Back to Journals » Drug Design, Development and Therapy » Volume 20
Comparison of the Effect of Different Administration Sequence of Propofol and Remifentanil on Sedation/Anesthesia During Gastroscopy in Obese Patients
Authors Tang J, Zhong Z, Jiang H, Li J, Liu J, Duan S, Liang S, Wu Z, Wang M ![]() , Hu D
, Hu D
Received 8 January 2026
Accepted for publication 10 April 2026
Published 25 April 2026 Volume 2026:20 594697
DOI https://doi.org/10.2147/DDDT.S594697
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Tin Wui Wong
Jieke Tang,1,* Zhao Zhong,1,* Hongxue Jiang,1 Jinying Li,2 Jingwen Liu,2 Shan’e Duan,1 Shuqing Liang,1 Zhenpeng Wu,3 Mengxia Wang,1 Donghua Hu1
1Department of Anesthesiology, The First Affiliated Hospital of Jinan University, Guangzhou, Guangdong, People’s Republic of China; 2Department of Digestive Endoscopy Center, The First Affiliated Hospital of Jinan University, Guangzhou, Guangdong, People’s Republic of China; 3Department of Metabolic and Bariatric Surgery, The First Affiliated Hospital of Jinan University, Guangzhou, Guangdong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Mengxia Wang, Department of Anesthesiology, The First Affiliated Hospital of Jinan University, No. 613, Huangpu West Avenue, Tianhe District, Guangzhou, Guangdong, 510630, People’s Republic of China, Email [email protected] Donghua Hu, Department of Anesthesiology, The First Affiliated Hospital of Jinan University, No. 613, Huangpu West Avenue, Tianhe District, Guangzhou, Guangdong, 510630, People’s Republic of China, Email [email protected]
Purpose: Obesity is associated with an elevated risk of hypoxemia during endoscopic procedures performed under anesthesia. However, whether the sequence of drug administration — specifically the order of propofol and remifentanil — affects the incidence of hypoxemia remains unclear. This study was designed to evaluate whether a novel administration sequence, in which propofol precedes remifentanil, can decrease the incidence of hypoxemia in obese individuals during endoscopy.
Patients and Methods: This prospective, single center, randomized controlled clinical trial recruited 296 obese patients scheduled for sedative/anesthesia gastroscopy prior to bariatric surgery. Patients were randomly assigned to either novel administration sequence with propofol-remifentanil (P-R) group or conventional administration of remifentanil-propofol (R-P) group. The primary outcome was the incidence of hypoxemia. Secondary outcomes included the lowest peripheral oxygen saturation (L-SpO2) during the procedure, hemodynamic parameters at six time points, and additional perioperative events.
Results: 284 patients were included in the analysis with 142 in each group. Hypoxemia occurred in 22 patients (15.5%) in the P-R group, and 42 patients (29.6%) in the R-P group (Relative Risk [RR], 1.44; 95% confidence interval [CI], 1.13 to 1.79; P = 0.007). The L-SpO2 during the procedure was significantly higher in the P-R group than in the R-P group (median [interquartile range, IQR], 94.0% [91.0 to 97.0] vs 93.0% [87.7 to 95.0]; P < 0.001). The P-R sequence technique was also associated with more stable hemodynamic profiles, shorter induction time, the start of drug administration to scope insertion and recovery time, improved patient’s satisfaction. Particularly, minimal respiratory depression was observed in subgroups such as body mass index (BMI) ≥ 40 kg/m2.
Conclusion: Propofol first and followed by remifentanil administration sequence significantly decreased the incidence of hypoxemia and increased the L-SpO2 in obese patients for their anesthesia/sedation gastroscopy.
Clinical Trial Registration: ChiCTR2400084998.
Keywords: administration sequence, gastroscopy, hypoxemia, obesity, propofol, remifentanil
Introduction
Obesity is increasing worldwide and has become a major global public health concern. According to the World Obesity Atlas 2025, the number of individuals affected by obesity is projected to 1.13 billion adults globally by 2030. 1 Therefore, effective treatment strategies for obesity are of major clinical importance. Bariatric surgery has been consistently recognized as the most effective and durable treatment for obesity.2,3 Preoperative endoscopy is routinely recommended before bariatric surgery because it can identify lesions or inflammatory conditions that may affect the choice of surgical technique, preoperative management, and the need for additional procedure. As a result, endoscopic evaluation has become a routine practice prior to the bariatric surgery.4–7
At the present, most patients prefer to undergo endoscopic procedures under sedation.8–10 For gastroscopy, sedation with preservation of spontaneous breathing is considered safe and highly effective.11 Hypoxemia is the most common sedation-related adverse event.8 Previous studies have reported that the incidence of hypoxemia in patients with normal body weight ranges from 1.8% to 69%.12 Obesity is associated with an increased risk of periprocedural apnea and hypoxemia,8,11,13 with the incidence of severe hypoxemia reported to be nearly six times higher than that in individuals with normal body mass index (BMI).14 In a study by Wang et al, the incidence of hypoxemia in obese patients with a mean BMI of 29.9 kg/m2 was 21.2%.12 Furthermore, for patients combined with STOP-Bang score ≥ 5, the incidence of hypoxemia has been reported to reach up to 54.6%.15
In a previously published clinical study, the incidence of hypoxemia during sedation for gastroscopy in obese patients with a median BMI of 39.2 kg/m2 was 27.5% using the novel Li anesthetic protocol for obesity (LAPO).16 This finding represented a meaningful reduction. Additionally, the median duration of anesthesia induction in obese patients was relatively prolonged (114 s), which prompted consideration of the timing and overlap of drug peak effects. Remifentanil, a synthetic opioid that acts directly on µ-receptors, is characterized by a rapid onset and a short time to peak effect.17 Following the traditional sequence of administering an analgesic prior to a sedative, remifentanil is typically given before propofol.18–20 However, the approximately two-minute induction period may cause the peak analgesic effect of remifentanil to occur earlier than the point at which gastric stimulation is most intense. Consequently, the analgesic effect from the initial remifentanil dose may be attenuated or no longer present at the time of greatest procedural stimulus. To date, no studies have yet evaluated the impact of the drug administration sequence — whether propofol is administered before or after remifentanil — on sedation outcomes in obese patients undergoing gastroscopy.
The aim of this study was to determine whether the sequence of anesthetic administration influences the efficacy of sedation/anesthesia in obese patients undergoing gastroscopy. It was hypothesized that administration of propofol followed by remifentanil would reduce the incidence of hypoxemia during sedation/anesthesia for gastroscopy, compared with the conventional administration of remifentanil followed by propofol.
Materials and Methods
Ethics and Trial Registration
This prospective, single-center, single-blind randomized controlled study was approved by the Scientific Research Ethics Committee of the First Affiliated Hospital of Jinan University (Ethics Number: KY-2024-066) and registered with the Chinese Clinical Trial Registry (ChiCTR2400084998). Eligible participants provided informed consent prior to randomization. Data were collected in accordance with the principles of the Declaration of Helsinki and the CONSORT guidelines from May 2024 to March 2025 at the First Affiliated Hospital of Jinan University.
Participant Recruitment
Obese patients who underwent sedation/anesthesia for gastroscopy before bariatric surgery were recruited. Inclusion criteria included: age 18–60 years, BMI ≥ 30 kg/m2, and American Society of Anesthesiologists (ASA) physical status I to III.
Exclusion criteria were defined as follows: 1. Patients with severe cardiopulmonary disease, including heart failure, stroke with neurological deficits, or under dialysis. 2. Patients with a history of abnormal recovery from anesthesia, such as delayed awakening after anesthesia, unplanned secondary tracheal intubation, and unplanned transfer to the intensive care unit (ICU). 3. Patients allergic to known emulsions or opioids. 4. Patients with alcohol dependence. 5. Lactating patients, or those with long-term preoperative use of opioids or nonsteroidal anti-inflammatory drugs (NSAIDs). 6. Patients on long-term β-blocker therapy with a resting heart rate < 50 beats per minute (bpm). 7. Uncooperative patients, loss to follow-up, or those deemed by investigators as unlikely to complete the study. 8. Procedure time of gastroscopy was more than 30 min.
Randomization and Blinding
The randomization sequence was generated by the anesthesiologist who was not involved in the specific implementation of the study using SPSS 17.0 (IBM Corp., USA) software at a 1:1 ratio.
This study was conducted as a single-blind clinical trial. The anesthesiologist responsible for drug administration was aware of the group assignment due to the distinct physical characteristics of the agents, with propofol appearing as a milky emulsion and remifentanil solution as a clear, colorless liquid. However, the other anesthesiologist, nurses, endoscopists and patients who observed the outcomes were unaware of the group assignment.
Study Intervention
In the propofol-remifentanil (P-R) group, propofol was given intravenously at a rate of 2.5 mg/s, with an initial dose of 100 mg, followed by remifentanil intravenously with a uniform fixed dose of 20 μg (diluted to 4 μg/mL in normal saline, 5 mL in total) at 1 μg/s. Additional propofol (5–10 mg) was administered if eyelash reflex disappeared after completion of remifentanil intravenously; If the eyelash reflex remained present, propofol was further titrated until loss of eyelash reflex, and the Modified Observer’s Assessment of Alertness/Sedation Score (MOAA/S) of 0 was reached, at which point gastroscopy was initiated. The patients in the remifentanil-propofol (R-P) group were intravenously injected a fixed dose of remifentanil (20 μg) and then a titrated propofol, with all other procedures identical to those in the P-R group. During gastroscopy, supplemental propofol (10–20 mg) each time was administered as required based on patient response.
Anesthesia and Postoperative Management
The anesthesia and postoperative management as described previously.16 All patients adhered to a standardized fasting protocol and preparation before anesthesia including establishment of peripheral venous access, oral administration 10 mL of dyclonine mucilage for oropharyngeal topical anesthesia, positioning in a left head-up ramped position (head height 15–30°), preoxygenation through a nasal cannula at a flow of 5 L/min for more than 3 min using an easy-to-create mask, and routine monitoring of blood pressure, peripheral oxygen saturation (SpO2), electrocardiogram and heart rate (HR), and respiratory rate (R).
Anesthesia was performed by an anesthesiologist according to group-specific protocols. While the patient was falling asleep, an anesthesiologist supported the jaw thrust with EC clamp technique; when the respiratory rate was less than 10 bpm or the SpO2 was less than 95%, manual right hypochondrial compression (MRHC) was performed as described previously.16 After completion of the procedure and recovery of orientation, the patient was transferred to the post-anesthesia care area. When the standard of leaving the room was reached (Aldrete score ≥ 9) and the observation time was more than 30 min, the patient could leave.
The anesthetic procedure was performed by the same two experienced anesthesiologists, the endoscopy was performed by the endoscopists with at least 5 years of experience.
Data Collection and Outcome Assessment
Vital signs were recorded using a video monitoring system. Anesthesia nurses documented baseline characteristics, injection pain, body movement, cough, vomiting, aspiration, and satisfaction. Telephone follow-up which was performed 24 hours after endoscopy.
The primary outcome was the incidence of hypoxemia during gastroscopy, defined as SpO2 below 90% and lasting for more than 10 s.16
The secondary outcomes were included the following: 1. The lowest peripheral oxygen saturation (L-SpO2) during anesthesia. 2. SpO2, HR and R of the baseline (T0), before induction (T1), MOAA/S score = 0 (T2), the gastroscope was inserted (T3), the gastroscope was removed (T4), and during awakening (T5). 3. Induction dose and total dose of propofol. 4. Induction time defined as the start of drug administration to MOAA/S score of 0. Operation time, defined as the time of insertion and removal of the gastroscopy from the mouth. Recovery time, defined as the time form the end of operation to eyes opening on verbal command. Recovery time of orientation, defined as the time from the end of operation to be able to follow commands and touch the tip of the nose with the fingers. Time available to discharge, defined as the time from the end of operation to Aldrete score ≥ 9. 5. Duration of hypoxemia, injection pain, body movement, cough, aspiration of patient. 6. The same sedation/anesthesia gastroscopy will be chosen for review. 7. Patients, endoscopists and anesthesiologists’ satisfaction with the effect of anesthesia quality, assessed using a scale of 0 to 10 (0 = very dissatisfied, 10 = very satisfied). 8. Intraoperative awareness, evaluated using the modified Brice questionnaire after recovery of orientation and at 24 h post-operation.21
Sample Size Calculation
According to the previous study,16 the incidence of hypoxemia in obese patients was 27.5% receiving intravenous remifentanil followed by propofol. Based on pre-experiment result, the incidence of hypoxemia was 12% with the novel administration sequence. Using PASS 15.0 software, set α = 0.05, 1-β = 0.8, and it was estimated that 134 patients per group. Assuming a 5% dropout rate, a total of 284 patients were required, with 142 in each group.
Statistical Analysis
GraphPad Prism 10.0 (GraphPad Software, CA, USA) was used for statistical analysis. For data with continuous variables, the Shapiro–Wilk test was preferred to assess normality. Data were presented as mean ± standard deviation (SD) if normally distributed or as median [interquartile range] if non-normally distributed. For categorical variables, data were presented as numbers (%). Specifically, the Fisher’s exact test was performed to compare the rates of the two groups, such as the incidence of hypoxemia in the overall cohort and in certain subgroups, the proportion of males in each group. Mann–Whitney U-test was used to compare the outcomes of continuous values such as L-SpO2, age. Two-way analysis of variance (ANOVA) with Bonferroni’s multiple comparisons test was used to compare vital signs at six time points between the two groups. For all analyses, a two-sided P < 0.05 was considered statistically significant.
Results
Patients
A total of 296 obese patients were enrolled, of whom 12 were excluded (2 declined participation, 2 had severe arrhythmia, 3 had a mental disorder, 5 had an ASA physical status > III) (Figure 1). Consequently, the remaining 284 patients were randomly divided into two groups: the remifentanil-propofol group (R-P, n = 142) and propofol-remifentanil group (P-R, n = 142). Baseline characteristics, such as gender, age, and BMI were comparable between the two groups (Table 1).
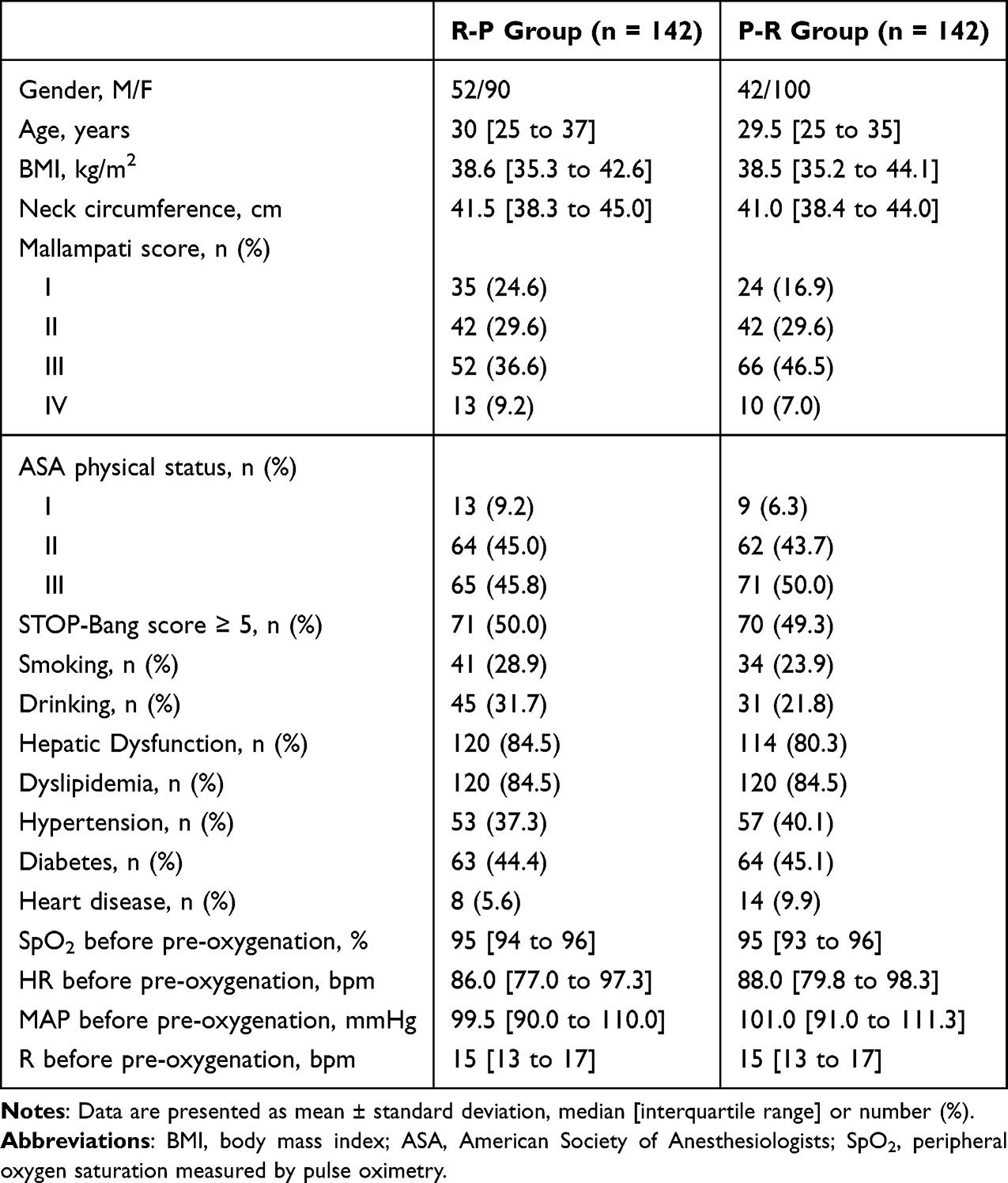 |
Table 1 Baseline Characteristics of the Intention-to-Treat Population |
 |
Figure 1 Flow diagram of selection and inclusion of participants. Abbreviations: ASA, American Society of Anesthesiologists. |
The Incidence of Hypoxemia
For the primary outcome, the incidence of hypoxemia was significantly lower in the P-R group than in the R-P group. Hypoxemia occurred in 22 patients (15.5%) in the P-R group and in 42 patients (29.6%) in the R-P group (Relative Risk [RR], 1.44; 95% confidence interval [CI], 1.13 to 1.79; P = 0.007) (Figure 2).
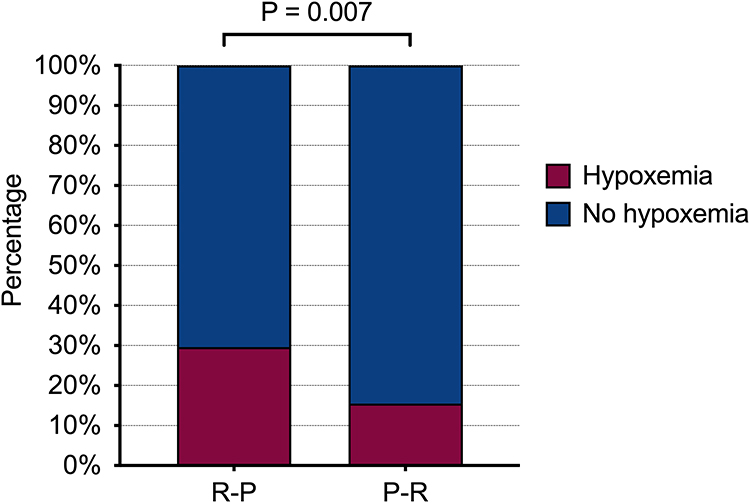 |
Figure 2 The incidence of hypoxemia of R-P and P-R sequence for obesity during sedative/anesthesia gastroscopy. The incidence of hypoxemia under P-R group (15.5%) was significantly lower than that under the R-P group (29.6%) (RR, 1.44; 95% CI, 1.13 to 1.79; P = 0.007). Abbreviations: R-P, remifentanil-propofol; P-R, propofol-remifentanil; RR, relative risk; CI, confidence interval. |
The L-SpO2 During Anesthesia
The L-SpO2 during anesthesia was recorded using video monitoring. The L-SpO2 was significantly higher in the P-R group compared to the R-P group (94.0% [91.0 to 97.0] vs 93.0% [87.7 to 95.0]; P < 0.001) (Figure 3).
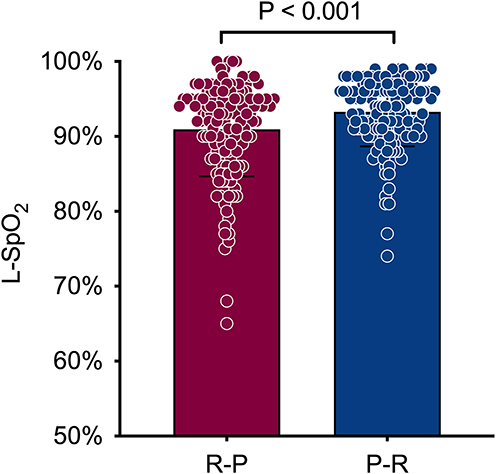 |
Figure 3 L-SpO2 in sedation/anesthesia for gastroscopy in obese patients. The L-SpO2 in the P-R group was significantly higher than in the R-P group (median [IQR], 94.0% [91.0 to 97.0] vs 93.0% [87.7 to 95.0]; P < 0.001). Abbreviations: L-SpO2, the lowest peripheral oxygen saturation during the anesthesia; P-R, propofol-remifentanil; R-P, remifentanil-propofol; IQR, interquartile range. |
Hemodynamic Data
In this study, we assessed hemodynamic data by two-way repeated-measures ANOVA (Figure 4). The patient’s SpO2, HR and R of six time points were presented. Those data had significant interaction effect of group and time. Therefore, we conducted comparisons between groups at each time point. At T4, SpO2 was significantly higher in the P-R group than in the R-P group (96.2% vs 94.6%; P = 0.009) (Figure 4A). Although at T3, SpO2 in the P-R group was a bit lower than in the R-P group (98.1% vs 99.2%; P < 0.001) (Figure 4A), it was unconvinced that the decreases were clinically meaningful. For HR, we observed higher values in the P-R group than in the R-P group at T2 (87.4 bpm vs 82.6 bpm; P = 0.007) and T3 (86.0 bpm vs 80.7 bpm; P = 0.003) (Figure 4B). At the same time, R was higher in the P-R group at T3 (16.5 bpm vs 14.5 bpm; P = 0.003) (Figure 4C).
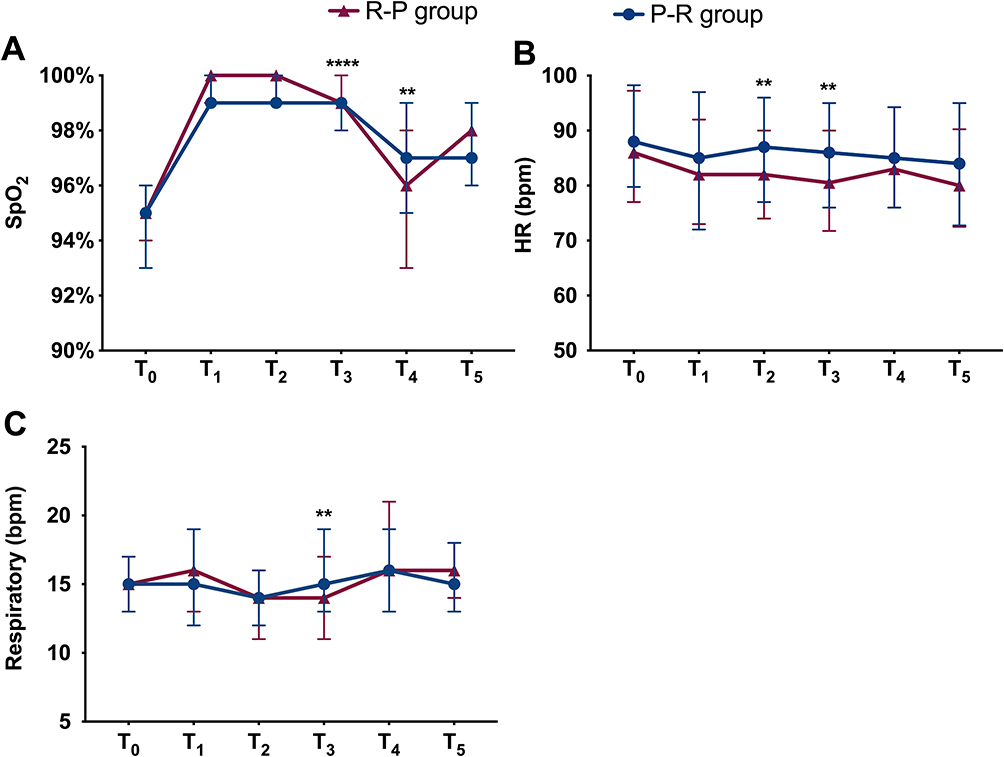 |
Figure 4 The changes in hemodynamic parameters of patients were observed at six time points. (A) Peripheral oxygen saturation (SpO2); (B) heart rate (HR); (C) respiratory rate (R). Data are presented as median and interquartile range. **P < 0.01, **** P < 0.0001. Abbreviations: T0, at the baseline; T1, before induction; T2, MOAA/S score = 0; T3, the gastroscope was inserted; T4, the gastroscope was removed; T5, during awakening. |
Procedure-Related Outcomes
Outcomes related to the procedure, such as induction dose and total dose of propofol, induction time, operation time, recovery time are presented in Table 2.
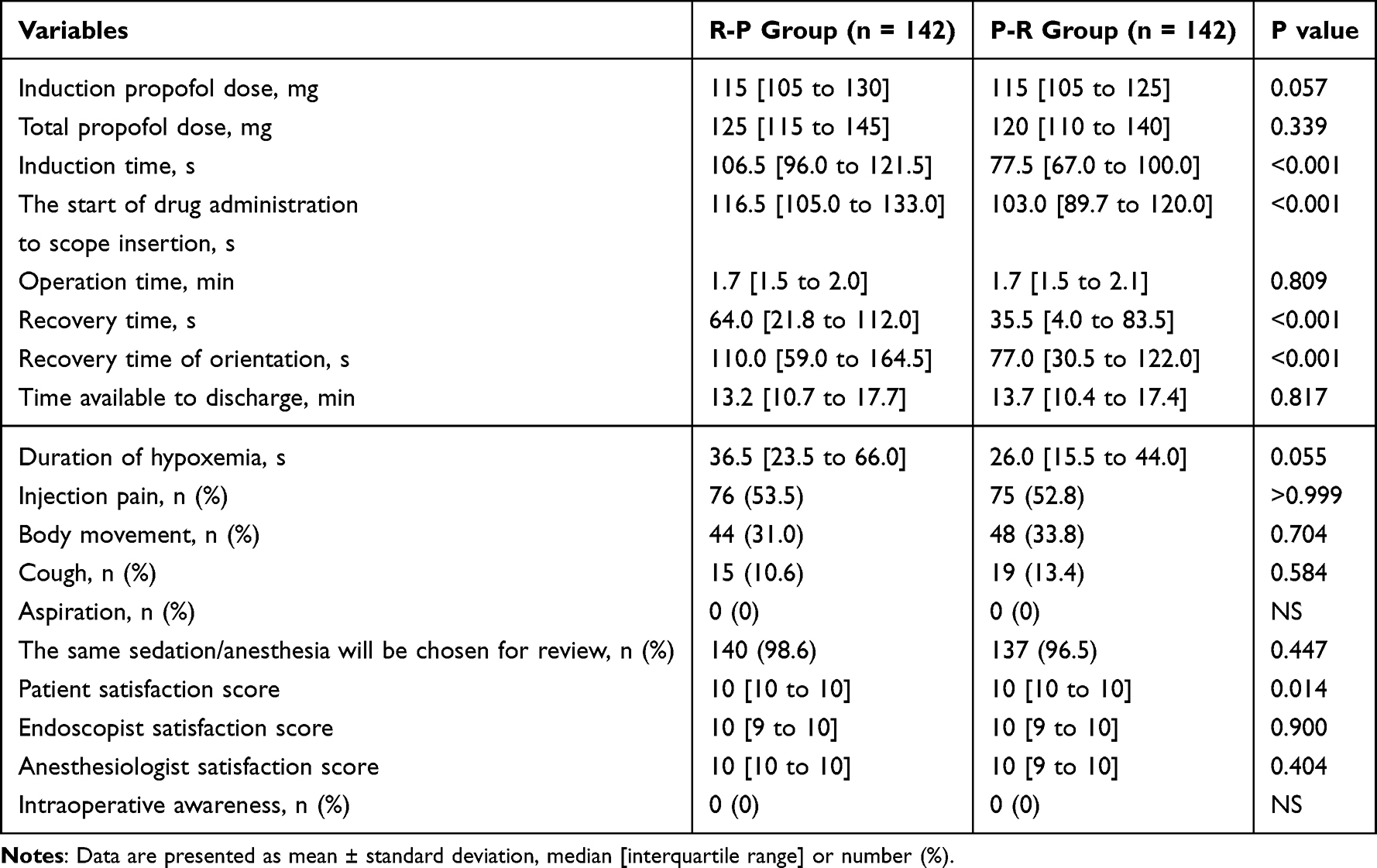 |
Table 2 Procedural Characteristics and Postoperative Scores |
As compared with the R-P group, the P-R group showed a significantly shorter induction time (77.5 [67.0 to 100.0] s vs 106.5 [96.0 to 121.5] s; P < 0.001), the start of drug administration to scope insertion (103.0 [89.7 to 120.0] s vs 116.5 [105.0 to 133.0] s; P< 0.001), recovery time (35.5 [4.0 to 83.5] s vs 64.0 [21.8 to 112.0] s; P < 0.001) and recovery time of orientation (77.0 [30.5 to 122.0] s vs 110.0 [59.0 to 164.5] s; P < 0.001).
For the induction propofol dose, the study did not demonstrate a statistically significant less in it, but rather a strong trend towards a decrease (R-P vs P-R: 115 [105 to 130] mg vs 115 [105 to 125] mg; P = 0.057). This was also the case for the duration of hypoxemia (R-P vs P-R: 36.5 [23.5 to 66.0] s vs 26 [15.5 to 44.0] s; P = 0.055).
The groups did not differ in the use of total propofol dose (R-P vs P-R: 125 [115 to 145] mg vs 120 [110 to 140] mg; P = 0.339), the operation time (R-P vs P-R: 1.7 [1.5 to 2.0] min vs 1.7 [1.5 to 2.1] min; P = 0.809), time available to discharge (R-P vs P-R: 13.2 [10.7 to 17.7] min vs 13.7 [10.4 to 17.4] min; P = 0.817).
Adverse Effects
We compared the incidence of adverse events and the preferred method of sedation for future gastroscopy between the two groups (Table 2). There was no significant difference in the incidence of injection pain, body movement, cough, and aspiration. Intraoperative awareness was assessed using the modified Brice questionnaire, and no cases of awareness were reported in either group.
Satisfaction with the Effect of Anesthesia
Patients in the P-R group had higher satisfaction scores than those in the R-P group (10 [10 to 10] vs 10 [10 to 10]; P = 0.014). Although 98.6% of patients in the R-P group and 96.5% of patients in the P-R group indicated that they would choose the same sedation method for their next gastroscopy, the difference between groups was not statistically significant (P = 0.447). For endoscopist satisfaction, there was no significant trend (10 [9 to 10] vs 10 [9 to 10]; P = 0.900) between the two groups. The similar result was found for anesthesiologist satisfaction (10 [10 to 10] vs 10 [9 to 10]; P = 0.404).
Exploratory Analyses
To further explore the beneficial effect of sequential propofol-remifentanil administration technique on the incidence of hypoxemia, subgroup analyses were performed based on patient characteristics such as BMI, neck circumference, Mallampati score, and other clinical factors (Figure 5). The propofol-first sequence was associated with a reduced incidence of hypoxemia in obese patients with BMI ≥ 40 kg/m2, neck circumference ≥ 40 cm, Mallampati score < III, STOP-Bang score ≥ 5, hepatic dysfunction, dyslipidemia, hypertension, diabetes, and without heart disease.
 |
Figure 5 Forest plot of relative risk of hypoxemia across patient subgroups. P values were obtained by Fisher’s exact test, and methods used to compute CIs according to Koopman asymptotic score. Abbreviations: RR, relative risk; CI, confidence interval. |
Discussion
Previous studies on the sequence of anesthetic administration have primarily focused on first-attempt failure during emergency intubation,22 and the different sequences of gastroenteroscopy in patients with difficult airway.23 Research investigating the sequence of anesthetic administration during sedation/anesthesia for gastroscopy remains limited. In this study, we found that among obese patients undergoing gastroscopic sedation/anesthesia, the novel propofol-remifentanil sequence significantly reduced the incidence of hypoxemia compared with the conventional remifentanil-propofol sequence. Furthermore, this sequence improved the lowest peripheral oxygen saturation (L-SpO2) during anesthesia, stabilized hemodynamic parameters, shortened induction time, the start of drug administration to scope insertion time, recovery times, and enhanced patient satisfaction. Notably, subgroup analyses further indicated greater respiratory benefits with the propofol-first sequence in patients with BMI ≥ 40 kg/m², neck circumference ≥ 40 cm, and certain other subgroups.
Administering Propofol Followed by Remifentanil Was Associated with a Lower Incidence of Hypoxemia and Higher L-SpO2 During Gastroscopy
During gastroscopy, the most uncomfortable and technically challenging phases typically occur early in the procedure — namely endoscope insertion and passage through the pharynx, as well as adequate gastric insufflation.10,24 These steps occur within the initial phase of the procedure, corresponding to advancement from the mouth to the cardia, which generally requires approximately 15 s.25 Intravenous anesthetic/sedative is typically administered in small, titrated doses to reach the desired depth of sedation.26 This approach facilitates alignment of peak effect coincides with the period of maximal procedural stimulation, while minimizing excessive overlap of peak effects during less stimulating phases and thereby reducing the risk of respiratory depression.
The observed differences between the two administration sequences can be explained by the pharmacodynamic properties of propofol and remifentanil. Propofol acts rapidly, with an onset time of 0.5–1 minute and a peak effect within 1–2 minutes, followed by a short duration of action lasting 4–8 minutes.27 Remifentanil similarly exhibits a fast onset of approximately 1 minute and a short context-sensitive half-time of 3–4 minutes.28 In propofol-remifentanil sequence, the timing of the respective peak effects appeared to align better with procedural stimulation. Specifically, following an induction time of 77.5 s, the peak effect of propofol was already established at the onset of gastroscopy. With an interval of approximately 103.0 s from the start of drug administration to scope insertion, remifentanil administered at about the 40th s of induction reached peak effect near the time of insertion (approximately 63 s from the scope insertion). This timing allowed adequate coverage of the most stimulating phases of the procedure, including the initial 15 s and the overall duration of gastroscopy (approximately 1.7 min).
In contrast, the conventional remifentanil-propofol sequence resulted in overlapping peak effects near the end of induction (approximately 106.5 s), producing a deeper level of anesthesia during a time of relatively low procedural stimulation. This overlap may have contributed to respiratory suppression and the higher incidence of hypoxemia observed. Moreover, the peak effect of remifentanil administered at the onset of induction may have diminished by the time of scope insertion (approximately 116.5 s), resulting in insufficient coverage of procedural stimulation. These findings suggest that optimizing drug administration timing to better match procedural demands represents a practical strategy for reducing hypoxemia risk while maintaining procedural conditions and patient comfort.
Administering Propofol Followed by Remifentanil Induced Moderate Sedation Appropriate for Obese Patients
Moderate sedation is recommended for most endoscopic procedures,29 and was applied in the present study. The propofol-remifentanil sequence exhibited more stable HR and R compared with the remifentanil-propofol sequence (Figure 4B and C), which was reflected in more stable SpO2 levels during the procedure (Figure 4A). Clinically, this translated into shorter recovery times — both for regaining orientation and overall recovery — in the P-R group (Table 2). These findings support the advantage of the propofol-remifentanil sequence in achieving adequate yet safer sedation in obese patients undergoing gastroscopy.
Given the relatively high rate of body movement observed during the procedure, no instances of intraoperative awareness were reported in either group, as assessed by the modified Brice questionnaire. These findings alleviate concerns regarding insufficient depth of moderate sedation. Moreover, patient satisfaction was higher in the propofol-remifentanil (P-R) group than in the remifentanil-propofol (R-P) group. This may be attributed to better synchronization between the depth of anesthesia and the procedural stimulation, resulting in improved comfort and faster recovery (Table 2). Collectively, these findings suggest that the propofol-remifentanil sequential administration not only enhances physiological stability but also improves the overall patient experience during gastroscopy.
The Propofol–Remifentanil Administration Sequence Demonstrated Superior Outcomes in Specific Patient Subgroups
Considering established risk factors for hypoxemia and the clinical characteristics of obesity,11,16 post hoc exploratory analyses were performed. The propofol-remifentanil sequence was associated with a lower incidence of hypoxemia in certain subgroups, such as participants with a BMI ≥ 40 kg/m2, neck circumference ≥ 40 cm, and Mallampati score < III (Figure 5). However, because the number of patients with heart disease was limited, precluding a definitive evaluation of the effect of the propofol-remifentanil administration strategy in this subgroup. These findings provide preliminary evidence to support individualized anesthesia protocol for obese individuals undergoing gastroscopy.
Limitations
Several limitations should be acknowledged. First, the single-center study and relatively limited sample size may introduce inherent biases and affect the generalizability. Future multi-center studies with larger cohorts are needed to validate these findings. Second, due to the distinct physical properties and dosage requirements of propofol and remifentanil, blinding the attending anesthesiologists was not feasible. Inevitably, the knowledge of group allocation could have introduced performance bias. To minimize this effect, the anesthesiologist responsible for supporting the jaw was not involved in drug administration. Third, although we performed subgroup analyses and observed some findings, it should be acknowledged that these analyses were post-hoc exploratory, rather than pre-specified. As such, the results should be interpreted as hypothesis-generating and intended to provide preliminary insights for clinical practice, rather than confirmatory evidence. Fourth, this study did not continuously monitor more sensitive indicators of stress response, such as heart rate variability (HRV)30 nor did it include objective measures of consciousness, such as the bispectral index (BIS).31 Incorporating these monitoring parameters in future studies may provide a more comprehensive assessment of anesthetic depth and physiological responses.
Conclusion
In obese patients undergoing preoperative gastroscopy prior to bariatric surgery, the propofol-first sequential administration strategy resulted in a lower incidence of hypoxemia and higher L-SpO2 during the procedure compared with the remifentanil-first sequence. These clinical benefits were particularly evident in selected high-risk subgroups. Further research is warranted to determine whether the propofol-first sequence can be extended to other populations with reduced respiratory reserve or an increased risk of hypoxemia — such as elderly or critically ill patients — and to confirm its broader clinical applicability.
Data Sharing Statement
The data associated with this study are available in electronic form upon reasonable request. Interested researchers may contact the corresponding author, Mengxia Wang (wangmengxia@ jnu.edu.cn).
Acknowledgments
The authors would like to express sincere gratitude to the participants in this study. We also thank the staff of the Department of Digestive Endoscopy Center, Department of Anesthesiology and the Department of Metabolic and Bariatric Surgery of The First Affiliated Hospital of Jinan University for their invaluable assistance.
Funding
This study was supported by the Medical Scientific Research Foundation of Guangdong Province of China (B2025066).
Disclosure
All authors declare no conflicts of interest related to this work.
References
1. Obesity W. World Obesity Atlas 2025, March. Available from: https://www.worldobesityday.org/assets/downloads/World_Obesity_Atlas_2025.pdf. 2025;
2. Jirapinyo P, Hadefi A, Thompson CC, et al. American society for gastrointestinal endoscopy-european society of gastrointestinal endoscopy guideline on primary endoscopic bariatric and metabolic therapies for adults with obesity. Gastrointestinal Endoscopy. 2024;99(6):867–885.e64. doi:10.1016/j.gie.2023.12.004
3. Mohammed N, Buckley A, Elsheikh M, et al. Bariatric surgery in the treatment of patients with obesity and type 1 diabetes: a retrospective study of clinical data. Diabetes Obesity Metab. 2021;23(7):1562–13. doi:10.1111/dom.14369
4. Kanat BH, Doğan S. Is gastroscopy necessary before bariatric surgery? World J Gastrointest Endosc. 2022;14(1):29–34. doi:10.4253/wjge.v14.i1.29
5. Angrisani L, Santonicola A, Iovino P, Ramos A, Shikora S, Kow L. Bariatric surgery survey 2018: similarities and disparities among the 5 IFSO chapters. Obes Surg. 2021;31(5):1937–1948. doi:10.1007/s11695-020-05207-7
6. Wölnerhanssen BK, Meyer-Gerspach AC, Nussbaumer R, et al. Prospective clinical cohort study: low incidence of Barrett esophagus but high rate of reflux disease at 5-year follow-up after sleeve gastrectomy versus Roux-en-Y gastric bypass. Surg Obes Relat Dis. 2023;19(7):707–715. doi:10.1016/j.soard.2023.02.012
7. Dimou F, Huynh S, Dakin G, et al. Nasal positive pressure with the SuperNO2VA™ device decreases sedation-related hypoxemia during pre-bariatric surgery EGD. Surg Endosc. 2019;33(11):3828–3832. doi:10.1007/s00464-019-06721-1
8. Sidhu R, Turnbull D, Haboubi H, et al. British society of gastroenterology guidelines on sedation in gastrointestinal endoscopy. Gut. 2024;73(2):219–245. doi:10.1136/gutjnl-2023-330396
9. Triantafyllou K, Sidhu R, Tham T, et al. Sedation practices in gastrointestinal endoscopy: European Society of Gastrointestinal Endoscopy (ESGE) survey. Endoscopy. 2024;56(12):964–974. doi:10.1055/a-2416-4866
10. Yu B, Hazlewood PJ, Yin X, et al. Effect of electroacupuncture on discomfort during gastroscopy: a study protocol for a randomized controlled trial. Trials. 2022;23(1):364. doi:10.1186/s13063-022-06165-4
11. Sundararaman L, Goudra B. Sedation for GI endoscopy in the morbidly obese: challenges and possible solutions. J Clin Med. 2024;13(16). doi:10.3390/jcm13164635
12. Wang L, Zhang Y, Han D, et al. Effect of high flow nasal cannula oxygenation on incidence of hypoxia during sedated gastrointestinal endoscopy in patients with obesity: multicentre randomised controlled trial. BMJ. 2025;388(e080795). doi:10.1136/bmj-2024-080795
13. Zheng L, Wang Y, Ma Q, et al. Efficacy and safety of a subanesthetic dose of esketamine combined with propofol in patients with obesity undergoing painless gastroscopy: a prospective, double-blind, randomized controlled trial. Drug Des Devel Ther. 2023;17:1347–1356. doi:10.2147/dddt.S408076
14. Laffin AE, Kendale SM, Huncke TK. Severity and duration of hypoxemia during outpatient endoscopy in obese patients: a retrospective cohort study. Can J Anaesth. 2020;67(9):1182–1189. doi:10.1007/s12630-020-01737-x
15. Riccio CA, Sarmiento S, Minhajuddin A, Nasir D, Fox AA. High-flow versus standard nasal cannula in morbidly obese patients during colonoscopy: a prospective, randomized clinical trial. J Clin Anesth. 2019;54:19–24. doi:10.1016/j.jclinane.2018.10.026
16. Wang M, Tang J, Pan Z, et al. Prospective single-arm study of remifentanil-propofol anesthesia with manual right hypochondrial compression for painless gastroscopy in obese patients. Drug Des Devel Ther. 2025;19:877–890. doi:10.2147/dddt.S498238
17. Michelsen LG, Hug CC. The pharmacokinetics of remifentanil. J Clin Anesth. 1996;8(8):679–682. doi:10.1016/s0952-8180(96)00179-1
18. Ahn JH, Kim D, Chung IS, Lee JJ, Lee EK, Jeong JS. Pre-administration of remifentanil in target-controlled propofol and remifentanil anesthesia prolongs anesthesia induction in neurosurgical patients: a double-blind randomized controlled trial. Medicine. 2019;98(3):e14144. doi:10.1097/md.0000000000014144
19. Kim J, Kim D, Lee HG. Effect-site concentration of remifentanil for preventing propofol injection pain during induction of balanced anesthesia. Anesth Pain Med. 2020;15(2):152–156. doi:10.17085/apm.2020.15.2.152
20. Liu M, Wu H, Yang D, et al. Effects of small-dose remifentanil combined with index of consciousness monitoring on gastroscopic polypectomy: a prospective, randomized, single-blinded trial. Trials. 2018;19(1):392. doi:10.1186/s13063-018-2783-4
21. Valdez MA, Tellor Pennington BR, Politi MC, et al. Refining the modified Brice questionnaire: patient perspectives and clarity enhancement. J Clin Anesth. 2025;105:111876. doi:10.1016/j.jclinane.2025.111876
22. Catoire P, Driver B, Prekker ME, Freund Y. Effect of administration sequence of induction agents on first-attempt failure during emergency intubation: a Bayesian analysis of a prospective cohort. Acad Emerg Med. 2025;32(2):123–129. doi:10.1111/acem.15031
23. Sun H, Zhang L, Liu Z, Zhang Y, Li J, Pang K. Study on different sequences of painless gastroenteroscopy in patients with difficult airway. Biotechnol Genet Eng Rev. 2024;40(2):1379–1388. doi:10.1080/02648725.2023.2193774
24. Lee SH, Park YK, Cho SM, Kang JK, Lee DJ. Technical skills and training of upper gastrointestinal endoscopy for new beginners. World J Gastroenterol. 2015;21(3):759–785. doi:10.3748/wjg.v21.i3.759
25. Sugimoto K, Osawa S. ‘Four-position method’ makes beginner endoscopists aware of spatial positioning of the left hand to master upper gastrointestinal endoscopy. Endosc Int Open. 2020;8(10):E1225–e1230. doi:10.1055/a-1197-6418
26. Analgesia TASoATFoMPSa. Practice guidelines for moderate procedural sedation and analgesia 2018. Anesthesiology. 2018;128(3):437–479. doi:10.1097/aln.0000000000002043
27. Lin OS. Sedation for routine gastrointestinal endoscopic procedures: a review on efficacy, safety, efficiency, cost and satisfaction. Intest Res. 2017;15(4):456–466. doi:10.5217/ir.2017.15.4.456
28. Battershill AJ, Keating GM. Remifentanil. Drugs. 2006;66(3):365–385. doi:10.2165/00003495-200666030-00013
29. Vargo JJ, DeLegge MH, Feld AD, et al. Multisociety sedation curriculum for gastrointestinal endoscopy. Gastrointest Endosc. 2012;76(1):e1–25. doi:10.1016/j.gie.2012.03.001
30. Rudics E, Buzás A, Pálfi A, et al. Quantifying stress and relaxation: a new measure of heart rate variability as a reliable biomarker. Biomedicines. 2025;13(1). doi:10.3390/biomedicines13010081
31. Zhang X, Zhu T, Chen G, et al. Respiratory-related safety profiles of ciprofol (cipepofol) for anesthesia/sedation in Chinese elderly patients undergoing gastroscopy: a multicenter, parallel controlled clinical trial (REST trial). J Clin Anesth. 2025;106:111976. doi:10.1016/j.jclinane.2025.111976.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect of Remimazolam Tosilate on Respiratory Depression in Elderly Patients Undergoing Gastroscopy: A Multicentered, Prospective, and Randomized Study
Hu B, Jiang K, Shi W, Xiao S, Zhang S, Zhang Y, Zhou Y, Tan C, Tan S, Zou X
Drug Design, Development and Therapy 2022, 16:4151-4159
Published Date: 5 December 2022
Prospective Single-Arm Study of Remifentanil-Propofol Anesthesia with Manual Right Hypochondrial Compression for Painless Gastroscopy in Obese Patients
Wang M, Tang J, Pan Z, Jiang H, Hu D, Zhu B, Liang Z, Zhao X, Li Y
Drug Design, Development and Therapy 2025, 19:877-890
Published Date: 11 February 2025
Safety and Effectiveness of Electroacupuncture During Colon Endoscopic Submucosal Dissection: A Randomized Controlled Trial
Zhang J, Zhang H, Zheng J, Niu C, Zhu S, Hu H, Lu Y, Zhu M
Journal of Pain Research 2025, 18:1221-1229
Published Date: 13 March 2025
Comparison of Esketamine/Propofol and Sufentanil/Propofol on Intraoperative Hypoxemia During Bronchoscopy: A Randomized Trial
Huang X, Li X, Sun Y, Wu A, Ai P
Drug Design, Development and Therapy 2025, 19:4429-4436
Published Date: 27 May 2025