Back to Journals » International Journal of General Medicine » Volume 19
Comprehensive Analysis of the Relationship Between Cardiometabolic Index and Coronary Heart Disease
Authors Guo R ![]() , Sun M
, Sun M ![]() , Lin W, Yang H
, Lin W, Yang H ![]() , Dou J, Gao J
, Dou J, Gao J ![]() , Wang J, Liu L, Wei T, Liu T, Yang X, Luo D
, Wang J, Liu L, Wei T, Liu T, Yang X, Luo D ![]()
Received 29 September 2025
Accepted for publication 8 January 2026
Published 22 January 2026 Volume 2026:19 563397
DOI https://doi.org/10.2147/IJGM.S563397
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Redoy Ranjan
Ruoling Guo,1,* Mingliang Sun,1,* Wenxin Lin,1 Huihui Yang,1 Jie Dou,1 Jie Gao,2 Ji Wang,3 Lina Liu,3 Tiejun Wei,3 Tong Liu,4 Xiaoyun Yang,3 Donglei Luo3,5
1Graduate School, Chengde Medical University, Chengde, 067000, People’s Republic of China; 2Department of Emergency Medicine, Handan First Hospital, Handan, 056000, People’s Republic of China; 3Department of Cardiology, Chengde Central Hospital/Second Clinical College of Chengde Medical University, Chengde, 067000, People’s Republic of China; 4Tianjin Key Laboratory of Ionic-Molecular Function of Cardiovascular Disease, Department of Cardiology, Tianjin Institute of Cardiology, second Hospital of Tianjin Medical University, Tianjin, 300000, People’s Republic of China; 5Information Centre, Chengde Central Hospital/Second Clinical College of Chengde Medical University, Chengde, 067000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Donglei Luo, Department of Cardiology, Information Centre, Chengde Central Hospital/Second Clinical College of Chengde Medical University, Chengde, 067000, People’s Republic of China, Email [email protected] Xiaoyun Yang, Department of Cardiology, Chengde Central Hospital/Second Clinical College of Chengde Medical University, Chengde, 067000, People’s Republic of China, Email [email protected]
Objective: Emerging evidence substantiates the cardiometabolic index (CMI) as a pivotal indicator demonstrating robust associations with an array of cardiovascular pathologies. However, its specific link to coronary heart disease (CHD) remains insufficiently explored. This study aimed to investigate both the association and the predictive value of CMI for CHD in a clinical cohort.
Methods: This retrospective study included patients with suspected CHD who underwent coronary angiography at the Cardiology Department of Chengde Central Hospital between October 2023 and December 2024. Participants were stratified into CHD and non-CHD groups based on angiographic results. A LASSO regression and a logistic regression framework was implemented to examine the influence of age, sex, hypertension, diabetes, smoking, WBC, CK, CMI, and LDL-C on CHD. The association between CMI and CHD was explored using restricted cubic spline (RCS) methodology. The diagnostic efficacy of the model was scrutinized through the utilization of the area under the curve (AUC).
Results: CMI exhibits an independent predictor for CHD, particularly in individuals with high CMI values (Q4 group), where the risk of CHD is markedly elevated. Furthermore, a linear relationship exists between CMI and CHD. Calibration curves demonstrate a strong alignment correlation linking predicted to observed probabilities. Decision curve analysis (DCA) reveals that the model provides substantial clinical benefit within a threshold probability range of 0.13 to 0.72. Receiver operating characteristic (ROC) curve analysis indicates that CMI possesses certain predictive merit for the occurrence of CHD.
Conclusion: A positive association exists between CMI and incidence of CHD. Additionally, CMI serves as an independent risk factor, demonstrating certain predictive power in clinical settings, thereby effectively forecasting the risk of CHD occurrence.
Keywords: coronary heart disease, cardiometabolic index, restricted cubic spline
Introduction
CHD represents a formidable challenge in global public health, maintaining a persistently high disease burden. Epidemiological evidence reveals that CHD not only occupies a preeminent position within the global spectrum of cardiovascular diseases but also contributes significantly to morbidity and mortality rates.1 Projections indicate that by 2035, CHD is anticipated to account for approximately 32% of global mortality.2 Notably, contemporary studies demonstrate a discernible downward tendency in CHD incidence within developed nations,3 primarily attributed to the rigorous implementation of evidence-based primary and secondary preventive strategies.4 This epidemiological transition underscores the imperative of early disease detection through advanced diagnostic modalities. Consequently, there exists an urgent requirement to expedite the identification of robust predictive indicators, enhance recognition of subclinical CHD manifestations, and formulate targeted therapeutic regimens to mitigate its epidemiological impact.
With the shift in dietary patterns, the global prevalence of obesity has exhibited a gradual upward trajectory. Current statistics delineate that approximately 1.6 billion adults manifest obesity-related phenotypes, with projections indicating this figure will escalate exponentially to 3.3 billion by 2030.5 Obesity is pathophysiologically recognized as a significant risk factor for the progression of CHD, primarily mediated through its synergistic interaction with atherogenic dyslipidemia6 — a metabolic derangement characterized by hypertriglyceridemia and depressed high-density lipoprotein cholesterol (HDL-C) concentrations.7 Emerging evidence substantiates the clinical significance of novel visceral adiposity indices. In 2015, Wakabayashi I. pioneered CMI, an innovative indicator integrating lipidemic perturbations with central adiposity parameters through mathematical derivation of the product between triglyceride-to-HDL-C ratio (TG/HDL-C) and waist-to-height ratio (WHtR).8 CMI surpasses traditional anthropometric measures such as BMI, Waist Circumference (WC), and WHtR in risk stratification for diabetes, atherosclerosis, and cardiovascular diseases,9 and holds promise as a crucial indicator for the prevention of cardiovascular diseases. Cai et al10 discerned a positive correlation between CMI levels and the risk of incident cardiovascular diseases in patients with hypertension and obstructive sleep apnea. Moreover, within individuals exhibiting elevated baseline cardiovascular metabolic risks, the degree of increase in CMI over time was found to be significantly associated with a heightened risk of subsequent cardiovascular events.11 Currently, elevated levels of CMI are associated with an increased risk of cardiovascular disease (CVD), chronic kidney disease (CKD), and non-alcoholic fatty liver disease (NAFLD).12,13
As an innovative visceral fat index, the cardiometabolic index (CMI) has been substantiated as being closely linked to cardiovascular metabolic disorders. Even so, limited research has investigated the link between CMI and the onset of CHD. Previous research has predominantly concentrated on broader cardiovascular outcomes or metabolic syndrome, thereby leaving the relationship between CMI and CHD—particularly among clinically relevant populations suspected of having CHD, insufficiently explored. This dearth of evidence targeting specific diseases consequently constrains the clinical applicability of CMI in the risk stratification and management of CHD. Therefore, the principal objective of this study is to explore the relationship between CMI and the onset of CHD.
Material and Methods
Study Subjects
This study is a single-center retrospective study. This enrollment cohort comprised 913 admitted patients undergoing diagnostic coronary angiography (CAG) for suspected CHD at the Cardiology Department of Chengde Central Hospital between October 2023 and December 2024. Based on the CAG results, eligible patients were classified into the CHD cohort and the non - CHD cohort.
Inclusion and Exclusion Criteria
Inclusion Criteria
(1) Consecutive enrollment of patients aged exceeding 18 years presenting with angina-equivalent symptoms (chest discomfort or dyspnea) who are deemed appropriate candidates for invasive CAG; (2) Patients with complete general clinical data and relevant auxiliary examination results.
Exclusion Criteria
(1) Patients with a documented history of coronary revascularization, encompassing fibrinolytic therapy, percutaneous coronary intervention (PCI), or surgical bypass grafting (CABG); (2) Patients with a history of valvular heart disease or severe heart failure (NYHA classification ≥2); (3) Individuals with documented histories of chronic kidney disease (CKD) or decompensated hepatic insufficiency; (4) Patients with contraindications to CAG.
Data Collection
Baseline data were collected for all patients, including: (1) Demographic characteristics: age, sex, height, weight, and waist circumference (WC), with the body mass index (BMI) derived by dividing weight in kilograms (kg) by the square of height in meters (m2); (2) Medical history: smoking, drinking, diabetes mellitus (DM), and hypertension; (3) Vital signs: diastolic blood pressure (DBP) and heart rate (HR); (4) Initial laboratory parameters following admission (obtained from morning fasting venous blood samples drawn on admission): red blood cells (RBC), white blood cells (WBC), hemoglobin (Hb), platelets (PLT), thyroid-stimulating hormone (TSH), aspartate aminotransferase (AST), creatine kinase (CK), triglycerides (TG), total cholesterol (TC), lipoprotein(a) [Lp(a)], high-density lipoprotein (HDL-C), cystatin C (CysC) and low-density lipoprotein (LDL-C).
Relevant Definitions
Diagnostic criteria for suspected CHD include the following: 1. The presence of typical clinical symptoms, such as characteristic or atypical chest pain, angina pectoris, and palpitations, which align with the clinical features of angina. These symptoms are often related to physical exertion or emotional distress and may be alleviated by rest or the administration of nitrates. 2. Electrocardiographic findings: The electrocardiogram (ECG) may exhibit signs of myocardial ischemia, such as ST-segment depression or T-wave inversion, either at rest or during episodes of discomfort. 3. Cardiac biomarkers: There may be a mild elevation or inconclusive range of cardiac troponins (cTnI/cTnT). 4. Cardiovascular risk factors: The patient should present with at least two major risk factors, which may include hypertension, diabetes mellitus, dyslipidemia, smoking, and a family history of early-onset coronary heart disease. If two or more of the specified criteria are met, a diagnosis of suspected coronary heart disease can be established.
CHD was angiographically defined as ≥50% luminal diameter stenosis (LDS) in at least one major coronary artery (left anterior descending, circumflex, or right coronary artery) or their primary tributaries.14 The CAG procedure was performed by an experienced cardiologist, and the results were independently assessed by two proficient, interventional cardiologists, who had no conflicts of interest with the study. In the event of any discrepancies between assessments, a third cardiologist was consulted to reach a consensus.
CMI is characterized as the product of TG/HDL-C and WHtR. [CMI = (TG/HDL-C) * (WC/Height)].13
Data Quality and Missing Data
A comprehensive assessment of the data’s integrity and consistency was performed. All missing values were classified as missing completely at random (MCAR), with the proportion of missing data being less than 10% of the overall sample size. Any discrepancies or incomplete data were rectified and completed. For cases with a substantial amount of missing data, direct deletion was employed. For continuous independent variables with complete data, regression estimation using SPSS was applied, while for categorical independent variables with complete data, mode imputation was utilized.
Statistical Analysis
This study employed SPSS 27.0 software (IBM Corporation, Armonk, NY, USA) for comprehensive statistical analyses, while graphical visualizations were generated using GraphPad Prism 8.0 and R 4.4.1, facilitating data interpretation. The normality distribution assumption for continuous parameters was rigorously evaluated through the implementation of the Shapiro–Wilk. Parametrically distributed continuous variables were characterized by arithmetic mean ± standard deviation (± SD) and analyzed using the independent samples t-tests, while non-Gaussian variables were expressed as median with interquartile range (Q1, Q3) and evaluated via Wilcoxon-Mann–Whitney U-tests. Categorical data are presented as percentages (%), and the Chi-square (χ2) test was employed for analysis, with statistical significance thresholding at P < 0.05. We incorporated the baseline data into a Least Absolute Shrinkage and Selection Operator Regression (LASSO) regression framework to facilitate variable selection. Utilizing a ten-fold cross-validation methodology, we determined the optimal penalty coefficient (λ). Adopting a more conservative λ value, specifically the λ.1se, we identified the following variables with non-zero coefficients: hypertension, gender, smoking status, CMI, diabetes, LDL-C, age, WBC, and CK. Subsequently, these nine variables were integrated into a multifactorial logistic regression analysis to compute the odds ratios (OR) and their 95% confidence intervals (CI). The multivariable logistic regression model was visualized, and the corresponding nomogram was plotted. The interrelationship between CMI and CHD was further evaluated using RCS to determine linearity. Subgroup analyses were carried out to determine whether covariates modified the connection between CMI and CHD, with an interaction considered significant at P < 0.05. We utilized receiver operating characteristic (ROC) curves and AUC to evaluate the diagnostic capability of the model. The Variance Inflation Factor (VIF) was assessed to evaluate the multicollinearity among the influencing factors. The Hosmer-Lemeshow test and calibration curve were employed to evaluate the predictive capability of CMI for CHD, with a P-value > 0.05 indicating strong model calibration and good fit. To ensure the reliability of the model, DCA was performed to assess its effectiveness in supporting clinical decision-making.
Results
Clinical Baseline Data Comparisons
In total, 226 individuals were excluded according to the established exclusion criteria, resulting in 687 participants eligible for inclusion in the study. Among them, 548 patients with CHD were assigned to the case group, while 139 non-CHD patients were placed in the control group. Statistically significant disparities were identified between the Non-CHD and CHD groups concerning age, sex, hypertension, smoking, WBC, TG, HDL-C, CK, and CMI (P < 0.05). (Table 1, Figure 1).
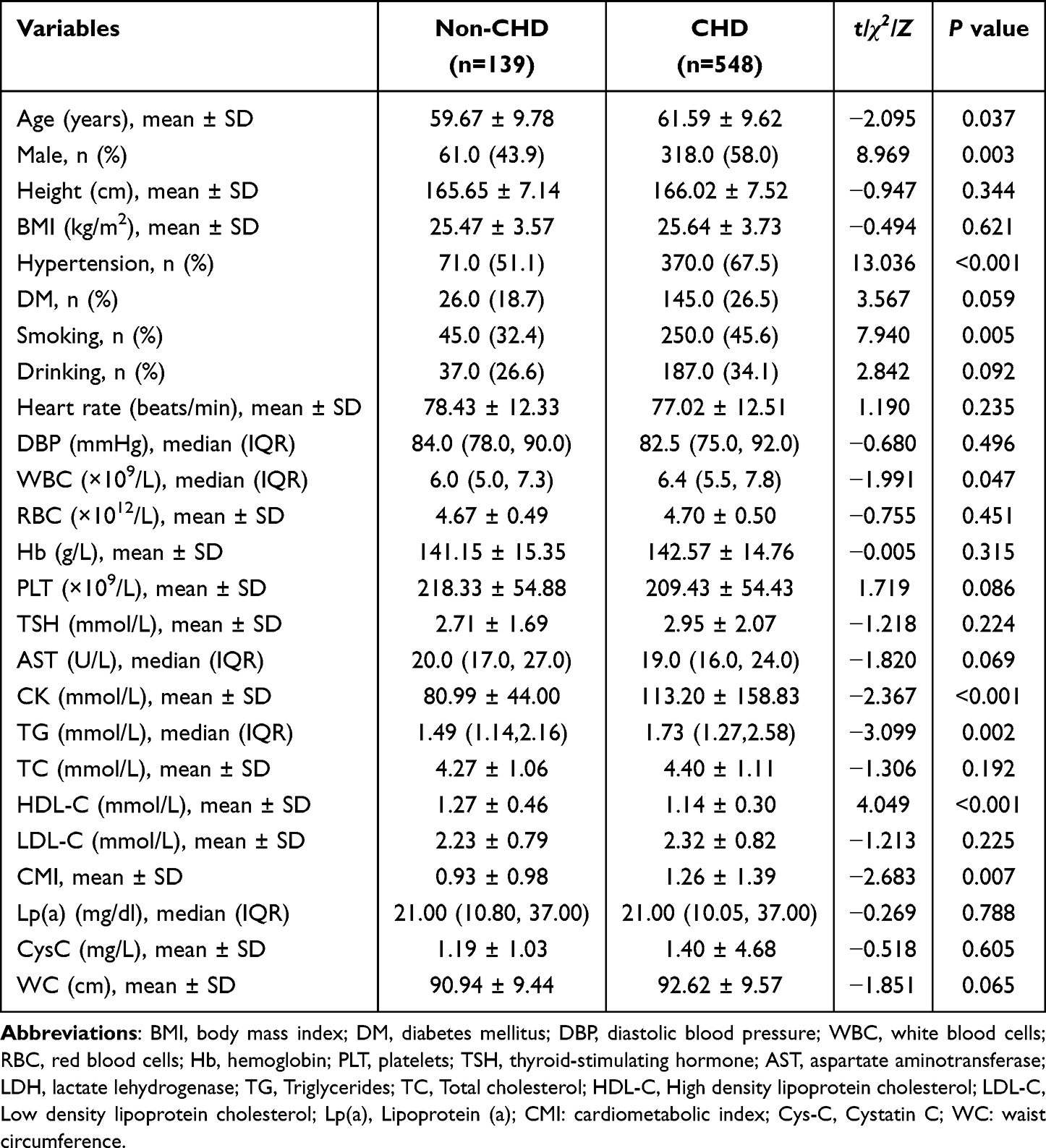 |
Table 1 Baseline Characteristics with and Without CHD |
 |
Figure 1 Flow-diagram illustrating patient flow in the trial. |
Association of CMI with CHD
We employed LASSO regression analysis to select relevant variables, utilizing the λ.1se criterion to identify nine significant factors: age, gender, hypertension, diabetes, smoking status, WBC, CK, CMI, and LDL-C. Subsequently, these variables were incorporated into a multifactorial logistic regression analysis to calculate the odds ratios OR and their corresponding 95% CI, thereby elucidating the associated risk factors. Multivariable logistic regression, accounting for these factors, manifested that age, sex, hypertension, CK, and CMI emerge as independent risk factors for CHD. The findings from the multivariable logistic regression were depicted through the development of a nomogram, enabling the estimation of the likelihood of CHD incidence. As illustrated in Figure 2a, the probability of CHD for the patient ranked 118th in the dataset is 85%. The unadjusted model results demonstrated a notable positive interrelation between CMI and CHD (OR: 1.421, 95% CI: 1.107–1.823). Subsequent to the adjustment for age and sex, the results of Model 2 remained consistent (OR: 1.510, 95% CI: 1.078–1.805). Further adjustment for hypertension, diabetes, smoking, WBC, and CK, LDL-C in Model 3 continued to show a significant positive correlation between CMI and CHD (OR: 1.360, 95% CI: 1.061–1.742). These findings suggest a statistically significant association between CMI and coronary heart disease (P = 0.008). When CMI was stratified into quartiles for group comparison, the results from Model 3, adjusted for covariates, revealed that, compared with the Q1 group, the OR for the Q4 group was 2.071 (95% CI: 1.019–4.210), with a significant trend (P = 0.003). As the quartile increased, the exposure risk also increased significantly (P < 0.05). Additionally, the connection between CMI and CHD was further explored using RCS, which indicated a linear interrelationship between the two variables (P for linearity > 0.05). (Table 2, Table 3, Supplementary Material Figure 1, Figure 2b, Figure 3).
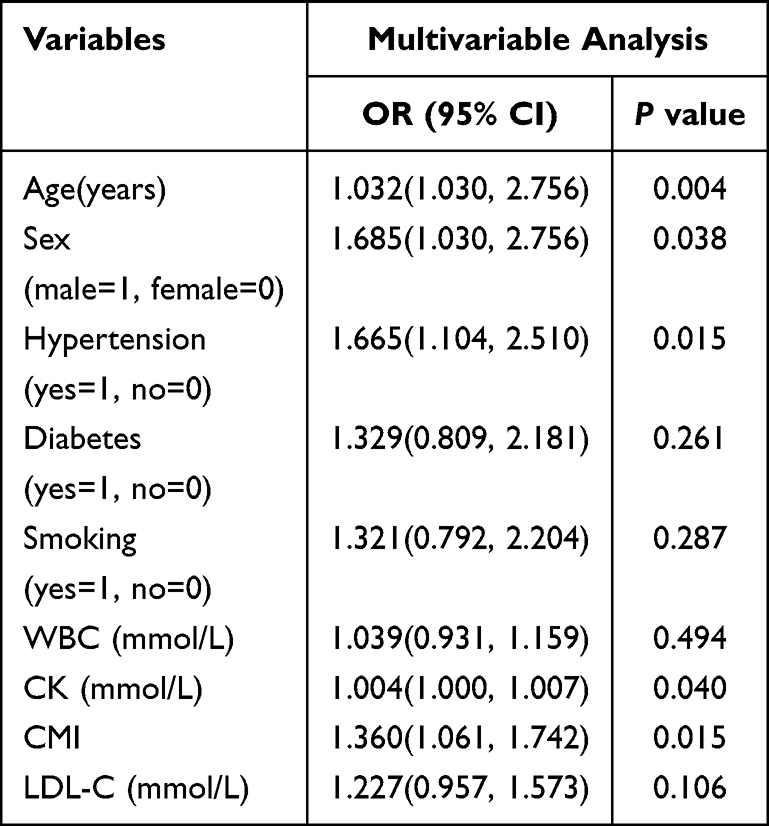 |
Table 2 The Multivariable Logistic Analysis of CHD by CMI |
 |
Table 3 Association Between Cardiometabolic Index and CHD |
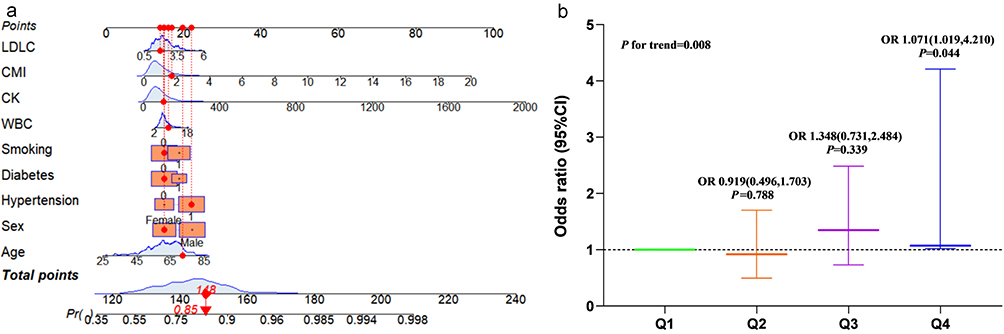 |
Figure 2 Nomogram of CMI and Forest plots for Model 3. (a): the predicted risk probability of CHD for the 118th patient in the nomogram. (b): the forest plot of model 3 quartiles. |
 |
Figure 3 RCS for CMI. |
Subgroup Analysis
We conducted a subgroup analysis based on age (≤ 65 years, > 65 years), sex (male, female), hypertension (yes, no), diabetes (yes, no), and smoking status (yes, no) to investigate the link between CMI levels and CHD, while also performing an interaction analysis. The stratified analysis results revealed no significant interaction effects among the aforementioned variables. This suggests that CMI is independently associated with CHD risk, and this association remains relatively consistent across different subgroups (P for interaction > 0.05). (Supplementary Material Figure 2).
Evaluation Model Value
We constructed calibration curves, DCA curves, and ROC curves to assess the predictive value of CMI for the occurrence of CHD. The calibration curve indicated a Hosmer-Lemeshow test result of 0.210, with VIF for each independent risk factor being less than 10, suggesting the absence of multicollinearity and indicating a good fit. (Supplementary Material Table 1). This further implies a strong concordance between the anticipated and actual probabilities. (Figure 4a). DCA was performed to assess the model’s effectiveness in facilitating clinical decision-making. The model demonstrated substantial clinical benefit across a threshold probability range of 0.13 to 0.72. (Figure 4b). The prognostic utility of CMI in CHD risk was quantified by an AUC of 0.680 (95% CI: 0.629–0.730), demonstrating 79.90% diagnostic sensitivity coupled with a 48.20% specificity threshold. (Figure 5). These findings imply that CMI possesses a modest prognostic potential in forecasting the onset of CHD.
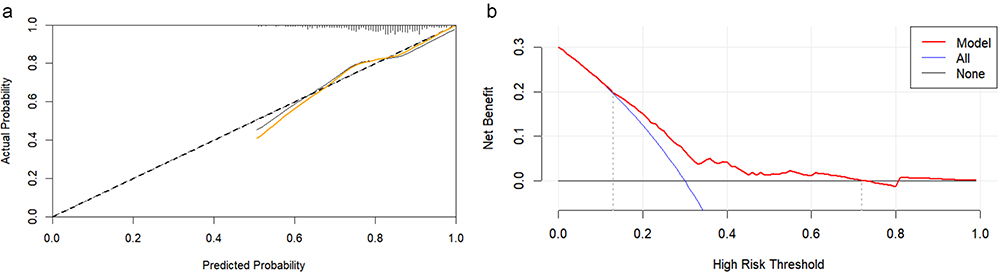 |
Figure 4 Calibration curves and Decision curve for CMI. (a): the calibration curve of CMI for predicting CHD. (b): the decision curve for CMI to predict CHD. |
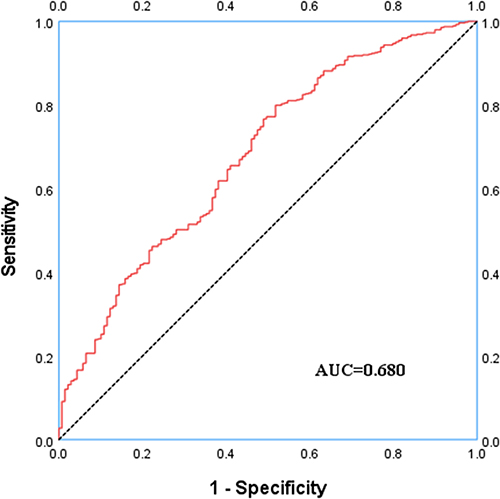 |
Figure 5 ROC analysis with respect to the detection of CHD. |
Discussion
This study demonstrates a modest association between CMI and CHD, establishing CMI as an independent risk factor for CHD. This finding highlights the potential of CMI as a predictive tool for the occurrence of coronary heart disease. We employed LASSO regression analysis to identify pertinent variables, ultimately selecting nine significant factors: age, sex, hypertension, diabetes, smoking status, WBC, CK, CMI, and LDL-C. We performed a quartile-based stratified analysis of CMI, adjusting for potential confounders such as age, sex, hypertension, diabetes, smoking, WBC, CK, and LDL-C. The findings reveal a stepwise increase in the prevalence of CHD as CMI levels rise, and this trend was further validated in a multivariable logistic regression model (P for trend < 0.05). Furthermore, we employed RCS analysis to explore the possible non-linear interconnection between CMI and CHD. The results indicated a linear association between CMI and CHD, with a nonlinearity P-value of 0.101, thereby confirming the linear correlation between the two. Subgroup analysis revealed no significant interaction effects among different subgroups (P for interaction > 0.05), uncovering that the association between CMI and CHD is independent and not significantly influenced by other variables. Therefore, this study further corroborates the close relationship between CMI and CHD, providing important evidence for the clinical application of CMI as an independent risk factor. A study from the National Health and Nutrition Examination Survey (NHANES) demonstrated a significant positive correlation between CMI and atherosclerotic cardiovascular disease (ASCVD) (OR:1.10, 95% CI:1.04–1.16), revealing a linear relationship. These findings are consistent with the results of the present study.15
In recent years, WHtR has emerged as a prominent metric, gaining increasing attention and widespread application in the screening of cardiovascular and metabolic disorder risks. Compared to traditional obesity indicators such as WC and BMI, WHtR offers a more accurate assessment of obesity risk,16 as it takes into account variations in height, sex, and ethnicity. Studies have demonstrated that WHtR outperforms WC or BMI alone in identifying abdominal fat accumulation, and its predictive value as a risk factor for cardiovascular diseases is superior.17 Existing studies have hinted that a WHtR threshold of 0.5 serves as a superior indicator for predicting cardiovascular disease risk in both sexes within European populations.18 In a study conducted on the Kurdish population, the critical values for WHtR were identified as 0.56 for males and 0.65 for females, demonstrating their utility in predicting the occurrence of cardiovascular events.19 TG and HDL-C are widely recognized as closely associated with CHD, with TG acting as a prominent risk factor and HDL-C providing a protective effect. As a result, there has been a burgeoning interest in the exploration of the complex interplay between elevated plasma triglyceride levels and lowered HDL-C concentrations within the context of cardiovascular pathologies. Notably, the TG/HDL-C ratio is strongly linked to central obesity, a key feature of metabolic syndrome (MetS), which is significantly associated with the risk of cardiovascular disease onset.20 Studies have demonstrated that the TG/HDL-C ratio is a significant risk factor for cardiovascular diseases.21,22 A study conducted in China confirmed that the TG/HDL-C ratio is an independent risk factor for coronary artery calcification and atherosclerosis, exhibiting strong diagnostic efficacy.23 Nevertheless, research has indicated that the optimal TG/HDL-C threshold for identifying cardiovascular metabolic risk varies between male and female populations.24 As an emerging composite metric integrating adiposity and dyslipidemia parameters, CMI demonstrates unique advantages in circumventing gender-specific confounders while quantifying visceral adipose tissue (VAT) distribution, with recent validation studies confirming its potential utility for obesity-associated metabolic disorders.25,26 Recent studies have further elucidated the deterministic association between CMI and CVD. For instance, a study involving 11,258 participants manifested that CMI was an independent predictor of left ventricular remodeling in the rural Chinese population, with a particularly pronounced predictive effect for left ventricular remodeling in females.27 A 2024 study investigated the link between CMI and heart failure, attesting that CMI holds substantial diagnostic value in heart failure, particularly within populations exhibiting abdominal obesity or dyslipidemia.28 This research represents the first investigation into the relationship between CMI and CHD, with the findings indicating a significant positive correlation between the two. The AUC of 0.680 postulates that CMI demonstrates commendable diagnostic performance in predicting CHD. Taken together, these findings underscore the broad potential of CMI in assessing cardiovascular health and preventing CVD.
Our research findings hold significant clinical implications. CMI, derived from simple routine assessments (WC, height, TG, and HDL-C), presents a practical tool for risk evaluation. It can be utilized in primary care settings or for the nuanced stratification of preliminary risk in patients suspected of coronary artery disease, potentially identifying individuals who might benefit from more proactive lifestyle modifications or pharmacological interventions—especially those whose traditional risk scores are categorized as moderate. Furthermore, this linear relationship indicates that even modest reductions in CMI achieved through weight management or lipid-lowering strategies may confer cardiovascular advantages. While it cannot supplant existing diagnostic modalities, CMI serves as a valuable monitoring parameter for the long-term tracking of metabolic health and the assessment of responses to preventive therapies. Future prospective studies and interventional research are warranted to validate its effectiveness in guiding clinical decision-making and enhancing patient prognoses.
Notwithstanding, this study has several limitations: (1) The WC measurement was assessed only once, which may introduce classification error bias; (2) The sample size in this study is relatively small, necessitating further expansion for greater statistical power; (3) This study did not incorporate dynamic body composition monitoring techniques, such as bioelectrical impedance analysis, to obtain data on visceral fat changes.
Conclusions
There exists a modest correlation between CMI and CHD, with CMI demonstrating a certain predictive value for the onset of this condition. Future research endeavors, should they further validate the clinical applicability of CMI, may enable clinicians to assess the risk of coronary heart disease by modulating individual CMI levels, thereby providing a valuable reference for enhancing patient prognosis.
Abbreviations
CMI, cardiometabolic index; CHD, coronary heart disease; CVD, cardiovascular disease; CKD, chronic kidney disease; NAFLD, non-alcoholic fatty liver disease; PCI, percutaneous coronary intervention; CAG, coronary angiography; CABG, coronary artery bypass grafting; BMI, body mass index; DM, diabetes mellitus; DBP, diastolic blood pressure; WBC, white blood cells; RBC, red blood cells; Hb, hemoglobin; PLT, platelets; TSH, thyroid-stimulating hormone; AST, aspartate aminotransferase; LDH, lactate lehydrogenase; TG, Triglycerides; TC, Total cholesterol; HDL-C, High density lipoprotein cholesterol; LDL-C, Low density lipoprotein cholesterol; Lp(a), Lipoprotein (a); Cys-C, Cystatin C; LASSO, Least Absolute Shrinkage and Selection Operator Regression; ROC, receiver operating characteristic; DCA, decision curve analysis; AUC, the area under ROC curve; MCAR, Missing Completely at Random; CI, confidence interval; OR, odds ratio; DCA, decision curve analysis; MetS, metabolic syndrome; NHANES, National Health and Nutrition Examination Survey; ASCVD, atherosclerotic cardiovascular disease; VAT, visceral adipose tissue.
Data Sharing Statement
The datasets generated and/or analysed during the current study are not publicly available due to patient privacy reasons but are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This study was approved by the Ethics Committee of Chengde Central Hospital. (Ethics number: ChiCTR2000041499). All participating subjects were fully aware of the trial and signed informed consent. All procedures strictly adhered to the guidelines outlined in the Declaration of Helsinki.
Acknowledgments
Ruoling Guo and Mingliang Sun are joint first authors for this study. The authors extend sincere thanks to the members of the Chengde Central Hospital for their contribution.
Author Contributions
DL: contributed to the design and conduct of the study, led data validation, project administration, funding acquisition, review and approval of the manuscript, and decision to submit the manuscript for publication. RL and ML: contributed to the collection, analysis, and interpretation of the data, as well as preparation and editing of the manuscript. WX, HH, JD, and JG: contributed to the collection and management of the data. XY: contributed to the design and conduct of the study, review and approval of the manuscript, and decision to submit the manuscript for publication. JW, LL, TJ, and TL facilitated the planning and carrying out of the study. All authors contributed to the final version of the manuscript. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was funded by Medical Science Research Project of Hebei Province (No. 20200348), S&T Program of Chengde (No. 202109A019), and Project for Cultivating Innovative Ability of Postgraduates at Chengde Medical University (No. CYCXZZ202508).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Bergmark BA, Mathenge N, Merlini PA, Lawrence-Wright MB, Giugliano RP. Acute coronary syndromes. Lancet. 2022;399(10332):1347–11. doi:10.1016/S0140-6736(21)02391-6
2. Ma X, Mei S, He Y, et al. Unraveling the association and regulatory role of miR-146b-5p in coronary artery disease. BMC Cardiovasc Disord. 2025;25(1):81. doi:10.1186/s12872-025-04530-0
3. Benjamin EJ, Blaha MJ, Chiuve SE, et al. Heart disease and stroke statistics-2017 update: a report from the American heart association. Circulation. 2017;135:e146–e603. doi:10.1161/CIR.0000000000000485
4. Chen ML, Li J, Iyer KR, et al. Premorbid predictors of death at initial presentation of coronary heart disease in the Women’s Health Initiative study. Am. J Prev Cardiol. 2025;21:100931. doi:10.1016/j.ajpc.2025.100931
5. Koenen M, Hill MA, Cohen P, Sowers JR. Obesity, adipose tissue and vascular dysfunction. Circ Res. 2021;128(7):951–968. doi:10.1161/CIRCRESAHA.121.318093
6. Valenzuela PL, Carrera-Bastos P, Castillo-García A, Lieberman DE, Santos-Lozano A, Lucia A. Obesity and the risk of cardiometabolic diseases. Nat Rev Cardiol. 2023;20(7):475–494.
7. Hokanson JE, Austin MA. Plasma triglyceride level is a risk factor for cardiovascular disease independent of high-density lipoprotein cholesterol level: a meta-analysis of population-based prospective studies. J Cardiovasc Risk. 1996;3(2):213–219. doi:10.1097/00043798-199604000-00014
8. Wakabayashi I, Daimon T. The cardiometabolic index as a new marker determined by adiposity and blood lipids for discrimination of diabetes mellitus. Clin Chim Acta. 2015;438:274–278. doi:10.1016/j.cca.2014.08.042
9. Guo T, Zhou Y, Yang G, Sheng L, Chai X. Association between cardiometabolic index and hypertension among US adults from NHANES 1999-2020. Sci Rep. 2025;15(1):4007. doi:10.1038/s41598-025-87029-0
10. Cai X, Hu J, Wen W, et al. Associations of the cardiometabolic index with the risk of cardiovascular disease in patients with hypertension and obstructive sleep apnea: results of a longitudinal cohort study. Oxid Med Cell Longev. 2022;2022:4914791. doi:10.1155/2022/4914791
11. Merkin SS, Karlamangla A, Elashoff D, Grogan T, Seeman T. Change in cardiometabolic score and incidence of cardiovascular disease: the multi-ethnic study of atherosclerosis. Ann Epidemiol. 2015;25(12):912–7.e1. doi:10.1016/j.annepidem.2015.09.006
12. Zou J, Xiong H, Zhang H, Hu C, Lu S, Zou Y. Association between the cardiometabolic index and non-alcoholic fatty liver disease: insights from a general population. BMC Gastroenterol. 2022;22(1):20. doi:10.1186/s12876-022-02099-y
13. Miao M, Deng X, Wang Z, et al. Cardiometabolic index is associated with urinary albumin excretion and renal function in aged person over 60: data from NHANES 2011–2018. Int J Cardiol. 2023;384:76–81. doi:10.1016/j.ijcard.2023.04.017
14. Xu B, Tu S, Song L, et al. Angiographic quantitative flow ratio-guided coronary intervention (FAVOR III China): a multicentre, randomised, sham-controlled trial. Lancet. 2021;398(10317):2149–2159. doi:10.1016/S0140-6736(21)02248-0
15. Wei Q, Cheng X, Li M, Wu K, Chen M, Zhang D. Associations between the cardiometabolic index and atherosclerotic cardiovascular disease acorss different glucose metabolism statuses: insights from NHANES. 1999-2020 Lipids Health Dis. 2025;24(1):93.
16. Zhuang Y, Wang Y, Sun P, Ke J, Chen F. Association between triglyceride glucose-waist to height ratio and coronary heart disease: a population-based study. Lipids Health Dis. 2024;23(1):162.
17. Chen J, Li M, Hao B, et al. Waist to height ratio is associated with an increased risk of mortality in Chinese patients with heart failure with preserved ejection fraction. BMC Cardiovasc Disord. 2021;21(1):263. doi:10.1186/s12872-021-02080-9
18. Ashwell M, Hsieh SD. Six reasons why the waist-to-height ratio is a rapid and effective global indicator for health risks of obesity and how its use could simplify the international public health message on obesity. Int J Food Sci Nutr. 2005;56(5):303–307.
19. Pasdar Y, Moradi S, Moludi J, et al. Waist-to-height ratio is a better discriminator of cardiovascular disease than other anthropometric indicators in Kurdish adults. Sci Rep. 2020;10(1):16228. doi:10.1038/s41598-020-73224-8
20. Kosmas CE, Rodriguez Polanco S, Bousvarou MD, et al. The triglyceride/high-density lipoprotein cholesterol (TG/HDL-C) ratio as a risk marker for metabolic syndrome and cardiovascular disease. Diagnostics. 2023;13(5):929. doi:10.3390/diagnostics13050929
21. Wu Z, Cui H, Li W, et al. Comparison of three non-insulin-based insulin resistance indexes in predicting the presence and severity of coronary artery disease. Front Cardiovasc Med. 2022;9:918359. doi:10.3389/fcvm.2022.918359
22. Che B, Zhong C, Zhang R, et al. Triglyceride-glucose index and triglyceride to high-density lipoprotein cholesterol ratio as potential cardiovascular disease risk factors: an analysis of UK biobank data. Cardiovasc Diabetol. 2023;22(1):34. doi:10.1186/s12933-023-01762-2
23. Wang B, Hua J, Ma L. Triglyceride to high-density lipoprotein ratio can predict coronary artery calcification. Pak J Med Sci. 2022;38(3Part–I):624–631.
24. Murguía-Romero M, Jiménez-Flores JR, Sigrist-Flores SC, et al. Plasma triglyceride/HDL-cholesterol ratio, insulin resistance, and cardiometabolic risk in young adults. J Lipid Res. 2013;54(10):2795–2799. doi:10.1194/jlr.M040584
25. Xi WF, Yang AM. Association between cardiometabolic index and controlled attenuation parameter in U.S. adults with NAFLD: findings from NHANES (2017-2020). Lipids Health Dis. 2024;23(1):40. doi:10.1186/s12944-024-02027-x
26. Acharya M, Berger R, Popov AF. The role of the advanced organ support (ADVOS) system in critically ill patients with multiple organ failure. Artif Organs. 2022;46(5):735–746. doi:10.1111/aor.14188
27. Wang H, Sun Y, Li Z, et al. Gender-specific contribution of cardiometabolic index and lipid accumulation product to left ventricular geometry change in general population of rural China. BMC Cardiovasc Disord. 2018;18(1):62. doi:10.1186/s12872-018-0798-0
28. Zhu XM, Xu Y, Zhang J. Cardiometabolic Index is associated with heart failure: a cross-sectional study based on NHANES. Front Med Lausanne. 2024;11:1507100. doi:10.3389/fmed.2024.1507100
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Assessment of the Association Between Cardiac Metabolic Markers and Carotid Atherosclerosis, and the Role of Insulin Resistance
Sun Y, Bai C, Yin S, Liu J
Diabetes, Metabolic Syndrome and Obesity 2025, 18:2899-2911
Published Date: 15 August 2025