Back to Journals » Patient Preference and Adherence » Volume 18
Comparison of Treatment Patterns in Patients with Migraine Initiating Calcitonin Gene-Related Peptide Monoclonal Antibodies: A Retrospective Real-World US Study
Authors Varnado OJ, Brady BL, Zagar AJ, Robles YP, Hoyt M
Received 29 August 2023
Accepted for publication 18 December 2023
Published 9 January 2024 Volume 2024:18 Pages 69—88
DOI https://doi.org/10.2147/PPA.S437396
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Oralee J Varnado,1 Brenna L Brady,2 Anthony J Zagar,1 Yvonne P Robles,2 Margaret Hoyt1
1Eli Lilly and Company, Indianapolis, IN, USA; 2Merative, Ann Arbor, MI, USA
Correspondence: Oralee J Varnado
Value, Evidence, and Outcomes, Eli Lilly and Company, Lilly Corporate Center, 893 Delaware Street, Indianapolis, IN, 46285, USA
, Tel +1 317 277 0599
, Email [email protected]
Background: Calcitonin gene-related peptide monoclonal antibodies (CGRP mAbs) are indicated for migraine prevention in the United States. Limited data comparing real-world treatment patterns for CGRP mAbs are available.
Objective: To compare the treatment patterns among patients with migraine initiating galcanezumab, fremanezumab, and erenumab.
Methods: This retrospective study included adult patients with one or more claims for a self-injectable CGRP mAb (galcanezumab, fremanezumab, or erenumab), with continuous enrollment in medical and pharmacy benefits for 12 months pre-index and 6 and 12 months post-index using MerativeTM MarketScan® Commercial and Medicare databases from May 2017 through March 2021. Propensity-score matching was used to address confounding by observed covariates. Outcomes analyzed included proportion of days covered (PDC), medication-possession ratio (MPR), persistence (≤ 60-day gap), treatment discontinuation, and switch to a non-index drug. Descriptive X2 and t-test analyses were conducted.
Results: At the 12-month follow-up, matched galcanezumab and fremanezumab cohorts each comprised 2674 patients and the galcanezumab and erenumab cohorts 3503 each. The mean (SD) PDC and MPR were both 0.6 (0.3) across all cohorts. Based on PDC ≥ 0.80 and MPR ≥ 0.80, a greater proportion of galcanezumab vs fremanezumab (46.2% vs 43.7%, p=0.053; 46.8% vs 44.3%, p=0.053) and galcanezumab vs erenumab (46.2% vs 44%, p=0.156; 46.7% vs 44.5%, p=0.262), respectively, initiators were adherent. Compared to galcanezumab, fremanezumab (248.0 days vs 236.5 days, p=0.001), and erenumab (247.8 days vs 241.7 days, p=0.061) initiators had lower mean persistence. Galcanezumab initiators were less likely to discontinue treatment than fremanezumab (47.8% vs 51.7%, p=0.005) and erenumab (47.7% vs 50.2%, p=0.040) initiators. Across cohorts, most switchers initiated onabotulinum toxin A as subsequent treatment. Similar results were observed for 6-month follow-up cohorts.
Conclusion: Patients with migraine who initiated treatment with galcanezumab showed higher persistence and lower treatment discontinuation rates than those initiating either fremanezumab or erenumab.
Plain Language Summary: What was known before? Calcitonin gene-related peptide monoclonal antibodies (CGRP mAbs) are medicines developed for migraine prevention. CGRP mAbs bind to the CGRP ligand or receptor and limit pain associated with migraine attacks. Currently, three self-injectable CGRP mAbs are approved for prevention: erenumab, fremanezumab, and galcanezumab. Use of erenumab, fremanezumab, and galcanezumab can slow or stop migraine-related symptoms and reduce migraine-related disability.
What does this study add? This study describes how migraine medications are used in the US by patients with migraine who started using galcanezumab, fremanezumab, or erenumab for migraine treatment. Over a period of 12 months, patients who started treatment for migraine with galcanezumab were more likely to continue their treatment than those who started using either fremanezumab or erenumab. At 12 months, fewer patients who started galcanezumab were likely to discontinue their treatment than patients who started using either fremanezumab or erenumab. Among patients who discontinued and switched, most patients switched to Botox A, a non-CGRP treatment. Among patients who switched to a different CGRP mAb, most patients in the fremanezumab and erenumab groups switched to galcanezumab, while most patients in the galcanezumab group switched to erenumab.
Interpretation: These findings suggest that patients remained on galcanezumab longer and were less likely to discontinue.
Keywords: CGRP mAb, erenumab, fremanezumab, galcanezumab, treatment patterns, migraine
Introduction
Migraine is a neurological disorder that negatively impacts health-related quality of life.1 Each migraine attack can last 4–72 hours accompanied by photophobia, phonophobia, nausea, and/or vomiting.2 Migraine is also a burdensome disease that impacts patients’ social and family relationships, along with work and school activities.3,4 In 2019, there were 1.1 billion (0.98–1.3) prevalent cases of migraine worldwide,5 and overall prevalence in the US was 12% (18% of women, and 6% of men).6 Migraine is classified as either episodic (EM; ≤14 headache days per month) or chronic (CM; ≥15 headache days per month for >3 months).2 The use of new-generation migraine-specific drugs, the monoclonal antibodies against the calcitonin gene-related peptide or its receptor (CGRP mAbs), have been proven to be safe and effective in the prevention of EM and CM.7–9 The American Headache Society (AHS) position statement recommends initiating CGRP mAbs in patients with low- (4–7 monthly headache days with at least moderate disability defined as migraine disability assessment >11 and Headache Impact Test 6 >50) or high-frequency (8–14 monthly headache days) EM or CM, and intolerance or inadequate response to at least two preventive migraine medications (for CM, intolerance and inadequate response is to a minimum of two quarterly injections of onabotulinum toxin A).10
Clinical data from the three self-injectable CGRP mAbs (galcanezumab, fremanezumab, and erenumab) have not only shown reduction in migraine symptoms7–9 but also disease burden and related disability.11–13 Following their regulatory approval, real-world evidence for these CGRP mAbs has demonstrated similar effectiveness, and data from the randomized clinical trials have shown fewer risks of adverse events compared with traditional oral medications.14,15 However, real-world evidence comparing treatment patterns of galcanezumab, fremanezumab, and erenumab is limited.
Little is currently known about how the three self-injectable CGRP mAbs differ in real-world settings. To the best of our knowledge, there have been no published reports directly comparing real-world outcomes of galcanezumab vs fremanezumab or erenumab among US patients. The current study aimed to describe patient demographics and clinical characteristics and assess treatment patterns (including adherence, persistence, discontinuation, and switching) of migraine medication prescription use among US patients with migraine who initiated galcanezumab, fremanezumab, or erenumab. Results of this study may help in understanding the current population using these treatments, and the associated treatment patterns may help providers and their patients make informed decisions on the choice of therapy.
Methods
Study Design and Data Source
This US retrospective, observational study compared treatment patterns between the self-injectable CGRP mAbs: galcanezumab vs fremanezumab and galcanezumab vs erenumab. The study was conducted using administrative claims data from the MerativeTM MarketScan® Commercial and Medicare Databases from May 1, 2017 through March 31, 2021 (study period). The index date was defined as the date of a patient’s first prescription fill for a self-injectable CGRP mAb between May 1, 2018 and September 30, 2020 (index period).
The MarketScan Commercial Claims and Encounters database contains inpatient, outpatient, and outpatient pharmacy claims from recipients of employer-sponsored health care. This also includes a variety of fee-for-service and managed-care health plans, including exclusive provider organizations, PPOs, POS plans, indemnity plans, and HMOs. The MarketScan Medicare database contains health-care experience (both medical and pharmaceutical) of retirees with Medicare supplemental insurance paid for by employers. Both the Medicare-covered portion of payment (represented as coordination of benefits amount, or COB) and the employer-paid portion are included in this database. Both databases provide detailed cost, use, and outcome data for health-care services performed in both inpatient and outpatient settings. All records from the Merative MarketScan Commercial and Medicare databases are deidentified and fully compliant with US patient confidentiality requirements, including the Health Insurance Portability and Accountability Act of 1996. Since the study used only deidentified patient records, neither institutional review board approval nor patient informed consent to conduct this study was required.
Patient Population
Adult patients (≥18 years) with one or more claims for galcanezumab, fremanezumab, or erenumab between May 1, 2018 and September 30, 2020 were included. Included patients were assigned to one of three cohorts based on the CGRP mAb initiated on the index date: galcanezumab, fremanezumab, or erenumab. Patients were required to have ≥12 months of continuous enrollment in medical and pharmacy benefits prior to the index date (baseline), and patients with continuous enrollment 12 of months post-index (12-month follow-up) were identified (Figure 1). Similarly, patients with continuous enrollment of 6 months post-index (6-month follow-up) were also identified (Supplementary Figure 1).
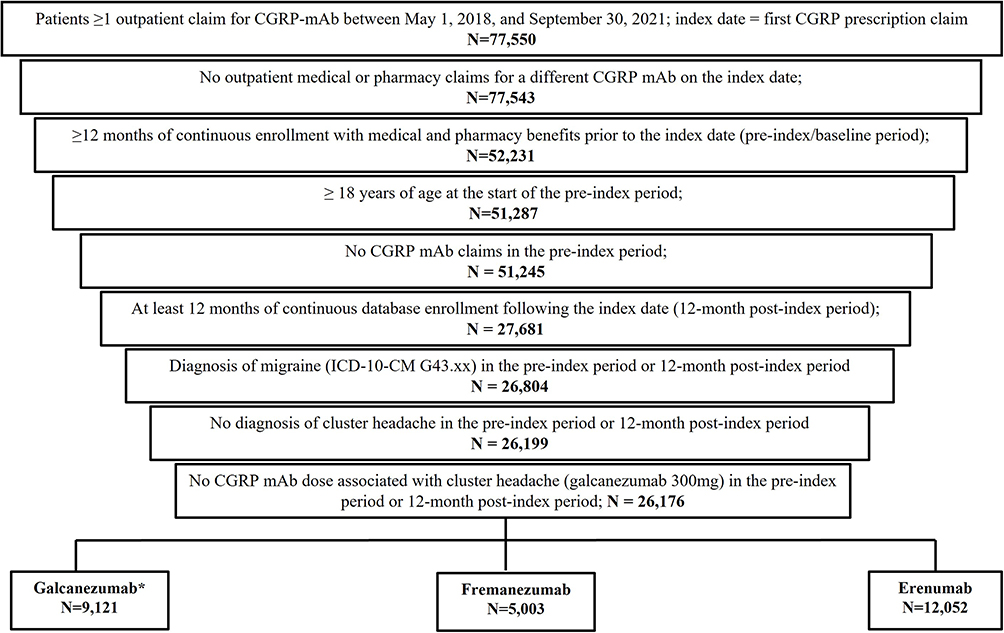 |
Figure 1 Patient disposition for the 12-month follow-up cohort. *Reference cohort. |
Selected patients were required to have one or more nondiagnostic claims in accordance with the International Classification of Diseases, 10th revision — clinical modification (ICD-10-CM) diagnosis of migraine (ICD-10-CM G43.xx) criteria during the study period. Patients with one or more claims with an ICD-10-CM diagnosis for cluster headache (ICD-10-CM G44.0x) or pharmacy claim for a medication dose associated with cluster headache during the study period were excluded, as were patients with claims for CGRP mAbs in the baseline period or claims for more than one CGRP mAb on the index date.
Study Outcomes
Baseline Demographics and Clinical Characteristics
Demographic characteristics were recorded on the index date and included age, sex, geographic region, insurance plan type, payer, and index year (2018, 2019, 2020). Clinical characteristics were measured during the pre-index period and included the Deyo Charlson Comorbidity Index (DCCI), comorbid medical conditions, and preventive and acute migraine medications.
Preventive and Acute Migraine Medications
Baseline and follow-up preventive and acute medications for migraine based on the 2021 AHS consensus statement were reported.16 Preventive and acute medications for migraine included medications with established efficacy or probable efficacy (Supplementary Table 1). Medications with one or more outpatient prescription claims or one or more medical claims with a procedure code for the administered medication were identified. Patients with claims for specific drug categories and number of unique preventive and acute treatments for migraine per patient in each cohort during baseline and follow-up periods were analyzed.
Treatment-utilization patterns meeting the following thresholds were defined as acute medication overuse.17,18
- Opioid use for 8+ days/month
- Barbiturate use for 5+ days/month
- Triptan use for 8+ days/month, or
- Any combination of ergotamine, triptans, analgesics, and/or opioids on 10+ days/month without overuse of a single class.
Medication overuse was calculated as the total days’ supply for each class medication class over the full follow-up-period.
Index Medication Adherence, Persistence, Discontinuation, and Switching
Treatment patterns for galcanezumab, fremanezumab, and erenumab were measured during the follow-up period. Treatment adherence was measured using the proportion of days covered (PDC) and medication-possession ratio (MPR).
- PDC was calculated as days covered or number of days exposed to index drug in the follow-up period divided by the duration of the follow-up period, regardless of discontinuation.
- MPR was capped at 100% and calculated as the ratio of sum of days’ supply from all prescriptions during the follow-up period divided by total number of days in the follow-up period.
- PDC and MPR ≥80% were considered treatment-adherent.
Treatment persistence was defined as number of days of continuous therapy from the index date until the end of follow-up, allowing for a maximum fixed gap between fills of 60 days. Discontinuation of index medication was defined as failure to refill the index medication within 60 days after the depletion of supply from previous fills. Switching was defined as initiation of any preventive migraine drug other than the index preventive drug following discontinuation of the index drug.
Statistical Analyses
Propensity-Score Matching
Propensity score matching was used to adjust for differences in baseline demographic and clinical characteristics that might have confounded the association between exposure and outcomes.19 Differences were assessed using a standardized difference. A standardized difference >10% in absolute value was considered for potential imbalances. Galcanezumab served as the reference treatment group, with match ratios of 2:1 and 1:1 to the fremanezumab and erenumab treatment groups, respectively. The propensity scores were estimated using a logistic regression model with the covariates of age, region, index quarter, index year, use of onabotulinum toxin A in the baseline period, evidence of any acute medication overuse in the baseline period, number of acute migraine medication classes in the baseline period, and number of preventive migraine medication classes in the baseline period.
Significance Level, Hypothesis Testing, and Multiplicity Adjustment
Statistical analyses were planned with an a priori significance level set at α=0.05. Descriptive analyses were performed pre- and post-matching and are reported as means, SD, frequencies, and percentages. Differences between CGRP mAb cohorts were assessed using X2 tests for categorical variables and t-tests or nonparametric Wilcoxon rank-sum tests (in cases where normality assumptions were not met) for continuous variables.
Index treatment persistence during the follow-up period was depicted using Kaplan–Meier curves, and differences between groups were assessed using a log-rank test. Patients who did not discontinue the index drug were censored at the end of follow-up. Statistical analyses were performed using WPS Analytics 4.1 (World Programming) and R (R Core Team [2020]).
Results
Baseline Demographics and Clinical Characteristics
Pre-matching Results
At the 12-month follow-up, a total of 26,176 patients were identified and grouped into three cohorts based on the index CGRP mAb: galcanezumab cohort (n=9121), fremanezumab cohort (n=5003), and erenumab cohort (n=12,052). Before propensity-score matching, all three cohorts predominantly consisted of female patients (range 86.3–87.7%), with similar clinical characteristics (Table 1 and Table 2). Patients on fremanezumab (44.4 years, standardized difference 5.07) and erenumab (44.7 years, standardized difference 8.28) were slightly older than those on galcanezumab (43.8 years; Table 1 and Table 2). Across all cohorts, triptans (range 67%–69.2%), nonopioid analgesics (range 62.6%–63.9%), and opioids (range 46.1%–48.5%) were the most commonly prescribed acute medication classes. The most commonly prescribed preventive medications were antiepileptic drugs (range 39.2%–9.9%) and antidepressants (range 23.7%–24.4%).
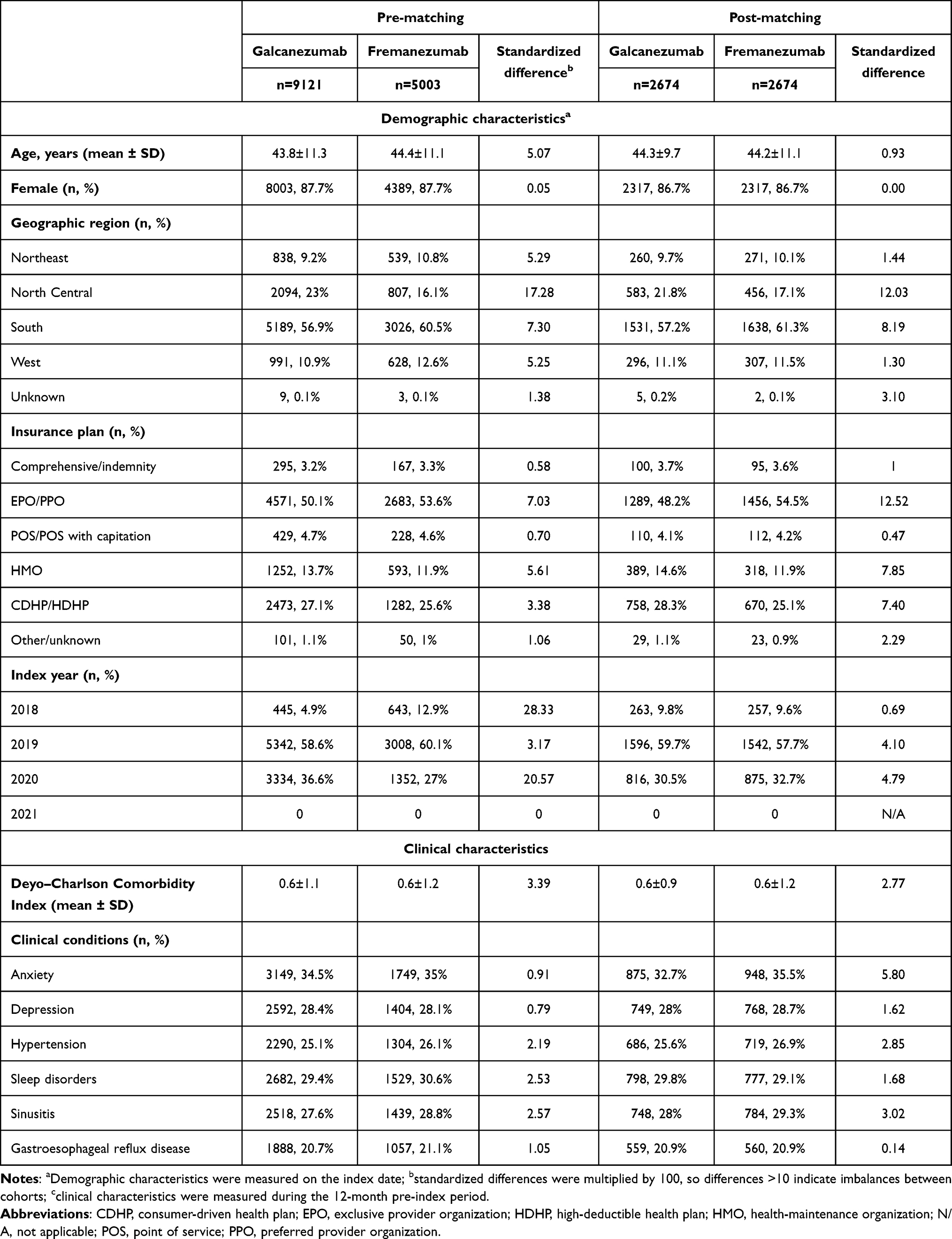 |
Table 1 Patient demographics and baseline clinical characteristics: galcanezumab versus fremanezumab |
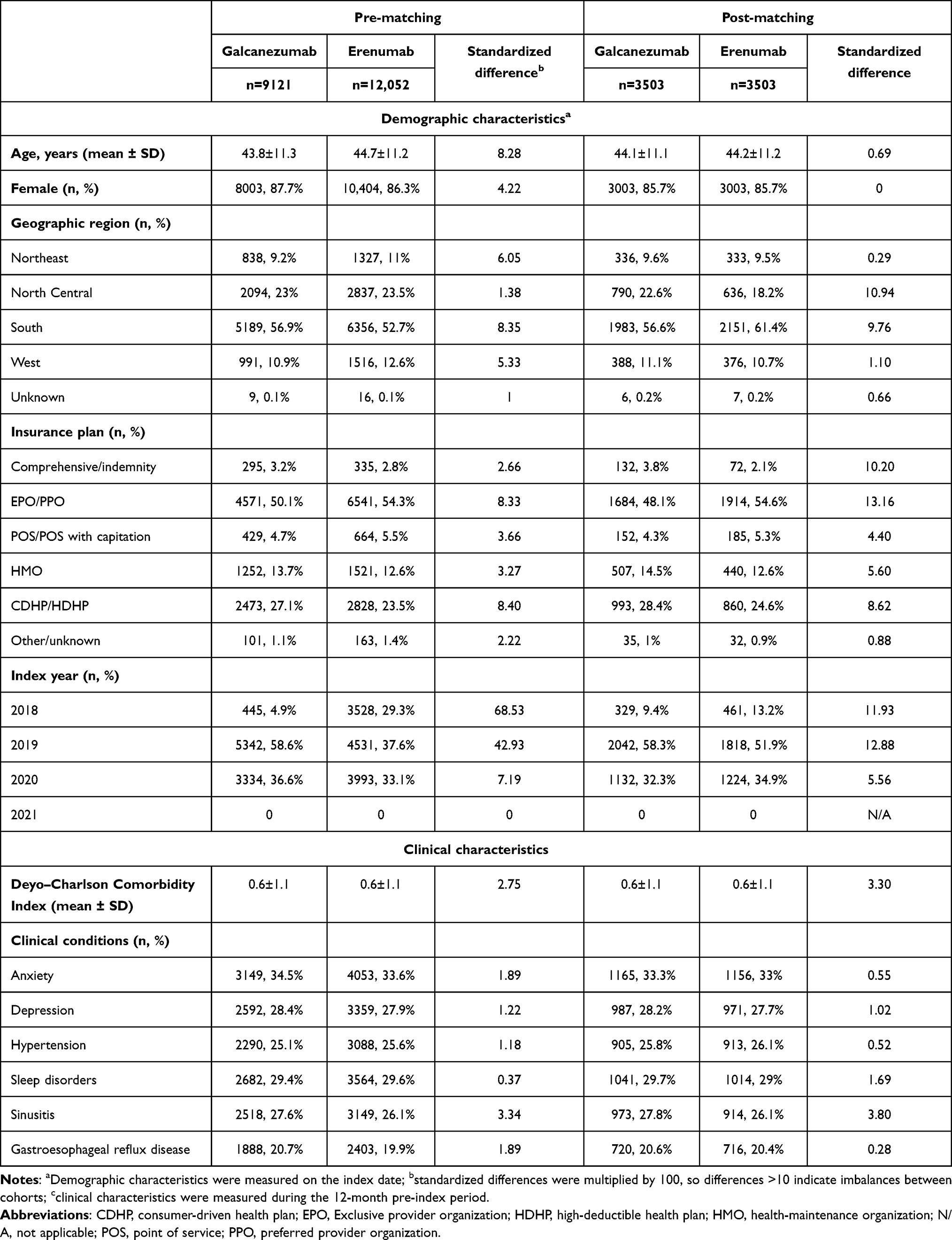 |
Table 2 Patient demographics and baseline clinical characteristics: galcanezumab versus erenumab |
Post-matching Results
After 2:1 and 1:1 propensity-score matching, respectively, the galcanezumab and fremanezumab matched cohorts each included 2674 patients, and the galcanezumab and erenumab cohorts included 3503 patients (Figure 1). In these matched cohorts, the majority were female (range 85.7–86.7%) with a mean age of 44 years (Table 1 and Table 2). Most patients resided in the South (range 56.6–61.4%) or North Central (range 17.1–22.6%) region of the US. Most patients (range 51.9%–59.7%) initiated their index CGRP mAb in 2019. The top-three comorbid conditions observed were anxiety (range 32.7%–35.5%), sleep disorders (range 29.1%–29.8%), and depression (range 27.7%–28.7%). Overall, the matched cohorts were well balanced.
Baseline and Follow-Up Preventive and Acute Medications Used for Migraine in the Matched Population
Baseline Results: Galcanezumab vs Fremanezumab
During the baseline period, patients initiating galcanezumab or fremanezumab received a mean of 1.1 unique preventive drug classes for migraine. Antiepileptic drugs and antidepressants were the most prescribed preventive drug classes in the galcanezumab (40.9% and 23.8%) and fremanezumab (39.9% and 23.7%) cohorts. Specifically, topiramate and amitriptyline were the most prescribed agents in these drug classes for the galcanezumab (38.3% and 15.9%) and fremanezumab (37% and 14.9%) cohorts (data not shown). A significantly greater proportion of galcanezumab vs fremanezumab initiators received onabotulinum toxin A (17.1% vs 14.9%, p=0.031). Patients in both cohorts received mean 2.2 unique acute drug classes for migraine, and similar proportions of galcanezumab vs fremanezumab patients received the following acute medications: triptans (68.1% vs 66.6%), opioids (46.4% vs 48.6%), antiemetics (32.8% vs 33.1%), and NSAIDs with established efficacy (53.4% vs 51.5%) (Table 3). Acute medication overuse was observed in a similar proportion of patients initiating galcanezumab vs fremanezumab (56% vs 58%, Table 4). Overuse was primarily attributed to possession of a combination of triptans, analgesics, ergotamines, and/or opioids. A significantly lower proportion of galcanezumab vs fremanezumab initiators had combination overuse (47% vs 49.9%, p=0.035). Additionally, a significantly lower proportion of galcanezumab vs fremanezumab initiators were observed to have opioid overuse (9.9% vs 12.5%, p=0.002; Table 4).
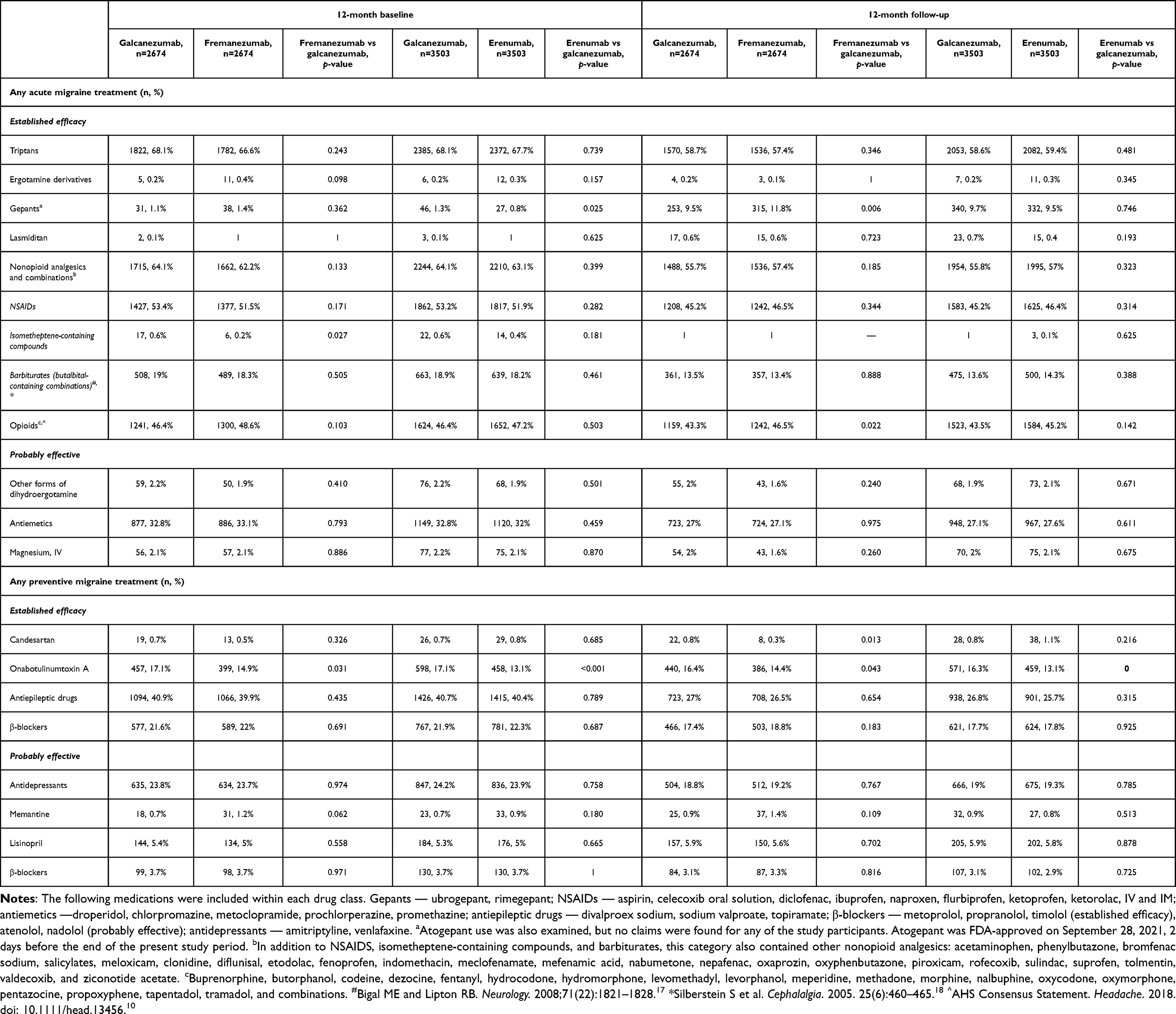 |
Table 3 Medications used during 12-month baseline and follow-up period |
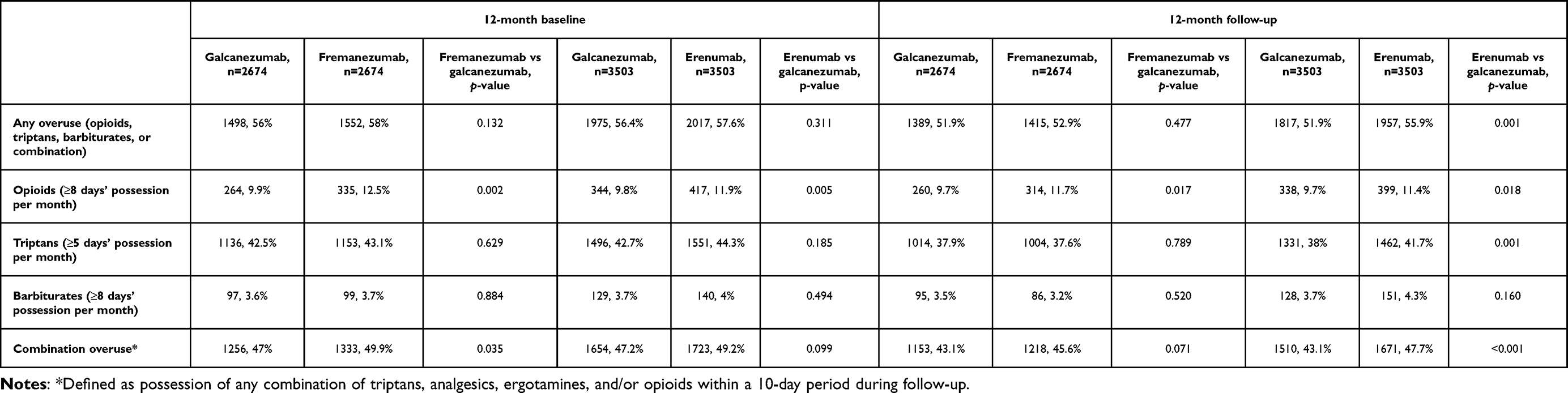 |
Table 4 Acute medication overuse during 12-month baseline and follow-up period |
12-Month Follow-Up Results: Galcanezumab vs Fremanezumab
During the 12-month follow-up period, patients initiating galcanezumab or fremanezumab received a mean of 0.9 unique preventive drug classes for migraine. A decrease in the proportion of patients receiving antiepileptic drugs and antidepressants was observed for both the galcanezumab (27% and 18.8%) and fremanezumab (26.5% and 19.2%) cohorts (Table 3), with a similar trend observed specifically for topiramate and amitriptyline use (data not shown). Similar proportions of galcanezumab vs fremanezumab patients added a nonindex preventive medication to their treatment regimen: most patients were prescribed onabotulinum toxin A (6% vs 5%), followed by antidepressants (4.5% vs 4.6%) and β-blockers (3.8% vs 4.2%, Table 4).
Minimal reductions in mean number of unique acute drug classes for migraine were observed for galcanezumab vs fremanezumab initiators (both 2). Reductions in the proportion of galcanezumab vs fremanezumab patients receiving the following acute medications were observed: triptans (58.7% vs 57.4%), opioids (43.4% vs 46.5%, p=0.022), antiemetics (27% vs 27.1%), and NSAIDs with established efficacy (45.2% vs 46.5%, Table 3). Similar proportions of galcanezumab vs fremanezumab patients added a nonindex acute medication to their treatment regimen: most patients were prescribed opioids (13.6% vs 13.4%), NSAIDs (12.7% and 14%) and antiemetics (10.3% vs 9.8%). Significantly fewer galcanezumab vs fremanezumab initiators added on gepants for acute use (8.7% vs 10.7%, p=0.013; Table 5). A reduction in acute medication overuse was observed in the proportion of patients initiating galcanezumab vs fremanezumab (51.9% vs 52.9%). Overuse was still primarily attributed to a combination of triptans, analgesics, ergotamines, and/or opioids (43.1% vs 45.6%). A significantly lower proportion of galcanezumab vs fremanezumab initiators were observed to have opioid overuse (9.7% vs 11.7%, p=0.017; Table 4).
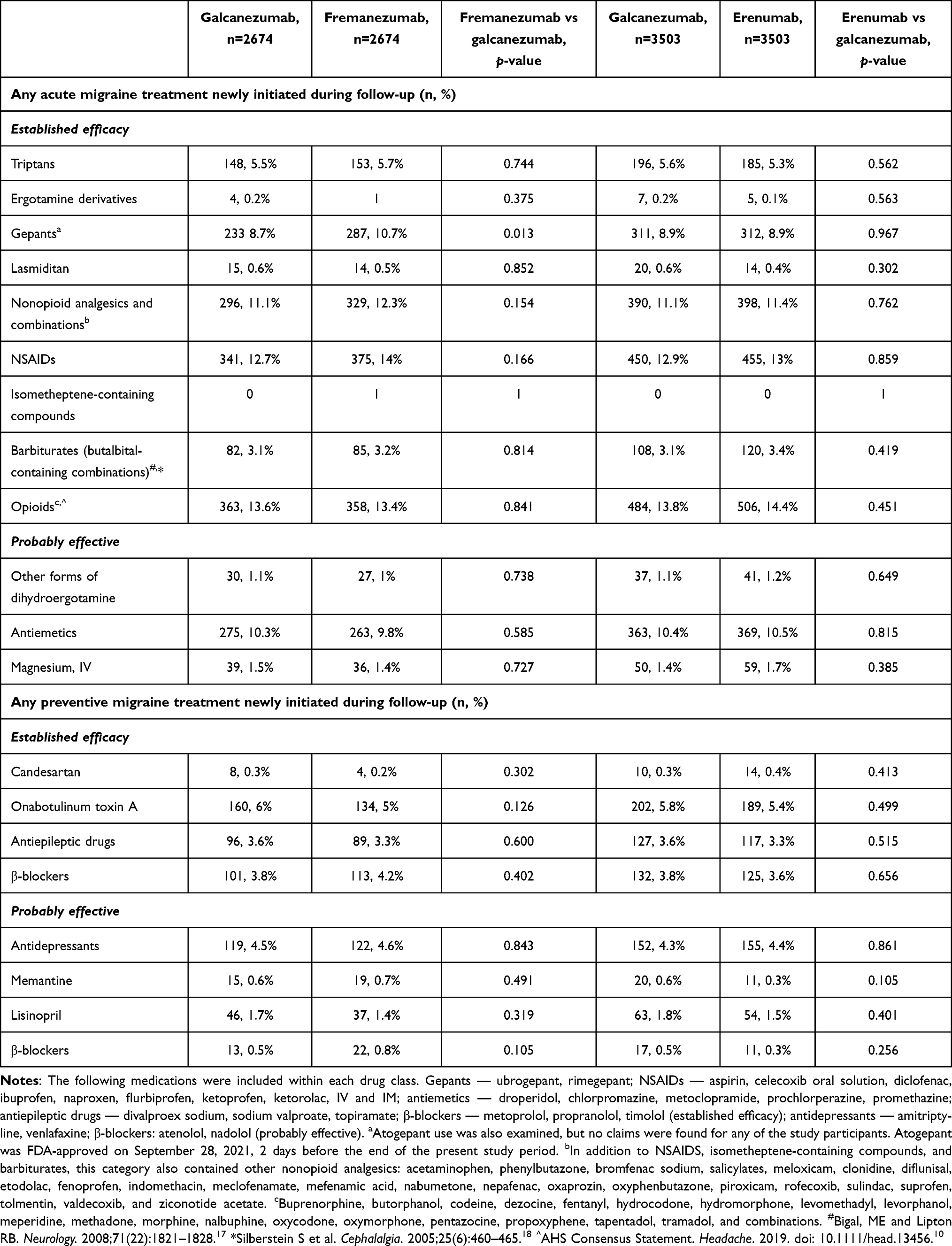 |
Table 5 Nonindexed medications newly initiated during 12-month follow-up period |
Baseline Results: Galcanezumab vs Erenumab
During the baseline period, patients initiating galcanezumab or erenumab received a mean of 1.1 unique preventive drug classes for migraine. Antiepileptic drugs and antidepressants were the most prescribed preventive drug classes in the galcanezumab (40.7% and 24.2%) and erenumab (40.4% and 23.9%) cohorts (Table 3). Specifically, topiramate and amitriptyline were the most prescribed agents in these drug classes for galcanezumab (37.9% and 16.3%) and erenumab (37.3% and 14.7%) cohorts (data not shown). A significantly greater proportion of galcanezumab vs erenumab initiators received onabotulinum toxin A (17.1% vs 13.1%, p<0.001). Patients in both cohorts received a mean of 2.2 unique acute drug classes for migraine, and similar proportions of galcanezumab vs erenumab patients received the following acute medications: triptans (68.1% vs 67.7%), opioids (46.4% vs 47.2%), antiemetics (32.8% vs 32%), and NSAIDs with established efficacy (53.2% vs 51.9%, Table 3). Acute medication overuse was observed in a similar proportion of patients initiating galcanezumab vs erenumab (56.4% vs 57.6%). Overuse was primarily attributed to a combination of triptans, analgesics, ergotamines, and/or opioids (47.2% vs 49.2%, p=0.099). A significantly lower proportion of galcanezumab vs erenumab initiators were observed to have opioid overuse (9.8% vs 11.9%, p=0.005).
12-Month Follow-Up Results: Galcanezumab vs Erenumab
During the 12-month follow-up period, patients initiating galcanezumab and erenumab received a mean of 0.9 unique preventive drug classes for migraine. A decrease in the proportion of patients receiving antiepileptic drugs and antidepressants was observed for both the galcanezumab (26.8% and 19%) and erenumab (25.7% and 19.3%) cohorts (Table 3), with a similar trend observed specifically for topiramate and amitriptyline use (data not shown). Similar proportions of galcanezumab vs erenumab patients added a nonindex preventive medication to their treatment regimen: most patients were prescribed onabotulinum toxin A (5.8% vs 5.4%), followed by antidepressants (4.3% vs 4.4%) and β-blockers (3.8 vs 3.6, Table 5). Minimal reductions in mean number of unique acute drug classes for migraine were observed for galcanezumab vs erenumab initiators (both 2). Reductions in the proportion of galcanezumab vs erenumab patients receiving the following acute medications were observed: triptans (58.6% vs 59.4%), opioids (43.5% vs 45.2%), antiemetics (27.1% vs 27.6%), and NSAIDs with established efficacy (45.2% vs 46.4%, Table 3). Similar proportions of galcanezumab vs erenumab patients added a nonindex acute medication to their treatment regimen: most patients were prescribed opioids (13.8% vs 14.4%), NSAIDs (12.9% and 13%), and antiemetics (10.4% vs 10.5%). Gepants for acute use were initiated by 8.9% of patients in the galcanezumab vs erenumab cohort (Table 5). A significantly lower proportion of galcanezumab vs erenumab initiators were observed to have acute medication overuse (51.9% vs 55.9%, p=0.001). Overuse was still primarily attributed to a combination of triptans, analgesics, ergotamines, and/or opioids (43.1% vs 47.7%, p<0.001). A significantly lower proportion of galcanezumab vs erenumab initiators were observed to have opioid overuse (9.7% vs 11.4%, p=0.018) and triptan overuse (38% vs 41.7%, p=0.018; Table 4).
Treatment Patterns
Treatment Adherence
At 12 months, mean ± SD PDC for galcanezumab vs fremanezumab initiators was 0.6±0.3. MPR was also 0.6±0.3 for both cohorts. A numerically greater proportion of galcanezumab vs fremanezumab initiators were considered adherent as measured by PDC ≥0.80 (46.2% vs 43.7%, p=0.053) and MPR ≥0.80 (46.8% vs 44.3%, p=0.053). Mean ± SD PDC and MPR were also 0.6±0.3 for galcanezumab vs erenumab initiators. A numerically greater proportion of galcanezumab vs erenumab initiators were considered adherent as measured by PDC ≥0.80 (46.2% vs 44%, p=0.156) and MPR ≥0.80 (46.7% vs 44.5%, p=0.262; Table 6).
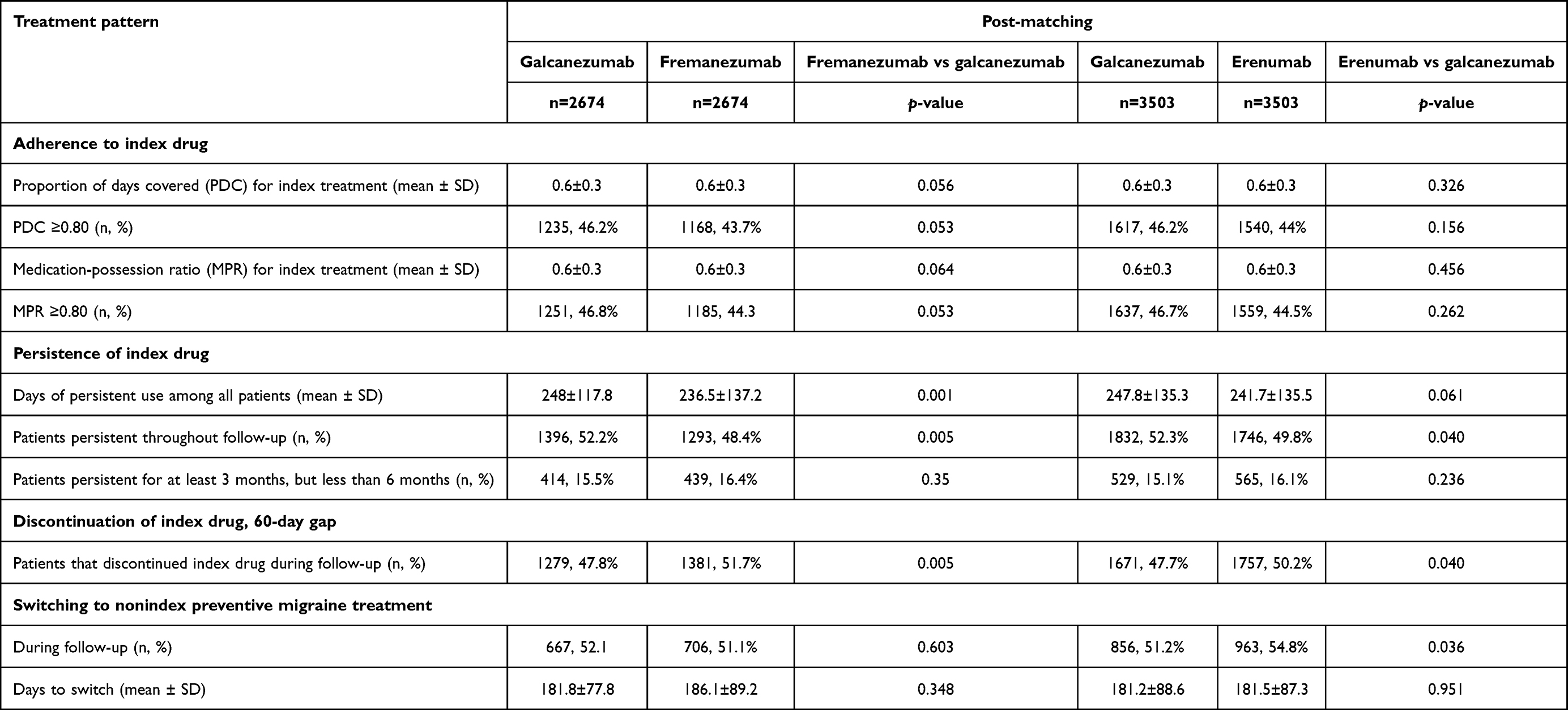 |
Table 6 Treatment patterns of prescribed index treatment of galcanezumab, fremanezumab, or erenumab during 12-month follow-up |
Persistence and Discontinuation of Index Treatment
During the 12-month follow-up, the galcanezumab cohort had significantly higher persistence (60-day gap) than the fremanezumab cohort (248.0 days vs 236.5 days, p=0.001). After 3 months of initiating index treatments, a greater proportion of fremanezumab initiators were not persistent with treatment than galcanezumab initiators (Figure 2). At the end of the 12-month follow-up, galcanezumab initiators were significantly less likely to discontinue treatment than fremanezumab initiators (47.8% vs 51.7%, p=0.005). Numerically higher persistence was observed for galcanezumab vs erenumab initiators (247.8 days vs 241.7 days, p=0.061; Table 6). Also, a greater proportion of erenumab initiators were not persistent with treatment after 3 months of starting treatment compared to galcanezumab initiators (Figure 2). At the end of the 12-month follow-up, galcanezumab initiators were significantly less likely to discontinue treatment than erenumab initiators (47.7% vs 50.2%, p=0.040).
 |
Figure 2 Proportion of patients that remained persistent with index drug during 12-month follow-up. |
Switch to a Nonindex Drug after Discontinuation
Among patients who discontinued galcanezumab vs fremanezumab treatment (1279 vs 1381), a similar proportion of patients switched to a nonindex preventive migraine treatment (52.1% vs 51.1%, Table 6). Among patients who switched to a nonindex drug, a similar mean time to switch was observed for the galcanezumab vs fremanezumab cohort (181.8 days vs 186.1 days). Most galcanezumab vs fremanezumab patients switched to onabotulinum toxin A (22.7% vs 17.9%), topiramate (14.8% vs 15.6%), or a different CGRP mAb (Figure 3).
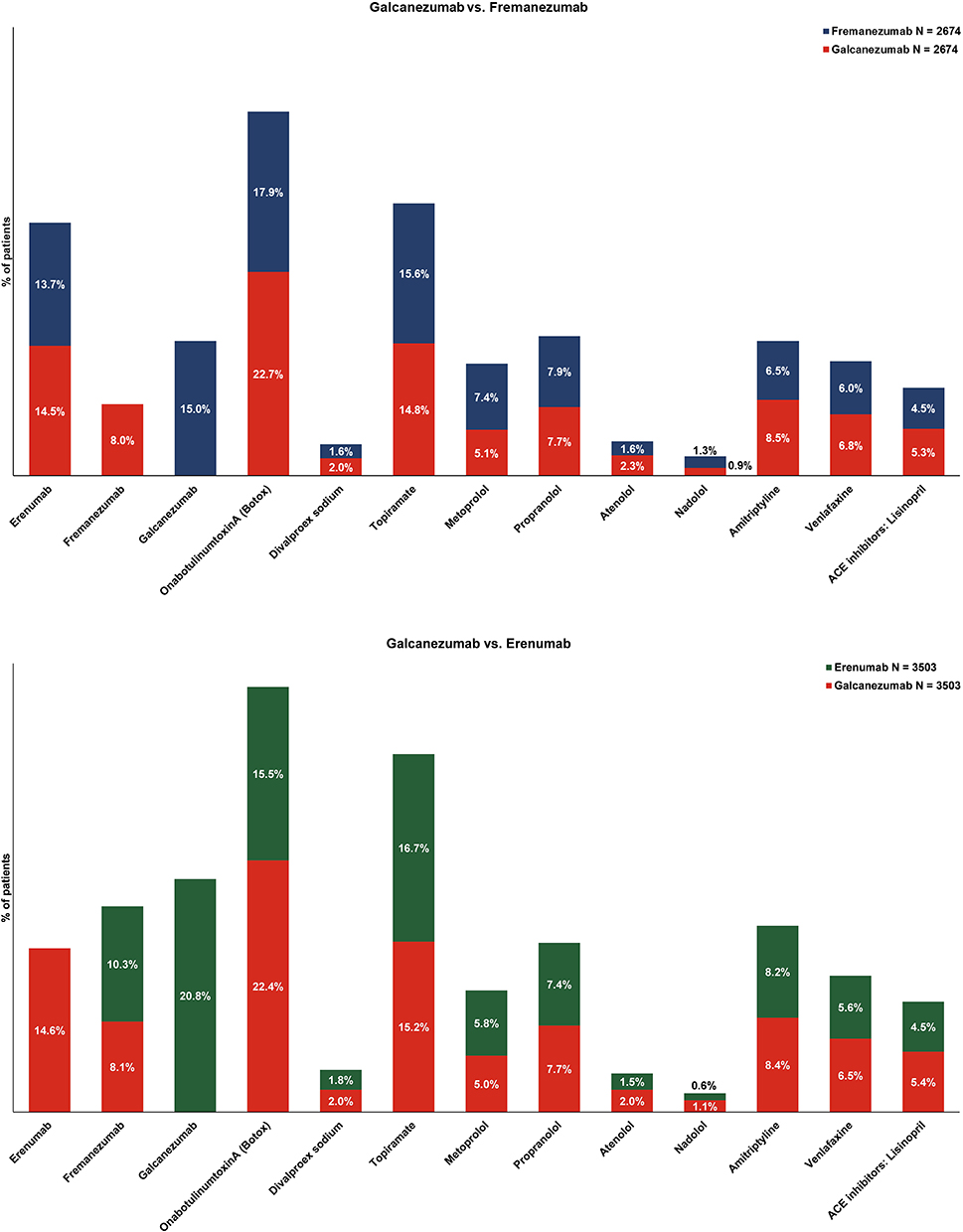 |
Figure 3 Common therapies switched to over the 12- months follow-up period post-matching. For non-CGRP-preventive therapies, drug classes with five or more patients are not presented in the graph: eptinezumab, divalproex sodium, sodium valproate, metoprolol, propranolol, atenolol, amitriptyline, venlafaxine, and the ACE inhibitor lisinopril. Drug classes included were classified as follows: CGRP mAbs (erenumab, fremanezumab, galcanezumab, eptinezumab); non-CGRP mAb migraine treatment: — angiotensin-receptor blocker (candesartan); antiepileptic drugs (divalproex sodium, sodium valproate, topiramate); β-blockers (metoprolol, propranolol, timolol, atenolol, nadolol); antidepressants (amitriptyline, venlafaxine); and the NMDA-receptor antagonist memantine. |
Among patients who discontinued galcanezumab vs erenumab treatment (1671 vs 1757), a significantly lower proportion of galcanezumab patients switched to a nonindex preventive migraine treatment (51.2% and 54.8%, p=0.036; Table 6). Among patients who switched to a nonindex drug, a similar mean time to switch was observed for the galcanezumab vs erenumab cohort (181.2 days vs 181.5 days). Most galcanezumab vs erenumab patients switched to onabotulinum toxin A (22.4% vs 15.5%), topiramate (15.2% vs 16.7%), or a different CGRP mAb (Figure 3).
Patient Sample, Baseline Characteristics, and Treatment Patterns for 6-Month Follow-Up Cohorts
For the 6-month follow-up cohort, a total of 35,628 patients were identified: galcanezumab cohort (n=12,621), fremanezumab cohort (n=6987), and erenumab cohort (n=16,020) (Supplementary Figure 1). After propensity-score matching, 3810 patients comprised each of the galcanezumab vs fremanezumab cohorts, and 4997 patients comprised each of the galcanezumab vs erenumab cohorts. Similar trends in the baseline patient demographics, clinical characteristics, and treatment patterns were observed for the 6-month follow-up cohorts and the 12-month follow-up cohorts (Supplementary Tables 2–7 and Supplementary Figures 1–3).
Discussion
This is the first real-world study to compare treatment patterns for patients with migraine initiating the three self-injectable CGRP mAbs (galcanezumab, fremanezumab, erenumab) with a 12-month follow-up. Key findings from this study showed that patients with migraine who initiated galcanezumab demonstrated significantly higher persistence, significantly lower treatment discontinuation rates, and similar adherence rates, but numerically higher proportions of adherent patients than those initiating fremanezumab or erenumab. Patients initiating galcanezumab were also less likely to switch to a nonindex preventative migraine medication over the 12-month follow-up than those initiating erenumab (51.2% vs 54.8%, respectively). Following index treatment discontinuation, most patients switched to onabotulinum toxin A or topiramate; however, switching within the CGRP mAb class indicated both fremanezumab and erenumab patients were most likely to switch to galcanezumab, while galcanezumab patients were most likely to switch to erenumab.
Anxiety, sleep disorders, and depression were the top three comorbid conditions observed in the current study. A strong correlation between these comorbidities and migraine have been reported in prior studies,6,20 and may contribute to antiepileptic drugs and antidepressants being commonly prescribed preventive medications for migraine during the baseline period. During the 12-month follow-up, reductions in the proportion of patients using preventive medications, including antiepileptic drugs and antidepressants, were observed across all patient cohorts. Patients newly initiating a concomitant preventive medication were most commonly prescribed onabotulinum toxin A. Reductions in the proportion of patients using acute medications, including triptans, opioids, antiemetics, and NSAIDs with established efficacy, were also observed across all patient cohorts. However, opioids were most commonly prescribed among patients newly initiating a concomitant acute medication. The galcanezumab cohort tended to have lower rates of acute medication overuse at baseline and during the 12-month follow-up, particularly opioids, than the fremanezumab and erenumab cohorts.
Despite the availability of several treatment options for migraine and associated improvements measured by patient-reported outcomes, patients demonstrate insufficient response to therapies.21 Lack of efficacy and poor tolerability have long been drivers of migraine-preventive medication discontinuation and low persistence rates.22 Galcanezumab, fremanezumab, and erenumab have all been shown to be safe and effective in reducing migraine symptoms and preventing attacks.7–9 These agents have also demonstrated improvements in functional impairment, reduced migraine-associated disability, overall work, and activity impairment.23–28 Albeit slightly higher, the adherence and persistence rates observed in this study are aligned with those of prior reports.14,29 These findings provide evidence that patients on CGRP mAbs are likely to remain adherent on treatment long enough (>3 months) to determine efficacy and assess appropriateness for continuation based on the AHS Consensus Statement.16 While minimal declines in persistence were first observed 30 days after initiation across all three CGRP mAbs, greater declines were observed 90 days after initiation through end of follow-up for fremanezumab and erenumab than galcanezumab. Furthermore, galcanezumab initiators were less likely to discontinue treatment than fremanezumab and erenumab initiators. About half of those patients who discontinued index treatment switched to a nonindex preventive migraine medication. Most patients switched to an antiepileptic drug, antidepressant, or different CGRP mAb. When switching occurred within the CGRP mAb class, both fremanezumab and erenumab initiators primarily switched to galcanezumab, while galcanezumab initiators switched to erenumab. Reasons for discontinuation and switching were not evaluated in the present study. Future studies evaluating reasons for discontinuation and switching among CGRP mAb initiators will aid in decision-making for providers and their patients when assessing benefits of their current preventive treatments and importance of prolonged therapy.
While findings from meta-analyses show that CGRP mAbs offer improved effectiveness with better medication adherence and persistence rates than traditional preventive migraine medications,14 gaps in clinical care for patients with migraine are still present. Findings from the largest multicohort, longitudinal survey-based study, OVERCOME, showed only ~15% of prevention-eligible patients with migraine: 1) seek care, 2) are diagnosed by a physician, and 3) receive recommended preventive medication.30 Furthermore, patients are reluctant to initiate and continue preventive migraine therapy. As observed in the survey-based American Migraine Prevalence and Prevention study, patients also face difficulty in accessing preventive treatments.31 Relatively high prescription costs and meeting the recommendation of failing at least two traditional preventive migraine medications are major impediments to accessing newer medications like the CGRP mAbs.
Given the prevailing evidence demonstrating improved efficacy along with adherence and persistence rates, CGRP mAbs are an ideal treatment option for some patients with migraine. In some regard, the results of this study demonstrate parity between galcanezumab, fremanezumab, and erenumab; however, differences in specific outcomes persist between cohorts, with generally favorable results for galcanezumab regarding acute medication overuse and medication adherence and persistence during the 12-month follow-up. There are likely specific patient subpopulations who would experience improved outcomes with galcanezumab versus one of the other CGRP mAbs evaluated in this study; however, analyses in broad migraine patient populations suggest that all three agents appear to be effective and offer advantages over traditional migraine-preventive therapies.
Strengths and Limitations
This study has certain strengths. It is the first study to address the gap in literature with respect to treatment patterns comparing the three self-injectable CGRP mAbs with a 12-month follow-up duration. Use of propensity-score matching in this study ensured minimum selection or confounder bias, which otherwise is common with observational studies. This analysis was limited in terms of generalizability, as only data from the Merative MarketScan Commercial and Medicare databases were used, and thus results cannot be generalized to patients with other types of insurance or without insurance. As with other claims-based studies, there is also the potential for misclassification of disease, severity status, or other outcomes. This analysis only examined use of prescription medications. It is likely that over-the-counter pain medications such as NSAIDs were used to manage migraine attacks, making it difficult to discern the quantity of acute treatments that were excluded from this analysis. Although propensity-score matching was used to control for differences between cohorts, there may be remaining unobserved confounders in demographic characteristics between cohorts.
Conclusion
Findings from this real-world study demonstrated that patients with migraine who initiated CGRP mAb treatment with galcanezumab showed higher persistence, lower treatment discontinuation rates, and similar adherence than those initiating either fremanezumab or erenumab. Future studies including provider and patient surveys exploring reasons for treatment discontinuation, such as improved or lack of efficacy or tolerability issues, may provide insight into the treatment patterns observed in the current study.
Data Sharing
The data that support the study findings were provided by Merative. Restrictions apply to the availability of these data, which were used under license for this study and therefore are not publicly available. Requests may be sent to Merative for more information on data availability and licensing.
Ethics Approval
This study was conducted in accordance with the Declaration of Helsinki of 1975 by the World Medical Association, as revised by the 59th WMA General Assembly 2008 in Seoul. Since the study used only deidentified patient records, neither institutional review board approval nor patient informed consent to conduct this study was required. Informed consent was obtained from all participants.
Acknowledgments
Medical writing support was provided by Priyanka Bannikoppa, PhD and Keerthana Muthiah from Eli Lilly Services India.
Author Contributions
All authors have made significant contributions to the work reported, including study conception, design, execution, acquisition of data, analysis, and interpretation. The authors also contributed towards drafting the manuscript, revising, or critically reviewing the draft, and gave final approval to the version to be published, have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
This study was funded by Eli Lilly and Company.
Disclosure
Brenna L Brady is an employee of Merative who received funding from Eli Lilly and Company to conduct this analysis. Yvonne P Robles was an employee of Merative, Ann Arbor, MI, USA for the entire period of this study, and is now an employee of Panalgo (265 Franklin Street, Boston, MA 02110, USA). Oralee J Varnado, Anthony J Zagar, and Margaret Hoyt are full-time employees and shareholders at Eli Lilly and Company.
References
1. Domitrz I, Golicki D. Health-related quality of life in migraine: EQ-5D-5L-based study in routine clinical practice. J Clin Med. 2022;11(23):6925. doi:10.3390/jcm11236925
2. Headache Classification Committee of the International Headache Society (IHS). The international classification of headache disorders, 3rd. Cephalalgia. 2018;38(1):1–211.
3. Leonardi M, Raggi A. A narrative review on the burden of migraine: when the burden is the impact on people’s life. J Headache Pain. 2019;20(1):41. doi:10.1186/s10194-019-0993-0
4. Raffaelli B, Neeb L, Reuter U. Monoclonal antibodies for the prevention of migraine. Expert opin biol ther. 2019;19(12):1307–1317. doi:10.1080/14712598.2019.1671350
5. Safiri S, Pourfathi H, Eagan A, et al. Global, regional, and national burden of migraine in 204 countries and territories, 1990 to 2019. Pain. 2022;163(2):e293–e309. doi:10.1097/j.pain.0000000000002275
6. Burch RC, Buse DC, Lipton RB. Migraine: epidemiology, burden, and comorbidity. Neurol Clinics. 2019;37(4):631–649. doi:10.1016/j.ncl.2019.06.001
7. Aimovig™ (erenumab-aooe subcutaneous injection). Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/761077s000lbl.pdf.
8. Emgality™ (galcanezumab-gnlm subcutaneous injection). Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/761063s000lbl.pdf.
9. Ajovy™ (fremanezumab-vfrm subcutaneous injection). Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/761089s000lbl.pdf.
10. American Headache Society. The American headache society position statement on integrating new migraine treatments into clinical practice. Headache. 2019;59(1):1–18. doi:10.1111/head.13456
11. Goadsby PJ, Silberstein SD, Yeung PP, et al. Long-term safety, tolerability, and efficacy of fremanezumab in migraine: a randomized study. Neurology. 2020;95(18):e2487–e2499. doi:10.1212/WNL.0000000000010600
12. Ford JH, Foster SA, Stauffer VL, Ruff DD, Aurora SK, Versijpt J. Patient satisfaction, health care resource utilization, and acute headache medication use with galcanezumab: results from a 12-month open-label study in patients with migraine. Patient Preference Adherence. 2018;12:2413–2424. doi:10.2147/PPA.S182563
13. Garland SG, Smith SM, Gums JG. Erenumab: a first-in-class monoclonal antibody for migraine prevention. Ann Pharmacother. 2019;53(9):933–939. doi:10.1177/1060028019835166
14. Varnado OJ, Manjelievskaia J, Ye W, Perry A, Schuh K, Wenzel R. Treatment patterns for calcitonin gene-related peptide monoclonal antibodies including galcanezumab versus conventional preventive treatments for migraine: a retrospective US claims study. Patient Preference Adherence. 2022;16:821–839. doi:10.2147/PPA.S346660
15. Vandervorst F, Van Deun L, Van Dycke A, et al. CGRP monoclonal antibodies in migraine: an efficacy and tolerability comparison with standard prophylactic drugs. J Headache Pain. 2021;22(1):128. doi:10.1186/s10194-021-01335-2
16. Ailani J, Burch RC, Robbins MS. The American headache society consensus statement: update on integrating new migraine treatments into clinical practice. Headache. 2021;61(7):1021–1039. doi:10.1111/head.14153
17. Bigal ME, Lipton RB. Excessive acute migraine medication use and migraine progression. Neurology. 2008;71(22):1821–1828. doi:10.1212/01.wnl.0000335946.53860.1d
18. Silberstein SD, Olesen J, Bousser MG, et al. The International Classification of Headache Disorders, 2nd Edition (ICHD-II)--revision of criteria for 8.2 Medication-overuse headache. Cephalalgia. 2005;25(6):460–465. doi:10.1111/j.1468-2982.2005.00878.x
19. D’Agostino RB
20. Caponnetto V, Deodato M, Robotti M, et al. Comorbidities of primary headache disorders: a literature review with meta-analysis. J Headache Pain. 2021;22(1):71. doi:10.1186/s10194-021-01281-z
21. Ford JH, Jackson J, Milligan G, Cotton S, Ahl J, Aurora SK. A real-world analysis of migraine: a cross-sectional study of disease burden and treatment patterns. Headache. 2017;57(10):1532–1544. doi:10.1111/head.13202
22. Hepp Z, Dodick DW, Varon SF, et al. Persistence and switching patterns of oral migraine prophylactic medications among patients with chronic migraine: a retrospective claims analysis. Cephalalgia. 2017;37(5):470–485. doi:10.1177/0333102416678382
23. Ayer DW, Skljarevski V, Ford JH, Nyhuis AW, Lipton RB, Aurora SK. Measures of functioning in patients with episodic migraine: findings from a double-blind, randomized, placebo-controlled phase 2b trial with galcanezumab. Headache. 2018;58(8):1225–1235. doi:10.1111/head.13383
24. Buse DC, Gandhi SK, Cohen JM, et al. Improvements across a range of patient-reported domains with fremanezumab treatment: results from a patient survey study. J Headache Pain. 2020;21(1):109. doi:10.1186/s10194-020-01177-4
25. Buse DC, Lipton RB, Hallström Y, et al. Migraine-related disability, impact, and health-related quality of life among patients with episodic migraine receiving preventive treatment with erenumab. Cephalalgia. 2018;38(10):1622–1631. doi:10.1177/0333102418789072
26. Ford J, Tassorelli C, Leroux E, et al. Changes in patient functioning and disability: results from a Phase 3, double-blind, randomized, placebo-controlled clinical trial evaluating galcanezumab for chronic migraine prevention (REGAIN). Qual Life Res. 2021;30(1):105–115. doi:10.1007/s11136-020-02623-1
27. Lipton RB, Cohen JM, Gandhi SK, Yang R, Yeung PP, Buse DC. Effect of fremanezumab on quality of life and productivity in patients with chronic migraine. Neurology. 2020;95(7):e878–e888. doi:10.1212/WNL.0000000000010000
28. Lipton RB, Tepper SJ, Reuter U, et al. Erenumab in chronic migraine: patient-reported outcomes in a randomized double-blind study. Neurology. 2019;92(19):e2250–e2260. doi:10.1212/WNL.0000000000007452
29. Hines DM, Shah S, Multani JK, Wade RL, Buse DC, Bensink M. Erenumab patient characteristics, medication adherence, and treatment patterns in the United States. Headache. 2021;61(4):590–602. doi:10.1111/head.14068
30. Ashina S. Identifying barriers to care-seeking, diagnosis, and preventive medication among those with migraine: results of the OVERCOME study. Headache. 2020;60:132–133.
31. Lipton RB, Serrano D, Holland S, Fanning KM, Reed ML, Buse DC. Barriers to the diagnosis and treatment of migraine: effects of sex, income, and headache features. Headache. 2013;53(1):81–92. doi:10.1111/j.1526-4610.2012.02265.x
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Treatment Patterns, Healthcare Resource Utilization, and Direct Costs Among Patients Initiating Concomitant Use of a Calcitonin Gene-Related Peptide Monoclonal Antibody (CGRP mAb) and Novel Acute Medication in the United States
Varnado OJ, Gulati T, Wheeler A, Hoyt M
Patient Preference and Adherence 2023, 17:3449-3459
Published Date: 18 December 2023