")
Back to Journals » Drug Design, Development and Therapy » Volume 17
Comparison of the Pharmacokinetics, Safety, and Tolerability of Two Empagliflozin Formulations in Healthy Korean Subjects
Authors Jiang X , Bae S , Yoon DY, Park SJ, Oh J , Cho JY , Yu KS
Received 14 March 2023
Accepted for publication 28 June 2023
Published 24 July 2023 Volume 2023:17 Pages 2137—2145
DOI https://doi.org/10.2147/DDDT.S409368
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Manfred Ogris
Xu Jiang,1 Sungyeun Bae,1 Deok Yong Yoon,2 Shin Jung Park,3 Jaeseong Oh,1 Joo-Youn Cho,1,4 Kyung-Sang Yu1,4
1Department of Clinical Pharmacology and Therapeutics, Seoul National University College of Medicine and Hospital, Seoul, Republic of Korea; 2Department of Pharmaceutics, Center for Pharmacometrics and Systems Pharmacology, College of Pharmacy, University of Florida, Orlando, FL, USA; 3Department of Pharmaceutical Research Laboratory, Chong Kun Dang Research Institute, Chong Kun Dang Pharmaceutical Corporation, Yongin, Republic of Korea; 4Department of Biomedical Sciences, Seoul National University College of Medicine, Seoul, Republic of Korea
Correspondence: Kyung-Sang Yu, Department of Clinical Pharmacology and Therapeutics, Seoul National University College of Medicine and Hospital, 101, Dae-hak ro, Jong-ro gu, Seoul, 03080, Republic of Korea, Tel/Fax +82-2072-1666, Email [email protected]
Purpose: Empagliflozin is a sodium-glucose cotransporter 2 inhibitor that is commonly used for the treatment of type 2 diabetes mellitus. As cocrystal formulation can improve the chemical properties of drugs, CKD-370 was newly developed as a cocrystal formulation of empagliflozin with solvate L-proline. This study aimed to compare the pharmacokinetics, safety, and tolerability of these two empagliflozin formulations in healthy Korean subjects.
Methods: A randomized, open-label, two-sequence, two-period crossover study was conducted on healthy Korean participants. The subjects received a single oral 25 mg dose of either test (CKD-370) or reference treatment (Jardiance®) tablet at each period. Plasma empagliflozin concentrations were determined using liquid chromatography with tandem mass spectrometry. Pharmacokinetic (PK) parameters were analyzed using non-compartmental methods. The primary PK parameters included the maximum concentration (Cmax) and the area under the concentration-time curve from 0 to last (AUClast). The safety of both formulations was monitored and evaluated.
Results: A total of 28 healthy Korean adult subjects were randomized, and 27 subjects were included in the PK analysis. The mean ± standard deviation values of the primary PK parameters, Cmax and AUClast after administration of the test treatment, were 442.02 ± 103.37 μg/L and 3131.08 ± 529.30 μg·h/L, respectively, and those after administration of the reference treatment were 436.29 ± 118.74 μg/L and 3006.88 ± 514.21 μg·h/L, respectively. The geometric mean ratio and its 90% confidence interval of test to reference treatment for Cmax and AUClast were 1.0221 (0.9527– 1.0967) and 1.0411 (1.0153– 1.0677), respectively, which were within the commonly accepted bioequivalence criteria of 0.80 to 1.25. Both treatments were well-tolerated.
Conclusion: The two formulations of empagliflozin showed similar PK characteristics and were generally well tolerated in healthy subjects.
Keywords: T2DM, cocrystal, L-proline, biosimilar, CKD-370
Introduction
Type 2 diabetes mellitus (T2DM) is a chronic metabolic disease with increasing prevalence worldwide. A previous study estimated that there were about 451 million people with diabetes worldwide in 2017, which is expected to increase to 693 million by 2045.1 In South Korea, the socioeconomic development has resulted in a sharp increase in the prevalence of overeating, physical inactivity, and stress, and the average annual prevalence of diabetes is estimated to be 10.7%.2 In addition, the proportion of diabetes among the causes of death has also increased gradually in South Korea. Diabetes ranks sixth among the causes of death in Koreans.3 Most patients with T2DM have macrovascular complications such as cardiovascular disease as well as microvascular complications that affect the kidney, retina, and nervous system.4 T2DM and complications significantly affect quality of life and may even cause morbidity and mortality. Therefore, blood sugar control is required to treat T2DM and to prevent complications. Several antidiabetic drugs with different mechanisms of action have been developed and approved for T2DM treatment.
A sodium-glucose cotransporter 2 (SGLT2) inhibitor was first developed in 2013 as an oral hypoglycemic agent.5 It was highly selective and could specifically inhibit the mechanism of renal tubular reabsorption of glucose. SGLT2 inhibitors increase the glucose excretion in urine, thereby lowering blood glucose levels.5 Unlike other antidiabetic agents, such as sulfonylureas, SGLT2 inhibitors do not depend on islet or beta cell function to regulate blood sugar.6 Moreover, the SGLT2 inhibitors show greater HbA1c reduction and lower the risk of hypoglycemia in patients with T2DM when compared to sulfonylureas.7–9 Furthermore, it rarely causes ketoacidosis and even has additional therapeutic effects such as promoting weight loss, lowering blood pressure, and protecting insulin B cells.10–13 Recent studies showed that SGLT2 inhibitors could also exert cardiac benefits with improvement in hard clinical endpoints in heart failure with reduced ejection fraction14 and heart failure with preserved ejection fraction.15 SGLT2 inhibitors can improve the quality of life in heart failure16 and reverse cardiac remodeling with improvement in exercise capacity.17
These cardiac benefits of SGLT2 inhibitors are due to a metabolic shift in myocardial metabolism away from the energy-inefficient glucose towards enhanced consumption of fatty acids and ketone bodies,18 thus improving energetics and diastolic function19 and also reducing myocardial infarction size.20
Currently, cocrystal technology is widely used in the pharmaceutical industry to facilitate the development pharmaceutical formulation.21 Cocrystal formulation can improve the chemical properties of the drugs, such as stability, compressibility, flowability, and hygroscopicity, comparing to the free compound.22–25 For example, an SGLT2 inhibitor, Suglat® (Ipragliflozin L-proline) was developed as a cocrystal formulation using the solvate of L-proline. Furthermore, a novel dapagliflozin di-L-proline cocrystal-loaded tablet with low hygroscopicity and low water content was developed to solve the problems caused by the severe hygroscopic properties of dapagliflozin, such as inaccurate weighing, sticking in the compression process, and instability.26
Empagliflozin (Jardiance®, or the reference treatment), a representative SGLT2 inhibitor that had no solvate, was first launched in 2014 under license from Boehringer Ingelheim International GmbH, Ingelheim, Germany.27 The pharmacokinetic (PK) characteristics of empagliflozin are well known.28 To improve chemical properties, a single agent with a solvate of L-proline was developed from the reference treatment as CKD-370 (empagliflozin L-proline, or the test treatment). The test treatment was hypothesized to have similar PK characteristics to empagliflozin but improved chemical properties. In the present study, the test treatment was evaluated and compared with the reference treatment. We aimed to evaluate the PK, safety, and tolerability of the test and reference treatments following a single oral administration under fasting conditions in healthy Korean subjects.
Materials and Methods
The present study (ClinicalTrials.gov identifier: NCT03849495) was approved by the Ministry of Food and Drug Safety of the Republic of Korea and Institutional Review Board of Seoul National University Hospital (Seoul, Republic of Korea). This study was conducted between 19 February 2019 and 8 April 2019, and it was conducted in accordance with the International Conference on Harmonization Good Clinical Practice and the ethical principles of the Declaration of Helsinki.
Study Population
In this study, healthy Korean subjects aged between 19 and 50 years and weighing 55–90 kg with a BMI of 18–27 kg/m2 were enrolled. Participants who had an allergy to the study medications and those who could not abstain from drinking alcohol, smoking, or drug use throughout the study were excluded. The participants were asked to take effective contraceptive measures during the screening period as well as the subsequent at least 28 days. In addition, the study required that the participants should not have participated in another clinical trial in the three months before the present study. Signed informed consent was obtained from all the participants prior to the study.
Study Design
The present study included a randomized, open-label, two-sequence, two-period crossover study design. The eligible participants were hospitalized in the afternoon before the first administration of the drug during each period. They were randomized into two sequences (A and B), maintaining fasting conditions for at least 10 h before administration. Sequence A was the reference treatment followed by the test treatment and sequence B was the test treatment followed by the reference treatment. The subjects received a single oral administration of 25 mg of either the test or reference drug with 150 mL of water. They received a single oral dose of the other treatment after a 7-day wash-out period.
Sample Size
According to the data in previous studies, the intra-individual coefficient variability of primary endpoints the maximum concentration (Cmax) and the area under the concentration-time curve from 0 to last (AUClast) was at most 18.7%.29 Thus, a total of 21 participants were required in the two-way crossover study to demonstrate the bioequivalence between treatments with a power of 90% at a 5% significance level. We assumed a dropout rate of 20%, and hence, a total of 28 subjects with 14 in each sequence were included in the present study.
Blood Sampling
Based on previous studies, the time to maximum plasma concentration (Tmax) of empagliflozin was 1.5 to 2.1 h, and the elimination half-life ranged between 10.2 and 12.4 h.27,30,31 Therefore, blood samples for PK assessment were collected in each period at the following time points: before study drug administration (0 h), 0.33 h, 0.67 h, 1 h, 1.5 h, 2 h, 2.5 h, 3 h, 4 h, 6 h, 8 h, 10 h, 12 h, 24 h, 34 h, and 48 h after study drug administration. The blood samples (5 mL) were collected into EDTA-K2 tubes and centrifuged for 10 minutes at 3000 rpm and 4°C within 30 minutes. Plasma was aliquoted and stored below −70°C until analysis.
Sample Analysis
The plasma concentrations of empagliflozin were quantified using a developed and validated liquid chromatography with tandem mass spectrometry (LC-MS/MS) method in accordance with good laboratory practice standards. The LC-MS/MS system was equipped with a Shimadzu UFLC system (Shimadzu, Kyoto, Japan) and an API5000(3) triple quadrupole mass spectrometer (SCIEX, CA, USA). We used 1 mg/mL empagliflozin-d4 as an internal standard for calibration. The internal standard (10 μL) and methyl tert-butyl ether (1 mL) were added to each 100 μL plasma sample. The ether mix was vortexed for 3 min, centrifuged at 13,000 rpm for 3 min, and stored at −80°C for 20 min. The ether layer was transferred to another tube and evaporated under a stream of nitrogen gas. Then, 300 μL of 50% acetonitrile was added and a multi-vortexer was used to solubilize the residue. Five microliters of this solution were injected into the LC-MS/MS system for analysis. The method was fully validated for its linearity, selectivity, sensitivity, stability, accuracy, and precision according to the Ministry of Food and Drug Safety (MFDS) guidelines in the calibration range of 2–1500 ng/mL.
Pharmacokinetic Analysis
PK parameters were analyzed by non-compartmental methods using Phoenix WinNonlin® (Version 8.0 Certara, NJ, USA). Primary PK endpoints were identified as AUClast calculated by the linear trapezoidal model and Cmax by observation. Secondary PK endpoints were the area under the plasma drug concentration-time curve from 0 to infinity (AUCinf) calculated by adding Clast/λz to AUClast, where Clast is the last plasma concentration measurement, and λz is the elimination rate constant. Tmax is presented as an observed value, and the elimination half-life (t1/2) was calculated as log (2)/λz using the natural logarithm. The apparent clearance (CL/F) was calculated by dividing the dosage by the AUC, and the apparent volume of distribution (Vd/F) was calculated by dividing CL/F by λz.
Statistical Analysis
A linear mixed model was performed on the logarithmically transformed values of the primary PK parameters, Cmax and AUClast, using SAS (version 9.4; SAS Institute Inc., Cary, NC, USA) for the evaluation of bioequivalence. The fixed effects included period, sequence, and treatment were considered, and subjects within each sequence group were considered random effects. The geometric mean ratios (GMR) of Cmax and AUClast (test/reference) and 90% confidence intervals (CIs) were calculated. The two treatments were considered bioequivalent if the 90% CIs of the primary PK parameters were within a predefined range of 80–125%. In addition, arithmetic means, standard deviations (SDs), median, maximum, and minimum values of subject demographics and PK parameters were also calculated.
Safety/Tolerability Assessment
Safety and tolerability were assessed for every participant who was administered at least once. Adverse drug reactions (ADRs) were assessed for severity, duration, and relationship with the study drug throughout the study. Physical examination, clinical laboratory tests, and 12-lead electrocardiography (ECG) were also conducted, and vital signs were recorded. All adverse events (AEs) were recorded.
Results
Subject Characteristics
A total of 33 subjects were screened, and 28 healthy Korean subjects were randomized and enrolled, with 14 subjects in each sequence. One subject from sequence B dropped out after administration of the test treatment in period 1 due to consent withdrawal, and another subject from sequence A was lost to follow-up during the post-study visit period. Consequently, 27 subjects who were able to evaluate PK parameters were included in the PK analysis set, and 28 subjects were included in the safety analysis set (Figure 1). The demographics of the participants are summarized in Table 1.
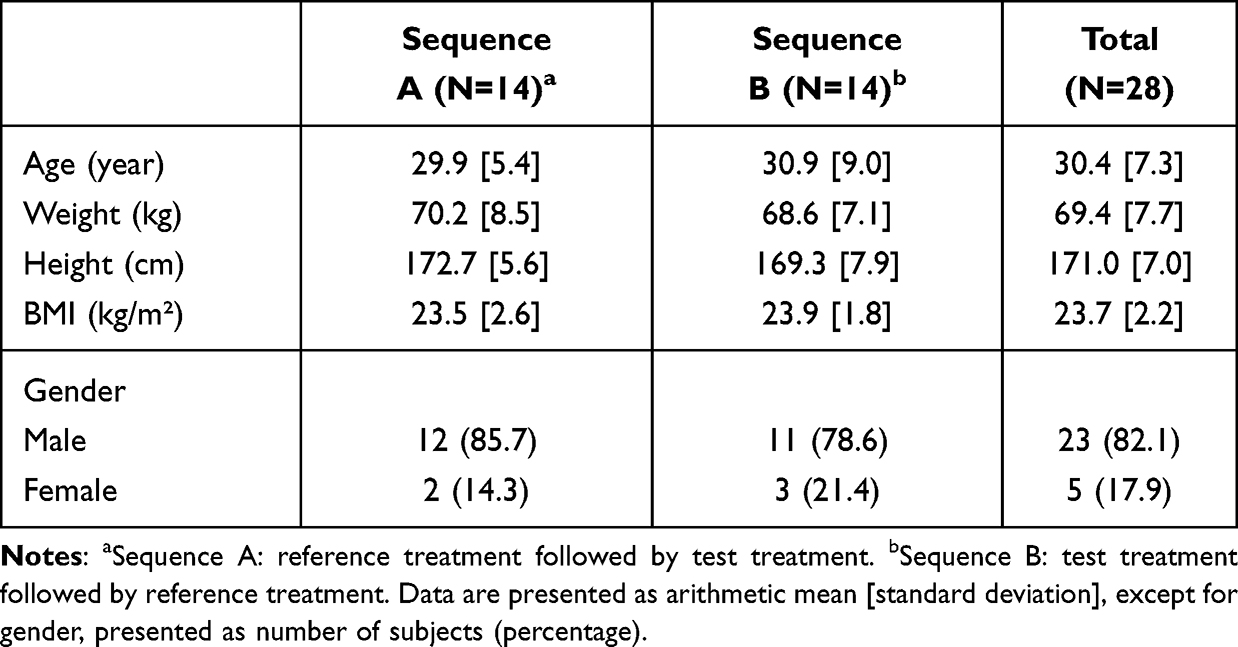 |
Table 1 Demographic Characteristics Between Sequences |
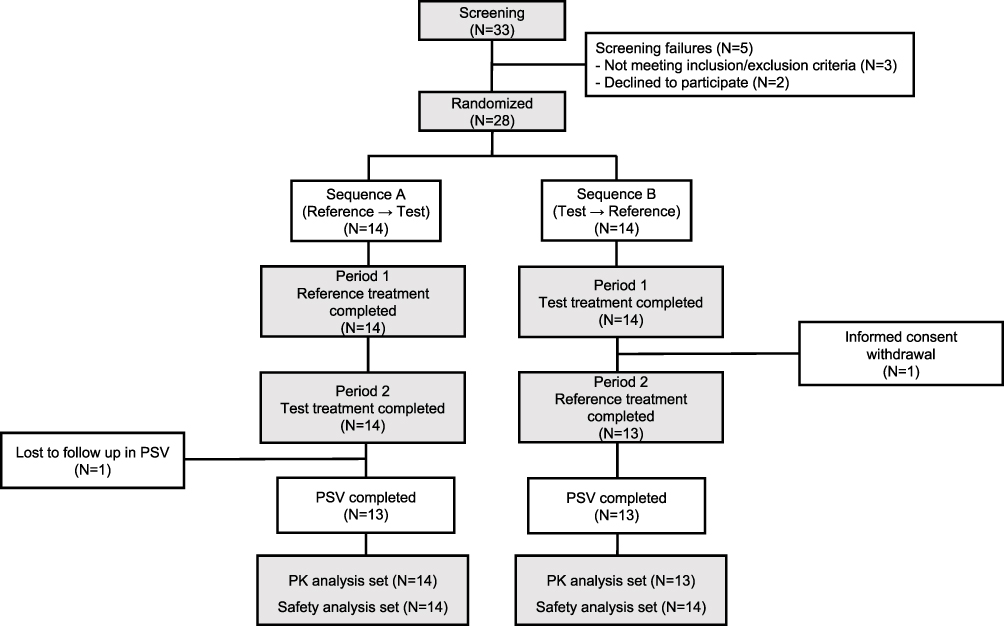 |
Figure 1 Subject dispositions for the sequence A (reference treatment followed by test treatment) and sequence B (test treatment followed by reference treatment). |
Pharmacokinetic Analysis
PKs were evaluated in 27 subjects who completed the single-dose administration of both test and reference treatments. The mean concentration-time curves of the test and reference treatments were similar (Figure 2). The mean ± SD values of the primary PK parameters Cmax and AUClast of the test treatment were 442.02 ± 103.37 μg/L and 3131.08 ± 529.30 μg·h/L, respectively, and those of the reference treatment were 436.29 ± 118.74 μg/L, and 3006.88 ± 514.21 μg·h/L, respectively. The individual values of Cmax and AUClast showed not significantly different between the two treatments (Figure 3). The PK parameters of the test and reference treatments are summarized in Table 2. The GMR (90% CIs) for Cmax and AUClast were 1.0221 (0.9527–1.0967) and 1.0411 (1.0153–1.0677), respectively. These ranges were within the predefined acceptance range of 80–125% (Table 2).
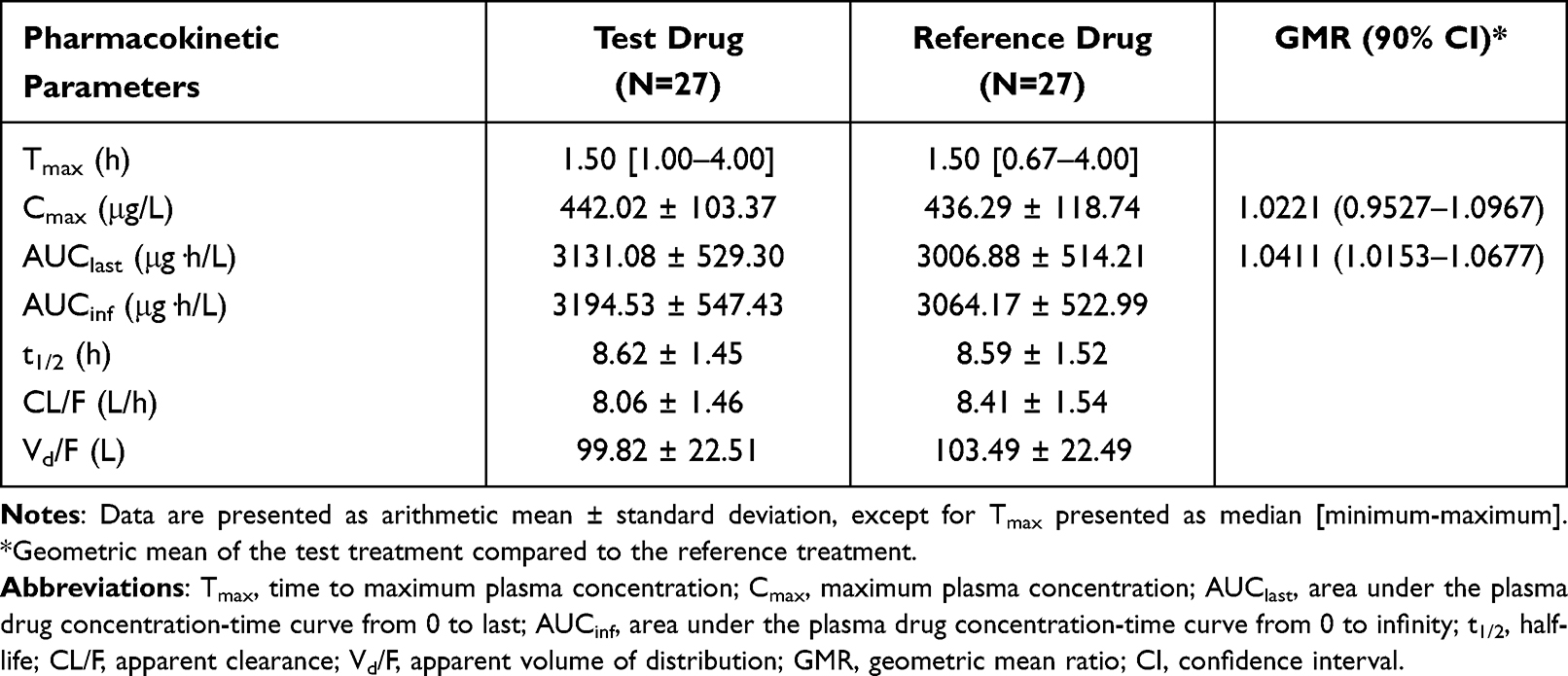 |
Table 2 Summary of Pharmacokinetic Parameters of Empagliflozin in Plasma After Single Oral Dose of Test or Reference Drug |
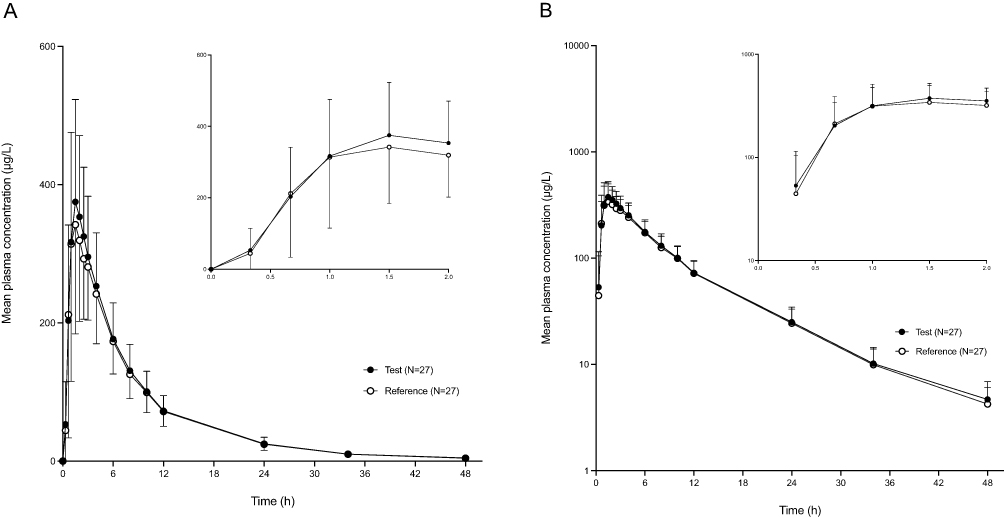 |
Figure 2 Linear (A) and Semi-logarithmic (B) plots of mean plasma concentration-time profiles following single oral administration of 25 mg test or reference treatment. The error bars represent the standard deviations. |
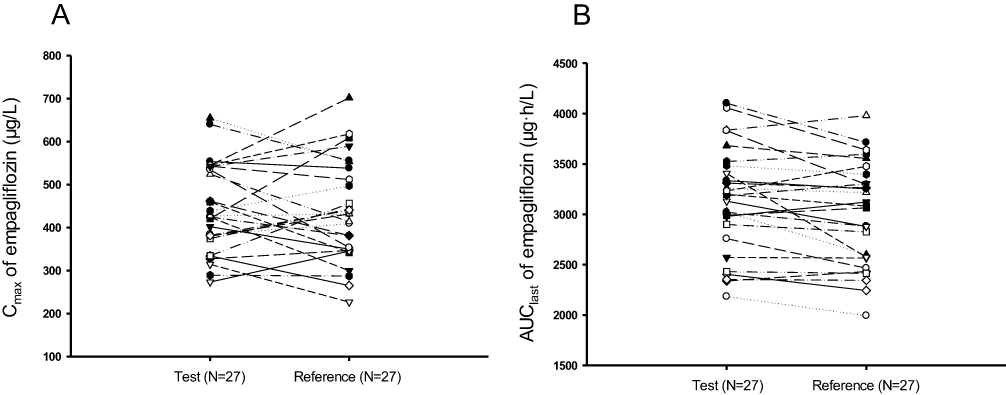 |
Figure 3 Individual changes of primary pharmacokinetic parameters Cmax (A) and AUClast (B) after single oral dose of 25 mg test or reference treatment. Abbreviations: Cmax, maximum plasma concentration; AUClast, area under the plasma drug concentration-time curve from 0 to the last. |
Safety/Tolerability Assessment
Safety and tolerability were assessed in all subjects enrolled in this clinical study. A total of 13 cases of ADRs occurred in six patients, and all of them recovered without sequelae. All ADRs which occurred in this study were mild and previously reported.32 The drug-specific ADRs of empagliflozin such as urine tract infection33 and genital mycotic infections34 were not observed in this study. None of the subjects had serious adverse events (Table 3). There were four gastrointestinal ADRs including two ADRs of nausea and one ADR of vomiting which were observed in the test treatment group and one ADR of nausea which was observed in the reference treatment group. An ADR related to hyperglycemia only occurred once in one subject from test treatment group. The most common ADRs were neurological disorder. There were two ADRs of dizziness in the test treatment group and one in the reference treatment group. There was one ADR event of headache during the test treatment and two during the reference treatment. Moreover, hypoesthesia occurred once in the test treatment and tremor occurred once in the reference treatment. No abnormal findings or clinically significant changes were found in the clinical laboratory tests, vital signs, physical examination, or electrocardiography.
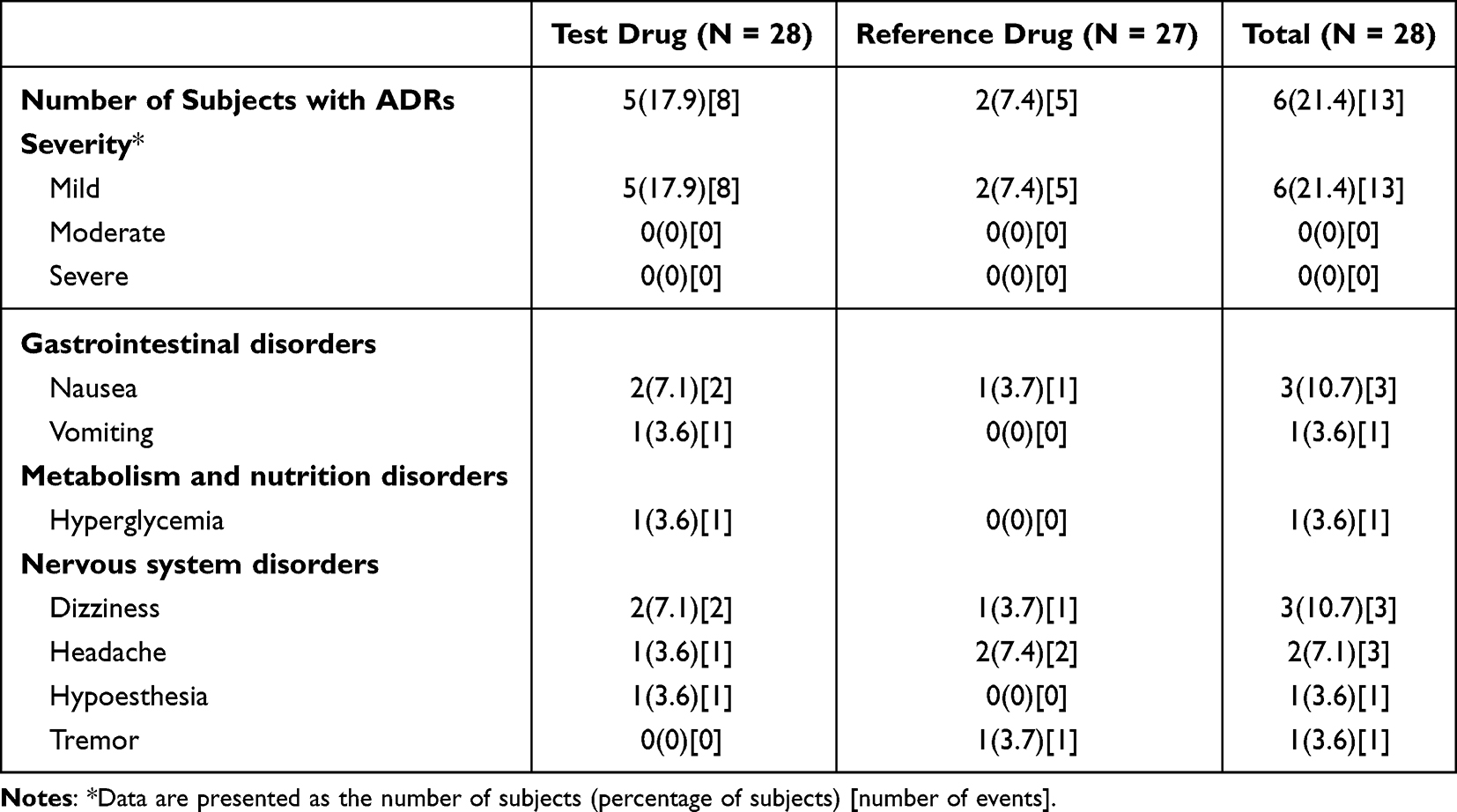 |
Table 3 Summary of All Adverse Drug Reactions (ADRs) by Treatment, Severity, System Organ Class (SOC) and Preferred Term (PT) |
Discussion
CKD-370, a novel drug with similar PK characteristics and improved chemical properties, was developed. It is a single agent of empagliflozin with a solvate of L-proline by cocrystallization. L-proline is an abundant amino acid in foods of animal and plant origin, indicating that addition of this solvate would have no safety problems.35 This study was conducted to compare the PK, tolerability, and safety between the 25 mg test and reference treatment. The reference treatment has two dosages, 10 mg and 25 mg, which are currently approved in Korea. In this study, to test the adequacy of product performance, the highest dosage of 25 mg and the crossover study design were chosen to evaluate and compare PK properties.36
In this clinical study, the similar absorption phase of both treatments was observed with the median Tmax of both formulations were the same 1.50 h, and the Cmax of the test and the reference treatment were 442.02 ± 103.37 μg/L and 436.29 ± 118.74 μg/L, respectively. L-proline is absorbed from the gastrointestinal tract.37 Preclinical tests revealed that empagliflozin L-proline may be broken down to empagliflozin in the digestive system and be absorbed in the form of empagliflozin (data on file). This clinical study revealed similar absorption outcomes.
The plasma concentration-time profiles of both the treatments were similar. The PK parameters were comparable, indicating that empagliflozin with L-proline solvate had similar pharmacokinetic properties to those of empagliflozin. As shown in Table 2, the mean t1/2 of both formulations was 8.62 h and 8.59 h for the test and reference formulations, respectively, indicating that the 7-day washout period was adequate for this study. In addition, the ratio of AUClast to AUCinf of these two formulations was over 80%, suggesting that the time covered by blood sampling was sufficient to adequately describe the plasma concentration-time profile in this study. Furthermore, this clinical study showed that the 90% CIs for the GMRs of Cmax and AUClast were within the accepted bioequivalence range of 80.00% – 125.00%, indicating that the test and reference treatments were pharmacokinetically equivalent.38
The safety profiles of both empagliflozin formulations in this study were similar to those reported previously.32 The frequency of ADRs was similar between the two treatments. Moreover, a previous study on post-marketing surveillance of empagliflozin in South Korea reported that the three most frequent ADRs of empagliflozin in patients with T2DM were frequent urination, vulvovaginal pruritus, and weight decrease, however, these ADRs were not observed in the present study.39 The small sample size in this study limited the extrapolation of drug safety conclusions to the entire population. In addition, although this study confirmed the bioequivalence, safety and tolerability of two empagliflozin formulations, the potential issues associated with the cocrystal formulation should be further studied in more subjects.
Conclusion
In conclusion, the test treatment CKD-370 was well tolerated and showed PK characteristics and safety profiles comparable to those of the reference treatment. No drug-specific ADRs were noted in this study. The results of this study imply that both formulations are bioequivalent.
Data Sharing Statement
The individual deidentified participant data that supporting the published results in this study are available from the corresponding author or sponsor on a reasonable request.
Acknowledgments
Deok Yong Yoon, PhD, was previously employed in the Department of Clinical Pharmacology and Therapeutics, Seoul National University College of Medicine and Hospital. His contribution to this article is based on his prior employment, and the current article does not reflect any position in the Department of Pharmaceutics, Center for Pharmacometrics and Systems Pharmacology, College of Pharmacy, University of Florida.
The abstract of this paper was presented at the 2022 American College of Clinical Pharmacology (ACCP) Annual Conference as a poster presentation with interim findings. The poster’s abstract was published in “Poster Abstracts” in Clinical Pharmacology in Drug Development: https://accp1.onlinelibrary.wiley.com/doi/10.1002/cpdd.1151.
Funding
This study was sponsored by a research grant from Chong Kun Dang Pharmaceutical Corporation, South Korea. The funders had no role in data collection and analysis or preparation of the manuscript.
Disclosure
Shin Jung Park is a full-time employee of Chong Kun Dang Pharmaceutical Corporation. The authors report no other conflicts of interest associated with this work.
References
1. Cho NH, Shaw JE, Karuranga S, et al. IDF diabetes atlas: global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res Clin Pract. 2018;138:271–281. doi:10.1016/j.diabres.2018.02.023
2. Oh SH, Ku H, Park KS. Prevalence and socioeconomic burden of diabetes mellitus in South Korean adults: a population-based study using administrative data. BMC Public Health. 2021;21(1):548. doi:10.1186/s12889-021-10450-3
3. Department, S.R. Number of deaths in South Korea in 2020, by cause of death; 2021. Available from: http://kostat.go.kr.
4. Zheng Y, Ley SH, Hu FB. Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Nat Rev Endocrinol. 2018;14(2):88–98. doi:10.1038/nrendo.2017.151
5. Rieg T, Vallon V. Development of SGLT1 and SGLT2 inhibitors. Diabetologia. 2018;61(10):2079–2086. doi:10.1007/s00125-018-4654-7
6. Ni L, Yuan C, Chen G, et al. SGLT2i: beyond the glucose-lowering effect. Cardiovasc Diabetol. 2020;19(1):98. doi:10.1186/s12933-020-01071-y
7. Leiter LA, Langslet G, Vijapurkar U, et al. Simultaneous reduction in both HbA1c and body weight with canagliflozin versus glimepiride in patients with type 2 diabetes on metformin. Diabetes Ther. 2016;7(2):269–278. doi:10.1007/s13300-016-0163-1
8. Cefalu WT, Leiter LA, Yoon K-H, et al. Efficacy and safety of canagliflozin versus glimepiride in patients with type 2 diabetes inadequately controlled with metformin (CANTATA-SU): 52 week results from a randomised, double-blind, Phase 3 non-inferiority trial. Lancet. 2013;382(9896):941–950. doi:10.1016/S0140-6736(13)60683-2
9. Ridderstrale M, Rosenstock J, Andersen KR, et al. Empagliflozin compared with glimepiride in metformin-treated patients with type 2 diabetes: 208-week data from a masked randomized controlled trial. Diabetes Obes Metab. 2018;20(12):2768–2777. doi:10.1111/dom.13457
10. Rosenwasser RF, Sultan S, Sutton D, et al. SGLT-2 inhibitors and their potential in the treatment of diabetes. Diabetes Metab Syndr Obes. 2013;6:453–467. doi:10.2147/DMSO.S34416
11. Pereira MJ, Eriksson JW. Emerging Role of SGLT-2 Inhibitors for the Treatment of Obesity. Drugs. 2019;79(3):219–230. doi:10.1007/s40265-019-1057-0
12. Georgianos PI, Agarwal R. Ambulatory blood pressure reduction with SGLT-2 inhibitors: dose-response meta-analysis and comparative evaluation with low-dose hydrochlorothiazide. Diabetes Care. 2019;42(4):693–700. doi:10.2337/dc18-2207
13. Brunton SA. The potential role of sodium glucose co-transporter 2 inhibitors in the early treatment of type 2 diabetes mellitus. Int J Clin Pract. 2015;69(10):1071–1087. doi:10.1111/ijcp.12675
14. Packer M, Anker SD, Butler J, et al. Cardiovascular and renal outcomes with empagliflozin in heart failure. N Engl J Med. 2020;383(15):1413–1424. doi:10.1056/NEJMoa2022190
15. Anker SD, Butler J, Filippatos G, et al. Empagliflozin in heart failure with a preserved ejection fraction. N Engl J Med. 2021;385(16):1451–1461. doi:10.1056/NEJMoa2107038
16. Requena-Ibanez JA, Santos-Gallego CG, Rodriguez-Cordero A, et al. Empagliflozin improves quality of life in nondiabetic HFrEF patients. Sub-analysis of the EMPATROPISM trial. Diabetes Metab Syndr. 2022;16(2):102417. doi:10.1016/j.dsx.2022.102417
17. Santos-Gallego CG, Vargas-Delgado AP, Requena-Ibanez JA, et al. Randomized trial of empagliflozin in nondiabetic patients with heart failure and reduced ejection fraction. J Am Coll Cardiol. 2021;77(3):243–255. doi:10.1016/j.jacc.2020.11.008
18. Santos-Gallego CG, Mayr M, Badimon J. SGLT2 Inhibitors in heart failure: targeted metabolomics and energetic metabolism. Circulation. 2022;146(11):819–821. doi:10.1161/CIRCULATIONAHA.122.060805
19. Santos-Gallego CG, Requena-Ibanez JA, San Antonio R, et al. Empagliflozin ameliorates diastolic dysfunction and left ventricular fibrosis/stiffness in nondiabetic heart failure: a multimodality study. JACC Cardiovasc Imaging. 2021;14(2):393–407. doi:10.1016/j.jcmg.2020.07.042
20. Santos-Gallego CG, Requena-Ibáñez JA, Picatoste B, et al. cardioprotective effect of empagliflozin and circulating ketone bodies during acute myocardial infarction. Circ Cardiovasc Imaging. 2023;16(4):e015298. doi:10.1161/CIRCIMAGING.123.015298
21. Kavanagh ON, Croker DM, Walker GM, et al. Pharmaceutical cocrystals: from serendipity to design to application. Drug Discov Today. 2019;24(3):796–804. doi:10.1016/j.drudis.2018.11.023
22. Aguillon AR, Mascarello A, Segretti ND, et al. Synthetic Strategies toward SGLT2 Inhibitors. Org Process Res Dev. 2018;22(4):467–488. doi:10.1021/acs.oprd.8b00017
23. Bolla G, Nangia A. Pharmaceutical cocrystals: walking the talk. Chem Commun. 2016;52(54):8342–8360. doi:10.1039/C6CC02943D
24. Kale DP, Ugale B, Nagaraja CM, et al. Molecular basis of water sorption behavior of rivaroxaban-malonic acid cocrystal. Mol Pharm. 2019;16(7):2980–2991. doi:10.1021/acs.molpharmaceut.9b00227
25. Shinozaki T, Ono M, Higashi K, et al. A novel drug-drug cocrystal of levofloxacin and metacetamol: reduced hygroscopicity and improved photostability of levofloxacin. J Pharm Sci. 2019;108(7):2383–2390. doi:10.1016/j.xphs.2019.02.014
26. Cho HJ, Woo MR, Cho JH, et al. Novel dapagliflozin di-L-proline cocrystal-loaded tablet: preparation, physicochemical characterization, and pharmacokinetics in beagle dogs and mini-pigs. Pharm Dev Technol. 2022;27(3):331–340. doi:10.1080/10837450.2022.2052320
27. FDA. JARDIANCE® (empagliflozin) tablets, for oral use (5.3). Initial US Approval; 2014.
28. Garcia-Ropero A, Badimon JJ, Santos-Gallego CG. The pharmacokinetics and pharmacodynamics of SGLT2 inhibitors for type 2 diabetes mellitus: the latest developments. Expert Opin Drug Metab Toxicol. 2018;14(12):1287–1302. doi:10.1080/17425255.2018.1551877
29. Therapeutic Goods Administration, Department of Health, Australian Government. AusPAR Attachment 2: Extract from the clinical evaluation report for empagliflozin, second round CER. 2014. Available from: https://www.tga.gov.au/sites/default/files/auspar-empagliflozin-150127-cer.pdf.
30. Sarashina A, Koiwai K, Seman LJ, et al. Safety, tolerability, pharmacokinetics and pharmacodynamics of single doses of empagliflozin, a sodium glucose cotransporter 2 (SGLT2) inhibitor, in healthy Japanese subjects. Drug Metab Pharmacokinet. 2013;28(3):213–219. doi:10.2133/dmpk.DMPK-12-RG-082
31. Scheen AJ. Pharmacokinetic and pharmacodynamic profile of empagliflozin, a sodium glucose co-transporter 2 inhibitor. Clin Pharmacokinet. 2014;53(3):213–225. doi:10.1007/s40262-013-0126-x
32. Pathan MDF, Akter N, Selim S, et al. Efficacy and safety of empagliflozin in patients with type 2 diabetes mellitus fasting during ramadan: a real-world study from Bangladesh. Diabetes Metab Syndr Obes. 2022;15:4011–4021. doi:10.2147/DMSO.S380544
33. Yang H, Choi E, Park E, et al. Risk of genital and urinary tract infections associated with SGLT-2 inhibitors as an add-on therapy to metformin in patients with type 2 diabetes mellitus: a retrospective cohort study in Korea. Pharmacol Res Perspect. 2022;10(1):e00910. doi:10.1002/prp2.910
34. Levine MJ. Empagliflozin for type 2 diabetes mellitus: an overview of phase 3 clinical trials. Curr Diabetes Rev. 2017;13(4):405–423. doi:10.2174/1573399812666160613113556
35. Leal J, Teixeira-Santos L, Pinho D, et al. l-proline supplementation improves nitric oxide bioavailability and counteracts the blood pressure rise induced by angiotensin II in rats. Nitric Oxide. 2019;82:1–11. doi:10.1016/j.niox.2018.10.007
36. Davit B, Braddy AC, Conner DP, et al. International guidelines for bioequivalence of systemically available orally administered generic drug products: a survey of similarities and differences. AAPS J. 2013;15(4):974–990. doi:10.1208/s12248-013-9499-x
37. PubChem. PubChem Compound Summary for CID 145742, Proline. Bethesda (MD): National Library of Medicine (US), National Center for Biotechnology Information; 2004. Available from: https://pubchem.ncbi.nlm.nih.gov/compound/Proline.
38. Agency EM. Guideline on the Investigation of Bioequivalence; 2010.
39. Moon JS, Kim NH, Na JO, et al. Safety and effectiveness of empagliflozin in Korean patients with type 2 diabetes mellitus: results from a nationwide post-marketing surveillance. Diabetes Metab J. 2022;47(1):82–91.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.