Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 14
Comprehensive Effects of Organized Education for Patients with Chronic Obstructive Pulmonary Disease
Authors Jang JG ![]() , Kim JS, Chung JH
, Kim JS, Chung JH ![]() , Shin KC
, Shin KC ![]() , Ahn JH
, Ahn JH ![]() , Lee MS, Bang SH, Park DY, Nam MJ, Jin HJ
, Lee MS, Bang SH, Park DY, Nam MJ, Jin HJ ![]() , Lee KH
, Lee KH
Received 2 July 2019
Accepted for publication 1 November 2019
Published 25 November 2019 Volume 2019:14 Pages 2603—2609
DOI https://doi.org/10.2147/COPD.S221673
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Jong Geol Jang,1 Jee Seon Kim,2 Jin Hong Chung,1 Kyeong Cheol Shin,1 June Hong Ahn,1 Mi Sook Lee,3 So Hee Bang,3 Da Yeong Park,3 Mee Jung Nam,3 Hyun Jung Jin,1,* Kwan Ho Lee1,*
1Division of Pulmonology and Allergy, Department of Internal Medicine, Yeungnam University Medical Center, College of Medicine, Daegu, Republic of Korea; 2Department of Internal Medicine, Semyeong Christianity Hospital, Pohang, Republic of Korea; 3Department of Education and Management Services, Yeungnam University Medical Center,College of Medicine, Daegu, Republic of Korea
*These authors contributed equally to this work
Correspondence: Hyun Jung Jin
Division of Pulmonology and Allergy, Department of Internal Medicine, Yeungnam University College of Medicine, 170 Hyeonchung-ro, Nam-gu, Daegu 42415, Republic of Korea
Tel +82-53-640-6578
Fax +82-53-640-6449
Email [email protected]
Background: Despite the increasing prevalence of chronic obstructive pulmonary disease (COPD) worldwide, knowledge and awareness of COPD remain extremely low. This prospective study aimed to demonstrate the effectiveness of organized educational intervention.
Patients and methods: The study participants included patients diagnosed with COPD and receiving inhaler treatment. In this prospective study, the patients made three sequential visits to the hospital (baseline, 1 month, 3 months). On their first and second visits, patients received systematic education about COPD. On their first and third visits, each patient was evaluated using a COPD Assessment Test, COPD Knowledge Questionnaire, Hospital Anxiety and Depression Scale, and Rosenberg Self-Esteem Scale.
Results: Fifty-five participants were enrolled in the study. The mean COPD knowledge score before and after education was 12.51±3.19 and 17.89±1.37, respectively, indicating a significant increase in the score post-education (P<0.001). The measure of patients’ inhaler technique also significantly improved after education (5.40±1.50 vs 6.83±0.37 P=0.01). The rate of depression and anxiety after education decreased by 10.9% and 12.7%, respectively (P<0.001). In subgroup analysis, we compared the groups whose knowledge score increased by more than 5 points (Group B) and those whose score did not improve (Group A). In Group B, the mean CAT score significantly improved (2.61±5.88 vs −2.41±7.48, P=0.01), and the duration of their COPD diagnosis before enrollment was significantly shorter (2.72±2.43 vs 5.22±5.11 years, P=0.038) compared to those in Group A.
Conclusion: An organized educational program resulted in improved disease-specific knowledge. Disease-specific education is an important part of the treatment of COPD that affects the quality of life and emotional status of patients. Early education after COPD diagnosis can be beneficial.
Keywords: anxiety, chronic obstructive pulmonary disease, depression, education, quality of life
Introduction
Chronic obstructive pulmonary disease (COPD) is a common, progressive disease with persistent respiratory symptoms and airflow limitation.1,2 COPD is a major cause of chronic morbidity and mortality worldwide and is expected to be the third leading cause of death in 2030.3 A great number of patients with COPD have a poor knowledge of COPD and a misunderstanding of their own symptom control state.4,5 Thus, disease-specific education is an important part of management for patients with COPD,6 and enhancing patient knowledge will lead to improved self-management.7 The goal of education is to improve adherence of treatment and clinical outcome.8 Up to now, disease education has been implemented as part of pulmonary rehabilitation, and most studies reported that education alone did not impact on the quality of life.9 The purpose of this study was to develop an education program and evaluate the effectiveness of an organized education program in improving disease-specific knowledge and quality of life of patients with COPD.
Methods
Patient
Patients were recruited from a tertiary hospital in South Korea. Enrollment occurred from 2017 to 2018. The study included patients aged >40 years, with diagnosis of COPD according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria1 and receiving ongoing treatment with an inhaler. Exclusion criteria were as follows: 1) the patient who is impossible to communicate in written or spoken Korean and 2) the patient who had received prior education of COPD in the last year.
This study was conducted in accordance with the Declaration of Helsinki and was reviewed and approved by the Institutional Review Board of Yeungnam University Hospital (IRB number YUMC IRB 2017-08-027). All patients provided written informed consent before participating in the study.
Study Design and Intervention
This trial was a prospective study comparing specific patient metrics before and after educational intervention. Participants visited the facility three times and received two sessions of face-to-face education individually, each lasting 30 mins, with a nurse with expertise in managingpatients with COPD and a pulmonologist (first session and final refreshment were conducted by the nurse and second session by the pulmonologist). Intervention was conducted by using a leaflet made by the pulmonologist and it was given to the patients after the educational session. Contents of the first educational session (on enrollment) were as follows: definition of COPD, COPD diagnosis, pulmonary function test, signs and symptoms, treatment, vaccination, and nutrition. Contents of the second educational session (1 month after the first visit) included correct use of an inhaler, benefits of exercise and physical activities, recognition and action plan of acute exacerbation, and management of comorbidities. At their third visit (3 months after the first visit), we assessed the change in each patient metric. Thereafter, the prior educational contents were refreshed (Figure S1).
Outcome Measures
At baseline, data on age, gender, body mass index, level of education, history of smoking, comorbidities, duration of COPD diagnosis, and spirometric measures (forced vital capacity (FVC), forced expired volume in 1 second (FEV1) and FEV1/FVC ratio) were collected.
The primary outcome was the change in COPD knowledge after education. It was assessed using 20 statements about COPD-related topics. It consisted of 8 topics and 20 items (Table S1). The 17 items on the questionnaire were a modification of the Bristol COPD Knowledge Questionnaire10 (BCKQ) and 3 items used were quoted from Lee et al.11
The secondary outcomes were the change in the modified Medical Research Council (mMRC) Dyspnea Scale score, COPD Assessment Test (CAT) score, Rosenberg Self-Esteem Scale (RSES) score, Hospital Anxiety and Depression Scale (HADS) score, and patient inhaler technique after education. All outcomes were measured at the first visit and third visit (3 months after the first visit). The mMRC scale consists of five statements that describe the range of dyspnea from none (grade 0) to almost complete incapacity (grade 4).12 The CAT score contains eight questions that cover domains relating to the impact of COPD symptoms and range from 0 to 40, with higher scores indicating more severe disease.13 The RSES is a widely used measure of self-esteem and includes a 10-item Likert scale with items answered on a four-point scale, from strongly agree to strongly disagree.14 The HADS measurement was acquired via a self-assessment questionnaire to assess the state of anxiety and depression among the medically ill patients.15 It is a 14-item questionnaire composed of 7 items each for the anxiety subscale and depression.15 A possible presence of anxiety and depression can be considered when the HADS score is ≥8. The inhaler technique was assessed by using a scoring system that consists of seven steps (Table S2). The checklist of inhalers was made based on previous studies.11,16 The final score is reported as the sum of the scores for each step (1 for a correct answer, 0 for an incorrect or skipped answer).
Sample Size Calculation and Statistical Analysis
Calculation using power analysis indicated that the overall sample size of 44 patients was required to detect 15% improvement of knowledge score after education by using a paired t-test (90% power, α=0.05, effect size=0.5). The 15% improvement was chosen because the previous study reported a 15% improvement of knowledge after educational intervention. Eleven participants were added to allow for a 20% drop-out rate.
Continuous variables were compared using Student’s t-test or the Mann−Whitney U-test and are expressed as the mean±standard deviation (SD). Categorical variables were compared using the Chi-square test or Fisher’s exact test. A comparison of differences in values of variables before and after education was conducted using a paired t-test. In all analyses, a P value of <0.05 was considered as indicative of statistical significance based on two-tailed tests. All statistical procedures were performed using SPSS software (version 21.0; IBM Corp., Armonk, NY, USA).
Results
A total of 55 patients were enrolled and their data were analyzed. The baseline characteristics are shown in Table 1. The participants were 68.2±7.9 years and the majority were male (n=54, 98.2%).
 |
Table 1 Baseline Clinical Characteristics |
Primary Outcome
The mean score of COPD knowledge before and after education is presented in Table 2. Compared with the knowledge score before education, the score improved significantly after education (12.51±3.19 vs 17.89±1.37; P < 0.001), with a mean change of 5.38±2.90. The number of correct responses for each item on the knowledge questionnaire improved, andthe result is presented in Table S1.
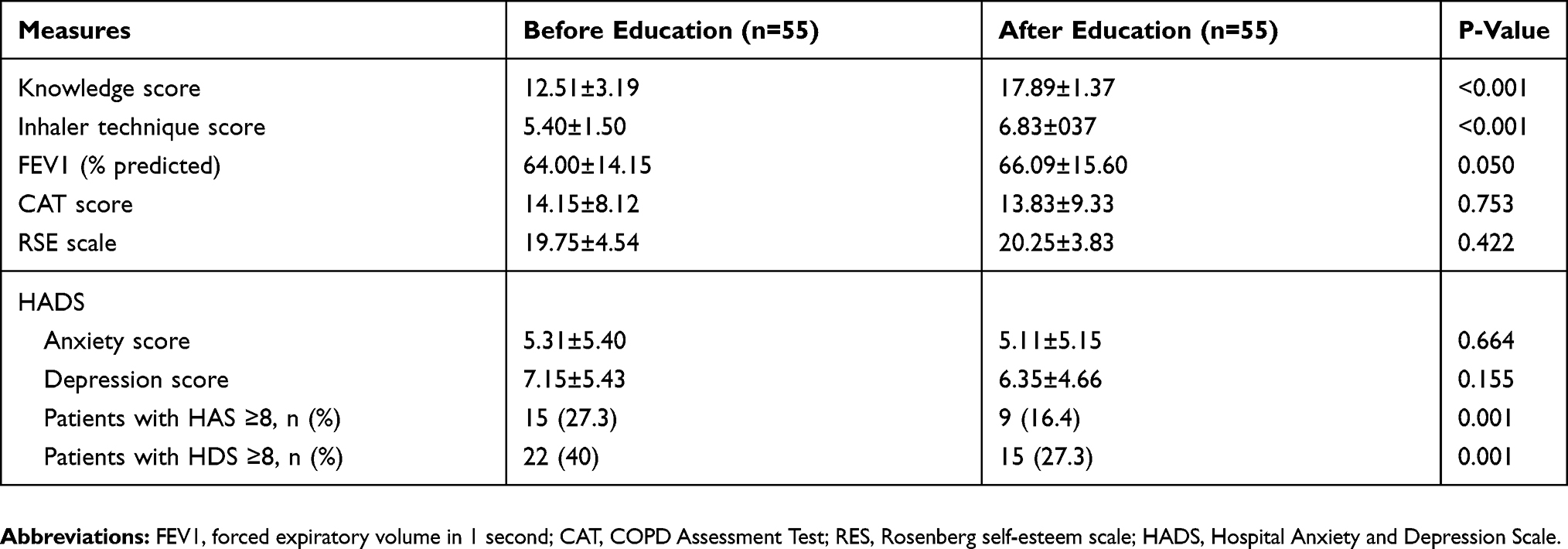 |
Table 2 Change of Measures Before and After Education |
Secondary Outcome
Changes in secondary outcomes between baseline (first visit before education) and third visit are presented in Table 2. Patient inhaler technique was improved following education (5.42±1.50 vs 6.83±0.37). Patient HADSscore also decreased but not significantly (5.31±5.40 vs 5.11±5.15, 7.15±5.43 vs 6.35±4.66, respectively). However, the prevalence of depression and anxiety after education decreased significantly (27.3% vs 16.4%, 40% vs 27.3%, respectively). Patient CAT score decreased but not significantly (14.15±8.12 vs 13.83±9.33; P=0.753). There was no measured difference in mean patient RSES score following education (19.75±4.54 vs 20.25±3.83; P=0.606). FEV1 improved after education but not significantly (64.00±14.15 vs 66.09±15.60; P=0.050).
A comparison was made between the group whose knowledge had increased by more than 5 points (Group B) and the group whose knowledge had not (Group A). Group A had 23 patients and Group B had 32 patients. There was no difference in the level of education between the two groups. In Group B, the CAT score after education was significantly improved (2.61±5.88 vs −2.41±7.48, P=0.01) and the duration of COPD diagnosis before enrollment was significantly shorter (2.72±2.43 vs 5.22±5.11 years, P=0.038) compared to Group B (Table 3).
 |
Table 3 Comparison Between Two Groups |
Discussion
The aim of this study was to provide systematic intensive education to patients with COPD for a short period and to identify the effects of this education comprehensively. To date, there are no studies investigating the appropriate duration of education required to be effective, but several studies have shown that long-term education (12 months,17 48 months18) resulted in a meaningful effect. We wanted to see whether short-term education was as effective as long-term education. For this purpose, a nurse was assigned and trained to educate patients with COPD, and five dedicated respiratory physicians, each with over 10 years of experience, created the contents of the educational program for patients. As shown in the results, two sessions of the face-to-face educational program resulted in a clinical improvement in disease-specific knowledge, enhanced inhaler technique, and a decreased rate of anxiety and depression.
Although pulmonary rehabilitation improved the mean patient CAT score,19 most studies did not show that education alone improves health-related quality of life.20 Our study also failed to prove that disease education affects patient quality of life, as no significant change in mMRC scale and CAT score was observed following education. However, when we made a comparison between the group whose knowledge score after education had increased by 5 points or more (Group B) and those whose knowledge score had not (Group A), the CAT score was significantly improved in Group A. This result may indicate that the more effectively educated group could see benefits with regard to symptom control. Our results also revealed that the duration between COPD diagnosis and receipt of education was shorter in Group A, suggesting that early detection and disease education might enhance disease-specific knowledge and health-related quality of life.
We measured disease-specific knowledge using 17 items from domains in BCKQ10 and 3 items from the article by Lee et al.11 In treatment-related topics, we wanted to emphasize the importance of actual usage of inhaler since treatment adherence is associated with symptom improvement, enhancement of exercise capacity, and quality of life. Therefore, instead of using items in BCKQ which contains more technical questions, we used the items from the study of Lee et al.11
The correct response rate for nearly all items of the questionnaire, as well as total score of knowledge, also improved after education, even though not all scores improved to 100%. The correct response rate for treatment-related questions, which was one of the most emphasized parts during the education, improved to 100% after education. The topics that were answered incorrectly most frequently before education were regarding epidemiology and vaccination, such as “In COPD the word ‘chronic’ means it is severe”, and “A pneumonia jab protects against all forms of pneumonia.” The correct response rate of these topics still remained lowest compared to others even though a slight improvement was shown after education. The low percentage of correct answers to the COPD-definition question demonstrates that awareness for the disease is still low. This point will be more heavily emphasized in future COPD education.
Anxiety and depression are common psychological problems and are associated with a poor prognosis in COPD.21,22 Depression is a significant predictor of medical adherence23 and its prevalence among patients with COPD ranges from 10% to 42%22 and increases with the severity of COPD.24 In this study, the frequency of anxiety and depression among participants was 27% and 40%, respectively, which was similar to that reported previously. Lou et al reported that the incidence of anxiety and depression in the intervention group was significantly lower than in the control group at 48-month assessment,18 but studies on the effectiveness of short-term education and follow-up on anxiety and depression in patients with COPD are relatively rare. As shown in our results, there was no significant change in patient HADS score following education, but the incidence of anxiety and depression was significantly lower after education. Our study showed that the incidence of anxiety and depression was significantly reduced following short-term education, and it is presumed to be due to increased awareness of the disease through education.
Several studies have been conducted that indicate the beneficial effects of pulmonary rehabilitation, including the effects of disease education on self-esteem.25,26 However, there are no studies to date on the relationship between education only and self-esteem. We aimed to assess the effect of education on patients’ self-esteem by using the RSES.14 However, our study did not show a significant relationship between the two. When answering the question about self-esteem, most of the patients did not understand the questions correctly and many hesitated to answer to “strongly agree” or “strongly disagree”. Along with this, the small sample size of our study may have also affected the reliability of the study result. More studies are needed to investigate the relationship between education and self-esteem.
Our study has several limitations. First, our knowledge score was not validated although we quoted many of the items from some parts of the BCKQ. Since the number of questions on the BCKQ is substantial, the patient’s concentration during assessment might decrease and this may lead to unreliable results. However, our questionnaire includes essential items from BCKQ and its validity was confirmed with the consent of five physicians who each had more than 10 years of experience in respiratory medicine. Thus, we assumed that it was appropriate for assessing patient disease-specific knowledge of COPD. Second, due to our small sample size and relatively short-term follow-up period, it was difficult to show a significant association between disease education and its effect on variable measures. However, through short but intensive education, we found that short-term education is also effective. The third limitation of our study is the absence of a control group. We did not recruit a control group because we evaluated the effect of disease education through comparing measures before and after the education in the same patients. As shown in our results, we found important findings in subgroup analysis. But, if our study included an uneducated control group from the beginning, our study could have resulted in a higher level of evidence and ruled out factors that would interfere with the interpretation of the results. The fourth limitation of our study is a remarkably high proportion of male participants at the time of enrollment. This is probably due to the fact that the prevalence of COPD in Korea is still much higher in males than in females,27 and voluntary participation in the study (without gender matching step at the time of enrollment) has led to an extreme increase in the ratio of males. However, in previous studies, the impact of education by gender difference has not been reported.18,28 Therefore, we assumed that there would be no significant problem in interpreting the results of our study.
Conclusion
An organized educational program resulted in improved patient disease-specific knowledge. Disease-specific education is an important part of the treatment of COPD that affects the quality of life and emotional status of patients. Early education after COPD diagnosis is recommended, and the earlier the education starts, the better the result expected.
Abbreviations
BCKQ, Bristol COPD Knowledge Questionnaire; CAT, COPD Assessment Test; COPD, chronic obstructive pulmonary disease; FEV1, forced expired volume in 1 second; FVC, forced vital capacity; HADS, Hospital Anxiety and Depression Scale; mMRC, modified Medical Research Council; RSES, Rosenberg Self-Esteem Scale.
Acknowledgments
This study was supported by a grant from Yeungnam University Research Grant (2016)
Disclosure
The authors report no conflicts of interest in this work.
References
1. Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease 2017 Report. GOLD executive summary. Am J Respir Crit Care Med. 2017;195(5):557–582. doi:10.1164/rccm.201701-0218PP
2. Murray CJ, Lopez AD. Alternative projections of mortality and disability by cause 1990–2020: Global Burden of Disease Study. Lancet. 1997;349(9064):1498–1504. doi:10.1016/S0140-6736(96)07492-2
3. Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2095–2128. doi:10.1016/S0140-6736(12)61728-0
4. Siddique HH, Olson RH, Parenti CM, et al. Randomized trial of pragmatic education for low-risk COPD patients: impact on hospitalizations and emergency department visits. Int J Chron Obstruct Pulmon Dis. 2012;7:719–728. doi:10.2147/COPD.S36025
5. Barnes N, Calverley PM, Kaplan A, Rabe KF. Chronic obstructive pulmonary disease and exacerbations: patient insights from the global hidden depths of COPD survey. BMC Pulm Med. 2013;13:54. doi:10.1186/1471-2466-13-54
6. Ries AL, Bauldoff GS, Carlin BW, et al. Pulmonary rehabilitation: joint ACCP/AACVPR evidence-based clinical practice guidelines. Chest. 2007;131(5 Suppl):4s–42s. doi:10.1378/chest.06-2418
7. Choi JY, Chung HI, Han G. Patient outcomes according to COPD action plan adherence. J Clin Nurs. 2014;23(5–6):883–891. doi:10.1111/jocn.12293
8. Bourbeau J, Nault D, Dang-Tan T. Self-management and behaviour modification in COPD. Patient Educ Couns. 2004;52(3):271–277. doi:10.1016/S0738-3991(03)00102-2
9. Emery CF, Schein RL, Hauck ER, MacIntyre NR. Psychological and cognitive outcomes of a randomized trial of exercise among patients with chronic obstructive pulmonary disease. Health Psychol. 1998;17(3):232–240. doi:10.1037/0278-6133.17.3.232
10. White R, Walker P, Roberts S, Kalisky S, White P. Bristol COPD Knowledge Questionnaire (BCKQ): testing what we teach patients about COPD. Chron Respir Dis. 2006;3(3):123–131. doi:10.1191/1479972306cd117oa
11. Lee JY, Yoo KH, Kim DK, et al. Effects of educational interventions for chronic airway disease on primary care. J Korean Med Sci. 2016;31(7):1069–1074. doi:10.3346/jkms.2016.31.7.1069
12. Bestall JC, Paul EA, Garrod R, Garnham R, Jones PW, Wedzicha JA. Usefulness of the Medical Research Council (MRC) dyspnoea scale as a measure of disability in patients with chronic obstructive pulmonary disease. Thorax. 1999;54(7):581–586. doi:10.1136/thx.54.7.581
13. Jones PW, Harding G, Berry P, Wiklund I, Chen WH, Kline Leidy N. Development and first validation of the COPD assessment test. Eur Respir J. 2009;34(3):648–654. doi:10.1183/09031936.00102509
14. Rosenberg M. Society and the Adolescent Self-Image. Princeton university press; 1965.
15. Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand. 1983;67(6):361–370. doi:10.1111/acp.1983.67.issue-6
16. Price DB, Roman-Rodriguez M, McQueen RB, et al. Inhaler errors in the CRITIKAL study: type, frequency, and association with asthma outcomes. J Allergy Clin Immunol Pract. 2017;5(4):1071–1081.e1079. doi:10.1016/j.jaip.2017.01.004
17. Hernández C, Alonso A, Garcia-Aymerich J, et al. Effectiveness of community-based integrated care in frail COPD patients: a randomised controlled trial. NPJ Primary Care Respir Med. 2015;25:15022.
18. Lou P, Chen P, Zhang P, et al. A COPD health management program in a community-based primary care setting: a randomized controlled trial. Respir Care. 2015;60(1):102–112.
19. Dodd JW, Hogg L, Nolan J, et al. The COPD assessment test (CAT): response to pulmonary rehabilitation. A multicentre, prospective study. Thorax. 2011;66(5):425–429. doi:10.1136/thx.2010.156372
20. Monninkhof E, van der Valk P, Schermer T, van der Palen J, van Herwaarden C, Zielhuis G. Economic evaluation of a comprehensive self-management programme in patients with moderate to severe chronic obstructive pulmonary disease. Chron Respir Dis. 2004;1(1):7–16. doi:10.1191/1479972304cd005oa
21. Cafarella PA, Effing TW, Usmani ZA, Frith PA. Treatments for anxiety and depression in patients with chronic obstructive pulmonary disease: a literature review. Respirology. 2012;17(4):627–638. doi:10.1111/j.1440-1843.2012.02148.x
22. Maurer J, Rebbapragada V, Borson S, et al. Anxiety and depression in COPD: current understanding, unanswered questions, and research needs. Chest. 2008;134(4 Suppl):43s–56s. doi:10.1378/chest.08-0342
23. Khdour MR, Hawwa AF, Kidney JC, Smyth BM, McElnay JC. Potential risk factors for medication non-adherence in patients with chronic obstructive pulmonary disease (COPD). Eur J Clin Pharmacol. 2012;68(10):1365–1373. doi:10.1007/s00228-012-1279-5
24. Omachi TA, Katz PP, Yelin EH, et al. Depression and health-related quality of life in chronic obstructive pulmonary disease. Am J Med. 2009;122(8):
25. Ketelaars CA, Abu-Saad HH, Schlosser MA, Mostert R, Wouters EF. Long-term outcome of pulmonary rehabilitation in patients with COPD. Chest. 1997;112(2):363–369. doi:10.1378/chest.112.2.363
26. Ninot G, Moullec G, Desplan J, Prefaut C, Varray A. Daily functioning of dyspnea, self-esteem and physical self in patients with moderate COPD before, during and after a first inpatient rehabilitation program. Disabil Rehabil. 2007;29(22):1671–1678. doi:10.1080/09638280601055949
27. Kim DS, Kim YS, Jung KS, et al. Prevalence of chronic obstructive pulmonary disease in Korea: a population-based spirometry survey. Am J Respir Crit Care Med. 2005;172(7):842–847. doi:10.1164/rccm.200502-259OC
28. Hill K, Mangovski-Alzamora S, Blouin M, et al. Disease-specific education in the primary care setting increases the knowledge of people with chronic obstructive pulmonary disease: a randomized controlled trial. Patient Educ Couns. 2010;81(1):14–18. doi:10.1016/j.pec.2009.09.035
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.