")
Back to Journals » Drug Design, Development and Therapy » Volume 16
Comparison of Prophylactic Norepinephrine and Phenylephrine Infusions During Spinal Anaesthesia for Primary Caesarean Delivery in Twin Pregnancies: A Randomized Double-Blinded Clinical Study
Authors Du W, Song Y, Li J, Zhou X, Xu Z, Liu Z
Received 7 January 2022
Accepted for publication 12 March 2022
Published 24 March 2022 Volume 2022:16 Pages 789—798
DOI https://doi.org/10.2147/DDDT.S357507
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Tin Wui Wong
Weijia Du,* Yujie Song,* Jiang Li, Xianjin Zhou, Zhendong Xu, Zhiqiang Liu
Department of Anesthesiology, Shanghai First Maternity and Infant Hospital, Tongji University School of Medicine, Shanghai, 200092, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhiqiang Liu; Zhendong Xu, Department of Anesthesiology, Shanghai First Maternity and Infant Hospital School of Medicine, Tongji University, No. 2699, West Gaoke Road, Shanghai, People’s Republic of China, Email [email protected]; [email protected]
Background: Norepinephrine has been associated with improved heart rate (HR) and cardiac output (CO) compared to phenylephrine as a treatment for post-spinal hypotension during caesarean delivery (CD) in singleton pregnancies. Our current study compared the effects of norepinephrine and phenylephrine in maintaining maternal hemodynamics after spinal anaesthesia in twin pregnancies during elective CD.
Methods: This was a double-blinded, randomized, controlled study. From December 2017 to December 2018, 62 women with healthy twin term pregnancies undergoing elective CD under spinal anaesthesia were studied. Following spinal induction, either norepinephrine (6 μg/mL) or phenylepinephrine (75 μg/mL) was infused at 60 mL/h to maintain systolic blood pressure (SBP) near baseline until delivery. HR, SBP, systemic vascular resistance (SVR), and CO were collected using anaesthesia monitors and continuous-pulse waveform analysis. The primary outcome was maternal CO. Other parameters of maternal hemodynamics, umbilical cord blood gases, and adverse events were also compared.
Results: Hemodynamic variables (CO, SBP, HR, and SVR) between spinal anaesthesia induction to skin incision were similar between the two groups (P = 0.889, 0.057, 0.977, and 0.416, respectively). The incidence of bradycardia was significantly higher in the phenylephrine group (69%) than in the norepinephrine group (24.2%, P< 0.001). Maternal nausea and vomiting, hypotension, reactive hypertension, and neonatal outcomes did not differ between the groups.
Conclusion: When administered as a prophylactic fixed-rate infusion, phenylephrine and norepinephrine are both capable of maintaining maternal blood pressure following spinal anaesthesia in twin pregnancies. There were no differences in the maternal hemodynamics or foetal outcomes between women receiving norepinephrine and phenylephrine.
Previous Presentations: Presented at the 51st Society for Obstetric Anesthesia and Perinatology Annual Meeting, Phoenix, Arizona, May 1– 5, 2019.
Clinical Trial Number and Registry: No. ChiCTR-IOR-17013358.
Keywords: caesarean section, hypotension, norepinephrine, phenylephrine, spinal anaesthesia, twins
Introduction
Multiple gestation pregnancies, especially twin pregnancies, have become considerably frequent with assisted reproductive technology. Twin pregnancy usually occurs among older mothers with more medical and obstetric conditions.1 Even in uncomplicated twin pregnancies, hemodynamic changes are considered greater than those in singleton pregnancies.2–4 Limited data exist on the adaptation to hemodynamic changes during spinal anaesthesia for caesarean delivery (CD).5–7
Phenylephrine is a popular vasopressor used for the treatment of spinal hypotension during CD. Being a pure α-adrenergic agonist, it is associated with a dose-dependent decrease in maternal heart rate (HR) and cardiac output (CO).8,9 Norepinephrine, with its β-adrenergic properties, is associated with improved HR and CO over phenylephrine during CD.10–13 However, studies have focused on comparing the use of these two vasopressors during CD in singleton but not twin pregnancies.10–13 Although healthy parturients and healthy fetuses seem to tolerate these hemodynamic changes well, the findings may not be extrapolated to twin pregnancies. Concerns persist over the effect of decrease in maternal CO on two fetuses and their uteroplacental blood flow, as not much is known about it.
Twin gestation presents a particular challenge owing to more severe aortocaval compression and greater cardiovascular changes compared with singleton gestation.14,15 We aimed to compare maternal hemodynamics and foetal outcomes in women receiving prophylactic norepinephrine and phenylephrine infusions following spinal injection for CD. The primary outcome of this prospective study was changes of maternal CO which was used as a surrogate marker of uteroplacental perfusion.16 We hypothesized that the β-adrenergic effects of norepinephrine offer greater maternal and foetal benefits in twin pregnancies.
Materials and Methods
This study was approved by the Ethical Committee of Shanghai First Maternity and Infant Hospital (Ethical Committee No. KS17105), and written informed consent was obtained from all participants in the trial. The trial was registered prior to patient enrolment in the Chinese Clinical Trial Registry (Reference number: ChiCTR-IOR-17013358, Principal investigator: Weijia Du, Date of registration: November 13, 2017). The hospital is the largest birth and referral centre in China, with an annual delivery volume of more than 30,000 babies.
Sixty-four women were enrolled from December 2017 to December 2018. Informed consent was obtained from all participating women after explaining the nature of the study and procedures involved, including the need for an arterial catheter. Data are reported according to the CONSORT guidelines. The following inclusion criteria were to be met: women with primary twin pregnancy at term (37–38 weeks) without any medical or obstetric complications undergoing elective CD under a single-shot spinal anaesthesia. Exclusion criteria included pre-existing/pregnancy-induced hypertension, known cardiovascular/cerebrovascular diseases, known foetal abnormality, allergy to study medications, extreme weight (<50 or >100 kg) or height (<140 or >180 cm), or those with contraindications for spinal anaesthesia.
Women were allowed to have clear liquids up to 2 h prior to scheduled anaesthesia induction. Upon arrival in the operating room, they were placed in the supine position with a left lateral tilt and attached to standard anaesthesia monitors (Infinity C500; Dräger Medical, Lübeck, Germany). Following lidocaine infiltration, a 20-G arterial catheter was placed in the right radial artery after an Allen test, and an 18-G intravenous catheter was placed on the forearm. Continuous arterial-pulse waveforms were interfaced with a pulse analysis module (PulseCOTM, Cambridge, United Kingdom), an integrated part of the LiDCOrapid Monitoring System (LiDCO Ltd., Cambridge, United Kingdom).
Baseline hemodynamic data were collected over 3 min following arterial line insertion. The patient was then placed in a left lateral decubitus position. Following skin infiltration with 2–3 mL of 1% lidocaine, a 25-G Whitacre needle (BD Medical, Franklin Lakes, NJ) was inserted through an introducer at the L3 or L4 level. After confirmation of free flow of cerebrospinal fluid, 12 mg 0.5% isobaric ropivacaine (Naropin, AstraZeneca AB, Södertälje, Sweden) and 5 μg sufentanil were injected intrathecally. After induction of spinal anaesthesia, the patient was returned to the left-tilted supine position. Rapid co-loading with 500 mL lactated Ringer’s solution was completed over 5 min followed by continuous infusion so as not to exceed the total volume of 1000 mL before delivery.
For randomization and blinding, 64 slips (32 for each group) were prepared and sealed in envelopes by staff not involved in the study. An online random number generator (available at: http://www.psychicscience.org/random.aspx, accessed July 9, 2017) was used to obtain the randomization codes, which were calculated using a closed-sequence algorithm to ensure equal numbers in each group. The study drug was prepared in a 50-mL syringe according to the randomization code by an unblinded research nurse. An additional 20-mL solution of the same drug was also prepared for additional boluses. The concentrations of the drugs (6 μg/mL norepinephrine and 75 μg/mL phenylephrine) were determined based on the potency ratio of approximately 13:1.12 The infusion and bolus drugs were blinded to the patients and the personnel performing the study as well as the surgery and anaesthesia providers.
Infusion of the study drug was initiated upon spinal injection via a side limb of the intravenous fluid access. The initial infusion was commenced at a fixed rate of 60 mL/h for 3 min, after which the infusion was either stopped or continued based on the systolic blood pressure (SBP): the infusion was stopped if the SBP was above 110% baseline, and it was continued or restarted if the SBP was less than 90% baseline. If hypotension (defined as SBP at or below 80% baseline) was observed, 1 mL of the bolus solution was given and repeated as needed. The total volumes of study solutions given by bolus and infusion up to the time of delivery were recorded.
The incidences of hypotension, hypertension (defined as SBP at or above 120% baseline), and bradycardia (defined as HR < 60 bpm) were recorded. Severe bradycardia (defined as HR < 50 bpm) was to be treated by stopping the infusion. Severe bradycardia accompanied by hypotension was to be treated with intravenous atropine.
Spinal block level was tested by loss of cold sensation 5 min following the spinal injection. The density of the surgical block was confirmed with pinpricks. Times of spinal injection (induction), skin incision, uterine incision, and the two deliveries (twin A and twin B) were recorded. Umbilical venous (UV) blood samples were drawn for blood gas analysis from a double-clamped umbilical cord segment. In our experience, umbilical arterial (UA) samples are not always reliably obtained in twins, and thus, UV samples were therefore used as surrogates. Apgar scores at 1 and 5 min following delivery were also recorded. Complications observed during the spinal anaesthetic technique were recorded and managed as deemed appropriate by the anaesthesia care team.
The LiDCOrapid system was connected to the monitor to extract data from the arterial line. Beat-to-beat data were regularly checked for extreme values and replaced using non-linear interpolation. Most extreme values resulting from zeroing, flushing, blocking, or kinking of the arterial catheter can be automatically identified by LiDCOrapid monitor as “bad”. While there were also some values closed to “bad” records, we set the upper and lower acceptable limits based on clinical discretion for these variables: SBP, HR, CO, and SVR. These limits were set individually for every data file.
Statistical Analysis
The primary outcome measurement was standardized CO prior to skin incision. The secondary outcomes were group differences in hemodynamic variables, including SBP, HR, SVR, and side effects. The sample size calculation was based on data from previous studies conducted by Ngan Kee et al.17 We used PASS Software (NCSS, Kaysville, UT) to calculate that a sample size of 30 patients per group would have greater than 80% power to detect a 20% difference in CO between groups following spinal injection with a two-sided α error probability of 0.05 assuming an anticipated mean value in the phenylephrine group of 5.4 L/min and standard deviation (SD) of 1.5 L/min. To account for potential dropouts, the sample size was increased by 5%, resulting in a final sample size of 32 patients per group.
Statistical analyses were performed using SPSS version 22 (IBM, Armonk, NY). Q-Q plots and the Shapiro–Wilk test were used to test the normality of the distribution of univariate intergroup data. Normally distributed outcome data were presented as mean (SD) and analysed among groups using the Student’s t-test. Non-normally distributed data were summarized as median (interquartile range) and were compared using the Mann–Whitney U-test. Categorical variables were analysed using the chi-squared test. Statistical significance was set at P <0.05.
Summary measures were used to compare serial hemodynamic data between the two groups.18 All values were calculated as percentages of baseline. Values were only analysed from spinal induction to skin incision since the table tilting upon skin incision and the external fundal pressure to facilitate delivery could alter the intra-abdominal pressure and lead to inaccurate results.19 Areas under the curve (AUCs) for values plotted against time were calculated using the trapezium rule18 as described by Ngan Kee et al.13 Since the time between spinal induction and skin incision varies amongst women, we divided the AUCs of SBP, CO, HR, and SVR for each patient by the number of data points to obtain standardized values. Calculated AUCs were compared between the groups using the Mann–Whitney U-test.
Results
Patient recruitment and flow are shown in Figure 1. A total of 85 women were screened and 64 women were enrolled. Two patients were excluded because of failed spinal block and data loss. After exclusions, data were analysed for 62 patients, with 31 in each group. Demographics and baseline hemodynamic data were comparable between the two groups (Table 1). The spinal block height and operative characteristics are shown in Table 1. The total volume of the study drug was comparable when using norepinephrine (9 mL [interquartile range, 6–14 mL]) or phenylephrine (7 mL [interquartile range, 5.5–9 mL]) to maintain SBP in the target range (P=0.079).
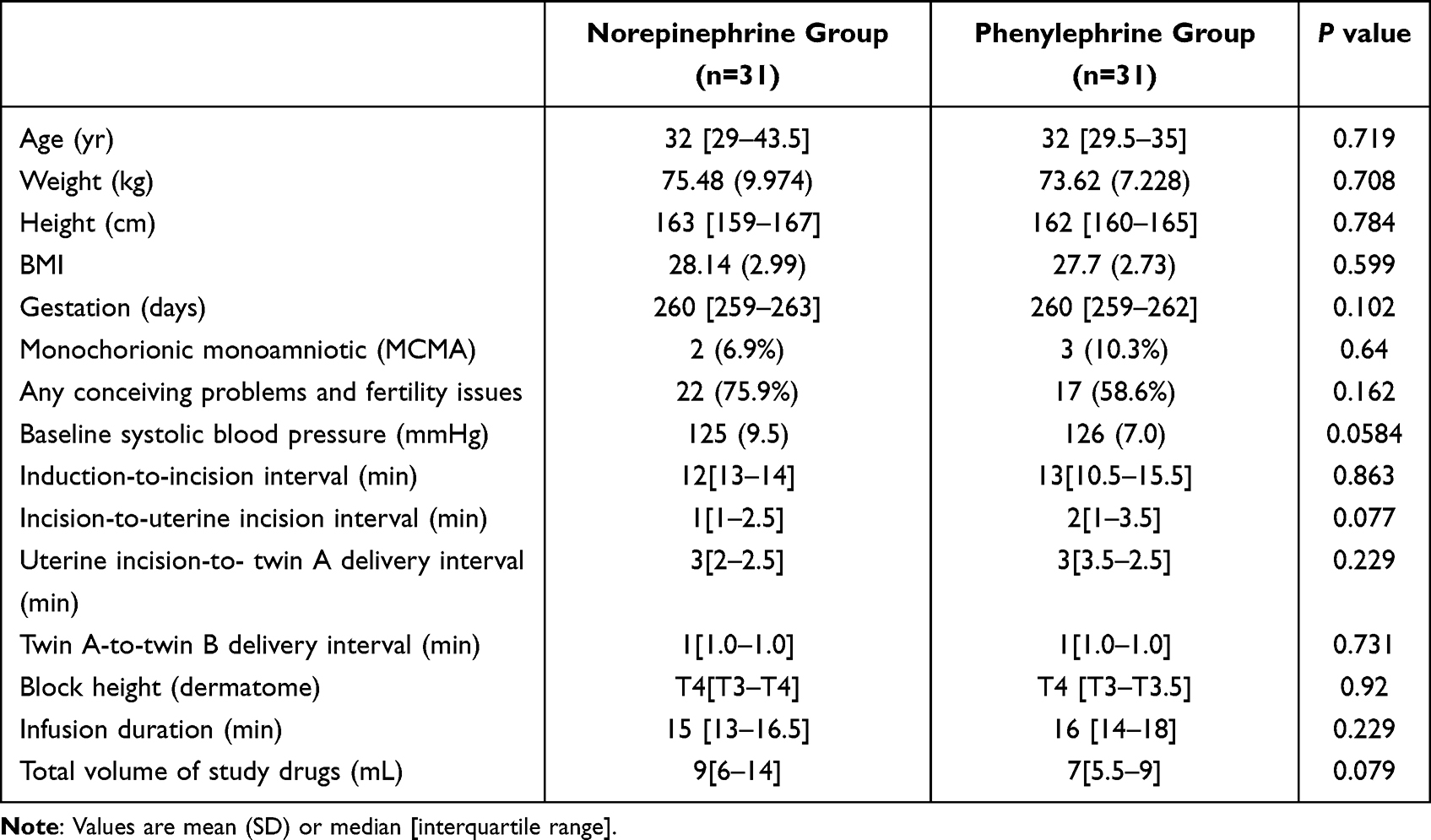 |
Table 1 Patient and Intra-Operative Characteristics |
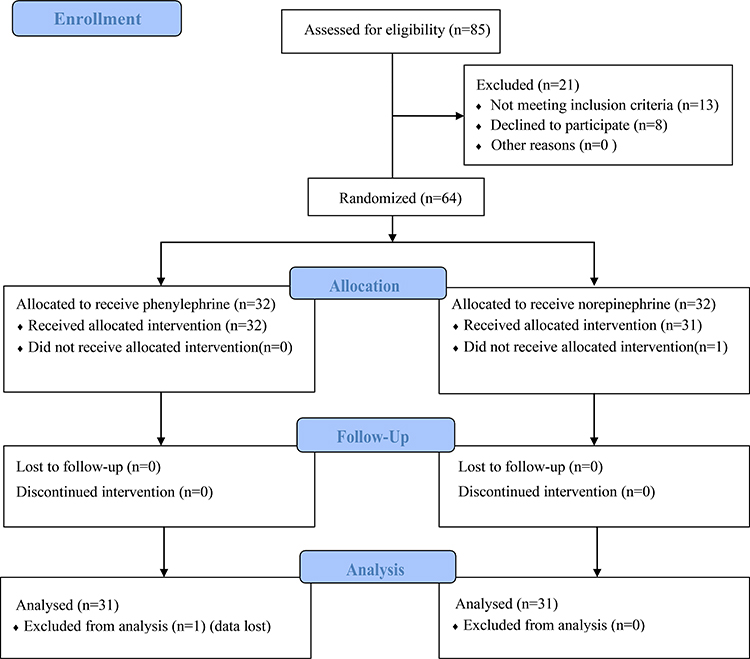 |
Figure 1 Study CONSORT diagram showing patient recruitment and flow. |
Comparison of the calculated AUCs standardized for each patient from spinal induction to skin incision showed that CO (P=0.889), SBP (P=0.057), HR (P=0.977), and SVR (P=0.416) were not significantly different between the two groups (Figure 2). For demonstration purposes, continuous changes of standardized CO, SBP, HR, and SVR, respectively, collected by the LiDCOrapid monitor were expressed as data over a 10-min window immediately after drug infusion (Figure 2). In our institution, the typical time between spinal induction and skin incision for primary CD is between 10 and 15 min. We, therefore, used 10 min as the common denominator.
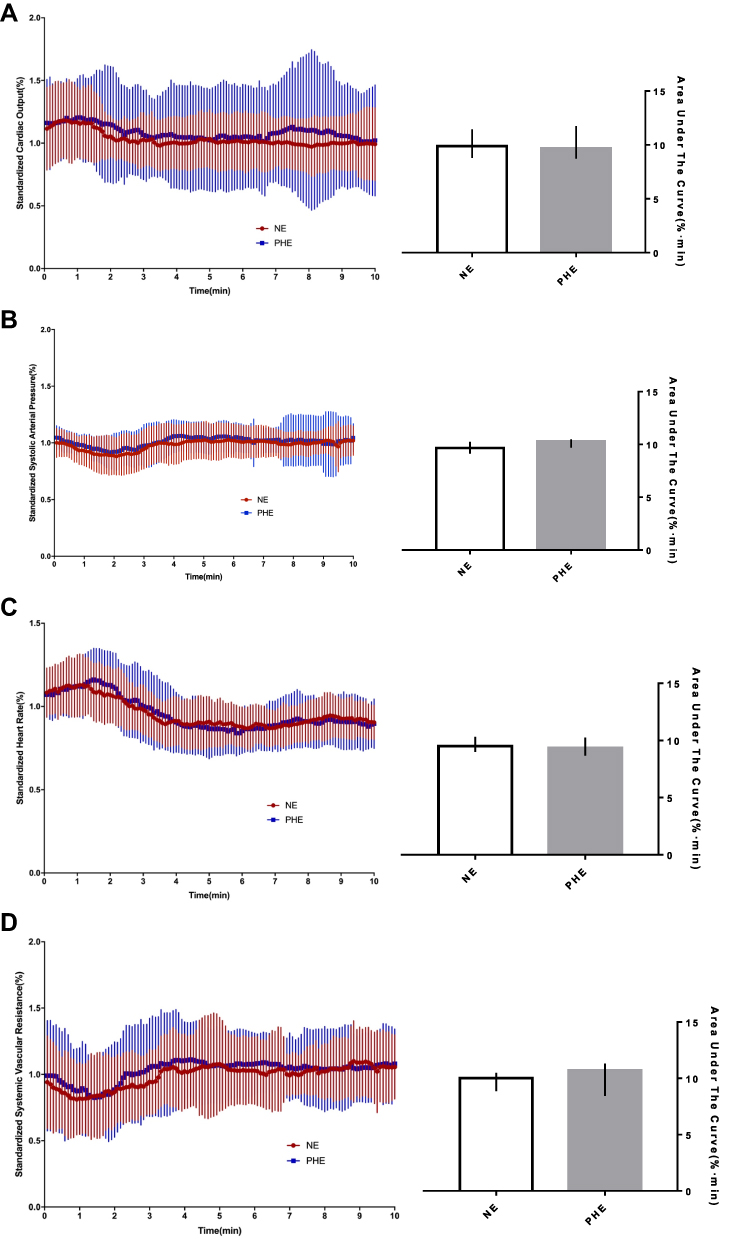 |
Figure 2 Continuous changes in cardiac output (A), systolic blood pressure (B), heart rate (C) and systemic vascular resistance (D) standardized to the percentage of baseline values. On the left side of the panels, data are continuous values for the first 10 min from drug infusion. On the right side of the panels, bars show the area under the curve for the two groups. Abbreviations: NE, norepinephrine; PHE, phenylephrine. |
The incidence of HR below 60 bpm was higher in the phenylephrine group (69%) than in the norepinephrine group (24.2%, P<0.001, Table 2). Both groups had comparable rates of hypotension (norepinephrine vs phenylephrine: 41.4% vs 44.8%, P=0.791), hypertension (norepinephrine vs phenylephrine: 34.5% vs 58.6%, P=0.065), and intraoperative nausea and vomiting (norepinephrine vs phenylephrine: 31.0% vs 24.1%, P=0.557).
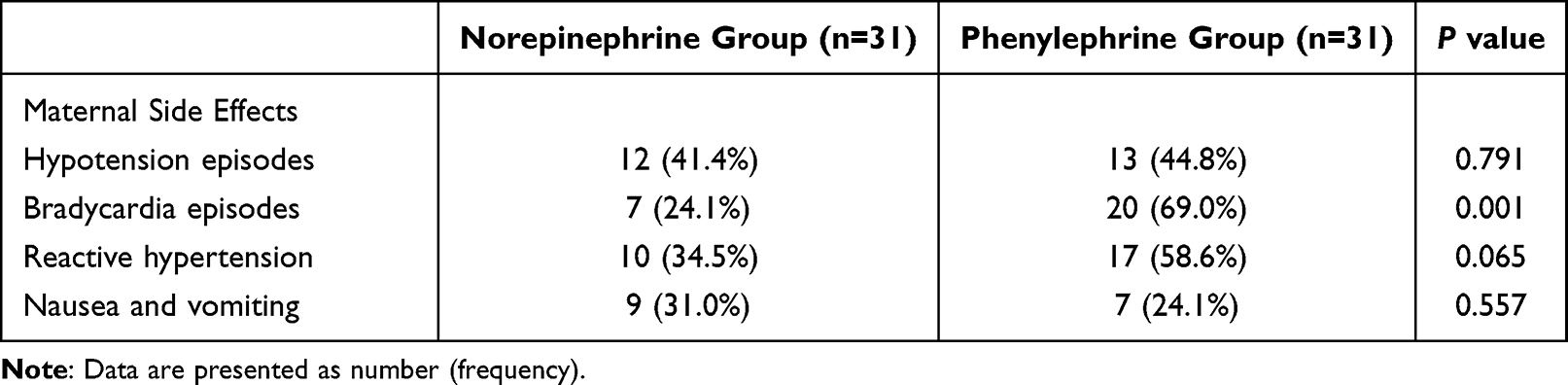 |
Table 2 Maternal and Neonatal Side Effects |
The neonatal outcomes are summarized in Table 3. There were no differences in the UV pH between the groups. Apgar scores at 1 and 5 min were comparable between the groups. None of the neonates required positive-pressure ventilation or newborn intensive care unit admissions.
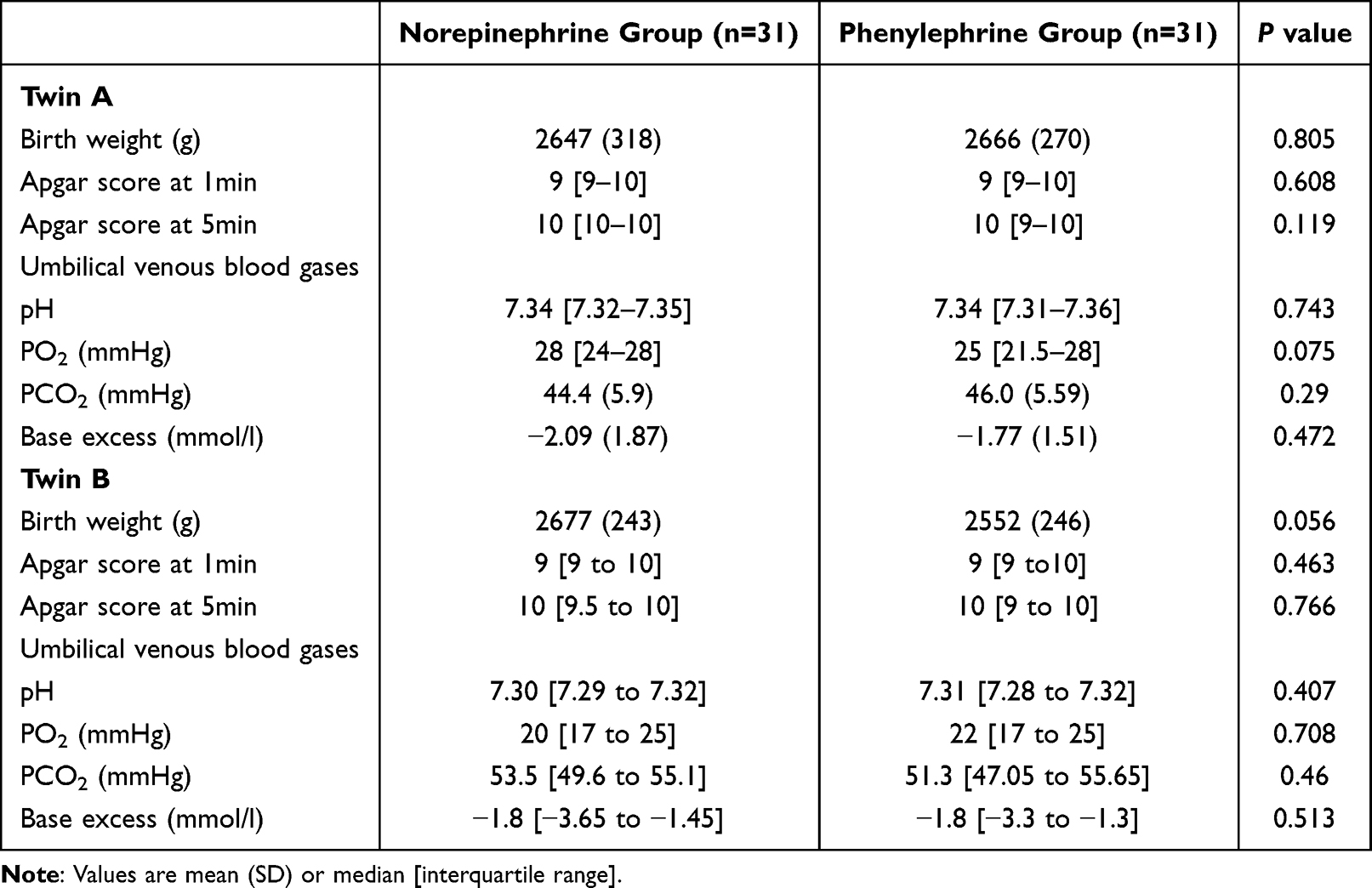 |
Table 3 Neonatal Outcomes |
Discussion
We found that phenylephrine and norepinephrine have similar efficacy in maintaining maternal CO and other hemodynamic variables following spinal anaesthesia in twin pregnancies, and the foetal outcomes were similar. These findings are different from those of Ngan Kee et al13 in single pregnancies, which showed an advantage of norepinephrine in maintaining CO and HR over phenylephrine.
Maternal CO, rather than blood pressure, could be an important factor in determining uterine blood flow and foetal acid-base balance.16,20 The hemodynamic benefits of norepinephrine shown by Ngan Kee et al in singleton pregnancy13 should, in theory, be more pronounced in women with twins since an increase in CO could help offset severe aortocaval compression from the larger gravid uterus. In our study in twin pregnancy, however, not only did we not see any foetal benefits, but the hemodynamic advantages described by Ngan Kee et al were not observed.13 We offer several explanations for the difference. First, a twin pregnancy is associated with a more cephalic spread of the spinal block than a singleton pregnancy,7 which partially reversed the β-adrenergic effects of norepinephrine with a relative increase in parasympathetic activity and decreased venous return.21 In addition, hyperbaric spinal bupivacaine is not available in our market, and the isobaric ropivacaine could have contributed to a more cephalad spread during spinal anaesthesia. The obstruction to venous return from the gravid uterus could be more severe in twin pregnancy and the extremely limited venous return in twin pregnancy could have restricted the left ventricular end-diastolic volume available to generate a higher CO. To complicate the issue, we were not able to tilt the operating table beyond 15° with twin pregnancy owing to the risk of a fall. Studies have found that a 30° left-tilted position improved the cross-sectional area of the inferior vena cava compared with 15° or supine positioning in singleton women;22,23 however, it was hard to achieve this in our study. Notably, while norepinephrine is not a pure β1-selective adrenergic agonist, its effect on β2-adrenoceptors leading to vasodilation is considered to be minor; however, little is known of this effect on pregnancy, particularly on twin pregnancy. It is not certain to what extent the β2-adrenergic effect contributed to the findings in our study. Second, the main difference between this study and Ngan Kee et al13 is that we measured cardiac output and other hemodynamic variables invasively and continuously, which is the strength of our study. LiDCO cardiac output monitor has been demonstrated to be reliable in many different physiological and pathological conditions, and be able to measure the effect of therapeutic interventions in the obstetric population.24–26
In this study, we compared norepinephrine at a concentration of 6 μg/mL with phenylephrine at a concentration of 75 μg/mL (at a potency ratio of 13:1). Although several dose-finding studies suggest that 50 μg/min could be a preferable starting point for prophylactic phenylephrine infusion,27,28 we used a relatively high initial infusion rate of phenylephrine (75 μg/min) considering that post-spinal hypotension in twin pregnancies could occur earlier and is more severe when compared with singleton pregnancies.7 Despite the high dose, however, SBP could not be maintained at baseline level with the infusions alone during the first 4 min following spinal induction in both groups. This phenomenon can be explained by the more rapid onset and higher cephalic spread of spinal anaesthesia in twin pregnancies.7 Twin gestation is associated with a more severe aortocaval compression29 and a lower vascular tone,2,15 which both contribute to a more rapid and severe development of hypotension following spinal anaesthesia.30 Further studies are warranted to investigate the optimal vasopressor choices and protocols for managing hypotension following spinal anaesthesia in twin pregnancies.
The incidence of bradycardia was significantly higher in the phenylephrine group than in the norepinephrine group, which is consistent with other studies.31,32 However, none of the women experienced severe bradycardia warranting atropine treatment, and no significant differences were observed in continuous HR changes between the two groups. Thus, we suggest that bradycardia related to phenylephrine is not a predominant clinical problem in this study and could be rapidly corrected by switching off the infusion.33 Relatively higher incidences of hypotension (41.4% vs 44.8%) and hypertension (34.5% vs 58.6%) were observed in our study using continuous hemodynamic data collection via an arterial line compared to previous studies with routine intermittent measurements.13,34
Our study has certain limitations. First, we were only able to report UV blood gas values rather than UA samples owing to the technical challenge of obtaining UA blood from twins. In a study comparing graded mixtures of phenylephrine and ephedrine by Ngan Kee et al,35 there was a certain degree of correlation between UA and UV blood gas values. UV blood gas values, while being less sensitive, may serve as a “crude” measure for severe foetal distress. Our study involved low-risk women only, and there was no clinical foetal distress. Second, for the study purpose, we used a fixed on-and-off infusion of drugs to attain the baseline systems.11,13 Integration with BP recordings may offer more practical utility for the management of BP in the future. Third, this study failed to achieve significance of the primary outcome. The underlying reason may be due to inadequate power. Further studies are warranted to investigate the effectiveness and safety of norepinephrine in twin pregnancies by improving the design of the study, including increasing the sample size, modifying the primary outcome to enhance the likelihood of reaching a decisive conclusion.
In summary, when administered as a prophylactic fixed-rate infusion, phenylephrine and norepinephrine had similar efficacy for maintaining maternal hemodynamics including CO, SBP, HR, and SVR after spinal anaesthesia induced with 12 mg 0.5% isobaric bupivacaine and 5 μg sufentanil. The neonatal outcomes were similar. Considering the lack of additional benefits and the fact that it is best administered through a central venous access or upper extremity,30,36 the routine use of norepinephrine in CD, particularly for a twin pregnancy, needs to be further investigated.
Data Sharing Statement
All data generated or analyzed during this study were included in this published article. Further inquiries can be directed to Professor Zhiqiang Liu on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Ethical Committee of Shanghai First Maternity and Infant Hospital (Ethical Committee No. KS17105), and in accordance with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The trial was registered prior to patient enrolment in the Chinese Clinical Trial Registry (Reference number: ChiCTR-IOR-17013358, Principal investigator: Weijia Du, Date of registration: November 13, 2017). Informed consent was obtained from all of the participants.
Consent for Publication
All authors have read the manuscript, attest to the validity and legitimacy of the data and its interpretation, and agree to its publication.
Acknowledgments
WD participated in the design and conducted the study, analyzed the data, and prepared the manuscript. YS participated in the design and conducted the study, analyzed the data and prepared the manuscript. JL participated in collecting and analyzing the data and contributed to preparation of the manuscript. XZ participated in collecting and analyzing the data and contributed to preparation of the manuscript. ZX led in the design supervised the performance of the study, participated in analyzing of data, and participated in the preparation of the manuscript. ZL led in the design and oversaw performance of the study, reviewed and analyzed data, and supervised preparation of the manuscript.
Funding
This work was supported in part by the Clinical Research Plan of SHDC (SHDC22020205), Science and Technology Commission of Shanghai Municipality (19401930500) and Research Fund of Shanghai Association of Chinese Integrative Medicine.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Spellacy WN, Handler A, Ferre CD. A case-control study of 1253 twin pregnancies from a 1982–1987 perinatal data base. Obstet Gynecol. 1990;75(2):168–171.
2. Kuleva M, Youssef A, Maroni E, et al. Maternal cardiac function in normal twin pregnancy: a longitudinal study. Ultrasound Obstet Gynecol. 2011;38(5):575–580. doi:10.1002/uog.8936
3. Ghi T, Degli Esposti D, Montaguti E, et al. Maternal cardiac evaluation during uncomplicated twin pregnancy with emphasis on the diastolic function. Am J Obstet Gynecol. 2015;213(376):e1–8. doi:10.1016/j.ajog.2015.05.003
4. Sima RM, Findeklee S, Badarau IA, et al. Comparison of maternal third trimester hemodynamics between singleton pregnancy and twin pregnancy. J Perinat Med. 2021;49(5):566–571. doi:10.1515/jpm-2020-0169
5. Lavie A, Ram M, Lev S, et al. Maternal hemodynamics in late gestation and immediate postpartum in singletons vs. twin pregnancies. Arch Gynecol Obstet. 2018;297(2):353–363. doi:10.1007/s00404-017-4601-8
6. Ngan Kee WD, Khaw KS, Ng FF, et al. A prospective comparison of vasopressor requirement and hemodynamic changes during spinal anesthesia for cesarean delivery in patients with multiple gestation versus singleton pregnancy. Anesth Analg. 2007;104(2):407–411. doi:10.1213/01.ane.0000252461.97656.3e
7. Jawan B, Lee JH, Chong ZK, Chang CS. Spread of spinal anaesthesia for caesarean section in singleton and twin pregnancies. Br J Anaesth. 1993;70(6):639–641. doi:10.1093/bja/70.6.639
8. Mon W, Stewart A, Fernando R, et al. Cardiac output changes with phenylephrine and ephedrine infusions during spinal anesthesia for cesarean section: a randomized, double-blind trial. J Clin Anesth. 2017;37:43–48. doi:10.1016/j.jclinane.2016.11.001
9. Jain K, Makkar JK, Subramani VS, Gander S, Kumar P. A randomized trial comparing prophylactic phenylephrine and ephedrine infusion during spinal anesthesia for emergency cesarean delivery in cases of acute fetal compromise. J Clin Anesth. 2016;34:208–215. doi:10.1016/j.jclinane.2016.03.015
10. Vallejo MC, Attaallah AF, Elzamzamy OM, et al. An open-label randomized controlled clinical trial for comparison of continuous phenylephrine versus norepinephrine infusion in prevention of spinal hypotension during cesarean delivery. Int J Obstet Anesth. 2017;29:18–25. doi:10.1016/j.ijoa.2016.08.005
11. Ngan Kee WD, Khaw KS, Tam YH, Ng FF, Lee SW. Performance of a closed-loop feedback computer-controlled infusion system for maintaining blood pressure during spinal anaesthesia for caesarean section: a randomized controlled comparison of norepinephrine versus phenylephrine. J Clin Monit Comput. 2017;31(3):617–623. doi:10.1007/s10877-016-9883-z
12. Ngan KWD. A random-allocation graded dose-response study of Norepinephrine and Phenylephrine for treating hypotension during spinal Anesthesia for Cesarean delivery. Anesthesiology. 2017;127(6):934–941. doi:10.1097/ALN.0000000000001880
13. Ngan Kee WD, Lee SW, Ng FF, Tan PE, Khaw KS. Randomized double-blinded comparison of norepinephrine and phenylephrine for maintenance of blood pressure during spinal anesthesia for cesarean delivery. Anesthesiology. 2015;122(4):736–745. doi:10.1097/ALN.0000000000000601
14. Rovinsky JJ, Jaffin H. Cardiovascular hemodynamics in pregnancy. II. Cardiac output and left ventricular work in multiple pregnancy. Am J Obstet Gynecol. 1966;95(6):781–786. doi:10.1016/0002-9378(660079-2
15. Kametas NA, McAuliffe F, Krampl E, Chambers J, Nicolaides KH. Maternal cardiac function in twin pregnancy. Obstet Gynecol. 2003;102(4):806–815. doi:10.1016/s0029-7844(030807-x
16. Robson SC, Boys RJ, Rodeck C, Morgan B. Maternal and fetal haemodynamic effects of spinal and extradural anaesthesia for elective caesarean section. Br J Anaesth. 1992;68(1):54–59. doi:10.1093/bja/68.1.54
17. Ngan Kee WD, Lee SW, Khaw KS, Ng FF. Haemodynamic effects of glycopyrrolate pre-treatment before phenylephrine infusion during spinal anaesthesia for caesarean delivery. Int J Obstet Anesth. 2013;22(3):179–187. doi:10.1016/j.ijoa.2013.03.008
18. Matthews JN, Altman DG, Campbell MJ, Royston P. Analysis of serial measurements in medical research. BMJ. 1990;300(6719):230–235. doi:10.1136/bmj.300.6719.230
19. Chun R, Baghirzada L, Tiruta C, Kirkpatrick AW. Measurement of intra-abdominal pressure in term pregnancy: a pilot study. Int J Obstet Anesth. 2012;21(2):135–139. doi:10.1016/j.ijoa.2011.10.010
20. Langesaeter E, Dyer RA. Maternal haemodynamic changes during spinal anaesthesia for caesarean section. Curr Opin Anaesthesiol. 2011;24(3):242–248. doi:10.1097/ACO.0b013e32834588c5
21. Shen CL, Hung YC, Chen PJ, Tsao CM, Ho YY. Mobitz type II AV block during spinal anesthesia. Anesthesiology. 1999;90(5):1477–1478. doi:10.1097/00000542-199905000-00034
22. Higuchi H, Takagi S, Zhang K, Furui I, Ozaki M. Effect of lateral tilt angle on the volume of the abdominal aorta and inferior vena cava in pregnant and nonpregnant women determined by magnetic resonance imaging. Anesthesiology. 2015;122(2):286–293. doi:10.1097/ALN.0000000000000553
23. Fujita N, Higuchi H, Sakuma S, et al. Effect of right-lateral versus left-lateral tilt position on compression of the inferior vena cava in pregnant women determined by magnetic resonance imaging. Anesth Analg. 2019;128(6):1217–1222. doi:10.1213/ANE.0000000000004166
24. Rosseland LA, Hauge TH, Grindheim G, Stubhaug A, Langesaeter E. Changes in blood pressure and cardiac output during cesarean delivery: the effects of oxytocin and carbetocin compared with placebo. Anesthesiology. 2013;119(3):541–551. doi:10.1097/ALN.0b013e31829416dd
25. Dyer RA, Piercy JL, Reed AR, et al. Comparison between pulse waveform analysis and thermodilution cardiac output determination in patients with severe pre-eclampsia. Br J Anaesth. 2011;106(1):77–81. doi:10.1093/bja/aeq292
26. Langesaeter E, Rosseland LA, Stubhaug A. Continuous invasive blood pressure and cardiac output monitoring during cesarean delivery: a randomized, double-blind comparison of low-dose versus high-dose spinal anesthesia with intravenous phenylephrine or placebo infusion. Anesthesiology. 2008;109(5):856–863. doi:10.1097/ALN.0b013e31818a401f
27. Stewart A, Fernando R, McDonald S, et al. The dose-dependent effects of phenylephrine for elective cesarean delivery under spinal anesthesia. Anesth Analg. 2010;111(5):1230–1237. doi:10.1213/ANE.0b013e3181f2eae1
28. Allen TK, George RB, White WD, Muir HA, Habib AS. A double-blind, placebo-controlled trial of four fixed rate infusion regimens of phenylephrine for hemodynamic support during spinal anesthesia for cesarean delivery. Anesth Analg. 2010;111(5):1221–1229. doi:10.1213/ANE.0b013e3181e1db21
29. Hughes SCLG, Rosen MA. Anesthesia for Obstetrics. Lippincott Williams and Wilkins; 2002.
30. Kinsella SM, Carvalho B, Dyer RA, et al. International consensus statement on the management of hypotension with vasopressors during caesarean section under spinal anaesthesia. Anaesthesia. 2018;73(1):71–92. doi:10.1111/anae.14080
31. Sharkey AM, Siddiqui N, Downey K, et al. Comparison of intermittent intravenous boluses of phenylephrine and norepinephrine to prevent and treat spinal-induced hypotension in cesarean deliveries: randomized controlled trial. Anesth Analg. 2019;129(5):1312–1318. doi:10.1213/ANE.0000000000003704
32. Wang X, Mao M, Zhang SS, et al. Bolus norepinephrine and phenylephrine for maternal hypotension during elective cesarean section with spinal anesthesia: a randomized, double-blinded study. Chin Med J. 2020;133(5):509–516. doi:10.1097/CM9.0000000000000621
33. Ngan Kee WD, Khaw KS, Ng FF. Prevention of hypotension during spinal anesthesia for cesarean delivery: an effective technique using combination phenylephrine infusion and crystalloid cohydration. Anesthesiology. 2005;103(4):744–750. doi:10.1097/00000542-200510000-00012
34. Hasanin A, Amin S, Refaat S, et al. Norepinephrine versus phenylephrine infusion for prophylaxis against post-spinal anaesthesia hypotension during elective caesarean delivery: a randomised controlled trial. Anaesth Crit Care Pain Med. 2019;38(6):601–607. doi:10.1016/j.accpm.2019.03.005
35. Ngan Kee WD, Lee A, Khaw KS, et al. A randomized double-blinded comparison of phenylephrine and ephedrine infusion combinations to maintain blood pressure during spinal anesthesia for cesarean delivery: the effects on fetal acid-base status and hemodynamic control. Anesth Analg. 2008;107(4):1295–1302. doi:10.1213/ane.0b013e31818065bc
36. Owen VS, Rosgen BK, Cherak SJ, et al. Adverse events associated with administration of vasopressor medications through a peripheral intravenous catheter: a systematic review and meta-analysis. Crit Care. 2021;25(1):146. doi:10.1186/s13054-021-03553-1
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.