Back to Journals » Journal of Pain Research » Volume 18
Comprehensive Mechanisms and Non-Invasive Treatment for Complex Regional Pain Syndrome: A Narrative Review
Received 25 April 2025
Accepted for publication 3 September 2025
Published 11 September 2025 Volume 2025:18 Pages 4699—4726
DOI https://doi.org/10.2147/JPR.S534655
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor King Hei Stanley Lam
Hoa Ngan Doan, Min Cheol Chang
Department of Physical Medicine and Rehabilitation, College of Medicine, Yeungnam University, Daegu, Republic of Korea
Correspondence: Min Cheol Chang, Department of Physical Medicine and Rehabilitation, College of Medicine, Yeoungnam University, 317-1, Daemyungdong, Namku, Daegu, 705-717, Republic of Korea, Tel +82-53-620-4682, Email [email protected]
Abstract: Complex Regional Pain Syndrome (CRPS) is a chronic pain condition characterized by an exaggerated response to an initial stimulus, accompanied by autonomic, sensory, motor, and sudomotor dysfunctions. Recognized as a systemic disorder, CRPS involves complex interactions among inflammatory, immunologic, neurogenic, genetic, and psychological factors. The primary mechanisms include peripheral and central sensitization, sympathetic nervous system dysregulation, and altered somatosensory processing. However, the exact pathophysiology remains unclear, contributing to ongoing debate about optimal treatment approaches. Management typically involves a multimodal approach. Pharmacologic options such as corticosteroids, ketamine, and bisphosphonates have demonstrated relative safety and efficacy in clinical practice. Moreover, rehabilitation therapies —including cortically directed sensorimotor rehabilitation, range-of-motion or aerobic exercises, exposure therapy, transcutaneous electrical nerve stimulation, and thermal therapy —serve as valuable nonpharmacologic interventions. No consensus currently exists on standardized treatment protocols for CRPS, particularly regarding the choice of non-invasive approaches. In this context, a comprehensive understanding of the underlying pathophysiological mechanisms is essential for guiding appropriate management strategies. This review provides updated insights into the pathophysiological mechanisms of the disease, alongside a synthesis of evidence-based non-invasive treatment, to support mechanism-driven clinical decision-making, potentially improving treatment outcomes.
Keywords: complex regional pain syndrome, pathophysiology, neuroinflammation, pharmacological therapy, rehabilitation
Introduction
Complex Regional Pain Syndrome (CRPS) is a chronic and debilitating pain condition that typically develops following trauma, operation, or limb immobilization, with a reported prevalence of 5.46 to 26.2 per 100,000 individuals annually.1,2 CRPS occurs more commonly in females than in males, with reported female-to-male ratios ranging from 2:1 to 4:1.3,4 Patients with CRPS often experience substantial socioeconomic challenges. Approximately 30%–40% of affected patients with CRPS are unable to return to their jobs, and 27%–35% require workplace adaptations.5 At diagnosis, total healthcare and pain medication prescription costs are 2.17 and 2.56 times higher than baseline, respectively, peaking within the first year and gradually decreasing over time.6 Overall, their healthcare costs are approximately 20% higher than those of non-CRPS patients.7 Consequently, CRPS is associated with significantly reduced quality of life and represents a notable societal burden.7,8
It is characterized by disproportionate pain not confined to a single peripheral nerve distribution, accompanied by varying combinations of sensory, vasomotor, sudomotor, trophic, and motor abnormalities. CRPS has previously been referred to by several names, including reflex sympathetic dystrophy, causalgia, Sudeck’s atrophy, algoneurodystrophy, and shoulder-hand syndrome.1,2 In 1994, a consensus conference in Orlando standardized the terminology as CRPS. The diagnosis of CRPS lacks specific confirmatory tests and is primarily clinical, based on patient history and symptomatology. In 2003, the Budapest criteria were introduced by the International Association for the Study of Pain (IASP)9 to improve diagnostic consistency and were revised in 2012.10 In 2019, the IASP CRPS Special Interest Group convened a workshop in Valencia and proposed pragmatic updates to diagnostic instructions and taxonomy (Table 1). These revisions refined the definitions of CRPS type II (CRPS II) and CRPS Not Otherwise Specified (NOS), added a third CRPS subtype—CRPS with Remission of Some Features, and clarified symptom assessment procedures, while retaining the original phrasing to preserve criterion validity.11
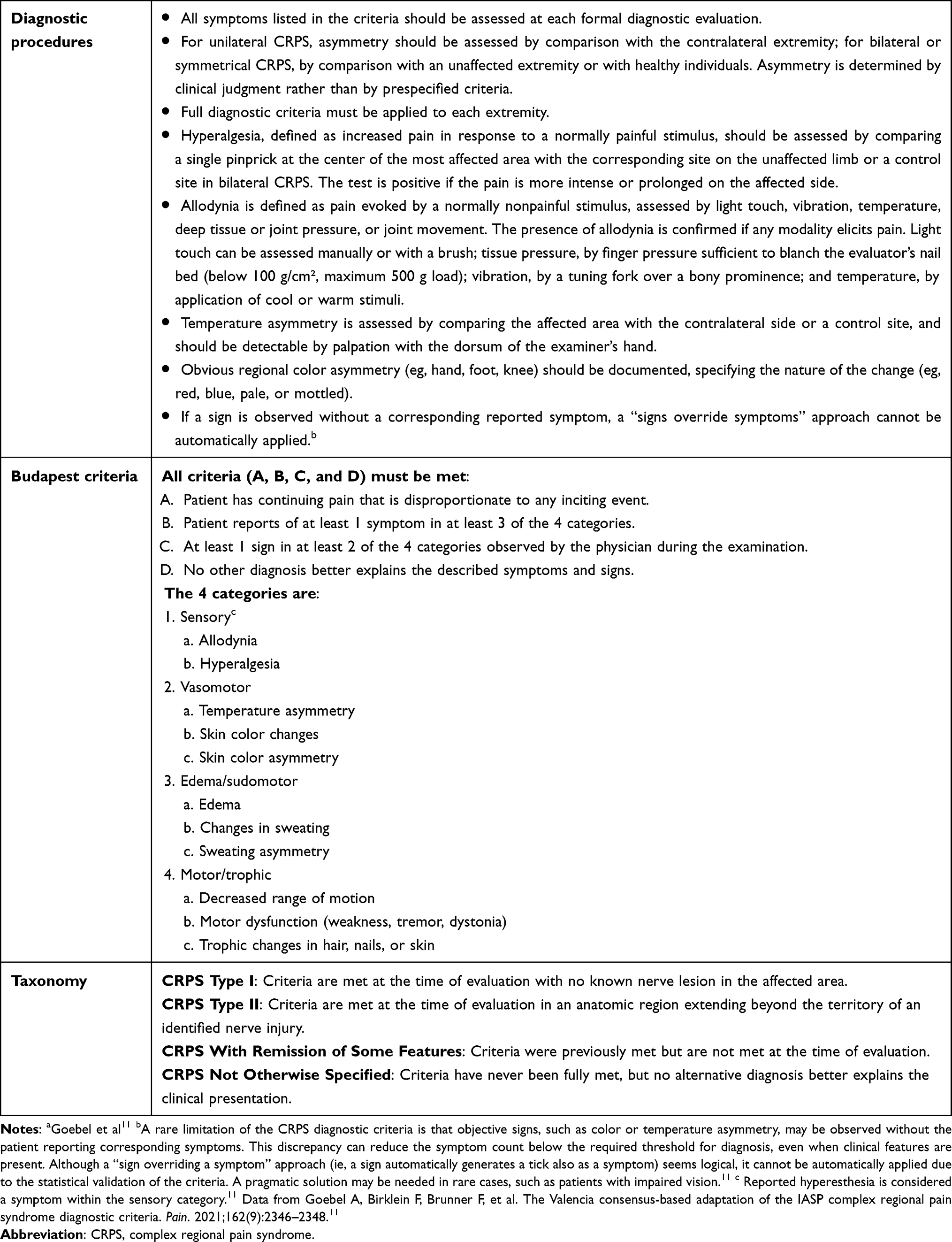 |
Table 1 Diagnostic Procedures, Budapest Criteria, and Taxonomy of Complex Regional Pain Syndrome (CRPS)a |
Many patients with CRPS experience refractory pain that significantly restricts their daily activities. Although a range of therapeutic interventions, including pharmacological, procedural, and rehabilitative therapy, have been explored, pain management is often suboptimal. Effective management requires a comprehensive understanding of CRPS pathophysiology and the available treatment modalities.
This review explores the underlying mechanisms of CRPS and highlights non-invasive treatment approaches—pharmacological and rehabilitative—aiming to support clinical decision-making and improve symptom management. The following sections present the pathophysiological mechanisms of CRPS, pharmacological treatments, and rehabilitative treatment approaches for managing the condition.
Mechanisms of Complex Regional Pain Syndrome
CRPS is a multifactorial syndrome involving an interplay of nociceptive, neuropathic, and nociplastic mechanisms.9 The specific mechanisms of CRPS are illustrated in Figure 1. Understanding these mechanisms enables a shift from symptom-based to mechanism-targeted treatment approaches.12
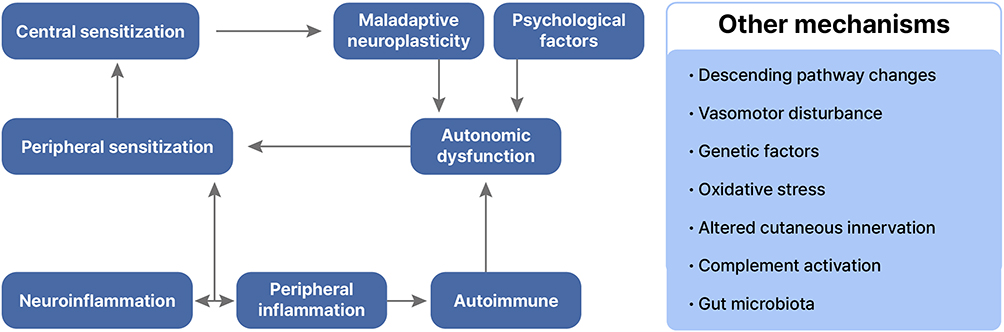 |
Figure 1 Summary of mechanisms of complex regional pain syndrome (CRPS). Notes: Following an inciting event (such as trauma, immobilization, disuse, or hypoxia), peripheral inflammation and neuroinflammation occur, leading to peripheral sensitization and subsequently central sensitization. Central sensitization affects the brain, resulting in maladaptive neuroplasticity. Evidence suggests that autoimmune dysfunction and autonomic disturbances contribute to the pathogenesis of CRPS. Maladaptive plasticity, autoimmune factors, and psychological influences are believed to contribute to autonomic dysfunction are thought to result from autonomic dysfunction, peripheral inflammation, and autoimmunity. Moreover, factors such as vasomotor disturbances; changes in descending pathways; genetic factors; oxidative stress; altered cutaneous innervation; complement activation; and gut microbiota may play a role in CRPS pathophysiology. |
Peripheral Inflammation and Neuroinflammation
Peripheral inflammation represents the biological response to tissue injury and infection, characterized by immune cell activation and the release of inflammatory mediators. Neuroinflammation, occurring in both the peripheral and central nervous systems, involves immune cell infiltration, glial cell activation, and mediator release, contributing to peripheral and central sensitization.13,14 Neuroinflammation is essential in the onset and maintenance of CRPS-related chronic pain.14,15
Trauma is a common precursor to CRPS, with fractures accounting for approximately 44%, sprains for 18%, and elective surgeries for approximately 12% of cases.16 Additional risk factors include limb immobilization, disuse, and tissue hypoxia. Following injury, both innate and adaptive immune cells —including mast cells,17–19 macrophages, monocytes,20,21 and T cells,21,22—the non-immune cells such as keratinocytes23–26 and dendritic cells27 are recruited to the site. These cells release inflammatory mediators, including serotonin, histamine, prostaglandin E2 (PGE2), bradykinin, adenosine triphosphate (ATP), protons (H+), nerve growth factors (NGF), and various cytokines,28,29 which cause vasodilation and increased vascular permeability, manifesting as clinical signs such as warmth, erythema, and edema.
Studies in CRPS have demonstrated a cytokine imbalance characterized by elevated levels of proinflammatory cytokines [tumor necrosis factor-alpha (TNF-α), interleukin-1 beta (IL-1β), and IL-6] and decreased anti-inflammatory cytokines (IL-4 and IL-10) in local blister fluid,30 skin,31 plasma,32 and cerebrospinal fluid.33 These mediators interact with receptors and ion channels on nociceptive peripheral nerve terminals, sensitizing and exciting primary afferent nociceptors (particularly C-fibers), lowering activation thresholds, and inducing ectopic discharges;29 this process constitutes a key mechanism of peripheral sensitization. Therapeutic agents that promote the metabolism of these mediators or inhibit their nociceptor interactions may reduce inflammation and represent a promising avenue for drug development. As multiple mediators and diverse receptors are involved (Figure 2), targeting a single mediator may be insufficient.
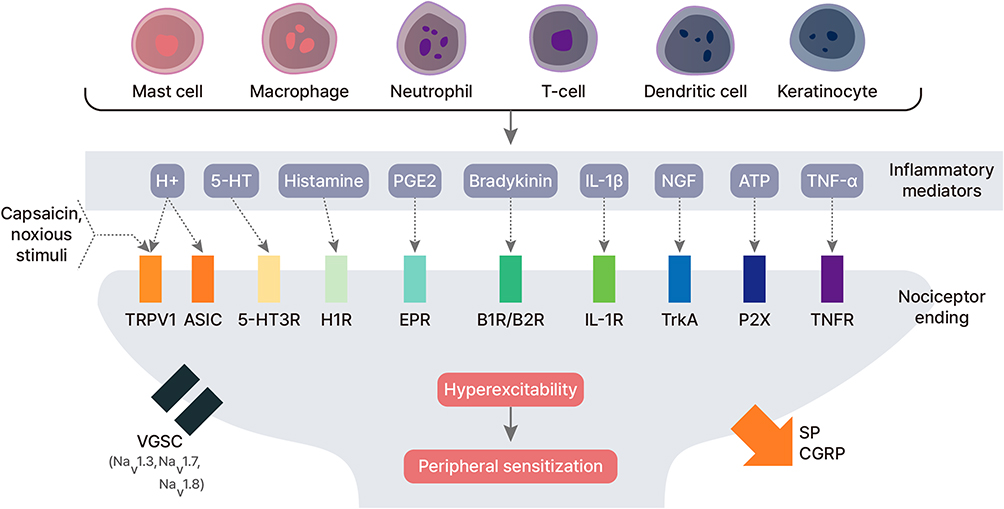 |
Figure 2 Peripheral sensitization in complex regional pain syndrome (CRPS). Abbreviations: TRPV-1, transient receptor potential vanilloid 1; ASIC, acid-sensing ion channel; 5-HT, 5-hydroxytryptamine; 5-HT3R, 5-hydroxytryptamine 3 receptor; H1R, histamine receptor; PGE2, prostaglandin E2; EPR, E prostanoid receptor, B1R/B2R, bradykinin 1 receptor/bradykinin 2 receptor; IL-1β, interleukin-1 beta; IL-1R, interleukin 1 receptor; NGF, nerve growth factor; TrkA, tyrosine kinase A; ATP, adenosine triphosphate; P2X, purinergic receptor of ATP; TNF-α, tumor necrosis factor alpha; TNFR, tumor necrosis factor receptor; VGSC, voltage-gated sodium channels; SP, substance P; CGRP, calcitonin gene-related peptide. Notes: In CRPS, local production and release of inflammatory mediators occur around the primary afferent nociceptor endings due to the activation of both immune and non-immune cells. These mediators interact with their corresponding receptors, resulting in neuronal hyperexcitability and peripheral sensitization. Furthermore, the upregulation of VGSC, including Nav1.3, Nav1.7, and Nav1.8, contributes to the sensitization of primary afferent nociceptors. Activated nociceptors also release SP and CGRP, leading to vasodilation and increased vascular permeability in CRPS. |
The interaction between immune cells and nociceptors is bidirectional and central to CRPS pathogenesis.34 Upon activation, primary afferent nociceptors in the dorsal root ganglion (DRG) release neurotransmitters both centrally and peripherally. Among these, neuropeptides such as calcitonin gene-related peptide (CGRP) and substance P (SP) are pivotal mediators of both peripheral and central sensitization in CRPS.35–37 At peripheral nerve endings, CGRP induces vasodilation,38,39 enhances sweat gland activity,40,41 and stimulates hair follicles,40 resulting in clinical signs such as elevated skin temperature, erythema, excessive sweating, and enhanced hair growth. CGRP-mediated vasodilation also contributes to edema formation.42 SP increases capillary permeability, promoting plasma extravasation and edema.43 Moreover, CGRP and SP activate and recruit immune cells, exacerbating inflammation.38,42,44
At the dorsal horn of the spinal cord, primary afferent nociceptors release neurotransmitters that interact with dorsal horn neurons and activate glial cells, promoting central sensitization. Neurotransmitters such as brain-derived neurotrophic factor (BDNF), SP, and glutamate heighten neural excitability in dorsal horn neurons, marking the onset of central sensitization. Glial cell activation, particularly of microglia and astrocytes, further amplifies this process45–47 and contributes to the chronicity of CRPS.48 Microglia are the first glial cells to respond to peripheral nerve injury, typically activating within 24 hours in the spinal cord and usually subsiding within 3 months.45 Upon activation, microglia express specific markers such as Toll-like receptor 4 (TLR4), regulate immune responses, proliferate, and release proinflammatory mediators. This release creates a proinflammatory milieu in the dorsal horn that sensitizes peripheral afferents and dorsal horn neurons, leading to pain hypersensitivity and persistence.45,48 TLR4 activation enhances proinflammatory cytokine release within the central nervous system, making it a therapeutic target for mitigating neuroinflammation.49 Astrocytes become activated around the third day after injury and may remain active for up to 3 months.45,50 Beyond releasing inflammatory mediators that sensitize secondary neurons in the spinal cord, astrocytes modulate microglial activity and contribute to pain processing in higher-order central nervous system structures.50–52
Peripheral Sensitization
Peripheral sensitization refers to the process by which primary afferent nociceptors lower their activation threshold, become hyperexcitable, and generate spontaneous ectopic discharges.28,53 Inflammation and neuroinflammation are key contributors to this process. Following nerve injury, alterations in ion channel expression further enhance sensitization.29 Increased expression and aberrant distribution of voltage-gated sodium channels (VGSC), including Nav1.3, Nav1.7, and Nav1.8, lowers the activation threshold and promotes ectopic discharges (Figure 2).54 Certain calcium channels (N-type, T-type, and L-type) and potassium channels (hyperpolarization-activated cyclic nucleotide-gated channels) contribute to heightened neuronal excitability.29 Sympathetic sprouting, discussed in Section 2.4, is implicated in developing peripheral sensitization.28
As a result of these mechanisms, primary afferent nociceptors exhibit heightened excitability and spontaneous discharges, contributing to hallmark CRPS symptoms. These include spontaneous pain (from ectopic nociceptor activity), allodynia (due to lowered stimulation thresholds), and primary hyperalgesia (localized to the site of tissue injury due to peripheral sensitization).29
Central Sensitization
Central sensitization refers to a prolonged but reversible increase in the excitability and synaptic efficacy of neurons in the central nervous system. Clinically, it manifests as dynamic tactile allodynia, secondary punctate hyperalgesia, aftersensations, and enhanced temporal summation,46,47,55 which are commonly observed in CRPS. This process is considered a key mechanism underlying chronic pain,47,55 including that seen in CRPS. As previously described, primary afferent nociceptors release neurotransmitters (including SP and glutamate), which activate their respective postsynaptic receptors on second-order neurons in the spinal cord (Figure 3). SP binds to the neurokinin-1 receptor (NK1R), increasing intracellular calcium levels, while glutamate stimulates alpha-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid (AMPA) receptors, leading to further calcium influx and depolarization of postsynaptic neurons. When this depolarization reaches sufficient amplitude and duration, it removes the Mg2+ block on N-methyl-D-aspartate (NMDA) channels, permitting additional calcium entry and further enhancing neuronal excitability.56,57
 |
Figure 3 Central sensitization in complex regional pain syndrome (CRPS). Abbreviations: BDNF, brain-derived neurotrophic factor; SP, substance P; Glu, glutamate; TrkB, tropomyosin receptor kinase B; NK1, neurokinin 1; AMPAR, α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid receptor; NMDAR, N-methyl-D-aspartate receptor. Notes: In CRPS, afferent nociceptor terminals release BDNF, SP, and glutamate. SP acts on NK1 receptors, while glutamate stimulates AMPA receptors, leading to Ca2+ influx into dorsal horn neurons and depolarization. When this depolarization reaches sufficient amplitude and duration, the Mg²⁺ block on NMDA channels is removed, and in combination with the action of glutamate, this facilitates additional Ca²⁺ influx, ultimately leading to neuronal hyperexcitability and central sensitization. Activation of glial cells (microglia and astrocytes) further sensitizes both primary afferent nociceptors and dorsal horn neurons in the spinal cord, contributing to peripheral and central sensitization. |
The activation of NMDA receptors is central to the phenomenon of “wind-up”, which refers to a progressive increase in dorsal horn neuron firing following repeated C-fiber activation, ultimately causing long-term neuroplastic changes in the spinal cord).29 Moreover, glial cell activation (as mentioned in “Peripheral Inflammation and Neuroinflammation” Section) significantly contributes to central sensitization and the persistence of chronic pain.
Autonomic Dysfunction
Sympathetic nervous system dysfunction is a major contributor to CRPS pathogenesis and is frequently referred to as sympathetically maintained pain. In the early stage of CRPS, plasma norepinephrine levels in the affected limb are significantly reduced, indicating diminished sympathetic outflow.58,59 Clinically, this phenomenon presents as vasodilation, redness, warmth, and edema. However, the decreased norepinephrine release may trigger a compensatory upregulation of vascular α1-adrenoceptors, leading to vasoconstriction and the characteristic cold, bluish appearance of the limb during the chronic “cold” phase of CRPS.60 In patients with CRPS, increased expression and density of α-adrenoceptors have been observed in epidermal cells and nociceptors on the affected and unaffected sides compared to healthy controls.61 Epidermal cells expressing α-adrenoceptors, such as keratinocytes, under norepinephrine stimulation, may release proinflammatory mediators that stimulate nociceptors and contribute to peripheral pain. Moreover, sympathetic-afferent coupling, the interactions between sympathetic and sensory nerves that heighten pain sensitivity, plays a significant role in peripheral and central sensitization in CRPS.28 Structural brain changes have also been reported in CRPS, including atrophy in regions associated with autonomic regulation, such as the ventromedial frontal cortex and the right anterior insula, indicating central involvement in autonomic dysfunction.62 Moreover, psychological factors and autoimmune mechanisms are believed to influence autonomic dysfunction and will be discussed in subsequent sections.
Autoimmune Mechanisms
Growing evidence supports an autoimmune component in CRPS pathogenesis. Serological studies have identified previous infections—such as Chlamydia, Parvovirus, and Campylobacter—in patients with CRPS,63–65 prompting Goebel et al to investigate the presence of pathogen-specific antibodies. Their findings revealed significantly elevated immunoglobulin M (IgM) and immunoglobulin G (IgG) titers against specific bacterial and viral surface epitopes in patients with CRPS compared to healthy controls, suggesting abnormal immune responses may lead to cross-reactive autoantibody production.66 Furthermore, CRPS patient sera contain IgG targeting autonomic nervous system components, including β2-adrenergic and muscarinic M2 receptors,67 providing additional evidence for autoimmunity’s contribution to autonomic dysfunction in CRPS. Dharmalingam et al demonstrated that antibodies from patients with CRPS can bind to endothelial cells in vitro, inducing proinflammatory and cytotoxic effects that may contribute to CRPS development.68 Similarly, Dubuis et al found that serum IgG from patients with chronic CRPS targets α-1a adrenergic receptors, modulating cardiomyocyte excitability and supporting an autoimmune mechanism.69 Tékus et al demonstrated that transferring IgG from patients with chronic CRPS into trauma-inflicted mice induced mechanical hyperalgesia, edema, and increased proinflammatory markers, mimicking human CRPS symptoms.70 Guo et al highlighted the role of IgM antibodies in a CRPS mouse model, where bone fractures led to the expression of neoantigens in the limb skin, sciatic nerve, and spinal cord. This antigen expression triggered B-cell production of IgM antibodies bound to these antigens, eliciting a pronociceptive immune response.71 Additionally, the female-to-male ratio in CRPS, ranging from 2:1 to 4:1,2,3 corresponds with the female predominance commonly observed in many autoimmune diseases.72 Given growing evidence for autoimmune mechanisms in CRPS, intravenous immunoglobulin (IVIG) therapy has emerged as a promising treatment option. However, clinical outcomes with IVIG are variable and inconsistent across studies.73,74 This issue will be discussed in greater detail in the treatment section concerning immunoglobulin therapy. The inconsistent findings regarding the efficacy of IVIG limit the strength of the evidence supporting the autoimmune hypothesis in CRPS. Nevertheless, autoimmunity remains a plausible contributing mechanism in the pathogenesis of this condition.
Maladaptive Neuroplasticity
Neuroplasticity, also called neural or brain plasticity, refers to the nervous system’s ability to reorganize its structure, functions, or connections in response to internal or external stimuli.75 In CRPS, neuroplastic changes associated with central sensitization contribute to sensory and motor dysfunctions.
Alterations in the primary somatosensory cortex (S1) have been well-documented in CRPS and are associated with sensory disturbances.76,77 The reorganization of the S1 region representing the affected hand, including a marked reduction in size and a shift toward the cortical representation of the lips, has been correlated with pain severity and mechanical hyperalgesia.78 Importantly, this somatotopic reorganization has been shown to reverse alongside pain reduction.76 The S1 processes tactile input and integrates proprioceptive, vestibular, and visual cues to construct a central somatosensory representation of the body—called the body schema. Disruptions to this neural map have been hypothesized to contribute to body perception disturbances (BPD) in CRPS.77 Pleger et al demonstrated that reorganization in S1 and the secondary somatosensory cortex (S2) is associated with impaired tactile discrimination.79
Neuroimaging studies have linked brain alterations to motor dysfunction in CRPS. Using functional magnetic resonance imaging (fMRI) during finger tapping tasks involving the affected limb, Maihöfner et al reported increased activation in the contralateral primary motor cortex (M1) and supplementary motor area (SMA), both of which were correlated with motor impairment severity.80 Similarly, Freund et al observed heightened activation in the posterior cingulated cortex during painful stimulation, suggesting enhanced motor inhibition. They also observed reduced activity in the opercular region, indicating impaired sensory-discriminative processing compared to healthy controls.81 Furthermore, Azqueta-Gavaldon et al identified abnormalities in M1, SMA, the posterior parietal cortex, and basal ganglia, potentially underlying motor symptoms such as dystonia and reduced range of motion (ROM) in patients with CRPS.82
Visual input is believed to significantly influence pain perception.83,84 Viewing one’s body has been shown to reduce neural responses to pain and lower perceived pain intensity—a phenomenon known as visually induced analgesia.84 However, in some patients with CRPS, ambiguous visual input can trigger pain, sensory disturbances, peripheral vasomotor responses, and even dystonia.85 Hall et al demonstrated that observing a bistable spatial image increased pain intensity and evoked additional symptoms in patients with CRPS.86 Moreover, distorted body perception and cortical reorganization can alter motor and sensory maps, impairing sensorimotor integration and promoting pain development.87–89 In McCabe et al’s study, healthy individuals experienced pain and sensory disturbances, temperature changes, and altered limb perception when performing incongruent limb movements while viewing a mirror reflection, creating a sensory-motor mismatch. These symptoms were reported in the limb hidden behind the mirror, suggesting that visual-proprioceptive incongruence alone can induce pain-like sensations.90
Dysfunction of Descending Inhibitory Pathways
Dysfunction of descending modulatory pathways significantly contributes to CRPS-related pain. Under normal conditions, descending pathways from regions such as the periaqueductal gray-rostral ventromedial medulla system and the dorsal reticular nucleus–ventrolateral medulla exert inhibitory control over spinal nociceptive transmission through neurotransmitters such as serotonin, norepinephrine, dopamine, and endogenous opioids.29,91 However, the balance between descending inhibition and facilitation is disrupted in chronic pain conditions. Reducing noradrenergic inhibitory tone and shifting serotonergic signaling from inhibitory to facilitatory enhances spinal cord excitability and promotes pain transmission.92 The interplay between pain and comorbidities such as sleep disturbances, anxiety, and depression is attributed to the shared involvement of norepinephrine and serotonin in regulating both pain and mood.93 Consequently, monoamine reuptake inhibitors, such as tricyclic antidepressants (TCAs) and selective serotonin-norepinephrine reuptake inhibitors (SNRIs), are effective in alleviating both pain and psychiatric symptoms in patients with CRPS.
Genetic Factors
Increasing evidence implicates genetic predisposition in CRPS pathogenesis. Studies have identified associations between CRPS and several major histocompatibility complex (MHC) alleles, including human leukocyte antigen (HLA)-DR6, HLA-DR13, HLA-DR2, HLA-DQ1, HLA-B62, and HLA-DQ8, as well as a promoter polymorphism in the TNF-α gene.94 Notably, HLA-B62 and HLA-DQ8 have been associated with CRPS with fixed dystonia, while HLA-DQ8 alone is associated with CRPS without dystonia.95,96 The presence of these alleles in affected individuals supports the hypothesis that autoimmune mechanisms may contribute to CRPS pathogenesis.72 Moreover, patients with CRPS exhibit significantly elevated expression of the matrix metalloproteinase 9 (MMP9) gene compared to healthy controls, suggesting a role in pain progression.97 Recent research has also identified several hub genes, including MMP9, Prostaglandin-Endoperoxide Synthase 2 (PTGS2), C-X-C Motif Chemokine Ligand 8 (CXCL8), Oncostatin M (OSM), and Talin 1 (TLN1), as being associated with CRPS, providing novel insights into potential therapeutic targets.98
Psychological Factors
Psychological factors are both potential risk factors and consequences of CRPS.99 The CRPS is associated with adverse psychological outcomes such as depression and anxiety, as well as psychosocial challenges, including reduced quality of life and impaired occupational functioning. Children with CRPS report experiencing more stressful life events than those with other chronic pain conditions, such as headaches or abdominal pain.100 Furthermore, the prevalence of posttraumatic stress disorder (PTSD) is significantly higher in individuals with CRPS than in the general population.101 According to Levit-Binnun et al, disturbances in sensory, motor, and regulatory functions may serve as behavioral indicators of increased vulnerability to future psychological challenges.102
The influence of psychological factors in the development of CRPS has been well-documented. A higher number of stressful life events is associated with an increased risk of developing CRPS type I.103 In an extensive retrospective cohort study, Pereira et al found that those with preexisting anxiety or mood disorders had a significantly elevated risk of CRPS I following fractures (hazard ratio, upper limb: 1.8; lower limb: 2.2).104 Similarly, a meta-analysis on risk factors for CRPS after radius fractures showed that psychiatric conditions significantly increased CRPS incidence (relative risk: 2.04; 95% confidence interval: 1.83–2.28).105
One proposed mechanism linking psychological and psychiatric conditions to CRPS involves chronic stress-induced elevations in systemic catecholamine levels.106 Elevated catecholamine levels may sustain autonomic dysfunction, contributing to CRPS pathogenesis. Moreover, psychological stress is associated with increased production of proinflammatory mediators, potentially exacerbating CRPS-related inflammation.2
Other Mechanisms
Vasomotor Disturbance
In patients with CRPS, the affected limb often exhibits an imbalance between vasoconstrictive and vasodilatory mediators, with elevated endothelin-1 (a potent vasoconstrictor) and reduced nitric oxide (a powerful vasodilator) compared to the unaffected limb.107 This imbalance results in vasoconstriction and tissue hypoxia, promoting acidosis and free radical production. These metabolic changes activate nociceptors and contribute to peripheral sensitization.
Oxidative Stress
Oxidative stress results from an excess of reactive oxygen species (ROS) overwhelming the body’s antioxidant defenses. Free radicals generated via the mitochondrial respiratory chain are hypothesized to contribute to the pathophysiology of CRPS I. Taha et al reported evidence of mitochondrial dysfunction in muscle tissue from patients with CRPS I. However, it remains unclear whether oxidative stress and mitochondrial dysfunction are causative factors or secondary effects of CRPS I.108 Therapeutic strategies targeting mitochondrial dysfunction have included compounds that activate endogenous antioxidant enzymes through nuclear transcription factors such as nuclear factor erythroid 2–related factor 2 (Nrf2) and mitochondria-targeted antioxidants including Mito-Vitamin E and Mito-Coenzyme Q.108
Altered Cutaneous Innervation
Multiple studies have demonstrated altered cutaneous innervation in CRPS. Histopathological analyses of CRPS I-affected limbs have revealed degeneration of small nerve fibers, specifically C and A-delta (Aδ) fibers.109,110 Morellini et al hypothesized that reduced cutaneous nerve fiber density increases the distance between nerve endings and dermal mast cells, weakening chemotactic signaling. Given the critical role of mast cells in immune responses and wound healing, this disruption may prolong inflammation and impair tissue repair.111 Moreover, the upregulation of α1-adrenoceptors in CRPS-affected skin may suppress nerve growth factor production, impairing neurite outgrowth and further disrupting nerve–mast cell communication.111 Conversely, Yvon et al analyzed peripheral nerves in a patient with CRPS; they found selective degeneration of only Aα fibers (responsible for motor function and proprioception) and C fibers (pain perception), while Aδ fibers (nociceptive) remained intact. The loss of Aα fibers may disrupt nerve signaling, leading to aberrant activation of intact Aδ fibers, which mediate pain and autonomic responses.112 Further research is needed to elucidate the precise role of altered cutaneous innervation in CRPS pathophysiology.
Complement Activation
The complement system is a cascade of plasma proteins that, upon activation, initiate enzymatic reactions resulting in cell lysis. Emerging evidence supports the role of complement activation in the pathogenesis of CRPS. In animal models of neuropathic pain following peripheral nerve injury, microglial cells become strongly activated and stimulate various complement components.45 In a study by Shi et al, intraplantar injection of CRPS-derived IgM elevated C5a levels in wild-type mice and increased C1q levels in B-cell-deficient mice. These IgM-induced effects were attenuated by a C5a receptor antagonist (PMX53) or a broad-spectrum cytokine inhibitor (pentoxifylline).113 Further research is needed to clarify the role of the complement system in CRPS and to inform the development of novel therapeutic strategies.
Gut Microbiota
The microbiota-gut-brain axis is believed to contribute to CRPS pathophysiology; however, its role remains unclear. Gut microbiota can interact with immune cells and macrophages through TLRs, triggering the release of proinflammatory mediators. They can also secrete factors that influence nociceptor excitability by targeting receptors on the DRG neurons and modulate glial activity directly or through intermediary pathways.114 Crock et al proposed that gut microbiota influence metabolic pathways, immune responses, and microglial activation, contributing to CRPS development and persistence.115 Reichenberger et al analyzed the gut microbiome of 16 patients with CRPS (including five with intestinal discomfort) and 16 healthy controls using deoxyribonucleic acid (DNA) and ribosomal ribonucleic acid (RNA) sequencing. Patients with CRPS showed significantly more diverse lower gut microbiota and elevated Proteobacteria levels. These alterations were associated with heightened inflammation and microglial activation, potentially contributing to CRPS pathogenesis.116 Further research is needed to clarify the role of microbiota, which may provide a foundation for novel therapeutic strategies in CRPS.
Pharmacological Treatment
The CRPS is a complex disorder with no single causative mechanism. Multiple intricate pathophysiological processes are believed to contribute to its diverse clinical presentations. This complexity presents significant challenges in establishing standardized, evidence-based treatment protocols. Although several therapeutic algorithms using various medications have been proposed, no universal regimen for CRPS treatment currently exists. The key pharmacologic options currently employed in CRPS management are summarized in Table 2 to support clinicians in selecting appropriate pharmacologic interventions tailored to individual patients.
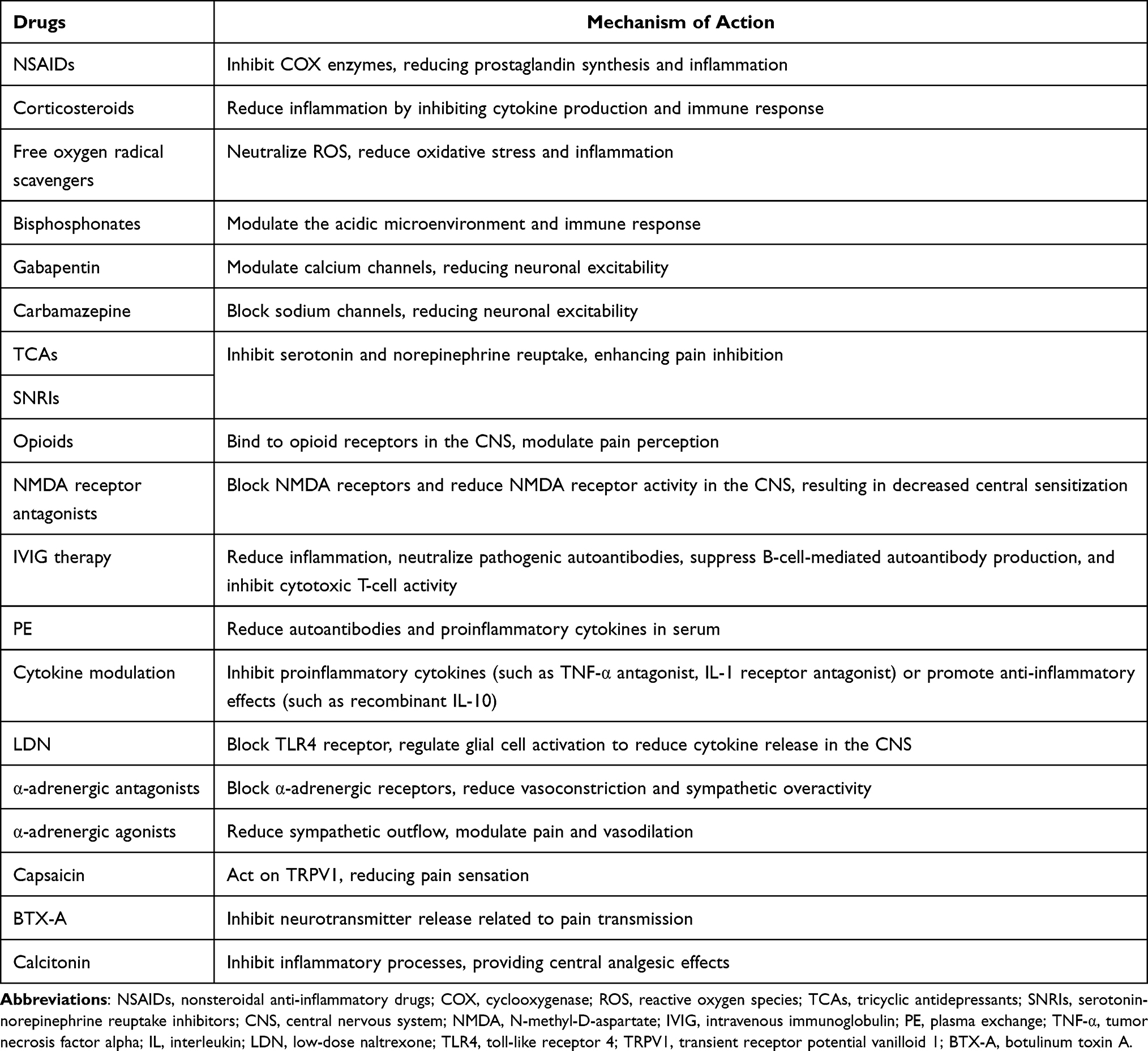 |
Table 2 Mechanisms of Action and Pharmacologic Interventions for Complex Regional Pain Syndrome (CRPS) |
Prevention of CRPS
ROS are known contributors to CRPS development. Vitamin C (ascorbic acid), an antioxidant, neutralizes ROS, protects cell membranes, maintains microcirculatory integrity, reduces vascular permeability and edema, and has been shown to prevent CRPS I following orthopedic surgery or trauma.117 Multiple systematic reviews and meta-analyses have demonstrated that high-dose Vitamin C (ascorbic acid) (500–1000 mg/day for 45–50 days) significantly reduces the incidence of CRPS I following orthopedic procedures.117–121 In these studies, vitamin C was consistently more effective than placebo in preventing CRPS I.118 However, a meta-analysis by Evaniew et al examining patients with distal fractures reported unclear efficacy and low-quality evidence regarding the use of vitamin C for CRPS prevention before surgery.122 Thus, although high-dose vitamin C has demonstrated efficacy in some studies, its routine use for CRPS prevention before surgery remains controversial.
Anti-Inflammatory Drugs
An exaggerated inflammatory response is a central feature of CRPS pathophysiology. Accordingly, anti-inflammatory agents offer a targeted, mechanism-based therapeutic approach. Standard options include nonsteroidal anti-inflammatory drugs (NSAIDs), corticosteroids, and free radical scavengers.
Nonsteroidal Anti-Inflammatory Drugs (NSAIDs)
The NSAIDs exert their effects by inhibiting cyclooxygenase (COX), an enzyme essential for prostaglandin synthesis—key mediators of inflammation and pain.123 Despite their widespread use, evidence supporting the efficacy of selective COX-2 inhibitors (such as celecoxib) in CRPS is limited. A recent meta-analysis by Zhu et al reported no significant difference in therapeutic outcomes between NSAIDs and placebo.124 Furthermore, NSAIDs carry risks of cardiovascular and gastrointestinal side effects, warranting cautious use in clinical practice.125
Corticosteroids
Corticosteroids are frequently employed in CRPS management due to their potent anti-inflammatory properties. They suppress the expression of multiple inflammation-related genes activated during chronic inflammation, thereby alleviating swelling, pain, and immune responses.126 Moreover, corticosteroids may inhibit microglial activation in the central nervous system, thereby reducing central sensitization and promoting pain relief.127 The efficacy of oral corticosteroids in controlling inflammatory symptoms, such as edema, localized warmth, and erythema, in patients with CRPS has been demonstrated in several studies. However, evidence supporting their analgesic effects remains limited.124,128,129 A systematic narrative review by Kwak et al suggests that prednisolone may help alleviate various CRPS symptoms, including pain, sensory and motor disturbances, edema, and limited range of motion.128 A scoping review by Her et al indicates that systemic corticosteroids provide effective short-term pain relief but do not lead to improved functional outcomes.129 However, a meta-analysis by Zhu et al reveals that corticosteroids did not produce significant analgesic effects in the short or long term. Moreover, the study reports that glucocorticoids are safe, exhibiting no significant difference in adverse events compared to that of a placebo.124 Overall, while evidence regarding the analgesic efficacy of systemic corticosteroids in CRPS remains inconsistent, their safety profile appears to be well-established. Regarding dosage, earlier studies administered 30 to 100 mg/day of prednisolone. Conversely, several reports suggest that even 30 mg/day can yield significant clinical benefits, suggesting it is an optimal dose. Moreover, a comparative study found no significant difference in efficacy between low-dose (30 mg/day) and high-dose (60 mg/day) regimens, supporting the lower dose’s effectiveness and safety. While typical treatment duration ranges from 1 to 3 months, shorter courses of 1–2 weeks have shown effectiveness. Approximately 30% of patients may experience mild, reversible side effects, including gastrointestinal discomfort, mood changes, and weight gain.128
Free Radical Scavengers
Antioxidants such as dimethyl sulfoxide (DMSO) and N-acetylcysteine (NAC) have also demonstrated efficacy in CRPS treatment. A 2003 randomized, double-dummy controlled, double-blind trial involving 146 participants revealed that both topical 50% DMSO (applied five times daily) and oral NAC (600 mg, three times daily) administered over 17 weeks were effective in treating CRPS I. DMSO was preferred for warm CRPS I, while NAC appeared to be favored for cold CRPS I. However, the therapeutic efficacy of both agents diminished with longer disease duration.130 A meta-analysis by Zhu et al later reported that DMSO was ineffective for short-term pain relief,124 and the evidence supporting NAC’s benefits in CRPS remains insufficient. Overall, the effectiveness of DMSO and NAC in CRPS management remains controversial.131
Bisphosphonates
Bisphosphonates, primarily known for their anti-osteoclastic properties, have demonstrated analgesic efficacy in treating CRPS.132 However, the exact mechanism underlying their pain-relieving effects remains unclear. A recent study reported elevated osteoblastic activity in acute CRPS, while osteoclastic activity was not elevated. This finding suggests that bisphosphonates work through mechanisms beyond osteoclast inhibition.133 One proposed mechanism involves modulation of the acidic microenvironment characteristic of CRPS. Bisphosphonates may reduce proton concentration in bone tissue, thereby decreasing activation of acid-sensing nociceptors and alleviating pain.134 Moreover, bisphosphonates exhibit immunomodulatory effects, by inhibiting the production of proinflammatory mediators.135–137 Their analgesic benefit may also relate to the clinical presence of osteopenia or osteoporosis in patients with CRPS, conditions that reflect altered bone metabolism and heightened nociceptor sensitivity to mechanical or chemical stimuli. By stabilizing bone turnover and improving bone density, bisphosphonates help alleviate pain in this patient population. A scoping review by Her et al also suggested that oral and intravenous bisphosphonates are effective in reducing pain and improving function in patients with CRPS.129 A meta-analysis by Chevreau et al, incorporating four randomized controlled trials (RCTs) (n=181), found that bisphosphonates significantly reduced pain in the short term (within 40 days) and mid-term (months 2–3) in patients with CRPS I, without serious adverse events.134 In contrast, another meta-analysis by Zhu et al reported no significant pain reduction during the first month but demonstrated meaningful pain relief thereafter, also with a favorable safety profile.124 Despite differences in the timing of therapeutic effects, both meta-analyses support bisphosphonates as an effective and safe treatment option for pain management in patients with CRPS.
Anticonvulsants
Gabapentin, a first-line agent for neuropathic pain,138 exerts its effect by inhibiting the α2δ subunit of voltage-dependent calcium channels, thereby reducing neuronal excitability. However, studies evaluating gabapentin’s role in CRPS are limited. Van de Vusse et al conducted a randomized, double-blind, placebo-controlled crossover study in 58 patients with CRPS I. They found that gabapentin produced mild pain relief and significantly improved sensory deficits in the affected limb.139 In a prospective study by Tan et al, 22 patients with CRPS received an initial gabapentin dose of 600 mg/day, which was titrated until adequate pain control was achieved. The results confirmed gabapentin’s efficacy in pain reduction, although it did not affect other CRPS symptoms.140 Pregabalin, sharing a mechanism similar to gabapentin, is widely used in clinical settings; however, its effectiveness in CRPS is supported only by case reports.141,142
Carbamazepine, a first-line treatment for trigeminal neuralgia, inhibits voltage-gated sodium channels to prevent repetitive neuronal firing.143 In an RCT by Harke et al, 22 patients with CRPS I who had previously responded to spinal cord stimulation were administered 600 mg/day of carbamazepine for 8 days while stimulation was paused. The results suggested modest analgesic benefits.144 Oxcarbazepine, a derivative of carbamazepine with a similar mechanism but fewer adverse effects, has not yet been evaluated in patients with CRPS.2
Clinical evidence supporting the use of anticonvulsants in CRPS remains limited, underscoring the need for further robust research to establish their efficacy.
Drugs Enhancing Descending Inhibitory Activity
Antidepressants, including TCAs and SNRIs, enhance descending inhibitory pain pathways by inhibiting norepinephrine reuptake at the presynaptic membrane. However, research on their effectiveness in CRPS is limited. Brown et al conducted an RCT including 34 patients aged 7–18 years with CRPS I or neuropathic pain, randomly assigning them to receive either 10 mg amitriptyline or 300 mg gabapentin. Both drugs significantly reduced pain intensity and improved sleep, with no significant difference between them in pain relief or sleep outcomes.145 TCAs and SNRIs are established agents in neuropathic pain management.146 Moreover, antidepressants can offer dual benefits in CRPS, as psychiatric comorbidities are common in these patients. The α2-adrenergic agonists, such as clonidine, enhance descending inhibition by stimulating presynaptic α2-receptors in the central nervous system. This inhibitory action reduces excitatory neurotransmitter release and attenuates pain signal transmission at the spinal cord level.
Opioids
Opioids relieve pain in CRPS by binding to mu(µ)-opioid receptors in the central and peripheral nervous systems, inhibiting nociceptive neurotransmission.147 Although they may be effective for short-term pain control in early-stage CRPS, prolonged use is discouraged. Repeated opioid administration can activate glial cells, potentially worsening neuropathic pain.148 While low-dose opioids can be considered as second- or third-line treatment options, dose escalation should be avoided due to the risks of overdose and opioid-induced hyperalgesia. Evidence on the effectiveness of opioids in treating CRPS is very limited. In the two available RCTs,144,149 opioids (morphine) were used in combination with other drugs, making it difficult to isolate their specific therapeutic effect.
NMDA Receptor Antagonists
The activation and upregulation of NMDA receptors in the dorsal horn of the spinal cord play a crucial role in the “wind-up” phenomenon. Increased excitability of primary afferent nociceptors amplifies incoming pain signals, contributing to the development of central sensitization. The NMDA antagonists exert their effects by blocking NMDA receptors, thereby reducing receptor activity in the central nervous system150 and attenuating central sensitization.
Ketamine
Ketamine is a well-known NMDA receptor antagonist. Several studies have highlighted its efficacy in treating CRPS. Sigtermans et al conducted a randomized, double-blind, placebo-controlled trial involving 60 patients with chronic CRPS I; 30 received a 4-day intravenous low-dose ketamine infusion (max 0.43 mg/kg/h), and the other 30 received a placebo. Ketamine significantly reduced pain for up to 11 weeks, although it did not improve functional outcomes. Psychomimetic side effects, such as hallucinations, dysphoria, and derealization, were common but generally tolerable and transient.151 In another randomized, double-blind, placebo-controlled trial, Schwartzman et al studied 19 patients with severe CRPS. Nine received low-dose intravenous ketamine (up to 0.35mg/kg/hour for 4 hours daily over 10 days) and ten received a placebo. The ketamine group experienced significant pain relief lasting up to 12 weeks, with no significant psychomimetic side effects reported.152 According to a meta-analysis by Zhu et al, ketamine provides adequate short-term analgesia in CRPS with moderate certainty and without severe adverse effects.124
Magnesium
Magnesium is a naturally occurring element vital for various cellular processes, including enzyme activation and DNA synthesis. In the nervous system, it functions as a competitive NMDA receptor antagonist, helping modulate abnormal neural activity. However, findings on the effectiveness of magnesium sulfate (MgSO₄) in those with CRPS I have been inconsistent. Collins et al conducted an RCT involving 10 patients with CRPS I, where one group (eight patients) received intravenous MgSO₄ (70 mg/kg), and the other two received 0.9% NaCl over 4 hours daily for 5 days. Results showed significant improvements in pain, function, and quality of life with MgSO₄, which was well tolerated.153 Conversely, Fischer et al replicated this design in a larger RCT, with 29 patients receiving MgSO₄ and 27 receiving a placebo. They concluded that the MgSO₄ offered no significant benefit in chronic CRPS compared to the placebo.154 A recent meta-analysis by Zhu et al also reported that MgSO₄ did not provide substantial short- or long-term pain relief compared to placebo.124
Immune Modulation
Intravenous Immunoglobulin
The mechanism by which IVIG exerts therapeutic effects in CRPS remains unclear. It is believed to work by reducing inflammation, neutralizing pathogenic autoantibodies, suppressing B-cell-mediated autoantibody production, and inhibiting cytotoxic T-cell activity.155 However, RCTs investigating IVIG’s efficacy in CRPS have shown inconsistent results. An RCT by Goebel et al conducted in 2010 reported that low-dose IVIG (0.5 g/kg) reduced pain in patients with refractory CRPS.73 Conversely, a subsequent multicenter, Phase III randomized, placebo-controlled trial by the same group, conducted in 2017, found no significant benefit.74 The discrepancy between these two studies may be attributed to differences in sample size and disease duration.156 In the 2010 study, Goebel et al73 enrolled only 13 patients with CRPS, while the study74 in 2017 included a significantly larger sample of 111 patients. The average duration of CRPS was 1.6 ± 0.7 years and 2.4 ± 0.9 years, respectively, in 201073 and 201774 studies. Therefore, one possible explanation for the greater efficacy of IVIG in the study by Goebel et al in 201073 compared to 201774 is that patients were enrolled at a comparatively earlier stage of the disease. Nevertheless, given these conflicting results and the high cost of IVIG, larger, well-designed studies are needed to determine its actual therapeutic value.
Plasma Exchange
Plasma exchange (PE) therapy, or plasmapheresis, is a promising treatment option for CRPS, particularly due to its presumed autoimmune basis. However, current evidence is limited, primarily comprising retrospective studies,157 case reports,158 and case series.159 In a retrospective study of 33 patients with CRPS, Aradillas et al157 reported significant pain relief in 30 patients with long-standing disease. Sustained improvement was achieved with ongoing maintenance therapy using weekly PE, IVIG, or other immunomodulatory agents.157 Notably, six patients who did not receive maintenance therapy experienced a recurrence of pain to baseline levels. However, evidence supporting the efficacy of PE therapy in CRPS remains limited, as most studies are case reports, case series, or retrospective analyses. Therefore, well-designed prospective studies are needed to verify the therapeutic value of PE.
Cytokine Modulation
Cytokine modulation represents a novel therapeutic approach in CRPS management. Immunomodulatory agents inhibiting proinflammatory cytokines (such as TNF-α antagonists and IL-1 receptor antagonists) or exerting anti-inflammatory effects (such as recombinant IL-10) can reduce peripheral sensitization and relieve pain. The potential of TNF-α antagonists in CRPS has been demonstrated in case reports and one RCT. Huygen et al reported two CRPS I cases successfully treated with infliximab, demonstrating clinical improvement and marked reductions in local TNF-α and IL-6 levels, suggesting a role for anti-TNF therapy.160 In a preliminary double-blind RCT, Dirckx et al studied 13 patients with CRPS (six in the infliximab group and seven in the placebo group). They observed that although infliximab did not yield significant clinical improvement, a trend toward TNF-α reduction indicated potential anti-inflammatory effects.161 In a pilot case series, Eisenberg et al treated 10 patients with CRPS I with subcutaneous adalimumab injections, reporting variable individual responses—some with notable relief and functional improvement—although no significant overall effect was noted.162 Given the low level of evidence, potential cost, and adverse effects—including injection site reactions, infusion reactions, neutropenia, and increased risk of severe infections,163 TNF-α antagonist therapy in CRPS should be approached cautiously and further investigated through higher-quality studies. In CRPS animal models, recombinant IL-10164 and IL-1 receptor antagonists (such as anakinra)165 have shown promising results, warranting additional clinical research to assess their potential in human treatment.
Glial Modulation
Low-Dose Naltrexone
Low-dose naltrexone (LDN) involves administering naltrexone at subtherapeutic doses—typically 1–5 mg per day—much lower than Food and Drug Administration (FDA)-approved levels for opioid or alcohol dependence. LDN has been shown to suppress glial inflammation via TLR4 signaling and enhance endogenous opioid activity through transient opioid receptor blockade.166,167 Chopra et al reported significant clinical improvement in two patients with severe, long-standing CRPS following 2 months of LDN and reduced ketamine usage.166 Similarly, Weinstock et al described a case of chronic CRPS in a patient with Ehlers–Danlos syndrome achieving sustained remission following a multimodal treatment regimen—including LDN—targeting small intestinal bacterial overgrowth, obstructive sleep apnea, and neuroinflammation.168 The LDN is cost-effective, well tolerated, and has no known abuse potential. However, data on optimal dosing and long-term safety remain limited.169 Moreover, as naloxone is an opioid antagonist, it may diminish opioid efficacy if used concurrently. Therefore, the effectiveness and safety of LDN in CRPS should be validated through rigorous, high-quality clinical trials.
Potential Glial Activation Inhibitors
Glial activation inhibitors, such as ibudilast and propentofylline, offer therapeutic effects by acting on glial cells. Ibudilast inhibits TLR4 signaling,170 whereas propentofylline suppresses proinflammatory cytokine production.171 Both ibudilast172–174 and propentofylline173,175 have demonstrated analgesic and anti-allodynia effects in animal models of neuropathic pain, suggesting their potential role in treating CRPS. However, further research is needed to validate their efficacy and safety in clinical settings.
Alpha-Adrenergic Modulators
Alpha-Adrenergic Agonists
Alpha(α)-adrenergic agonists reduce sympathetic activity by mimicking the inhibitory effects of norepinephrine, thereby suppressing preganglionic sympathetic neurons. These agents effectively treat CRPS-related pain, which involves heightened sympathetic nervous system activity.176 Clonidine, the most commonly used α-adrenergic agonist, can be administered orally, transdermally, intravenously, or epidurally.177–179 Epidural clonidine administration provides pain relief for up to six hours in severe CRPS cases, though it is associated with significant side effects, including sedation and hypotension.180 While clonidine is effective in alleviating pain, its systemic use is limited by centrally mediated side effects.
Alpha-Adrenergic Antagonists
Alpha(α)-adrenergic antagonists are used when an overactive sympathetic system causes pain. Phenoxybenzamine and phentolamine, both α-adrenergic antagonists, are occasionally considered third-line treatments for CRPS. However, minimal clinical evidence supports their efficacy, with only a few studies available.2 Furthermore, their use is often limited in practice due to a high incidence of adverse effects, including hypotension, tachycardia, vomiting, dizziness, and headache.49
Topical Treatment
Topical medications act locally by targeting dermal nerve endings, blood vessels, and skin cells. Their primary advantage is a low risk of systemic side effects, with skin irritation and allergic reactions being the primary concerns. Potential topical treatments for CRPS include 5% lidocaine patches, 8-methyl-N-vanillyl-noneamide (capsaicin), and DMSO. The lidocaine 5% patch, commonly used for postherpetic neuralgia,181 may also provide analgesia in CRPS. Capsaicin, a selective transient receptor potential vanilloid 1 (TRPV1) agonist, has demonstrated efficacy in specific neuropathic pain conditions, though evidence for its use in CRPS is limited to a few case reports.182,183 A retrospective study of 12 patients with CRPS suggested capsaicin may help reduce pain intensity and the affected area size.184 However, its application is often limited by intense local burning sensations. The DMSO 50% cream has shown therapeutic benefit in CRPS I.130 Moreover, Russo et al conducted a retrospective study involving 13 patients with CRPS treated with a compound analgesic cream (CAC) containing ketamine 10%, pentoxifylline 6%, clonidine 0.2%, and DMSO 6%-10%, reporting symptom relief in nine patients.185 These findings suggest that this topical combination could be a valuable addition to multimodal therapy for CRPS patients. Previous studies on topical treatment for CRPS are limited; most have a very low level of evidence.
Other Drugs
Botulinum Toxin-A
Botulinum toxin-A (BTX-A), widely used for treating movement disorders and spasticity, modulates neuronal exocytosis and temporarily blocks the presynaptic release of neurotransmitters—primarily acetylcholine and SP—at the neuromuscular junction.186 It also inhibits the release of pain-related neurotransmitters, making it a potential therapy for neuropathic pain.187 However, research on BTX-A for CRPS remains limited and yields mixed outcomes. Carroll et al conducted a randomized, double-blind, crossover trial involving nine patients with refractory CRPS I. They found that adding BTX-A to a lumbar sympathetic block substantially prolonged the anesthesia compared to the block alone (median 71 vs <10 days). The treatment was well tolerated, with minimal adverse events, and considerably reduced the pain intensity over time. These results suggest that sympathetic block combined with BTX-A may offer a promising non-destructive approach to CRPS pain management.188 Similarly, Yoo et al reported in an RCT that lumbar sympathetic block with BTX-A raised the affected foot’s temperature for three months and alleviated pain without severe adverse events.189 Conversely, Safarpour et al conducted a pilot study using intradermal and subcutaneous BTX-A in 14 patients with CRPS-related allodynia and observed no significant pain relief. Most patients discontinued treatment due to poor tolerability and injection-related discomfort.190 In summary, sympathetic ganglion block with BTX-A shows potential as a safe and effective option for CRPS pain relief.186,191 However, further well-designed studies are necessary to support widespread clinical adoption.
Calcitonin
Calcitonin treats CRPS because it inhibits inflammatory processes and provides central analgesic effects.192,193 Gobelet et al conducted a double-blind, randomized study, involving 66 patients with CRPS, dividing them into two groups of 33 each. Group I received 300 IU/day of salmon calcitonin via intranasal spray, while group II received three sprays of a placebo. Both groups received conventional rehabilitative treatment. Their study found that salmon calcitonin significantly improved pain relief and ROM.194 Bickerstaff et al conducted an RCT including 40 patients with CRPS randomized into two groups of 20 for 4 weeks. The intervention group received 400 IU of nasal calcitonin, while the control group received saline. No additional treatments were administered during the study. Results showed no substantial differences in pain reduction, swelling, stiffness, vascular instability, or strength between the calcitonin and placebo groups.195 Sahin et al studied 35 patients with CRPS I in an RCT, dividing them into two groups: one group of 17 patients received paracetamol (1500 mg/day), and the other group of 18 patients received 200 IU/day of salmon calcitonin for 2 months, along with conventional physical therapy. Both groups showed considerable improvement in symptoms such as hyperalgesia, tropic changes, and allodynia, with no significant difference between treatments.196 Due to conflicting results from previous studies, using calcitonin in CRPS remains limited in clinical practice.
Summary of Pharmacological Treatment
Currently, no universally accepted pharmacological treatment is considered optimal for CRPS. However, current evidence allows a tentative ranking of available pharmacological treatments according to their efficacy and the quality of supporting research findings.
Bisphosphonates and ketamine demonstrate the most consistent analgesic efficacy in meta-analyses, reporting no serious adverse events, therefore making them preferred treatment options. Systemic corticosteroids are widely used in clinical practice and are generally regarded as safe; however, their analgesic effectiveness remains controversial across studies.
Neuropathic pain medications—including anticonvulsants (eg, gabapentin, pregabalin), TCAs, and SNRIs—are commonly prescribed for CRPS, but evidence supporting their use in CRPS is limited and is primarily extrapolated from studies on broader neuropathic pain conditions.
Opioids are occasionally prescribed for CRPS, and the evidence supporting their effectiveness is sparse and insufficient to recommend routine use.
Meta-analyses show that NSAIDs, magnesium sulfate, and free radical scavengers (eg, DMSO and NAC) lack significant analgesic benefit and are therefore not recommended as core treatment options.
BTX-A, particularly when administered to the stellate ganglion or other sympathetic regions, demonstrates efficacy and safety in a limited number of studies. However, supporting evidence remains scarce. Calcitonin has yielded conflicting results across studies and is infrequently used in clinical practice. Similarly, alpha-adrenergic modulators are not routinely recommended owing to limited research and a higher risk of adverse effects.
Topical agents, including ketamine cream and lidocaine, remain under-investigated but may offer localized symptom relief.
Finally, emerging therapies, such as immunomodulatory approaches (eg, IVIG and PE) and cytokine or glial cell modulation (eg, TNF-α antagonists and LDN), show preliminary promise in small studies and case reports, but high-quality clinical trials are needed to validate their efficacy and safety.
Future pharmacological research in CRPS should prioritize high-quality RCTs to confirm the efficacy and safety of promising agents such as bisphosphonates and ketamine. Additionally, further studies are needed to better define the role of routinely used medications such as systemic corticosteroids and neuropathic pain medications (anticonvulsants, TCAs, and SNRIs). Emerging therapies—including immunomodulatory agents (eg, IVIG and PE) and cytokine or glial modulators (eg, TNF-α antagonists and LDN)—also warrant further investigation. Future trials should also be designed to account for different CRPS subtypes and disease stages, facilitating the identification of patient groups most likely to benefit from targeted treatment approaches. Additionally, greater attention should be given to evaluating the long-term efficacy of pharmacological treatments.
Rehabilitation
Rehabilitation is considered one of the primary treatment options for patients with CRPS,197 as it has been reported to be effective in managing symptoms. This approach emphasizes an interdisciplinary or multidisciplinary strategy focused on pain reduction and functional restoration.
Cortically Directed Sensory-Motor Rehabilitation
Patients with CRPS may experience neglect-like symptoms, where the affected limb feels foreign (“cognitive neglect”), and directed mental and visual attention is required to move it (“motor neglect”).198 As described in the mechanism of CRPS section, cortical reorganization is thought to cause disturbances in body perception. This reorganization correlates with pain intensity and mechanical hyperalgesia,78 and it can reverse in parallel with clinical improvements in CRPS.76 Furthermore, incongruence between motor intention, proprioception, and vision in patients with CRPS is hypothesized to contribute to the affective sensation of pain. The goal of cortically directed sensory-motor rehabilitation is to reverse cortical reorganization, restore the integrity of sensorimotor cortical information processing, or both.198–200 This training includes mirror therapy (MT), graded motor imagery (GMI), and virtual reality (VR).
Mirror Therapy
Mirror therapy (MT) involves the movement of the extremities within a mirror box, where the visual feedback of the affected hand is replaced with that of the unaffected hand reflected in the mirror (Figure 4). MT is believed to aid in reversing cortical changes and restoring accurate sensorimotor processing in the brain.198 Several studies have investigated the effectiveness of MT in treating CRPS. Cacchio et al conducted an RCT involving 48 patients with CRPS I with upper extremity involvement, dividing them into two groups: the MT group (n=24) and the control group (n=24). Both groups participated in a 4-week standard stroke rehabilitation program consisting of five 1-hour sessions weekly, including neurorehabilitation, occupational therapy, and optional speech therapy.201 The MT group received additional MT, starting with 30 minutes per session in the first 2 weeks and 1 hour per session in the final 2 weeks. At the 6-month follow-up, the MT group showed significant improvements in pain relief, functional ability, and mean performance time, while the control group exhibited no notable changes. Considerable differences were observed in the MT group compared to the control group, after treatment and at the 6-month follow-up. Pervane Vural et al conducted an RCT on 30 patients with CRPS I with upper limb involvement following a stroke, randomly assigning them to the MT group (n=15) or the control group (n=15). Both groups participated in a 4-week conventional stroke rehabilitation program (5 days/week, 2–4 hours/day), which included neurodevelopmental facilitation techniques, occupational therapy, physiotherapy, and speech therapy (if required).202 The MT group also received 30 minutes of daily MT. Both groups showed significant improvements in pain relief and independent motor function, with the MT group demonstrating more substantial gains, including significant improvements in hand and arm motor recovery and hand function. In an RCT involving 38 patients with CRPS with upper limb involvement following a stroke, Saha et al reported that MT significantly improved edema, pain, and hand function, with significant differences compared to the control group.203 Shafiee et al conducted a meta-analysis and demonstrated that adding MT to conventional stroke rehabilitation results in substantial improvements in pain [standardized mean difference (SMD): 1.88, 95% CI: 0.73 to 3.02] and disability (SMD: 1.3, 95% CI: 0.11 to 2.49) in patients with CRPS I after stroke, with effects lasting up to 6 months.204 More extensive studies involving patients with various CRPS classifications are needed to more accurately assess the effectiveness of MT.
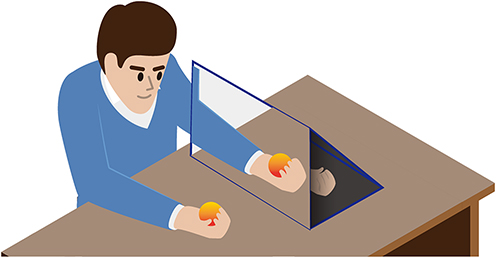 |
Figure 4 Mirror therapy for complex regional pain syndrome (CRPS). This figure illustrates a patient with CRPS affecting the left hand. The patient positions the left hand behind a mirror, and the therapist demonstrates a simple hand movement. The patient is instructed to replicate the movement with both hands, focusing on the reflection of the right (unaffected) hand in the mirror. |
Graded Motor Imagery
Graded motor imagery (GMI) is known to help reverse cortical alterations and restore precise sensorimotor processing in patients with CRPS.200 GMI comprises hand laterality recognition, imagined hand movements, and MT (Figure 5). Moseley et al conducted an RCT with 13 patients with chronic CRPS, dividing them into two groups: an intervention group (received GMI and conventional treatment, n=7) and a control group (received conventional treatment only, n=6).200 Each component was conducted over 2 weeks. The study found that GMI significantly reduced pain compared to the control group after 12 weeks of follow-up. In the meta-analysis by Shafiee et al, GMI was shown to lead to significant improvements in pain (SMD 1.36, 95% CI 0.75 to 1.96) and disability (SMD 1.64, 95% CI: 0.53 to 2.74) in patients with CRPS.204
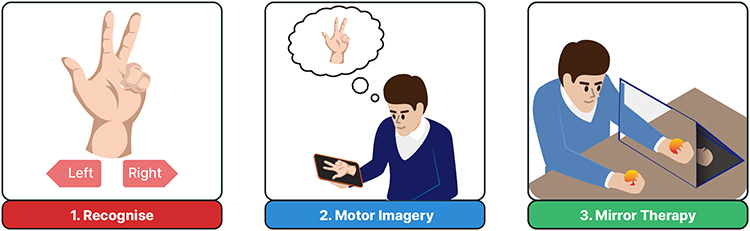 |
Figure 5 Graded motor imagery program for complex regional pain syndrome (CRPS). The graded motor imagery program consists of three sequential components, each typically lasting about two weeks: (1) recognition of hand laterality, (2) imagined hand movements, and (3) mirror therapy. (1) Patients with CRPS are asked to determine whether the pictured limbs are left or right. (2) Patients view images of the affected limb (in this case, the left hand) performing simple activities and are instructed to mentally simulate these movements. (3) For mirror therapy, the affected hand is placed behind a mirror, and patients focus on the reflection of the unaffected hand while replicating movements with both hands. |
Virtual Reality
Virtual reality (VR) therapy has been developed to treat chronic pain and has shown promising outcomes for various conditions, including CRPS.205 The VR therapy aims to replace real sensory experiences with a simulated, computer-generated environment.206 It is hypothesized that VR therapy can promote brain reorganization, which can help relieve pain in patients with CRPS.207 Moreover, VR therapy assists in developing coping skills, supports daily activities, boosts mood, and reduces the fear of movement, all of which positively impact CRPS treatment. Lewis et al conducted an RCT involving 45 patients with refractory upper-limb CRPS and BPD. In the intervention group (n=23), patients viewed a digital image of their affected hand for one minute, which was modified based on their description of how they wanted it to appear. The control group (n=22) viewed the unaltered image.208 Lewis et al found that visual body illusion improved pain and BPD in those with chronic CRPS, with pain reduction lasting at least 2 weeks.208 Several other studies also reported the positive effects of VR therapy on pain relief or BPD improvement in CRPS.209–212 However, further high-quality studies are needed to draw definitive conclusions about the effectiveness of VR therapy in CRPS treatment.
Exercise
Exercise is increasingly recognized for its potential to alleviate pain and improve physical function in CRPS. Exercise benefits CRPS treatment through mechanisms such as central and peripheral nervous system remodeling, vasodilation regulation, adrenaline level modulation, endogenous opioid release, and increased anti-inflammatory cytokines.213 Exercise in CRPS should follow a gradual progression, starting with passive ROM exercises, then transitioning to active ROM exercises, followed by stress loading, aerobic training, and eventually load-bearing exercises.2
Oh et al reported a case of CRPS I in which the patient showed reduced pain and swelling, along with functional improvement, after 20 days of passive ROM exercises administered under sedation.214
Topcuoglu et al conducted a 4-week prospective RCT involving 40 patients with post-stroke CRPS I with affected upper limbs, randomly assigned to an intervention group (n=20) receiving arm crank ergometry (5 W/min, 5 days a week, for 30 minutes per session) combined with conventional physiotherapy, and a control group (n = 20) receiving only conventional physiotherapy.215 The intervention group reported significantly greater pain relief compared to controls. Shafiee et al, in a meta-analysis, demonstrated that incorporating aerobic exercise into conventional treatment significantly improved CRPS-related pain (SMD 0.86, 95% CI 0.23 to 1.5).204
Additional exercise approaches, including strength training, proprioception exercises, functional task practice, postural training, and hydrotherapy, are also used in CRPS management,216 though further studies are needed to confirm their effectiveness.
Exposure Therapy
Exposure therapy involves gradually confronting situations or activities that provoke fear. In CRPS, it can help reduce kinesiophobia and fear of skin contact, alleviating psychological symptoms and promoting greater engagement in rehabilitation. Consequently, exposure therapy may contribute to pain reduction in patients with CRPS.
Pain exposure physical therapy (PEPT) is a commonly used exposure therapy technique for patients with CRPS. The PEPT combines physical exercise with the management of pain-avoidance behaviors to treat chronic pain. Ek et al reported a case series of 106 patients with CRPS I treated with PEPT. In their study, 95 patients (90%) showed functional improvement in the affected limbs, and 49 (46%) achieved full functional recovery after 3 months of treatment. Moreover, 75 patients (71%) experienced pain reduction, and only four discontinued due to increased pain. The authors concluded that PEPT is effective and safe for CRPS management.217 Similarly, Van de Meent et al evaluated PEPT in 20 patients with CRPS I in a multiple single-case design study and supported its safety and effectiveness.218 Barnhoorn et al conducted an RCT involving 56 patients with CRPS I, with 28 receiving PEPT and 28 receiving conventional treatment. The PEPT group demonstrated greater pain relief and improved active ROM.219 Den Hollander et al conducted another RCT involving 46 patients with CRPS I, where 23 patients receiving pain exposure (including daily activity training and education) showed significantly more pain reduction than those receiving conventional pain-reducing therapy (n=23).220 Based on the studies by Barnhoorn et al and den Hollander et al, a meta-analysis by Shafiee et al also confirmed that pain exposure therapy leads to significant pain reduction (SMD 0.81, 95% CI 0.12 to 1.49), with effects lasting up to six months post-treatment.204
Moreover, tactile and thermal desensitization techniques are frequently used in clinical CRPS management; however, no clinical trials have evaluated their efficacy.
Transcutaneous Electrical Nerve Stimulation
Transcutaneous electrical nerve stimulation (TENS) delivers electrical currents to stimulate nerves and modulate pain perception.221 It is widely used in clinical settings for pain management. Although its precise mechanisms remain unclear, TENS is believed to work via the gate control theory of pain,221 the release of endogenous opioids,222 reduction in central excitability, and peripheral α-adrenergic receptor blockade.222 Bilgili et al conducted an RCT involving 30 patients with upper-extremity CRPS I, randomly assigned to two groups. The experimental group (n=15) received 20 minutes of active TENS, while the control group (n=15) received sham TENS. Patients in the experimental group showed significantly greater improvements in pain, edema, and ROM in the second and third fingers compared with controls.223
Thermal Therapy
Thermal therapy, including the application of heat or cold, is another approach used in CRPS management. Fluidotherapy circulates warm, dry air and fine solid particles to deliver heat and tactile stimulation to affected limbs, thereby alleviating pain.224 Sezgin Ozcan et al in an RCT administered 15 sessions of fluidotherapy (five sessions/week in 3 weeks) alongside conventional stroke rehabilitation to 15 patients with post-stroke CRPS I. Outcomes were compared with another 15 patients with post-stroke CRPS I who received only conventional stroke rehabilitation. The group receiving fluidotherapy demonstrated greater reductions in neuropathic pain and edema.224 Sethy et al in an RCT compared fluidotherapy combined with stress-loading exercises (n=11) to routine occupational therapy (n=11), and reported significantly greater improvements in pain, arm function, and disability in patients receiving the combined intervention.225
Contrast bath therapy, another commonly used thermal intervention in clinical practice, involves alternating immersion of the affected limb in warm and cold water. Protocols vary in temperature ranges, immersion times, and overall duration. Cold water typically ranges from 7.2°C to 22°C, and warm water from 26.7°C to 45°C. A standard protocol begins with 10 minutes in warm water, alternated with a 1-minute dip in cold water, followed by alternating 4 minutes in warm water and 1 minute in cold water for 3–4 cycles over 30 minutes. Some protocols omit the initial warm phase and use a 4:1 or 3:1 warm-to-cold ratio.226 Although the exact mechanism remains unclear, contrast bath therapy is believed to induce cycles of vasodilation and vasoconstriction, producing a vascular pumping effect that enhances tissue perfusion and oxygenation, thereby reducing edema and pain.227 Furthermore, it has been shown to significantly reduce sympathetic activity on the affected side in patients with post-stroke CRPS.228
Summary of Rehabilitation
Rehabilitation plays a key role in the multidisciplinary management of CRPS, aiming to alleviate pain, restore limb function, and prevent chronic disability. Although studies remain limited, approaches such as MT, GMI, and PEPT show promising analgesic effects and are considered potential therapeutic options. Other physiotherapeutic interventions may also offer benefits; however, given the limited available evidence, their effectiveness should be interpreted with caution. Moreover, most rehabilitation studies for patients with CRPS have small sample sizes and are primarily focused on individuals with CRPS type I. Therefore, to establish more comprehensive evidence on rehabilitation strategies for CRPS, future studies should prioritize high-quality RCTs involving patients with different CRPS subtypes. Additionally, greater emphasis should be placed on evaluating the long-term effectiveness of rehabilitation interventions.
Conclusion
CRPS is a multifactorial condition involving a complex interplay of immune and neuroimmune responses, peripheral and central sensitization, autonomic dysregulation, and maladaptive neuroplasticity. Nonetheless, a comprehensive understanding of CRPS pathophysiology has remained necessary, especially to resolve ongoing controversies related to mechanisms such as autoimmunity. The involvement of various mechanisms in CRPS highlights the need for individualized, multidisciplinary therapeutic strategies. Although several pharmacological options have been proposed, there is insufficient evidence to fully support their effectiveness and safety. Corticosteroids, ketamine, and bisphosphonates appear to be relatively safe and effective options for clinical use. Moreover, rehabilitation approaches, including cortically directed sensory-motor rehabilitation, ROM or aerobic exercises, exposure therapy, TENS, and thermal therapy, should be considered integral components of CRPS treatment. Currently, no universally accepted pharmacological or rehabilitative “best treatment” approach exists for CRPS, forcing clinicians to base their therapeutic decisions on the best available evidence. Therefore, future research should prioritize high-quality, large-scale, and long-term clinical trials to help establish standardized treatment protocols, ultimately improving prognosis and quality of life for patients with CRPS.
Funding
This work was supported by the National Research Foundation of Korea grant funded by the Korean government (MSIT) (No. RS-2023-00219725).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Todorova J, Dantchev N, Petrova G. Complex regional pain syndrome acceptance and the alternative denominations in the medical literature. Med Princ Pract. 2013;22(3):295–300. doi:10.1159/000343905
2. Harden RN, McCabe CS, Goebel A, et al. Complex regional pain syndrome: practical diagnostic and treatment guidelines, 5th edition. Pain Med. 2022;23(Suppl 1):S1–S53. doi:10.1093/pm/pnac046
3. Lima Pessôa B, Netto JGM, Adolphsson L, et al. Complex regional pain syndrome: diagnosis, pathophysiology, and treatment approaches. Cureus. 2024;16(12):e76324. doi:10.7759/cureus.76324
4. Pérez Vertti Valdés M, Jüngel A, Bitterli P, et al. Identification of two biological subgroups of complex regional pain syndrome type 1 by transcriptomic profiling of skin and blood in women. Mol Med. 2025;31(1):94. doi:10.1186/s10020-025-01148-y
5. Johnson S, Cowell F, Gillespie S, et al. Complex regional pain syndrome what is the outcome? a systematic review of the course and impact of CRPS at 12 months from symptom onset and beyond. Eur J Pain. 2022;26(6):1203–1220. doi:10.1002/ejp.1953
6. Elsamadicy AA, Yang S, Sergesketter AR, et al. Prevalence and cost analysis of complex regional pain syndrome (CRPS): a role for neuromodulation. Neuromodulation. 2018;21(5):423–430. doi:10.1111/ner.12691
7. Duong HP, Léger B, Scholz-Odermatt SM, et al. Healthcare costs, time to fitness for work, and related factors in chronic complex regional pain syndrome: a comparative and longitudinal study of 5-year follow-up. J Pain Res. 2023;16:683–693. doi:10.2147/JPR.S400659
8. Van Velzen GAJ, Perez RSGM, Van Gestel MA, et al. Health-related quality of life in 975 patients with complex regional pain syndrome type 1. Pain. 2014;155(3):629–634. doi:10.1016/j.pain.2013.12.017
9. Mangnus T, Dirckx M, Huygen FJ. Different types of pain in complex regional pain syndrome require a personalized treatment strategy. J Pain Res. 2023;16:4379–4391. doi:10.2147/JPR.S432209
10. Abd-Elsayed A, Stark CW, Topoluk N, et al. A brief review of complex regional pain syndrome and current management. Ann Med. 2024;56(1):2334398. doi:10.1080/07853890.2024.2334398
11. Goebel A, Birklein F, Brunner F, et al. The Valencia consensus-based adaptation of the IASP complex regional pain syndrome diagnostic criteria. Pain. 2021;162(9):2346–2348. doi:10.1097/j.pain.0000000000002245
12. Mangnus TJP, Bharwani KD, Dirckx M, et al. From a symptom-based to a mechanism-based pharmacotherapeutic treatment in complex regional pain syndrome. Drugs. 2022;82(5):511–531. doi:10.1007/s40265-022-01685-4
13. Matsuda M, Huh Y, Ji RR. Roles of inflammation, neurogenic inflammation, and neuroinflammation in pain. J Anesth. 2019;33(1):131–139. doi:10.1007/s00540-018-2579-4
14. Ji RR, Xu ZZ, Gao YJ. Emerging targets in neuroinflammation-driven chronic pain. Nat Rev Drug Discov. 2014;13(7):533–548. doi:10.1038/nrd4334
15. Shi Y, Gelman BB, Lisinicchia JG, et al. Chronic-pain-associated astrocytic reaction in the spinal cord dorsal horn of human immunodeficiency virus-infected patients. J Neurosci. 2012;32(32):10833–10840. doi:10.1523/JNEUROSCI.5628-11.2012
16. De Mos M, De Bruijn AGJ, Huygen FJPM, et al. The incidence of complex regional pain syndrome: a population-based study. Pain. 2007;129(1):12–20. doi:10.1016/j.pain.2006.09.008
17. Huygen FJPM, Ramdhani N, Van Toorenenbergen A, et al. Mast cells are involved in inflammatory reactions during complex regional pain syndrome type 1. Immunol Lett. 2004;91(2–3):147–154. doi:10.1016/j.imlet.2003.11.013
18. Dirckx M, Groeneweg G, Van Daele PLA, et al. Mast cells: a new target in the treatment of complex regional pain syndrome? Pain Pract. 2013;13(8):599–603. doi:10.1111/papr.12049
19. Schlereth T, Birklein F. Mast cells: source of inflammation in complex regional pain syndrome? Anesthesiology. 2012;116(4):756–757. doi:10.1097/ALN.0b013e31824bb143
20. Trevisan G, Benemei S, Materazzi S, et al. TRPA1 mediates trigeminal neuropathic pain in mice downstream of monocytes/macrophages and oxidative stress. Brain. 2016;139(Pt 5):1361–1377. doi:10.1093/brain/aww038
21. Kobayashi Y, Kiguchi N, Fukazawa Y, et al. Macrophage-T cell interactions mediate neuropathic pain through the glucocorticoid-induced tumor necrosis factor ligand system. J Biol Chem. 2015;290(20):12603–12613. doi:10.1074/jbc.M115.636506
22. Russo MA, Fiore NT, Van Vreden C, et al. Expansion and activation of distinct central memory T lymphocyte subsets in complex regional pain syndrome. J Neuroinflammation. 2019;16(1):63. doi:10.1186/s12974-019-1449-9
23. Piipponen M, Li D, Landén NX. The immune functions of keratinocytes in skin wound healing. Int J Mol Sci. 2020;21(22):8790. doi:10.3390/ijms21228790
24. Ji RR, Chamessian A, Zhang YQ. Pain regulation by non-neuronal cells and inflammation. Science. 2016;354(6312):572–577. doi:10.1126/science.aaf8924
25. Talagas M, Lebonvallet N, Berthod F, et al. Cutaneous nociception: role of keratinocytes. Exp Dermatol. 2019;28(12):1466–1469. doi:10.1111/exd.13975
26. Dussor G, Koerber HR, Oaklander AL, et al. Nucleotide signaling and cutaneous mechanisms of pain transduction. Brain Res Rev. 2009;60(1):24–35. doi:10.1016/j.brainresrev.2008.12.013
27. Russo M, Georgius P, Santarelli DM. A new hypothesis for the pathophysiology of complex regional pain syndrome. Med Hypotheses. 2018;119:41–53. doi:10.1016/j.mehy.2018.07.026
28. Gierthmühlen J, Binder A, Baron R. Mechanism-based treatment in complex regional pain syndromes. Nat Rev Neurol. 2014;10(9):518–528. doi:10.1038/nrneurol.2014.140
29. Cohen SP, Mao J. Neuropathic pain: mechanisms and their clinical implications. BMJ. 2014;348(feb05 6):f7656. doi:10.1136/bmj.f7656
30. Lenz M, Üçeyler N, Frettlöh J, et al. Local cytokine changes in complex regional pain syndrome type I (CRPS I) resolve after 6 months. Pain. 2013;154(10):2142–2149. doi:10.1016/j.pain.2013.06.039
31. Krämer HH, Eberle T, Üçeyler N, et al. TNF-alpha in CRPS and ‘normal’ trauma – significant differences between tissue and serum. Pain. 2011;152(2):285–290. doi:10.1016/j.pain.2010.09.024
32. Üçeyler N, Eberle T, Rolke R, et al. Differential expression patterns of cytokines in complex regional pain syndrome. Pain. 2007;132(1):195–205. doi:10.1016/j.pain.2007.07.031
33. Alexander GM, Van Rijn MA, Van Hilten JJ, et al. Changes in cerebrospinal fluid levels of pro-inflammatory cytokines in CRPS. Pain. 2005;116(3):213–219. doi:10.1016/j.pain.2005.04.013
34. Pinho-Ribeiro FA, Verri WA, Chiu IM. Nociceptor sensory neuron–immune interactions in pain and inflammation. Trends Immunol. 2017;38(1):5–19. doi:10.1016/j.it.2016.10.001
35. Littlejohn G. Neurogenic neuroinflammation in fibromyalgia and complex regional pain syndrome. Nat Rev Rheumatol. 2015;11(11):639–648. doi:10.1038/nrrheum.2015.100
36. Li WW, Guo TZ, Shi X, et al. Substance P spinal signaling induces glial activation and nociceptive sensitization after fracture. Neuroscience. 2015;310:73–90. doi:10.1016/j.neuroscience.2015.09.036
37. Gradl G, Finke B, Schattner S, et al. Continuous intra-arterial application of substance P induces signs and symptoms of experimental complex regional pain syndrome (CRPS) such as edema, inflammation and mechanical pain but no thermal pain. Neuroscience. 2007;148(3):757–765. doi:10.1016/j.neuroscience.2007.06.024
38. Chiu IM, Von Hehn CA, Woolf CJ. Neurogenic inflammation and the peripheral nervous system in host defense and immunopathology. Nat Neurosci. 2012;15(8):1063–1067. doi:10.1038/nn.3144
39. Sohn I, Sheykhzade M, Edvinsson L, et al. The effects of CGRP in vascular tissue - classical vasodilation, shadowed effects and systemic dilemmas. Eur J Pharmacol. 2020;881:173205. doi:10.1016/j.ejphar.2020.173205
40. Hagner S, Haberberger RV, Overkamp D, et al. Expression and distribution of calcitonin receptor-like receptor in human hairy skin. Peptides. 2002;23(1):109–116. doi:10.1016/S0196-9781(01)00586-1
41. Schlereth T, Dittmar JO, Seewald B, et al. Peripheral amplification of sweating – a role for calcitonin gene‐related peptide. J Physiol. 2006;576(Pt 3):823–832. doi:10.1113/jphysiol.2006.116111
42. Mashaghi A, Marmalidou A, Tehrani M, et al. Neuropeptide substance P and the immune response. Cell Mol Life Sci. 2016;73(22):4249–4264. doi:10.1007/s00018-016-2293-z
43. Saria A. Substance P in sensory nerve fibres contributes to the development of oedema in the rat hind paw after thermal injury. British J Pharmacol. 1984;82(1):217–222. doi:10.1111/j.1476-5381.1984.tb16461.x
44. Assas BM, Pennock JI, Miyan JA. Calcitonin gene-related peptide is a key neurotransmitter in the neuro-immune axis. Front Neurosci. 2014;8:23. doi:10.3389/fnins.2014.00023
45. Mika J, Zychowska M, Popiolek-Barczyk K, et al. Importance of glial activation in neuropathic pain. Eur J Pharmacol. 2013;716(1–3):106–119. doi:10.1016/j.ejphar.2013.01.072
46. Latremoliere A, Woolf CJ. Central sensitization: a generator of pain hypersensitivity by central neural plasticity. J Pain. 2009;10(9):895–926. doi:10.1016/j.jpain.2009.06.012
47. Woolf CJ. Central sensitization: implications for the diagnosis and treatment of pain. Pain. 2011;152(3):S2–S15. doi:10.1016/j.pain.2010.09.030
48. Wen B, Pan Y, Cheng J, et al. The role of neuroinflammation in complex regional pain syndrome: a comprehensive review. J Pain Res. 2023;16:3061–3073. doi:10.2147/JPR.S423733
49. Candan B, Gungor S. Current and evolving concepts in the management of complex regional pain syndrome: a narrative review. Diagnostics. 2025;15(3):353. doi:10.3390/diagnostics15030353
50. Cheng T, Xu Z, Ma X. The role of astrocytes in neuropathic pain. Front Mol Neurosci. 2022;15. doi:10.3389/fnmol.2022.1007889
51. Lu HJ, Gao YJ. Astrocytes in chronic pain: cellular and molecular mechanisms. Neurosci Bull. 2023;39(3):425–439. doi:10.1007/s12264-022-00961-3
52. Ji RR, Donnelly CR, Nedergaard M. Astrocytes in chronic pain and itch. Nat Rev Neurosci. 2019;20(11):667–685. doi:10.1038/s41583-019-0218-1
53. Devor M. Sodium channels and mechanisms of neuropathic pain. J Pain. 2006;7(1 Suppl 1):S3–S12. doi:10.1016/j.jpain.2005.09.006
54. Basbaum AI, Bautista DM, Scherrer G, et al. Cellular and molecular mechanisms of pain. Cell. 2009;139(2):267–284. doi:10.1016/j.cell.2009.09.028
55. McClain BC. Primary and secondary hyperalgesia. In: The Essence of Analgesia and Analgesics.
56. VanDongen A, Blanke M. Activation mechanisms of the nmda receptor. In: Biology of the NMDA Receptor. Vol. 20085482. CRC Press/Taylor Francis; 2009: 283–312. https://www.ncbi.nlm.nih.gov/books/NBK5283/
57. Brodin E, Ernberg M, Olgart L. Neurobiology: general considerations – from acute to chronic pain. Nor Tannlegeforen Tid. 2016;126(1):28–33.
58. Harden RN, Duc TA, Williams TR, et al. Norepinephrine and epinephrine levels in affected versus unaffected limbs in sympathetically maintained pain. Clin J Pain. 1994;10(4):324–330. doi:10.1097/00002508-199412000-00014
59. Knudsen LF, Terkelsen AJ, Drummond PD, et al. Complex regional pain syndrome: a focus on the autonomic nervous system. Clin Auton Res. 2019;29(4):457–467. doi:10.1007/s10286-019-00612-0
60. Drummond PD, Drummond ES, Dawson LF, et al. Upregulation of α1-adrenoceptors on cutaneous nerve fibres after partial sciatic nerve ligation and in complex regional pain syndrome type II. Pain. 2014;155(3):606–616. doi:10.1016/j.pain.2013.12.021
61. Finch PM, Drummond ES, Dawson LF, et al. Up-regulation of cutaneous α1 -adrenoceptors in complex regional pain syndrome type I. Pain Med. 2014;15(11):1945–1956. doi:10.1111/pme.12548
62. Geha PY, Baliki MN, Harden RN, et al. The brain in chronic CRPS pain: abnormal gray-white matter interactions in emotional and autonomic regions. Neuron. 2008;60(4):570–581. doi:10.1016/j.neuron.2008.08.022
63. Goebel A, Vogel H, Caneris O, et al. Immune responses to Campylobacter and serum autoantibodies in patients with complex regional pain syndrome. J Neuroimmunol. 2005;162(1–2):184–189. doi:10.1016/j.jneuroim.2005.01.018
64. Goebel A, Schedel R, Frosch M, et al. IgA Seropositivität für Chlamydia pneumoniae, aber nicht Chlamydia trachomatis, ist assoziiert mit Komlexem Regionalem Schmerzsyndrom (CRPS). Der Schmerz. 2000;14:70–71.
65. Gross O, Tschernatsch M, Bräu ME, et al. Increased seroprevalence of parvovirus B 19 IgG in complex regional pain syndrome is not associated with antiendothelial autoimmunity. Eur J Pain. 2007;11(2):237–240. doi:10.1016/j.ejpain.2006.01.006
66. Goebel A, Blaes F. Complex regional pain syndrome, prototype of a novel kind of autoimmune disease. Autoimmun Rev. 2013;12(6):682–686. doi:10.1016/j.autrev.2012.10.015
67. Kohr D, Singh P, Tschernatsch M, et al. Autoimmunity against the β2 adrenergic receptor and muscarinic-2 receptor in complex regional pain syndrome. Pain. 2011;152(12):2690–2700. doi:10.1016/j.pain.2011.06.012
68. Dharmalingam B, Singh P, Schramm P, et al. Autoantibodies from patients with complex regional pain syndrome induce pro-inflammatory effects and functional disturbances on endothelial cells in vitro. Pain. 2022;163(12):2446–2456. doi:10.1097/j.pain.0000000000002646
69. Dubuis E, Thompson V, Leite MI, et al. Longstanding complex regional pain syndrome is associated with activating autoantibodies against alpha-1a adrenoceptors. Pain. 2014;155(11):2408–2417. doi:10.1016/j.pain.2014.09.022
70. Tékus V, Hajna Z, Borbély É, et al. A CRPS-IgG-transfer-trauma model reproducing inflammatory and positive sensory signs associated with complex regional pain syndrome. Pain. 2014;155(2):299–308. doi:10.1016/j.pain.2013.10.011
71. Guo TZ, Shi X, Li WW, et al. Passive transfer autoimmunity in a mouse model of complex regional pain syndrome. Pain. 2017;158(12):2410–2421. doi:10.1097/j.pain.0000000000001046
72. David Clark J, Tawfik VL, Tajerian M, et al. Autoinflammatory and autoimmune contributions to complex regional pain syndrome. Mol Pain. 2018;14:1744806918799127. doi:10.1177/1744806918799127
73. Goebel A, Baranowski A, Maurer K, et al. Intravenous immunoglobulin treatment of the complex regional pain syndrome: a randomized trial. Ann Intern Med. 2010;152(3):152–158. doi:10.7326/0003-4819-152-3-201002020-00006
74. Goebel A, Bisla J, Carganillo R, et al. Low-dose intravenous immunoglobulin treatment for long-standing complex regional pain syndrome: a randomized trial. Ann Intern Med. 2017;167(7):476–483. doi:10.7326/M17-0509
75. Mateos-Aparicio P, Rodríguez-Moreno A. The impact of studying brain plasticity. Front Cell Neurosci. 2019;13:66. doi:10.3389/fncel.2019.00066
76. Maihöfner C, Handwerker HO, Neundörfer B, et al. Cortical reorganization during recovery from complex regional pain syndrome. Neurology. 2004;63(4):693–701. doi:10.1212/01.WNL.0000134661.46658.B0
77. Bailey J, Nelson S, Lewis J, et al. Imaging and clinical evidence of sensorimotor problems in crps: utilizing novel treatment approaches. J Neuroimmune Pharmacol. 2013;8(3):564–575. doi:10.1007/s11481-012-9405-9
78. Maihöfner C, Handwerker HO, Neundörfer B, et al. Patterns of cortical reorganization in complex regional pain syndrome. Neurology. 2003;61(12):1707–1715. doi:10.1212/01.WNL.0000098939.02752.8E
79. Pleger B, Ragert P, Schwenkreis P, et al. Patterns of cortical reorganization parallel impaired tactile discrimination and pain intensity in complex regional pain syndrome. Neuroimage. 2006;32(2):503–510. doi:10.1016/j.neuroimage.2006.03.045
80. Maihöfner C, Baron R, DeCol R, et al. The motor system shows adaptive changes in complex regional pain syndrome. Brain. 2007;130(Pt 10):2671–2687. doi:10.1093/brain/awm131
81. Freund W, Wunderlich AP, Stuber G, et al. Different activation of opercular and posterior cingulate cortex (PCC) in patients with complex regional pain syndrome (CRPS I) compared with healthy controls during perception of electrically induced pain: a functional MRI study. Clin J Pain. 2010;26(4):339–347. doi:10.1097/AJP.0b013e3181cb4055
82. Azqueta‐Gavaldon M, Schulte‐Göcking H, Storz C, et al. Basal ganglia dysfunction in complex regional pain syndrome – a valid hypothesis? Eur J Pain. 2017;21(3):415–424. doi:10.1002/ejp.975
83. Mancini F, Longo MR, Kammers MPM, et al. Visual distortion of body size modulates pain perception. Psychol Sci. 2011;22(3):325–330. doi:10.1177/0956797611398496
84. Longo MR, Betti V, Aglioti SM, et al. Visually induced analgesia: seeing the body reduces pain. J Neurosci. 2009;29(39):12125–12130. doi:10.1523/JNEUROSCI.3072-09.2009
85. Cohen HE, Hall J, Harris N, et al. Enhanced pain and autonomic responses to ambiguous visual stimuli in chronic Complex Regional Pain Syndrome (CRPS) type I. Eur J Pain. 2012;16(2):182–195. doi:10.1016/j.ejpain.2011.06.016
86. Hall J, Harrison S, Cohen H, et al. Pain and other symptoms of CRPS can be increased by ambiguous visual stimuli - an exploratory study. Eur J Pain. 2011;15(1):17–22. doi:10.1016/j.ejpain.2010.04.009
87. McCabe CS, Blake DR. Evidence for a mismatch between the brain’s movement control system and sensory system as an explanation for some pain-related disorders. Curr Pain Headache Rep. 2007;11(2):104–108. doi:10.1007/s11916-007-0006-x
88. McCabe CS, Cohen H, Hall J, et al. Somatosensory conflicts in complex regional pain syndrome type 1 and fibromyalgia syndrome. Curr Rheumatol Rep. 2009;11(6):461–465. doi:10.1007/s11926-009-0067-4
89. Harris AJ. Cortical origin of pathological pain. Lancet. 1999;354(9188):1464–1466. doi:10.1016/S0140-6736(99)05003-5
90. McCabe CS. Simulating sensory-motor incongruence in healthy volunteers: implications for a cortical model of pain. Rheumatology. 2005;44(4):509–516. doi:10.1093/rheumatology/keh529
91. Heinricher MM, Tavares I, Leith JL, et al. Descending control of nociception: specificity, recruitment and plasticity. Brain Res Rev. 2009;60(1):214–225. doi:10.1016/j.brainresrev.2008.12.009
92. Ossipov MH, Dussor GO, Porreca F. Central modulation of pain. J Clin Invest. 2010;120(11):3779–3787. doi:10.1172/JCI43766
93. Bannister K, Bee LA, Dickenson AH. Preclinical and early clinical investigations related to monoaminergic pain modulation. Neurotherapeutics. 2009;6(4):703–712. doi:10.1016/j.nurt.2009.07.009
94. Modarresi S, Aref-Eshghi E, Walton DM, et al. Does a familial subtype of complex regional pain syndrome exist? Results of a systematic review. Can J Pain. 2019;3(1):157–166. doi:10.1080/24740527.2019.1637249
95. Van Rooijen DE, Roelen DL, Verduijn W, et al. Genetic HLA associations in complex regional pain syndrome with and without dystonia. J Pain. 2012;13(8):784–789. doi:10.1016/j.jpain.2012.05.003
96. De Rooij AM, Gosso FM, Haasnoot GW, et al. HLA-B62 and HLA-DQ8 are associated with complex regional pain syndrome with fixed dystonia. Pain. 2009;145(1):82–85. doi:10.1016/j.pain.2009.05.015
97. Jin EH, Zhang E, Ko Y, et al. Genome-wide expression profiling of complex regional pain syndrome. PLoS One. 2013;8(11):e79435. doi:10.1371/journal.pone.0079435
98. Zhu H, Wen B, Xu L, et al. Identification of potential inflammation-related genes and key pathways associated with complex regional pain syndrome. Biomolecules. 2023;13(5):772. doi:10.3390/biom13050772
99. Lohnberg JA, Altmaier EM. A review of psychosocial factors in complex regional pain syndrome. J Clin Psychol Med Settings. 2013;20(2):247–254. doi:10.1007/s10880-012-9322-3
100. Wager J, Brehmer H, Hirschfeld G, et al. Psychological distress and stressful life events in pediatric complex regional pain syndrome. Pain Res Manag. 2015;20(4):189–194. doi:10.1155/2015/139329
101. Speck V, Schlereth T, Birklein F, et al. Increased prevalence of posttraumatic stress disorder in CRPS. Eur J Pain. 2017;21(3):466–473. doi:10.1002/ejp.940
102. Levit-Binnun N, Golland Y. Finding behavioral and network indicators of brain vulnerability. Front Hum Neurosci. 2012;6:10. doi:10.3389/fnhum.2012.00010
103. Beerthuizen A, Van ‘T Spijker A, Huygen FJPM, et al. Is there an association between psychological factors and the complex regional pain syndrome type 1 (CRPS1) in adults? A systematic review. Pain. 2009;145(1):52–59. doi:10.1016/j.pain.2009.05.003
104. Pereira DE, Momtaz D, Gonuguntla R, et al. Patients with preexisting anxiety and mood disorders are more likely to develop complex regional pain syndrome after fractures. Clin Orthop Relat Res. 2024;482(2):222–230. doi:10.1097/CORR.0000000000002957
105. Lorente A, Mariscal G, Lorente R. Incidence and risk factors for complex regional pain syndrome in radius fractures: meta-analysis. Arch Orthop Trauma Surg. 2023;143(9):5687–5699. doi:10.1007/s00402-023-04909-8
106. Bruehl S, Warner DS. An update on the pathophysiology of complex regional pain syndrome. Anesthesiology. 2010;113(3):713–725. doi:10.1097/ALN.0b013e3181e3db38
107. Kortekaas MC, Niehof SP, Stolker RJ, et al. Pathophysiological mechanisms involved in vasomotor disturbances in complex regional pain syndrome and implications for therapy: a review. Pain Pract. 2016;16(7):905–914. doi:10.1111/papr.12403
108. Taha R, Blaise GA. Update on the pathogenesis of complex regional pain syndrome: role of oxidative stress. Can J Anesth. 2012;59(9):875–881. doi:10.1007/s12630-012-9748-y
109. Albrecht PJ, Hines S, Eisenberg E, et al. Pathologic alterations of cutaneous innervation and vasculature in affected limbs from patients with complex regional pain syndrome. Pain. 2006;120(3):244–266. doi:10.1016/j.pain.2005.10.035
110. Oaklander AL, Rissmiller JG, Gelman LB, et al. Evidence of focal small-fiber axonal degeneration in complex regional pain syndrome-I (reflex sympathetic dystrophy). Pain. 2006;120(3):235–243. doi:10.1016/j.pain.2005.09.036
111. Morellini N, Finch PM, Goebel A, et al. Dermal nerve fibre and mast cell density, and proximity of mast cells to nerve fibres in the skin of patients with complex regional pain syndrome. Pain. 2018;159(10):2021–2029. doi:10.1097/j.pain.0000000000001304
112. Yvon A, Faroni A, Reid AJ, et al. Selective fiber degeneration in the peripheral nerve of a patient with severe complex regional pain syndrome. Front Neurosci. 2018;12:207. doi:10.3389/fnins.2018.00207
113. Shi X, Zhi GT, wu LW, et al. C5a complement and cytokine signaling mediate the pronociceptive effects of complex regional pain syndrome patient IgM in fracture mice. Pain. 2021;162(5):1400–1415. doi:10.1097/j.pain.0000000000002150
114. Lin B, Wang Y, Zhang P, et al. Gut microbiota regulates neuropathic pain: potential mechanisms and therapeutic strategy. J Headache Pain. 2020;21(1):103. doi:10.1186/s10194-020-01170-x
115. Crock LW, Baldridge MT. A role for the microbiota in complex regional pain syndrome? Neurobiol Pain. 2020;8:100054. doi:10.1016/j.ynpai.2020.100054
116. Reichenberger ER, Alexander GM, Perreault MJ, et al. Establishing a relationship between bacteria in the human gut and complex regional pain syndrome. Brain Behav Immun. 2013;29:62–69. doi:10.1016/j.bbi.2012.12.005
117. Ranjbar_moghaddam M, Nasiri-Formi E, Merajikhah A. Efficacy of vitamin C supplementation in preventing and treating complex regional pain syndrome type I (CRPS-I) in orthopedic patients: a systematic review and meta-analysis. Int J Orthop Trauma Nurs. 2024;55:101140. doi:10.1016/j.ijotn.2024.101140
118. Seth I, Bulloch G, Seth N, et al. Effect of perioperative vitamin C on the incidence of complex regional pain syndrome: a systematic review and meta-analysis. J Foot Ankle Surg. 2022;61(4):748–754. doi:10.1053/j.jfas.2021.11.008
119. Zollinger PE, Tuinebreijer WE, Kreis RW, et al. Effect of vitamin C on frequency of reflex sympathetic dystrophy in wrist fractures: a randomised trial. Lancet. 1999;354(9195):2025–2028. doi:10.1016/S0140-6736(99)03059-7
120. Shibuya N, Humphers JM, Agarwal MR, et al. Efficacy and safety of high-dose vitamin C on complex regional pain syndrome in extremity trauma and surgery—systematic review and meta-analysis. J Foot Ankle Surg. 2013;52(1):62–66. doi:10.1053/j.jfas.2012.08.003
121. Giustra F, Bosco F, Aprato A, Artiaco S, Bistolfi A, Masse A. Vitamin C could prevent complex regional pain syndrome type I (CRPS-I) in trauma and orthopedic care? A systematic review of the literature and current findings. Sisli Etfal Hastan Tıp Bul. 2021;55(2):139–145. doi:10.14744/SEMB.2021.82335
122. Evaniew N, McCarthy C, Kleinlugtenbelt YV, et al. Vitamin C to prevent complex regional pain syndrome in patients with distal radius fractures: a meta-analysis of randomized controlled trials. J Orthop Trauma. 2015;29(8):e235–e241. doi:10.1097/BOT.0000000000000305
123. Vane JR, Botting RM. Anti-inflammatory drugs and their mechanism of action. Inflamm Res. 1998;47(Suppl 2):S78–S87. doi:10.1007/s000110050284
124. Zhu H, Wen B, Xu J, et al. Efficacy and safety of pharmacological treatment in patients with complex regional pain syndrome: a systematic review and meta-analysis. Pharmaceuticals. 2024;17(6):811. doi:10.3390/ph17060811
125. Bhala N, Emberson J, Merhi A, et al. Vascular and upper gastrointestinal effects of non-steroidal anti-inflammatory drugs: meta-analyses of individual participant data from randomised trials. Lancet. 2013;382(9894):769–779.
126. Barnes PJ. How corticosteroids control inflammation: quintiles Prize Lecture 2005. Br J Pharmacol. 2006;148(3):245–254. doi:10.1038/sj.bjp.0706736
127. Nair A, Bonneau RH. Stress-induced elevation of glucocorticoids increases microglia proliferation through NMDA receptor activation. J Neuroimmunol. 2006;171(1–2):72–85. doi:10.1016/j.jneuroim.2005.09.012
128. Kwak SG, Choo YJ, Chang MC. Effectiveness of prednisolone in complex regional pain syndrome treatment: a systematic narrative review. Pain Pract. 2022;22(3):381–390. doi:10.1111/papr.13090
129. Her YF, Kubrova E, Dombovy-Johnson M, et al. Complex Regional pain syndrome: updates and current evidence. Curr Phys Med Rehabil Rep. 2024;12(1):50–70. doi:10.1007/s40141-023-00426-2
130. Perez MRSG, Zuurmond AWW, Bezemer DP, et al. The treatment of complex regional pain syndrome type I with free radical scavengers: a randomized controlled study. Pain. 2003;102(3):297–307. doi:10.1016/S0304-3959(02)00414-1
131. Cochrane Pain, Palliative and Supportive Care Group, Ferraro MC, Cashin AG, Wand BM, et al. Interventions for treating pain and disability in adults with complex regional pain syndrome- an overview of systematic reviews. Cochrane Database Syst Rev. 2023;2023(6):CD009416.
132. Yanow J, Pappagallo M, Pillai L. Complex regional pain syndrome (CRPS/RSD) and neuropathic pain: role of intravenous bisphosphonates as analgesics. ScientificWorldJournal. 2008;8:229–236. doi:10.1100/tsw.2008.33
133. Varenna M, Zucchi F, Di Taranto R, et al. Osteoclast in CRPS: an alleged guilty fully acquitted. Osteoporos Int. 2025;36(4):737–740. doi:10.1007/s00198-025-07415-2
134. Chevreau M, Romand X, Gaudin P, et al. Bisphosphonates for treatment of complex regional pain syndrome type 1: a systematic literature review and meta-analysis of randomized controlled trials versus placebo. Joint Bone Spine. 2017;84(4):393–399. doi:10.1016/j.jbspin.2017.03.009
135. Vannala V, Palaian S, Shankar P. Therapeutic dimensions of bisphosphonates: a clinical update. Int J Prev Med. 2020;11(1):166. doi:10.4103/ijpvm.IJPVM_33_19
136. Sansoni P, Passeri G, Fagnoni F, et al. Inhibition of antigen-presenting cell function by alendronate in vitro. J Bone Miner Res. 1995;10(11):1719–1725. doi:10.1002/jbmr.5650101115
137. Maksymowych W. Bisphosphonates—anti-inflammatory properties. Curr Med Chem Antiinflamm Antiallergy Agents. 2002;1(1):15–28. doi:10.2174/1568014024606539
138. Mellick GA, Mellick LB. Reflex sympathetic dystrophy treated with gabapentin. Arch Phys Med Rehabil. 1997;78(1):98–105. doi:10.1016/S0003-9993(97)90020-4
139. Van De Vusse AC, Stomp-van Den Berg SG, Kessels AH, et al. Randomised controlled trial of gabapentin in complex regional pain syndrome type 1 [ISRCTN84121379]. BMC Neurol. 2004;4(1):13. doi:10.1186/1471-2377-4-13
140. Tan AK, Duman I, Taşkaynatan MA, et al. The effect of gabapentin in earlier stage of reflex sympathetic dystrophy. Clin Rheumatol. 2007;26(4):561–565. doi:10.1007/s10067-006-0350-y
141. Saltık S, Sözen HG, Basgul S, et al. Pregabalin treatment of a patient with complex regional pain syndrome. Pediatr Neurol. 2016;54:88–90. doi:10.1016/j.pediatrneurol.2014.01.015
142. Wössner S, Weber K, Steinbeck AC, et al. Pregabalin as adjunct in a multimodal pain therapy after traumatic foot amputation — a case report of a 4-year-old girl. Scand J Pain. 2017;17(1):146–149. doi:10.1016/j.sjpain.2017.09.001
143. Gambeta E, Chichorro JG, Zamponi GW. Trigeminal neuralgia: an overview from pathophysiology to pharmacological treatments. Mol Pain. 2020;16:1744806920901890. doi:10.1177/1744806920901890
144. Harke H, Gretenkort P, Ladleif H, et al. The response of neuropathic pain and pain in complex regional pain syndrome I to carbamazepine and sustained-release morphine in patients pretreated with spinal cord stimulation: a double-blinded randomized study. Anesth Analg. 2001;92(2):488–495. doi:10.1213/00000539-200102000-00039
145. Brown S, Johnston B, Amaria K, et al. A randomized controlled trial of amitriptyline versus gabapentin for complex regional pain syndrome type I and neuropathic pain in children. Scand J Pain. 2016;13(1):156–163. doi:10.1016/j.sjpain.2016.05.039
146. Cavalli E, Mammana S, Nicoletti F, et al. The neuropathic pain: an overview of the current treatment and future therapeutic approaches. Int J Immunopathol Pharmacol. 2019;33:2058738419838383. doi:10.1177/2058738419838383
147. Lambert DG. Opioids and opioid receptors; understanding pharmacological mechanisms as a key to therapeutic advances and mitigation of the misuse crisis. BJA Open. 2023;6:100141. doi:10.1016/j.bjao.2023.100141
148. Watkins LR, Hutchinson MR, Ledeboer A, et al. Glia as the “bad guys”: implications for improving clinical pain control and the clinical utility of opioids. Brain Behav Immun. 2007;21(2):131–146. doi:10.1016/j.bbi.2006.10.011
149. Gustin SM, Schwarz A, Birbaumer N, et al. NMDA-receptor antagonist and morphine decrease CRPS-pain and cerebral pain representation. Pain. 2010;151(1):69–76. doi:10.1016/j.pain.2010.06.022
150. Niesters M, Martini C, Dahan A. Ketamine for chronic pain: risks and benefits. brit J Clin pharma. 2014;77(2):357–367. doi:10.1111/bcp.12094
151. Sigtermans MJ, Van Hilten JJ, Bauer MCR, et al. Ketamine produces effective and long-term pain relief in patients with complex regional pain syndrome type 1. Pain. 2009;145(3):304–311. doi:10.1016/j.pain.2009.06.023
152. Schwartzman RJ, Alexander GM, Grothusen JR, et al. Outpatient intravenous ketamine for the treatment of complex regional pain syndrome: a double-blind placebo controlled study. Pain. 2009;147(1):107–115. doi:10.1016/j.pain.2009.08.015
153. Collins S, Zuurmond WWA, De Lange JJ, et al. Intravenous magnesium for complex regional pain syndrome type 1 (CRPS 1) patients: a pilot study. Pain Med. 2009;10(5):930–940. doi:10.1111/j.1526-4637.2009.00639.x
154. Fischer SGL, Collins S, Boogaard S, et al. Intravenous magnesium for chronic complex regional pain syndrome type 1 (CRPS-1). Pain Med. 2013;14(9):1388–1399. doi:10.1111/pme.12211
155. Xu J, Yang J, Lin P, et al. Intravenous therapies for complex regional pain syndrome: a systematic review. Anesth Analg. 2016;122(3):843–856. doi:10.1213/ANE.0000000000000999
156. Chang MC, Park D. Effectiveness of intravenous immunoglobulin for management of neuropathic pain: a narrative review. J Pain Res. 2020;13:2879–2884. doi:10.2147/JPR.S273475
157. Aradillas E, Schwartzman RJ, Grothusen JR, Goebel A, Alexander GM. Plasma exchange therapy in patients with complex regional pain syndrome. Pain Physician. 2015;18(4):383–394.
158. Hendrickson JE, Hendrickson ET, Gehrie EA, et al. Complex regional pain syndrome and dysautonomia in a 14‐year‐old girl responsive to therapeutic plasma exchange. J Clin Apher. 2016;31(4):368–374. doi:10.1002/jca.21407
159. Goebel A, Jones S, Oomman S, et al. Treatment of long-standing complex regional pain syndrome with therapeutic plasma exchange: a preliminary case series of patients treated in 2008–2014. Pain Med. 2014;15(12):2163–2164. doi:10.1111/pme.12601
160. Huygen FJPM, Niehof S, Zijlstra FJ, et al. Successful treatment of CRPS 1 with anti-TNF. J Pain Symptom Manage. 2004;27(2):101–103. doi:10.1016/j.jpainsymman.2003.12.006
161. Dirckx M, Groeneweg G, Wesseldijk F, et al. Report of a Preliminary Discontinued Double-Blind, Randomized, Placebo-Controlled Trial of the Anti- TNF-α Chimeric Monoclonal Antibody Infliximab in Complex Regional Pain Syndrome. Pain Pract. 2013;13(8):633–640. doi:10.1111/papr.12078
162. Eisenberg E, Sandler I, Treister R, et al. Anti tumor necrosis factor ‐ alpha Adalimumab for complex regional pain syndrome type 1 (CRPS‐I): a case series. Pain Pract. 2013;13(8):649–656. doi:10.1111/papr.12070
163. Gerriets V, Goyal A, Khaddour K. Tumor cecrosis factor inhibitors. StatPearls. StatPearls Publishing; 2025. https://www.ncbi.nlm.nih.gov/books/NBK482425/
164. Kim JH, Park JS, Park D. Anti-allodynic effect of interleukin 10 in a mouse model of complex regional pain syndrome through reduction of NK1 receptor expression of microglia in the spinal cord. J Pain Res. 2018;11:1729–1741. doi:10.2147/JPR.S166624
165. Helyes Z, Tékus V, Szentes N, et al. Transfer of complex regional pain syndrome to mice via human autoantibodies is mediated by interleukin-1–induced mechanisms. Proc Natl Acad Sci USA. 2019;116(26):13067–13076. doi:10.1073/pnas.1820168116
166. Chopra P, Cooper MS. Treatment of complex regional pain syndrome (CRPS) using low dose naltrexone (LDN). J Neuroimmune Pharmacol. 2013;8(3):470–476. doi:10.1007/s11481-013-9451-y
167. Toljan K, Vrooman B. Low-dose naltrexone (LDN)—review of therapeutic utilization. Med Sci. 2018;6(4):82.
168. Weinstock LB, Myers TL, Walters AS, et al. Identification and treatment of new inflammatory triggers for complex regional pain syndrome: small intestinal bacterial overgrowth and obstructive sleep apnea. A a Case Rep. 2016;6(9):272–276. doi:10.1213/XAA.0000000000000292
169. Younger J, Parkitny L, McLain D. The use of low-dose naltrexone (LDN) as a novel anti-inflammatory treatment for chronic pain. Clin Rheumatol. 2014;33(4):451–459. doi:10.1007/s10067-014-2517-2
170. Watkins LR, Hutchinson MR, Rice KC, et al. The “Toll” of opioid-induced glial activation: improving the clinical efficacy of opioids by targeting glia. Trends Pharmacol Sci. 2009;30(11):581–591. doi:10.1016/j.tips.2009.08.002
171. Dorazil-Dudzik M, Mika J, Schafer MKH, et al. The effects of local pentoxifylline and propentofylline treatment on formalin-induced pain and tumor necrosis factor-alpha messenger RNA levels in the inflamed tissue of the rat paw. Anesth Analg. 2004;98(6):1566–1573. doi:10.1213/01.ANE.0000113235.88534.48
172. Hama AT, Broadhead A, Lorrain DS, et al. The antinociceptive effect of the asthma drug ibudilast in rat models of peripheral and central neuropathic pain. J Neurotrauma. 2012;29(3):600–610. doi:10.1089/neu.2011.1863
173. Ellis A, Wieseler J, Favret J, et al. Systemic administration of propentofylline, ibudilast, and (+)-naltrexone each reverses mechanical allodynia in a novel rat model of central neuropathic pain. J Pain. 2014;15(4):407–421. doi:10.1016/j.jpain.2013.12.007
174. Fujita M, Tamano R, Yoneda S, et al. Ibudilast produces anti-allodynic effects at the persistent phase of peripheral or central neuropathic pain in rats: different inhibitory mechanism on spinal microglia from minocycline and propentofylline. Eur J Pharmacol. 2018;833:263–274. doi:10.1016/j.ejphar.2018.06.009
175. Tawfik VL, Nutile-McMenemy N, LaCroix-Fralish ML, et al. Efficacy of propentofylline, a glial modulating agent, on existing mechanical allodynia following peripheral nerve injury. Brain Behav Immun. 2007;21(2):238–246. doi:10.1016/j.bbi.2006.07.001
176. Motsch J, Kamler M. Alpha 2-adrenergic agonists. Use in chronic pain—a meta-analysis. Schmerz. 1997;11(5):339–344. doi:10.1007/s004820050108
177. Knezevic NN, Tverdohleb T, Nikibin F, et al. Management of chronic neuropathic pain with single and compounded topical analgesics. Pain Manag. 2017;7(6):537–558. doi:10.2217/pmt-2017-0020
178. Goyagi T, Tanaka M, Nishikawa T. Oral clonidine premedication enhances postoperative analgesia by epidural morphine. Anesth Analg. 1999;89(6):1487–1491. doi:10.1213/00000539-199912000-00032
179. Carroll D, Jadad A, King V, et al. Single-dose, randomized, double-blind, double-dummy cross-over comparison of extradural and I.V. clonidine in chronic pain. Br J Anaesth. 1993;71(5):665–669. doi:10.1093/bja/71.5.665
180. Rauck R, Eisenach J, Jackson K, et al. Epidural clonidine treatment for refractory reflex sympathetic dystrophy. Anesthesiology. 1993;79(6):1163–1169. doi:10.1097/00000542-199312000-00005
181. Galer BS, Rowbotham MC, Perander J, et al. Topical lidocaine patch relieves postherpetic neuralgia more effectively than a vehicle topical patch: results of an enriched enrollment study. Pain. 1999;80(3):533–538. doi:10.1016/S0304-3959(98)00244-9
182. Ribbers GM, Stam HJ. Complex regional pain syndrome type I treated with topical capsaicin: a case report. Arch Phys Med Rehabil. 2001;82(6):851–852. doi:10.1053/apmr.2001.21911
183. Butchart AG, Mathews M, Surendran A. Complex regional pain syndrome following protracted labour*. Anaesthesia. 2012;67(11):1272–1274. doi:10.1111/j.1365-2044.2012.07301.x
184. Goncalves D, Rebelo V, Barbosa P, et al. 8% Capsaicin patch in treatment of peripheral neuropathic pain. Pain Physician. 2020;23(5):E541–E548. doi:10.36076/ppj.2020/23/E541
185. Russo MA, Santarelli DM. A novel compound analgesic cream (ketamine,pentoxifylline,clonidine,
186. Poenaru D, Sandulescu MI, Cinteza D. Pain modulation in chronic musculoskeletal disorders: botulinum toxin, a descriptive analysis. Biomedicines. 2023;11(7):1888. doi:10.3390/biomedicines11071888
187. Dekhne A, Goklani HD, Doshi N, et al. Effectiveness of botulinum toxin in the treatment of neuropathic pain: a literature review. Cureus. 2023;15(10):e46848. doi:10.7759/cureus.46848
188. Carroll I, Clark JD, Mackey S. Sympathetic block with botulinum toxin to treat complex regional pain syndrome. Ann Neurol. 2009;65(3):348–351. doi:10.1002/ana.21601
189. Yoo Y, Lee CS, Kim J, et al. Botulinum toxin type A for lumbar sympathetic ganglion block in complex regional pain syndrome: a randomized trial. Anesthesiology. 2022;136(2):314–325. doi:10.1097/ALN.0000000000004084
190. Safarpour D, Salardini A, Richardson D, et al. Botulinum toxin A for treatment of allodynia of complex regional pain syndrome: a pilot study. Pain Med. 2010;11(9):1411–1414. doi:10.1111/j.1526-4637.2010.00897.x
191. Attal N, de Andrade DC, Adam F, et al. Botulinum toxin – neuropathic pain: safety and efficacy of repeated injections of botulinum toxin a in peripheral neuropathic pain (BOTNEP): a randomised, double-blind, placebo-controlled trial. Lancet Neurol. 2016;15(6):555–565. doi:10.1016/S1474-4422(16)00017-X
192. Abdullahi SE, Arrigoni Martelli E, Bramm E, et al. Effect of calcitonin on different inflammatory models. Agents Actions. 1977;7(5–6):533–538. doi:10.1007/BF02111126
193. Appelboom T. Calcitonin in reflex sympathetic dystrophy syndrome and other painful conditions. Bone. 2002;30(5):84–86. doi:10.1016/S8756-3282(02)00702-0
194. Gobelet C, Waldburger M, Meier JL. The effect of adding calcitonin to physical treatment on reflex sympathetic dystrophy. Pain. 1992;48(2):171–175. doi:10.1016/0304-3959(92)90055-G
195. Bickerstaff DR, Kanis JA. The use of nasal calcitonin in the treatment of post-traumatic algodystrophy. Br J Rheumatol. 1991;30(4):291–294. doi:10.1093/rheumatology/30.4.291
196. Sahin F, Yilmaz F, Kotevoglu N, et al. Efficacy of salmon calcitonin in complex regional pain syndrome (type 1) in addition to physical therapy. Clin Rheumatol. 2006;25(2):143–148. doi:10.1007/s10067-005-1153-2
197. Stanton-Hicks M, Baron R, Boas R, et al. Complex regional pain syndromes: guidelines for therapy. Clin J Pain. 1998;14(2):155–166. doi:10.1097/00002508-199806000-00012
198. Sayegh SA, Filén T, Johansson M, et al. Mirror therapy for complex regional pain syndrome (CRPS)—a literature review and an illustrative case report. Scand J Pain. 2013;4(4):200–207. doi:10.1016/j.sjpain.2013.06.002
199. McCabe C. Mirror visual feedback therapy. a practical approach. J Hand Ther. 2011;24(2):170–179. doi:10.1016/j.jht.2010.08.003
200. Moseley LG. Graded motor imagery is effective for long-standing complex regional pain syndrome: a randomised controlled trial. Pain. 2004;108(1):192–198. doi:10.1016/j.pain.2004.01.006
201. Cacchio A, De Blasis E, De Blasis V, et al. Mirror therapy in complex regional pain syndrome type 1 of the upper limb in stroke patients. Neurorehabil Neural Repair. 2009;23(8):792–799. doi:10.1177/1545968309335977
202. Pervane Vural S, Nakipoglu Yuzer GF, Sezgin Ozcan D, et al. Effects of mirror therapy in stroke patients with complex regional pain syndrome type 1: a randomized controlled study. Arch Phys Med Rehabil. 2016;97(4):575–581. doi:10.1016/j.apmr.2015.12.008
203. Saha S, Sur M, Ray chaudhuri G, et al. Effects of mirror therapy on oedema, pain and functional activities in patients with poststroke shoulder‐hand syndrome: a randomized controlled trial. Physiotherapy Res Intl. 2021;26(3):e1902. doi:10.1002/pri.1902
204. Shafiee E, MacDermid J, Packham T, et al. The Effectiveness of rehabilitation interventions on pain and disability for complex regional pain syndrome: a systematic review and meta-analysis. Clin J Pain. 2023;39(2):91–105. doi:10.1097/AJP.0000000000001089
205. Pourmand A, Davis S, Marchak A, et al. Virtual reality as a clinical tool for pain management. Curr Pain Headache Rep. 2018;22(8):53. doi:10.1007/s11916-018-0708-2
206. Chuan A, Zhou JJ, Hou RM, et al. Virtual reality for acute and chronic pain management in adult patients: a narrative review. Anaesthesia. 2021;76(5):695–704. doi:10.1111/anae.15202
207. Arcos-Holzinger M, Biebl JT, Storz C, et al. Virtual reality in managing complex regional pain syndrome (CRPS): a scoping review. Front Neurol. 2023;14:1069381. doi:10.3389/fneur.2023.1069381
208. Lewis JS, Newport R, Taylor G, et al. Visual illusions modulate body perception disturbance and pain in complex regional pain syndrome: a randomized trial. Eur J Pain. 2021;25(7):1551–1563. doi:10.1002/ejp.1766
209. Matamala-Gomez M, Diaz Gonzalez AM, Slater M, et al. Decreasing pain ratings in chronic arm pain through changing a virtual body: different strategies for different pain types. J Pain. 2019;20(6):685–697. doi:10.1016/j.jpain.2018.12.001
210. Solcà M, Ronchi R, Bello-Ruiz J, et al. Heartbeat-enhanced immersive virtual reality to treat complex regional pain syndrome. Neurology. 2018;91(5):e479–e489. doi:10.1212/WNL.0000000000005905
211. Sato K, Fukumori S, Matsusaki T, et al. Nonimmersive virtual reality mirror visual feedback therapy and its application for the treatment of complex regional pain syndrome: an open-label pilot study. Pain Med. 2010;11(4):622–629. doi:10.1111/j.1526-4637.2010.00819.x
212. Chau B, Phelan I, Ta P, et al. Immersive virtual reality for pain relief in upper limb complex regional pain syndrome: a pilot study. Innov Clin Neurosci. 2020;17(4–6):47–52.
213. Li TS, Wang R, Su X, et al. Effect and mechanisms of exercise for complex regional pain syndrome. Front Mol Neurosci. 2023;16:1167166. doi:10.3389/fnmol.2023.1167166
214. Oh HM, Kim CH, Kim AR. Dramatic effect in passive ROM exercise under sedation in a patient with intractable complex regional pain syndrome (type I): a case report. Medicine. 2019;98(13):e14990. doi:10.1097/MD.0000000000014990
215. Topcuoglu A, Gokkaya NKO, Ucan H, et al. The effect of upper-extremity aerobic exercise on complex regional pain syndrome type I: a randomized controlled study on subacute stroke. Top Stroke Rehabil. 2015;22(4):253–261. doi:10.1179/1074935714Z.0000000025
216. Miller C, Williams M, Heine P, et al. Current practice in the rehabilitation of complex regional pain syndrome: a survey of practitioners. Disabil Rehabil. 2019;41(7):847–853. doi:10.1080/09638288.2017.1407968
217. Ek JW, Van Gijn JC, Samwel H, et al. Pain exposure physical therapy may be a safe and effective treatment for longstanding complex regional pain syndrome type 1: a case series. Clin Rehabil. 2009;23(12):1059–1066. doi:10.1177/0269215509339875
218. Van De Meent H, Oerlemans M, Bruggeman A, et al. Safety of “pain exposure” physical therapy in patients with complex regional pain syndrome type 1. Pain. 2011;152(6):1431–1438. doi:10.1016/j.pain.2011.02.032
219. Barnhoorn KJ, Van De Meent H, Van Dongen RTM, et al. Pain exposure physical therapy (PEPT) compared to conventional treatment in complex regional pain syndrome type 1: a randomised controlled trial. BMJ Open. 2015;5(12):e008283. doi:10.1136/bmjopen-2015-008283
220. Den Hollander M, Goossens M, De Jong J, et al. Expose or protect? A randomized controlled trial of exposure in vivo vs pain-contingent treatment as usual in patients with complex regional pain syndrome type 1. Pain. 2016;157(10):2318–2329. doi:10.1097/j.pain.0000000000000651
221. Sluka KA, Walsh D. Transcutaneous electrical nerve stimulation: basic science mechanisms and clinical effectiveness. J Pain. 2003;4(3):109–121. doi:10.1054/jpai.2003.434
222. Vance CG, Dailey DL, Rakel BA, et al. Using TENS for pain control: the state of the evidence. Pain Manag. 2014;4(3):197–209. doi:10.2217/pmt.14.13
223. Bilgili A, Çakır T, Doğan ŞK, et al. The effectiveness of transcutaneous electrical nerve stimulation in the management of patients with complex regional pain syndrome: a randomized, double-blinded, placebo-controlled prospective study. J Back Musculoskelet Rehabil. 2016;29(4):661–671. doi:10.3233/BMR-160667
224. Sezgin Ozcan D, Tatli HU, Polat CS, et al. The effectiveness of fluidotherapy in poststroke complex regional pain syndrome: a randomized controlled study. J Stroke Cerebrovasc Dis. 2019;28(6):1578–1585. doi:10.1016/j.jstrokecerebrovasdis.2019.03.002
225. Sethy D, Sahoo S, Bajpai P, et al. Effect of stress loading combined with fluido-therapy on CRPS-I in stroke hemiplegics. Inter J Ther Rehab Res. 2017;6:242–248.
226. Stanton DB, Bear-Lehman J, Graziano M, et al. Contrast baths: what do we know about their use? J Hand Ther. 2003;16(4):343–346. doi:10.1197/S0894-1130(03)00161-3
227. Shadgan B, Pakravan AH, Hoens A, et al. Contrast baths, intramuscular hemodynamics, and oxygenation as monitored by near-infrared spectroscopy. J Athl Train. 2018;53(8):782–787. doi:10.4085/1062-6050-127-17
228. Yavuz Keleş B, Önder B, Kesiktaş FN, et al. Acute effects of contrast bath on sympathetic skin response in patients with poststroke complex regional pain syndrome. Somatosens Mot Res. 2020;37(4):320–325. doi:10.1080/08990220.2020.1830756
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Preferences for Rehabilitation in Persons with a History of Stroke: A Discrete Choice Experiment
Noto S, Murata T, Saito S, Watanabe T, Kobayashi M
Patient Preference and Adherence 2023, 17:1611-1620
Published Date: 12 July 2023