Back to Journals » Neuropsychiatric Disease and Treatment » Volume 17
Comparison of Residual Depressive Symptoms, Functioning, and Quality of Life Between Patients with Recurrent Depression and First Episode Depression After Acute Treatment in China
Authors Zu S, Wang D, Fang J, Xiao L, Zhu X, Wu W, Wang G, Hu Y
Received 8 May 2021
Accepted for publication 27 August 2021
Published 1 October 2021 Volume 2021:17 Pages 3039—3051
DOI https://doi.org/10.2147/NDT.S317770
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Taro Kishi
Si Zu,1 Dong Wang,1 Jiexin Fang,1 Le Xiao,2 Xuequan Zhu,2 Wenyuan Wu,3 Gang Wang,2,4 Yongdong Hu1
1Department of Psychiatry, Beijing Chaoyang Hospital, Capital Medical University, Beijing, People’s Republic of China; 2The National Clinical Research Center for Mental Disorders & Beijing Key Laboratory of Mental Disorders, Beijing Anding Hospital, Capital Medical University, Beijing, People’s Republic of China; 3Department of Psychiatry, Tongji Hospital of Tongji University, Shanghai, People’s Republic of China; 4Advanced Innovation Center for Human Brain Protection, Capital Medical University, Beijing, People’s Republic of China
Correspondence: Gang Wang
The National Clinical Research Center for Mental Disorders & Beijing Key Laboratory of Mental Disorders, Beijing Anding Hospital, Capital Medical University, No. 5 Ankang Lane, Xicheng District, Beijing Anding Hospital, Beijing, 100088, People’s Republic of China
Email [email protected]
Yongdong Hu
Department of Psychiatry, Beijing Chaoyang Hospital, Capital Medical University, No. 8 Gongtinanlu, Chaoyang District, Beijing Chaoyang Hospital, Beijing, 100020, People’s Republic of China
Tel +86-10-85231754
Email [email protected]
Objective: This prospective study aimed to investigate the prognosis and rehabilitation of patients with recurrent depression and first episode depression after acute treatment in China.
Methods: A total of 434 patients with first-episode or recurrent depression who received acute treatment respectively from sixteen hospitals in thirteen cities in China were enrolled in this prospective study. All patients were followed up for 6 months after acute treatment. The following data were collected at baseline period and 1, 3, and 6 months after acute treatment: general information of patients, medication information and patient’s condition changes, brief 16-item quick inventory of depressive symptomatology self-report (QIDS-SR16), patient health questionnaire-15 (PHQ-15), quality of life enjoyment and satisfaction questionnaire-short form (Q-LES-Q-SF), Sheehan disability scale (SDS) and digit symbol substitution test (DSST).
Results: During the baseline period, there was a significant difference in QIDS-SR16 between recurrent patients and first-episode patients (p < 0.05), and there was no significant difference in other indicators (p > 0.05). At one month after acute treatment, there were significant differences in the total QIDS-SR16 score, the total Q-LES-SF score, the social life score, and the family life/home responsibilities score of SDS in patients with recurrent depression and first-episode depression (p < 0.05). At three months after acute treatment, there were significant differences in the total Q-LES-SF score and social life score of SDS in patients with recurrent depression and first-episode depression (p < 0.05). At six months after acute treatment, there were significant differences in the total QIDS-SR16 score, the social life score, and the total Q-LES-SF score in patients with recurrent depression and first-episode depression (p < 0.05). Compared with that data during the baseline period, the QIDS-SR16 scores and the SDS scores of all patients decreased, and the Q-LES-SF scores of all patients gradually increased as time went on during the consolidation period.
Conclusion: The recurrent patients have more severe social function impairment, depressive symptoms, and lower life quality than that of the first-episode depressed patients. Given the negative impact of depressed symptom on recurrent patient, more attention should be paid to the treatment of recurrent patient and recurrence prevention of first episode patient.
Keywords: depression, first-episode, recurrent patient, prognosis
Background
Depression is a mood disorder characterized by persistent depression, loss of interest, and pleasure.1 At present, there are 350 million patients with depression in the world. It is expected that depression will become the second-largest potential disease which will threaten human physical and mental health by 2020.1 Half of the patients with depression could get temporary treatment by the routine primary prevention treatment; however, 20% to 40% of the patients only have substantial improvement over 24 months.2 Frank et al defined recurrent depression as a new episode of depression after a recovery cycle. Recovery refers to the complete remission after a depressive episode, which lasts for 2 weeks at least.3 The average time from the second episode to the first episode was three years.4 Each person with depression has an average of five to nine separate depressive episodes in his or her lifetime.5,6 In a long-term follow-up of depressed patients who responded to electroconvulsive therapy (ECT), investigators found a 42.3% recurrence of depression in their total sample over an 8-year follow-up data.7
Depression can cause certain damage to the physical health, psychological state, and sexual function of patients.8 Besides, patients with depression often have cognitive dysfunction especially in patients with refractory depression.9,10 Approximately 55% of patients with major depressive disorder respond to initial antidepressant treatment, with remission in 33% of these patients.10 However, patients who respond or remit to antidepressant treatment often have residual symptoms, such as anxiety, depression, sleep problems, fatigue, cognitive dysfunction, etc, which may interfere with their somatic and social function, affect their quality of life, and increase the risk of recurrence.11 Therefore, the observation of residual symptoms is of great significance for the judgment of prognosis and the choice of treatment plan. Previous studies have shown that the patients with less depressive symptoms often have better social function, social relation and role function. For many patients, even if the depressive symptoms are relieved, the impaired function cannot be completely recovered.12 The degree of functional impairment in patients with depression is closely related to the quality of life and the severity of symptoms.13 The patients with more obvious depressive symptoms often have worse quality of life.14 In China, the quality of life of outpatients with depression is also poor.15 Therefore, the goal of treatment of depression is not only to alleviate the symptoms of depression, but also to improve the social function, life function and quality of life of patients.16 Pharmacological treatment of depression is almost exclusively aimed at relieving mood symptoms, the treatment of the remaining symptoms as well as patient function also require further exploration.17
It has been demonstrated that there are some differences in cognitive function, memory function between the first-episode patients and the recurrent patients;17 Talarowska et al18 reported that the cognitive function of recurrent patients was worse than that of first-episode patients. Other studies showed that there was no significant difference in the severity of anxiety and depression between first-episode patients and recurrent patients, but the performance of recurrent patients was significantly worse than that of first-episode patients in Wisconsin Card Sorting Test (WCST).19 These studies contribute to understand the differences in symptoms and cognition between first-episode patients and recurrent patients, and to develop more specific treatment to complete remission and prevent recurrence in the management of depression. In the western countries, there are many studies on the difference between first-episode patients and recurrent patients, but there are few systematic studies in China. Due to cultural differences, it is worth exploring whether the comparison results of the two groups of patients in various aspects will be different from the studies in other countries. Additionally, long-term follow-up comparative data require to be further supplemented and in-depth analyzed after treatment in the acute phase in China. In this prospective study, we observed the changes of assessment indicators of patients with first-episode or recurrent depression during the first 6 months of follow-up after acute treatment in China, and then evaluate the prognosis and rehabilitation of these patients, which may contribute to understand these change characteristics of Chinese patients and provide specific treatment plan for the depressed patients in China.
Methods
Patients
This study was conducted in thirteen cities of China from June 2016 to December 2016, and the eligible patients who received acute treatment respectively from sixteen hospitals were enrolled in this study. These patients were diagnosed with depressive disorders according to the ICD-10.20 All participants provided written informed consent. This study was approved by Ethics Committee of Beijing Chaoyang Hospital, Beijing Anding Hospital, and Tongji Hospital of Tongji University ((2016) Scientific research No. (37) - 201640fs-2), complies with the principles of the Declaration of Helsinki.
Inclusion Criteria
(1) over 18 years old; (2) conformity with the ICD-10 diagnosis of a depressive episode (F32) or recurrent depressive disorder (F33); (3) According to the visual analogue scale (VAS), current state (depression) of patients recovered 50% or more compared with the beginning of the onset of this episode; (4) According to the doctor’s judgment, antidepressants were the main treatment for patients. The categories of “antidepressants” include tricyclic and tetracyclic antidepressants, SSRI antidepressants, SNRI antidepressants, NaSSA antidepressants, NDRI antidepressants (bupropion, etc.), SARI antidepressants (trazodone, nefazodone, etc.), α2-adrenergic receptor antagonists and 5-HT1, 5-HT2 receptor antagonists (mianserin, etc.), NARI antidepressants (rui, etc.), and other classes such as Agomelatine. (6) After the depressive episode, the patient received antidepressants for 8 weeks (inclusive) to 12 weeks (inclusive), and the cumulative days of drug withdrawal during that period was less than 14 days; (7) According to the doctor’s judgment, the patient’s education level and reading comprehension ability of Chinese did not affect the accuracy and speed of completing the self-rating scale by themselves; (8) The patients were followed up for at least 6 months.
Exclusion Criteria
(1) A clear history of manic or hypomanic episodes, or a diagnosis of bipolar affective disorder, schizophrenia, schizoaffective disorder, or psychiatric disorders associated with other diseases; (2) Patients had been enrolled in the pre-trial study; (3) Based on the investigator’s judgment, patients could not follow the study protocol.
Assessment Instruments
Brief 16-Item Quick Inventory of Depressive Symptomatology Self-Report (QIDS-SR16)
QIDS-SR16,21 a patient self-rating scale with 16 items, is a good tool for measuring depressive symptoms. The QIDS-SR16 bases on the nine symptom domains (Sleep, Sad Mood, Appetite/Weight, Concentration/Decision Making, Self-view, Thoughts of Death or Suicide, General Interest, Energy Level, and Restlessness/Agitation) that define a major depressive episode. The “Sleep, Appetite/Weight, and Restlessness/Agitation” domains are based upon two or more questions. The other domains are each rated by a single item. Each domain is scored from 0 to 3 and reflects increasing amounts of pathology, so the total test score ranges from 0 to 27.22
Patient Health Questionnaire-15 (PHQ-15)
PHQ-1523 is a patient self-rating scale. A total of 15 items of the Patient Health Questionnaire-15 (PHQ-15) are used to assess the severity of patients’ somatic symptoms. Each item score ranges from 0 to 2 and the total score ranges from 0 to 30, and the higher the PHQ-15 scores meant the more severe the physical symptoms.
Quality of Life Enjoyment and Satisfaction Questionnaire-Short Form (Q-LES-Q-SF)
The life quality of patients was assessed using the Quality of Life Enjoyment and Satisfaction Questionnaire-Short Form (Q-LES-Q-SF),24 which included 16 question items reflecting subjective satisfaction with the quality of life in the past week. The 1–14 items (scored from 1 to 5) reflect the subjective satisfaction of all aspects of life quality (including physical health; social relations; ability to function in daily life; ability to get around physically; mood; family relations; sexual drive and interest; ability to work on hobbies, work, leisure time activities; economic status; household activities; living/housing situation; and overall sense of well-being); the 15–16 items reflect the daily medical level and overall life satisfaction. The total score ranged from 0 to 70 comes from the sum of scores of 1–14 items. A higher score meant higher life quality.25
Sheehan Disability Scale (SDS)
The patients were administered the Sheehan Disability Scale (SDS)20,26 to assess the extent to which depression interfered with functioning in work/school, household, relationship, and social roles in the worst month of the past year. Responses are scored according to a 0-to-10 visual analog scale (none (0), mild (1–3), moderate (4–6), severe (7–9), and very severe (10)), and the total score ranges from 0 to 30. A higher score means more functional impairment.
Digit Symbol Substitution Test (DSST)
Cognitive functioning was assessed using the Digit Symbol Substitution Test (DSST: executive functioning, speed of processing, and attention). The test score ranges from 0 to 133.27
Sample Size Calculation and Sampling Method
There was no formal sample size calculation in this study. The estimated sample size was based on the feasibility of the study. Patients were selected by continuous sampling in each center.
Research Process
Before the study began, all medical staff in different hospitals would be required to gather together and learn the standard diagnosis and evaluation conduction. Residual symptoms referred to subthreshold depressive symptoms after a depression attack, which usually occurred after treatment but not cured. All patients were followed up for 6 months after acute treatment (Figure 1). The following data were collected at baseline period and 1, 3, and 6 months after acute treatment: general information of patients, medication information and patient’s condition changes, QIDS-SR16, PHQ-15, Q-LES-Q-SF, SDS, and DSST. During the follow-up period, the patient’s condition was stable, and could enter the next round of observation. The patient would withdraw from this study if the condition resumed. All assessments were conducted by an independent worker who was blinded to this study. All assessments have a validated Chinese version.
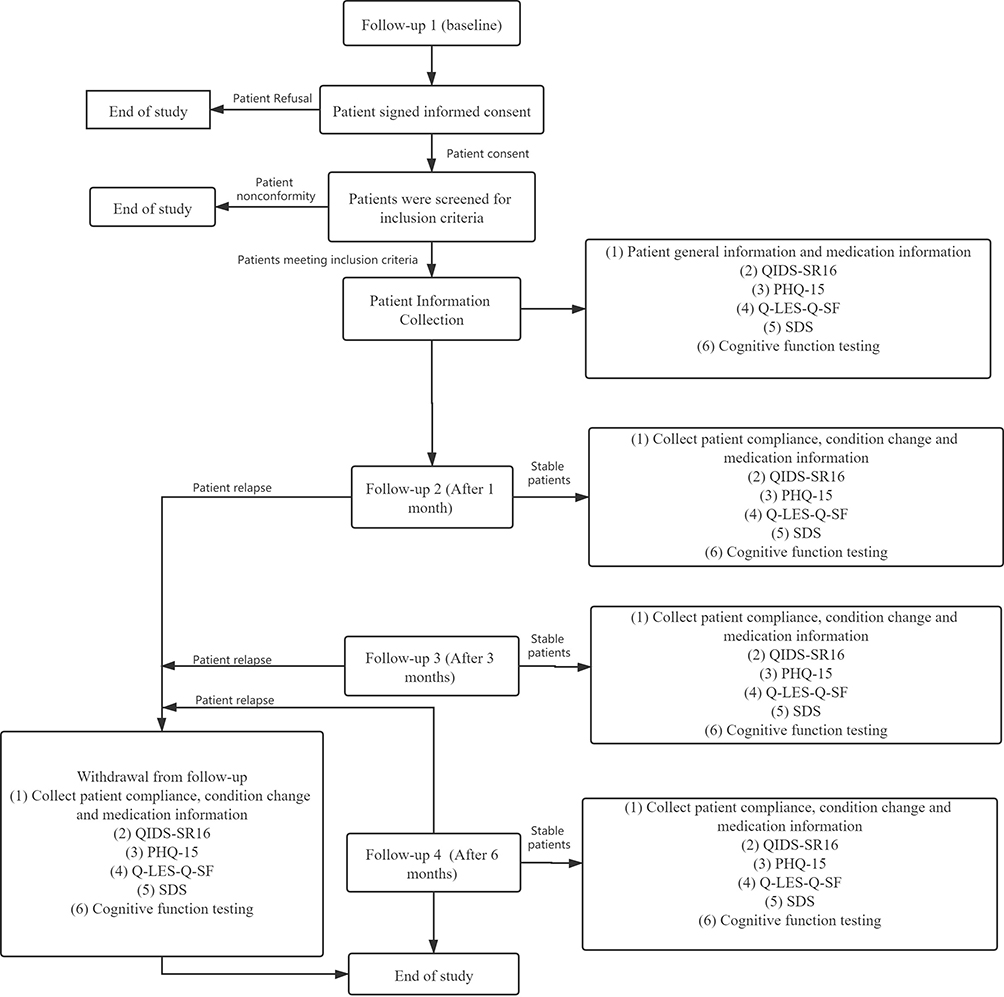 |
Figure 1 Research flow chart. |
Statistical Analysis
Data was analyzed by Statistic analysis system (SAS9.4). Normally distributed measurement data were expressed as mean ± standard deviation (SD), while non-normally distributed measurement data were expressed as median (interquartile range), and the comparisons were examined by Student t-test and nonparametric rank-sum test (non-parametric distribution). The categorical or hierarchical data were expressed as n (%), and the differences between the two groups were examined by the CMH test. Negative binomial regression was used to control for non-normally distributed dependent variables. Multiple comparisons were corrected using the Bonferroni method. After adjusting for covariates with significant statistical differences between groups in baseline assessment and other univariate analyses, we adjusted estimates of differences between groups and P < 0.05 was considered statistically significant.
Results
General Information of Patients
A total of 434 patients were enrolled, during follow-up, 6 patients were diagnosed with bipolar affective disorder and were excluded from analysis. Finally, a total of 428 patients were calculated, including 261 (61.0%) patients with the first depressive episode and 167 (39.0%) patients with recurrent depressive disorder. There were no significant differences between the two groups in age, sex, years of education, the duration of antidepressants treatment in this episode, and mode of administration (p > 0.05), but the duration of the current episode was significantly different (p < 0.001) (Table 1).
 |
Table 1 General Information of Patients |
Differences in Symptoms Between Recurrent and First-Episode Depression Patients at Baseline After Acute Treatment
Comparing the baseline symptoms of patients with first-episode depression and recurrent depression, there were no significant differences in the total score of QIDS-SR16, PHQ15, SDS, DSST test (p > 0.05); however, the total scores of Q-LES-SF in patients with recurrent depression were significantly lower than that of patients with first-episode depression (p < 0.05) (Table 2).
 |
Table 2 Differences in Symptoms Between Recurrent and First-Episode Depression Patients at Baseline and 1, 3, 6 Months After Acute Treatment |
Differences in Symptoms Between Recurrent and First-Episode Depression Patients at One Month After Acute Treatment
At one month after acute treatment, the total QIDS-SR16 score, the social life score and the family life/home responsibilities score in SDS of patients with recurrent depression was significantly higher than that of patients with first-episode depression (p < 0.05), the total Q-LES-SF score of patients with recurrent depression was significantly lower than that of patients with first-episode depression (p < 0.05). There was no significant difference between the two groups in the assessment of the remaining aspects (p > 0.05) (Table 2).
Differences in Symptoms Between Recurrent and First-Episode Depression Patients at Three Months After Acute Treatment
At three months after acute treatment, the total Q-LES-SF score of patients with recurrent depression was significantly lower than that of patients with first-episode depression (p < 0.05). The social life score in SDS of patients with recurrent depression was significantly higher than that of patients with first-episode depression (p < 0.05) (Table 2).
Differences in Symptoms Between Recurrent and First-Episode Depression Patients at Six Months After Acute Treatment
At six months after acute treatment, the total QIDS-SR16 score, the social life score in SDS of patients with recurrent depression was significantly higher than that of patients with first-episode depression (p < 0.05), the total Q-LES-SF score of patients with recurrent depression was significantly lower than that of patients with first-episode depression (p < 0.05).
In summary, the follow-up results showed that the recovery results (depressive symptoms, quality of life, and personal impact on society) of first-episode patients were better than that of the recurrent patients.
Follow-Up QIDS-SR16 Data in the Consolidation Phase
The current results showed that the QIDS-SR16 scores of all patients decreased over time, which indicated that the depressive symptoms of all patients were alleviated. The QIDS-SR16 scores of the recurrent patients were higher than that of the first episode patients at each time point (Figure 2).
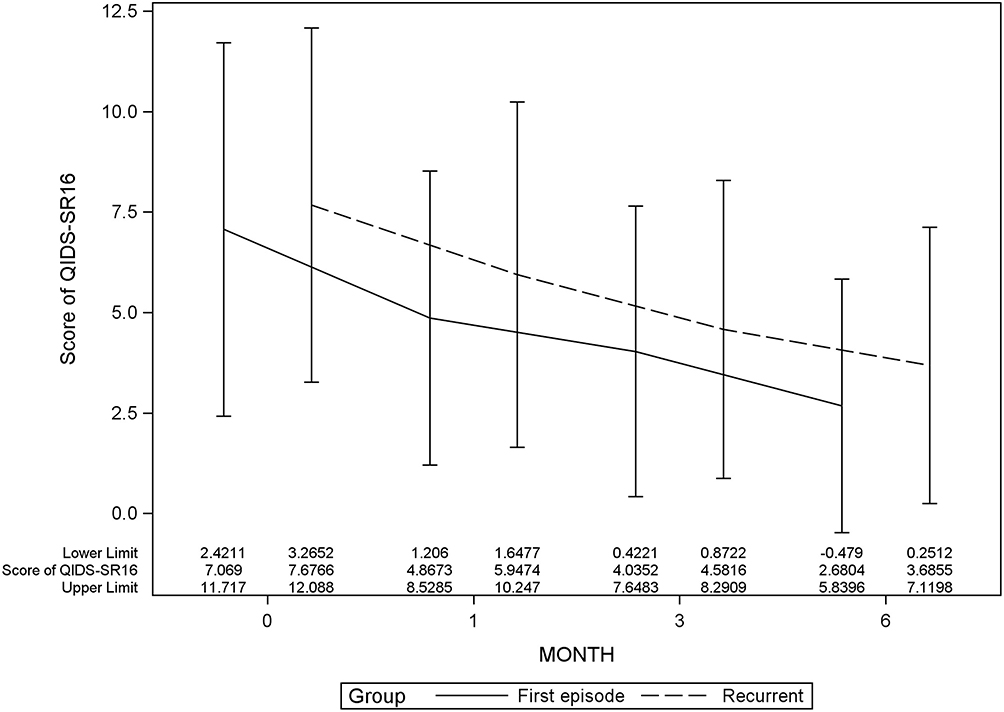 |
Figure 2 Comparison of QIDS-SR16 scores between patients with recurrent depression and patients with first-episode of depression. |
Follow-Up SDS Data in the Consolidation Phase
The follow-up data showed that the SDS scores of all patients decreased gradually with time (Figure 3), which indicated that the impairment of depression to patients’ social functions (work/school (Figure 3B), social life (Figure 3C) and family (Figure 3D)) was gradually decreasing.
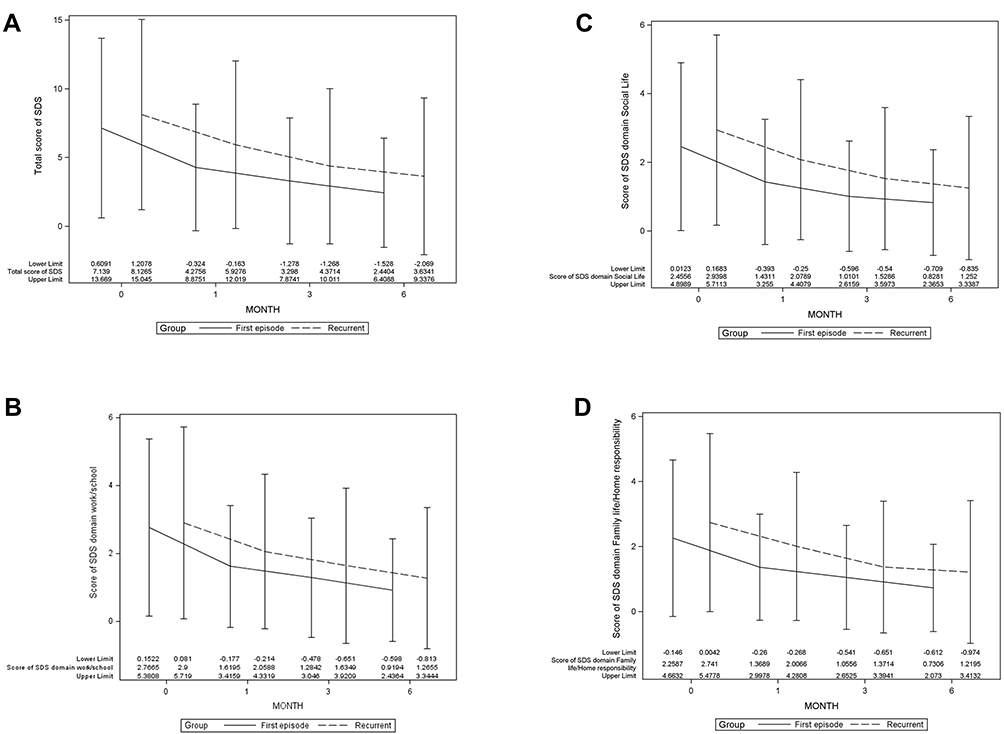 |
Figure 3 Comparison of SDS scores between patients with recurrent depression and that of patients with first-episode of depression. (A) The SDS scores of all patients decreased gradually with time; (B) the score of SDS domain: work/school decreased gradually with time; (C) the score of SDS domain: social life decreased gradually with time; (D) the score of SDS domain: family life decreased gradually with time. |
Follow-Up Q-LES-SF Data in the Consolidation Phase
The Q-LES-SF scores of all patients gradually increased over time, which indicated that the life quality of all patients gradually improved (Figure 4). Then the life quality scores of the first-episode patients were higher than that of the recurrent patients.
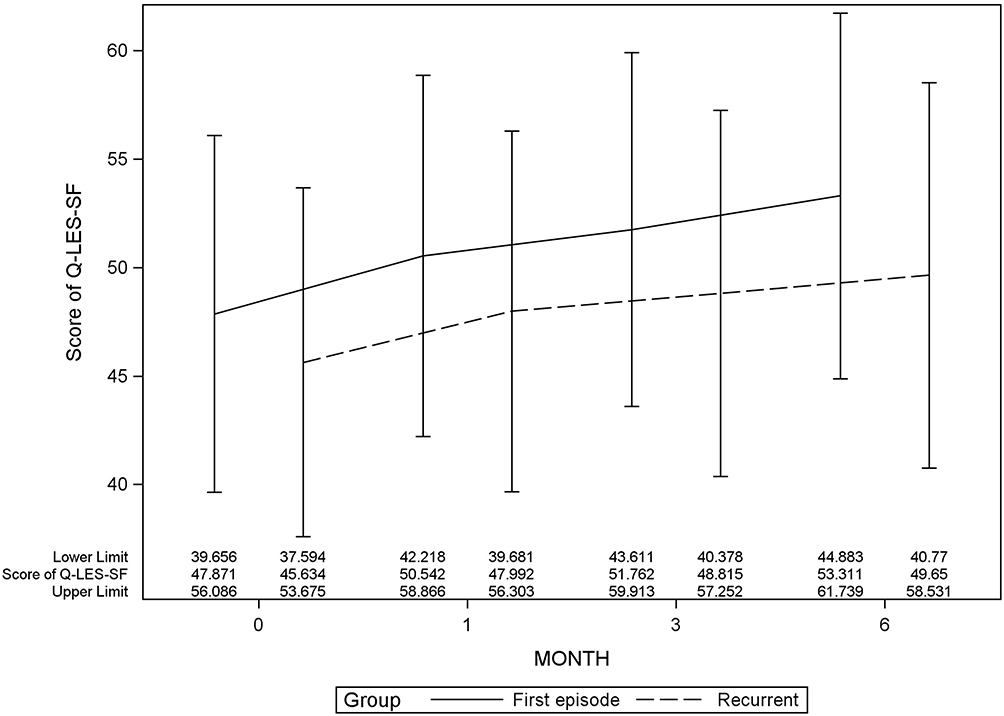 |
Figure 4 Comparison of Q-LES-SF scores and between patients with recurrent depression and that of patients with first-episode of depression. |
Digit Symbol Substitution Test (DDST) Results
There were no significant differences in DDST outcomes between the first-episode and recurrent episode patients after treatment in the acute phase with either baseline or later follow-up data. The DDST data were elevated in both groups as recommended by follow-up time (Table 2).
Discussion
Depression is a psychiatric disorder with a high prevalence, which can lead to recurrent depression due to incomplete relief of symptoms or residual symptoms.28 Lopez et al29 found that unipolar depression had a cumulative probability of recurrence of 13% within six months, and recurrence rates reached 75% and 87% in 10- and 15-year after the first episode, respectively. Depression will present an enormous burden to the family and the community. It is very meaningful to follow up the treatment and prognosis of depression. However, the comparison between the two groups of patients during the consolidation period after acute treatment has not been reported in depth. At present, the study focused on the comparison of depressive symptoms, social function impairment or cognitive function between the patients with first-episode depression and patients with recurrent depression after acute treatment.
Previous studies have shown that there was a certain biological specificity in the first-episode and recurrent patients with depression. On the one hand, non-linear dynamic analysis of EEG activity showed that there was an overall difference between patients with first-episode and recurrent depression.30 Brain dynamics results varied with the number of previous depressive episodes: the complexity of brain electrodynamics in patients with first depressive episode returned to normal levels after the clinic, whereas that did not happen for the recurrent patients.30 These results indicated that with the onset of depression, the complexity of dynamics and adaptive ability decreased. On the other hand, structural brain imaging studies of the patients with major depression showed significant hippocampal atrophy, which may explain inadequate memory, besides, hippocampal abnormalities occurred mainly in recurrent patients and depended on the duration of depression.31 These results may explain that the social function, depressive symptoms, and cognitive function of the first episode patients were better than that of the recurrent patients biologically,32,33 and this conclusion was also confirmed by clinical data.29
Rapp et al34 compared the depressive symptoms between the first episode and recurrent patients and found that the social function of the first episode and recurrent depression patients were both impaired; however, there was no significant difference between the two groups. In present finding, there was no significant difference in social function at baseline between recurrent patients and first-episode patients, but in the consolidation period, with the passage of time, the social function of recurrent patients gradually showed significant differences from first-episode patients, and was weaker than that of first-episode patients. In order to understand the inconsistency of current result with previous study, social-culture difference should be taken into account. In foreign countries, in addition to medication, both the first-episode patients and recurrent patients benefit a lot from perfect psychotherapy system and community mental health care.35–41 In China, the system of psychotherapy and community rehabilitation is not well established. Recurrent patients may suffer from a lot of difficulties in work and interpersonal relationship because of repeated depressive symptoms and poor access to psychological and community mental health care. The rehabilitation systems may be different in different countries, and the different effect on the social function of patients by the rehabilitation systems is worthy of further study. In this study, the family function of the recurrent group was worse than that of the first-episode group in the first month after acute phase, but there was no difference between the two groups at the third and sixth months. This may be because severe depressive symptoms of recurrent patients lead to more function impairment at the beginning stage of consolidation period. To our best knowledge, Chinese culture advocates the concept of collective and family. Thus, family support for patients is consistent regardless of the duration of the disease. This may be the reason why there is little difference in family function between the two groups over time. At the same time, to what extent and how different cultures affect the social function of patients with different episodes of depression is worth more detailed study.
In validating the differences in cognitive function between patients with first-episode depression and those with recurrent episodes, Talarowska et al18 found that patients with first episode were better than patients with recurrent episodes in information processing speed, visuospatial and auditory verbal memory and executive function, auditory verbal immediate and delayed memory, learning ability, and verbal fluency. In a study of neuropsychological cognitive function between patients with first-episode and patients with recurrent depression, Rapp et al34 found that elderly patients with first-episode major depression showed significant attention and executive impairment, while recurrent patients showed significant deficits in episodic memory. In present finding, there was no significant difference between recurrent patients and first-episode patients at baseline, 1, 3, and 6 six months after acute treatment. Our research is inconsistent with the results of previous studies. The difference of sample objects and evaluation tools is the possible reason. In addition, our subjects required that the VAS had recovered 50% from the onset of the episode, which may be the reason for no significant difference in cognitive function.
Maeshima et al42 demonstrated by follow-up data after three years that memory dysfunction in patients with a single episode of depression may improve to normal levels over time after remission. However, memory dysfunction may still be impaired in patients with recurrent depression. Our study was followed up for only 6 months. As time goes on, is it possible to have the same results? Whether the current difference is caused by the different follow-up time points of the two studies, we should also look forward to further research. On the other hand, whether there is a relationship between cognitive difference and hippocampal volume in the first episode patients is worthy of further study and discussion.
Somatic symptoms are not uncommon in depression, about 70% of the patients have a variety of somatic symptoms, including sleep disorders, appetite disorders, fatigue, sexual dysfunction, pain, etc. These symptoms sometimes also known as functional somatic symptoms that cannot be attributed to any physical disease.43,44 PHQ-15 mainly evaluates the physical state of patients, and depression with a PHQ-15 score of more than 10 is called somatic symptoms. In this study, we found that there was no difference between the two groups in terms of physical state in the baseline period, and at 1, 3, and 6 months after acute treatment, and the average PHQ-15 score was lower than 10 points at each time point, which meant no somatic symptoms on average. Which was not consistent with previously reported in other countries.45 We should consider this problem from the actual clinical situation. Although the average score of all patients is less than 10, in clinical practice, the physical symptoms of patients are different. Some patients’ PHQ-15 score is higher than 10, and some patients may tend to zero. Novick et al43 reported that somatic symptoms were common in patients with depression and were associated with severe depression, low treatment effectiveness, and cure rate in six Asian countries or regions. Novick et al,45 in their evaluation of treatment outcomes in depressed patients, found that depressed patients of different severity had different remission rates of somatic symptoms, that general somatic symptoms were associated with higher clinical severity and lower remission rates, and that pain symptoms had lower remission rates. Therefore, we can further study the relationship between somatic symptoms and the severity and remission rate of depressive symptoms in patients in the consolidation phase in China. Presently, there are few reports on the comparison between the first episode patients and the recurrent patients in somatic symptoms at the consolidation period in China. In this study, we compared the somatic symptoms of first-episode patients with that of recurrent patients. Although the current results show that there is no significant difference between the two groups, whether the results will be different needs further study if we expand the study to all patients with depression in consolidation stage.
QIDS-SR16 is a comprehensive assessment of patients’ depression symptoms including physical state, emotional state, anxiety state, etc. In our study, the score of QIDS-SR16 gradually decreased with time during the consolidation period, which indicated that the patients were gradually recovery. We also found that there was a significant difference in QIDS-SR16 score between the two groups of patients at the first month and sixth months after acute treatment, which indicated that the treatment effect of the first-episode patients was more obvious than that of the recurrent patients over time during the consolidation period, so in clinical treatment and family care, we should pay more attention to the depressive symptoms of recurrent patients and prevention recurrence of first episode patients.
Decreased life quality in patients with depression is associated with poorer response to medical treatment.46 In this study, the Q-LES-Q-SF score of recurrent patients was significantly lower than that of the first episode patients at each time point during the follow-up period, which indicated that the quality of life enjoyment and satisfaction of recurrent patients was significantly lower than that of patients with first episode after acute treatment. The recurrent patients might have worse compliance or medication outcomes than that of patients with first-episode depression. This suggests that in addition to medical treatment, psychological intervention, community mental health care and family support are important rehabilitation factors for the patients with recurrent depression.
Limitations and Expectations
There are still some limitations in this experiment. Firstly, the samples were not representative enough, as the patients were selected from big cities of China. Secondly, the follow-up time was short, and it is better to extend the follow-up time to make the comparative difference results more sufficient. Thirdly, the duration of the current episode between the two groups was significantly different, which needs to be controlled in future research. Fourthly, The scales in this study were all self-rating scales, and other more scales should be included in future studies. The prevention and correction of depression is a systematic project involving multiple disciplines and requiring the use of a variety of research methods. It is professional, complex, long-term, and urgent work. Although good clinical results have been achieved in the current study, more in-depth studies are needed.
Conclusions
We examined the differences between Chinese patients with recurrent and first episodes of depression in terms of depressive symptoms, social functioning, life satisfaction, somatic symptoms, and cognition after treatment in the acute phase. The results showed that patients with recurrence were more severely impaired in social function, life satisfaction, and depressive symptoms than those with the first episode.
There were two implications for clinical work according to our results: Firstly, we should strengthen the prevention of recurrence for patients who experience the first depression attack. Secondly, we should strengthen the community rehabilitation and psychological rehabilitation for recurrent patients to improve their life satisfaction and social function.
Acknowledgment
This research was funded by National Key Research & Development Program of China (2017YFC1311101), 2018 Beijing key clinical specialty construction project (Psychiatry) and Capital’s Funds for Health Improvement and Research (2018-1-2121).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Smith K. Mental health: a world of depression. Nature. 2014;515(7526):181. doi:10.1038/515180a
2. Brown WA
3. Frank E, Prien RF, Jarrett RB, et al. Conceptualization and rationale for consensus definitions of terms in major depressive disorder. Arch Gen Psychiatry. 1991;48:851–855. doi:10.1001/archpsyc.1991.01810330075011
4. Nuggerud-Galeas S, Sáez-Benito Suescun L, Berenguer Torrijo N. Analysis of depressive episodes, their recurrence and pharmacologic treatment in primary care patients: a retrospective descriptive study. PLoS One. 2020;15(5):e0233454. doi:10.1371/journal.pone.0233454
5. Kessler RC, Walters EE. Epidemiology of DSM-III-R major depression and minor depression among adolescents and young adults in the national comorbidity survey. Depress Anxiety. 1998;7(1):3–14. doi:10.1002/(SICI)1520-6394(1998)7:1<3::AID-DA2>3.0.CO;2-F
6. Kessler RC, Zhao S, Blazer DG, Swartz M. Prevalence, correlates, and course of minor depression and major depression in the national comorbidity survey. J Affect Disord. 1997;45(1–2):19–30. doi:10.1016/S0165-0327(97)00056-6
7. Van Beusekom BS, van den Broek WW, Birkenhäger TK. Long-term follow-up after successful electroconvulsive therapy for depression. J ECT. 2007;23(1):17–20. doi:10.1097/01.yct.0000263255.98796.30
8. Feldman HA, Goldstein I, Hatzichristou DG, Krane RJ, McKinlay JB. Impotence and its medical and psychosocial correlates: results of the Massachusetts male aging study. J Urol. 1994;151(1):54–61. doi:10.1016/S0022-5347(17)34871-1
9. Story TJ, Potter GG, Attix DK, Welsh-Bohmer KA, Steffens DC. Neurocognitive correlates of response to treatment in late-life depression. Am J Geriatr Psychiatry. 2008;16(9):752–759. doi:10.1097/JGP.0b013e31817e739a
10. Papke-Shields KE, Malhotra MK. Assessing the impact of the manufacturing executive’s role on business performance through strategic alignment. J Oper Manag. 2001;19(1):5–22. doi:10.1016/S0272-6963(00)00050-4
11. Harkness KL, Sc. JETB, Jeremy GSMS, Bagby RM. Acute and chronic stress exposure predicts 1‐year recurrence in adult outpatients with residual depression symptoms following response to treatment. Depress Anxiety. 2014;31(1):1–8. doi:10.1002/da.22177
12. Sheehan KH, Sheehan DV. Assessing treatment effects in clinical trials with the discan metric of the Sheehan disability scale. Int Clin Psychopharmacol. 2008;23:70–83. doi:10.1097/YIC.0b013e3282f2b4d6
13. Zimmerman M, McGlinchey JB, Posternak MA, Friedman M, Boerescu D, Attiullah N. Remission in depressed outpatients: more than just symptom resolution? J Psychiatr Res. 2008;42:797–801. doi:10.1016/j.jpsychires.2007.09.004
14. Trivedi MH, Dunner DL, Kornstein SG, et al. Psychosocial outcomes in patients with recurrent major depressive disorder during 2 years of maintenance treatment with venlafaxine extended release. J Affect Disorder. 2010;126:420–429. doi:10.1016/j.jad.2010.04.011
15. Sivertsen H, Bjorklof GH, Engedal K, Selbake G, Helvik AS. Depression and quality of life in older persons: a review. Dement Geriatr Cogn Disorder 2015;40:311–339. doi:10.1159/000437299
16. Abrantes AM, Battle CL, Strong DR, Ing E, Gordon A, Brown RA. Exercise preferences of patients in substance abuse treatment. Ment Health Phys Act. 2011;4:79–87. doi:10.1016/j.mhpa.2011.08.002
17. Nandrino JL, Pezard L, Posté A, Réveillère C, Beaune D. Autobiographical memory in major depression: a comparison between first-episode and recurrent patients. Psychopathology. 2002;35(6):335–340. doi:10.1159/000068591
18. Talarowska M, Zajączkowska M, Gałecki P. Cognitive functions in first-episode depression and recurrent depressive disorder. Psychiatr Danub. 2015;27(1):38–43.
19. Karabekiroğlu A, Topçuoğlu V, Gimzal Gönentür A, Karabekiroğlu K. Executive function differences between first episode and recurrent major depression patients. Turk J Psychiatry. 2010;21(4):280–288.
20. Sartorius N. The ICD-10 and depression. Acta Psychiatr Scand Suppl. 1983;68(S310):103–105. doi:10.1111/acps.1983.68.s310.103
21. Zhen L, Wang G, Xu G, et al. Evaluation of the paper and smartphone versions of the Quick Inventory of Depressive Symptomatology-Self-Report (QIDS-SR16) and the patient health questionnaire-9 (PHQ-9) in depressed patients in China. Neuropsychiatr Dis Treat. 2020;16:993. doi:10.2147/NDT.S241766
22. Joan T, Javier DAO, Albert FS, et al. Looking into the effect of multi-item symptom domains on psychometric characteristics of the Quick Inventory of Depressive Symptomatology-Self Report (QIDS-SR16). Psychiatry Res. 2018;267:126. doi:10.1016/j.psychres.2018.05.076
23. Kroenke K, Spitzer RL, Williams JBW. The PHQ-15: validity of a new measure for evaluating the severity of somatic symptoms. Psychosom Med. 2002;64(2):258–266. doi:10.1097/00006842-200203000-00008
24. Lee YT, Liu SI, Huang HC, Sun FJ, Huang CR, Yeung A. Validity and reliability of the Chinese version of the short form of Quality of Life Enjoyment and Satisfaction Questionnaire (Q-LES-Q-SF). Qual Life Res. 2014;23(3):907–916. doi:10.1007/s11136-013-0528-0
25. Rapaport MH, Clary C, Fayyad R, Endicott J. Quality-of-life impairment in depressive and anxiety disorders. Am J Psychiatry. 2005;162(6):1171–1178.
26. Kessler RC, Berglund P, Demler O, et al. The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R). JAMA. 2003;289(23):3095–3105. doi:10.1001/jama.289.23.3095
27. Baune BT, Mélanie B, Groes LK. A network meta-analysis comparing effects of various antidepressant classes on the Digit Symbol Substitution Test (DSST) as a measure of cognitive dysfunction in patients with major depressive disorder. Int J Neuropsychopharmacol. 2018;2:97–107.
28. Judd LL, Akiskal HS, Maser JD, Zeller PJ, Keller MB. Major depressive disorder: a prospective study of residual subthreshold depressive symptoms as predictor of rapid relapse. J Affect Disord. 1998;50(2–3):97–108. doi:10.1016/S0165-0327(98)00138-4
29. Lopez AD, Mathers CD. Measuring the global burden of disease and epidemiological transitions: 2002–2030. Ann Trop Med Parasitol. 2006;100(5–6):481–499. doi:10.1179/136485906X97417
30. Čukić M, Stokić M, Slavoljub R, Ljubisavljevic M, Slobodan S, Savic D. Nonlinear analysis of EEG complexity in episode and remission phase of recurrent depression. Int J Methods Psychiatr Res. 2020;29(2):e1816. doi:10.1002/mpr.1816
31. Kronmüller KT, Schröder J, Köhler S, et al. Hippocampal volume in first episode and recurrent depression. Psychiatry Res. 2009;174(1):62–66. doi:10.1016/j.pscychresns.2008.08.001
32. Basso MR, Bornstein RA. Relative memory deficits in recurrent versus first-episode major depression on a word-list learning task. Neuropsychology. 1999;13(4):557. doi:10.1037/0894-4105.13.4.557
33. Globus GG, Arpaia JP. Psychiatry and the new dynamics. Biol Psychiatry. 1994;35(5):352–364. doi:10.1016/0006-3223(94)90039-6
34. Rapp MA, Dahlman K, Sano M, Grossman HT, Haroutunian V, Gorman JM. Neuropsychological differences between late-onset and recurrent geriatric major depression. Am J Psychiatry. 2005;162(4):691–698. doi:10.1176/appi.ajp.162.4.691
35. Pirkola S, Sund R, Sailas E, et al. Community mental health services and suicide rate in Finland: a nationwide small area analysis. Lancet. 2009;373:147–153. doi:10.1016/S0140-6736(08)61848-6
36. Giovanni DG, Bassi M, Neri G, et al. The current state of mental health care in Italy: problems, perspectives, and lessons to learn. Eur Arch Psychiatry Clin Neurosci. 2007;257:83–91. doi:10.1007/s00406-006-0695-x
37. Ito H, Rg F, Nakatani Y, Fukuda Y. The regional health care strategic plan: the growing impact of mental disorder in Japan. Psychiatr Serv. 2013;64:617–619. doi:10.1176/appi.ps.201200518
38. Cuijpers P, Sijbrandij M, Koole SL, Andersson G, Beekman AT, Reynolds CF
39. Kamenov K, Twomey C, Cabello M, Prina AM, Ayuso-Mateos JL. The efficacy of psychotherapy, pharmacotherapy and their combination on functioning and quality of life in depression: a meta-analysis. Psychol Med. 2017;47:414–425. pmid:27780478. doi:10.1017/S0033291716002774
40. Nelson JC, Papakostas GI. Atypical antipsychotic augmentation in major depressive disorder: a meta-analysis of placebo-controlled randomized trials. Am J Psychiatry. 2009;166:980–991. doi:10.1176/appi.ajp.2009.09030312
41. Ramanuj P, Ferenchick EK, Pincus HA. Depression in primary care: part2-management. Br Med J. 2019;365:1835.
42. Maeshima H, Baba H, Nakano Y, et al. Residual memory dysfunction in recurrent major depressive disorder-a longitudinal study from Juntendo University mood disorder project. J Affect Disord. 2012;143(1–3):84–88. doi:10.1016/j.jad.2012.05.033
43. Novick D, Montgomery WS, Aguado J, Peng X, Brugnoli R, Haro JM. Which somatic symptoms are associated with an unfavorable course in Asian patients with major depressive disorder? J Affect Disord. 2013;149(4):182–188. doi:10.1016/j.jad.2013.01.020
44. Han H, Wang SM, Han C, Lee SJ, Pae CU. The relationship between somatic symptoms and depression. Neuro Endocrinol Lett. 2014;35(6):463–469.
45. Novick D, Montgomery WS, Aguado J, Peng X, Brugnoli R, Haro JM. Which somatic symptoms are associated with an unfavorable course in Chinese patients with major depressive disorder? Asia Pac Psychiatry. 2015;7(4):427–435. doi:10.1111/appy.12189
46. Laura S, Mercedes S, Alejandra L, Silvia O, Silvia K. To what extent does depression influence quality of life of people with pharmacoresistant epilepsy in Argentina? Epilepsy Behav. 2017;69:133–138.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.