attenuation, frequency, acoustic shadowing, angle of incidence, and relevant anatomy.74 A fluoroscopic-guided approach is reasonable when targeting nerves that reside in predictable, replicable locations along osseous targets. Imaging modalities may be combined for educational value, future reference for programming, to replicate lead placement for permanent implants, or as a guide for future revision procedures.
Ultrasound guidance is recommended whenever possible for brachial plexus (and its branches), axillary, suprascapular, median, ulnar, radial, intercostal, femoral, lateral femoral cutaneous, saphenous, sciatic, tibial, and common peroneal nerve lead placement.75,76 Nerves that are commonly targeted using fluoroscopic guidance include medial branch nerves (cervical, thoracic, and lumbar), cluneal (superior and medial), genicular,77 infrapatellar saphenous, and in some cases, suprascapular nerve. Multiple cadaveric studies have shown a predictable location for these nerves relative to bony landmarks with minimal risk for vascular trauma when utilizing fluoroscopic guidance.78,79 Ultrasound has also been used effectively for these targets.69,80
When utilizing ultrasound, the skin entry should be at least 2 cm to 4 cm distal to the probe to ensure adequate lead length implanted to mitigate the risk of lead migration. The trajectory of the stimulating probe should violate as few muscles as possible to reach the nerve, and intraoperative sensory or motor testing should be performed before lead securement. Patients may describe sensory stimulation as pressure, tingling, tapping, or buzzing. Cases of uncomfortable or overly intense sensory stimulation that cannot be resolved with decreased amplitude may be solved by moving the lead contacts further away from the targeted nerve. If unintentional motor contraction is noted when approaching a sensory nerve, the stimulating probe is likely intramuscular and should be repositioned. When implanting at a motor target, contraction can be visualized on ultrasound, and needle movement due to contraction is noted.
Monopolar systems disburse energy in a field, allowing for placement to be parallel or perpendicular to the nerve, whereas bipolar systems are optimally placed parallel to the nerve. If a simple bi-pole program does not provide an adequate field of stimulation, a guarded cathode configuration may be programmed to capture a larger area. A low-frequency program (12–30 hertz) will provide motor activation, whereas a higher frequency (≥100 hertz) will provide sensory activation. The decision to place a single or dual lead is influenced by the site of service (hospital outpatient versus ambulatory surgery center), the number of dermatomes/nerves involved in pain transmission, and the size of the target nerve. When placing leads near large, mobile joints, care must be taken not to cross the joint line to mitigate the risk of lead fracture.
Consensus Guideline 7: Most PNS anatomic targets can be easily identified and accessed using ultrasound or fluoroscopic guidance while some targets may be preferentially identified using one modality or the other. Multiple factors including equipment availability and physician preference with imaging modalities may dictate an optimal approach for each case. Thus, payor policies should be inclusive of multiple approaches permitting physician selection of appropriate imaging guidance during PNS placement.
Anesthetic for Trial and Implant and Sensory Testing
The approach to PNS implants varies based on the targeted nerve, imaging modality, and preferred position (Table 4). Intraoperative testing is an essential tool in ensuring proximity to the target nerve. It is recommended to avoid injection of local anesthetic deep and proximal to the target nerve until sensory and/or motor testing is completed. Every manufacturer has a different testing paradigm, but the principle is the same: if neural activation is seen in a relatively low amplitude or predefined stimulation setting, the lead may be too close or intraneural and should be withdrawn. If the energy required to activate the nerve is high, the electrode should be advanced closer to the nerve. SPR Therapeutics recommends lead placement approximately 1 cm distal to the target nerve for robust activation of A-beta fibers. SPR also defines their ideal stimulation window between an intensity of 20–70 on their programmer. Nalu, Bioventus, Curonix, and other manufacturers conduct testing in milliamps with an optimal stimulation window between 0.5–2.0 mA.
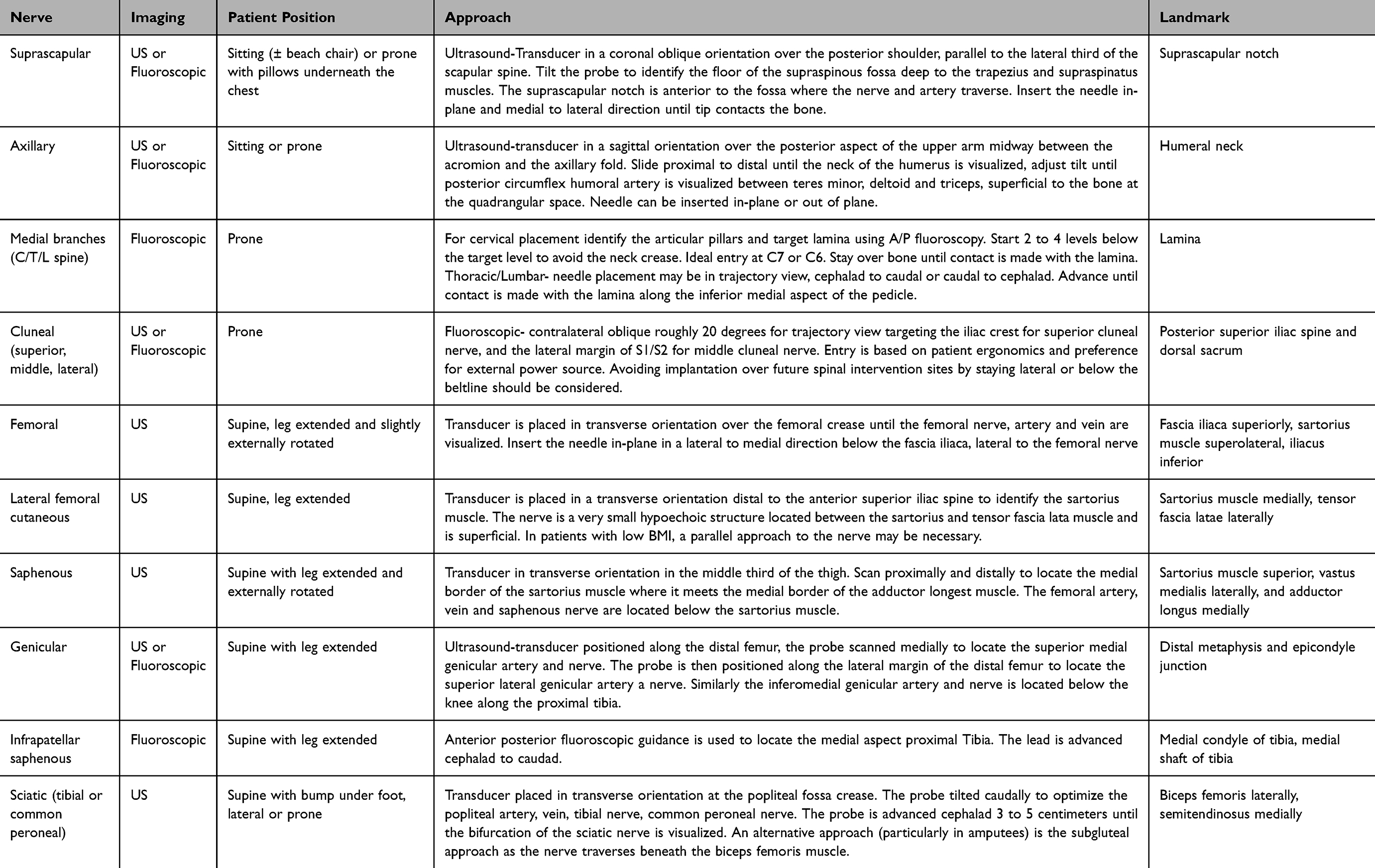 |
Table 4 Recommended Approach by Nerve Target |
Most permanent PNS leads have tines to mitigate the risk of lead migration. It is essential to ensure satisfactory sensory and/or motor testing before deploying the tined portion of the lead. Due to this requirement, the PNS trial should be completed with local anesthetic and, at most, light sedation so that patients can provide feedback about stimulation efficacy. For implant, monitored anesthesia care can be considered with a period of light sedation for lead placement to confirm correct neural identification and appropriate target stimulation. Lower-concentration local anesthetic containing epinephrine can help avoid dense sensory block while providing hemostasis.
Nerve Regeneration and Low-Frequency Stimulation
Electrical stimulation (ES) of the peripheral nerves has been shown in animal models to improve axonal regeneration, myelination, and target reinnervation. The ES is conducted in a retrograde fashion to the soma of the neuron, which upregulates multiple genes associated with regeneration81,82 (Figure 3). The pro-regenerative effect of ES has also been shown in 4 human randomized clinical trials, including severe carpal tunnel syndrome, repair of injured digital nerves, spinal accessory nerve traction injury, and severe cubital tunnel syndrome.83–85 ES has also shown benefits in nerve transection and repair models, in isograft nerve repairs, traction injuries, and chronic compression injuries.83,84,86–88 Initial animal studies found that brief electrical stimulation consisting of stimulation at 20 Hz for 1 hour was superior to higher frequency and/or longer duration in improving sensorimotor regeneration.89–93 Recent clinical studies in humans suggest that 10 minutes of ES is as effective as 1 hour of stimulation for nerve regeneration.81,86,88 Sequential ES may be superior to single-session ES for motor recovery, based on rat models.94
 |
Figure 3 Nerve Regeneration Electrical stimulation proximal to the injury site stimulates the upregulation of RAG through a calcium-dependent mechanism. Increased expression of BDNF and trkB drives increased expression of cAMP which activates CREB to maximize the pro-regenerative axon phenotype, stimulating axonal sprouting and neuron survival. Abbreviations: BDNF, brain derived neurotrophic factor; cAMP, cyclic adenosine monophosphate; CREB, cAMP response element binding protein; trkB, tyrosine receptor kinase B; pKA, phosphokinase A; GAP-43, growth-associated protein; MAPK, mitogen-activated protein kinase. Notes: Reprinted from Juckett L, Saffari TM, Ormseth B, Senger JL, Moore AM. The effect of electrical stimulation on nerve regeneration following peripheral nerve injury. Biomolecules. 2022;12(12). Creative Commons.81 |
Nerve Targets And Conditions
Efficacy of PNS
Multiple well-designed studies have explored the efficacy of PNS across a wide range of nerve targets and indications. The COMFORT randomized controlled trial consisted of two arms: patients in the active arm receiving PNS and conventional medical management (CMM) and patients in the control arm receiving CMM alone.95 Pain target areas included the shoulder, low back, knee, and foot/ankle. At 12 months, 87% of patients in the active arm had at least 50% pain relief, with the average pain relief being 69%, compared to the control arm, which had a responder rate of 3%, with average pain relief being 6% (Level 1, Grade A).
The confirmatory randomized controlled COMFORT 2 Trial used an identical protocol to allow for pooling of data between the two studies.96 Similar results were seen at 3 months in the COMFORT 2 subjects, with the active PNS group achieving an 80% responder rate (≥50% pain relief) and a 66% average pain reduction, compared to a 4% responder rate and 3% pain reduction in the control group receiving conventional medical management alone. These significant outcomes were sustained at 6 months, with the active arm maintaining a 79% responder rate and 64% pain relief (Level 1, Grade A).
Pooled data analysis of 250 subjects from the COMFORT and COMFORT 2 trials demonstrated a significant difference between the treatment groups at 3 months.96 The active arm, receiving peripheral nerve stimulation, had an 81% responder rate with a 66% average pain reduction, compared to the control arm’s 4% responder rate and 4% pain reduction (p<0.001). These benefits proved to be durable, as the active arm maintained an 82% responder rate and 66% pain relief at the 6-month follow-up with 33% having at least 80% pain relief. Responder rates and pain relief were robust at the 6-month follow-up across the four treatment areas, low back, knee, foot/ankle, and shoulder, all with a strong safety profile (Level 1, Grade A).
Huntoon et al published a retrospective review of 6,160 patients following 60-day PNS.55 Seventy-one percent of patients (4,348/6,160) were responders with ≥ 50% pain relief and/or improvement in quality of life. Pain relief among responders averaged 63%. There were 38 different nerve targets within the population, and the responder rate and percent pain relief were relatively consistent across the multitude of pain indications and nerves (Level II-2, Grade A).
Consensus Guideline 8: The evidence for PNS independent of nerve target or pain indication is strong. Due to the broad array of studies, including randomized controlled trials and large retrospective studies in addition to smaller, more focused studies, the overall evidence is Level 1, Grade A. It is important to note that responder rate and average pain relief are clinically significant and consistent across a variety of pain indications and nerve targets including within studies that examined multiple targets.
Upper Extremity
Shoulder pain is the third most common musculoskeletal complaint,97 with a median prevalence of 16% globally.98 Innervation of the shoulder is predominantly from the axillary and suprascapular nerves, with a small contribution from the lateral pectoral nerve.99 Image guidance with either fluoroscopy or ultrasound can be used to target the suprascapular nerve deep to the transverse scapular ligament in the suprascapular notch or inferior to the spine of the scapula as it exits from the spinoglenoid notch. The axillary nerve can be targeted at the quadrangular space with ultrasound or via fluoroscopy at the posterior lateral aspect of the surgical neck of the humerus.99 There have been two randomized control trials for PNS of the shoulder, and both used a temporary PNS system to treat the axillary nerve with low-frequency motor stimulation at 12Hz in patients with post-stroke shoulder pain. Compared to the control group, the PNS groups showed clinically significant sustained pain relief at 3–12 months. There is Level 1 Grade B evidence for PNS for treatment of post-stroke shoulder pain.8,39,76,100,101
There are various observational studies, case reports/series for PNS for other upper extremity pain syndromes such as mononeuropathy, brachial plexopathy, complex regional pain syndrome, acute post-operative pain, and other shoulder pathologies (impingement syndrome, adhesive capsulitis, primary osteoarthritis, post-operative shoulder pain) – demonstrating modest to moderate pain relief, Level II-2 Grade B evidence.8,102–106 Ultrasound is conventionally used to place PNS at target nerves of the upper extremity to avoid neurovascular damage. The COMFORT and COMFORT 2 RCTs demonstrated efficacy and safety for shoulder pain with a pooled 6-month responder rate of 74% and pain relief of 62% (p<0.001).95,96 (Level 1, Grade A)
Craniofacial Nerve Targets
The most common targets for craniofacial neuromodulation include the occipital nerve, supraorbital, and infraorbital branches of the trigeminal nerve, the supratrochlear nerve, the sphenopalatine ganglion (SPG), and the auriculotemporal nerve (Table 5). PNS may be utilized to manage chronic neuropathic facial pain and headache disorders. Given the limited tissue real estate and mobility of the craniofacial region, there may be an increased risk of skin erosion and increased lead migration or fracture, and an implanted pulse generator is often placed at the infraclavicular region.107 Previous consensus recommendations support the consideration of neuromodulation for chronic craniofacial pain syndromes before long-term, long-acting opioid therapy107,108(Table 6).
 |
Table 5 Common Craniofacial PNS Targets and Indications |
 |
Table 6 Quality of Evidence by Indication |
Occipital Nerves
Occipital PNS has been employed to treat primary headache disorders, such as occipital neuralgia, cluster, paroxysmal hemicrania, and migraines refractory to conventional medical management.108 Traditionally, lead placement at the nuchal line using landmark or fluoroscopic techniques has been implemented to target the occipital nerve; however, advancements in high-resolution ultrasound have facilitated targeting the greater occipital nerve in the upper neck at C2.109 The summarized results of several randomized clinical studies investigating the safety and efficacy of occipital nerve stimulation for chronic headache management indicate positive outcomes.110–115 There is high-quality evidence for PNS of the occipital nerves for chronic migraines and low-quality evidence for occipital neuralgia, tension headaches, and cluster headaches.116
Trigeminal Nerve
PNS of the trigeminal nerve to treat craniofacial pain most commonly involves targeting terminal sensory branches such as the supraorbital, infraorbital, supratrochlear, and the auriculotemporal nerves.107 There is low-quality evidence for supraorbital and supratrochlear nerve stimulation for trigeminal neuropathic pain or other craniofacial pain syndromes, with a few clinical studies reporting limited benefit.117–120 Low-quality evidence recommends infraorbital stimulation for trigeminal neuropathic pain and craniofacial pain, with three observational studies describing positive outcomes.116 Limited evidence supports the use of auriculotemporal PNS for treating refractory head and jaw pain.117,121–124
Sphenopalatine Ganglion
The SPG is theorized to exert a pivotal role in the genesis of trigeminal autonomic cephalalgia, cluster headache, and paroxysmal hemicranias.125,126 There is limited evidence to support the use of SPG neurostimulation in chronic craniofacial pain, with only one randomized controlled study and a few case series.127–129 There is sparse literature to recommend SPG neuromodulation in idiopathic facial pain, trigeminal neuralgia, and paroxysmal hemicrania. Still, SPG neuromodulation combined with trigeminal PNS may play a role in treating cluster headaches in selected cases.108,126,130 The evidence remains limited but promising for cluster headaches based on results from one high-quality study.128,131
Pudendal Nerve
The pudendal nerve originates from the second, third, and fourth sacral nerve roots and provides sensation to the anus, perineum, and genitals.132,133 Urologists have utilized peripheral nerve stimulation (PNS) targeting the pudendal and sacral nerves for treatment of voiding dysfunction and interstitial cystitis associated chronic pelvic pain for over a decade - Level I evidence, Grade B recommendation.134–137 These devices have been traditionally implanted through an ischial-rectal approach. Recently, pudendal nerve stimulation has been proposed as a means for the management of chronic pelvic pain in the field of pain medicine. Both ultrasound-guided and fluoroscopic-guided techniques have been proposed to minimize the risks of neurovascular injury, but large randomized control trials assessing efficacy and safety are lacking.138,139 Pudendal nerve PNS for chronic pelvic pain is Level II-3 evidence, Grade C recommendation.
Transverse Abdominal Plane (TAP)
The transverse abdominal plane (TAP) is located between the transversus abdominis and internal oblique muscles,140 and contains the thoracoabdominal nerves (arising from the seventh to eleventh intercostal, subcostal and first lumbar nerves)141 and ilioinguinal and iliohypogastric nerves in the lower abdominal quadrants.142 The thoracoabdominal nerves have been implicated as providing somatic sensation to the abdominal wall (between the T5-T12 dermatome).143 As such, nerves within the TAP have been targeted by nerve blocks to treat chronic somatic and neuropathic abdominal pain.144–147 Similarly, the ilioinguinal and iliohypogastric nerves have been targeted in the past for nerve blocks to treat somatic and neuropathic pain after inguinal herniorrhaphy.142 Recently, utilization of a percutaneous, ultrasound-guided technique has been explored to place peripheral nerve stimulation leads in this region for the management of chronic abdominal pain. However, further investigation is needed to validate the safety and efficacy of this modality.2 (Level II-3 evidence, Grade C)
Low Back Pain
When considering modern PNS devices, chronic low back pain is probably the most well-studied PNS indication in the literature. Permanent devices targeting the multifidus muscle directly at the lumbar spine provide functional improvement in disability and prolonged pain relief in 5-year, longitudinal randomized trial data, Level I-A, Grade A.148 Furthermore, a direct target of the medial branch nerves innervating the multifidus muscle with temporary 60-day systems has shown efficacy beyond the treatment time. Prospective data supports that 60-day PNS treatment may lead to 12 months of 30–50% pain relief in patients with and without a previous thermal ablation.149,150 Current literature suggests Level I-B, Grade B moderate evidence for PNS and low back pain syndromes, primarily related to heterogenicity of technique, device, and study population.151 In a health economic study, PNS provides significant cost savings compared to conventional interventional therapies for chronic low back pain over a year of treatment.152
Cluneal Nerves
Targeting the cluneal nerves for treating iliolumbar or chronic low back pain syndromes has been described in the literature. The superior and middle cluneal nerves are commonly implicated as pain generators in the lower back, buttock, and posterior thigh distribution and are composed of the cutaneous branches of the lateral dorsal rami branches from T11 to S4.153 Evidence for this target consists of case reports and small series with promising results as well as two robust RCTs.34,95,96,154–156 The cluneal nerve was one of the primary targets within the COMFORT and COMFORT 2 RCTs and demonstrated an 81% responder rate in the pooled cohort.95,96 (Level 1, Grade A)
Intercostal Nerves
The intercostal nerve innervates the skin and muscle of the thorax and part of the abdominal wall.69 These nerves can be targeted for treating rib pain, post-herpetic pain, and postsurgical pain. The neurovascular bundle runs inferior to the rib, deep to the intercostal muscle, and superficial to the pleura at each level. Case reports have shown the potential for this technique, especially for breast cancer treatment-related pain, post-herpetic neuralgia, and abdominal pain.157–159 A case series for treatment of focal mononeuropathy pain with 39 patients revealed that 78% noted improvement in their pain, and patients with intercostal PNS had a 40% improvement in activity.160 A retrospective review of 6,160 patients following 60-day PNS revealed consistent outcomes across a multitude of nerve targets, with a responder rate of 71% of patients having at least 50% pain relief or improvement in quality of life.55 Sub-analysis of 103 patients with intercostal nerve PNS revealed equivalent outcomes. (Level II-3, Grade B)
Ilioinguinal/Iliohypogastric Nerves
Ilioinguinal and Iliohypogastric peripheral nerve stimulation (PNS) for groin pain has been achieved via surgical implantation, ultrasound-guided, and anatomic placement and has been published in multiple case presentations. One surgical implantation of the paddle (iliohypogastric) and percutaneous (ilioinguinal) leads yielded 0/10 pain 1-year post-implantation.161 Another surgical implant (ilioinguinal) reported minimal pain at 3-months.162 Four cases were described in a published series using ultrasound-guided placement (ilioinguinal), of which two were 7-day trials with >85% pain relief.163 Other published cases yielded mixed results: one with >50% relief for 1 year and one without relief at 2 months post-implantation.161,164 Eight cases of anatomic placement (ilioinguinal, iliohypogastric) reported pain reduction by >50%, ranging from 1 month to 2 years.161,165–167 (Level II-3, Grade C)
Genitofemoral Nerve
Genitofemoral PNS for groin pain has also been described via anatomic, ultrasound-guided (USG), and surgical approaches. Three cases of anatomic placement with fluoroscopic confirmation reported 50–75% pain relief ranging from 1 to 5 months post-implantation.166–168 Under USG, one case reported >90% pain relief at 5 months post-op and improved physical functioning on the 12-item Short Form Survey.169 A retroperitoneal surgical approach, named the “sandwich technique”, reported >60% relief before losing efficacy from scar tissue formation and explant at 12 months.161 Finally, one patient with genitofemoral PNS reported 50% relief at 1 year in a randomized control trial of 10 kHz PNS.170 (Level II-3, Grade B)
Meralgia Paresthetica (Lateral Femoral Cutaneous Nerve)
Meralgia paresthetica is characterized by entrapment of the lateral femoral cutaneous nerve, originating from spinal levels L2-3 and often presenting with numbness, dysesthesia, and occasionally pain over the anterior thigh. Evidence is currently limited to case reports and one case series. One case report,171 demonstrated 100% pain reduction using a 60-day temporary stimulator (SPRINT) sustained at 12 months with discontinuation of gabapentin. Another case report,172 described 80% relief at 3 months with a temporary device (SPRINT). One final case series (n=3),160 implanted a permanent peripheral nerve stimulator (Bioness Stimrouter) with an external generator and achieved 100% VAS improvement and 70% activity improvement. More extensive case series are necessary to assess long-term results for meralgia paresthetica PNS. (Level II-3, Grade B)
Lower Extremity (Sciatic, Femoral, Saphenous Nerves)
Peripheral nerve stimulation has been applied to the femoral, sciatic, and saphenous nerves for managing nociceptive and neuropathic postoperative and chronic lower extremity pain. Femoral nerve PNS and sciatic nerve PNS are effective in a sham-controlled RCT managing immediate postoperative pain using temporary lead placement for 14 days and were effective in reducing opioid requirements and pain173 (Level 1, Grade A evidence). Other studies have demonstrated the use of PNS in postoperative pain management, improving recovery times and reducing opioid requirements.105 Femoral nerve PNS is a desirable target nerve for managing postoperative knee pain, particularly post ACL reconstruction.174 Sciatic nerve stimulation has been used for postoperative pain after foot/ankle surgery. Unfortunately, knee and ankle pain can persist beyond the immediate postoperative period. Permanently implanted saphenous nerve stimulation has been used to treat persistent knee pain.175,176 Future studies will help better understand candidates for therapy and long-term success rates. (Level II-3, Grade B evidence)
Knee Pain
Peripheral nerve stimulation for knee pain can include the femoral, saphenous, and genicular nerves. Genicular nerves have long been the target of radiofrequency ablation for knee pain. PNS of the genicular nerves has been used for persistent postoperative knee pain and osteoarthritis in the absence of surgical intervention. A case report,177 of focal knee pain due to osteoarthritis showed successful treatment with temporary PNS of the superomedial genicular nerve and saphenous nerve, but the long-term benefit was not established. Several studies have applied genicular nerve PNS to patients with chronic pain after total knee arthroplasty or patients unable or unwilling to undergo knee replacement; PNS may be considered in temporary form for pain management. Small case series have shown limited success.178 A systematic review,179 identified 7 studies limited to case reports and series that showed improved pain and functionality; however, there was variability in technique workup and included both temporary and permanent devices. The COMFORT and COMFORT 2 RCTs demonstrated a pooled responder rate of 96% for subjects being treated for chronic knee pain.95,96 By convention, lead placement for PNS should not span across a joint due to the risk of lead migration and lead fracture. Both fluoroscopic and ultrasound-based techniques have been used for genicular PNS, targeting the superior medial and superior lateral genicular nerves. Future studies are necessary to help characterize responders and best practice models. (Level I, Grade A evidence)
Ankle/Foot Pain
As with postoperative knee pain management, sciatic nerve PNS is effective in the immediate postoperative period in reducing opioid requirements and pain in a randomized, sham-controlled trial173 (Level I, Grade A evidence). The ease and availability of ultrasound have allowed for better nerve visualization. Commonly targeted nerves for ankle pain include the sural, superficial peroneal, and posterior tibial nerves. Tarsal tunnel syndrome results in tendinous compression of the posterior tibial nerve posterior to the medial malleolus. The superficial peroneal and sural nerves can be injured in ankle fractures and operative intervention.180 In a case series of permanent wireless PNS placement for peripheral neuralgias, one patient was treated successfully with PNS of the sural nerve.167 Limited evidence exists for PNS of the nerves of the ankle. Some evidence suggests the utility of stimulating the sciatic nerve in postoperative pain management for ankle surgery.173 The COMFORT and COMFORT 2 RCTs demonstrated durable benefit for ankle and foot pain with pooled data demonstrating a 75% responder rate and 65% pain relief at 6 months (p<0.001).95,96 (Level 1, Grade A evidence)
Neuropathic Pain
Peripheral neuropathy may be present in up to 12% of the population and as high as 30% in older demographics.181 A retrospective study of PNS for neuropathic pain in 63 patients found that NRS decreased from 7.24 at baseline to 3.43 at 2–3 week follow-up. Among the 24 patients who completed long-term follow-ups of 8 months or longer, 79% had pain relief of ≥50%. PNS for chemotherapy-induced peripheral neuropathy (CIPN) is an area of recent study, and a systematic review found that there is some evidence supporting PNS for CIPN based on a study with 50 subjects182 (Level II-3, Grade B evidence).
Studies evaluating PNS for lower extremity neuropathic pain have focused primarily on mononeuropathies, which is appropriate given the focal nature of PNS treatment. One potential target application is peripheral small fiber neuropathy; however, no studies currently validate PNS for this indication. Spinal cord stimulation has seen wide implementation and innovation, such as variable waveforms and hardware optimization. PNS can experience similar growth as new indications are evaluated and specific nerve targets are explored.183
Complex Regional Pain Syndrome
The literature describing the use of PNS for CRPS encompasses the treatment of both upper and lower extremity CRPS with targets including the sciatic, common peroneal, tibial, femoral, lateral femoral cutaneous, saphenous, radial, median, and ulnar nerves.184 In a case series of 3 patients with CRPS Type I affecting the foot, 60 days of percutaneous PNS therapy applied to the tibial and common peroneal nerves in the popliteal fossa resulted in the resolution of autonomic symptoms. Two of the three patients experienced pain relief for more than 8 months after discontinuing therapy.185 Similarly, in a case series of 11 patients diagnosed with upper or lower extremity CRPS Type 2, all received an implantable PNS system after successfully responding to the trial phase. These patients experienced clinically significant pain reduction after a permanent PNS implant of about 5 points on the Numeric Rating Scale (NRS) of pain.186 In a retrospective chart review of 165 patients receiving surgical PNS implantation for CRPS type 1 or 2 of the upper or lower extremities with paddle-type SCS electrodes to function as PNS, pain scores on the NRS were about 1.9 points lower after 12 months. Concurrently, the percentage of patients receiving opioid therapy decreased from 62% to 41% after 12 months. In addition, 51% of patients reported an improvement in functional status. As 34% of patients in this study required surgical revision, outcomes with modern, dedicated percutaneous PNS systems will likely improve with reduced complication rates.187 In a case series of 14 patients with refractory upper extremity CRPS, 10 received permanent PNS implants at the brachial plexus after a successful trial. At 12-month follow-up, these patients reported a 57.4% improvement in VAS scores and a 60% improvement in neuropathic pain symptoms, similarly demonstrating sustained treatment response to PNS among patients with CRPS.188 Goree et al reported on a randomized, sham-controlled trial of 60-day PNS for post-knee replacement CRPS Type 2.189 Sixty percent of patients in the PNS group had at least 50% pain compared to a 24% response rate in the sham group. Additional randomized clinical trials will further establish the broad application of modern PNS systems in treating CRPS and determine patient and therapy-specific factors associated with positive treatment response. (Level I, Grade B)
Post-Amputation Pain
The ASPN Evidence-Based Clinical Guidelines for the Use of PNS in the Treatment of Chronic Pain recommend that
PNS may be considered for lower-extremity post-amputation pain following the failure of conservative treatment options and is associated with modest to moderate pain relief.8
This recommendation stems in part from an RCT of 28 traumatic lower extremity amputees with post-amputation pain receiving either 8 weeks of percutaneous PNS targeting the femoral and sciatic nerves or 4 weeks of placebo followed by 4 weeks of PNS after crossover. At 12 months, 6 of 9 patients receiving 8 weeks of PNS reported ≥50% reductions in average weekly pain, while 0 of 14 patients in the control group reported a significant reduction in pain after the 4-week placebo period.190 Given the 36% attrition rate from randomization to 12-month follow-up, additional research is needed to replicate these promising findings. In a pilot RCT of 16 veterans undergoing lower extremity amputation who had received femoral and sciatic peripheral nerve catheters, patients were eligible for enrollment if they reported pain scores ≥4 out of 10 in the 24 to 48 hours after catheter removal. Patients were randomized to 60 days of PNS targeting the femoral and sciatic nerves combined with standard medical therapy or standard medical therapy alone. Initial outcomes at 3 months demonstrate greater reductions in phantom limb pain, residual limb pain, and daily opioid consumption among those receiving PNS, signaling a role for PNS in the subacute phase after amputation.191 PNS may serve as an important bridge therapy to prevent the development of persistent pain after amputation and phantom limb pain. (Level I, Grade A)
Consensus Guideline 9: In addition to strong evidence from RCTs and large retrospectives spanning a wide range of indications and nerve targets, focused studies support impactful treatment of a variety of anatomic targets, specific nerves, and specific painful conditions including shoulder (Level 1, Grade A), occipital nerve (Level 1, Grade B), sphenopalatine ganglion (Level 1, Grade C), pudendal nerve (Level 1, Grade B for voiding dysfunction and interstitial cystitis and Level II-3 Grade C for chronic pelvic pain), medial branch nerve (Level 1, Grade A), cluneal nerve (Level 1, Grade A), lower extremity (Level 1, Grade A), knee (Level 1, Grade A), ankle/foot pain (Level 1, Grade A), CRPS (Level 1, Grade B), lateral femoral cutaneous nerve (Level II-3 Grade B) and post-amputation pain (Level 1, Grade A). (See Table 7)
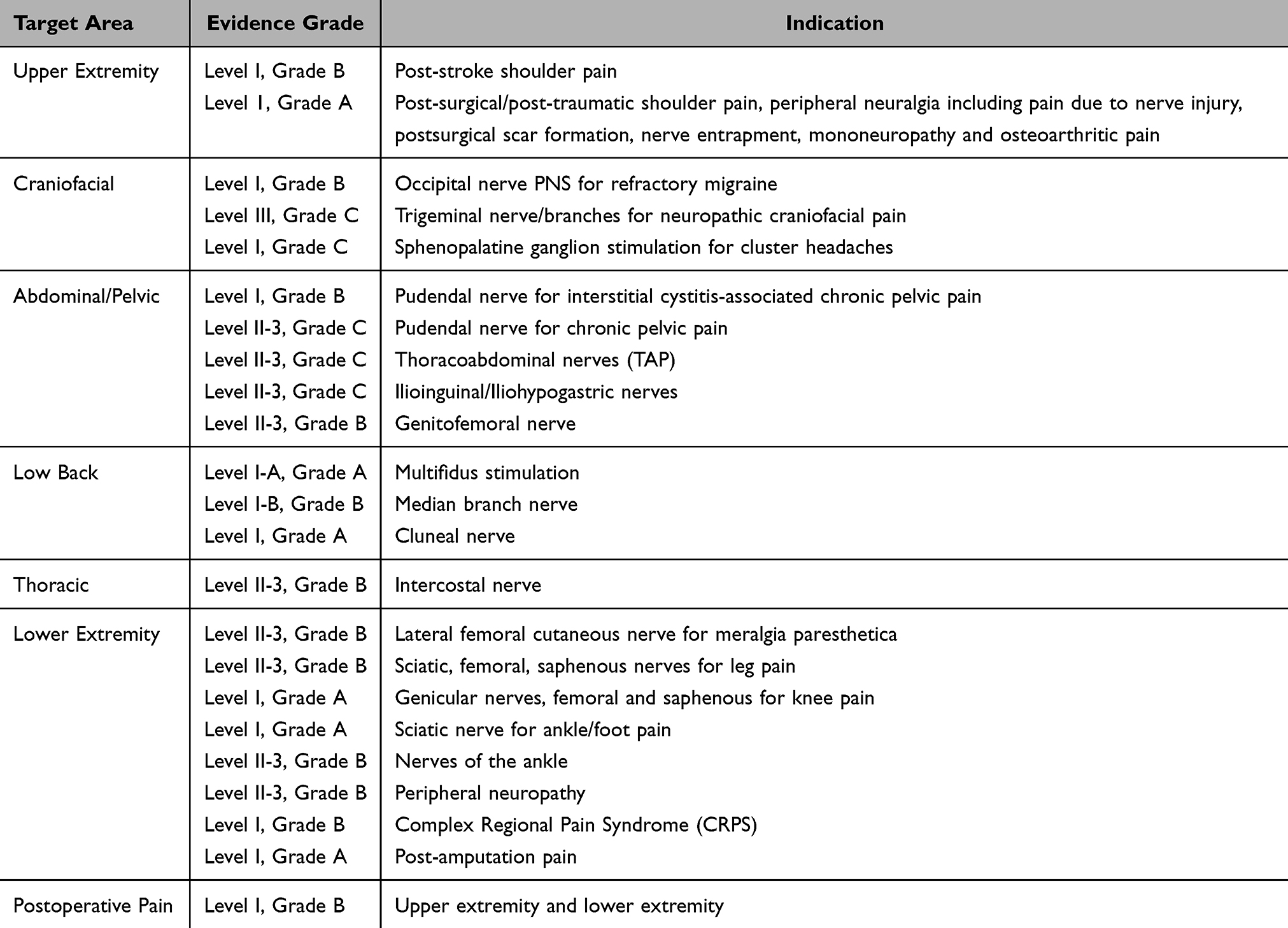 |
Table 7 Level of Evidence by Pain Indication |
Postoperative Pain
While a few small (<20 subjects) randomized proof-of-concept studies have suggested reduced pain and opioid requirements with PNS following various surgical procedures,174,191–193 only one trial prospectively powered to determine efficacy has been published involving postoperative pain.173 Participants undergoing ambulatory surgery were randomized to receive either active stimulation (n=32) or a sham (n=34) for 2 weeks in a double-masked fashion. During the first 7 postoperative days, opioid consumption in participants given active stimulation was a median [IQR] of 5 mg [0, 30] versus 48 mg [25, 90] in patients given sham treatment (P<0.001). During this same period, the average pain intensity measured with a 0–10 numeric rating scale in patients given active stimulation was a mean ± SD of 1.1 ± 1.1 versus 3.1 ± 1.7 in those given sham (P<0.001). No intervention-related adverse events were identified. Perhaps most compelling, participants who received active treatment had far less physical and emotional interference due to pain throughout the day following lead removal as measured with the Brief Pain Inventory (Interference Scale).194 While this technique’s potential benefits include prolonged analgesia duration (up to 60 days currently) and lack of induced motor, sensory, and proprioception block, unit cost and time for lead insertion may be limiting factors.195 (Level I, Grade B)
Consensus Guideline 10: PNS in the post-operative period has demonstrated reduced opioid consumption, pain scores, and physical/emotional interference scores with Level 1 data. PNS is a highly effective treatment in the postoperative period, but payor policies are a restricting factor.
Non-Pain Targets, Rehabilitation, and Motor Strengthening
Posterior Tibial Nerve
Tibial nerve stimulation (TNS) represents an important treatment modality for several urologic and gastrointestinal conditions via parasympathetic nervous system activation. Percutaneous TNS protocols for these indications often involve frequent visits for percutaneous needle placement to receive PNS. TNS applied via transcutaneous devices is an alternative approach. Percutaneous TNS represents a promising alternative to sacral nerve neuromodulation in treating fecal incontinence. In a meta-analysis of 4 RCTS spanning 439 adults with fecal incontinence, percutaneous TNS demonstrated superior efficacy compared to sham electrical stimulation in reducing weekly episodes of fecal incontinence, and a higher proportion of patients receiving percutaneous TNS reported a greater than 50% reduction in weekly fecal incontinence episodes.196 Percutaneous TNS for the treatment of overactive bladder has demonstrated more efficacy in reducing urgency urinary incontinence compared to certain antimuscarinics and results in improved daytime micturition frequency and nocturia frequency comparable to other rehabilitation modalities.197 Still, more research is needed to determine its role in managing overactive bladder compared to more first-line therapies.198 When comparing neuromodulation modalities, including percutaneous/transcutaneous TNS, vaginal electrical stimulation, sacral neuromodulation, parasacral stimulation, pudendal neuromodulation, or placebo in a network meta-analysis of 21 RCTs spanning 1,433 participants with overactive bladder, both percutaneous and transcutaneous TNS were most efficacious for reducing urgency incontinence episodes.199 Additional reported indications for percutaneous TNS include low anterior resection syndrome,200 lower urinary tract symptoms (urgency, frequency, nocturia, urge urinary incontinence) among patients with multiple sclerosis,201 and chronic prostatitis/chronic pelvic pain syndrome.202 (Level I, Grade A evidence)
Vagus Nerve
The ability to modulate activity in the parasympathetic nervous system via the vagus nerve is central in disease management in a wide range of disorders. Through its afferent projections to the brainstem’s nucleus tractus solitarius, which accounts for 80% of its fibers, the vagus nerve regulates brain physiology, chemistry, plasticity, and behavior.203 Several methods of action have been identified with vagus nerve stimulation (VNS), including modulation of neurotransmitters such as glutamate, norepinephrine, and serotonin, modulation of cortical spreading depression and electrical excitability, modulation of the autonomic nervous system, and modulation of inflammatory cytokines.
VNS has been FDA-cleared in the United States for treating epilepsy, major depression, multiple primary headaches, abdominal pain in children, addiction, post-stroke rehabilitation, and painful diabetic neuropathy. A systematic review of transcutaneous VNS for treating epilepsy found that multiple studies showed improved quality of life and that two showed statistically significant reductions in seizure frequency.204 The FDA also granted an EUA for known or suspected COVID-19 and a breakthrough designation for post-traumatic stress disorder. An RCT with 97 randomized COVID patients demonstrated reduced CRP levels in patients receiving non-invasive VNS205 (Level I, Grade B evidence). VNS has also shown promise in inflammatory disorders such as Sjogren’s disease, Rheumatoid Arthritis, and Crohn’s Disease.206 (Level II-3, Grade B evidence) Currently used implantable VNS devices include multiple systems by Livanova (formerly Cyberonics) (Houston, TX) that are used for the treatment of epilepsy207 and depression208 and by MicroTransponder (Austin, TX) that are used for post-stroke rehabilitation.209
Phrenic Nerve
Phrenic nerve stimulation was first introduced in the 1960s as respiratory support for high cervical spinal cord injury and central alveolar hypoventilation syndrome.210 Following initial pilot studies of transvenous phrenic nerve stimulation (TPNS) in central sleep apnea (CSA) and co-morbid heart failure (HF), a large, randomized control trial evidenced long-term safety and efficacy in reducing CSA severity up to 4 years post-implant.211–213 (Level I, Grade B evidence). Later studies demonstrated safety and efficacy in HF patients, including those with implantable electronic devices.214,215 TPNS may be effective in weaning select ventilator-dependent patients; however, this was not substantiated in large, randomized control trials (RESCUE-2, RESCUE-3 NCT03783884).216,217 Currently, the US FDA approves phrenic nerve stimulation using the Avery Mark IV Breathing Pacemaker (Avery Biomedical, Commack, NY) for various indications.218
Hypoglossal Nerve
Hypoglossal nerve stimulation (HNS) evolved after loss of genioglossus muscle tone at sleep onset was linked to pharyngeal obstruction and obstructive sleep apnea (OSA).219,220 An initial 1997 study prompted further feasibility trials of fully implantable systems, confirming airflow dynamics and sleep apnea improvements.221 Following a landmark trial (STAR), HNS obtained Food and Drug Administration (FDA) approval in 2014 as second-line treatment for moderate to severe OSA that is refractory to positive airway pressure (PAP).222,223 Given proper patient selection, HNS has been extensively studied with evidenced effectiveness in reducing аpnеa-hypopnea index (AHI) up to nine years post-implantation.221 (Level I, Grade A evidence)
Occipital Nerve
Luckey et al examined memory in 30 subjects in a double-blind, sham-controlled, randomized trial.224 Half the participants received transcutaneous occipital nerve stimulation, whereas the other half received sham stimulation. Occipital nerve stimulation enhanced memory after just one session, with results lasting 28 days. The proposed mechanism is via the locus-coeruleus-noradrenaline pathway. This study observed changes in alpha-amylase, a noradrenaline biomarker, following occipital nerve stimulation. Additional studies have demonstrated that occipital nerve stimulation can boost the retention of memories when applied around the time of learning by enhancing memory consolidation via this pathway.225,226 (Level I, Grade B evidence)
Trigeminal Nerve
Trigeminal nerve stimulation (TNS) has garnered interest in treating neurologic and psychiatric disorders.227 Initially described in case studies, TNS for drug-resistant epilepsy has been proven safe and effective for up to 12 months.228 Based on the trigeminal nerve projections to the ascending reticular activating system, spinal locus, and cortex, along with a case report of awakening from a coma, TNS has been studied in recovery from traumatic brain injury with modest yet promising results.229 There is evidence to suggest that TNS may improve major depression, attention deficit hyperactivity disorder, and refractory schizophrenia.230–233 One study showed improved olfaction with TNS.234 (Level II-3, Grade B evidence) A recent prospective, double-blind, randomized controlled study evaluated the effect of trigeminal nerve stimulation on cerebral infarction occurrence in patients with aneurysmal subarachnoid hemorrhage. Still, no decrease in the stroke rate was observed secondary to vasospasm occurrence.235
Peroneal Nerve
Since the 1960s, common peroneal nerve stimulation (CPNS) has been investigated for improving post-stroke foot drop; the FDA has approved three distinct external devices.236 Many studies indicate that external and implanted CPNS systems are non-inferior to ankle-foot orthoses (AFO) for foot drop in stroke and gait in multiple sclerosis.237–239 Notably, combined sensory and functional CPNS variations in meta-analyses and a standalone study report contrasting outcomes240–242 (Level I, Grade C evidence). CPNS has also been shown to be safe and effective in improving symptoms of medication-refractory restless leg syndrome (RLS) for up to 6 months, leading to its eventual FDA approval in 2023243 (Level I, Grade A evidence).
Pudendal Nerve
Pudendal nerve stimulation has been described as a treatment for urinary retention.244 Another study demonstrated that daily pudendal nerve stimulation accelerated recovery from stress urinary incontinence.245 Feng et al conducted a parallel design randomized controlled trial with 96 subjects who had undergone radical prostatectomy, allocated as 64 patients in a group receiving pudendal nerve stimulation and 32 receiving pelvic floor muscle training and transanal electrical.246 Treatments were administered three times a week for eight weeks. The efficacy rate of 68.7% in the pudendal nerve stimulation group was nearly double the responder rate of 34.4% in the pelvic floor muscle training group. This indicates that pudendal PNS can almost double the likelihood of regaining urinary continence following radical prostatectomy. The mechanism of action is believed to be that pudendal nerve stimulation simulates pelvic floor muscle training. (Level I, Grade A evidence)
PNS for Sexual Dysfunction
Percutaneous tibial nerve stimulation (TNS) results in improvements related to both male and female sexual dysfunction in patients with overactive bladder, chronic pelvic pain, and nonobstructive retention. Patients report significant improvements in overall satisfaction, libido, and frequency of sexual activity in response to percutaneous TNS.247 In a prospective observational study of 41 women receiving percutaneous TNS for OAB reporting sexual dysfunction, participants reported significant improvements in sexual function independent of urinary symptoms.248 Among female patients with fecal incontinence who had failed to respond to biofeedback, percutaneous TNS resulted in significant improvements in bowel continence, bowel-related quality of life, and bowel-related sexual function, but not dyspareunia.249 A systematic review of PNS across a variety of nerve targets for sexual dysfunction by Jin et al found that male patients experienced an improvement in erectile function, desire, and satisfaction, whereas desire, arousal, orgasm, lubrication, quality of “sex life”, intercourse capability, and dyspareunia improved in female patients.250 (Level II-3, Grade B evidence)
PNS for Tremors and Tics
Peripheral nerve stimulation has demonstrated benefits in treating tremors and tics. Small studies indicated that median and radial nerve stimulation reduced Parkinson’s and essential tremors.251,252 In 2021, the first FDA external stimulator device (Cala kIQ) obtained approval for Parkinson’s disease (action hand tremors) and essential tremors. Though stimulation of the median and radial nerves is proven safe, larger studies report mixed results on efficacy253,254 (Level II-3, Grade C evidence). Among tic spectrum disorders, case reports of Tourette’s syndrome describe improved motor and phonic tics after a vagal nerve stimulator implant.255,256 Two clinical trials of wearable median nerve stimulation (MNS) also evidenced efficacy in improving chronic tic disorder257,258 (Level I, Grade B evidence).
Consensus Guideline 11: A variety of nerve targets have demonstrated efficacy for non-pain applications, including posterior tibial nerve for urological issues (Level 1A), phrenic nerve for central sleep apnea (Level 1B), hypoglossal nerve for obstructive sleep apnea (Level 1A), occipital nerve for memory enhancement (Level 1B), common peroneal nerve for medication refractory restless leg syndrome (Level 1A), pudendal nerve to reduce urinary incontinence following radical prostatectomy (Level 1A), nerve stimulation for migraines, cluster headache, post traumatic stress syndrome, post stroke recovery (Level 1A) among numerous other inflammatory mediated disorders and median nerve for chronic tic disorder (Level 1B). (See Table 8)
 |
Table 8 Level of Evidence by Functional Indication |
Surgical Best Practices
Tined vs Non-Tined and Anchoring
When deciding between tined and non-tined electrodes for peripheral nerve stimulation (PNS), consider anatomical factors and the desired outcome. Tined electrodes are ideal for areas with frequent movement, requiring secure fixation to prevent migration. They are suitable for deep nerve targets or regions prone to lead displacement. Non-tined electrodes are simple to place, may be preferred for superficial nerves or sites with less expected movement, and can be anchored to fascia at the insertion site. Factors such as patient comfort, anticipated duration of therapy, and lead stability should also be considered. Ultimately, the choice between tined and non-tined electrodes should be based on individual patient needs and the specific requirements of the procedure.
Closure
Saline irrigation prior to closure may reduce microbial burden.259 For optimal closure of a peripheral nerve stimulator (PNS) system, use absorbable sutures for deep tissue layers to minimize the risk of irritation and ensure stability. A cut-down should be deep enough to allow for a multi-layer closure to prevent future erosion of any implant material. For superficial skin closure, options range from sub-cuticular absorbable sutures to non-absorbable sutures such as nylon or staples at the dermal-epidermal junction. Close the incision in at least 2–3 layers, ensuring that each layer is adequately approximated to promote proper healing.
Consensus Guideline 12:Best surgical practice for permanent PNS includes strategies to promote optimal wound healing, infection prevention, and prevent lead migration. Effective strategies include saline irrigation prior to closure, a deep enough cut down to allow for multi-layer closure, and closing in at least 2-3 layers when appropriate based on the implanted hardware.
Post-Op Care
Advise patients to avoid bending, lifting, or twisting excessively for the first few weeks. Encourage gentle movement and walking to promote healing. Patients should keep the incision site clean and dry and follow the specific wound care instructions provided. They should immediately report any signs of infection, such as redness, swelling, or drainage. Emphasize the importance of attending the seven-to-ten-day follow-up appointment to monitor the system’s function and make necessary adjustments. Providing clear and comprehensive postoperative care instructions can help ensure optimal outcomes for patients with PNS systems.
Troubleshooting and Complications
Due to the relative novelty of peripheral nerve stimulation, there have not been many publications on troubleshooting PNS systems. Most of the literature centers on sacral neuromodulation when used to treat urogynecological disorders. However, based on the properties of peripheral nerves, we can better understand best practices for troubleshooting PNS systems. One major issue with PNS is an inability to get stimulation to target. While pre-implant diagnostic nerve blocks do not necessarily predict the success of PNS,52 some clinicians may use a peripheral nerve block to determine if the area supplied by the peripheral nerve gets appropriately anesthetized. Suppose the diagnostic block does not provide an appropriate response. This may predict an inability to get the PNS system to respond appropriately to electrical stimulation due to peripheral nerve damage.52
Undesirable motor and painful stimulation are also possible side effects of PNS. They are usually due to being too close to the nerve target, nonspecific stimulation, and/or using higher amplitudes than are required to achieve pain relief. New technologies that are not yet commercially available allow for selective stimulation of sensory and motor nerve fibers,260 but current technology does not allow this yet. Lastly, loss of efficacy can be an issue with PNS, as it is with many technologies. Loss of effectiveness is most commonly due to lead migration,261 with other possible etiologies, including lead fracture, habituation, and scar tissue around the lead contacts. Clinically, patients may also need a stimulation holiday when there is a perceived loss of efficacy, but more literature is required to support this theory.
Complications with PNS are similar to those seen with Spinal Cord Stimulation (SCS). Complications can be divided into hardware-related and biological complications. Hardware complications include lead migration, which can be higher in PNS than in SCS systems.261 Complications almost exclusively unique to PNS include lead erosion, which can be ~7% in PNS systems261 and are less common in modern systems and when employing techniques with deeper implantation of lead anchoring devices. Finally, other serious complications for PNS systems include deep and superficial infection, pain over the implant site, and malfunction of the lead and/or implanted pulse generator.261,262 Fortunately, serious complications are rare, and PNS allows avoidance of risks associated with SCS, such as serious spinal cord injury or inadvertent dural puncture.
Billing, Insurance Coverage, and Requirements
Billing
CPT Codes for Leads
Physicians utilize unique CPT codes for the different types of peripheral nerve electrodes on the market for peripheral nerve stimulation (Table 9). A peripheral neurostimulator system includes an implanted pulse generator or implanted receiver with an external transmitter, a collection of contacts, electrodes (electrode array), an extension (if applicable), an external controller, and an external charger (if applicable). The electrode array conducts the electrical stimulation. The pulse generator or receiver may be integrated with the electrode array (single-component implant) or have a detachable connection to the electrode array (two or more component implant).
 |
Table 9 wRVU Values for PNS CPT Codes (64555–64596) Compared to SCS CPT Codes (63650–63688) |
Trial vs Implant
Trials are typically performed before implantation to assess the effectiveness of PNS in managing neuropathic pain. They are minimally invasive and reversible, offering a valuable opportunity to evaluate patient response and adjust stimulation parameters. However, trial success rates vary, and factors such as patient selection, trial duration, and trial lead location influence outcomes.
The decision to proceed with implantation after a successful trial is usually based on the degree of pain relief and improvement in function experienced by the patient. Although implantation is a more invasive procedure, it offers the potential for long-term pain relief in carefully selected patients.
Careful patient selection, proper trial design, and close collaboration between pain specialists and patients must be prioritized to optimize outcomes with PNS therapy.
Single vs Multiple Leads
The decision to use one or two leads for peripheral nerve stimulation depends on several medical factors already outlined. However, there are also factors related to payor coverage tied to Place of Service (POS). When POS is the Hospital Outpatient Department (HOPD), a flat charge is provided for lead placement and does not increase when two leads are placed. In the ASC setting, there is an additional payment for the second lead. Therefore, a local cost and payment analysis may need to be performed to determine the viability of two lead trials in a healthcare setting. POS is less important when considering permanent implantation as overall reimbursement rates generally support two lead placements in either setting (see Table 11).
Coding for IPG/Micro-IPG Placement
The updated CPT descriptions distinguish between integrated and non-integrated peripheral nerve stimulator (PNS) codes. For example, CPT code 64590 involves creating a pocket and connecting an electrode array to a pulse generator or receiver without specifying the size or type of the IPG. On the other hand, CPT code 64596 involves inserting an electrode array with an integrated neurostimulator, including imaging guidance, when performed. Incorrect labeling or coding can lead to non-reimbursement or the need for repayment after audit (“claw back”). An integrated neurostimulator contains the pulse generator or receiver and the electrode array as an all-in-one unit. A small incision is made, and the electrode array is tunneled percutaneously to the appropriate site. The same incision site is then used to create the pocket for the pulse generator or receiver. If more than one electrode array is used, add-on code 64597 may be reported for each additional electrode array. All of the aforementioned codes have a Global Period of 10 days.
Consensus Guideline 13: Given the rapid advancement of PNS technologies and variability between platforms, physicians should be familiar with the details of the device they are utilizing and how it fits into the existing CPT code descriptions to ensure accurate coding.
Coding for Imaging Guidance
For peripheral nerve stimulator procedures, fluoroscopic needle guidance is included in CPT code 64555 for lead placement and should not be billed separately. However, ultrasound needle guidance can be billed separately, if performed, as CPT 76942, typically with the −26 modifier to indicate the professional component.
Insurance Coverage and Reimbursement
Medicare NCD (National Coverage Determination) and LCD (Local Coverage Determination) for PNS
CMS defines NCDs, and regional MACs define LCDs, which dictate the coverage and provision of care to patients (Figure 4). In simpler terms, NCDs can be viewed as the national standard and LCDs as regional guidelines that cannot override the national standard but can provide more specific criteria. There is currently an NCD - Electric Nerve Stimulators (160.7) from CMS and LCD - Peripheral Nerve Stimulation (L34328 and L37360) from the Medicare Contractor Noridian. This contractor covers the states of Washington, Alaska, American Samoa, Arizona, California, Guam, Hawaii, Idaho, Nevada, Northern Mariana Islands and Oregon.
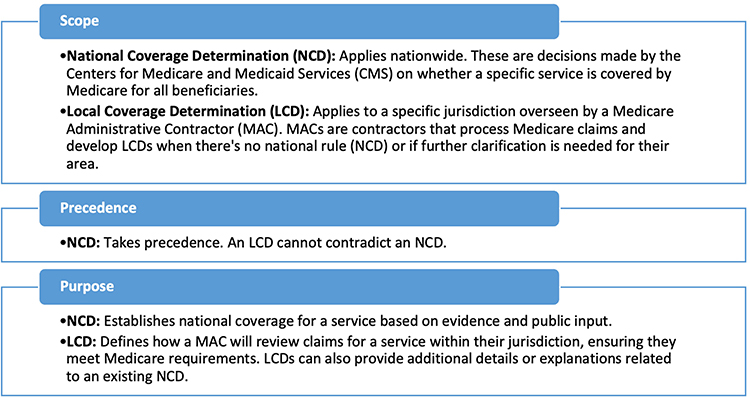 |
Figure 4 NCD and LCD Overview Overview of determinations for Medicare coverage. Abbreviations: NCD, National Coverage Determination; LCD, Local Coverage Determination. |
The Medicare NCD describes electric nerve stimulators as prosthetic devices. It does not provide medical necessity requirements. The Medicare Local Coverage Determination (LCD) for Peripheral Nerve Stimulation (PNS) by Noridian states that a peripheral nerve stimulation trial can be considered for the management of chronic pain if all the criteria are met (Table 10).
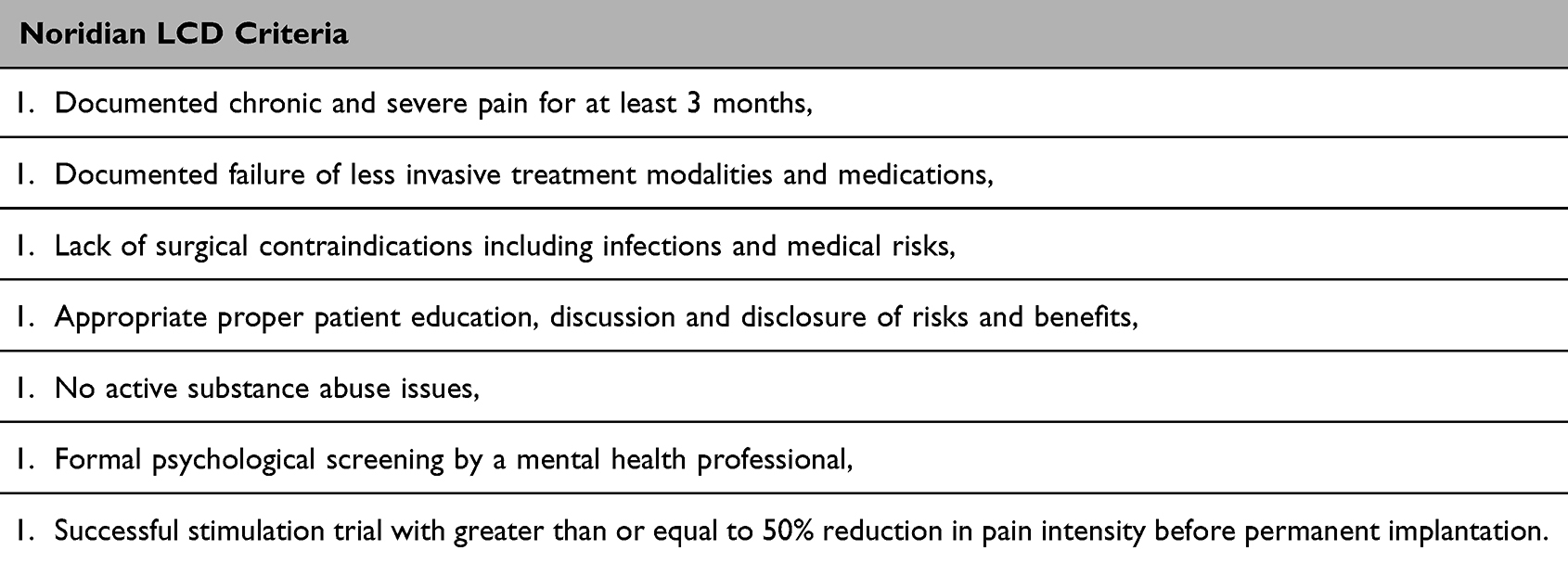 |
Table 10 Noridian LCD Criteria |
Peripheral nerve stimulation (PNS) may be covered for relief of chronic intractable pain for patients with conditions known to be responsive to this form of therapy after attempts to cure the underlying conditions, and appropriate attempts at medication management, physical therapy, psychological therapy, and other less invasive interventional treatments. An effective trial is a prerequisite for permanent implantation. The current LCD does not support the use of PNS for fibromyalgia, phantom limb pain, diffuse polyneuropathy, nociceptive pain in the trunk or lower back, or angina pectoris. Claims with these diagnoses will be denied as unreasonable and not medically necessary. The LCD provides a non-comprehensive list of indications with sufficient evidence of efficacy (Table 10).
There are significant access issues for PNS regarding coverage under Medicare Advantage plans, also known as Option C. Medicare Advantage plans are obligated to provide, at a minimum, coverage of all care that would apply under a Medicare plan. Specifically, Final Rule CMS-4201-F requires that Medicare Advantage plans must comply with established NCDs and LCDs (https://www.cms.gov/newsroom/fact-sheets/2024-medicare-advantage-and-part-d-final-rule-cms-4201-f). Unfortunately, many Advantage plans detail criteria that impede patients from accessing PNS coverage in violation of federal regulation. Some Option C carriers defer their policies to the Noridian LCD (L37360), while others do not provide such a path for patient selection and treatment. These authors have had nearly 100% success in taking denials to Administrative Law Judges (ALJ), where medical necessity is not a factor, but rather, cases are settled as a matter of regulation on the basis that Medicare Advantage plans must comply with the traditional Medicare coverage determinants. Medicare Advantage plans rely on star ratings, which is a tool used by the Centers for Medicare & Medicaid Services (CMS) to measure and rate the performance of Medicare Advantage (Part C) and Medicare Prescription Drug (Part D) plans. These ratings help Medicare beneficiaries compare plans and make an informed decision about their healthcare coverage. These ratings are negatively impacted when they lose cases in front of ALJs, which indicates they impede patient access to care.
Consensus Guideline 14: PNS is a covered therapy under traditional Medicare. Medicare Advantage (Part C) must comply with established NCDs and LCDs. NCD 160.7 grants coverage of PNS. Physicians should pursue appeal for Medicare Advantage denials as Administrative Law Judges (ALJ) primarily rectify denials to ensure coverage is aligned with CMS guidance.
Medicaid Coverage
Medicaid coverage of PNS is relatively poor. Most state Medicaid plans do not offer coverage of PNS and label it as experimental/investigational despite extensive studies, including RCTs, documenting the efficacy of PNS across a plethora of indications.56,95,96,263 Where there are rare exceptions allowing coverage of PNS under Medicaid plans, the reimbursement is generally insufficient to make it a viable option (https://pcl.promedica.org/-/media/paramount/assets/documents/medicalpolicy/pg0406_implantable_peripheral_nerve_stimulation.pdf?rev=c1117433a00c409ead91da74695f745d). Due to significant advocacy efforts, Colorado, Kentucky, Michigan, and Tennessee have Medicaid reimbursement rates that closely mimic Medicare, providing patients access to 60-day PNS treatment. There is data to suggest that Oklahoma, Missouri, Idaho, New Mexico, and possibly Nevada and Florida have Medicaid reimbursement rates that support permanent PNS implantation.
Commercial Insurers
Most commercial insurance plans do not cover peripheral nerve stimulation despite the evidence mentioned throughout this publication. Insurers may respond to pretreatment queries for PNS coverage with a statement of “no preauthorization required.” This language is misleading, commonly misinterpreted as a treatment is covered, and may proceed without a preauthorization submission. This misinterpretation creates frequent conflict between care teams, their facilities, and patients as payment is denied post-treatment. The resultant 5-figure cost transfers to patients with chronic intractable pain, their care teams, and the healthcare system. In the opinion of these authors, the use of “preauthorization not required” or “no auth required” in response to a patient or clinical team query should not be permitted without a concurrent statement on whether the benefit is even theoretically covered versus noncovered in the plan itself. These authors have generally found that coverage among commercial payors is successful approximately 30% of the time, following prior authorization attempts, peer-to-peers, and appeals.
Consensus Guideline 15: Given the large body of evidence supporting the efficacy of PNS across multiple indications and nerve targets as well as individual studies focused on specific indications, payors should cover PNS for chronic pain in patients who have failed to improve with conservative treatment.
Requirement of Nerve Blocks Before PNS Trial
Policies on the requirement for diagnostic nerve injections before the PNS trial vary by payors. Most policies do not have any clear guidance on nerve blocks before trial. CMS guidance states explicitly that the PNS trial is the ultimate determinant of the appropriateness of a patient for PNS implantation. While there may be a perception that nerve blocks help determine the pain generator, this has not been born out as a successful predictor of PNS success.52 An analysis of 173 patients undergoing PNS by Hoffmann et al showed no difference in pain relief at 3- or 6-months post-implant between patients who had successful preimplant diagnostic nerve injections and those in the control group.
Reimbursement Variance by Location of Service
Place of service significantly impacts reimbursement for most medical procedures. Codes indicating the place of service include Office (code 11), ASC (code 24), and Hospital Outpatient Department (HOPD, code 22 or 19). While reimbursement and costs vary widely based on geographical location, supplier contracts, and payor policies, data on CMS reimbursement provides insight into the differential (Table 11).
 |
Table 11 Medicare National Average Reimbursement Differential Between ASC and HOPD |
Utility of Psychological Evaluation
Studies, reviews, and guidelines continue to recommend the exclusion of patients with “psychiatric disease” as resulting in a negative impact on patients’ potential to respond favorably to PNS,264,265 relying on “consensus”, at best, rather than providing empirical evidence.266 Even studies that have attempted to predict PNS outcomes have excluded patients based on psychological factors, irrespective of the lack of evidence for doing so.267 Campbell et.al concluded that psychological evaluation is generally included pre-SCS”, although no consensus to date has been reached regarding what specifically the assessment should include and what cut-off levels should be adopted for various questionnaire measures.”268 There has been no subsequent evidence basis for these assessments nor any consensus.
Although patients with pain are routinely denied PNS because of depression, the empirical literature strongly suggests that PNS is associated with decreases in depression scores in headache patients at 6 and 12 months following the initiation of treatment.269 This finding is consistent with 3-month data in an earlier study of headache patients,270 as well as data demonstrating post-PNS reductions in depression in post-amputation patients, those with chronic knee pain,176 and likely other pain conditions. Accordingly, psychological evaluation requirements before PNS have the potential to exclude depressed patients when the empirical evidence points to this treatment’s potential to reduce depression.
Even though strong, evidence-based guidelines8 for PNS have recommended psychological evaluation before PNS, no empirical evidence supports such. Until data or even a strong consensus demonstrating a significant relationship between psychological factors and PNS outcomes is available, the insurance industry-mandated requirement for a psychological evaluation before PNS should be reconsidered.
Consensus Guideline 16: Given the lack of empirical evidence and a failure to establish a significant relationship between psychological factors and PNS outcomes, psychological evaluation before PNS should not be mandated by payors.
Health Economics
Increasing patient access to PNS will require improved payor coverage of the therapy. In addition to the growing body of evidence that strongly supports the efficacy of PNS and systematic reviews further reinforcing this, healthcare utilization and cost-effectiveness studies will help make the financial argument to payors. A cost-benefit analysis that looked collectively at PNS, as well as SCS, found that patients experience reductions in physician office visits, nerve blocks, radiologic imaging, emergency department visits, hospitalizations, and surgical procedures, totaling a net annual savings of approximately $30,221.271 This resulted in an overall net per patient per year cost savings of roughly $17,903. Bulsei et al examined the financial impact of occipital nerve stimulation and found that while cost went up on a short time horizon, such as 3 months, it was lower by 1,344 Euros in one year.272 Furthermore, when looking at indirect costs such as disability and sick leave, there was a reduction of 377 Euros for the occipital nerve stimulation group in the first 3 months.
Kalia et al evaluated the healthcare utilization and costs of 122 patients with chronic pain treated with PNS using a micro-implantable pulse generator.273 The authors observed a postop vs preop reduction in outpatient visits (4.9 vs 5.7), a 50% reduction in mean total medical costs ($13,717 vs $27,493), and a 57% reduction in median total medical costs ($5,094 vs $11,809). Furthermore, the proportion of patients using opioids was 31.4% lower.
Consensus Guideline 17: Multiple healthcare economics analyses have concluded that utilization of PNS reduces healthcare visits and total medical costs. This evidence supports reductions in hospitalizations, other surgical procedures, and opioid use. Future prospective studies should incorporate these metrics as an additional outcome measure.
Moving PNS Forward
Future Areas of Research
The body of research in PNS has grown significantly over the last 40 years, with the most significant surge in the previous decade (Figure 5). To further establish PNS as a standard of treatment for common neuropathic pain conditions, additional high-level evidence will be beneficial. Prospective randomized studies do exist that add credibility to the grading and proof, as outlined in this paper. Further studies are required to better understand best practices for PNS. This would include more disease-specific studies that give insight into which disease states are most responsive and how to optimize patient selection. A prospective registry of future cases on PNS would provide insight into patient selection and target sites.
 |
Figure 5 Clinical Trial and Retrospective Study Publications on PNS Annual PNS-related publications over a 40-year period. Source: PubMed Search, 02/10/2025. |
While RCTs are growing in prevalence and demonstrate the efficacy of PNS across many painful conditions, a continued focus on RCTs and, particularly, sham-controlled studies will help expand payor coverage of this beneficial therapy. Comparisons of lead designs, neural targets, and waveforms could be used in study design.72,173,274,275 Additional research to further identify the potential role of age, gender, body mass index (BMI), tobacco and alcohol use, and other demographics may further clarify selection criteria, thereby further boosting PNS efficacy. Furthermore, with multiple available platforms for PNS, studies focused on the personalization and titration of stimulation to optimize responder rates will be useful for physician decision-making.
Expanding indications for PNS supported by safe and replicable procedural techniques for each novel target will help extend the reach of the therapy. Beyond pain indications, as discussed in this paper, there is great potential in applying PNS to non-pain indications. This promising research area may position interventional pain providers as best suited to deliver innovative therapy across various atypical indications. The first step may be to collect a broader range of non-pain secondary outcome measures as part of future study design.
Future Product Development
Significant advances in the design of PNS-specific hardware have been made over the last decade, and current devices represent a substantial improvement over the initial implants that led to insurance coverage for this treatment.
There is still great potential to advance the physical and intangible technologies underpinning the therapy. New lead designs and miniaturization could expand the market for PNS by increasing physician confidence and comfort in placement across a variety of targets through collapsible lead tines for mobile areas such as joints and the axilla, smaller diameter lead designs for safety in facial, head, and neck applications, closed-loop PNS to improve consistency and reduce habituation and uncomfortable paresthesias, EMG feedback, resorbable leads for time-limited applications, and improved instrumentation to remove non-functioning implanted devices.261,276 The future of pulse generators may lie in even smaller battery-inclusive, fully implantable devices or decoupled devices with external batteries with enhancements to minimize pairing issues with a greater tolerance for distance between the internal IPG/receiver and the external power source. Furthermore, smaller profiles and more form-fitting external devices will improve patient acceptance and compliance. Some innovations are already being reported in the literature in early form that may predict future products that could enter the market (Table 12).
 |
Table 12 PNS Innovations Discussed in the Literature |
Conclusion
Progress within peripheral nerve stimulation has brought us to a pivotal time in the field. Efficacy research, including RCTs yielding impactful data on outcomes, important work on healthcare utilization and economics is building the case for PNS among payors; data on secondary outcomes such as reduced opioid utilization, functional outcomes, and sleep as well as minimizing sick and disability leave all add to the value proposition of PNS for patients. The endless frontier of possibilities for nerve targets and indications and significant research and understanding in non-pain applications continue to expand. These consensus guidelines (See Table 13) provide an essential framework for skilled interventional pain practitioners, offering evidence-based recommendations intended to guide current clinical practice and support decision-making in this evolving field. These practitioners leading our field can help refine the education tracks of our training to optimize ultrasound skills, image-guided lead placement, and understanding of patient selection and nerve targeting. The future of PNS holds great promise powered by research, technological advancement, and the determination of practitioners who have seen transformative outcomes in their patients.
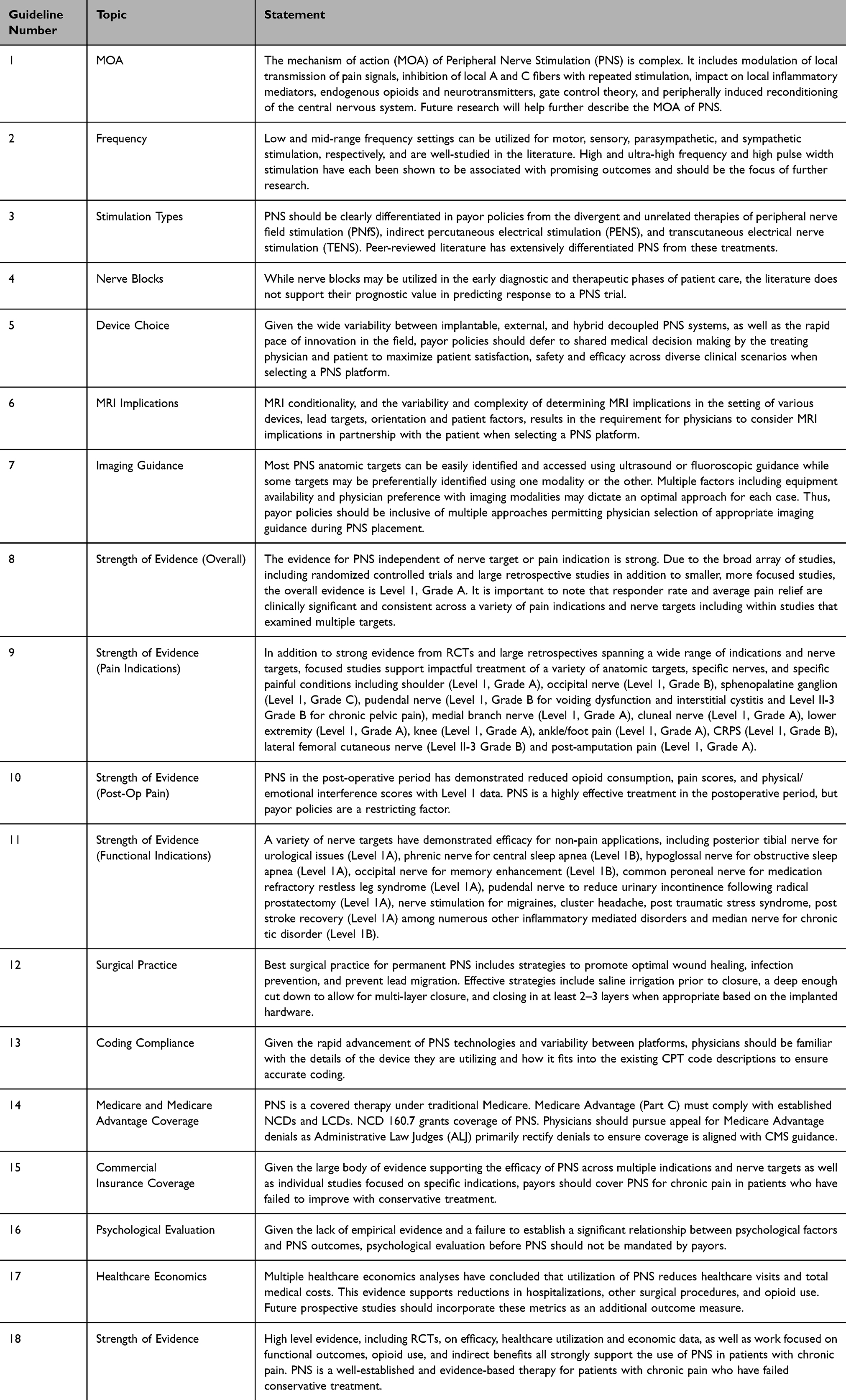 |
Table 13 Summary of ASPN NEURON PNS Consensus Guidelines |
Consensus Guideline 18: High level evidence, including RCTs, on efficacy, healthcare utilization and economic data, as well as work focused on functional outcomes, opioid use, and indirect benefits all strongly support the use of PNS in patients with chronic pain. PNS is a well-established and evidence-based therapy for patients with chronic pain who have failed conservative treatment.
Funding
Development of this guideline was supported by unrestricted educational grants from (in alphabetical order) Curonix, Nalu Medical, and SPR.
Disclosure
Dr Usman Latif reports personal fees from Abbott, Brixton Biosciences, Glucotrack, InFormed Consent, Nevro, Spinal Simplicity, Vertex Pharmaceuticals, Nalu Medical, SPR, Vertos Medical, Saluda Medical, Vivex Biologics, outside the submitted work. He is also part of the advisory board for Abbott, Nevro, Spinal Simplicity, Nalu Medical, Glucotrack, Vertos Medical, Saluda Medical, and Vivex Biologics; equity/stock options from Glucotrack, InFormed Consent, and Spinal Simplicity. Dr Robert Moghim reports grants from Curonix, Nalu Medical, SPR Therapeutics, during the conduct of the study; personal fees from Curonix and Abbott, outside the submitted work. Dr Ali Valimahomed reports grants, personal fees from SPR Therapeutics and Nalu, outside the submitted work. Dr Alaa Abd-Elsayed reports consultant for Medtronic, Curonix, Avanos and Averitas. Dr Amitabh Gulati is a consultant/advisory board member for Medtronic, AIS Healthcare, Neurovasis, SPR Therapeutics, Nalu Medical, Menda Health, Hinge Health, Symmetric PT, during the conduct of the study. Dr Mansoor Aman reports personal fees from SPR Therapeutics, Bioventus, Abbott, Medtronic, outside the submitted work. Dr Mehul Desai reports stock options from SPR Therapeutics; personal fees from Nalu Medical, during the conduct of the study; personal fees from Medtronic; stock options from SynerFuse, Virdio Health, HypreVention, outside the submitted work. Dr David Dickerson reports grants and/or personal fees from Abbott, SPR, Stryker, Vertos, Vertex, Biotronik, outside the submitted work. Vinicius Tieppo Francio is a consultant for Mainstay Medical. Dr Christopher Gilmore reports personal fees from SPR Therapeutics and Nalu, outside the submitted work. Dr Brandon Gish reports grants from Abbott, during the conduct of the study. Dr Jennifer Hah is a consultant for Nalu Medical. Dr Corey Hunter reports stock options from Mainstay; personal fees and/or grants from Abbott and Saluda, outside the submitted work. Dr Brian Ilfeld reports grants paid directly to his institution from SPR Therapeutics, Epimed International, Gate Science, Avanos, Masimo, Pacira BioSciences, outside the submitted work. Dr Denise Lester reports grants from SPR Therapeutics, during the conduct of the study. Dr Sean Li is a consultant for Abbott, Boston Scientific, Stryker; grants to his institution from Avanos, Averitas Pharma, Biotronik, Medtronic, Nalu, Presidio, PainTeq, Saluda, SPR Therapeutic; stock options from NeuroOne, outside the submitted work. Dr Ramana Naidu reports personal fees from SPR Therapeutics, Abbott, Boston Scientific, Biotronik, during the conduct of the study. Dr Einar Ottestad reports personal fees from SPR, BioVentus, Coloplast, Invicta Medical, Altamont Medical, during the conduct of the study. Dr Scott Pritzlaff reports personal fees from SPR Therapeutics, Medtronic, Bioness; royalties from Wolters Kluwer; educational grants to his institution from Biotronik, Medtronic, Abbott, Nevro, outside the submitted work. Dr Michael Schatman reports being a senior medical advisor for Apurano Pharma, outside the submitted work. Dr Samir Sheth reports personal fees from SPR, Medtronic, Vertos, SI Bone, Boston Scientific, during the conduct of the study. Dr Konstantin Slavin reports grants from Medtronic, Abbott, Boston Scientific, Saluda, Biotronik/MESI, Shiratronics, Curonix, outside the submitted work. Dr Tolga Suvar reports personal fees from Nalu, Nevro, Medtronic, Spinal Simplicity, Boston Scientific, Abbott, outside the submitted work. Dr Peter Staats reports a patent High dose Capsaicin with royalities paid to Averitas, a patent Vagus Nerve Stimulation licensed to electroCore. Dr Dawood Sayed reports stock options from Mainstay, SPR, PainTEQ, Surgentec; personal fees from Abbott, Painteq, Saluda, outside the submitted work. Dr Timothy Deer reports personal fees for consulting, advisory board, research and/or stock options from Abbott, SpineThera, Saluda Medical, Cornerloc, Boston Scientific, PainTEQ, Spinal Simplicity, Biotronik, Aurora, Nervonik, outside the submitted work; In addition, Dr Timothy Deer has a patent pending to Abbott. The authors report no other conflicts of interest in this work.
References
1. Ottestad E, Orlovich DS. History of peripheral nerve stimulation-update for the 21st century. Pain Med. 2020;21(Suppl 1):S3–S5. doi:10.1093/pm/pnaa165
2. Lam CM, Keim SA, Sayed D, et al. Novel implantation technique for thoracoabdominal peripheral nerve stimulation via a transversus abdominal plane approach for treatment of chronic abdominal pain. J Pain Res. 2024;17:981–987. doi:10.2147/JPR.S451955
3. Weiner RL, Reed KL. Peripheral neurostimulation for control of intractable occipital neuralgia. Neuromodulation. 1999;2(3):217–221. doi:10.1046/j.1525-1403.1999.00217.x
4. Harris RP, Helfand M, Woolf SH, et al. Current methods of the us preventive services task force: a review of the process. Am J Prev Med. 2001;20(3 Suppl).
5. Treede RD, Kenshalo DR, Gracely RH, Jones AK. The cortical representation of pain. Pain. 1999;79(2–3):105–111. doi:10.1016/s0304-3959(98)00184-5
6. Gracely RH, Lynch SA, Bennett GJ. Painful neuropathy: altered central processing maintained dynamically by peripheral input. Pain. 1992;51(2):175–194. doi:10.1016/0304-3959(92)90259-E
7. Tajerian M, Alvarado S, Millecamps M, et al. Peripheral nerve injury is associated with chronic, reversible changes in global DNA methylation in the mouse prefrontal cortex. PLoS One. 2013;8(1):e55259. doi:10.1371/journal.pone.0055259
8. Strand N, D’Souza RS, Hagedorn JM, et al. Evidence-based clinical guidelines from the American Society of Pain and Neuroscience for the use of implantable peripheral nerve stimulation in the treatment of chronic pain. J Pain Res. 2022;15:2483–2504. doi:10.2147/JPR.S362204
9. Kupers R, Laere KV, Calenbergh FV, et al. Multimodal therapeutic assessment of peripheral nerve stimulation in neuropathic pain: five case reports with a 20-year follow-up. Eur J Pain. 2011;15(2):161e1–9. doi:10.1016/j.ejpain.2010.06.015
10. Melzack R, Wall PD. Pain mechanisms: a new theory. Science. 1965;150(3699):971–979. doi:10.1126/science.150.3699.971
11. Goroszeniuk T, Pang D. Peripheral neuromodulation: a review. Curr Pain Headache Rep. 2014;18(5):412. doi:10.1007/s11916-014-0412-9
12. Cui JG, Wt O, Ungerstedt U, Linderoth B, Meyerson BA. Spinal cord stimulation attenuates augmented dorsal horn release of excitatory amino acids in mononeuropathy via a GABAergic mechanism. Pain. 1997;73(1):87–95. doi:10.1016/s0304-3959(97)00077-8
13. Yang F, Xu Q, Cheong YK, et al. Comparison of intensity-dependent inhibition of spinal wide-dynamic range neurons by dorsal column and peripheral nerve stimulation in a rat model of neuropathic pain. Eur J Pain. 2014;18(7):978–988. doi:10.1002/j.1532-2149.2013.00443.x
14. Radhakrishnan R, King EW, Dickman JK, et al. Spinal 5-HT(2) and 5-HT(3) receptors mediate low, but not high, frequency TENS-induced antihyperalgesia in rats. Pain. 2003;105(1–2):205–213. doi:10.1016/s0304-3959(03)00207-0
15. Jeong Y, Baik EJ, Nam TS, Paik KS. Effects of iontophoretically applied naloxone, picrotoxin and strychnine on dorsal horn neuron activities treated with high frequency conditioning stimulation in cats. Yonsei Med J. 1995;36(4):336–347. doi:10.3349/ymj.1995.36.4.336
16. Lin T, Gargya A, Singh H, Sivanesan E, Gulati A. Mechanism of peripheral nerve stimulation in chronic pain. Pain Med. 2020;21(Suppl 1):S6–S12. doi:10.1093/pm/pnaa164
17. Ong Sio LC, Hom B, Garg S, Abd-Elsayed A. Mechanism of action of peripheral nerve stimulation for chronic pain: a narrative review. Int J Mol Sci. 2023;24(5). doi:10.3390/ijms24054540
18. Han JS, Chen XH, Sun SL, et al. Effect of low- and high-frequency TENS on Met-enkephalin-Arg-Phe and dynorphin A immunoreactivity in human lumbar CSF. Pain. 1991;47(3):295–298. doi:10.1016/0304-3959(91)90218-M
19. Sluka KA, Vance CG, Lisi TL. High-frequency, but not low-frequency, transcutaneous electrical nerve stimulation reduces aspartate and glutamate release in the spinal cord dorsal horn. J Neurochem. 2005;95(6):1794–1801. doi:10.1111/j.1471-4159.2005.03511.x
20. Liao CF, Hsu ST, Chen CC, et al. Effects of electrical stimulation on peripheral nerve regeneration in a silicone rubber conduit in taxol-treated rats. Materials. 2020;13(5). doi:10.3390/ma13051063
21. Torebjork HE, Hallin RG. Responses in human A and C fibres to repeated electrical intradermal stimulation. J Neurol Neurosurg Psychiatry. 1974;37(6):653–664. doi:10.1136/jnnp.37.6.653
22. Bak MS, Park H, Kim SK. Neural Plasticity in the Brain during Neuropathic Pain. Biomedicines. 2021;9(6). doi:10.3390/biomedicines9060624
23. Wall PD, Sweet WH. Temporary abolition of pain in man. Science. 155(3758):108–109. doi:10.1126/science.155.3758.108
24. Shelden CH, Pudenz RH, Doyle J. Electrical control of facial pain. Am J Surg. 1967;114(2):209–212. doi:10.1016/0002-9610(67)90374-1
25. Hassenbusch SJ, Stanton-Hicks M, Schoppa D, Walsh JG, Covington EC. Long-term results of peripheral nerve stimulation for reflex sympathetic dystrophy. J Neurosurg. 1996;84(3):415–423. doi:10.3171/jns.1996.84.3.0415
26. Nashold BS Jr, Goldner JL. Electrical stimulation of peripheral nerves for relief of intractable chronic pain. Med Instrum. 1975;9(5):224–225.
27. Mobbs RJ, Blum P, Rossato R. Mesh electrode for peripheral nerve stimulation. J Clin Neurosci. 2003;10(4):476–477. doi:10.1016/s0967-5868(03)00090-0
28. Ignelzi RJ, Nyquist JK. Peripheral nerve stimulation for pain relief: effect on cutaneous peripheral nerve evoked activity. Surg Forum. 1975;26:474–476.
29. Slavin KV. History of peripheral nerve stimulation. Prog Neurol Surg. 2011;24:1–15. doi:10.1159/000323002
30. Smith BJ, Twohey EE, Dean KP, D’Souza RS. Peripheral nerve stimulation for the treatment of postamputation pain: a systematic review. Am J Phys Med Rehabil. 102(9):846–854. doi:10.1097/PHM.0000000000002237
31. Deer T, Pope J, Benyamin R, et al. Prospective, multicenter, randomized, double-blinded, partial crossover study to assess the safety and efficacy of the novel neuromodulation system in the treatment of patients with chronic pain of peripheral nerve origin. Neuromodulation. 2016;19(1):91–100. doi:10.1111/ner.12381
32. Birk DM, Yin D, Slavin KV. Regulation of peripheral nerve stimulation technology. Prog Neurol Surg. 2015;29:225–237. doi:10.1159/000434674
33. Deer T, Shah A, Slavin K, et al. Birds of a feather redux: defining ways to stimulate the peripheral nervous system. J Pain Res. 2023;16:1219–1224. doi:10.2147/JPR.S409158
34. Abd-Elsayed A, Moghim R. Efficacy of peripheral nerve stimulation with a high frequency electromagnetic coupled (HF-EMC) powered implanted receiver in treating different pain targets/neuralgias. J Pain Res. 2023;16:589–596. doi:10.2147/JPR.S399532
35. Kalia H, Abd-Elsayed A, Malinowski M, et al. Educational curriculum for peripheral nerve stimulation developed by the North American Neuromodulation Society. Neuromodulation. 2023;26(3):483–489. doi:10.1016/j.neurom.2022.09.015
36. Deer TR, Eldabe S, Falowski SM, et al. Peripherally induced reconditioning of the central nervous system: a proposed mechanistic theory for sustained relief of chronic pain with percutaneous peripheral nerve stimulation. J Pain Res. 2021;14:721–736. doi:10.2147/JPR.S297091
37. Deer TR, Naidu R, Strand N, et al. A review of the bioelectronic implications of stimulation of the peripheral nervous system for chronic pain conditions. Bioelectron Med. 2020;6:9. doi:10.1186/s42234-020-00045-5
38. Gilligan C, Volschenk W, Russo M, et al. An implantable restorative-neurostimulator for refractory mechanical chronic low back pain: a randomized sham-controlled clinical trial. Pain. 2021;162(10):2486–2498. doi:10.1097/j.pain.0000000000002258
39. Wilson RD, Gunzler DD, Bennett ME, Chae J. Peripheral nerve stimulation compared with usual care for pain relief of hemiplegic shoulder pain: a randomized controlled trial. Am J Phys Med Rehabil. 2014;93(1):17–28. doi:10.1097/PHM.0000000000000011
40. Gofeld M, Agur A. peripheral nerve stimulation for chronic shoulder pain: a proof of concept anatomy study. Neuromodulation. 2018;21(3):284–289. doi:10.1111/ner.12749
41. Gilmore CA, Kapural L, McGee MJ, Boggs JW. Percutaneous peripheral nerve stimulation (pns) for the treatment of chronic low back pain provides sustained relief. Neuromodulation. 2019;22(5):615–620. doi:10.1111/ner.12854
42. Gilligan C, Volschenk W, Russo M, et al. Three-year durability of restorative neurostimulation effectiveness in patients with chronic low back pain and multifidus muscle dysfunction. Neuromodulation. 2023;26(1):98–108. doi:10.1016/j.neurom.2022.08.457
43. Tieppo Francio V, Westerhaus BD, Carayannopoulos AG, Sayed D. Multifidus dysfunction and restorative neurostimulation: a scoping review. Pain Med. 2023;24(12):1341–1354. doi:10.1093/pm/pnad098
44. Deer TR, Levy RM, Rosenfeld EL. Prospective clinical study of a new implantable peripheral nerve stimulation device to treat chronic pain. Clin J Pain. 2010;26(5):359–372. doi:10.1097/AJP.0b013e3181d4d646
45. Soin A, Shah NS, Fang ZP. High-frequency electrical nerve block for postamputation pain: a pilot study. Neuromodulation. 2015;18(3):197–205. doi:10.1111/ner.12266
46. Kapural L, Syed Shah N, Fang ZP, Mekhail N. Multicenter, double-blinded, randomized, active-sham controlled clinical study design to assess the safety and effectiveness of a novel high frequency electric nerve block system in the treatment of post-amputation pain (The QUEST Study). J Pain Res. 2022;15:1623–1631. doi:10.2147/JPR.S353674
47. Deer TR, Levy RM, Verrills P, Mackey S, Abejon D. Perspective: peripheral nerve stimulation and peripheral nerve field stimulation birds of a different feather. Pain Med. 2015;16(3):411–412. doi:10.1111/pme.12662
48. Beltran-Alacreu H, Serrano-Munoz D, Martin-Caro Alvarez D, Fernandez-Perez J, Gomez-Soriano J, Avendano-Coy J. Percutaneous versus transcutaneous electrical nerve stimulation for the treatment of musculoskeletal pain. a systematic review and meta-analysis. Pain Med. 2022;23(8):1387–1400. doi:10.1093/pm/pnac027
49. Richmond SJ. Magnet therapy for the relief of pain and inflammation in rheumatoid arthritis (CAMBRA): a randomised placebo-controlled crossover trial. Trials. 2008;9:53. doi:10.1186/1745-6215-9-53
50. Fan Y, Ji X, Zhang L, Zhang X. The analgesic effects of static magnetic fields. Bioelectromagnetics. 2021;42(2):115–127. doi:10.1002/bem.22323
51. Kapural L, Patel J, Rosenberg JC, Li S, Amirdelfan K, Bedder M. Safety and efficacy of axon therapy (SEAT Study), utilizing magnetic peripheral nerve stimulation (mPNS) for treatment of neuropathic pain. J Pain Res. 2024;17:3167–3174. doi:10.2147/JPR.S481944
52. Hoffmann CM, Butler CS, Pingree MJ, Moeschler SM, Mauck WD, D’Souza RS. Is response to a pre-implant diagnostic peripheral nerve block associated with efficacy after peripheral nerve stimulation implantation? a ten-year enterprise-wide analysis. Neuromodulation. 2024;27(5):873–880. doi:10.1016/j.neurom.2023.10.003
53. Taylor A, McLeod G. Basic pharmacology of local anaesthetics. BJA Educ. 2020;20(2):34–41. doi:10.1016/j.bjae.2019.10.002
54. Ellrich J, Lamp S. Peripheral nerve stimulation inhibits nociceptive processing: an electrophysiological study in healthy volunteers. Neuromodulation. 2005;8(4):225–232. doi:10.1111/j.1525-1403.2005.00029.x
55. Huntoon MA, Slavin KV, Hagedorn JM, Crosby ND, Boggs JW. A retrospective review of real-world outcomes following 60-day peripheral nerve stimulation for the treatment of chronic pain. Pain Physician. 2023;26(3):273–281. doi:10.36076/ppj.2023.26.273
56. Pritzlaff SG, Latif U, Rosenow JM, et al. A review of prospective studies regarding percutaneous peripheral nerve stimulation treatment in the management of chronic pain. Pain Manag. 2024;14(4):209–222. doi:10.1080/17581869.2024.2352398
57. Ilfeld BM, Gabriel RA, Saulino MF, et al. infection rates of electrical leads used for percutaneous neurostimulation of the peripheral nervous system. Pain Pract. 2017;17(6):753–762. doi:10.1111/papr.12523
58. Marsolais EB, Kobetic R. Implantation techniques and experience with percutaneous intramuscular electrodes in the lower extremities. J Rehabil Res Dev. 1986;23(3):1–8.
59. Grill WM Jr, Mortimer JT. The effect of stimulus pulse duration on selectivity of neural stimulation. IEEE Trans Biomed Eng. 1996;43(2):161–166. doi:10.1109/10.481985
60. Deer TR, Grigsby E, Weiner RL, Wilcosky B, Kramer JM. A prospective study of dorsal root ganglion stimulation for the relief of chronic pain. Neuromodulation. 2013;16(1):67–71. doi:10.1111/ner.12013
61. Parker JL, Cameron T. Technology for Peripheral Nerve Stimulation. Prog Neurol Surg. 2015;29:1–19. doi:10.1159/000434651
62. Trevathan JK, Baumgart IW, Nicolai EN, et al. An injectable neural stimulation electrode made from an in-body curing polymer/metal composite. Adv Healthc Mater. 2019;8(23):e1900892. doi:10.1002/adhm.201900892
63. Howe A, Chen Z, Golobish K, et al. removal forces of a helical microwire structure electrode. Bioengineering. 11(6) doi:10.3390/bioengineering11060611
64. Yu DT, Chae J, Walker ME, Fang ZP. Percutaneous intramuscular neuromuscular electric stimulation for the treatment of shoulder subluxation and pain in patients with chronic hemiplegia: a pilot study. Arch Phys Med Rehabil. 2001;82(1):20–25. doi:10.1053/apmr.2001.18666
65. Kalia H, Pritzlaff S, Li AH, et al. Application of the novel nalu neurostimulation system for peripheral nerve stimulation. Pain Manag. 2022;12(7):795–804. doi:10.2217/pmt-2021-0050
66. Shellock FG, Zare A, Ilfeld BM, Chae J, Strother RB. In vitro magnetic resonance imaging evaluation of fragmented, open-coil, percutaneous peripheral nerve stimulation leads. Neuromodulation. 2018;21(3):276–283. doi:10.1111/ner.12705
67. Gargya A, Singh H, Lin T, Gulati A. extraforaminal thoracic and lumbar spinal nerve ultrasound-guided percutaneous peripheral nerve stimulation. Pain Med. 2020;21(Suppl 1):S38–S40. doi:10.1093/pm/pnaa166
68. Willsey M, Wilson TJ, Henning PT, Yang LJ. Intraoperative Ultrasound for Peripheral Nerve Applications. Neurosurg Clin N Am. 2017;28(4):623–632. doi:10.1016/j.nec.2017.05.013
69. Gupta S, Clendenen S, Ferreira-Dos-Santos G, Hurdle MF. Ultrasound-guided intercostal peripheral nerve stimulator implantation: technique report and feasibility study in a cadaver. Pain Med. 2020;21(Suppl 1):S32–S37. doi:10.1093/pm/pnaa012
70. Haider N, Gargya A. Fluoroscopy-guided lumbar spinal nerve stimulation to treat chronic scrotal pain. Cureus. 2023;15(7):e42298. doi:10.7759/cureus.42298
71. Kurt E, van Eijk T, Henssen D, Arnts I, Steegers M. Neuromodulation of the Suprascapular Nerve. Pain Physician. 2016;19(1):E235–9. doi:10.36076/ppj/2016.19.E235
72. Gilmore CA, Patel J, Esebua LG, Burchell M. A review of peripheral nerve stimulation techniques targeting the medial branches of the lumbar dorsal rami in the treatment of chronic low back pain. Pain Med. 2020;21(Suppl 1):S41–S46. doi:10.1093/pm/pnaa084
73. Jones JH, Brown A, Moyse D, Qi W, Roy L. Survival analysis of occipital nerve stimulator leads placed under fluoroscopic guidance with and without ultrasonography. Pain Physician. 2017;20(7):E1115–E1121. doi:10.36076/ppj/2017.7.E1115
74. Kossoff G. Basic physics and imaging characteristics of ultrasound. World J Surg. 2000;24(2):134–142. doi:10.1007/s002689910026
75. Singh V, Sandhu D, Xiang N. Techniques for peripheral nerve stimulator implantation of the upper extremity. Pain Med. 2020;21(Suppl 1):S27–S31. doi:10.1093/pm/pnaa185
76. Mazzola A, Spinner D. Ultrasound-guided peripheral nerve stimulation for shoulder pain: anatomic review and assessment of the current clinical evidence. Pain Physician. 2020;23(5):E461–E474.
77. Fonkoue L, Behets CW, Steyaert A, et al. Accuracy of fluoroscopic-guided genicular nerve blockade: a need for revisiting anatomical landmarks. Reg Anesth Pain Med. 2019;44:950–958. doi:10.1136/rapm-2019-100451
78. Shuang F, Hou SX, Zhu JL, et al. Clinical anatomy and measurement of the medial branch of the spinal dorsal ramus. Medicine. 2015;94(52):e2367. doi:10.1097/MD.0000000000002367
79. Kim JH, Shustorovich A, Arel AT, Downie SA, Cohen SP, Kim SY. Genicular nerve anatomy and its implication for new procedural approaches for knee joint denervation: a cadaveric study. Pain Med. 2022;23(1):144–151. doi:10.1093/pm/pnab238
80. Nisolle ML, Ghoundiwal D, Engelman E, et al. Comparison of the effectiveness of ultrasound-guided versus fluoroscopy-guided medial lumbar bundle branch block on pain related to lumbar facet joints: a multicenter randomized controlled non-inferiority study. BMC Anesthesiol. 2023;23(1):76. doi:10.1186/s12871-023-02029-9
81. Juckett L, Saffari TM, Ormseth B, Senger JL, Moore AM. The effect of electrical stimulation on nerve regeneration following peripheral nerve injury. Biomolecules. 2022;12(12). doi:10.3390/biom12121856
82. Zuo KJ, Gordon T, Chan KM, Borschel GH. Electrical stimulation to enhance peripheral nerve regeneration: update in molecular investigations and clinical translation. Exp Neurol. 2020;332:113397. doi:10.1016/j.expneurol.2020.113397
83. Gordon T, Amirjani N, Edwards DC, Chan KM. Brief post-surgical electrical stimulation accelerates axon regeneration and muscle reinnervation without affecting the functional measures in carpal tunnel syndrome patients. Exp Neurol. 2010;223(1):192–202. doi:10.1016/j.expneurol.2009.09.020
84. Barber B, Seikaly H, Ming Chan K, et al. Intraoperative Brief Electrical Stimulation of the Spinal Accessory Nerve (BEST SPIN) for prevention of shoulder dysfunction after oncologic neck dissection: a double-blinded, randomized controlled trial. J Otolaryngol Head Neck Surg. 2018;47(1):7. doi:10.1186/s40463-017-0244-9
85. Power HA, Morhart MJ, Olson JL, Chan KM. Postsurgical electrical stimulation enhances recovery following surgery for severe cubital tunnel syndrome: a double-blind randomized controlled trial. Neurosurgery. 2020;86(6):769–777. doi:10.1093/neuros/nyz322
86. Sayanagi J, Acevedo-Cintron JA, Pan D, et al. Brief electrical stimulation accelerates axon regeneration and promotes recovery following nerve transection and repair in mice. J Bone Joint Surg Am. 2021;103(20):e80. doi:10.2106/JBJS.20.01965
87. Keane GC, Pan D, Roh J, et al. The effects of intraoperative electrical stimulation on regeneration and recovery after nerve isograft repair in a rat model. Hand. 2022;17(3):540–548. doi:10.1177/1558944720939200
88. Roh J, Schellhardt L, Keane GC, et al. Short-duration, pulsatile, electrical stimulation therapy accelerates axon regeneration and recovery following tibial nerve injury and repair in rats. Plast Reconstr Surg.;149(4):681e–690e. doi:10.1097/PRS.0000000000008924.
89. Gordon T, Udina E, Verge VM, de Chaves EI. Brief electrical stimulation accelerates axon regeneration in the peripheral nervous system and promotes sensory axon regeneration in the central nervous system. Motor Control. 2009;13(4):412–441. doi:10.1123/mcj.13.4.412
90. Al-Majed AA, Brushart TM, Gordon T. Electrical stimulation accelerates and increases expression of BDNF and trkB mRNA in regenerating rat femoral motoneurons. Eur J Neurosci. 2000;12(12):4381–4390. doi:10.1046/j.1460-9568.2000.01341.x
91. Geremia NM, Gordon T, Brushart TM, Al-Majed AA, Verge VM. Electrical stimulation promotes sensory neuron regeneration and growth-associated gene expression. Exp Neurol. 2007;205(2):347–359. doi:10.1016/j.expneurol.2007.01.040
92. Brushart TM, Jari R, Verge V, Rohde C, Gordon T. Electrical stimulation restores the specificity of sensory axon regeneration. Exp Neurol. 2005;194(1):221–229. doi:10.1016/j.expneurol.2005.02.007
93. Ransom SC, Shahrestani S, Lien BV, et al. Translational approaches to electrical stimulation for peripheral nerve regeneration. Neurorehabil Neural Repair. 2020;34(11):979–985. doi:10.1177/1545968320962508
94. Birenbaum NK, Yan Y, Odabas A, Chandra NS, Ray WZ, MacEwan MR. Multiple sessions of therapeutic electrical stimulation using implantable thin-film wireless nerve stimulators improve functional recovery after sciatic nerve isograft repair. Muscle Nerve. 2023;67(3):244–251. doi:10.1002/mus.27776
95. Hatheway J, Hersel A, Engle M, et al. Clinical study of a micro-implantable pulse generator for the treatment of peripheral neuropathic pain: 12-month results from the COMFORT-randomized controlled trial. Reg Anesth Pain Med. 2024:rapm–2024–106099. doi:10.1136/rapm-2024-106099.
96. Engle M, Gutierrez G, Hersel A, Netzel C, Khemlani V. A confirmatory randomized controlled trial evaluating a micro-implantable pulse generator for the treatment of peripheral neuropathic pain: 3- and 6-month results from the COMFORT 2 Study. Chron Pain Manag. 2025;9:171. doi:10.29011/2576-957X.1000171
97. van der Windt DA, Koes BW, de Jong BA, Bouter LM. Shoulder disorders in general practice: incidence, patient characteristics, and management. Ann Rheum Dis. 1995;54(12):959–964. doi:10.1136/ard.54.12.959
98. Lucas J, van Doorn P, Hegedus E, Lewis J, van der Windt D. A systematic review of the global prevalence and incidence of shoulder pain. BMC Musculoskelet Disord. 2022;23(1):1073. doi:10.1186/s12891-022-05973-8
99. Eckmann MS, Bickelhaupt B, Fehl J, et al. Cadaveric study of the articular branches of the shoulder joint. Reg Anesth Pain Med. 2017;42(5):564–570. doi:10.1097/AAP.0000000000000652
100. Chae J, Yu DT, Walker ME, et al. Intramuscular electrical stimulation for hemiplegic shoulder pain: a 12-month follow-up of a multiple-center, randomized clinical trial. Am J Phys Med Rehabil. 2005;84(11):832–842. doi:10.1097/01.phm.0000184154.01880.72
101. Yu DT, Chae J, Walker ME, et al. Intramuscular neuromuscular electric stimulation for poststroke shoulder pain: a multicenter randomized clinical trial. Arch Phys Med Rehabil. 2004;85(5):695–704. doi:10.1016/j.apmr.2003.07.015
102. Mansfield JT, Desai MJ. Axillary peripheral nerve stimulation for chronic shoulder pain: a retrospective case series. Neuromodulation. 2020;23(6):812–818. doi:10.1111/ner.13096
103. Wilson RD, Harris MA, Gunzler DD, Bennett ME, Chae J. Percutaneous peripheral nerve stimulation for chronic pain in subacromial impingement syndrome: a case series. Neuromodulation. 2014;17(8):771–776. doi:10.1111/ner.12152.
104. Bouche B, Manfiotto M, Rigoard P, et al. Peripheral nerve stimulation of brachial plexus nerve roots and supra-scapular nerve for chronic refractory neuropathic pain of the upper limb. Neuromodulation. 2017;20(7):684–689. doi:10.1111/ner.12573
105. Kaye AD, Ridgell S, Alpaugh ES, et al. Peripheral nerve stimulation: a review of techniques and clinical efficacy. Pain Ther. 2021;10(2):961–972. doi:10.1007/s40122-021-00298-1
106. Ilfeld BM, Gelfand H, Dhanjal S, et al. Ultrasound-guided percutaneous peripheral nerve stimulation: a pragmatic effectiveness trial of a nonpharmacologic alternative for the treatment of postoperative pain. Pain Med.;21(Suppl 2):S53–S61. doi:10.1093/pm/pnaa332.
107. Deer TR, Mekhail N, Petersen E, et al. The appropriate use of neurostimulation: stimulation of the intracranial and extracranial space and head for chronic pain. neuromodulation appropriateness consensus committee. Neuromodulation. 2014;17(6):551–570. doi:10.1111/ner.12215
108. Antony AB, Mazzola AJ, Dhaliwal GS, Hunter CW. Neurostimulation for the treatment of chronic head and facial pain: a literature review. Pain Physician. 2019;22(5):447–477. doi:10.36076/ppj/2019.22.447
109. Hayek SM, Jasper JF, Deer TR, Narouze SN. Occipital neurostimulation-induced muscle spasms: implications for lead placement. Pain Physician. 2009;12(5):867–876. doi:10.36076/ppj.2009/12/867
110. Serra G, Marchioretto F. Occipital nerve stimulation for chronic migraine: a randomized trial. Pain Physician. 2012;15(3):245–253. doi:10.36076/ppj.2012/15/245
111. Slotty PJ, Bara G, Kowatz L, et al. Occipital nerve stimulation for chronic migraine: a randomized trial on subthreshold stimulation. Cephalalgia. 2015;35(1):73–78. doi:10.1177/0333102414534082
112. Saper JR, Dodick DW, Silberstein SD, et al. Occipital nerve stimulation for the treatment of intractable chronic migraine headache: ONSTIM feasibility study. Cephalalgia. 2011;31(3):271–285. doi:10.1177/0333102410381142
113. Mekhail NA, Estemalik E, Azer G, Davis K, Tepper SJ. Safety and efficacy of occipital nerves stimulation for the treatment of chronic migraines: randomized, double-blind, controlled single-center experience. Pain Pract. 2017;17(5):669–677. doi:10.1111/papr.12504
114. Dodick DW, Silberstein SD, Reed KL, et al. Safety and efficacy of peripheral nerve stimulation of the occipital nerves for the management of chronic migraine: long-term results from a randomized, multicenter, double-blinded, controlled study. Cephalalgia. 2015;35(4):344–358. doi:10.1177/0333102414543331
115. Silberstein SD, Dodick DW, Saper J, et al. Safety and efficacy of peripheral nerve stimulation of the occipital nerves for the management of chronic migraine: results from a randomized, multicenter, double-blinded, controlled study. Cephalalgia. 2012;32(16):1165–1179. doi:10.1177/0333102412462642
116. Zhou S, Hussain N, Abd-Elsayed A, et al. Peripheral nerve stimulation for treatment of headaches: an evidence-based review. Biomedicines. 2021;9(11). doi:10.3390/biomedicines9111588
117. Amin S, Buvanendran A, Park KS, Kroin JS, Moric M. Peripheral nerve stimulator for the treatment of supraorbital neuralgia: a retrospective case series. Cephalalgia. 2008;28(4):355–359. doi:10.1111/j.1468-2982.2008.01535.x
118. Narouze SN, Kapural L. Supraorbital nerve electric stimulation for the treatment of intractable chronic cluster headache: a case report. Headache. 2007;47(7):1100–1102. doi:10.1111/j.1526-4610.2007.00869.x
119. Elkholy MAE, Abd-Elsayed A, Raslan AM. Supraorbital Nerve Stimulation for Facial Pain. Curr Pain Headache Rep. 2023;27(6):157–163. doi:10.1007/s11916-023-01113-6
120. Vaisman J, Markley H, Ordia J, Deer T. The treatment of medically intractable trigeminal autonomic cephalalgia with supraorbital/supratrochlear stimulation: a retrospective case series. Neuromodulation. 2012;15(4):374–380. doi:10.1111/j.1525-1403.2012.00455.x
121. Deshpande KK, Wininger KL. Feasibility of combined epicranial temporal and occipital neurostimulation: treatment of a challenging case of headache. Pain Physician. 2011;14(1):37–44.
122. Simopoulos T, Bajwa Z, Lantz G, Lee S, Burstein R. Implanted auriculotemporal nerve stimulator for the treatment of refractory chronic migraine. Headache. 2010;50(6):1064–1069. doi:10.1111/j.1526-4610.2010.01694.x
123. Rodriguez-Lopez MJ, Fernandez-Baena M, Aldaya-Valverde C. Management of pain secondary to temporomandibular joint syndrome with peripheral nerve stimulation. Pain Physician. 2015;18(2):E229–36.
124. Zhang Y, Liu J, Li H, et al. Transcutaneous auricular vagus nerve stimulation at 1 Hz modulates locus coeruleus activity and resting state functional connectivity in patients with migraine: an fMRI study. Neuroimage Clin. 2019;24:101971. doi:10.1016/j.nicl.2019.101971
125. Robbins MS, Robertson CE, Kaplan E, et al. The Sphenopalatine Ganglion: anatomy, Pathophysiology, and Therapeutic Targeting in Headache. Headache. 2016;56(2):240–258. doi:10.1111/head.12729
126. Kwd H, Przkora R, Kumar S. Sphenopalatine ganglion: block, radiofrequency ablation and neurostimulation - a systematic review. J Headache Pain. 2017. 18(1):118. doi:10.1186/s10194-017-0826-y
127. Pietzsch JB, Garner A, Gaul C, May A. Cost-effectiveness of stimulation of the sphenopalatine ganglion (SPG) for the treatment of chronic cluster headache: a model-based analysis based on the Pathway CH-1 study. J Headache Pain. 2015;16:530. doi:10.1186/s10194-015-0530-8
128. Schoenen J, Jensen RH, Lanteri-Minet M, et al. Stimulation of the sphenopalatine ganglion (SPG) for cluster headache treatment. Pathway CH-1: a randomized, sham-controlled study. Cephalalgia. 2013;33(10):816–830. doi:10.1177/0333102412473667
129. Jurgens TP, Schoenen J, Rostgaard J, et al. Stimulation of the sphenopalatine ganglion in intractable cluster headache: expert consensus on patient selection and standards of care. Cephalalgia. 2014;34(13):1100–1110. doi:10.1177/0333102414530524
130. Maniam R, Kaye AD, Vadivelu N, Urman RD. Facial pain update: advances in neurostimulation for the treatment of facial pain. Curr Pain Headache Rep. 2016;20(4):24. doi:10.1007/s11916-016-0553-0
131. Lainez MJ, Puche M, Garcia A, Gascon F. Sphenopalatine ganglion stimulation for the treatment of cluster headache. Ther Adv Neurol Disord. 2014;7(3):162–168. doi:10.1177/1756285613510961
132. Pirro N, Sielezneff I, Le Corroller T, Ouaissi M, Sastre B, Champsaur P. Surgical anatomy of the extrapelvic part of the pudendal nerve and its applications for clinical practice. Surg Radiol Anat. 2009;31(10):769–773. doi:10.1007/s00276-009-0518-7
133. Shafik A, el-Sherif M, Youssef A, Olfat ES. Surgical anatomy of the pudendal nerve and its clinical implications. Clin Anat. 1995;8(2):110–115. doi:10.1002/ca.980080205
134. Peters KM, Killinger KA, Boguslawski BM, Boura JA. Chronic pudendal neuromodulation: expanding available treatment options for refractory urologic symptoms. Neurourol Urodyn. 2010;29(7):1267–1271. doi:10.1002/nau.20823
135. Peters KM, Killinger KA, Jaeger C, Chen C. Pilot study exploring chronic pudendal neuromodulation as a treatment option for pain associated with pudendal neuralgia. Low Urin Tract Symptoms. 2015;7(3):138–142. doi:10.1111/luts.12066
136. Peters KM, Feber KM, Bennett RC. A prospective, single-blind, randomized crossover trial of sacral vs pudendal nerve stimulation for interstitial cystitis. BJU Int. 2007;100(4):835–839. doi:10.1111/j.1464-410X.2007.07082.x
137. Peters KM, Feber KM, Bennett RC. Sacral versus pudendal nerve stimulation for voiding dysfunction: a prospective, single-blinded, randomized, crossover trial. Neurourol Urodyn. 2005;24(7):643–647. doi:10.1002/nau.20174
138. Lam CM, Keim SA, Latif U. Novel implantation technique for pudendal nerve peripheral nerve stimulation for treatment of chronic pelvic pain. Reg Anesth Pain Med. 2023;48(11):567–571. doi:10.1136/rapm-2023-104551
139. Gregory NS, Terkawi AS, Prabhakar NK, Tran JV, Salmasi V, Hah JM. Peripheral nerve stimulation for pudendal neuralgia: a technical note. Pain Med. 2020;21(Suppl 1):S51–S55. doi:10.1093/pm/pnaa171
140. Rozen WM, Tran TM, Ashton MW, Barrington MJ, Ivanusic JJ, Taylor GI. Refining the course of the thoracolumbar nerves: a new understanding of the innervation of the anterior abdominal wall. Clin Anat. 2008;21(4):325–333. doi:10.1002/ca.20621
141. Standring S, Ellis H, Healy J, et al. Gray’s anatomy: the anatomical basis of clinical practice. Am J Neuroradiol. 2005;26(10):2703.
142. Wijsmuller AR, Lange JF, Kleinrensink GJ, et al. Nerve-identifying inguinal hernia repair: a surgical anatomical study. World J Surg. 2007;31(2):414–420. doi:10.1007/s00268-006-0376-y
143. Ozen V, Acik ME, Ozen N. The modified thoracoabdominal nerve block for post-operative analgesia in paediatric laparoscopic cholecystectomy. J Minim Access Surg. 2024;20(4):452–455. doi:10.4103/jmas.jmas_174_22
144. Abd-Elsayed A, Malyuk D. Efficacy of transversus abdominis plane steroid injection for treating chronic abdominal pain. Pain Pract. 2018;18(1):48–52. doi:10.1111/papr.12580
145. Abd-Elsayed A, Luo S, Falls C. Transversus Abdominis Plane Block as a Treatment Modality for Chronic Abdominal Pain. Pain Physician. 2020;23(4):405–412. doi:10.36076/ppj.2020/23/405
146. Sellam S, Nguyen AT, Pogu M, Kianmanesh R, Malinovsky JM, Renard Y. Transversus abdominis plane block in the treatment of chronic postsurgical abdominal wall pain improves patient quality of life: a retrospective study and literature review. Pain Physician. 2023;26(2):E91–E100. doi:10.36076/ppj.2023.26.E91
147. Nizamuddin SL, Koury KM, Lau ME, watt LD, Gulur P. Use of targeted transversus abdominus plane blocks in pediatric patients with anterior cutaneous nerve entrapment syndrome. Pain Physician. 2014;17(5):E623–7.
148. Gilligan C, Volschenk W, Russo M, et al. Five-Year longitudinal follow-up of restorative neurostimulation shows durability of effectiveness in patients with refractory chronic low back pain associated with multifidus muscle dysfunction. Neuromodulation. 2024;27(5):930–943. doi:10.1016/j.neurom.2024.01.006
149. Deer TR, Gilmore CA, Desai MJ, et al. Percutaneous peripheral nerve stimulation of the medial branch nerves for the treatment of chronic axial back pain in patients after radiofrequency ablation. Pain Med. 2021;22(3):548–560. doi:10.1093/pm/pnaa432
150. Gilmore CA, Desai MJ, Hopkins TJ, et al. Treatment of chronic axial back pain with 60-day percutaneous medial branch PNS: primary end point results from a prospective, multicenter study. Pain Pract. 2021;21(8):877–889. doi:10.1111/papr.13055
151. D’Souza RS, Jin MY, Abd-Elsayed A. peripheral nerve stimulation for low back pain: a systematic review. Curr Pain Headache Rep. 2023;27(5):117–128. doi:10.1007/s11916-023-01109-2
152. Sheth SJ, Mauck WD, Russo DP, et al. Potential cost savings with 60-day peripheral nerve stimulation treatment in chronic axial low back pain. Pain Ther. 2024;13(5):1187–1202. doi:10.1007/s40122-024-00630-5
153. Karl HW, Helm S, Trescot AM. Superior and middle cluneal nerve entrapment: a cause of low back and radicular pain. Pain Physician. 2022;25(4):E503–E521.
154. Soteropoulos C, Pergolizzi J, Nagarakanti S, Gharibo C. Peripheral nerve stimulation for treatment of cluneal neuropathy case study. Cureus. 2022;14(8):e28033. doi:10.7759/cureus.28033
155. Vu PD, Robinson CL, Kaye AD, Hasoon J. Stimulating superior cluneal nerves via peripheral nerve stimulation as a treatment for chronic low back pain. Cureus. 2024;16(1):e51952. doi:10.7759/cureus.51952
156. Chauhan G, Levy I, DeChellis D. Superior cluneal neuralgia treated with wireless peripheral nerve stimulation. Cureus. 2022;14(3):e23711. doi:10.7759/cureus.23711
157. Billet B, Wynendaele R, Vanquathem NE. A novel minimally invasive wireless technology for neuromodulation via percutaneous intercostal nerve stimulation for post-herpetic neuralgia: a case report with short-term follow-up. Pain Pract. 2018;18(3):374–379. doi:10.1111/papr.12607
158. Amorizzo E, De Sanctis F, Baldeschi GC, Ricci F, Varrassi G. Peripheral nerve stimulation (PNS): a valid and definitive therapeutical option for a case of anterior cutaneous nerve entrapment syndrome (ACNES). Agri. 2024;36(2):126–128. doi:10.14744/agri.2023.07673
159. Mainkar O, Solla CA, Chen G, Legler A, Gulati A. Pilot study in temporary peripheral nerve stimulation in oncologic pain. Neuromodulation. 2020;23(6):819–826. doi:10.1111/ner.13139
160. Oswald J, Shahi V, Chakravarthy KV. Prospective case series on the use of peripheral nerve stimulation for focal mononeuropathy treatment. Pain Manag. 2019;9(6):551–558. doi:10.2217/pmt-2019-0028
161. Shaw A, Sharma M, Zibly Z, Ikeda D, Deogaonkar M. Sandwich technique, peripheral nerve stimulation, peripheral field stimulation and hybrid stimulation for inguinal region and genital pain. Br J Neurosurg. 2016;30(6):631–636. doi:10.1080/02688697.2016.1199777
162. Banh DP, Moujan PM, Haque Q, Han TH. Permanent implantation of peripheral nerve stimulator for combat injury-related ilioinguinal neuralgia. Pain Physician. 2013;16(6):E789–91.
163. Carayannopoulos A, Beasley R, Sites B. Facilitation of percutaneous trial lead placement with ultrasound guidance for peripheral nerve stimulation trial of ilioinguinal neuralgia: a technical note. Neuromodulation. 2009;12(4):296–301. doi:10.1111/j.1525-1403.2009.00233.x
164. Kalava A, Khan AA, Mihaylov SV. Post-renal Transplantation Triple Neuralgia: a Case Report. Cureus. 2023;15(11):e49518. doi:10.7759/cureus.49518
165. Al Tamimi M, Davids HR, Barolat G, Krutsch J, Ford T. Subcutaneous peripheral nerve stimulation treatment for chronic pelvic pain. Neuromodulation. 2008;11(4):277–281. doi:10.1111/j.1525-1403.2008.00176.x
166. Rosendal F, Moir L, de Pennington N, Green AL, Aziz TZ. Successful treatment of testicular pain with peripheral nerve stimulation of the cutaneous branch of the ilioinguinal and genital branch of the genitofemoral nerves. Neuromodulation. 2013;16(2):121–124. doi:10.1111/j.1525-1403.2011.00421.x
167. Abd-Elsayed A. Wireless peripheral nerve stimulation for treatment of peripheral neuralgias. Neuromodulation. 2020;23(6):827–830. doi:10.1111/ner.13131
168. Walter J, Reichart R, Vonderlind C, Kuhn SA, Kalff R. Neuralgia of the genitofemoral nerve after hernioplasty. Therapy by peripheral nerve stimulation. Chirurg. 2009;80(8):741–744. doi:10.1007/s00104-008-1624-5
169. Dana E, Gupta H, Pathak R, Khan JS. Genitofemoral peripheral nerve stimulator implantation for refractory groin pain: a case report. Can J Anaesth. 2023;70(1):163–168. doi:10.1007/s12630-022-02348-4
170. Finch P, Price L, Drummond P. High-Frequency (10 kHz) Electrical Stimulation of Peripheral Nerves for Treating Chronic Pain: a Double-Blind Trial of Presence vs Absence of Stimulation. Neuromodulation. 2019;22(5):529–536. doi:10.1111/ner.12877
171. Langford B, Mauck WD. Peripheral nerve stimulation: a new treatment for meralgia paresthetica. Pain Med. 2021;22(1):213–216. doi:10.1093/pm/pnaa326
172. Dalal S, Berger AA, Orhurhu V, Kaye AD, Hasoon J. Peripheral Nerve Stimulation for the Treatment of Meralgia Paresthetica. Orthop Rev. 2021;13(2):24437. doi:10.52965/001c.24437
173. Ilfeld BM, Plunkett A, Vijjeswarapu AM, et al. Percutaneous peripheral nerve stimulation (neuromodulation) for postoperative pain: a randomized, sham-controlled pilot study. Anesthesiology. 2021;135(1):95–110. doi:10.1097/ALN.0000000000003776
174. Ilfeld BM, Said ET, JJt F, et al. Ultrasound-Guided Percutaneous peripheral nerve stimulation: neuromodulation of the femoral nerve for postoperative analgesia following ambulatory anterior cruciate ligament reconstruction: a proof of concept study. Neuromodulation. 2019;22(5):621–629. doi:10.1111/ner.12851
175. McCullough M, Kenney D, Curtin C, Ottestad E. Peripheral nerve stimulation for saphenous neuralgia. Reg Anesth Pain Med. 2024;49(6):455–460. doi:10.1136/rapm-2023-104538
176. Fruh A, Sargut TA, Hussein A, et al. Peripheral nerve stimulation for the treatment of chronic knee pain. Sci Rep. 2023;13(1):15543. doi:10.1038/s41598-023-42608-x
177. Hasoon J, Chitneni A, Urits I, Viswanath O, Kaye AD. Peripheral stimulation of the saphenous and superior lateral genicular nerves for chronic knee pain. Cureus. 13(4):e14753. doi:10.7759/cureus.14753
178. Zhu CC, Gargya A, Haider N. A case report of three patients who underwent temporary peripheral nerve stimulation for treatment of knee pain secondary to osteoarthritis. Cureus. 2023;15(6):e40473. doi:10.7759/cureus.40473
179. Amirianfar E, Rosales R, Logan A, Doshi TL, Reynolds J, Price C. Peripheral nerve stimulation for chronic knee pain following total knee arthroplasty: a systematic review. Pain Manag. 2023;13(11):667–676. doi:10.2217/pmt-2023-0057
180. Hanyu-Deutmeyer A, Pritzlaff SG. Peripheral nerve stimulation for the 21st century: sural, superficial peroneal, and tibial nerves. Pain Med. 2020;21(Suppl 1):S64–S67. doi:10.1093/pm/pnaa202
181. Lin E. Peripheral nerve stimulation using high-frequency electromagnetic coupling (HF-EMC) Technology to Power an Implanted Neurostimulator With a Separate Receiver for Treating Peripheral Neuropathy. Pain Physician. 2024;27(7):E725–E730. doi:10.36076/ppj.2024.27.E725
182. D’Souza RS, Her YF, Jin MY, Morsi M, Abd-Elsayed A. Neuromodulation therapy for chemotherapy-induced peripheral neuropathy: a systematic review. Biomedicines 2022. 10(8). doi:10.3390/biomedicines10081909
183. Busch C, Smith O, Weaver T, Vallabh J, Abd-Elsayed A. Peripheral nerve stimulation for lower extremity pain. Biomedicines. 2022;10(7). doi:10.3390/biomedicines10071666
184. Ruan QZ, Chang J, Pak D, et al. Literature review: mechanism, indications, and clinical efficacy of peripheral nerve stimulators in lower extremity pain. Curr Pain Headache Rep. 2024;28(6):469–479. doi:10.1007/s11916-024-01240-8
185. Gutierrez GJ, Zurn CA, Crosby ND. Sustained Relief of Complex Regional Pain Syndrome (CRPS) Pain Following a 60-Day Peripheral Nerve Stimulation: a Report of Three Cases. Cureus. 2024;16(2):e54458. doi:10.7759/cureus.54458
186. Sawetz I, Smolle C, Girsch W. First experiences with peripheral nerve stimulation using an implantable system as a treatment method for the complex regional pain syndrome CRPS 2. Handchir Mikrochir Plast Chir. 2022;54(2):131–138. doi:10.1055/a-1687-9374
187. Chmiela MA, Hendrickson M, Hale J, et al. Direct peripheral nerve stimulation for the treatment of complex regional pain syndrome: a 30-year review. Neuromodulation. 2021;24(6):971–982. doi:10.1111/ner.13295
188. Frederico TN, da Silva Freitas T. Peripheral nerve stimulation of the brachial plexus for chronic refractory CRPS pain of the upper limb: description of a new technique and case series. Pain Med. 2020;21(Suppl 1):S18–S26. doi:10.1093/pm/pnaa201
189. Goree JH, Grant SA, Dickerson DM, et al. Randomized placebo-controlled trial of 60-day percutaneous peripheral nerve stimulation treatment indicates relief of persistent postoperative pain, and improved function after knee replacement. Neuromodulation. 2024;27(5):847–861. doi:10.1016/j.neurom.2024.03.001
190. Gilmore CA, Ilfeld BM, Rosenow JM, et al. Percutaneous 60-day peripheral nerve stimulation implant provides sustained relief of chronic pain following amputation: 12-month follow-up of a randomized, double-blind, placebo-controlled trial. Reg Anesth Pain Med. 2019;44:637–645. doi:10.1136/rapm-2019-100937
191. Albright-Trainer B, Phan T, Trainer RJ, et al. Peripheral nerve stimulation for the management of acute and subacute post-amputation pain: a randomized, controlled feasibility trial. Pain Manag. 2022;12(3):357–369. doi:10.2217/pmt-2021-0087
192. Ilfeld BM, Gabriel RA, Said ET, et al. Ultrasound-guided percutaneous peripheral nerve stimulation: neuromodulation of the sciatic nerve for postoperative analgesia following ambulatory foot surgery, a proof-of-concept study. Reg Anesth Pain Med. 2018;43(6):580–589. doi:10.1097/AAP.0000000000000819
193. Ilfeld BM, JJt F, Gabriel RA, et al. Ultrasound-guided percutaneous peripheral nerve stimulation: neuromodulation of the suprascapular nerve and brachial plexus for postoperative analgesia following ambulatory rotator cuff repair. A proof-of-concept study. Reg Anesth Pain Med. 2019;44(3):310–318. doi:10.1136/rapm-2018-100121
194. Ilfeld BM, Plunkett A, Vijjeswarapu AM, et al. Percutaneous neuromodulation of the brachial plexus and sciatic nerve for the treatment of acute pain following surgery: secondary outcomes from a multicenter, randomized, controlled pilot study. Neuromodulation. 2023;26(3):638–649. doi:10.1111/ner.13492
195. Ilfeld BM, Finneran JJ. Cryoneurolysis and percutaneous peripheral nerve stimulation to treat acute pain. Anesthesiology. 2020;133(5):1127–1149. doi:10.1097/ALN.0000000000003532
196. Luo C, Wei D, Pang K, Mei L, Chen Y, Niu X. Is percutaneous tibial nerve stimulation (PTNS) effective for fecal incontinence (FI) in adults compared with sham electrical stimulation? A meta-analysis. Tech Coloproctol. 2024;28(1):37. doi:10.1007/s10151-024-02910-w
197. Bai J, Tian Y, Wang Y, Zhang X, Wang P. Physical and rehabilitation therapy for overactive bladder in women: a systematic review and meta-analysis. Int J Clin Pract. 2023;2023:6758454. doi:10.1155/2023/6758454
198. Farag F, Sakalis VI, Arteaga SM, et al. What are the short-term benefits and potential harms of therapeutic modalities for the management of overactive bladder syndrome in women? a review of evidence under the auspices of the european association of urology, female non-neurogenic lower urinary tract symptoms guidelines panel. Eur Urol. 2023;84(3):302–312. doi:10.1016/j.eururo.2023.05.014
199. Huang J, Fan Y, Zhao K, et al. Comparative Efficacy of Neuromodulation Technologies for Overactive Bladder in Adults: a Network Meta-Analysis of Randomized Controlled Trials. Neuromodulation. 2023;26(8):1535–1548. doi:10.1016/j.neurom.2022.06.004
200. Zhou L, Zhang Z, Wang L. Treatment of anterior resection syndrome: a systematic review and network meta-analysis. Eur J Surg Oncol. 2024;50(6):108336. doi:10.1016/j.ejso.2024.108336
201. Guitynavard F, Mirmosayyeb O, Razavi ERV, et al. Percutaneous posterior tibial nerve stimulation (PTNS) for lower urinary tract symptoms (LUTSs) treatment in patients with multiple sclerosis (MS): a systematic review and meta-analysis. Mult Scler Relat Disord. 2022;58:103392. doi:10.1016/j.msard.2021.103392
202. Cohen JM, Fagin AP, Hariton E, et al. Therapeutic intervention for chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS): a systematic review and meta-analysis. PLoS One. 2012;7(8):e41941. doi:10.1371/journal.pone.0041941
203. Henssen D, Derks B, van Doorn M, et al. Vagus nerve stimulation for primary headache disorders: an anatomical review to explain a clinical phenomenon. Cephalalgia. 2019;39(9):1180–1194. doi:10.1177/0333102419833076
204. Lampros M, Vlachos N, Zigouris A, Voulgaris S, Alexiou GA. Transcutaneous Vagus Nerve Stimulation (t-VNS) and epilepsy: a systematic review of the literature. Seizure. 2021;91:40–48. doi:10.1016/j.seizure.2021.05.017
205. Tornero C, Pastor E, Garzando MDM, et al. Non-invasive Vagus Nerve Stimulation for COVID-19: results From a Randomized Controlled Trial (SAVIOR I). Front Neurol. 2022;13:820864. doi:10.3389/fneur.2022.820864
206. Staats PS, Poree L. Vagus nerve stimulation in rheumatoid arthritis. Lancet Rheumatol. 2021;3(1):e14. doi:10.1016/S2665-9913(20)30360-X
207. Cukiert A. Vagus nerve stimulation for epilepsy: an evidence-based approach. Prog Neurol Surg. 2015;29:39–52. doi:10.1159/000434654
208. Eljamel S. Vagus nerve stimulation for major depressive episodes. Prog Neurol Surg. 2015;29:53–63. doi:10.1159/000434655
209. Liu CY, Russin J, Adelson DP, et al. Vagus nerve stimulation paired with rehabilitation for stroke: implantation experience from the VNS-REHAB trial. J Clin Neurosci. 2022;105:122–128. doi:10.1016/j.jocn.2022.09.013
210. Kaufmann EM, Krause S, Geisshuesler L, Scheidegger O, Haeberlin A, Niederhauser T. Feasibility of transesophageal phrenic nerve stimulation. Biomed Eng Online. 2023;22(1):5. doi:10.1186/s12938-023-01071-5
211. Goldberg LR, Fox H, Stellbrink C, et al. Design of the remede System Therapy (reST) study: a prospective non-randomized post-market study collecting clinical data on safety and effectiveness of the remede system for the treatment of central sleep apnea. Sleep Med. 2022;100:238–243. doi:10.1016/j.sleep.2022.08.026
212. Fox H, Bitter T, Horstkotte D, Oldenburg O, Gutleben KJ. Long-term experience with first-generation implantable neurostimulation device in central sleep apnea treatment. Pacing Clin Electrophysiol. 2017;40(5):498–503. doi:10.1111/pace.13049
213. Costanzo MR, Ponikowski P, Javaheri S, et al. Transvenous neurostimulation for central sleep apnoea: a randomised controlled trial. Lancet. 2016;388(10048):974–982. doi:10.1016/S0140-6736(16)30961-8
214. Voigt J, Emani S, Gupta S, Germany R, Khayat R. Meta-analysis comparing outcomes of therapies for patients with central sleep apnea and heart failure with reduced ejection fraction. Am J Cardiol. 2020;127:73–83. doi:10.1016/j.amjcard.2020.04.011
215. Nayak HM, Patel R, McKane S, et al. Transvenous phrenic nerve stimulation for central sleep apnea is safe and effective in patients with concomitant cardiac devices. Heart Rhythm. 2020;17(12):2029–2036. doi:10.1016/j.hrthm.2020.06.023
216. Dres M, de Abreu MG, Merdji H, et al. Randomized clinical study of temporary transvenous phrenic nerve stimulation in difficult-to-wean patients. Am J Respir Crit Care Med. 2022;205(10):1169–1178. doi:10.1164/rccm.202107-1709OC
217. Spiesshoefer J, Kersten A, Enriquez Geppert J, et al. State-of-the-art opinion article on ventilator-induced diaphragm dysfunction: update on diagnosis, clinical course, and future treatment options. Respiration. 2023;102(1):74–82. doi:10.1159/000527466
218. Abdunnur SV, Kim DH. phrenic nerve stimulation: technology and clinical applications. Prog Neurol Surg. 2015;29:64–75. doi:10.1159/000434657
219. Mezzanotte WS, Tangel DJ, White DP. Influence of sleep onset on upper-airway muscle activity in apnea patients versus normal controls. Am J Respir Crit Care Med. 1996;153(6):1880–1887. doi:10.1164/ajrccm.153.6.8665050
220. Remmers JE, deGroot WJ, Sauerland EK, Anch AM, deGroot WJ. Pathogenesis of upper airway occlusion during sleep. J Appl Physiol Respir Environ Exerc Physiol. 1978;44(6):931–938. doi:10.1152/jappl.1978.44.6.931
221. Kim DH, Kim SW, Han JS, Kim GJ, Basurrah MA, Hwang SH. hypoglossal nerve stimulation effects on obstructive sleep apnea over time: a systematic review and meta-analysis. Otolaryngol Head Neck Surg. 2024;170(3):736–746. doi:10.1002/ohn.617
222. Strollo PJ Jr, Soose RJ, Maurer JT, et al. Upper-airway stimulation for obstructive sleep apnea. N Engl J Med. 2014;370(2):139–149. doi:10.1056/NEJMoa1308659
223. Asarkar AA, Bui R, Calligas J, Gillespie MB, Nathan CO. Where does hypoglossal nerve stimulator implant fit in the surgical management algorithm of obstructive sleep apnea? Laryngoscope. 2024;134(10):4165–4166. doi:10.1002/lary.31486
224. Luckey AM, McLeod SL, Robertson IH, To WT, Vanneste S. Greater occipital nerve stimulation boosts associative memory in older individuals: a randomized trial. Neurorehabil Neural Repair. 2020;34(11):1020–1029. doi:10.1177/1545968320943573
225. Vanneste S. Let’s shape learning into lasting memories. Neurosci Insights. 2024;19:26331055241227220. doi:10.1177/26331055241227220
226. Luckey AM, McLeod LS, Huang Y, Mohan A, Vanneste S. Making memories last using the peripheral effect of direct current stimulation. Elife. 2023;12. doi:10.7554/eLife.75586.
227. Powell K, Lin K, Tambo W, et al. Trigeminal nerve stimulation: a current state-of-the-art review. Bioelectron Med. 2023;9(1):30. doi:10.1186/s42234-023-00128-z
228. Soss J, Heck C, Murray D, et al. A prospective long-term study of external trigeminal nerve stimulation for drug-resistant epilepsy. Epilepsy Behav. 2015;42:44–47. doi:10.1016/j.yebeh.2014.10.029
229. Calderone A, Cardile D, Gangemi A, et al. Traumatic brain injury and neuromodulation techniques in rehabilitation: a scoping review. Biomedicines. 12(2). doi:10.3390/biomedicines12020438
230. Generoso MB, Taiar IT, Garrocini LP, et al. Effect of a 10-day transcutaneous trigeminal nerve stimulation (TNS) protocol for depression amelioration: a randomized, double blind, and sham-controlled Phase II clinical trial. Epilepsy Behav. 2019;95:39–42. doi:10.1016/j.yebeh.2019.03.025
231. Shiozawa P, Fasanella NA, Marinho C, et al. Trigeminal nerve stimulation (TNS) for treating negative symptoms in schizophrenia: a case study. Schizophr Res. 2017;184:139–140. doi:10.1016/j.schres.2016.11.036
232. Shiozawa P, Duailibi MS, da Silva ME, Cordeiro Q, da Silva ME. Trigeminal nerve stimulation (TNS) protocol for treating major depression: an open-label proof-of-concept trial. Epilepsy Behav. 2014;39:6–9. doi:10.1016/j.yebeh.2014.07.021
233. Loo SK, Salgari GC, Ellis A, Cowen J, Dillon A, McGough JJ. Trigeminal nerve stimulation for attention-deficit/hyperactivity disorder: cognitive and electroencephalographic predictors of treatment response. J Am Acad Child Adolesc Psychiatry. 2021;60(7):856–864e1. doi:10.1016/j.jaac.2020.09.021
234. Badran BW, Gruber EM, O’Leary GH, et al. Electrical stimulation of the trigeminal nerve improves olfaction in healthy individuals: a randomized, double-blind, sham-controlled trial. Brain Stimul. 2022;15(3):761–768. doi:10.1016/j.brs.2022.05.005
235. Rigoard P, Billot M, Moens M, et al. Evaluation of external trigeminal nerve stimulation to prevent cerebral vasospasm after subarachnoid hemorrhage due to aneurysmal rupture: a randomized, double-blind proof-of-concept pilot trial (TRIVASOSTIM Study). Int J Environ Res Public Health. 2023;20(10). doi:10.3390/ijerph20105836
236. Liberson WT, Holmquest HJ, Scot D, Dow M. Functional electrotherapy: stimulation of the peroneal nerve synchronized with the swing phase of the gait of hemiplegic patients. Arch Phys Med Rehabil. 1961;42:101–105.
237. Taylor PN, Wilkinson Hart IA, Khan MS, Slade-Sharman DE. Correction of footdrop due to multiple sclerosis using the stimustep implanted dropped foot stimulator. Int J MS Care. 2016;18(5):239–247. doi:10.7224/1537-2073.2015-038
238. Martin D, Patriciu A, Schulz AK, Schackert G. Long-term results following electrical stimulation of the peroneal nerve using the ActiGait(R) system in 33 patients with central drop foot. Innov Surg Sci. 2021;6(1):20191003. doi:10.1515/iss-2019-1003
239. Dunning K, Mw O, Kluding P, McBride K. Peroneal Stimulation for foot drop after stroke: a systematic review. Am J Phys Med Rehabil. 2015;94(8):649–664. doi:10.1097/PHM.0000000000000308
240. Hachisuka K, Ochi M, Kikuchi T, Saeki S. Clinical effectiveness of peroneal nerve functional electrical stimulation in chronic stroke patients with hemiplegia (PLEASURE): a multicentre, prospective, randomised controlled trial. Clin Rehabil. 2021;35(3):367–377. doi:10.1177/0269215520966702
241. Hong Z, Sui M, Zhuang Z, et al. Effectiveness of neuromuscular electrical stimulation on lower limbs of patients with hemiplegia after chronic stroke: a systematic review. Arch Phys Med Rehabil. 2018;99(5):1011–1022e1. doi:10.1016/j.apmr.2017.12.019
242. Chen S, Gao J, Zhou Y, et al. Implications of neuromuscular electrical stimulation on gait ability, balance and kinematic parameters after stroke: a systematic review and meta-analysis. J Neuroeng Rehabil. 2024;21(1):164. doi:10.1186/s12984-024-01462-2
243. Bogan RK, Roy A, Kram J, et al. Efficacy and safety of tonic motor activation (TOMAC) for medication-refractory restless legs syndrome: a randomized clinical trial. Sleep. 46(10). doi:10.1093/sleep/zsad190
244. Marinkovic SP, Miller B, Hughes S, Marinkovic C, Gillen L. Successful bilateral pudendal neuromodulation to treat male detrusor areflexia following severe pubic symphysis fracture, a case report. BMC Urol. 2015;15:115. doi:10.1186/s12894-015-0108-4
245. Deng K, Balog BM, Lin DL, et al. Daily bilateral pudendal nerve electrical stimulation improves recovery from stress urinary incontinence. Interface Focus. 2019;9(4):20190020. doi:10.1098/rsfs.2019.0020
246. Feng X, Lv J, Li M, Lv T, Wang S. Short-term efficacy and mechanism of electrical pudendal nerve stimulation versus pelvic floor muscle training plus transanal electrical stimulation in treating post-radical prostatectomy urinary incontinence. Urology. 2022;160:168–175. doi:10.1016/j.urology.2021.04.069
247. van Balken MR, Vergunst H, Bemelmans BL. Sexual functioning in patients with lower urinary tract dysfunction improves after percutaneous tibial nerve stimulation. Int J Impot Res Sep-Oct. 2006;18(5):470–475. doi:10.1038/sj.ijir.3901457
248. Musco S, Serati M, Lombardi G, et al. Percutaneous tibial nerve stimulation improves female sexual function in women with overactive bladder syndrome. J Sex Med. 2016;13(2):238–242. doi:10.1016/j.jsxm.2015.12.025
249. Kelly SL, Radley SC, Brown SR. Does percutaneous tibial nerve stimulation improve global pelvic function in women with faecal incontinence? Colorectal Dis. 2016;18(5):O158–63. doi:10.1111/codi.13329
250. Jin MY, Rs D, Abd-Elsayed AA. Efficacy of neuromodulation interventions for the treatment of sexual dysfunction: a systematic review. Neuromodulation. 2023;26(8):1518–1534. doi:10.1016/j.neurom.2022.07.004
251. Arruda BS, Reis C, Sermon JJ, Pogosyan A, Brown P, Cagnan H. Identifying and modulating distinct tremor states through peripheral nerve stimulation in Parkinsonian rest tremor. J Neuroeng Rehabil. 2021;18(1):179. doi:10.1186/s12984-021-00973-6
252. Hao MZ, Xu SQ, Hu ZX, et al. Inhibition of Parkinsonian tremor with cutaneous afferent evoked by transcutaneous electrical nerve stimulation. J Neuroeng Rehabil. 2017;14(1):75. doi:10.1186/s12984-017-0286-2
253. Pascual-Valdunciel A, Hoo GW, Avrillon S, et al. Peripheral electrical stimulation to reduce pathological tremor: a review. J Neuroeng Rehabil.;18(1):33. doi:10.1186/s12984-021-00811-9.
254. Wagle Shukla A. Rationale and evidence for peripheral nerve stimulation for treating essential tremor. Tremor Other Hyperkinet Mov. 2022;12:20. doi:10.5334/tohm.685
255. Diamond A, Kenney C, Jankovic J. Effect of vagal nerve stimulation in a case of Tourette’s syndrome and complex partial epilepsy. Mov Disord. 2006;21(8):1273–1275. doi:10.1002/mds.20949
256. Sperling W, Reulbach U, Maihofner C, Kornhuber J, Bleich S. Vagus nerve stimulation in a patient with Gilles de la Tourette syndrome and major depression. Pharmacopsychiatry. 2008;41(3):117–118. doi:10.1055/s-2008-1062698
257. Maiquez BM, Smith C, Dyke K, et al. A double-blind, sham-controlled, trial of home-administered rhythmic 10-Hz median nerve stimulation for the reduction of tics, and suppression of the urge-to-tic, in individuals with Tourette syndrome and chronic tic disorder. J Neuropsychol. 2023;17(3):540–563. doi:10.1111/jnp.12313
258. Iverson AM, Arbuckle AL, Song DY, Bihun EC, Black KJ. median nerve stimulation for treatment of tics: a 4-week open trial with ecological momentary assessment. J Clin Med. 12(7). doi:10.3390/jcm12072545
259. Papadakis M. Wound irrigation for preventing surgical site infections. World J Methodol. 2021;11(4):222–227. doi:10.5662/wjm.v11.i4.222
260. Cheng J, Yang Z, Overstreet CK, Keefer E. Fascicle-specific targeting of longitudinal intrafascicular electrodes for motor and sensory restoration in upper-limb amputees. Hand Clin. 2021;37(3):401–414. doi:10.1016/j.hcl.2021.04.004
261. Eldabe S, Buchser E, Duarte RV. Complications of spinal cord stimulation and peripheral nerve stimulation techniques: a review of the literature. Pain Med. 2016;17(2):325–336. doi:10.1093/pm/pnv025
262. Helm S, Shirsat N, Calodney A, et al. Peripheral nerve stimulation for chronic pain: a systematic review of effectiveness and safety. Pain Ther. 2021;10(2):985–1002. doi:10.1007/s40122-021-00306-4
263. Hatheway J, Hersel A, Song J, et al. Clinical study of a micro-implantable pulse generator for the treatment of peripheral neuropathic pain: 3-month and 6-month results from the COMFORT-randomised controlled trial. Reg Anesth Pain Med. 2024:rapm–2024–106099. doi:10.1136/rapm-2023-105264.
264. Slavin KV, Nersesyan H, Colpan ME, Munawar N. Current algorithm for the surgical treatment of facial pain. Head Face Med. 2007;3(1):30. doi:10.1186/1746-160X-3-30
265. Pritzlaff SG, Jung M, Singh N, et al. A review of the factors and outcomes of institutional interdisciplinary neuromodulation committees: a multicenter experience. Neuromodulation. 2024;27(5):805–811. doi:doi:10.1016/j.neurom.2023.12.003
266. Nayak R, Banik RK. Current innovations in peripheral nerve stimulation. Pain Res Treat. 2018;2018(1):9091216. doi:10.1155/2018/9091216
267. Campbell CM, Jamison RN, Edwards RR. Psychological screening/phenotyping as predictors for spinal cord stimulation. Curr Pain Headache Rep. 2012;17(1):307. doi:10.1007/s11916-012-0307-6
268. Ramineni T, Prusik J, De La Cruz P, et al. The Impact of peripheral nerve stimulation on disability and depression. Neuromodulation. 2016;19(3):306–310. doi:doi:10.1111/ner.12363
269. Schwedt T, Dodick D, Hentz J, Trentman T, Zimmerman R. Occipital nerve stimulation for chronic headache—long-term safety and efficacy. Cephalalgia. 2007;27(2):153–157. doi:10.1111/j.1468-2982.2007.01272.x
270. Gilmore CA, Ilfeld BM, Rosenow JM, et al. Percutaneous 60-day peripheral nerve stimulation implant provides sustained relief of chronic pain following amputation: 12-month follow-up of a randomized, double-blind, placebo-controlled trial. Reg Anesth Pain Med. 2020;45(1):44. doi:10.1136/rapm-2019-100937
271. Mekhail NA, Aeschbach A, Stanton-Hicks M. Cost benefit analysis of neurostimulation for chronic pain. Clin J Pain. 2004;20(6):462–468. doi:10.1097/00002508-200411000-00012
272. Bulsei J, Leplus A, Donnet A, et al. Occipital nerve stimulation for refractory chronic cluster headache: a cost-effectiveness study. Neuromodulation. 2021;24(6):1083–1092. doi:10.1111/ner.13394
273. Kalia H, Thapa B, Staats P, et al. Real-world healthcare utilization and costs of peripheral nerve stimulation with a micro-IPG system. Pain Manag. 2025;15(1):27–36. doi:10.1080/17581869.2025.2449810
274. Char S, Jin MY, Francio VT, et al. Implantable peripheral nerve stimulation for peripheral neuropathic pain: a systematic review of prospective studies. Biomedicines. 2022;10(10). doi:10.3390/biomedicines10102606
275. Cohen SP, Gilmore CA, Rauck RL, et al. Percutaneous peripheral nerve stimulation for the treatment of chronic pain following amputation. Mil Med. 2019;184(7–8):e267–e274. doi:10.1093/milmed/usz114
276. Beauchene C, Zurn CA, Duan W, Guan Y, Sarma SV. The future of therapeutic peripheral nerve stimulation for chronic pain. Annu Rev Control. 2022;54:377–385. doi:doi:10.1016/j.arcontrol.2022.08.001
277. Van Schepdael J, Solvay H. Amiodarone in the treatment of disorders of cardiac rhythm. results of six years of clinical experience (author’s transl). Schweiz Rundsch Med Prax. 1975;64(2):30–34.
278. Kent DT, Zealear D, Schwartz AR. Ansa cervicalis stimulation: a new direction in neurostimulation for OSA. Chest. 2021;159(3):1212–1221. doi:10.1016/j.chest.2020.10.010
279. Olson MD, Junna MR. hypoglossal nerve stimulation therapy for the treatment of obstructive sleep apnea. Neurotherapeutics. 2021;18(1):91–99. doi:10.1007/s13311-021-01012-x
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.