")
Back to Journals » Journal of Pain Research » Volume 12
Comparisons of the efficacy and recurrence of adenomyomectomy for severe uterine diffuse adenomyosis via laparotomy versus laparoscopy: a long-term result in a single institution
Authors Zhu L, Chen S, Che X, Xu P, Huang X , Zhang X
Received 15 February 2019
Accepted for publication 24 May 2019
Published 27 June 2019 Volume 2019:12 Pages 1917—1924
DOI https://doi.org/10.2147/JPR.S205561
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Katherine Hanlon
Libo Zhu, Shuyi Chen, Xuan Che, Ping Xu, Xiufeng Huang, Xinmei Zhang
The Department of Gynecology, Women’s Hospital, School of Medicine, Zhejiang University, Hangzhou, Zhejiang 310006, People’s Republic of China
Purpose: Studies have shown that adenomyomectomy can effectively treat women with adenomyosis in a short period of time. However, the long-term efficacy of adenomyomectomy has rarely been reported. The objective of this study was to determine whether laparotomy is superior to laparoscopic surgery in the long-term efficacy of double-flap method adenomyomectomy for severe diffuse adenomyosis.
Methods: Between March 2011 and September 2018, a total of 148 patients with severe uterine diffuse adenomyosis who underwent laparoscopic (group A, n=72) and laparotomic (group B, n=76) double-flap adenomyomectomy were recruited. Adenomyomectomy efficacy and adenomyosis recurrence after surgery between groups A and B were comparatively analyzed.
Results: The effective rate at 6-year follow up after surgery was higher in group B (75.0%) than that in group A (62.1%), while the 6-year cumulative recurrence rate was higher in group A (27.8%) than that in group B (17.1%), but the differences did not reach statistical significance between the two groups (P>0.05). The recurrence rate was lower in patients who were treated with gonadotropin-releasing hormone agonist (GnRHa) plus Mirena or oral contraceptives post-surgically than that in patients who were treated with only GnRHa post-surgically in groups A (51.6% vs 9.8%, P<0.01) and B (33.3% vs 6.5%, P<0.05). Moreover, the recurrence rate of adenomyosis patients with endometriosis was higher than that of adenomyosis patients without endometriosis in group A (55.0% vs 17.3%, P<0.05) and group B (36.0% vs 7.8%, P<0.05).
Conclusion: The long-term outcomes of laparoscopic and laparotomic double-flap adenomyomectomy can be achieved for severe diffuse uterine adenomyosis, but laparotomy seems to have advantages over laparoscopy. Postoperative drug use may be beneficial to reduce the recurrence of adenomyosis, especially for adenomyosis with endometriosis.
Keywords: adenomyosis, adenomyomectomy, efficacy, recurrence, treatment
Introduction
Adenomyosis, characterized by the invasion of endometrial glands and stroma in the uterine myometrium, is a common benign gynecologic disease. The main symptoms of adenomyosis are hypermenorrhea, dysmenorrhea, and subfertility.1,2 Moreover, adenomyosis may be associated with recurrent abortion, premature delivery, and complications of late pregnancy such as placenta previa.3–8 Drug therapy includes gonadotropin-releasing hormone agonists (GnRHa), oral contraceptive pills (OCs), levonorgestrel-releasing intrauterine devices (LNG-IUS or Mirena), high-dose progestins, danazol, aromatase inhibitors, and selective estrogen/progesterone receptor modulators can relieve symptoms effectively,9–11 but these drugs are only temporary, and pregnancy is not possible during drug therapy. In addition, some patients are refractory to drug therapy. Although high intensity focused ultrasound (HIFU) and uterine arterial embolization (UAE) are both effective in the treatment of adenomyosis, yet, the therapeutic effects of these two techniques on adenomyosis still remain to be further investigated.12–16 As a matter of fact, only total hysterectomy can thoroughly treat adenomyosis.
Recently, the trend of uterus-sparing surgery in the treatment of adenomyosis has been gradually increasing with the delay of women’s childbearing age and their strong desire to retain uterus. For focal uterine adenomyosis, such as adenomyoma and cystic adenomyosis, the surgical procedure of adenomyomectomy for adenomyosis is relatively simple, which is the same as myomectomy for uterine leiomyoma.17 However, for diffuse uterine adenomyosis, the surgical procedure of adenomyomectomy for adenomyosis is always difficult, because diffuse uterine adenomyosis involves the entire myometrium or more than half of the total myometrium.18–20 Obviously, conservative surgery for diffuse uterine adenomyosis is only the partial resection of adenomyosis.21
Currently, many resection methods of uterus-sparing surgery have been demonstrated to treat diffuse uterine adenomyosis effectively, but only the triple-flap adenomyomectomy can almost completely remove the lesions of diffuse uterine adenomyosis.22 In our previous study, we modified the technique of the triple-flap method to perform laparoscopic double-flap adenomyomectomy in the treatment of uterine diffuse adenomyosis.1 Our previous results showed that laparoscopic double-flap adenomyomectomy can effectively treat severe diffuse uterine adenomyosis in a short time.1 However, the long-term efficacy and the surgical modes of adenomyomectomy are still debated. The objective of our present study was to evaluate the long-term outcomes of laparoscopic double-flap adenomyomectomy in the treatment of severe uterine diffuse adenomyosis and compare the efficacy of adenomyomectomy via laparoscopy and laparotomy in the treatment of severe diffuse uterine adenomyosis.
Patients and methods
Patients
The study was approved by the Ethics Committee of Women’s Hospital, Zhejiang University School of Medicine in accordance with the Declaration of Helsinki, and we obtained the written informed consent of each participant in this study.
Between March 2011 and September 2018, 148 women with severe diffuse uterine adenomyosis underwent laparoscopic and laparotomic double-flap adenomyomectomy in the women’s hospital of Zhejiang University School of Medicine. The indications of adenomyomectomy in the present study were previously described by Huang et al.1 Briefly, the patient complained of severe dysmenorrhea with or without hypermenorrhea but failed to respond to drug therapy. Adenomyosis was verified by ultrasonography and magnetic resonance imaging (MRI). Moreover, the patient wanted to retain the uterus. The 148 patients with diffuse adenomyosis were assigned to undergo laparoscopic double-flap adenomyometomy (Group A, n=72) and laparotomic double-flap adenomyometomy (Group B, n=76) based on patient requirements. All patients received GnRHa for six months, followed by LNG-IUS or OCs after surgery. None of the patients in the study withdrew their consent or did not follow-up after operation, and none of them were treated with sex hormone three months pre-operatively.
Procedure of double-flap adenomyomectomy
The surgical procedure of double-flap adenomyomectomy was previously described in detail by Huang et al.1 Laparotomic double-flap adenomyomectomy was performed through an abdominal straight incision, while laparoscopic double-flap adenomyomectomy was performed by four-port technique. The technique of laparotomic double-flap adenomyomectomy was the same as that of laparoscopic double-flap adenomyomectomy. Briefly, a sagittal midline incision was made on the serosal surface of the uterine fundus and entered the uterine cavity. Next, the incision extended further into the level of the internal os of the uterine cervix along the posterior and anterior walls of the uterus. Afterwards, adenomyotic lesions were excised from the uterine wall as far as possible. During the surgical procedures, the endometrium, uterine serosal surface, and tubal interstitium of the patients who desired to have future pregnancies should be avoided to damage. And the inner and outer myometrium of the uterus, which was 1 cm thick, usually remained, respectively. The endometrium, myometrium, and serosa of the uterus were reconstructed by using the double-flap technique of Huang et al (Figure 1).1 The specimens were confirmed by histopathological examination postoperatively.
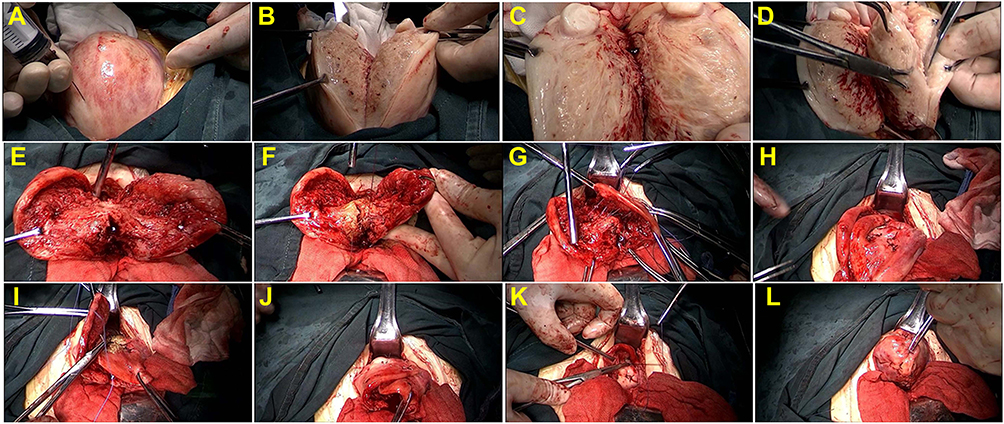 |
Figure 1 Surgical procedure of laparotomic double-flap adenomyomectomy. (A) Diluted pituitrin was injected into uterine wall; (B and C) An incision was made in the serosal surface midline of uterine fundus by using scalpel and continued along the sagittal direction until the uterine cavity was reached; (D and E) Adenomyomatous tissues were grasped with forceps, identified, and excised from the surrounding myometrium; (F) The endometrial lining was approximated with interrupted sutures of 3–0 Vicryl; (G and H) The first flap in one side wall of the uterus was brought into the second flap in another side of the uterine wall so that the other side wall of the uterus was covered; (I, J, K and L) The second flap in another side of the uterine wall was brought to cover the first flap in one side wall of the uterus. Before overlapping occurred, the serosal surface of the underlying flaps was stripped to ensure that only myometrial tissue flaps overlapped. |
Measurement of curative effect indexes
In this study, menorrhagia is arbitrarily defined as the use of menstrual products for more than 5 pads/day, and the severity of menorrhagia was divided into mild (5 to 7 pads/day), moderate (7 to 9 pads/day), and severe (>9 pads/day).1 The severity of dysmenorrhea was scored using a standardized questionnaire with a visual analog scale (VAS). The pain scale was subdivided into ten grades. “No pain” was indicated at the left side of the scale and “the maximum pain you could imagine” was designated at the right side of the scale. Serum CA125 levels were determined by enzyme-linked immunosorbent assay (ELISA) with a human CA125 ELISA kit (HM10776, Bio-swamp) according to the manufacturer’s instructions (the range of normal value was ≤35 kU/L). The size of the uterus was measured by ultrasonography [uterine volume=A×B×C×0.5233 (where A, B, and C are the uterine length, width, and thickness, respectively)].1
Evaluation of therapeutic efficacy
The therapeutic efficacy of adenomyomectomy was evaluated according to the following criteria in this study: ① Complete remission: Dysmenorrhea disappeared completely after surgery; ② Significant remission: Pain score (VAS score) decreased by more than 3 grades, but dysmenorrhea did not disappear completely after surgery; ③ Partial remission: Pain score was reduced by less than 2 grades, but dysmenorrhea did not disappear after surgery; ④ No remission: Pain score did not change after surgery; ⑤ Recurrence: Complete remission or significant remission was achieved, but dysmenorrhea recurred and aggravated progressively one year after operation, and the appearance of adenomyotic lesions was confirmed by ultrasound or MRI. As such, complete remission and significant remission were defined as clinically effective operations, while partial remission, no remission, and recurrence were defined as clinically ineffective operations. In addition, the presence of pregnancy and improvement of menorrhagia after surgery were also evaluated in this study.
Follow-up
All patients were followed up 1, 3, 6, and 12 months after surgery, and subsequently every year postoperatively. For each follow-up visit, gynecological examination and ultrasonography, serum CA125 levels, and the evaluation of dysmenorrhea and menorrhagia are required in the endometriosis clinic. In our previous study, laparoscopic adenomyomectomy by using the modified double-flap method has been shown to achieve good results in the treatment of severe uterine diffuse adenomyosis within 2 years. In the present study, we aimed to evaluate the long-term efficacy of adenomyomecyomy by using the double-flap method and compare the efficacy of adenomyomectomy by using the double-flap method via laparoscopy versus laparotomy. As such, we focused on two endpoints to determine the long-term surgical efficacy. The results of the preoperative visit were compared with those of the 2-year follow-up and those of the 6-year follow-up to observe the long-term efficacy after surgery.
Statistical analysis
We used SPSS version 17.0 (SPSS, IBM, Chicago, IL, USA) to perform statistical analyses. Results were expressed as the mean value±standard derivation (SD) although the measured values of the variables were not normally distributed. Mann–Whitney U test was performed to compare non-parametric data, Student’s t-test was used to compare parametric data, and Chi-square test was conducted to compare the frequency between groups. Differences were considered significant at P<0.05.
Results
All the 148 patients had severe dysmenorrhea, and 111 of them had simultaneous menorrhagia (pads>5). Before surgery, endometriosis was diagnosed in 29 patients, and 27 women had uterine leiomyoma. After surgery, 45 patients had endometriosis confirmed by laparoscopy/laparotomy or/and postoperative pathology. Of the 45 patients with endometriosis, peritoneal endometriosis was found during surgery in 16 women. There were no significant differences in age, pregnancy, parity, abortion, serum CA125 level, uterine volume, VAS score, and menorrhagia between the two groups, although the uterine volume of group B was larger than that of group A (P>0.05, Table 1). Whether laparotomy or laparoscopic adenomyomectomy, the effective rate was gradually decreased with the prolongation of the time after surgery, but the differences did not reach statistical significance (P>0.05). Each year except for the first year after surgery, the effective rate of laparotomy adenomyomectomy was always higher than that of laparoscopic adenomyomectomy; however, no significant differences between the two groups were found (P>0.05, Table 2). The cumulative recurrence rate within the 6 years after surgery was 17.1% (13/76) and 27.8% (20/72) in group B and group A, respectively. There was no significant difference with respect to the cumulative recurrence rate between the two groups (P>0.05, Table 2). Each year after surgery, the effective rate of complete pain relief in group B was always higher than that in group A, while the effective rate of significant pain relief was always higher in group A than that in group B. However, the differences with respect to the effective rate of complete or significant pain relief between the two groups did not reach statistical significance (P>0.05, Table 2).
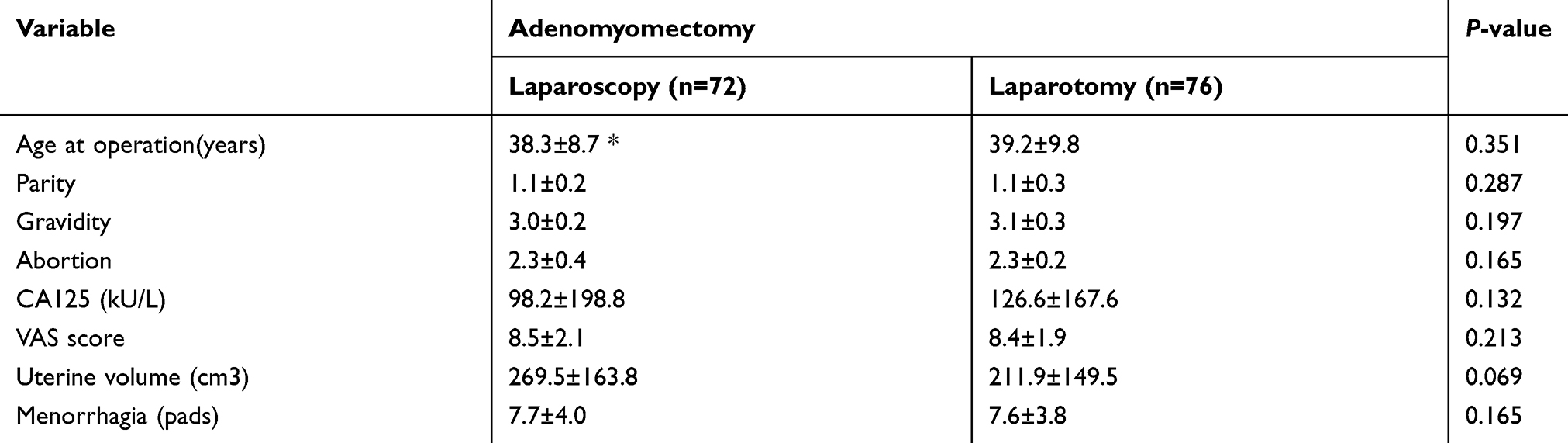 |
Table 1 Patients’ characteristics |
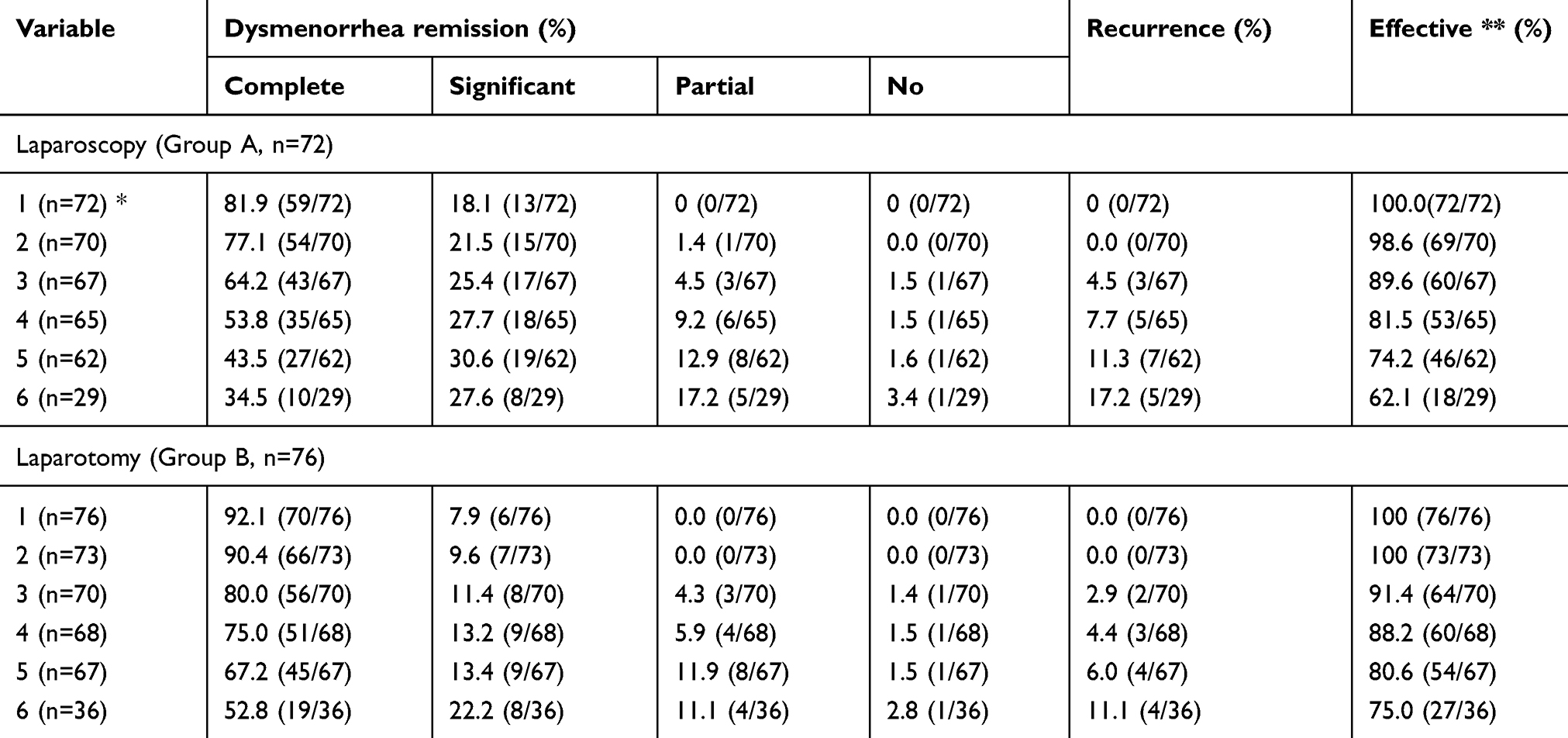 |
Table 2 Dysmenorrhea relief and adenomyosis recurrence after adenomyomectomy |
After surgery, VAS scores were both significantly decreased as compared with those before surgery in groups A and B (P<0.05), but the VAS scores were gradually increased with the prolongation of postoperative time in the two groups (Table 3). In group A, from the second year after operation, VAS score increased significantly year by year (P<0.05). In group B, from the fourth year after surgery, VAS score increased significantly each year (P<0.05). From the third year to the sixth year after surgery, the VAS score of group A was always higher than that of group B (P<0.05, Table 3). Similar to VAS score, the number of healthy pads used during menstruation after surgery was significantly lower than that before surgery in groups A and B, but the number of pads increased gradually with the prolongation of postoperative time in the two groups (Table 3). From the second year to the sixth year after operation, the number of pads used was always higher in group A than that in group B, but the differences between the two groups did not reach statistical significance (P>0.05, Table 3)
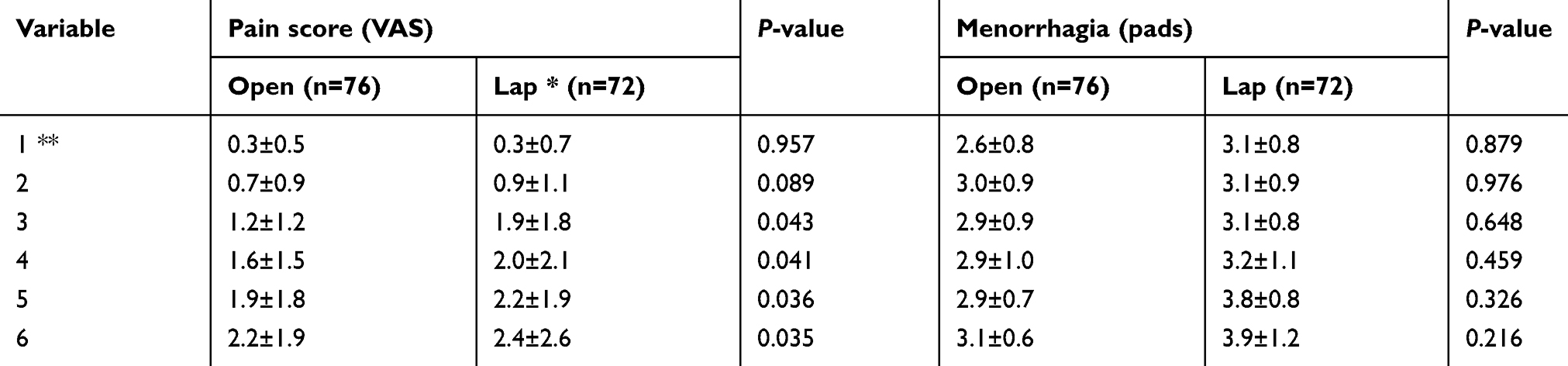 |
Table 3 Changes in pain score and menorrhagia after adenomyomectomy |
There were significant differences of the recurrence rate between patients who were only treated with GnRHa after surgery and patients who were treated with GnRHa plus LNG-IUS or OCs after surgery in the two groups (P<0.05). Moreover, the recurrence rate was significantly higher in patients with adenomyosis who coexisted with endometriosis than that in patients with only adenomyosis in the two groups (P<0.05). Although the recurrence rate was higher in patients with uterine volume >200 mm2, CA125 levels >200 kU/L, and age ≤35 years old compared with patients with uterine volume ≤200 mm2, CA125 levels ≤200 kU/L, and age >35 years old in the 2 groups, but the differences did not reach statistical significance (P>0.05, Table 4). In addition, no significant difference with respect to extent of adenomyosis or menorrhagia was found either in group A or group B (P>0.05, Table 4).
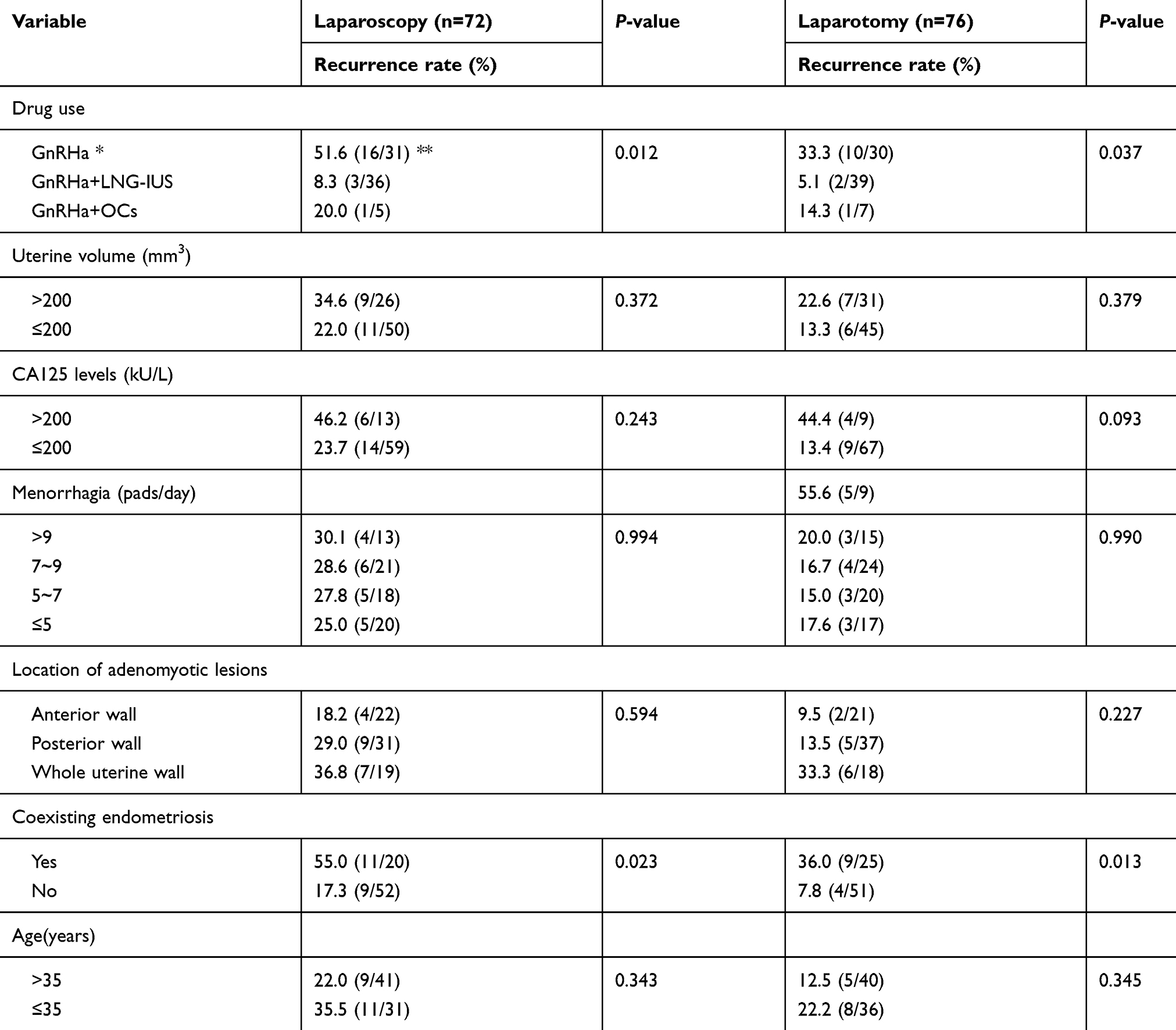 |
Table 4 Influence of factors on adenomyosis recurrence after adenomyomectomy |
Discussion
Our previous study has demonstrated a significant reduction in pain symptoms, menorrhagia, serum CA125 levels, and uterine size in patients with severe diffuse adenomyosis within the 2 years after laparoscopic adenomyomectomy using the modified double-flap method.1 Our current results showed that the effective rate was almost 100% within 2 years after laparoscopic or laparotomic adenomyomectomy by using the modified double-flap method in patients with severe diffuse uterine adenomyosis, which confirmed our previous results.1 Recently, one study by Kwack et al showed that dysmenorrhea was improved in 100% of the patients with diffuse uterine adenomyosis at the 7-month follow-up after adenomyomectomy using the muscle fold method.23 Another study by Jun-Min et al found that the effective rate was 94.9% in patients with diffuse uterine adenomyosis within 2 years after the U-shaped adenomyomectomy.24 Osada et al reported that the VAS score of dysmenorrhea was decreased from 10.00±0.00 pre-surgically to 1.67±1.79 at 2-year follow-up after the triple-flap method adenomyomectomy in patients with diffuse adenomyosis.22 As a matter of fact, although the therapeutic efficacy of adenomyomectomy is mainly dependent on the type and extent of adenomyosis as well as the modes of surgery, yet, different definitions of efficacy can also lead to different outcomes. Nevertheless, the short-term efficacy of adenomyomectomy is encouraging for the treatment of adenomyosis.18,19
However, the long-term efficacy of adenomyomectomy is rarely reported. Although there are long-term data in the literature, the evaluation of efficacy is still short term.18,23 Our results showed that although the therapeutic efficacy was decreased with the prolongation of postoperative time after laparoscopic or open adenomyomectomy, yet, the effective rate was both more than 60.0% at 6-year follow-up after surgery. It is indicated that the long-term therapeutic efficacy of adenomyomectomy by using the modified double-flap method can be achieved for the treatment of severe diffuse adenomyosis. Our results also showed that the effective rate was always higher in patients with adenomyosis undergoing open adenomyomectomy when compared with that in patients with adenomyosis undergoing laparoscopic adenomyomectomy although the differences the two groups did not reach statistical significance. Obviously, in terms of adenomyomectomy for the treatment of uterine diffuse adenomyosis, laparotomy seems to have an advantage to laparoscopy. Therefore, for near-complete excision of adenomyosis, especially for these patients who preserve fertility, diffuse adenomyotic lesions may be recommended to be treated with laparotomic adenomyomectomy while focal lesions less than 5 cm could be treated with laparoscopic conservative surgery.18,23
It is well known that conservative surgery for adenomyosis cannot remove all adenomyotic lesions, even if adenomyosis is characterized by focal lesions. As a result, adenomyosis recurrence (or residual adenomyotic lesions) is unavoidable, which is also the reason why the efficacy of adenomyomectomy decreases over time after surgery. Our results showed that the recurrence rate of adenomyosis after laparoscopic or laparotomic adenomyomecomy was significantly higher in adenomyosis patients with endometriosis than that in adenomyosis patients without endometriosis. Pain is also a characteristic symptom of endometriosis, and its recurrence is very common after conservative surgery for endometriosis.25 It is indicated that coexistence of endometriosis is a high-risk factor for the recurrence of adenomyosis after adenomyomectomy.26 Our results also showed that after laparoscopic or laparotomic adenomyomectomy, patients who were treated with GnRHa plus LNG-IUS or OCs had a significantly lower rate of recurrence when compared with patients who were only treated with GnRHa. These results are consistent with the previous report of Yu et al.26 Obviously, drug therapy is recommended for patients with adenomyosis after adenomyomectomy.
Although serum CA125 is considered as a high-risk factor for recurrence of adenomyosis and an indicator of therapeutic efficacy in adenomyosis,10,26–28 yet, our results did not find any significant differences with respect to the recurrence of adenomyosis between patients with CA 125 levels >200 kU/L and CA 125 levels ≤200 kU/L. Moreover, although the recurrence rates of adenomyosis were all higher in patients with adenomyosis infiltrating whole uterine wall, younger age, and large uterine size when compared with that in patients with adenomyosis infiltrating posterior or anterior uterine wall, old age, and small uterine size, yet, the differences did not reach statistical significance. In addition, our study also found that the recurrence rate in patients with diffuse adenomyosis was higher after laparoscopic adenomyomectomy compared with that after laparotomic adenomyomectomy, although there was no significant difference of adenomyosis recurrence between laparoscopic and laparotomic adenomyomectomy. Obviously, laparotomic adenomyomectomy seems to have an advantage over laparoscopic adenomyomectomy in terms of adenomyosis recurrence.18,23 Nevertheless, in order to obtain good surgical results, conservative surgery should also consider the patient’s age, serum CA125 levels, and uterine size as well as the extent and type of adenomyosis.
In summary, our results showed that the long-term outcomes of adenomyomectomy by using the modified double-flap method via laparoscopy or laparotomy could be achieved in the treatment of severe uterine diffuse adenomyosis, and the effective rates were both more than 60% at 6-year follow up after surgery. For the recurrence of adenomyosis after adenomyomectomy, drug therapy after surgery is a protective factor, while coexisting endometriosis is a high-risk factor. In terms of curative effect and recurrence of adenomyosis after adenomyomectomy, laparotomy seems to be superior to laparoscopy. Due to small samples in our study, further studies with large population to confirm these results are needed.
Acknowledgments
This work was supported by the grants of the National Key R&D Program of China ( 2017YFC1001202) and the National Natural Science Foundation of China (81471433, 81671429, 81471127).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Huang X, Huang Q, Chen S, et al. Efficacy of laparoscopic adenomyomectomy using double-flap method for diffuse uterine adenomyosis. BMC Womens Health. 2015;15:24. doi:10.1186/s12905-015-0182-5
2. Li Q, Ding Y, Zhang XY, Feng WW, Hua KQ. Drug therapy for adenomyosis: a prospective, nonrandomized, parallel-controlled study. J Int Med Res. 2018;46(5):1855–1865. doi:10.1177/0300060517752997
3. Buggio L, Monti E, Gattei U, Dridi D, Vercellini P. Adenomyosis: fertility and obstetric outcome. A comprehensive literature review. Minerva Ginecol. 2018;70(3):295–302. doi:10.23736/S0026-4784.17.04163-6
4. Bruun MR, Arendt LH, Forman A, Ramlau-Hansen CH. Endometriosis and adenomyosis are associated with increased risk of preterm delivery and a small-for-gestational-age child: a systematic review and meta-analysis. Acta Obstet Gynecol Scand. 2018;97(9):1073–1090. doi:10.1111/aogs.13364
5. Shin YJ, Kwak DW, Chung JH, Kim MY, Lee SW, Han YJ. The risk of preterm births among pregnant women with adenomyosis. J Ultrasound Med. 2018;37(8):1937–1943. doi:10.1002/jum.14540
6. Tamura H, Kishi H, Kitade M, et al. Complications and outcomes of pregnant women with adenomyosis in Japan. Reprod Med Biol. 2017;16(4):330–336. doi:10.1002/rmb2.12050
7. Yamaguchi A, Kyozuka H, Fujimori K, et al. Risk of preterm birth, low birthweight and small-for-gestational-age infants in pregnancies with adenomyosis: a cohort study of the Japan Environment and Children’s Study. Acta Obstet Gynecol Scand. 2018. [Epub ahead of print]. doi:10.1111/aogs.13498
8. Cozzolino M, Basile F, Pontrelli G. Effects of adenomyosis on obstetric outcomes: a literature review. Minerva Ginecol. 2018. [Epub ahead of print]. doi:10.23736/S0026-4784.18.04318-6
9. Vannuccini S, Luisi S, Tosti C, Sorbi F, Petraglia F. Role of medical therapy in the management of uterine adenomyosis. Fertil Steril. 2018;109(3):398–405. doi:10.1016/j.fertnstert.2018.01.013
10. Neriishi K, Hirata T, Fukuda S, et al. Long-term dienogest administration in patients with symptomatic adenomyosis. J Obstet Gynaecol Res. 2018;44(8):1439–1444. doi:10.1111/jog.13674
11. Wu J, Huang Y, Chen L, Hu J, Zou Y. Treatment of adenomyosis with subcutaneous etonogestrel implants: a clinical observational study in 17 patients. Med Sci Monit. 2018;24:6085–6092. doi:10.12659/MSM.908979
12. de Bruijn AM, Lohle PN, Huirne JA, de Vries J, Twisk M, Hehenkamp WJ, ; . Uterine artery embolization versus hysterectomy in the treatment of symptomatic adenomyosis: protocol for the randomized QUESTA trial. JMIR Res Protoc. 2018;7(3):e47. doi:10.2196/resprot.8512
13. Keung JJ, Spies JB, Caridi TM. Uterine artery embolization: a review of current concepts. Best Pract Res Clin Obstet Gynaecol. 2018;46:66–73. doi:10.1016/j.bpobgyn.2017.09.003
14. Liang E, Brown B, Rachinsky M. A clinical audit on the efficacy and safety of uterine artery embolisation for symptomatic adenomyosis: results in 117 women. Aust N Z J Obstet Gynaecol. 2018;58(4):454–459. doi:10.1111/ajo.12767
15. Guo Q, Xu F, Ding Z, Li P, Wang X, Gao B. High intensity focused ultrasound treatment of adenomyosis: a comparative study. Int J Hyperthermia. 2018:1–5. [Epub ahead of print]. doi:10.1080/02656736.2018.1509238
16. Keserci B, Duc NM. Magnetic resonance imaging features influencing high-intensity focused ultrasound ablation of adenomyosis with a nonperfused volume ratio of ≥90% as a measure of clinical treatment success: retrospective multivariate analysis. Int J Hyperthermia. 2018:1–11. [Epub ahead of print]. doi:10.1080/02656736.2018.1516301
17. Wang CJ, Yuen LT, Chang SD, Lee CL, Soong YK. Use of laparoscopic cytoreductive surgery to treat infertile women with localized adenomyosis. Fertil Steril. 2006;86(2):
18. Osada H. Uterine adenomyosis and adenomyoma: the surgical approach. Fertil Steril. 2018;109(3):406–417. doi:10.1016/j.fertnstert.2018.01.032
19. Oliveira MAP, Crispi CP
20. Grimbizis GF, Mikos T, Tarlatzis B. Uterus-sparing operative treatment for adenomyosis. Fertil Steril. 2014;101(2):472–487. doi:10.1016/j.fertnstert.2013.10.025
21. Horng HC, Chen CH, Chen CY, et al. Uterine-sparing surgery for adenomyosis and/or adenomyoma. Taiwan J Obstet Gynecol. 2014;53(1):3–7. doi:10.1016/j.tjog.2014.01.001
22. Osada H, Silber S, Kakinuma T, Nagaishi M, Kato K, Kato O. Surgical procedure to conserve the uterus for future pregnancy in patients suffering from massive adenomyosis. Reprod Biomed Online. 2011;22(1):94–99. doi:10.1016/j.rbmo.2010.09.014
23. Kwack JY, Im KS, Kwon YS. Conservative surgery of uterine adenomyosis via laparoscopic versus laparotomic approach in a single institution. J Obstet Gynaecol Res. 2018;44(7):1268–1273. doi:10.1111/jog.13658
24. Jun-Min X, Kun-Peng Z, Yin-Kai Z, et al. A new surgical method of u-shaped myometrial excavation and modified suture approach with uterus preservation for diffuse adenomyosis. Biomed Res Int. 2018;2018:1657237. doi:10.1155/2018/1657237
25. Liu X, Yuan L, Shen F, Zhu Z, Jiang H, Guo SW. Patterns of and risk factors for recurrence in women with ovarian endometriomas. Obstet Gynecol. 2007;109(6):1411–1420. doi:10.1097/01.AOG.0000265215.87717.8b
26. Yu W, Liu G, Liu C, Zhang Z. Recurrence-associated factors of laparoscopic adenomyomectomy for severely symptomatic adenomyoma. Oncol Lett. 2018;16(3):3430–3438. doi:10.3892/ol.2018.9082
27. Zheng R, Zeng D, Wan TT, Guo WB, Guo Y, Liu MJ. Predisposing factors for predicting the therapeutic response of adenomyosis after uterine artery embolization: serum CA125 levels and accompanying endometriosis. Diagn Interv Radiol. 2018;24(6):364–371. doi:10.5152/dir.2018.17479
28. Mu Y, Hu X, He J, et al. Serum levels of vascular endothelial growth factor and cancer antigen 125 are related to the prognosis of adenomyosis patients after interventional therapy. Int J Clin Exp Med. 2015;8(6):9549–9554.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.