Back to Journals » Advances in Medical Education and Practice » Volume 13
Competency Framework for Podiatric Medicine Training in Canada: An Adapted Delphi Study
Authors Blanchette V ![]() , Andoulsi Y
, Andoulsi Y ![]() , Brousseau M
, Brousseau M ![]() , Leblanc C, Guillemette F, Hue O
, Leblanc C, Guillemette F, Hue O ![]()
Received 28 April 2022
Accepted for publication 13 September 2022
Published 1 October 2022 Volume 2022:13 Pages 1207—1241
DOI https://doi.org/10.2147/AMEP.S372324
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Virginie Blanchette,1 Yassin Andoulsi,1 Martine Brousseau,2 Céline Leblanc,3 François Guillemette,4 Olivier Hue1
1Department of Human Kinetics and Podiatric Medicine, Université du Québec à Trois-Rivières, Trois-Rivières, QC, Canada; 2Occupational Therapy Department, Université du Québec à Trois-Rivières, Trois-Rivières, QC, Canada; 3Bureau de pédagogie et de formation à distance (Pedagogy and Distance Education Office), Université du Québec à Trois-Rivières, Trois-Rivières, QC, Canada; 4Education Department, Université du Québec à Trois-Rivières, Trois-Rivières, QC, Canada
Correspondence: Virginie Blanchette, Department of Human Kinetics and Podiatric Medicine, Université du Québec à Trois-Rivières, 3351 Boul. Des Forges, Trois-Rivières, QC, G8Z 4M3, Canada, Tel +1-819-376-5011 Extension: 3756, Email [email protected]
Purpose: Podiatrists are generally defined as professionals with high-level skills in the prevention and management of local foot conditions that are not systemic diseases. Across countries, different academic trainings are implemented due to the specific context and practice of podiatric medicine. It is thus essential to support country-specific podiatry education for the development of highly skilled podiatrists. Therefore, we report the development of a podiatric medicine competency framework to support training in Canada.
Participants and Methods: A Delphi process was conducted by 12 stakeholders (including 8 podiatry experts) from the University of Québec at Trois-Rivières which is the only university offering the degree of Doctor of Podiatric Medicine (DPM) in Canada. The developed framework is (1) based on the seven key roles of the Canadian medical education directives of specialists (CanMEDs) and, (2) closely aligned with the requirement of the College of Podiatrists of Québec which sets the standards of entry to practice in Québec.
Results: The developed framework represents the state of the development process and the consensus of the podiatry experts. It reflects the expected profile of the institution’s DPM graduates based on seven key roles (podiatry expert, communicator, collaborator, health advocate, leader and manager, scholar, and professional). This developed framework is an arborescence of complex skills defined in tangible indicators that characterize each expected part of a core competency. Twenty-four core competencies have been determined and divided into 84 enabling competencies and 288 observable indicators.
Conclusion: This competency framework has been designed to support high-quality education and to develop podiatry. Next steps include: (1) validation of this framework by external experts, (2) development of rigorous evaluation methods and, (3) concrete actions for its implementation and assessment. This framework would help to define the scope of practice and capabilities of podiatric medicine, both in Canada and internationally.
Keywords: podiatry, competency-based education, professional competence skills, clinical competence, attitude, Delphi technique
Introduction
Over the past two decades, competency-based medical education has emerged as an approach to educating health care professionals.1–3 Some benefits of this approach have been reported (eg, focus on achievements and outcomes, multidimensional assessment including formative and summative approaches and feedback, flexible trajectory supported throughout the curriculum, increased stakeholder accountability with a shared set of expectations).4–6 Provided and supported within the educational institution, the ultimate goal of a competency-based program has defined minimum threshold of competencies for the future health care professional to maximize quality and safe health care.7 Moreover, the competency development remains a continuous process and this grounded approach strengthens the ability of professionals to take control of their lifelong learning.3 Thus, several professions have adopted this approach, including podiatric medicine.8–12
Although a competency-based approach has emerged in podiatric medicine, this profession varies considerably across countries and, as a result, academic training differs.13–16 Podiatrists are generally defined as professionals with high-level skills in the prevention and management of local foot conditions that are not systemic diseases.17 Supporting country-specific podiatry education is essential to develop high-quality health professionals and their contextual practice. Currently in Canada, a four-year training program (total of 10 academic sessions) leading to the Doctorate in Podiatric Medicine degree (DPM) is offered at the Université du Québec à Trois-Rivières (UQTR) since 2004. This undergraduate DPM is the only degree program in the country and in French-speaking countries. This program was a priori modeled on American podiatric medicine programs to meet the standards of the Council of podiatric medical education but was never accredited by that organization. The first two years of the program are devoted to training in basic general medical knowledge. The last two years consist of podiatry-specific training (eg, dermatology, vascular, neurology, orthopedics, imaging, pharmacology, etc.) including clinical teaching through rotations of different specialties covered by podiatric medicine practice in various clinical settings.18,19 No surgical residency programs or fellowships are required to practice podiatry in Quebec compared to DPM in United States, but can be a concrete way to building capacity to extend the practice in-hospital.20 Once graduated from UQTR and registered to the Québec College of Podiatrists, podiatrists work mostly in private practice in the province.21,22 Defined by Québec’s legislator and operating under the Professional Code, the Podiatry act and numerous regulations including a Code of ethics, podiatrists in Québec treat and diagnose diseases of the foot and ankle witch are not systemic conditions.21–23 The podiatry practice is therefore closer to that of the United Kingdom and Australia, where the majority of practice is in the community.19 There is a desire to develop the profession within the public health system.24
After the creation of the UQTR podiatric medicine program in 2004 and its subsequent evaluation in 2014, evaluation’s stakeholders requested that a competency-based approach to education should be integrated. As a pioneer in teaching podiatry in Canada, the aim is to present the experience of developing this framework along with the work done to date to support next steps in the redesign process of the podiatric medicine program and its implementation.
Methods
Frameworks and Definition
The Canadian Medical Education Directives for Specialists (CanMEDS) Physician Competence framework has been determined to be the most appropriate for our purpose.25 There is no universally accepted framework for competency-based educational curriculum and this one is already used for other health profession in Canada.26 This comprehensive framework includes seven domains (medical expert, communicator, collaborator, health advocate, leader, scholar and professional), each characterized by several attributes. There are also variations across professions, including the role of the leader sometimes referring also to practice manager.9 Our choice was also supported by the Quebec Regulator’s requirement to align with the Québec College of Podiatrist’s entry-to-practice competencies. Our institution curriculum must match the required entry-to-practice competencies in order to maintain DPMs recognized by the College. Indeed, the Québec College of Podiatrists has also developed a framework based on an adaptation of the CanMEDS to define their entry-to-practice competencies that licensed podiatrists are expected to possess in adequacy with ethical obligations. The Québec College of Podiatrists obtained the rights to use the CanMEDS competency framework for educational purposes.27
A core competency is referred to as the academic, professional and cross-cutting competencies targeted in the training program. Competencies are defined as complex knowledge of how to act, based on the mobilization and effective combination of internal and external resources belonging to specific professional situations.28
Competency therefore refers to knowledges, attitudes and skills.55 The enactment of competencies in different healthcare setting is also the result of three factors: (1) competencies must have been developed in academic context, (2) the willingness of competencies deployment must be present and confers motivation for quality care and (3) the deployment of competencies must be supported by the context in which services are provided. Context empowers health professionals to provide competent practice and fully deploys all set of professional competencies.29 Taking into considerations how competencies are deployed, there was a need to define an educational framework (Boucher & Ste-Marie (2013)) in which different levels of competence development is expected along the curriculum which constitutes path competencies development and also refers to indicator as being expected level of competence.30–32
Research Design and Data Collection
This is a descriptive study of the chronology and stages of the competency-based approach in podiatric medicine being developed at UQTR. A real-time adapted Delphi technique as a part of the development process is presented (Figure 1) and is based on the guide on Conducting and REporting DElphi Studies (CREDES).33
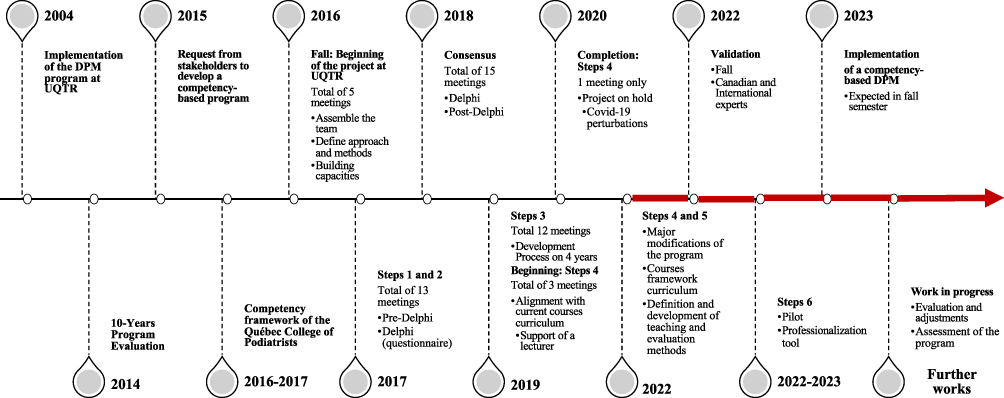 |
Figure 1 Framework development timeline including the Delphi Rounds. Red arrow: Ongoing work. Abbreviations: DPM, Doctorate in Podiatric Medicine; UQTR, University of Quebec at Trois-Rivieres. |
The adapted real-time Delphi technique was chosen given the small size of our group and the limited resource allocation. This technique allowed real-time discussion, iterations and consensus and facilitated the execution of specific tasks between meetings. The Delphi technique is considered as an effective way to measure and achieve consensus by structuring group communication that required anonymity and self-reflection.34,35 It is widely used in similar studies and has been successfully used to develop competency-based frameworks in other health profession.26
Group meetings (ie, steps 1 and 2 including pre-, the Delphi and post-Delphi meetings) were audio recorded. Main points of discussion were incorporated into working documents by some of the group members (CL, FG or OH). Updated documentation was shared with the entire group using Google Docs (Google, California, United States). Thus, only one round of questionnaires was conducted. There were seven questionnaires corresponding to each role. Developed in 2016 and in 2017 (pre-Delphi) (Figure 1), they used information gathered from frameworks, literature, and expert’s solicitations at UQTR.9,25 For each core competency developed (including indicators), the expert panel had to indicate their agreement on a Likert scale from 1 (strongly disagree) to 7 (strongly agree) relating to the logical relevance, the clarity, and their position stand related to other items. Panelists could add comments for further discussion. This was the only component of the process that was anonymous, but the whole process was conducted to allow time for self-reflection between group discussions. All scores below 5 were discussed by the group. There were several subsequent rounds of discussion related to each questionnaire (Step 2) and there were anonymous votes during meetings. Discrepancies were discussed in the group until a consensus was reached for each element (core competency, enabling competency and indicators) of the framework. At the end of these steps, the consensus threshold was set to 100% between experts as there is no standard.36,37 Discussion was moderated by the methodological experts for steps 1 and 2 (FG, CL and MB) and then, the program director (OH) for the steps 3. He (OH) also assumed leadership for the rest of the process (steps 4 to 6).
Setting and Participants
The UQTR is a regional French-speaking public university of 14,000 students supported by the provincial government of Québec (Canada). A cohort of 25 students in podiatry is admitted each year and teaching is supported by a team of six full-time and three part-time professors, several lecturers and internship/externship supervisors. A university clinic (CPUQTR) is operated on campus to support learning. In 2021, there were 286 practicing podiatrists in the province of Québec.38 The specific experts in podiatry were recruited within the institution. The only inclusion criterium was to be a professor at UQTR and all staff was included. An expert is defined as someone possessing the relevant knowledge and experience and considered as a peer with respected opinions by fellow workers in their field.36 Their characteristics are presented in the Table 1. The panel of competency framework development also included a methodological expert in education and particularly for the Delphi method (FG), in pedagogy (CL) and for professional competency framework development (MB). The program director, who is a health care professional and researcher (OH), also participated in the panel. Methodological experts and program director acted as leaders and advisors to stimulate progress, support development, documents’ preparation, and data collection. In addition, one lecturer has supported Step 4 and others are integrated into the current steps (Figure 1). The number of participants in the Delphi was justified by the objective to produce a framework mainly applicable to the institutional context, the development complexity and time investment requirement, the availability of financial resources and the limitation of French-speaking community.36
 |
Table 1 Baseline Characteristics of Podiatric Experts |
Development Process and Timeline
The development work is carried out in a sequence of macro- and micro-planning which is not yet completed as we are in the fourth stage. The literature outlines steps in designing a competency-based program as follows:5,10,39,40
- Identification of the competencies expected of graduates of the profession;
- Identification of the competencies and their components;
- Definition of the steps in the competency development process;
- Choice of methods, experiences and pedagogical tools;
- Designing of evaluation methods to measure progress of competency development; and
- Elaboration of the evaluation of program outcomes.
To this end, Figure 1 illustrates the development stages and timeline of the competency-based training program at UQTR and the on-going work.
Ethical Consideration
The willingness to participate was implicit when the experts agreed to join the process and, therefore, ethical approval was unnecessary since this voluntary activity was realized as part of their work at UQTR.
Results
Considering that it was not a priori intended to publish the Delphi method, we cannot provide in-depth details on the framework development discussion and questionnaires (eg, deletions, additions, and modifications). However, the following results summarize the final expert consensus. This crucial step to publish our framework and process in a common and accessible language (English) is supporting the team to move to the next stage of the process namely external expert validation before implementation (Figure 1). The roles (Figure 2) are developed and supported by seven definitions and the corresponding post Delphi results are documented in Tables 2–8.
 | 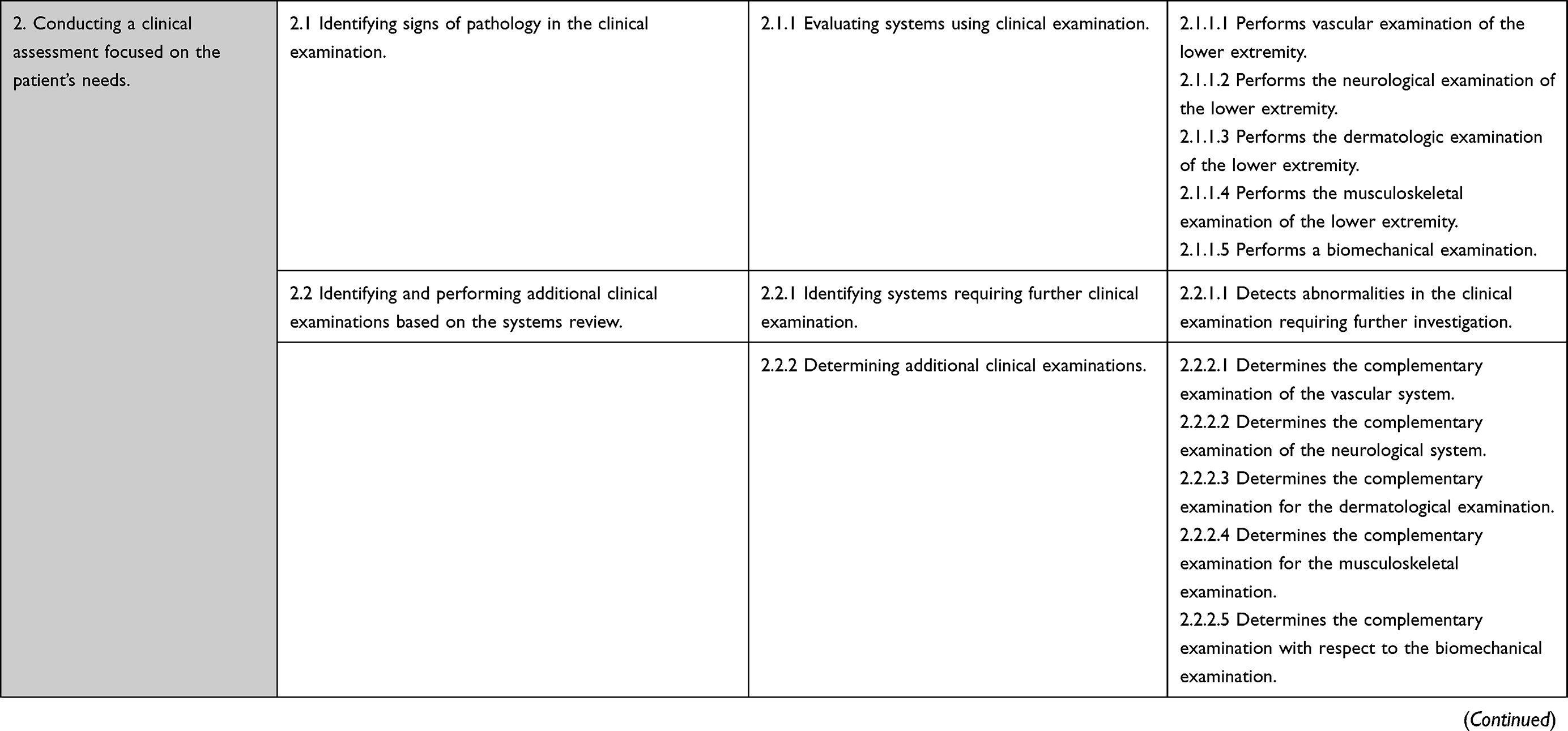 | 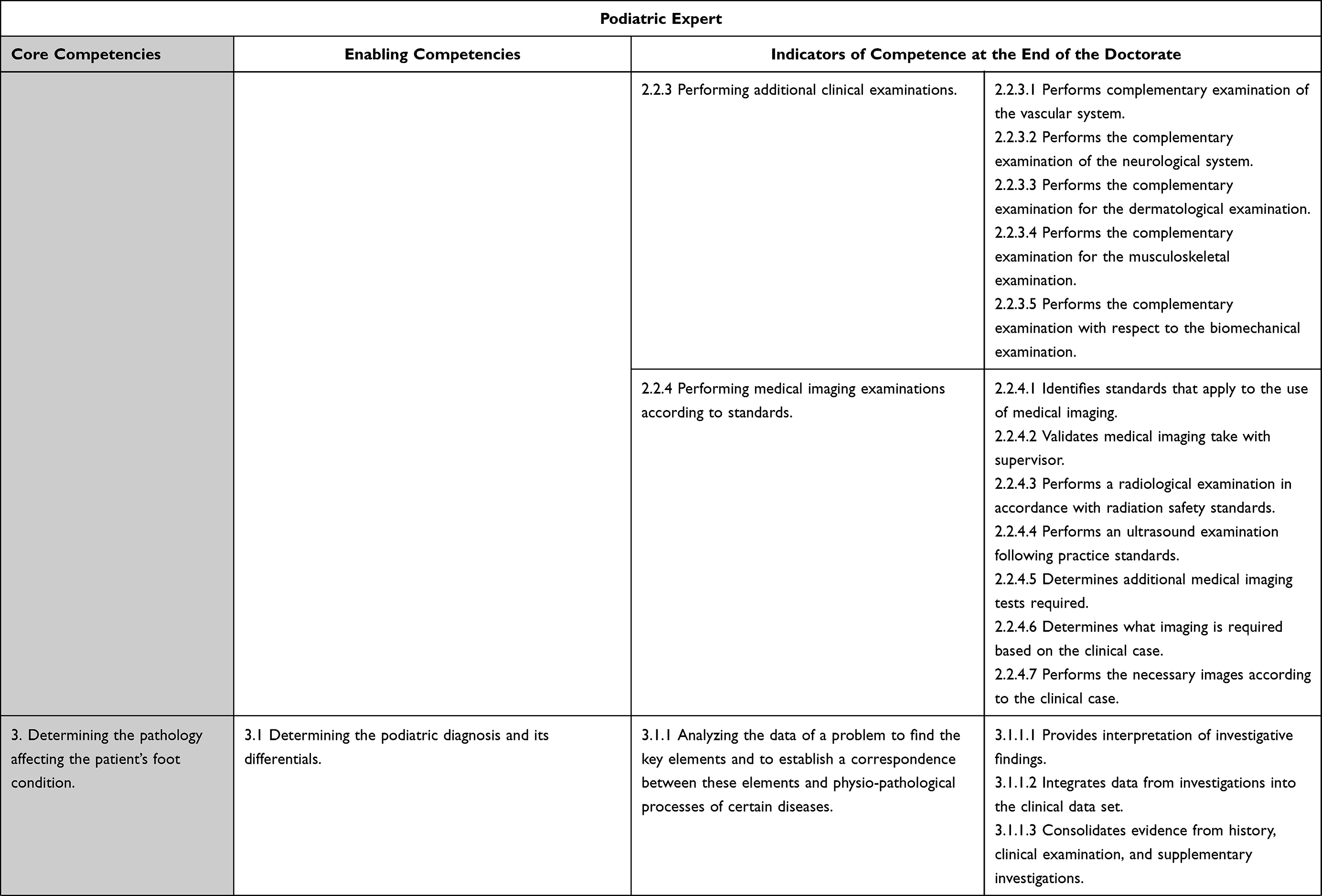 | 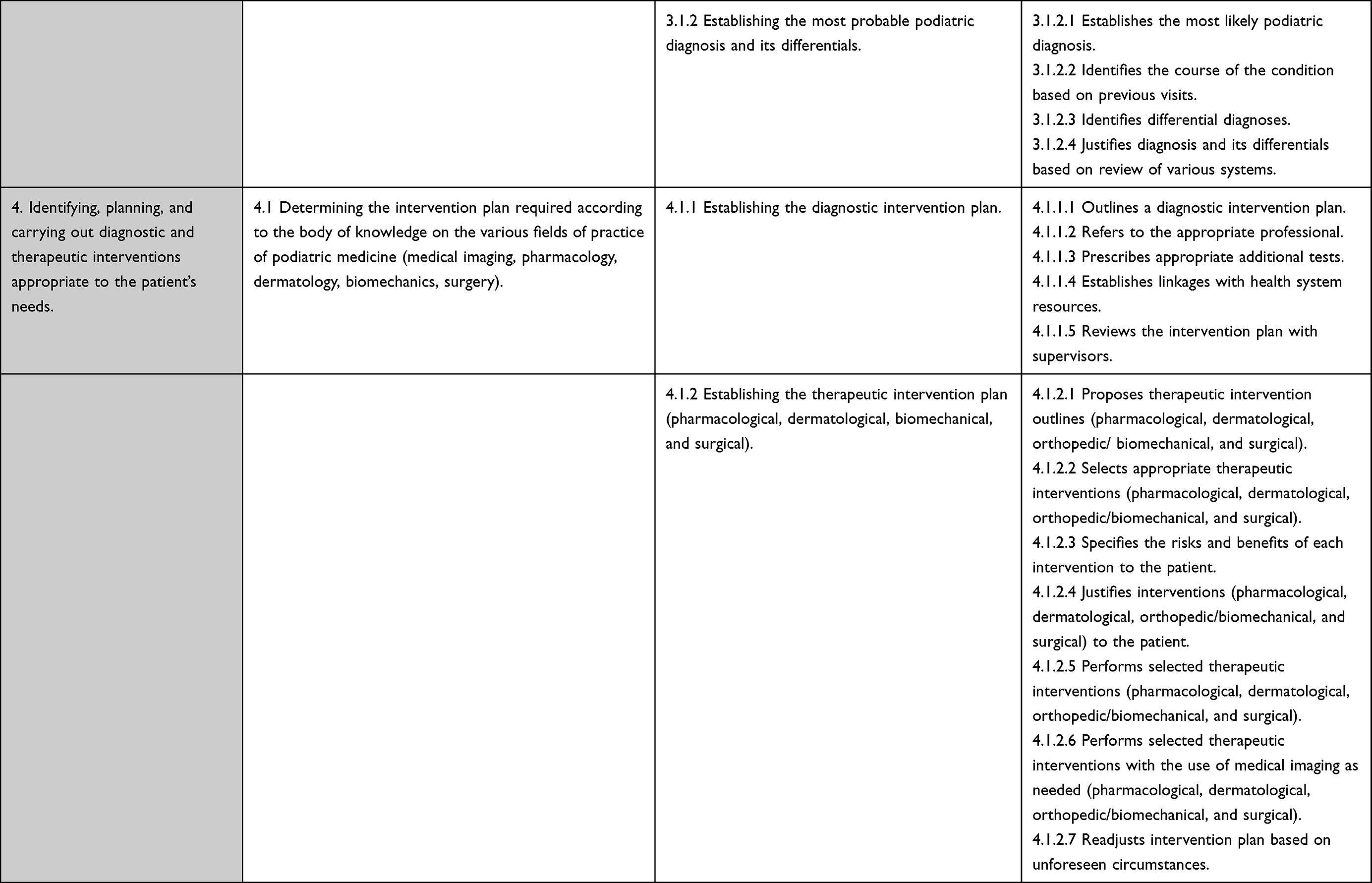 |
Table 2 Core and Enabling Competencies with Their Indicators for the Role of Podiatric Expert |
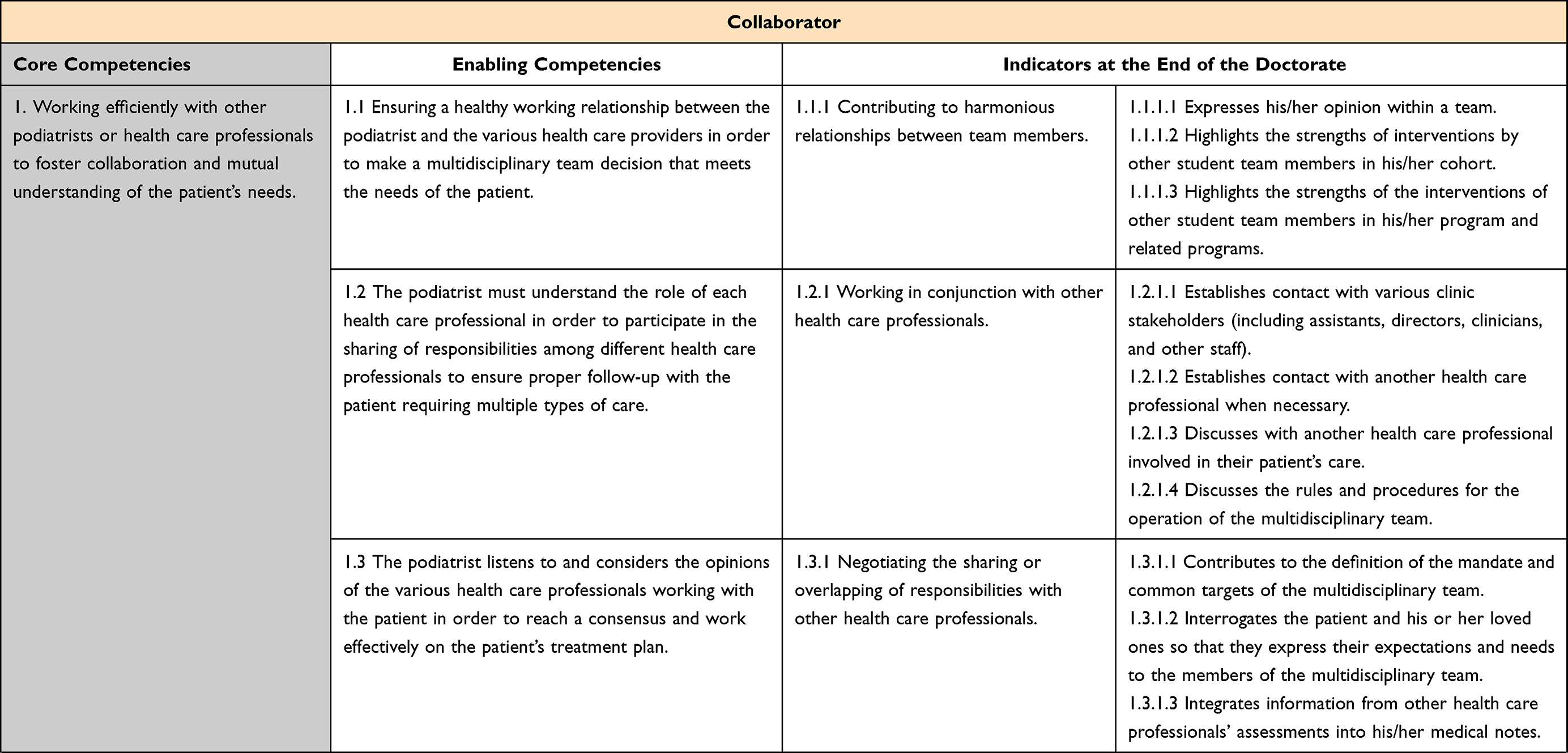 | 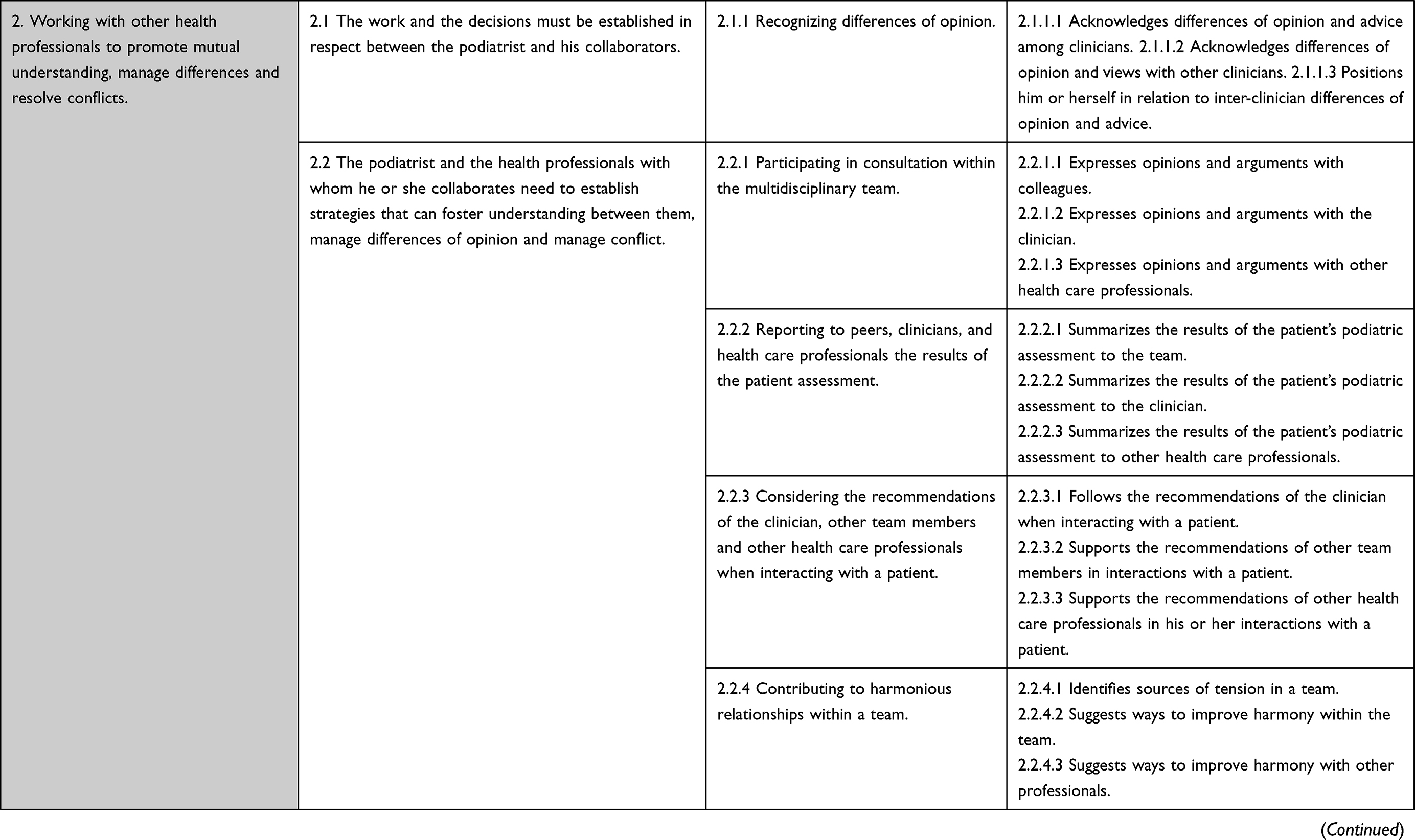 | 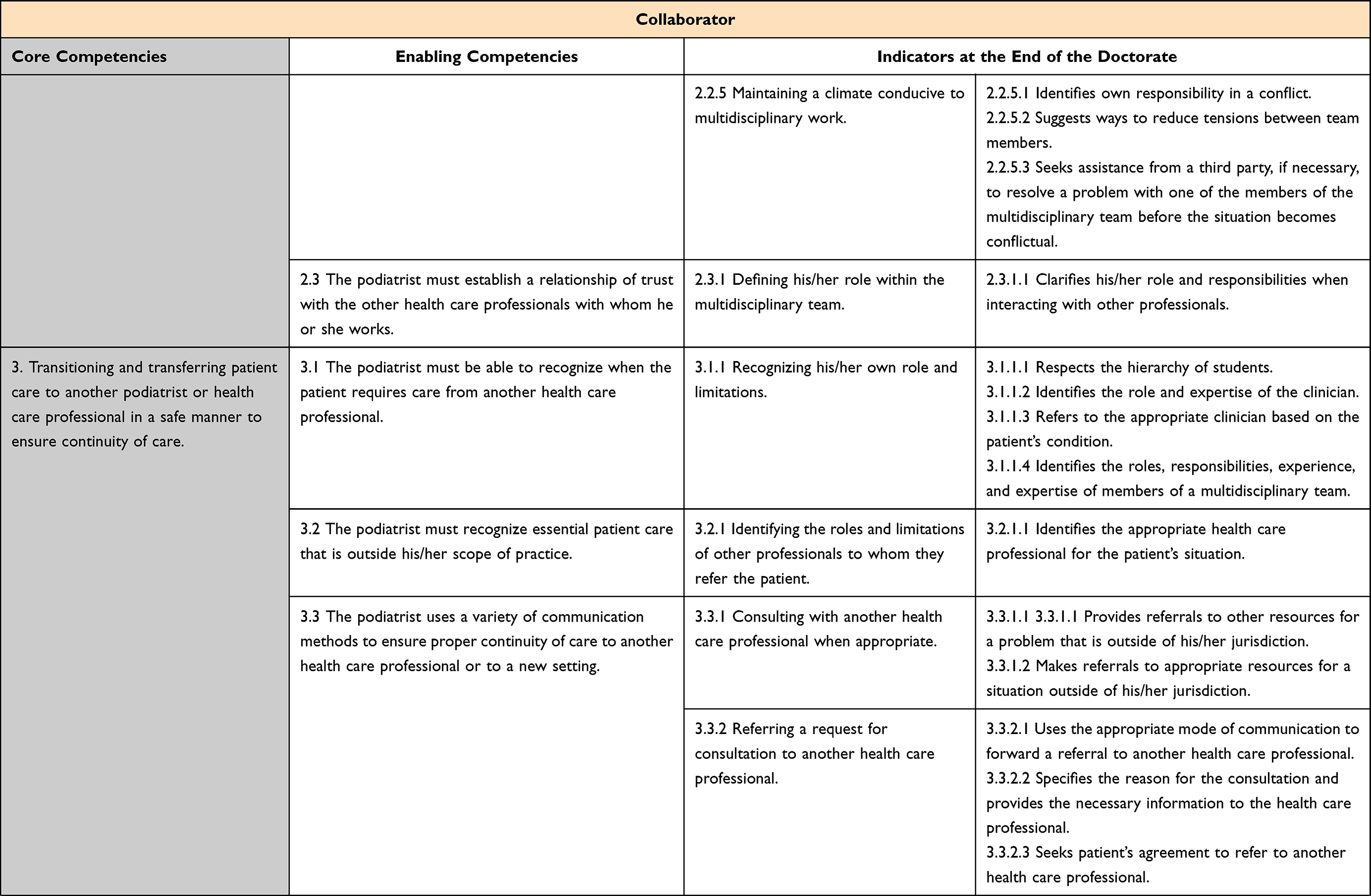 | 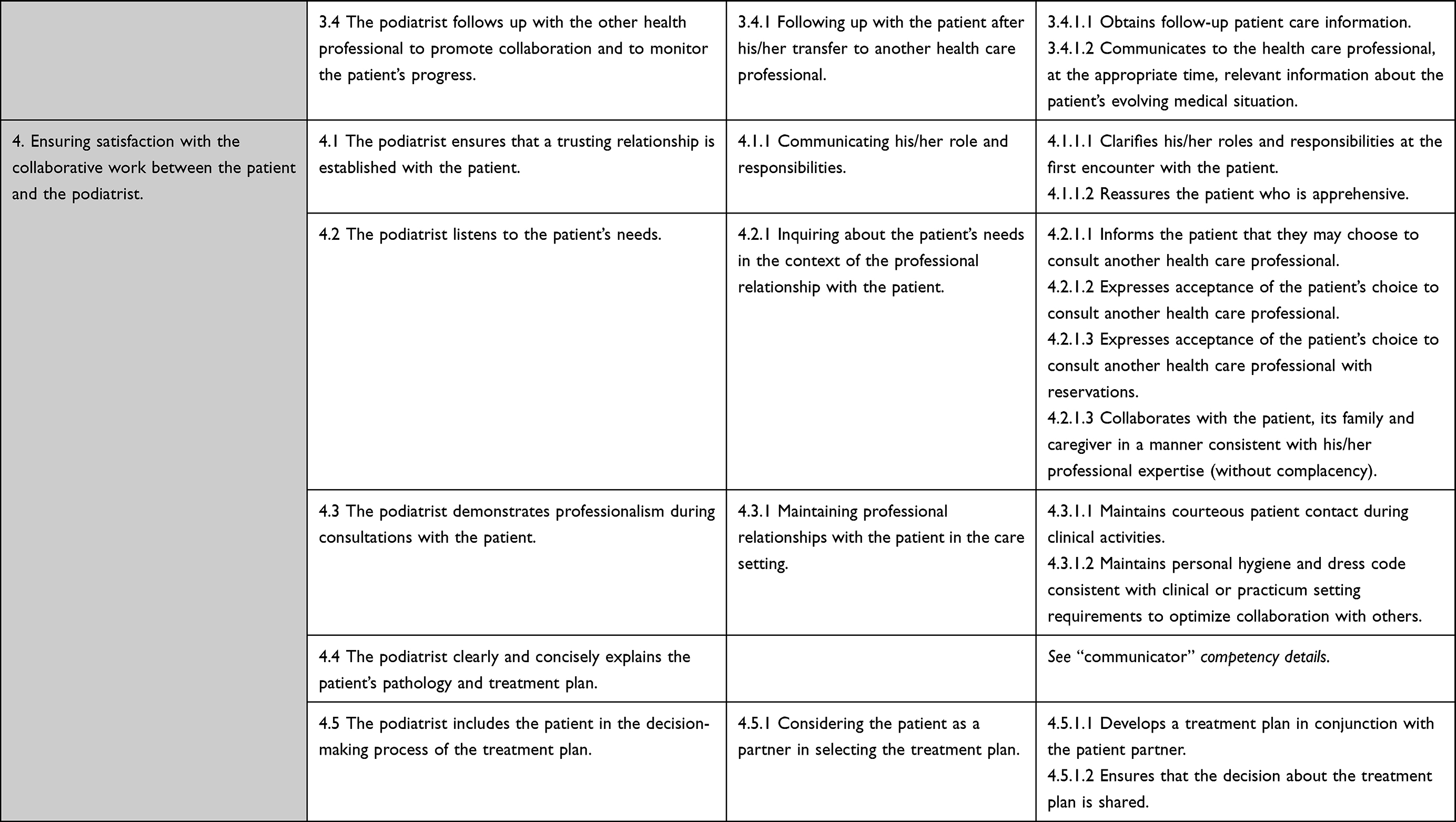 |
Table 3 Core and Enabling Competencies with Their Indicators for the Role of Collaborator |
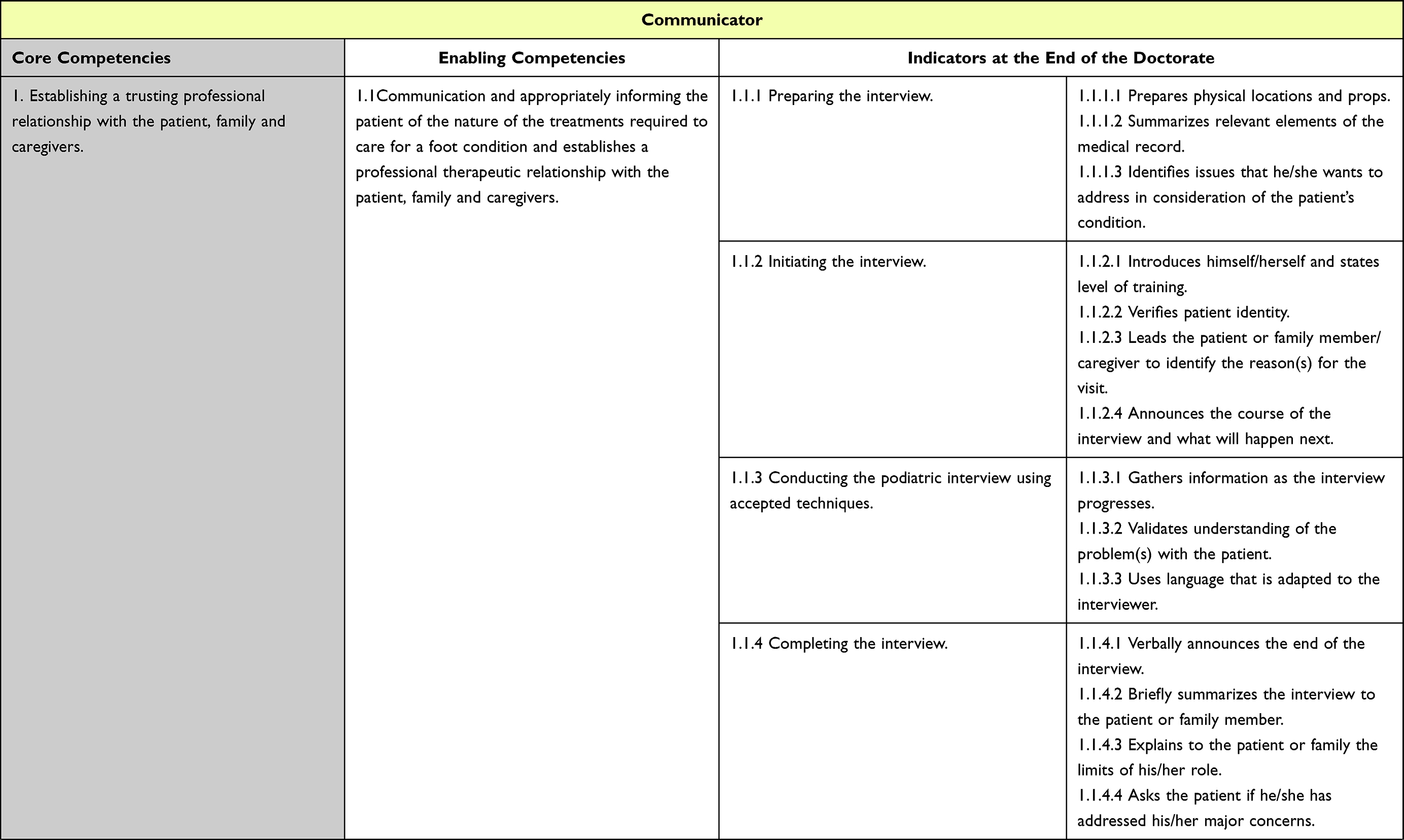 | 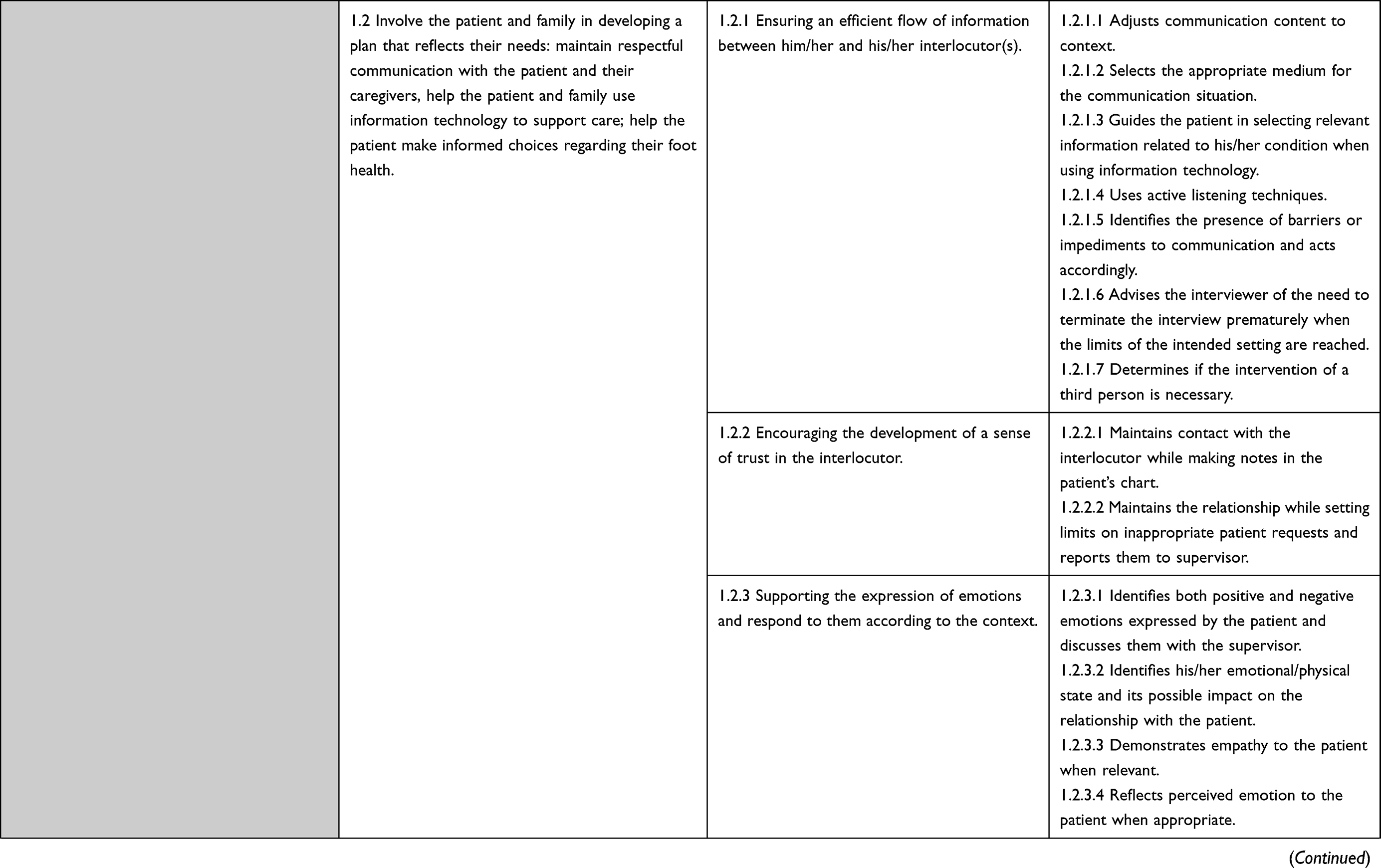 | 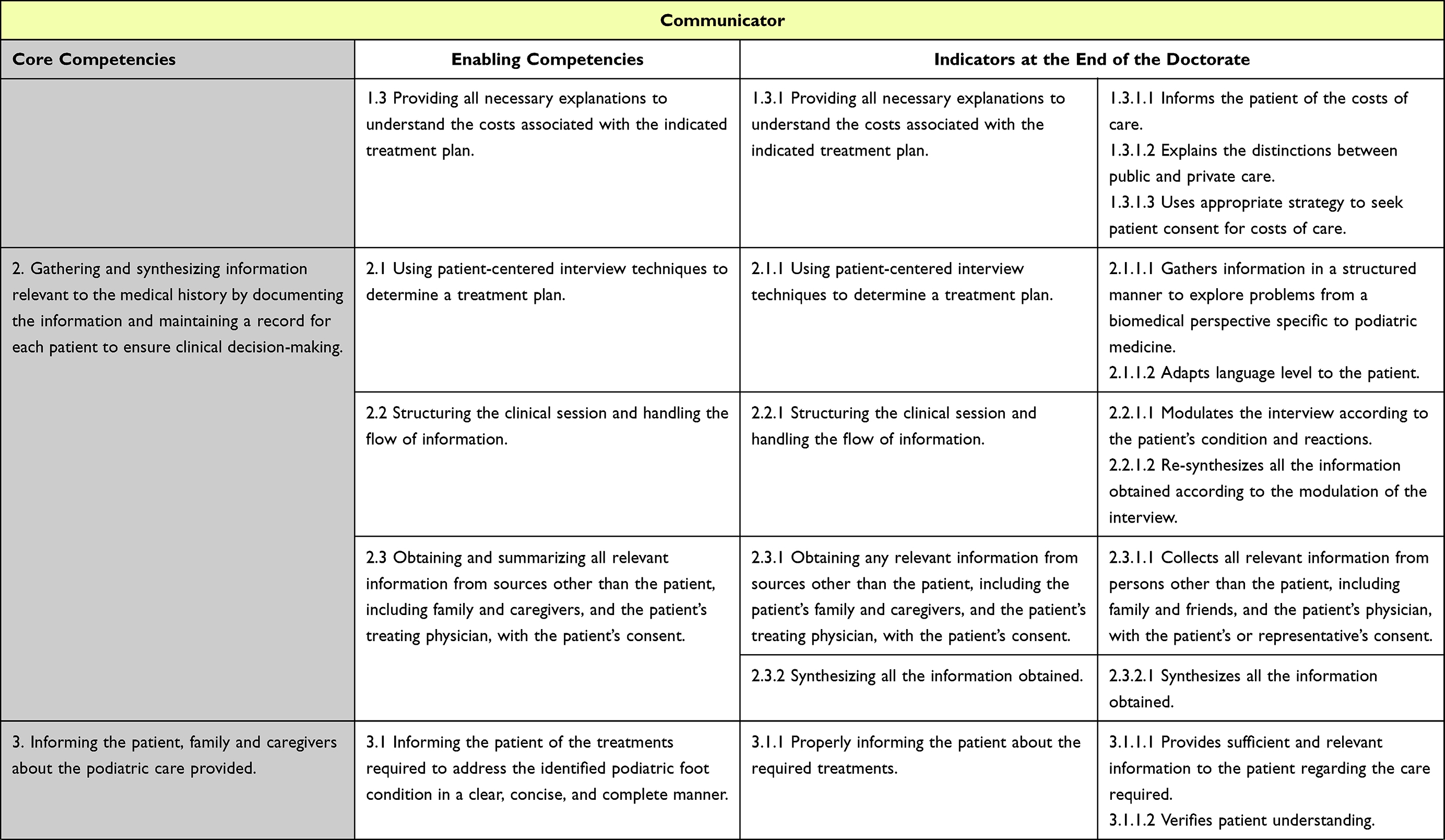 | 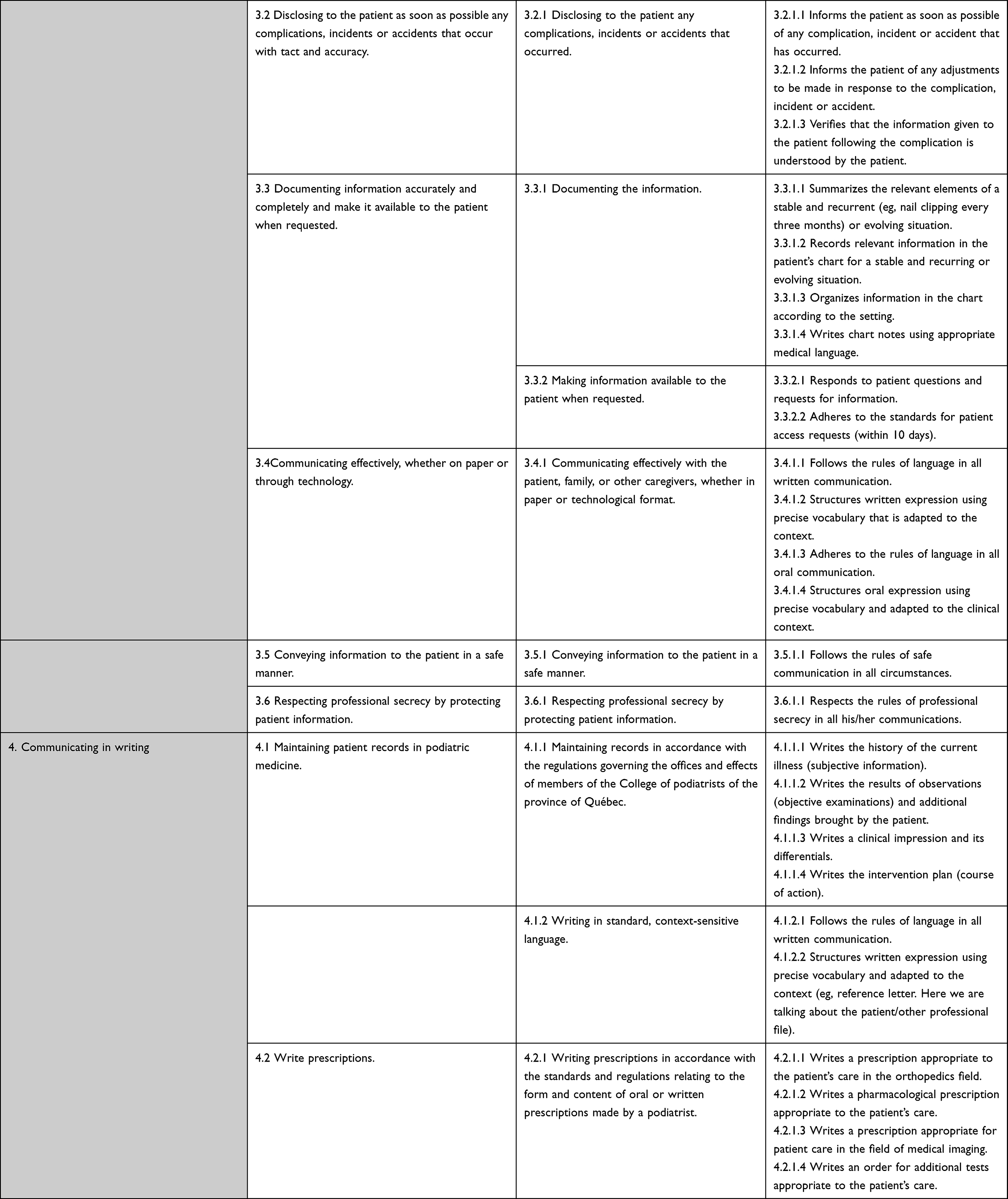 |
Table 4 Core and Enabling Competencies with Their Indicators for the Role of Communicator |
 |
Table 5 Core and Enabling Competencies with Their Indicators for the Role of Health Advocate |
 |
Table 6 Core and Enabling Competencies with Their Indicators for the Role of Leader and Manager |
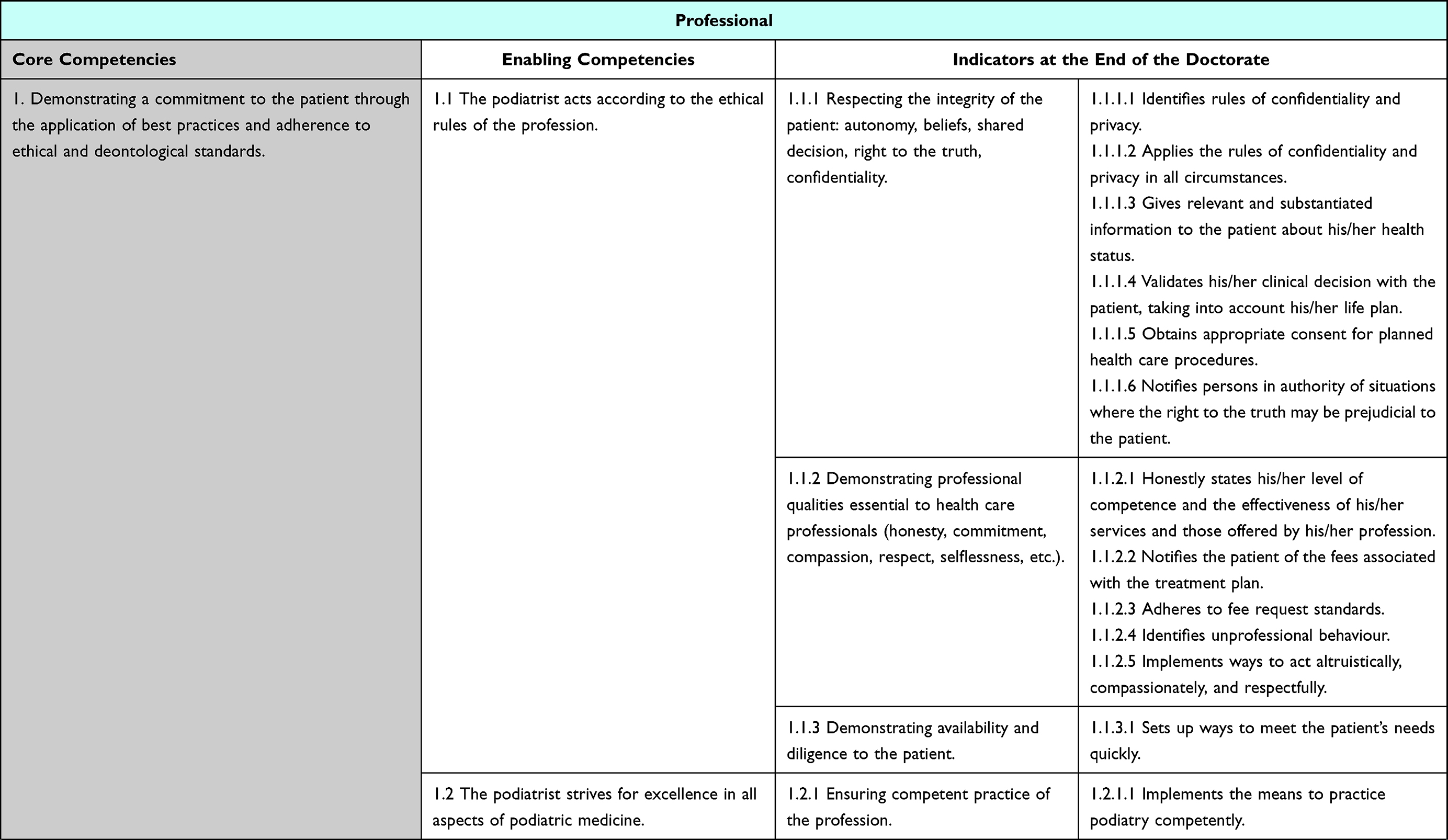 | 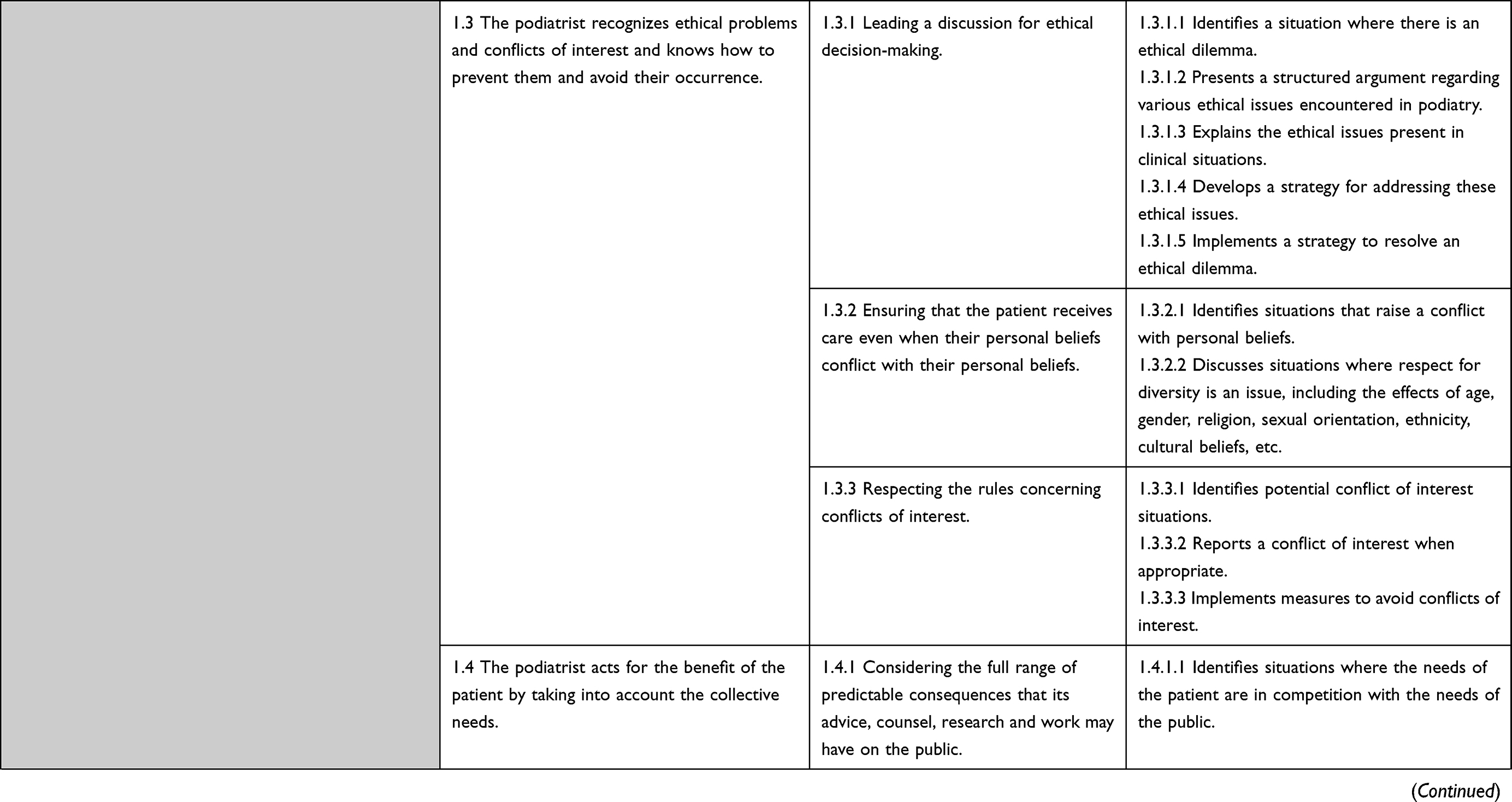 |  | 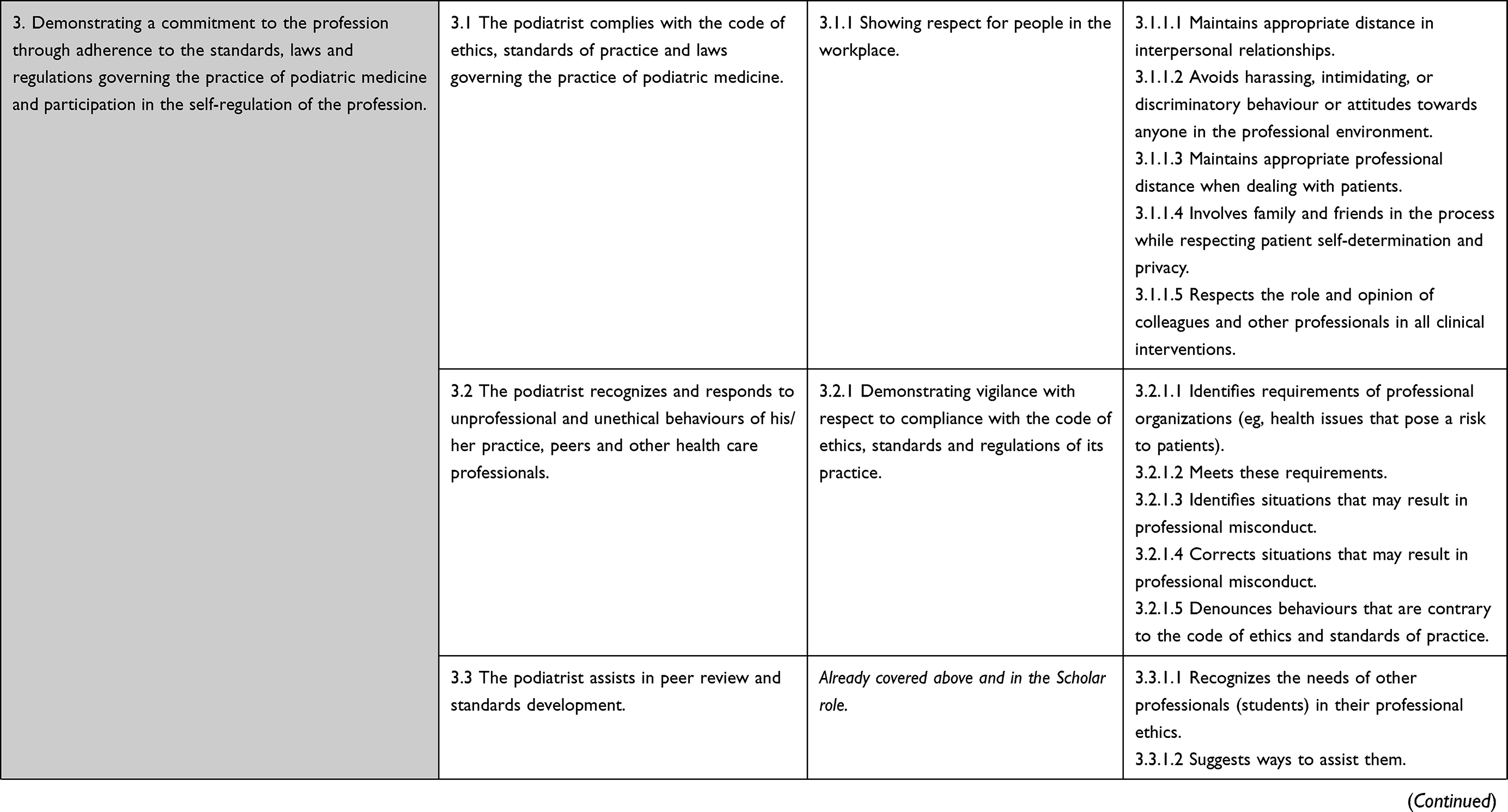 | 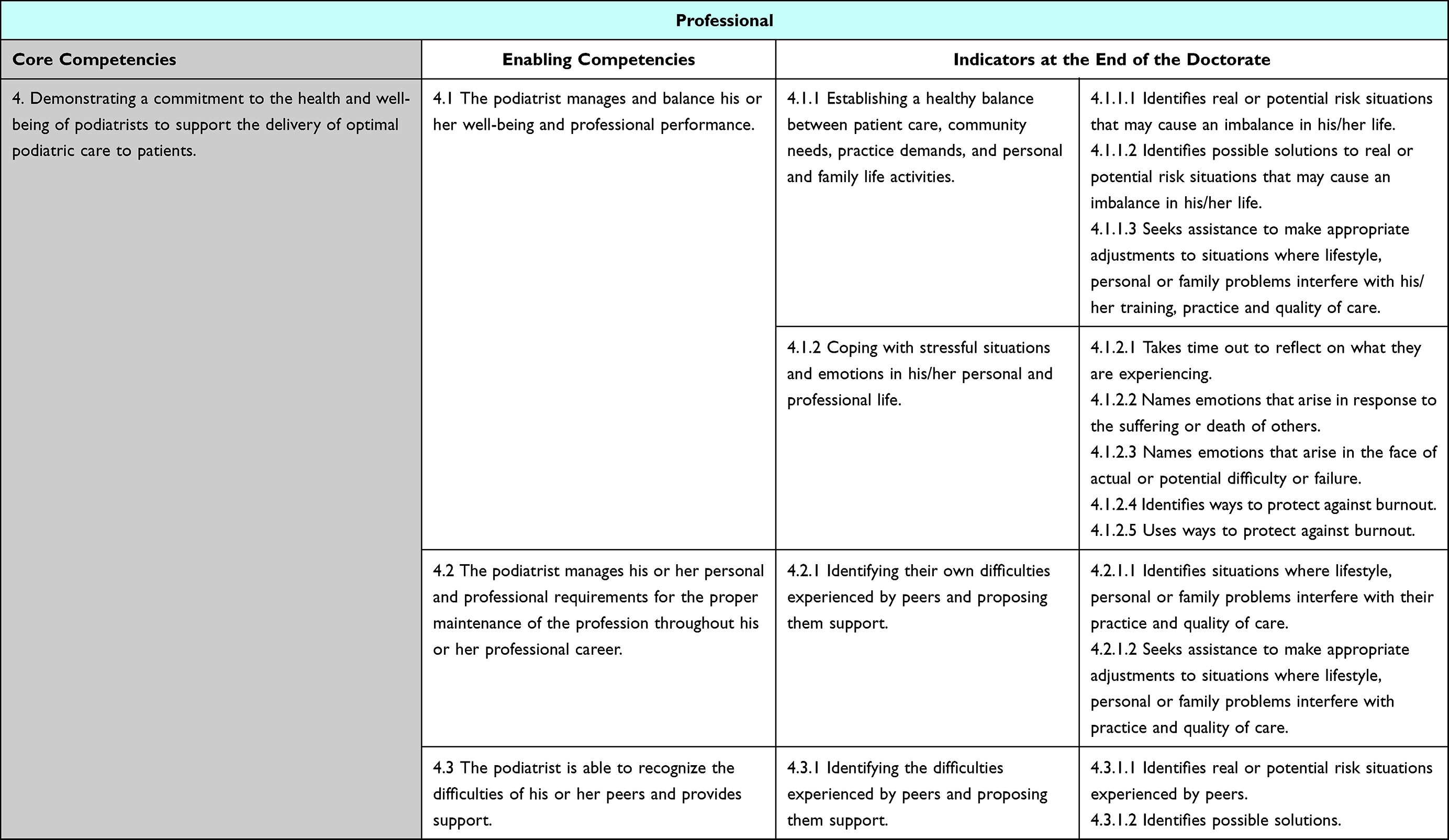 |
Table 7 Core and Enabling Competencies with Their Indicators for the Role of Professional |
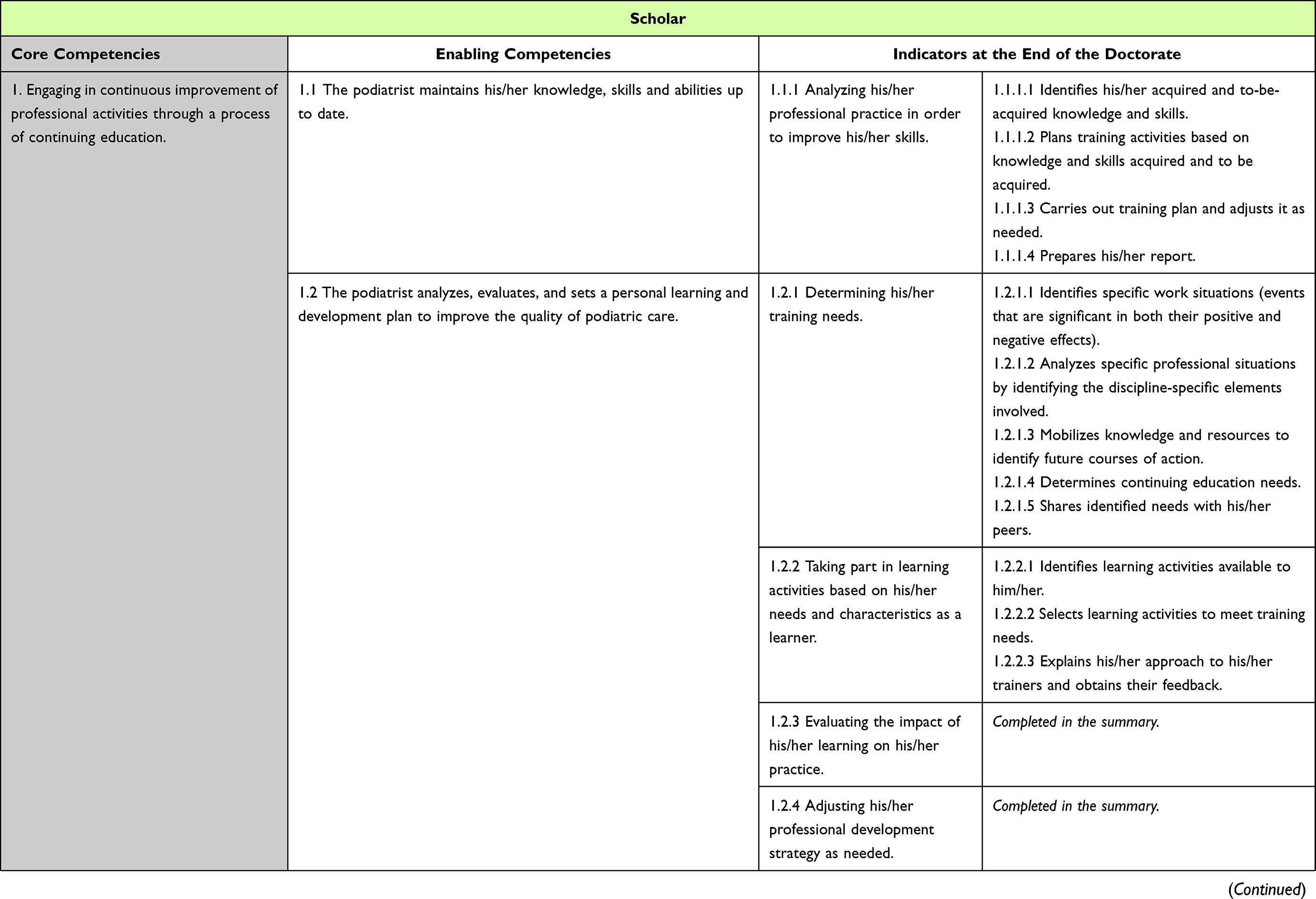 | 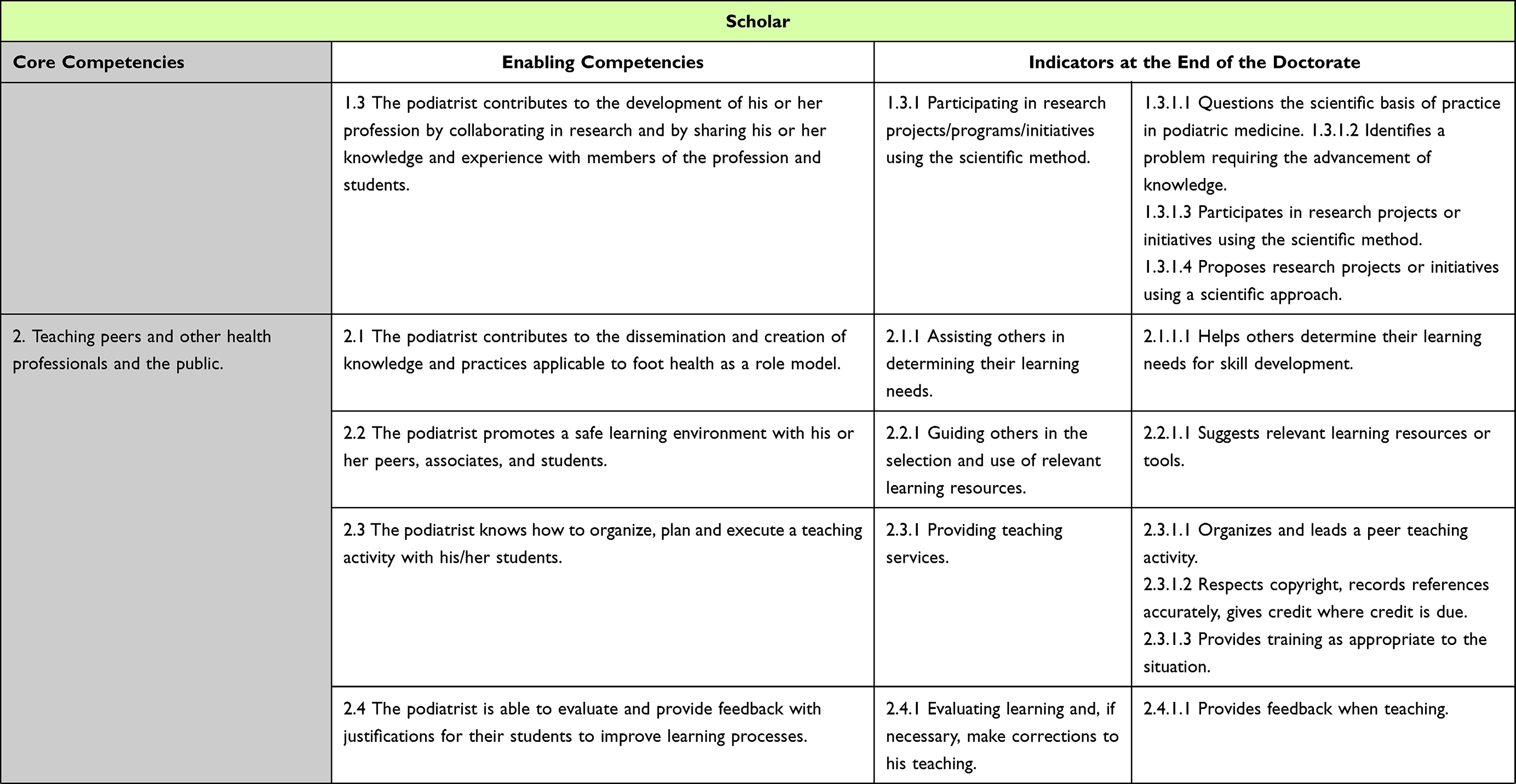 | 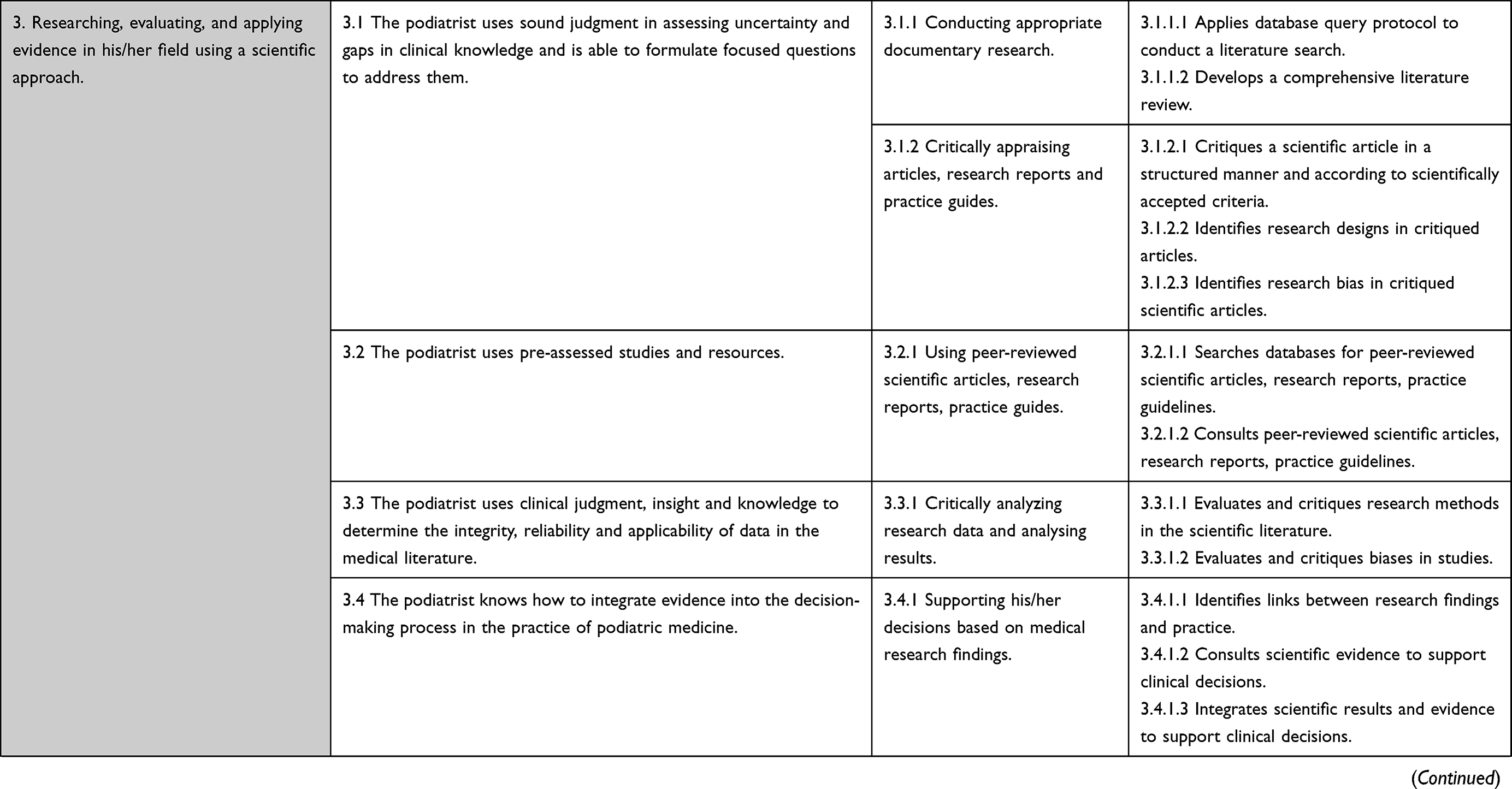 |  |
Table 8 Core and Enabling Competencies with Their Indicators for the Role of Scholar |
 |
Figure 2 Diagram representing the 7 roles of our podiatric medicine competency framework. |
Podiatric Expert
Podiatrist are empowered under the Podiatry Act to perform “any procedure” to treat local foot conditions that are not systemic diseases. As podiatric experts, they are aware of the limits of their knowledge and skills and determine the pathology affecting the health of the patient’s feet. They plan and apply the appropriate diagnostic and therapeutic examinations and provide the necessary treatments according to recognized and proven standards of practice in accordance with current data related to podiatric medicine. The environment in which podiatrists perform their professional services must be safe. The role of podiatric expert is essential to the podiatrist’s function and represents the central role overseeing the other six roles of the podiatric medicine competency framework namely the communicator, collaborator, leader, health advocate, scholar and professional (Table 2).
Collaborator
Podiatrists are primary health professionals. They must collaborate effectively with other health professionals in an effective way to provide appropriated quality care satisfying the patient’s needs. This may be accomplished by referring the patient to another health care professional or ensuring direct and continuous communication with another professional to ensure appropriate continuity of health care. Podiatrists must be aware of the limitation to their level of competence or the efficacy of their services. If the patient’s interest and needs require it, podiatrist must refer the patient to another health professional with the patient’s authorization. Collaborative decision-making among service providers require above all a full understanding of their individual roles, the optimization of patient care and the allocation of responsibilities. In addition to collaborating with their peers, podiatrists must also collaborate with their patient by including the patient’s perspective into the decision-making process of the treatment plan. Podiatrists must also respect a patient’s choice to consult another podiatrist or another health professional. Podiatrist must also respect the patient’s choice in having their care executed by another professional (Table 3).
Communicator
Podiatrists must seek to establish and maintain a professional relationship of mutual trust with their patients and their relatives since a disorder affects not only the patient, but also their relatives (eg, family, friends, caregivers). Podiatrists must be both professional and empathetical in their physical, mental, and emotional interaction with both patients and relatives. Podiatrists seek full knowledge of the state of health of their patient and their patient’s needs even if their field of activities is directed to treating local foot conditions. Podiatrists must communicate effectively and in a structured way, so that the patient understands the nature of problems identified, the risks and the benefits associated with each of the proposed treatments, and thus can give explicit and informed consent. The treatment plan must be explained in a way that considers the patient’s medical history, lifestyle, needs and socioeconomic situation. Podiatrists must inform their patient of the limit of their expertise, in cases where the patient must be referred to another medical specialty (Table 4).
Health Advocate
Podiatrists contribute to the development of the provision of foot care to the general public and in clinical situations. Podiatrists know how to communicate, educate and share their knowledge and expertise with patients, their family and their caregivers. Podiatrists promote their profession by informing and educating other health professionals to promote effective interprofessional collaboration and also ensure patient follow-up. Podiatrists promote education and information about podiatric medicine (Table 5).
Leader and Manager
Podiatrists ensure that the podiatric medical acts they perform comply with scientific and professional standards. Podiatrists ensure that their clinic or their place of practice is equipped in accordance with these standards and that the persons under their supervision know these standards and respect them at all times. They contribute to the evolution, development and practice of their profession by taking care to inform the other health professionals about their field of expertise. Podiatrists participate in making decisions in collaboration with other health professionals to contribute to the evolution of the provision of health care. Podiatrists also work to maintain a healthy work environment that is respectful to their personnel and their patients. Podiatrists take responsibility for time management, career management and professional practice management (Table 6).
Professional
As professionals, podiatrists have the duty to promote foot health, among both individuals and the collectivity. Podiatrists must subject their practice to the standards of their profession and the Code of ethics of podiatrists and respect the Podiatry Act. As health professionals, podiatrists must apply every effort to meet society’s expectations from the profession. They undertake to offer clinical competency, maintain that competency and practice in accordance with ethical standards. They also commit to demonstrate values such as integrity, honesty, altruism, respect for patients without judgment or discrimination, and to act transparently with respect to potential conflicts of interest (Table 7).
Scholar
As scholars, podiatrists demonstrate constant commitment to the excellence of podiatric medicine so that they can provide quality care. They pursue this excellence through continuing education, research and teaching, all in accordance with a rigorous scientific approach. Podiatrists aim to improve their knowledge and competencies through available training. They share knowledge, compare methods and the results obtained with peers, and seek feedback to maintain quality of care and preserve patient safety. They collaborate in research and share knowledge, expertise and experience with the members of their profession and students. Podiatrists show their mastery of the practice of their profession by using an approved scientific approach, based on evidence. They evaluate and apply evidence as part of their practice (evidence-based practice). They can recognize the limits, uncertainties and gaps in their profession and formulate research questions that seek to improve it (Table 8).
Discussion
This project outlines the process of competency-based education development which is used primarily to profile UQTR’s graduates in podiatric medicine. The framework developed is an arborescence of enabled competencies, defined by tangible indicators that characterize each expected part of a core competency. Thus, the competency framework includes a total of 24 core competencies divided into seven roles (ie, podiatry expert, communicator, collaborator, health advocate, leader and manager, scholar, and professional), 84 enabling competencies, and 288 expected indicators. The indicators are a valuable tool for the next steps, as they will be used to plan courses and assessment items. We have gone beyond the list of competencies and enabling competencies; each element in our work is specified by observable indicators, which provide guideposts for the podiatry program. Our work is in accordance with the Québec College of Podiatrists’ competency framework where professional knowledge and expertise and ethical integrity are mandatory. Thus, this may support the podiatrist-in-training to the podiatrist-in-practice transition as well as their continuing education program as seen in other profession.41 To our knowledge, this is the first publication of such process in podiatric medicine curriculum, although there are specific competency approaches for certain areas of practice.12,42,43
This work was conducted to support the next steps in the development timeline, ie, validation of the framework with external experts in podiatric medicine before the implementation of competency-based education at UQTR. Acceptability and validation are essential steps of the process as it was published in other educational professional frameworks.8,44–46 In addition, we are sharing our experience, albeit with some missing details and still as a work-in-progress, with the community to inspire other health programs interested in adopting a competency-based approach to their emerging profession. The results demonstrate the complexity of the competency required to become a podiatrist, supporting similar role, and core competency to the original CanMEDS.25 Our work supports the definition of the roles of the Québec College of Podiatrists considering that there is very little variation between those defined by the UQTR experts and those of the College.27 Clearly defining competencies and role definition is an important step in professionalization for healthcare professional education and research.47 Competency-based education relies on active, situation-based group learning strategies to prepare future health professionals to be connected to patient and population needs, and this project is going in that direction.47 Although this causal effect cannot be supported by the present results, the framework is a significant progress in assisting health care delivery to patients and their relatives to become safer, more efficient, and more effective.7
Limitations
The publication of this data can overcome the limitation of our progress given the development of the primary framework in French, and that podiatrists are essentially a profession present in the English-speaking countries.48 The lack of specific details related to the discussions may be a limitation of this study and the memory bias in the reporting data related to the process. However, it was not originally intended to be disseminated, but the team feels that this knowledge translation adds value to this area of interest and to the podiatry community at large. In addition, specific information about the iterations during the process does not influence the final reported results and further work.
It would have been appropriate to have more expert podiatrists recruited for the Delphi in order to reach at least 15 participants which would help obtain perspective saturation.36 However, we were limited by the number of professors in podiatry at UQTR. This was a huge commitment for the volunteer work of a podiatrist in private practice which justify the choice to stay within the institution. The group was homogeneous with respect to expertise and could rely on the support of a methodological team that increased the number of participants to 12 during the discussions. Expert participation and commitment were not always constant due to work overload which led to variability in the process over a long period of time (eg, assiduous presence at the meetings and return of documentation). The method has some flaws. As this is an adapted method, Delphi standards could have been followed more closely, especially to increase the anonymity in the discussion and self-reflection. Indeed, real-time Delphi does not always give equal weight to each expert’s opinion, anonymity of the experts is not always present and can lead to the domination of the consensus process by one or a few experts.49 Covid-19 has also slowed down the pace of work considering the difficulties encountered in clinical settings and the additional workload associated with the pandemic. Finally, there are still a lack of validation of the CanMEDS construct to demonstrate that it is the best framework for competency-based approach in education, which limits the validity of our results.50 However, many studies in health care support the use of the CanMEDS framework to structure competencies.51–53
Implications
The consensus within the expert group and their integration to the whole process may contribute to uniform education of podiatric medicine at our institution as well as the implementation of the framework elsewhere. Hence, this may be beneficial to engage lecturers in further development and their integration in academic projects. Moreover, research produce more relevant knowledge when different stakeholders are involved, especially users. This was clearly demonstrated in patient-oriented research.54 Therefore, we have integrated a podiatry student in this project (YA), and it changed our perspective when involving them in the process for the steps 5 and 6 (Figure 1). A harmonization in the podiatry education can have a pivotal role in the recognition of this profession. This framework can support the development of Canadian education in this area and lead to new curriculum development. This may also help define the scope of practice of podiatry in Canada, as student training will be based on a comprehensive curriculum that can be more easily understood by other health professions. Podiatrists are involved in many areas of health care (eg, dermatology, neurology, vascular, orthopedic, imagery, pediatric and geriatric population, traumatology, etc.) and collaboration is mandatory to achieve the best patient outcomes, since feet are part of a whole human being with complex needs. Highly trained professionals are needed to ensure safe and quality patient care.
Conclusion
The competency framework developed at UQTR is intended to support high-quality education and the development of the profession of podiatry. It helps define the scope of practice and capabilities of podiatric medicine, both in Canada and internationally. Next steps include validation of this framework with a panel of external experts, development of rigorous evaluation methods, and concrete actions for its implementation and assessment.
Acknowledgments
Thanks to experts for their participation in this work, which is essential to our institution (ie, François Allart, Magali Brousseau-Foley, William Lee, Benoît Gagné, Sébastien Hains, Zyad Hobeychi, and Marie-Christine Torchon). It is also important to thank Martine Gosselin, Chief Executive Officer and Registrar of the Québec College of Podiatrists, for her support throughout the process and this publication. Thanks to the lecturer Marc-Antoine Dion, and to all those who, in one way or another, participated in this project and its current progress. The authors appreciate the English editing of Joel Alleyne, the Executive Director of Canadian Podiatric Medicine Association.
Disclosure
All authors are affiliated to the Université du Québec à Trois-Rivières. The authors report no conflicts of interest in this work. VB, podiatrist was part of the panel of experts within the Delphi. This project was financially supported by Université du Québec à Trois-Rivières.
References
1. Long DM. Competency-based residency training: the next advance in graduate medical education. Acad Med. 2000;75(12):1178–1183. doi:10.1097/00001888-200012000-00009
2. Carraccio C, Wolfsthal SD, Englander R, Ferentz K, Martin C. Shifting paradigms: from Flexner to competencies. Acad Med. 2002;77(5):361–367. doi:10.1097/00001888-200205000-00003
3. Harris P, Snell L, Talbot M, Harden RM. Competency-based medical education: implications for undergraduate programs. Med Teach. 2010;32(8):646–650. doi:10.3109/0142159X.2010.500703
4. Hawkins RE, Welcher CM, Holmboe ES, et al. Implementation of competency‐based medical education: are we addressing the concerns and challenges? Med Edu. 2015;49(11):1086–1102. doi:10.1111/medu.12831
5. Frank JR, Snell LS, Cate OT, et al. Competency-based medical education: theory to practice. Med Teach. 2010;32(8):638–645. doi:10.3109/0142159X.2010.501190
6. Brydges R, Boyd VA, Tavares W, et al. Assumptions about competency-based medical education and the state of the underlying evidence: a critical narrative review. Acad Med. 2021;96(2):296–306. doi:10.1097/ACM.0000000000003781
7. Iobst WF, Sherbino J, Cate OT, et al. Competency-based medical education in postgraduate medical education. Med Teach. 2010;32(8):651–656. doi:10.3109/0142159X.2010.500709
8. Bok HG, Jaarsma DA, Teunissen PW, van der Vleuten CP, van Beukelen P. Development and validation of a competency framework for veterinarians. J Vet Med Educ. 2011;38(3):262–269. doi:10.3138/jvme.38.3.262
9. Verma S, Paterson M, Medves J. Core competencies for health care professionals: what medicine, nursing, occupational therapy, and physiotherapy share. J Allied Health. 2006;35(2):109–115.
10. Frank JR, Mungroo R, Ahmad Y, Wang M, De Rossi S, Horsley T. Toward a definition of competency-based education in medicine: a systematic review of published definitions. Med Teach. 2010;32(8):631–637. doi:10.3109/0142159X.2010.500898
11. John MS, Tong B, Li E, Wilbur K. Competency-based education frameworks across Canadian health professions and implications for multisource feedback. J Allied Health. 2020;49(1):1E–11E.
12. Levrio J. Podiatric medicine: a current assessment. J Am Podiatr Med Assoc. 2009;99(1):65–72. doi:10.7547/0980065
13. Wylie D, Butters V. An impact assessment of the podiatry competency framework for integrated diabetic foot care, 2012–2019. Diabetic Foot J. 2019;22(4):34–41.
14. American Association of college of Podiatric Medicine. Curricular guide for podaitric medical education. AACPM Council of Faculties; 2020: 319. Available from: https://aacpm.org/wp-content/uploads/2020-AACPM-Curricular-Guide-2.pdf.
15. Council AaNZPA. Podiatry competency standards for Australia and New Zealand; 2015. Available from: https://www.acps.edu.au/resource_redirect/downloads/sites/98874/themes/1958854/downloads/9XdYA3TjTpeUks3KHmUb_Competency_Standards_Jan_2010.pdf.
16. Reay J, Williams C, Nester C, Morrison SC. A step in the right direction: delphi consensus on a UK and Australian paediatric podiatry curriculum. BMC Med Educ. 2022;22(1):1–11. doi:10.1186/s12909-022-03138-8
17. Blouin C, Genet F, Perrier A. De la chiropodie à la podiatrie: progression des formations à l’international [From chiropody to podiatry: progression of international training]. Rev du Podol. 2021;17(100):15–18. doi:10.1016/j.revpod.2021.05.005
18. Kim PJ, Attinger CE, Evans KK, Steinberg JS. Role of the podiatrist in diabetic limb salvage. J Vasc Surg. 2012;56(4):1168–1172. doi:10.1016/j.jvs.2012.06.091
19. Farndon LJ. The function and purpose of core podiatry: an in-depth analysis of practice. Sheffield Hallam University; 2006.
20. Borthwick AM. Challenging medicine: the case of podiatric surgery. Work Employ Soc. 2000;14(2):369–383. doi:10.1177/09500170022118455
21. Ordre des podiatres du Québec. Qu’est-ce qu’un podiatre? [Québec College of Podiatrists. What is a podiatrist?] Available from: http://ordredespodiatres.qc.ca/public/quest-ce-quun-podiatre/.
22. UQTR. Doctorat de premier cycle en médecine podiatrique (7017) [UQTR. Doctorate in Podiatric Medicine]. Université du Québec à Trois-Rivières. Available from: https://oraprdnt.uqtr.uquebec.ca/pls/apex/f?p=PGMA000:10:::NO:RP,10:P10_CD_PGM:7017.
23. Québec Gd. Code des professions du Québec [Québec Government. Québec Professional Code]. Available from: https://www.legisquebec.gouv.qc.ca/fr/document/lc/C-26.
24. Blanchette V, Hains S, Cloutier L. Establishing a multidisciplinary partnership integrating podiatric care into the Quebec public health-care system to improve diabetic foot outcomes: a retrospective cohort. Foot. 2019;38:54–60. doi:10.1016/j.foot.2018.10.001
25. Frank JR, Danoff D. The CanMEDS initiative: implementing an outcomes-based framework of physician competencies. Med Teach. 2007;29(7):642–647. doi:10.1080/01421590701746983
26. Batt AM, Tavares W, Williams B. The development of competency frameworks in healthcare professions: a scoping review. Adv Health Sci Educ. 2020;25(4):913–987. doi:10.1007/s10459-019-09946-w
27. Québec Odpd. Podiatrist 2017 Competency Framework; April, 2022. Available from: https://www.ordredespodiatres.qc.ca/wp-content/uploads/2014/04/R%c3%a9f%c3%a9rentiel-de-comp%c3%a9tences-en-m%c3%a9decine-podiatrique-2017.pdf.
28. Tardif J. L’évaluation des compétences: documenter le parcours de développement [Competency assessment: documenting the developmental journey; Cheneliere Education]; 2006.
29. Le Boterf G. Repenser la compétence [Rethinking competence. Editions Eyrolles]. Pour Dépasser les Idées Reçues. 2008;15:978–2212547276.
30. Boucher A, Ste-Marie L-G. Pour un cursus d’études médicales axé sur les compétences: Cadre de formation [Toward a Competency-Based Medical Education Curriculum: An Educational Framework]. Les Presses du CPASS; 2013.
31. Poumay M, Georges F. Comment mettre en œuvre une approche par compétences dans le supérieur? [How to implement a competency-based approach in higher education?] De Boeck Supérieur; 2022.
32. Guillemette F. L’approche par compétences dans la programmation pédagogique [The competency-based approach in educational programming]. Enjeux et société. 2021;8(2):140–169. doi:10.7202/1078492ar
33. Jünger S, Payne SA, Brine J, Radbruch L, Brearley SG. Guidance on Conducting and REporting DElphi Studies (CREDES) in palliative care: recommendations based on a methodological systematic review. Palliat Med. 2017;31(8):684–706. doi:10.1177/0269216317690685
34. Jones J, Hunter D. Consensus methods for medical and health services research. BMJ. 1995;311(7001):376. doi:10.1136/bmj.311.7001.376
35. Harder A, Place NT, Scheer SD. Towards a competency-based extension education curriculum: a Delphi study. J Agric Educ. 2010;51(3):44. doi:10.5032/jae.2010.03044
36. De Villiers MR, De Villiers PJ, Kent AP. The Delphi technique in health sciences education research. Med Teach. 2005;27(7):639–643. doi:10.1080/13611260500069947
37. Keeney S, Hasson F, McKenna H. Consulting the oracle: ten lessons from using the Delphi technique in nursing research. J Adv Nurs. 2006;53(2):205–212. doi:10.1111/j.1365-2648.2006.03716.x
38. Québec College of Podiatrists. Annual Reports; 2020–2021. Available from: https://www.ordredespodiatres.qc.ca/ordre/liens-utiles-et-publications/. Accessed
39. Goudreau J, Pepin J, Dubois S, Boyer L, Larue C, Legault A. A second generation of the competency-based approach to nursing education. Int J Nurs Educ Scholarsh. 2009;6(1):1. doi:10.2202/1548-923X.1685
40. Brousseau M, Therriault P-Y, Sauvageau A, Aubin G. Enseignement des sciences de l’occupation: soutenir le déploiement des compétences et organiser les situations cliniques dans une approche occupationnelle [Occupational science education: supporting the deployment of skills andorganizing clinical situations in an occupational approach]. Revue Francophone de Recherche en Ergothérapie. 2018;4(2):43–61.
41. Westein MP, de Vries H, Floor A, Koster AS, Buurma H. Development of a postgraduate community pharmacist specialization program using CanMEDS competencies, and entrustable professional activities. Am J Pharm Educ. 2019;83(6):6. doi:10.5688/ajpe6863
42. Johnson CH. Competencies as an evaluation tool. Clin Podiatr Med Surg. 2007;24(1):103–117. doi:10.1016/j.cpm.2006.08.006
43. Smith KM, Geletta S, Langan T. Assessment of a cultural competency program in podiatric medical education. J Am Podiatr Med Assoc. 2016;106(1):68–75. doi:10.7547/14-067
44. Miranda FBG, Mazzo A, Alves Pereira-Junior G. Construction and validation of competency frameworks for the training of nurses in emergencies. Rev Lat Am Enfermagem. 2018;26:45.
45. Meadows N, Webb D, McRobbie D, Antoniou S, Bates I, Davies G. Developing and validating a competency framework for advanced pharmacy practice. Pharmaceut J. 2004;273:789–792.
46. Kopf RS, Watts PI, Meyer ES, Moss JA. A competency-based curriculum for critical care nurse practitioners’ transition to practice. Am J Crit Care. 2018;27(5):398–406. doi:10.4037/ajcc2018101
47. Bélisle M, Lavoie P, Pepin J, et al. A conceptual framework of student professionalization for health professional education and research. Int J Nurs Educ Scholarsh. 2021;18(1):1. doi:10.1515/ijnes-2020-0104
48. Cosma D-T, Gavan N. The podiatry role in the foot care. Sports Med J. 2017;13:1.
49. McPherson S, Reese C, Wendler MC. Methodology update: delphi studies. Nurs Res. 2018;67(5):404–410. doi:10.1097/NNR.0000000000000297
50. Ringsted C, Hansen TL, Davis D, Scherpbier A. Are some of the challenging aspects of the CanMEDS roles valid outside Canada? Med Edu. 2006;40(8):807–815. doi:10.1111/j.1365-2929.2006.02525.x
51. Herion C, Egger L, Greif R, Violato C. Validating international Can MEDS‐based standards defining education and safe practice of nurse anesthetists. Int Nurs Rev. 2019;66(3):404–415.
52. Penciner R, Langhan T, Lee R, Mcewen J, Woods RA, Bandiera G. Using a Delphi process to establish consensus on emergency medicine clerkship competencies. Med Teach. 2011;33(6):e333–e339. doi:10.3109/0142159X.2011.575903
53. Valani RA, Yanchar N, Grant V, Hancock B. The development of a national pediatric trauma curriculum. Med Teach. 2010;32(3):e115–e119. doi:10.3109/01421590903398240
54. Domecq JP, Prutsky G, Elraiyah T, et al. Patient engagement in research: a systematic review. BMC Health Serv Res. 2014;14(1):1–9.
55. Roe, R. A. (2002) What makes a competent psychologist? European Psychologist, 7(3), 192202. doi:10.1027//1016-9040.7.3.192
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.