Back to Journals » Infection and Drug Resistance » Volume 19
Comparison of Xpert MTB/RIF Assay and the Targeted Next-Generation Sequencing for the Diagnosis of Pleural Tuberculosis: A Prospective Comparative Diagnostic Accuracy Study
Authors Wen P ![]() , Wang SX, Ma XM, Chen HY, Ma ZX, Zhang YZ, Wei M
, Wang SX, Ma XM, Chen HY, Ma ZX, Zhang YZ, Wei M
Received 15 December 2025
Accepted for publication 7 April 2026
Published 22 May 2026 Volume 2026:19 589240
DOI https://doi.org/10.2147/IDR.S589240
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Hazrat Bilal
Peng Wen,1,* Shang Xue Wang,1,* Xiao Man Ma,1 Hong Yan Chen,1 Zeng Xia Ma,1 Yun Zeng Zhang,2 Min Wei1
1Department of Respiratory Medicine, Public Health Clinical Center Affiliated to Shandong University, Jinan, People’s Republic of China; 2Department of Thoracic Surgery, Public Health Clinical Center Affiliated to Shandong University, Jinan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Min Wei, Department of Respiratory Medicine, Public Health Clinical Center Affiliated to Shandong University, 2999# Gangxing West Road, Jinan, 250100, People’s Republic of China, Email [email protected] Yun Zeng Zhang, Department of Thoracic Surgery, Public Health Clinical Center Affiliated to Shandong University, 2999# Gangxing West Road, Jinan, 250100, People’s Republic of China, Email [email protected]
Purpose: To evaluate the diagnostic performance of targeted next-generation sequencing (tNGS), a multiplex PCR–based and hybrid-capture sequencing platform targeting 198 respiratory pathogens, versus Xpert MTB/RIF in diagnosing pleural tuberculosis (TB) across diverse specimen types, given the limited sensitivity of existing assays in paucibacillary disease.
Patients and Methods: Consecutive patients with suspected pleural TB were prospectively enrolled. Final diagnosis was established using a composite reference standard incorporating microbiological, histopathological, and clinical criteria. Paired sputum, pleural fluid, and pleural biopsy specimens underwent tNGS, Xpert MTB/RIF, and mycobacterial culture. Diagnostic performance metrics, including sensitivity and specificity, were calculated. A predefined paired comparison (n=105) between tNGS and Xpert MTB/RIF was performed, with agreement assessed using Cohen’s kappa.
Results: In the overall cohort (N = 142), tNGS demonstrated higher sensitivity than Xpert MTB/RIF and mycobacterial culture across specimen types when evaluated against the composite reference standard, while maintaining 100% specificity in the non-TB group (n = 8). In sputum samples, tNGS achieved a sensitivity of 72.73%, significantly outperforming Xpert MTB/RIF (21.43%) and MTB culture (16.30%). In pleural fluid, tNGS sensitivity (43.64%) exceeded that of Xpert MTB/RIF (30.49%) and MTB culture (24.14%), comparable to the performance of ADA ≥ 40 U/L (46.22%). The paired analysis confirmed that tNGS significantly outperformed Xpert MTB/RIF in overall diagnostic yield (p < 0.01), detecting 26 positive cases missed by Xpert. Among patients with culture-negative pleural tuberculosis, tNGS detected 24/60 (40.0%) cases compared with 6/60 (10.0%) by Xpert MTB/RIF.
Conclusion: tNGS provides incremental diagnostic value over conventional molecular and culture-based assays in pleural tuberculosis, particularly in paucibacillary and culture-negative disease. It increases microbiological confirmation in culture- and Xpert-negative cases and is best positioned as a complementary second-line assay within a tiered diagnostic framework, despite no assessment of downstream clinical impact.
Keywords: targeted next-generation sequencing, pleural tuberculosis, Xpert MTB/RIF, diagnosis
Introduction
Pleural tuberculosis (TB), a significant form of extrapulmonary TB, has seen a notable increase in incidence over the last two decades.1 The prevalence of pleural TB among TB patients varies between 3% and 30%, influenced by regional TB rates and comorbidities like human immunodeficiency virus (HIV),2 contributing to significant morbidity and mortality.
The gold standard for the diagnosis of pleural TB relies on detecting Mycobacterium tuberculosis (MTB) in pleural fluid or biopsy specimens through nucleic acid amplification tests (NAATs) and culture, or typical histological evidence.2 Pathophysiologically, pleural TB represents a delayed-type hypersensitivity reaction to mycobacterial antigens within the pleural space, typically accompanied by a low bacillary burden despite active disease.3 This paucibacillary immunopathogenesis markedly reduces the sensitivity of smear microscopy, culture, and NAATs, frequently resulting in false-negative microbiological findings even in clinically evident cases. Furthermore, the non-specific clinical presentation of pleural TB adds to the diagnostic challenges, making it difficult to identify early and accurately. Timely and accurate diagnosis is crucial for initiating appropriate treatment of pleural TB and minimizing associated morbidity. While NAATs like the Xpert MTB/RIF assay have revolutionized TB diagnostics with rapid results and rifampicin resistance detection, their sensitivity in pleural fluid remains insufficient, averaging around 21% with a composite reference standard as the benchmark and ranging from 26–60% even in culture-confirmed cases.4–7 Some studies have reported higher estimates (eg, 54.8%);8 however, these findings are context-dependent and remain insufficient for reliable rule-out in paucibacillary disease.
Targeted next-generation sequencing (tNGS) has recently emerged as a molecular platform integrating multiplex PCR enrichment with high-throughput sequencing. Compared with conventional NAATs, tNGS offers a lower theoretical limit of detection and the ability to detect fragmented or low-abundance mycobacterial DNA.9,10 These analytical characteristics may be particularly advantageous in extrapulmonary and paucibacillary specimens, in which bacillary loads often fall below the detection thresholds of standard assays. However, the clinical role of tNGS in pleural tuberculosis remains undefined. It is uncertain whether tNGS should replace established frontline molecular diagnostics or be deployed selectively in diagnostically challenging scenarios. The present study was therefore designed not to supplant Xpert MTB/RIF as an initial diagnostic test, but to evaluate whether tNGS confers incremental diagnostic yield in patients with clinically suspected pleural tuberculosis who test negative by Xpert MTB/RIF or mycobacterial culture.
Accordingly, a prospective head-to-head diagnostic accuracy study was conducted to compare tNGS with Xpert MTB/RIF and mycobacterial culture across multiple specimen types, including sputum, pleural fluid, and pleural biopsy specimens. The primary objective was to evaluate whether tNGS confers incremental diagnostic yield beyond conventional molecular and culture-based methods. Secondary objectives included comparison of diagnostic performance across specimen types and evaluation of performance in culture-negative and Xpert-negative subgroups.
Materials and Methods
Study Design and Participants
This investigation was designed as a prospective diagnostic accuracy study conducted in accordance with established diagnostic test accuracy methodology. Consecutive participants were enrolled over a predefined study period to reflect real-world clinical practice. A formal sample size calculation was not performed, as the primary objective was to assess incremental diagnostic yield under routine conditions rather than to test a prespecified superiority hypothesis. The final sample size was therefore determined by the number of eligible patients recruited during the study timeframe. Diagnostic performance estimates are reported with 95% CIs to indicate statistical precision.
This prospective study was conducted at the Shandong Public Health Clinical Center between January 2023 and September 2025. The study was approved by the Ethics Committee of the Shandong Provincial Public Health Clinical Center, Shandong University (approval number: GWLCZXEC2024-22-1), and conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants or their legal guardians.
Consecutive patients with suspected pleural TB, presenting with symptoms such as cough, chest pain, shortness of breath, fever, night sweats, weight loss, and showing evidence of pleural effusion on chest X-ray, were prospectively enrolled. Pleural fluid and biopsy samples obtained through thoracentesis or medical thoracoscopy, along with sputum samples, were sent for acid-fast bacilli (AFB) smear, MTB culture, Xpert MTB/RIF, and tNGS. Laboratory technicians were blinded to clinical and radiological information. Patients with contraindications to invasive procedures (such as severe coagulopathy or hemodynamic instability precluding thoracentesis or thoracoscopy) were excluded. Individuals unable to provide informed consent were not enrolled.
Patients were diagnosed based on the following criteria: 1) bacteriologically confirmed pleural TB, defined by a positive MTB culture (+), positive molecular tests (+; such as Xpert MTB/RIF and qPCR),11 or histological evidence of necrotizing caseating granulomas with clinical improvement following anti-TB treatment; 2) clinically diagnosed pleural TB, where clinical and radiological signs were suggested of TB, and the patient showed clinical resolution after anti-TB treatment, despite not meeting bacteriological criteria; and 3) non-TB, where there was no evidence of TB, an alternative diagnosis was made.
Lab Examination
Microbiological tests were performed using sputum, pleural fluid, and pleural biopsy specimens, including AFB smear (Auramine O stain), mycobacterial culture (Löwenstein–Jensen medium), Xpert MTB/RIF, and tNGS. For Xpert MTB/RIF, 1 mL specimen was transferred to a pretreatment tube with Xpert sample treatment solution, vortexed, incubated, and loaded into the Xpert cartridge for detection. Results were generated within 2 hours.
Routine laboratory investigations included pleural biochemical and cytological examinations, such as total protein, glucose, lactate dehydrogenase, and adenosine deaminase (ADA) levels. In addition, blood samples were collected for Interferon-Gamma Release Assays (IGRAs).
Pleural biopsy specimens were obtained via medical thoracoscopy when clinically indicated. Histopathological examination was performed to identify features consistent with tuberculosis, including necrotizing granulomatous inflammation.
tNGS
RP100™ Respiratory Pathogen Multiplex Testing Kit (KS608-100HXD96, KingCreate, Guangzhou, China) was used for pathogen detection, which targets 198 pathogens through multiplex PCR and NGS.12 The target selection of the kit accounted for clinically relevant respiratory pathogens supported by clinical expert consensus and authoritative books/literatures.13–16 The primer design method for this kit has been published in a paper authored by Yin et al.12
In this study, multiple specimen types were included, comprising sputum, pleural fluid, and pleural biopsy tissue. All specimens were processed using a standardized workflow to ensure comparability across sample types. For liquid specimens (sputum and pleural fluid), 650 μL of sample was mixed with an equal volume of 0.1 M dithiothreitol for liquefaction, followed by vortexing, incubation, and centrifugation to enrich microbial components. Subsequently, 500 μL of the processed sample was used for nucleic acid extraction. For tissue specimens, samples were rinsed with absolute ethanol and phosphate-buffered saline, followed by mechanical homogenization prior to extraction. Nucleic acids were extracted and purified using the MagPure Pathogen DNA/RNA Kit (R6672-01B; Magen, Guangzhou, China) according to the manufacturer’s instructions. In this study, DNA and RNA were co-extracted and processed together in a unified library preparation workflow, maintaining consistency without the need for separate DNA and RNA inputs. Libraries were constructed according to the manufacturer’s instructions and quantified using Equalbit DNA HS Assay Kit (EQ121, Vazyme, Nanjing, China) on a Qubit™ 3.0/4.0 Fluorometer (EQ121-02, Thermo Fisher Scientific, USA). Sequencing was performed on the KM MiniSeq Dx-CN platform (Illumina, San Diego, USA) with a single-end read length of 100 bp.
Raw sequencing reads were processed using fastp (v0.20.1 for mp-tNGS [multiplex PCR-based tNGS]; v0.23.1 for hc-tNGS [hybrid capture-based tNGS]) for adapter trimming and quality filtering under default parameters (–qualified_quality_phred 20; –length_required 50). High-quality reads from mp-tNGS were aligned to a curated pathogen reference database using Bowtie2 (v2.4.1) in “very-sensitive” mode. For hc-tNGS, host-derived reads were first removed by alignment to the human reference genome (hg38) using Burrows–Wheeler Aligner (BWA, v0.7.17-r1188); the remaining non-human reads were subsequently aligned to the microbial reference database for taxonomic classification. Unless otherwise specified, alignment tools were executed under default settings. Only samples meeting predefined criteria (Q30 score ≥75%, ≥50,000 clean reads) were analyzed. The total read count of each sample and the read pass ratio after Q30 filtering were used as quality control metrics for tNGS. The final sequencing data was compared to a pathogen database for pathogen identification (Supplementary File 1). The detailed bioinformatics pipeline and threshold-setting method can be referenced in the publication of Yin et al.12 A predefined interpretation threshold, established through manufacturer validation and prior analytical studies, was applied. A sample was considered positive when pathogen-specific reads exceeded the predefined cutoff and were absent in negative controls. All sequencing analyses were performed under blinded conditions without access to clinical classification results.
Statistical Analysis
For data analysis, we utilized SPSS Version 25.0 (IBM, Armonk, NY, USA) and MedCalc version 23.1.1 (available at https://www.medcalc.org/). Key metrics including sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV) and accuracy were calculated, with results expressed as percentages with 95% confidence intervals (CI). Continuous data were reported as Mean ± SD, except for non-normally distributed variables (eg, ADA) which were presented as median [interquartile range (IQR)]. Categorical data as cases/percentage [n (N, %)]. Continuous variables were compared using Student’s t-test when normally distributed, while the Mann–Whitney U-test was applied for non-normally distributed continuous variables. Categorical data were compared by Pearson’s χ2 test or Fisher’s exact test. For paired head-to-head comparisons between tNGS and Xpert MTB/RIF performed on the same specimens, McNemar’s test was used to evaluate differences in paired proportions. Agreement beyond chance was quantified using Cohen’s Kappa statistic with standard interpretation thresholds: 0.00–0.20 indicated minimal agreement, 0.21–0.40 slight agreement, 0.41–0.60 moderate agreement, 0.61–0.80 substantial agreement, and 0.81–1.00 almost perfect agreement. A p-value less than 0.05 was considered statistically significant.
Results
A total of 142 cases suspected of pleural TB were included in the study (see Figure 1). Of these, 54/142 (38.0%) were classified as bacteriologically confirmed TB, 80/142 (56.3%) as clinically diagnosed TB, and 8/142 (5.6%) as non-TB. A subset of 105/142 patients (73.9%) underwent paired testing with both tNGS and Xpert MTB/RIF to facilitate a head-to-head comparison. Raw data on patient demographics, and diagnostic outcomes are available in Supplementary Table 1.
 |
Figure 1 Flowchart of patient enrollment and diagnostic evaluation. A total of 142 patients with suspected pleural tuberculosis were included. Among them, 105 patients underwent paired testing with tNGS and Xpert MTB/RIF for head-to-head comparison. Final diagnoses were established based on a composite reference standard. |
As detailed in Table 1, the study cohort exhibited a marked male predominance in both the bacteriologically confirmed (43/54, 79.63%) and clinically diagnosed (65/80, 81.25%) TB groups. Demographic analysis revealed no statistically significant differences in age or gender distribution between the two TB subgroups, nor were there statistically significant differences in IGRA positivity rates (all p > 0.05). However, ADA levels were significantly elevated in patients with bacteriologically confirmed TB (median 45 U/L) compared to those with clinically diagnosed TB (30 U/L) or non-TB (11 U/L). Notably, a significantly higher proportion of bacteriologically confirmed cases presented with ADA levels ≥40 U/L compared to clinically diagnosed cases (60.42% vs 36.62%, p = 0.02). As shown in Table 2, a pleural ADA threshold of ≥40 U/L yielded a sensitivity of 46.22% (95% CI: 37.04%–55.59%; 55/119), a specificity of 100% (95% CI: 63.06%–100%; 8/8), and an overall accuracy of 49.61% (63/127).
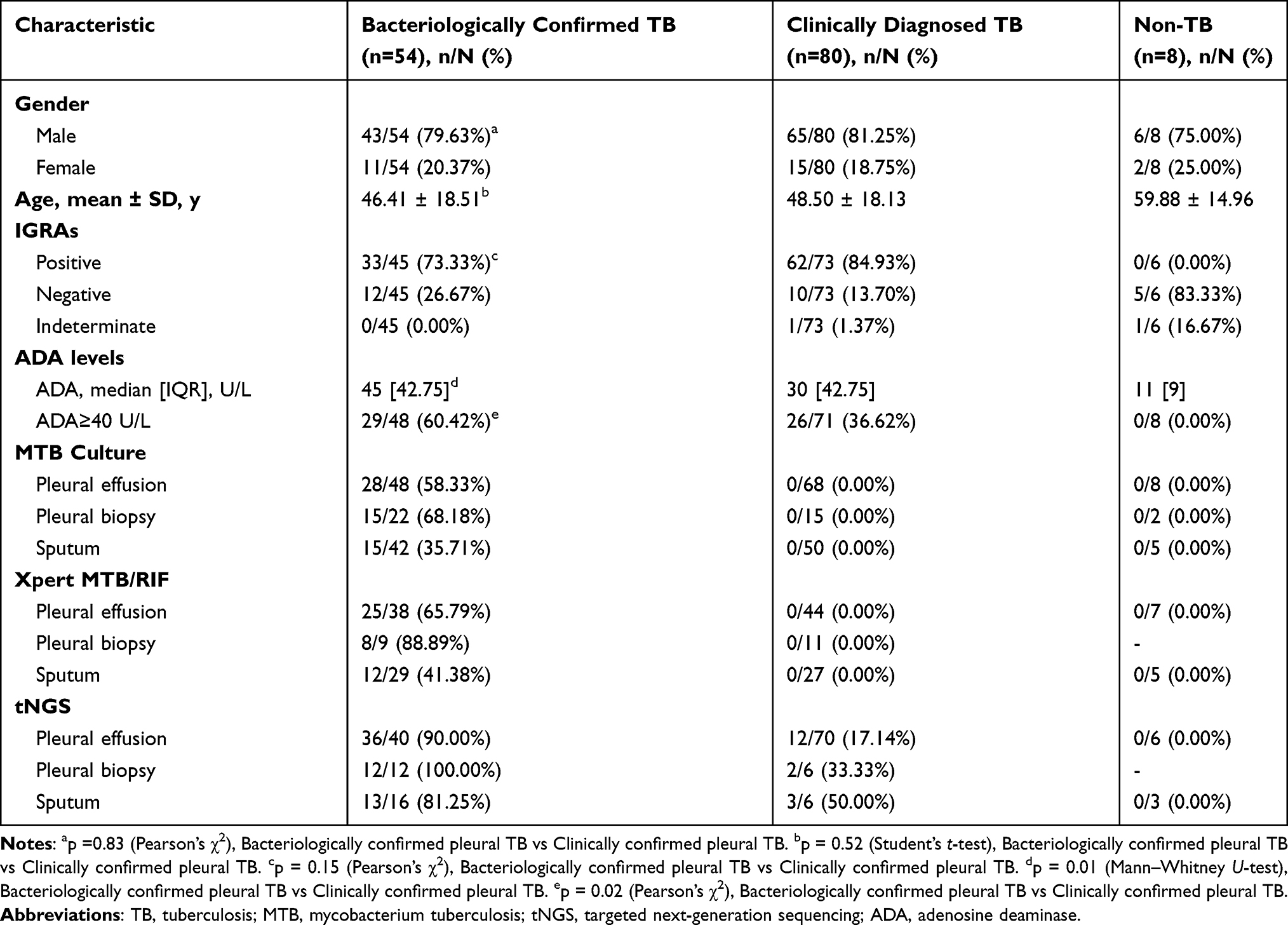 |
Table 1 Basic Characteristics of the Included Patients (n=142) |
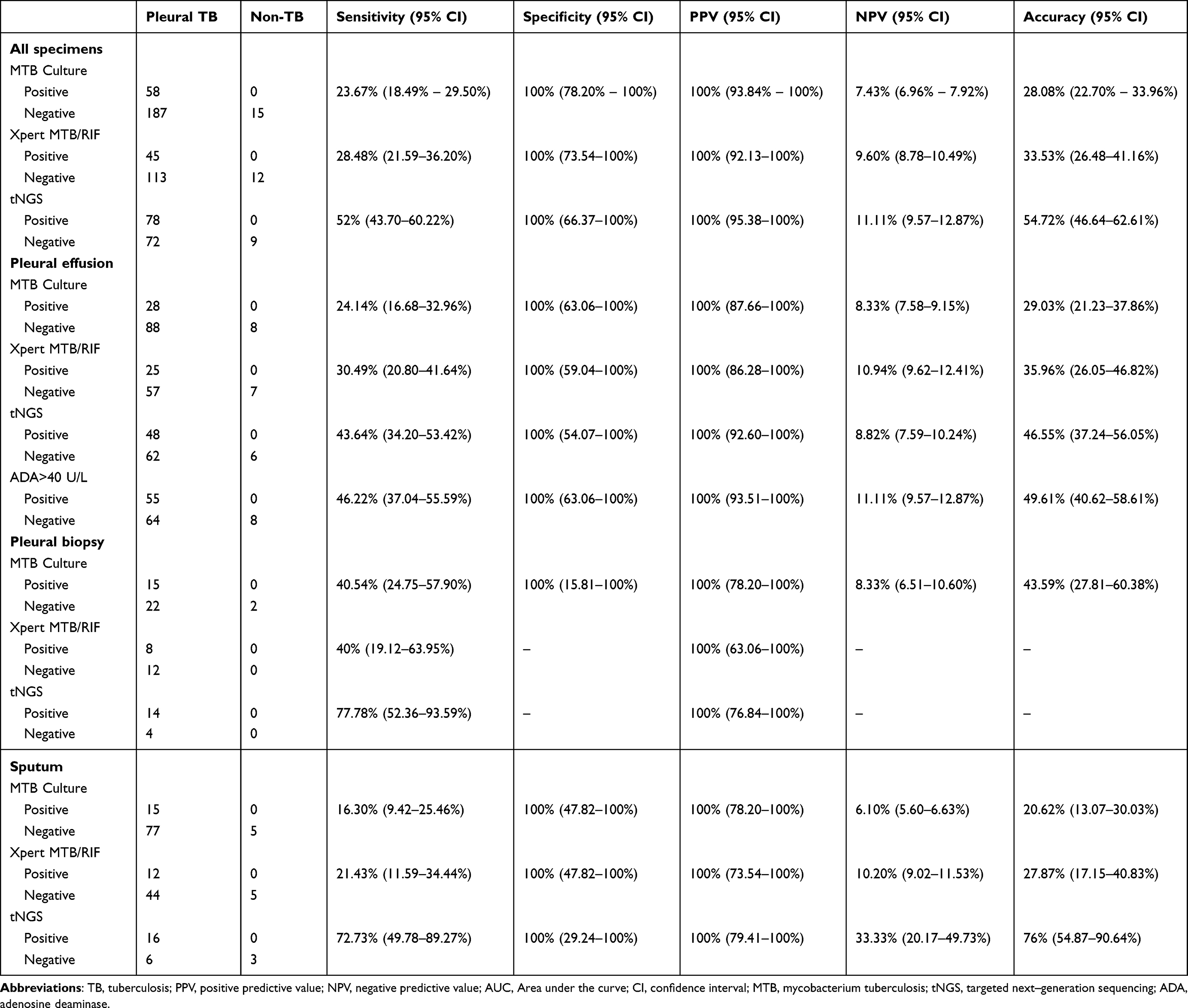 |
Table 2 The Diagnostic Yield of MTB Culture, Xpert MTB/RIF and tNGS for Pleural TB Across Different Specimens |
Diagnostic performance of mycobacterial culture, Xpert MTB/RIF, and tNGS was evaluated across sputum, pleural fluid, and pleural biopsy specimens (Table 2). Across all specimen types, tNGS achieved an observed specificity of 100% (8/8). However, this estimate was derived from a very small non-TB subgroup (n = 8) and is therefore statistically unstable, with wide confidence intervals. Accordingly, this finding should not be interpreted as definitive evidence of perfect specificity, and the possibility of false-positive results cannot be excluded. This advantage was particularly pronounced in sputum samples, where tNGS achieved a sensitivity of 72.73% (16/22) and an accuracy of 76.00% (19/25), numerically surpassing both MTB culture (sensitivity 16.30%, 7/43; accuracy 20.62%, 20/97) and Xpert MTB/RIF (sensitivity 21.43%, 9/42; accuracy 27.87%, 17/61). Furthermore, sputum tNGS yielded the highest NPV (33.33%, 3/9) among the sputum-based tests. A similar trend was observed in pleural fluid specimens, where tNGS displayed a sensitivity of 43.64% (48/110) and accuracy of 46.55% (54/116). While this outperformed MTB culture and Xpert MTB/RIF, it was slightly lower than the sensitivity provided by the ADA ≥40 U/L cutoff (46.22%, 50/108). Regarding pleural biopsies, tNGS achieved the highest sensitivity among all evaluated methods (77.78%, 14/18).
In the paired head-to-head cohort of 105 patients, tNGS demonstrated a superior overall diagnostic yield compared to Xpert MTB/RIF (Table 3). tNGS identified 26 positive cases that were missed by Xpert MTB/RIF, whereas no cases were Xpert-positive/tNGS-negative. This discrepancy was statistically significant (McNemar’s test, p < 0.01), with moderate agreement between the assays (Kappa = 0.49, p < 0.01). Of particularly clinical significance was the performance in the MTB culture-negative subgroup. In this challenging cohort, tNGS detected 24 cases (40.0%, 24/60) compared to only 6 (10.0%, 6/60) by Xpert MTB/RIF. Crucially, tNGS identified 18 cases that were negative by both MTB culture and Xpert MTB/RIF (p < 0.01). The superiority of tNGS was statistically significant in pleural fluid samples (p < 0.01). However, in sputum samples, despite the substantial difference in absolute sensitivity observed in the overall cohort (Table 2), the difference in the paired subset did not reach statistical significance (p = 0.16), likely due to the limited sample size (n=17). Similarly, in pleural biopsy samples, while agreement was substantial (Kappa = 0.78), the difference in yield was not statistically significant (p = 1.00).
 |
Table 3 The Comparison of Diagnostic Performance Between Xpert MTB/RIF and tNGS for Pleural TB |
Discussion
Pleural TB remains a diagnostic challenge due to its non-specific clinical presentation and the paucibacillary nature of pleural effusion, which often leads to false negatives with conventional diagnostic techniques. The present study demonstrates that tNGS provides meaningful incremental diagnostic yield over mycobacterial culture and Xpert MTB/RIF, particularly in culture-negative and Xpert-negative disease. The principal advantage of tNGS was its capacity to increase etiological confirmation among patients who would otherwise remain microbiologically unconfirmed. Importantly, enhanced diagnostic sensitivity does not automatically translate into clinical utility. The primary value of tNGS lies in reducing diagnostic uncertainty in patients with persistently high clinical suspicion despite negative initial microbiological testing. Accordingly, its role should be interpreted within a structured diagnostic algorithm, functioning as an adjunctive second-line assay rather than a universal frontline replacement.
A striking observation in our study was the high sensitivity of tNGS in sputum specimens (72.73% in the overall cohort), suggesting its potential utility as a non-invasive surrogate marker for pleural TB. This aligns with recent literature indicating that tNGS can detect lower concentrations of TB DNA compared to culture or smear microscopy, thereby facilitating earlier diagnosis.9,17,18 However, it is critical to interpret the statistical comparisons with caution. While the absolute sensitivity of sputum tNGS appeared much higher than Xpert in the overall analysis, the paired head-to-head comparison did not reach statistical significance (p = 0.16). This lack of significance is attributable to the small sample size in the paired sputum subgroup. Nevertheless, the trend strongly suggests that with a larger cohort, the superior analytical sensitivity of tNGS in sputum would likely be statistically confirmed. While tNGS demonstrated superior overall performance, its sensitivity in pleural fluid (43.64%) was notably lower than in sputum. This discrepancy suggests that diagnostic accuracy is heavily influenced by sample type and the local biological environment. This reduced sensitivity in pleural fluid, primarily due to the low mycobacterial load in this paucibacillary condition, was consistent with prior studies, which also indicated that PCR inhibitors or limited sample volumes may further compromise accuracy in pleural fluid.19 Supporting evidence from the literature20 demonstrated that tNGS achieved its highest sensitivity in sputum and pus samples at 80.0% (4/5), while sensitivity in pleural fluid decreased to 50.0% (2/4). However, additional research is needed to further validate these findings and elucidate the factors influencing tNGS performance across diverse specimen types. These results underscore the importance of utilizing a multi-modal approach, combining molecular, microbiological, and clinical data, to improve the accuracy of pleural TB diagnosis. ADA is widely recognized as a valuable screening tool, our study corroborates the utility of the standard cutoff (>40 U/L), which yielded a sensitivity of 46.22% and marginally higher than that of tNGS in pleural fluid (43.64%). While ADA serves as an excellent rule-out or screening tool, it should be interpreted in conjunction with other clinical assessments to ensure a comprehensive diagnosis.
The discordance observed in our paired analysis, specifically the 26 cases detected by tNGS but missed by Xpert MTB/RIF, underscores the complementary nature of these molecular tools. The low Kappa coefficient and significant McNemar’s test results (p < 0.01) indicate that these tests are not interchangeable. tNGS was particularly effective in rescuing diagnoses in culture-negative patients, identifying 40% of this difficult-to-diagnose cohort compared to only 10% by Xpert. This suggests a paradigm shift in diagnostic strategy: no single method is sufficient for all pleural TB cases. An integrated multi-modal approach is necessary, combining the broad screening capability of ADA, the rapidity of Xpert, and the high analytical sensitivity of tNGS. From a health economics and implementation perspective, the choice of test involves balancing cost, speed, and depth. In China, the per-sample costs of tNGS and Xpert MTB/RIF are relatively comparable (USD 82 vs USD 64, respectively), though recent price reductions in Xpert Ultra cartridges may widen this gap. Logistically, Xpert MTB/RIF offers a rapid (~2 hours), automated, sample-to-answer workflow ideal for frontline screening. In contrast, tNGS requires a longer turnaround (~48 hours), specialized infrastructure, and bioinformatic expertise. However, tNGS offers a lower limit of detection (LOD) and the ability to detect mixed infections. Collectively, these data support a tiered diagnostic algorithm in which Xpert MTB/RIF remains the primary rapid molecular assay, while tNGS is reserved as a second-line investigation for diagnostically uncertain presentations, particularly patients who are Xpert-negative and culture-negative despite high clinical suspicion, or those with extrapulmonary disease in which bacillary burden falls below the threshold of conventional PCR.9,20 When a non-invasive sample is available, sputum may be prioritized for tNGS because it showed higher sensitivity than pleural fluid in our cohort, although this observation requires confirmation in larger paired datasets. Pleural biopsy remains important in unresolved cases requiring histopathological or additional microbiological confirmation. Given the observational design of this study and incomplete parallel testing across specimen types, this proposed pathway should be interpreted as a conceptual framework rather than a definitive clinical algorithm.
Several limitations merit consideration. First, key subgroups were small, particularly pleural biopsy specimens and the paired sputum subset (n = 17), limiting statistical power for specimen-specific paired analyses. Consequently, some observed differences may represent type II error rather than true equivalence. The small non-TB subgroup (n = 8) also resulted in imprecise specificity estimates with wide confidence intervals and limited ability to detect false positives, a relevant concern for sequencing-based assays susceptible to contamination and low-level signal detection. Second, not all participants underwent complete testing across all specimen types. As a prospective real-world study, incomplete parallel testing due to specimen availability may have introduced bias in performance estimates. Third, the use of a composite reference standard may have introduced incorporation or verification bias, particularly in clinically diagnosed cases. Fourth, Xpert MTB/RIF rather than the more sensitive Xpert Ultra was used as the comparator; thus, the incremental diagnostic yield of tNGS may be overestimated relative to Ultra. Fifth, predictive values should be interpreted in the context of disease prevalence, as the TB-enriched cohort may inflate PPV and underestimate NPV. Finally, this single-center study in a high-burden setting may limit generalizability, and performance in HIV-positive populations could not be assessed. Multicenter studies across diverse settings are warranted.
Conclusion
tNGS demonstrated incremental diagnostic value over Xpert MTB/RIF and mycobacterial culture in pleural tuberculosis, particularly in paired analyses and in patients with culture-negative or Xpert-negative disease. In matched comparisons, tNGS identified additional microbiologically confirmed cases missed by Xpert MTB/RIF, supporting its role in reducing diagnostic uncertainty in paucibacillary conditions. These findings should be interpreted with caution given the single-center design, small non-TB group, and limited sample sizes in key paired subgroups, which constrain statistical precision and generalizability. Notably, although higher absolute sensitivity was observed in sputum, the paired comparison did not reach statistical significance, likely reflecting limited statistical power rather than true equivalence. Overall, the results support a tiered diagnostic strategy in which tNGS serves as a complementary second-line assay, particularly in patients with negative initial molecular and culture-based testing, rather than as a replacement for frontline diagnostics.
Funding
Supported by the Development Plan of Medicine and Health Science and Technology of Shandong Province (Grant No. 202303021558) and by the Medical and Health Science and Technology Project (Healthcare Project) of Shandong Province (Grant No. 2025BJ000027).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hassan M, Patel S, Sadaka AS, Bedawi EO, Corcoran JP, Porcel JM. Recent insights into the management of pleural infection. Int J Gen Med. 2021;14:3415–11. doi:10.2147/ijgm.S292705
2. Shaw JA, Diacon AH, Koegelenberg CFN. Tuberculous pleural effusion. Respirology. 2019;24(10):962–971. doi:10.1111/resp.13673
3. Porcel JM. Tuberculous pleural effusion. Lung. 2009;187(5):263–270. doi:10.1007/s00408-009-9165-3
4. Friedrich SO, von Groote-Bidlingmaier F, Diacon AH. Xpert MTB/RIF assay for diagnosis of pleural tuberculosis. J Clin Microbiol. 2011;49(12):4341–4342. doi:10.1128/jcm.05454-11
5. Denkinger CM, Schumacher SG, Boehme CC, Dendukuri N, Pai M, Steingart KR. Xpert MTB/RIF assay for the diagnosis of extrapulmonary tuberculosis: a systematic review and meta-analysis. Eur Respir J. 2014;44(2):435–446. doi:10.1183/09031936.00007814
6. Sehgal Inderpaul S, Dhooria S, Aggarwal Ashutosh N, Behera D, Agarwal R. Diagnostic performance of Xpert MTB/RIF in tuberculous pleural effusion: systematic review and meta-analysis. J Clin Microbiol. 2016;54(4):1133–1136. doi:10.1128/jcm.03205-15
7. Meldau R, Peter J, Theron G, et al. Comparison of same day diagnostic tools including Gene Xpert and unstimulated IFN-γ for the evaluation of pleural tuberculosis: a prospective cohort study. BMC Pulm Med. 2014;14(1):58. doi:10.1186/1471-2466-14-58
8. Rufai SB, Singh A, Kumar P, Singh J, Singh S. Performance of Xpert MTB/RIF assay in diagnosis of pleural tuberculosis by use of pleural fluid samples. J Clin Microbiol. 2015;53(11):3636–3638. doi:10.1128/JCM.02182-15
9. Zhang H, Dai X, Hu P, et al. Comparison of targeted next-generation sequencing and the Xpert MTB/RIF assay for detection of Mycobacterium tuberculosis in clinical isolates and sputum specimens. Microbiol Spectr. 2024;12(5):e04098–23. doi:10.1128/spectrum.04098-23
10. Schwab TC, Perrig L, Göller PC, et al. Targeted next-generation sequencing to diagnose drug-resistant tuberculosis: a systematic review and meta-analysis. Lancet Infect Dis. 2024;24(10):1162–1176. doi:10.1016/s1473-3099(24)00263-9
11. Committee WGAbtGR. WHO Consolidated Guidelines on Tuberculosis: Module 3: Diagnosis – Rapid Diagnostics for Tuberculosis Detection. World Health Organization© World Health Organization 2024.; 2024.
12. Yin Y, Zhu P, Guo Y, et al. Enhancing lower respiratory tract infection diagnosis: implementation and clinical assessment of multiplex PCR-based and hybrid capture-based targeted next-generation sequencing. EBioMedicine. 2024;107:105307. doi:10.1016/j.ebiom.2024.105307
13. Kasper DL, Fauci AS. Harrison’s Infectious Diseases, 3e. McGraw-Hill Education; 2017.
14. Huang XB, Yuan L, Ye CX, et al. Epidemiological characteristics of respiratory viruses in patients with acute respiratory infections during 2009-2018 in southern China. Int J Infect Dis. 2020;98:21–32. doi:10.1016/j.ijid.2020.06.051
15. Li ZJ, Zhang HY, Ren LL, et al. Etiological and epidemiological features of acute respiratory infections in China. Nat Commun. 2021;12(1):5026. doi:10.1038/s41467-021-25120-6
16. Liu YN, Zhang YF, Xu Q, et al. Infection and co-infection patterns of community-acquired pneumonia in patients of different ages in China from 2009 to 2020: a national surveillance study. Lancet Microbe. 2023;4(5):e330–e339. doi:10.1016/s2666-5247(23)00031-9
17. Wu X, Tan G, Sun C, et al. Targeted next-generation sequencing - a promising approach in the diagnosis of Mycobacterium tuberculosis and drug resistance. Infection. 2024. doi:10.1007/s15010-024-02411-w
18. Kambli P, Ajbani K, Kazi M, et al. Targeted next generation sequencing directly from sputum for comprehensive genetic information on drug resistant Mycobacterium tuberculosis. Tuberculosis. 2021;127:102051.
19. Christopher DJ, Schumacher SG, Michael JS, et al. Performance of Xpert MTB/RIF on pleural tissue for the diagnosis of pleural tuberculosis. Eur Respir J. 2013;42(5):1427–1429. doi:10.1183/09031936.00103213
20. Zheng H, Yang H, Wang Y, et al. Diagnostic value of tNGS vs Xpert MTB/RIF in childhood TB. Heliyon. 2024;10(1):e23217. doi:10.1016/j.heliyon.2023.e23217
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.