Back to Journals » International Journal of General Medicine » Volume 18
Conditional Survival Rate of Patients Undergoing Gastrectomy with D2 Lymph Node Dissection After Neoadjuvant Chemotherapy: A Retrospective Study
Authors Yang X, Meng F, Cai F, Deng J
Received 22 January 2025
Accepted for publication 15 March 2025
Published 25 March 2025 Volume 2025:18 Pages 1657—1668
DOI https://doi.org/10.2147/IJGM.S514702
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Christian Selinger
Xiuding Yang,* Feiyu Meng,* Fenglin Cai, Jingyu Deng
Department of Gastric Surgery, Tianjin Medical University Cancer Institute and Hospital, National Clinical Research Center for Cancer, Tianjin Key Laboratory of Digestive Cancer; Tianjin’s Clinical Research Center for Cancer, Tianjin, 300060, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jingyu Deng, Department of Gastric Surgery, Tianjin Medical University Cancer Institute and Hospital, West Huan-Hu Road, Ti Yuan Bei, Hexi District, Tianjin, 300060, People’s Republic of China, Email [email protected]
Background: The conditional survival rate is a dynamic estimation method that changes over time. Our research aimed to assesses the conditional disease-specific survival rate and conditional recurrence-free survival rate among patients who undergoing radical gastrectomy for gastric cancer after neoadjuvant chemotherapy.
Methods: This study included 260 patients who undergoing gastrectomy with D2 lymph node dissection after preoperative chemotherapy. The 2-year conditional disease-specific survival rate (CDS2) indicates that patients who have survived for x years after initial treatment will survive for another 2 years, calculated as follows: CDS2 = Disease-Specific Survival (DSS) (x + 2)/ Disease-Specific Survival (x). Similarly, the 2-year conditional recurrence free survival rate (CRFS2) formula is as follows: CRFS2 = Recurrence-Free Survival (RFS) (x + 2)/ Recurrence-Free Survival (x). Cox proportional risk regression analysis was used to identify factors related to DSS and RFS.
Results: The 1-, 3-, and 5-year actuarial DSS rates were 82%, 57.6%, and 50.7%, respectively. According to conditional disease-specific survival rate (CDS) estimation, the CDS2 of patients who have already survived for 1 year, 3 years, and 5 years is 70.2%, 88%, and 93.3%, respectively. The RFS actuarial rates for 1 year, 3 years, and 5 years were 73.1%, 52.5%, and 46.4%, respectively. According to conditional recurrence free survival rate (CRFS) estimation, the CRFS2 of patients who survived for 1 year, 3 years, and 5 years without recurrence was 71.8%, 88.4%, and 100%, respectively. Lymph vessel infiltration, ypN stage, tumor differentiation, TRG grading, and surgical type are risk factors for DSS and RFS.
Conclusion: The CDS and CRFS of patients undergoing gastrectomy with D2 lymph node dissection after neoadjuvant chemotherapy demonstrate gradual increase over time. Patients with adverse tumor characteristics exhibited the most substantial improvement in both CDS and CRFS.
Keywords: gastric cancer, conditional specific survival, conditional recurrence free survival
Graphical Abstract:

Introduction
Gastric cancer is one of the most common digestive system malignancies in the world.1 According to statistics, gastric cancer ranks third in cancer-related deaths, with more than 1 million new cases worldwide each year.2 Due to the lack of specific symptoms, more than 80% of gastric cancer patients are diagnosed at an advanced stage. In recent years, with the development of immunotherapy, targeted therapy and neoadjuvant chemotherapy, the prognosis of gastric cancer patients has been greatly improved, but the five-year survival rate for patients with stage IV gastric cancer remains below 10%.3–5
There is no consensus among different countries on the indications for neoadjuvant chemotherapy. The National Cancer Comprehensive Network Guidelines recommend neoadjuvant chemotherapy for resectable gastric cancer patients with clinical stages of T2N0-3M0.6 However, it has become a consensus that neoadjuvant chemotherapy can reduce tumor pathological stage and improve the survival rate. Accurate prognosis for cancer patients in the early stages in their treatment helps patients and doctors determine the frequency of adjuvant treatment and follow-up while providing prognostic information. In addition, providing timely prognostic information can greatly enhance shared decision-making between patients and healthcare professionals. The risk assessment for the mortality of gastric cancer patients rely on the TNM stage system developed by the United States Joint Commission on Cancer and the International Alliance against Cancer.7 The TNM stage system may provide valuable information for prognostic evaluation, but the survival estimates provided by this method is based on clinical-pathological features obtained post surgery, and the predicted survival estimate remains constant.8 Specifically, the predicted survival estimates remain constant, failing to reflect the changes in risk profiles that occur over time. Recently, a new statistical tool for predicting survival, called nomogram, has been used to assess prognosis with higher accuracy compared to traditional TNM staging systems. However, these methods can only provide a constant survival rate at a certain point in time. In reality, survival time is not only influenced by tumor characteristics, but also by the length of survival time. In fact, the risk of death and recurrence varies over time, and recent studies have shown that the risk of death or recurrence after surgery dynamically changes over time.9
Conditional survival (CS) reports the probability of survival a certificate number of years after diagnosis or treatment based on the time the patient has already survived.10 The conditional survival rate has been applied to various tumors such as colorectal cancer, lung cancer, and kidney cancer.11–13 Therefore, conditional survival analysis may offer more meaningful insights than traditional survival analysis, as it provides a more personalized prognosis over time, helping in the adjustment of postoperative follow-up strategies. Currently, the conditional survival rate of patients undergoing gastrectomy with D2 lymph node dissection for gastric cancer after neoadjuvant chemotherapy has not been studied. The purpose of this study was to assess the conditional survival rate of patients undergoing gastrectomy with D2 lymph node dissection for gastric cancer after receiving neoadjuvant chemotherapy, and to provide support for clinical decision-making by doctors.
Methods
Patient Source
This study included 260 patients with gastric cancer undergoing gastrectomy with D2 lymph node dissection who received preoperative chemotherapy in the Cancer Hospital of Tianjin Medical University from January 2015 to December 2020. This study has been approved by the Ethics Committee of Tianjin Cancer Hospital. All patients were given written informed consent to participate in this study. This study fully followed the principles outlined in the Declaration of Helsinki.
According to NCCN guidelines, patients receiving neoadjuvant chemotherapy have a T-stage greater than T2. The neoadjuvant chemotherapy regimen is mainly based on fluorouracil and platinum drugs, with a small number of cases receiving chemotherapy containing paclitaxel. The inclusion criteria for patients in this study are: (1) preoperative chemotherapy exceeding 2 cycles, (2) gastrectomy with D2 lymph node dissection for gastric cancer after chemotherapy, and (3) postoperative pathological confirmation of gastric adenocarcinoma. The exclusion criteria for patients are: (1) personal history of malignant tumors or distant tumor metastasis; (2) loss of follow-up or lack of clinical pathological data; (3) R1 or R2 resection. Finally, 260 patients were selected for further analysis (Figure S1).
For all patients, the following demographic and pathological features were collected: age, gender, tumor location, tumor size, lymphatic invasion, neural invasion, ypT stage, ypN stage, tumor differentiation, as well as TRG grading, survival time, and survival status. Classify ypT stage and ypN stage according to the 8th edition of AJCC. According to the Guidelines of the Japanese GC Association, upper third of GC (tumor located in the cardia or fundus of the stomach) is defined as adenocarcinoma in the upper third of the stomach. Middle third of GC (tumor located in the body of the stomach) and lower third of GC (tumor located in the pylorus of the gastric antrum) were defined as adenocarcinoma in the middle third and lower third respectively. All patients received standard follow-up. After undergoing gastrectomy with D2 lymph node dissection, patients were followed up every 3 to 6 months until the first 2 years, every 6 months for the next 3 years, and annually thereafter until the end of the study (June 2023) or death. The median follow-up time for the entire cohort was 35 (range 2–90) months.
Statistical Analyses
Continuous variables are represented by mean ± standard deviation (SD) values, while categorical variables are described as counts and proportions. DSS is defined as the time from gastrectomy with D2 lymph node dissection to death caused by gastric cancer. RFS is defined as the time from gastrectomy with D2 lymph node dissection to the first recurrence. DSS and RFS were calculated using the Kaplan-Meier method, and survival was compared using the Log rank test. The multivariate Cox proportional risk regression model was used to evaluate clinical pathological features associated with specific survival and relapse-free survival as independent prognostic factors. Variables with a p value<0.05 in univariate analysis were included in multivariate analysis.
Conditional survival rate originates from the conditional possibility in biostatistics, which describes the additional years of survival of an individual considering that he or she has already been in a specified amount of time. The 2-year conditional disease-specific survival (CS2) at x years indicates the likelihood of an additional 2-year survivorship for a survivor who has already survived for x years after the initial treatment, calculated as follows: CSS2 = DSS (x + 2) / DSS(x). Similarly, the 2-year conditional survival formula for recurrence free survival is as follows: CRFS2 = RFS (x + 2) / RFS(x).
All data were processed using SPSS version 26.0 (IBM Corp, Armonk, NY) and R software (version 4.2.1; R Foundation for Statistical Computing; available at: http://www.r-project.org/). All tests were two-sided with a significance level set to p<0.05.
Results
Clinicopathologic Characteristics
A total of 260 patients who undergoing gastrectomy with D2 lymph node dissection for gastric cancer after neoadjuvant chemotherapy were included in our study. The median age of our study population was 60 years old (IQR, 53–65 years), with most patients being males (N=187; 71.9%). The median tumor size was 4.0 cm (IQR, 2.8–6.0 cm). Almost one-half of the tumors were in the lower one-third of the stomach (N=124; 47.7%). Most patients were classified with ypT3 or ypT4 disease (67.7%; N=176), whereas only a minority of patients had ypT1 or ypT2 disease according to the eighth AJCC TNM stage system (32.3%; N=84). For ypN status, approximately 1 in 3 patients had no LN metastasis (38.5%; N=100). The mean ± SD numbers of metastatic and retrieved LNs were 4.29 ± 7.45 and 38.1 ± 16.37, respectively. (Supplementary Table 1)
Accurate Specific Survival and Recurrence Free Survival
As of the last follow-up, the median follow-up time was 35 months, with 117 deaths from gastric cancer (45%). (Figure 1A) The 1-year, 3-year, and 5-year specific survival rates were 82%, 57.6%, and 50.7%, respectively. In the COX univariate analysis, tumor size, lymphatic infiltration, neural infiltration, ypT stage, ypN stage, tumor differentiation, surgical type, and TRG grading were associated with specific survival (all p<0.05). Multivariate analysis revealed that lymph vessel infiltration, ypN stage, tumor differentiation, surgical type, and TRG grading were significantly correlated with specific survival rates (all p<0.05) (Table 1).
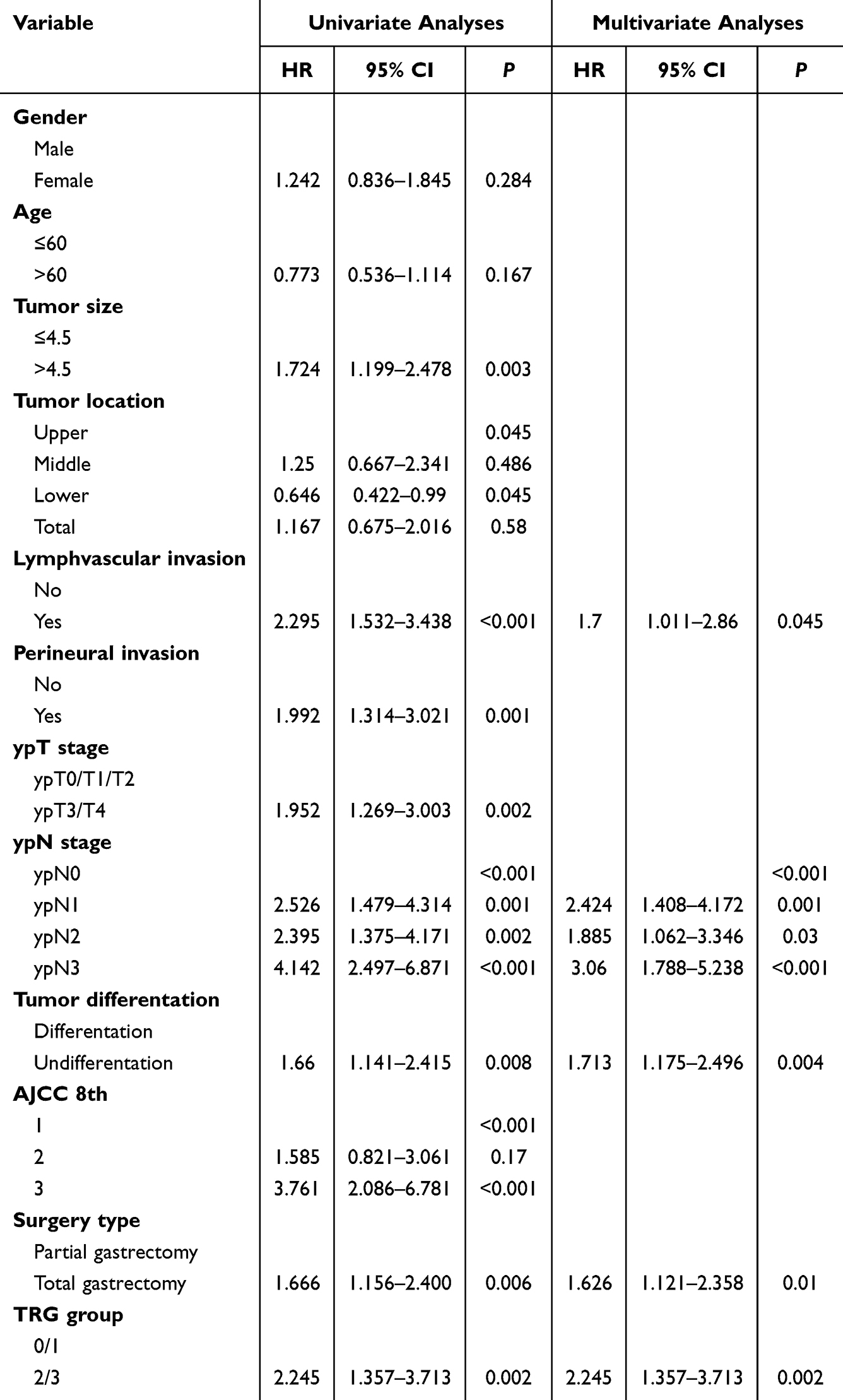 |
Table 1 Univariate and Multivariate Cox Proportional Risk Regression Analysis on Disease Specific Survival Rate |
 |
Figure 1 (A) Actuarial disease-specific survival (Kaplan-Meier survival curve). (B) Actuarial recurrence free survival (Kaplan-Meier survival curve). |
The median follow-up time for recurrence free survival analysis was 31 months, with 129 cases (49.6%) experiencing recurrence. (Figure 1B) The 1-year, 3-year, and 5-year recurrence free survival rates were 73.1%, 52.5%, and 46.4%, respectively. In the COX univariate analysis, tumor size, lymphatic infiltration, neural infiltration, ypT stage, ypN stage, tumor differentiation, AJCCth8 stage, surgical type, and TRG grading were associated with recurrence free survival (all p<0.05). Multivariate analysis revealed that lymph vessel infiltration, ypN stage, tumor differentiation, surgical type, and TRG grading were significantly correlated with the recurrence-free survival rate (all p<0.05) (Table 2).
 |
Table 2 Univariate and Multivariate Cox Proportional Risk Regression Analysis on Recurrence-Free Survival Rate |
Conditional Specific Survival Rate and Conditional Recurrence Free Survival Rate
When we evaluate the risk rate over a period, the risk of death immediately increases in patients undergoing gastrectomy with D2 lymph node dissection after neoadjuvant chemotherapy. The specific survival rate peaked at 13 months (Figure 2A), and the recurrence free survival rate peaked at 10 months (Figure 2B), both of which gradually decreased after reaching their peak. The actuarial DSS over the 2 years after surgery and 2-year CDS for those who had already survived 1 to 5 years after surgery are presented in Figure 2C. For the specific survival rate, the postoperative CDS2 (the probability of surviving to 3 years after surgery for patients who had already survived for 1 year) was 70.2% at 1 year, while the actuarial DSS at 3 years was 57.6%. Similarly, the postoperative CDS2 (the probability of surviving to 7 years after surgery for patients who have already survived for 5 years) was 93.3% at 5 years, while the actuarial DSS at 7 years was 47.3%. Over time, CDS2 increased from 66.5% to 93.3% (p<0.05), while the actuarial DSS decreased from 66.5% at 2 years to 47.3% at 7 years. For the recurrence-free survival rate, the postoperative CRF2 (probability of postoperative recurrence free survival for 3 years in patients who have already survived for 1 year) is 71.8% at 1 year, while the actuarial RFS at 3 years is 52.5%. (Figure 2D) Similarly, the postoperative CRFS2 (probability of postoperative recurrence-free survival for 7 years in patients who had survived for 5 years) was 100% at 5 years, while the actuarial RFS at 7 years was 46.4%. Over time, CRFS2 increased from 59.7% to 100% (p<0.05), while the actuarial RFS decreased from 59.7% at 2 years to 46.4% at 7 years.
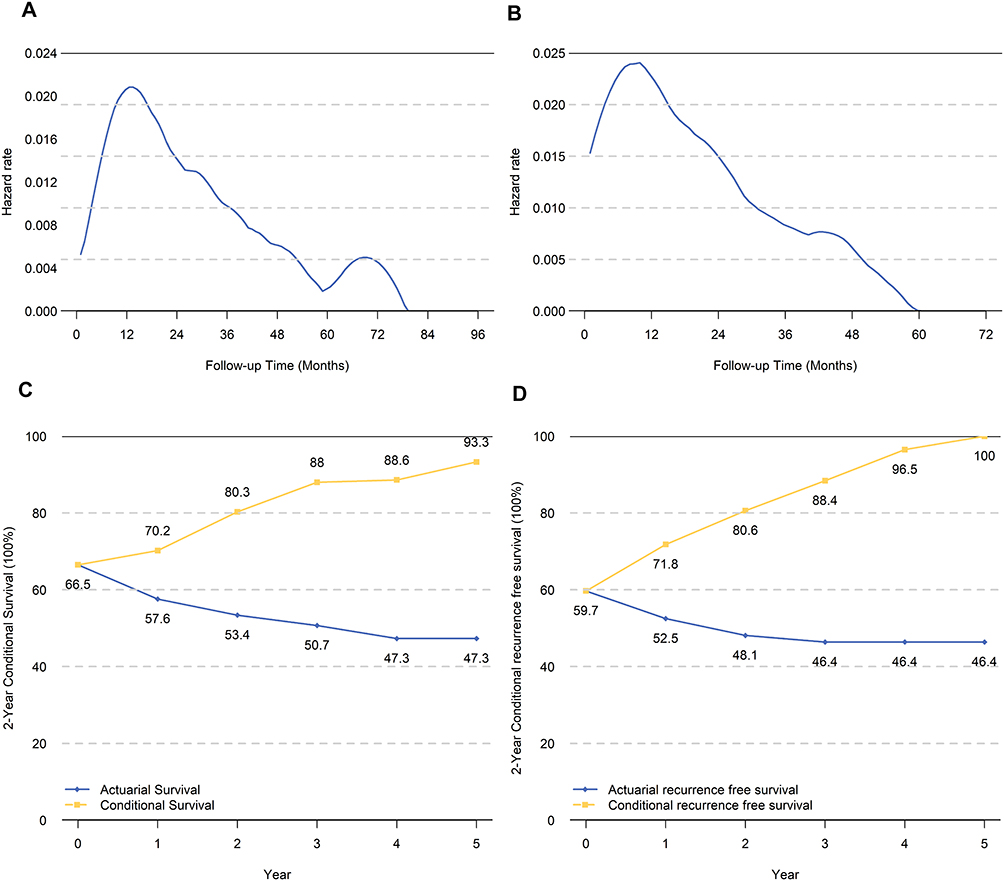 |
Figure 2 (A) Hazard estimates of death from gastric cancer are illustrated for all patients in the cohort. (B) Hazard estimates of gastric cancer recurrence are illustrated for all patients in the cohort. (C) Actuarial 2-year disease-specific survival and conditional 2-year disease-specific survival are compared for all patients in the cohort. (D) Actuarial 2-year recurrence free survival and conditional 2-year recurrence free survival are compared for all patients in the cohort. |
Independent prognostic factors related to DSS and RFS were identified based on Cox multivariate regression analysis, and the impact of clinical pathological features on specific survival and recurrence free survival was evaluated through subgroup analysis. Figures 3 and 4 show the subgroup analysis results for specific survival and recurrence-free survival, respectively. In the subgroup analysis of specific survival and conditional specific survival, the true specific survival rate decreased over time, while the conditional specific survival rate gradually increased after surgery. We obtained similar results in the subgroup analysis of recurrence-free survival and conditional recurrence-free survival. It is worth noting that the difference between actuarial specific survival and conditional specific survival is more significant in patients with initially unfavourable tumor characteristics. In contrast, there is no significant difference in survival rates among patients with initially unfavourable tumor characteristics. Additionally, subgroup analysis revealed significant changes in the conditional survival rate over time for patients with initially unfavourable tumor characteristics. For example, compared to patients without lymphatic invasion (73%-92%; p<0.001), patients with lymphatic invasion had a greater change in conditional specific survival (46–100%; p<0.001). This pattern also occurs in subgroup analyses of recurrence-free survival and conditional recurrence-free survival.
 |
Figure 3 A comparison of (A, C, E, G and I) actuarial disease-specific survival with (B, D, F, H and J) 2-year conditional disease-specific survival is illustrated. Patients were stratified according to (A and B) lymphatic invasion, (C and D) American Joint Committee on Cancer eighth edition tumor classification, (E and F) tumor differentiation, (G and H) surgical approach, (I and J) TRG grading. |
 |
Figure 4 A comparison of (A, C, E, G and I) actuarial recurrence free survival with (B, D, F, H and J) 2-year conditional recurrence free survival is illustrated. Patients were stratified according to (A and B) lymphatic invasion, (C and D) American Joint Committee on Cancer eighth edition tumor classification, (E and F) tumor differentiation, (G and H) surgical approach, (I and J) TRG grading. |
Discussion
The prognosis of gastric cancer patients has greatly improved with the development of immunotherapy, targeted therapy, and neoadjuvant chemotherapy. However, the five-year survival rate of stage IV gastric cancer is less than 10%.14 There are slight differences in the guidelines for neoadjuvant chemotherapy across various countries and regions. The National Comprehensive Cancer Network guidelines recommend neoadjuvant chemotherapy for resectable gastric cancer patients with clinical stages of T2N0-3M0.15 The Chinese Society of Clinical Oncology (CSCO) and the National Health Commission have recommended neoadjuvant chemotherapy in gastric cancer guidelines for patients with advanced gastric cancer who can tolerate surgery in a systemic condition and have a clinical stage of T2-4N0-3M0, which belongs to the category of resectability or potential resectability.16 While there is no consensus among countries regarding the indications for neoadjuvant chemotherapy, it has become a common consensus that neoadjuvant chemotherapy significantly reduce pathological stage and improve the R0 resection rate and 5-year survival rate.17 Indeed neoadjuvant chemotherapy also reduce the risk of recurrence and metastasis, thereby bringing survival benefits to locally advanced gastric cancer patients.18
According to traditional TNM stage prognosis assessment, early gastric cancer patients may have a 5-year survival rate of 90%, while the 5-year survival rate of stage IV gastric cancer patients is only 10%. In theory, the survival rate of patients with advanced gastric cancer decreases over time. In fact, the survival rate dynamically changes over time.19 Dynamic evaluation of the survival rate of patients undergoing gastrectomy with D2 lymph node dissection after neoadjuvant chemotherapy can better guide clinical treatment and follow-up.20 By dynamically evaluating the survival rate of patients, we can better understand the efficacy of neoadjuvant chemotherapy and develop more personalized treatment plans for patients. For example, based on the evaluation results, we can adjust the intensity of subsequent treatments or change treatment strategies. The dynamic evaluation of survival rate can help clinical doctors more accurately determine the prognosis of patients. This is very important for patients’ psychological support, communication with family members, and follow-up plans. Dynamic assessment of patient survival rate can also indicate the recurrence risk of different patients, enabling doctors to monitor more targetedly. Based on the dynamic changes in survival rates and related risk factors, doctors can develop more personalized follow-up plans, such as arranging more frequent examinations or evaluations for high-risk patients to ensure timely detection of problems.
The traditional TNM staging system and the recently emerging column chart have been widely used to evaluate the prognosis of cancer patients. However, these methods can only provide a constant survival rate at a certain point in time. As a new prognostic evaluation indicator, the conditional survival rate can provide more accurate and valuable prognostic information.21 In this study, we evaluated for the first time the conditional specific survival rate and conditional recurrence-free survival rate of patients undergoing gastrectomy with D2 lymph node dissection after neoadjuvant chemotherapy. We found that with the prolongation of postoperative time, the conditional specific survival rate and conditional recurrence free survival rate both increase, which is different from traditional prognostic evaluation systems. Wang et al found in a multicentre study that the conditional survival rate increases over time in patients undergoing gastrectomy with D2 lymph node dissection.22 In reality, patients who survive after danger have a lower mortality rate and a greater chance of survival over time.23 Survival time is not only influenced by tumor characteristics, but also by the length of survival time. For gastric cancer patients, most relapses and deaths occur within two years after surgery. Patients who survive or have no recurrence after this critical period have a lower risk of death and recurrence. This explains the trend of increasing conditional survival rate over time in patients undergoing radical gastrectomy for cancer after neoadjuvant chemotherapy. In the cumulative risk analysis of conditional specific survival, the initial risk of patient death gradually increases, reaching its peak at 2 years, and then gradually decreases. Similar results were obtained for the conditional recurrence-free survival rate.
Our study found that lymphatic invasion, ypN stage, tumor differentiation, TRG grading, and surgical type are risk factors for specific survival and recurrence free survival. These finding are consistent with previous research on factors influencing the prognosis of gastrectomy patients undergoing D2 lymph node dissection.24,25 Further analysis revealed that patients with initially unfavourable oncological features experienced the greatest improvement in both conditional specific survival and conditional recurrence free survival. For example, patients with lymphatic invasion, showed a 54% (46–100%) improvement in 5-year CDS2, while in patients without lymphatic invasion, there was only a 19% (73–92%) improvement in 5-year CDS2. Patients with ypN3 stage disease improved their CRFS2 by 50% (50–100%) over the past 5 years, while patients with ypN0 stage disease only improved their CRF2 by 20% (80–100%) over the past 5 years. Yuhree Kim et al found in a study on conditional disease-free survival after surgery for adrenal cortical cancer that patients with adverse oncological characteristics showed the most significant improvement in conditional disease-free survival.26 This is similar to our research results. The conditional survival rate not only provides more practical prognostic information, but also provides value for guiding postoperative follow-up strategies for patients. For instance, for patients with adverse oncological characteristics, this study suggests that we can increase the frequency of postoperative follow-up.
Our current study has numerous limitations that should be considered. First, our analysis is based on a single centre, retrospective cohort study. The research scale is relatively small, and some analysis results may have limitations. Second, the number of times the patients included in the study received neoadjuvant chemotherapy during the perioperative period varied, and there were also differences in the level of surgical treatment received by patients from different treatment groups, which can also affect specific survival and recurrence-free survival, thus leading to limitations in the results.
Conclusion
In conclusion, this study indicates that the conditional specific survival rate and conditional recurrence free survival rate of patients undergoing gastrectomy with D2 lymph node dissection after preoperative chemotherapy increase with the passage of survival time. Specifically, assuming that the patient survives at 1 year, 3 years, and 5 years, the probability of an additional 2 years of survival is 70.2%, 88%, and 93.3%, respectively. Assuming that the patient has no disease recurrence at 1 year, 3 years, and 5 years, the probability of no recurrence in the next 2 years is 71.8%, 88.4%, and 100%, respectively. Patients who had unfavourable tumor characteristics had the greatest improvement in CDS and CRFS. This method of dynamically estimating survival may help oncologists and patients develop prognostic indicators for treatment decisions, determine follow-up strategies, and predict short-term and long-term survival status.
Data Sharing Statement
The dataset generated and analyzed during the current study is not publicly available due to patient privacy restrictions and ongoing data collection for research purposes but are available from the corresponding author (Jingyu Deng, [email protected]) on reasonable request.
Ethics Approval
This study was performed in line with the principles of the Declaration of Helsinki. Approvals were granted by the Ethics Committee of Tianjin Medical University Cancer Institute and Hospital. All patients were informed and agreed to participate in this study.
Consent for Publication
All authors gave their consent for publication.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas. Xiuding Yang, Feiyu Meng and Fenglin Cai took part in drafting, revising and critically reviewing the article. Jingyu Deng gave final approval of the version to be published. All authors have agreed on the journal to which the article has been submitted. All authors agree to be accountable for all aspects of the work.
Funding
This work was jointly funded by the Tianjin Key Medical Discipline (Specialty) Construction Project (TJYXZDXK-009A), the Distinguished professor of Tianjin (JTZB [2019] No. 120) and the Programs of National Natural Science Foundation of China (No. 81572372).
Disclosure
There are no conflicts of interest or financial ties to disclose from any authors.
References
1. Smyth EC, Nilsson M, Grabsch HI, van Grieken NC, Lordick F. Gastric cancer. Lancet. 2020;396(10251):635–648. doi:10.1016/S0140-6736(20)31288-5
2. Ajani JA, D’Amico TA, Bentrem DJ, et al. Gastric cancer, version 2.2022, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2022;20(2):167–192. doi:10.6004/jnccn.2022.0008
3. Yeong J, Lum HYJ, Teo CB, et al. Choice of PD-L1 immunohistochemistry assay influences clinical eligibility for gastric cancer immunotherapy. Gastric Cancer. 2022;25(4):741–750. doi:10.1007/s10120-022-01301-0
4. Patel TH, Cecchini M. Targeted therapies in advanced gastric cancer. Curr Treat Options Oncol. 2020;21(9):70. doi:10.1007/s11864-020-00774-4
5. Li S, Yu W, Xie F, et al. Neoadjuvant therapy with immune checkpoint blockade, antiangiogenesis, and chemotherapy for locally advanced gastric cancer. Nat Commun. 2023;14(1):8. doi:10.1038/s41467-022-35431-x
6. Wang XZ, Zeng ZY, Ye X, Sun J, Zhang ZM, Kang WM. Interpretation of the development of neoadjuvant therapy for gastric cancer based on the vicissitudes of the NCCN guidelines. World J Gastrointest Oncol. 2020;12(1):37–53. doi:10.4251/wjgo.v12.i1.37
7. He X, Wu W, Lin Z, Ding Y, Si J, Sun LM. Validation of the American Joint Committee on Cancer (AJCC) 8th edition stage system for gastric cancer patients: a population-based analysis. Gastric Cancer. 2018;21(3):391–400. doi:10.1007/s10120-017-0770-1
8. Graziosi L, Marino E, Donini A. Survival comparison in gastric cancer patients between 7th and 8th edition of the AJCC TNM staging system: the first western single center experience. Eur J Surg Oncol. 2019;45(6):1105–1108. doi:10.1016/j.ejso.2018.12.010
9. Machlowska J, Baj J, Sitarz M, Maciejewski R, Sitarz R. Gastric cancer: epidemiology, risk factors, classification, genomic characteristics and treatment strategies. Int J Mol Sci. 2020;21(11). doi:10.3390/ijms21114012
10. Zheng Z, Wang X, Liu Z, Lu X, Huang Y, Chi P. Individualized conditional survival nomograms for patients with locally advanced rectal cancer treated with neoadjuvant chemoradiotherapy and radical surgery. Eur J Surg Oncol. 2021;47(12):3175–3181. doi:10.1016/j.ejso.2021.06.010
11. Han L, Dai W, Mo S, et al. Nomogram of conditional survival probability of long-term survival for metastatic colorectal cancer: a real-world data retrospective cohort study from SEER database. Int J Surg. 2021;92:106013. doi:10.1016/j.ijsu.2021.106013
12. Tichanek F, Forsti A, Hemminki A, Hemminki O, Hemminki K. Survival in kidney and bladder cancers in four Nordic countries through a half century. Cancers. 2023;15(10). doi:10.3390/cancers15102782
13. Yoo JE, Han K, Shin DW, et al. Conditional relative survival and competing mortality in patients who underwent surgery for lung cancer: a nationwide cohort study. Int J Cancer. 2021;148(3):626–636. doi:10.1002/ijc.33239
14. Liang Y, Wu L, Liu L, et al. Impact of extranodal tumor deposits on prognosis and N stage in gastric cancer. Surgery. 2019;166(3):305–313. doi:10.1016/j.surg.2019.04.027
15. Thiels CA, Hanson KT, Habermann EB, Boughey JC, Grotz TE. Integrated cancer networks improve compliance with national guidelines and outcomes for resectable gastric cancer. Cancer. 2020;126(6):1283–1294. doi:10.1002/cncr.32660
16. Wang FH, Zhang XT, Li YF, et al. The Chinese Society of Clinical Oncology (CSCO): clinical guidelines for the diagnosis and treatment of gastric cancer, 2021. Cancer Commun. 2021;41(8):747–795. doi:10.1002/cac2.12193
17. Fong C, Johnston E, Starling N. Neoadjuvant and adjuvant therapy approaches to gastric cancer. Curr Treat Options Oncol. 2022;23(9):1247–1268. doi:10.1007/s11864-022-01004-9
18. Andre T, Tougeron D, Piessen G, et al. Neoadjuvant nivolumab plus ipilimumab and adjuvant nivolumab in localized deficient mismatch repair/microsatellite instability-high gastric or esophagogastric junction adenocarcinoma: the GERCOR NEONIPIGA phase II study. J Clin Oncol. 2023;41(2):255–265. doi:10.1200/JCO.22.00686
19. Wang JB, Zhong Q, Wang W, et al. Postoperative dynamic survival of gastric cancer patients: a multi-institutional, international analysis of 22 265 patients. J Surg Oncol. 2019;120(4):685–697. doi:10.1002/jso.25637
20. Xu SJ, Zhang SY, Dong LY, Lin GS, Zhou YJ. Dynamic survival analysis of gastrointestinal stromal tumors (GISTs): a 10-year follow-up based on conditional survival. BMC Cancer. 2021;21(1):1170. doi:10.1186/s12885-021-08828-y
21. Jung SH, Lee HY, Chow SC. Statistical methods for conditional survival analysis. J Biopharm Stat. 2018;28(5):927–938. doi:10.1080/10543406.2017.1405012
22. Wang P, Sun Z, Wang W, et al. Conditional survival of patients with gastric cancer who undergo curative resection: a multi-institutional analysis in China. Cancer. 2018;124(5):916–924. doi:10.1002/cncr.31160
23. Ayloor Seshadri R, Soman AC, Aggrawal A, Karnawat A, Patidar S, Swaminathan R. Conditional survival in patients treated for gastric cancer with a curative intent. J Surg Oncol. 2023;127(6):937–944. doi:10.1002/jso.27209
24. Chen QY, Xie JW, Zhong Q, et al. Safety and efficacy of indocyanine green tracer-guided lymph node dissection during laparoscopic radical gastrectomy in patients with gastric cancer: a randomized clinical trial. JAMA Surg. 2020;155(4):300–311. doi:10.1001/jamasurg.2019.6033
25. Deng ZJ, Lu J, Nie RC, et al. Indications for adjuvant chemotherapy in stage II gastric cancer after D2 Gastrectomy-A Chinese Multicenter Study. Ann Surg Oncol. 2022;29(13):8214–8224. doi:10.1245/s10434-022-12108-9
26. Kim Y, Margonis GA, Prescott JD, et al. Curative surgical resection of adrenocortical carcinoma: determining long-term outcome based on conditional disease-free probability. Ann Surg. 2017;265(1):197–204. doi:10.1097/SLA.0000000000001527
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.