Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
Comparison of Pathway Referrals for Liver Fibrosis Risk Stratification Performed in Diabetology and Nutrition Clinics
Authors Caussy C ![]() , Telliam C, Al-Nuaimi B, Maynard-Muet M, Dumortier J, Zoulim F, Disse E, Colin C, Levrero M, Moulin P
, Telliam C, Al-Nuaimi B, Maynard-Muet M, Dumortier J, Zoulim F, Disse E, Colin C, Levrero M, Moulin P
Received 7 February 2023
Accepted for publication 27 April 2023
Published 8 June 2023 Volume 2023:16 Pages 1721—1729
DOI https://doi.org/10.2147/DMSO.S407511
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Cyrielle Caussy,1– 3 Charlène Telliam,2,4 Bader Al-Nuaimi,2 Marianne Maynard-Muet,5,6 Jérôme Dumortier,3,7 Fabien Zoulim,3,5,6 Emmanuel Disse,1– 3 Cyrille Colin,3,8 Massimo Levrero,3,5,6 Philippe Moulin1,3,4
1CarMen Laboratory, INSERM, INRA, INSA Lyon, Université Claude Bernard Lyon 1, Pierre-Bénite, 69495, France; 2Département Endocrinologie, Diabète et Nutrition, Hôpital Lyon Sud, Hopices Civils de Lyon, Pierre-Bénite, 69495, France; 3Université de Lyon, Université Claude Bernard, Lyon, France; 4Département Endocrinologie, Diabète et Nutrition, Hôpital Cardiologique, Hospices Civils de Lyon, Bron, France; 5Service d’Hépatologie, Hôpital Croix-Rousse, Hospices Civils de Lyon, Lyon, France; 6Centre de Recherche sur le Cancer de Lyon, INSERM, Unité 1052, CNRS, UMR 5286, Lyon, France; 7Fédération des Spécialités Digestives, Hôpital Edouard Herriot, Hospices Civils de Lyon, Lyon, France; 8Unité d’Evaluation Médico-Economique, Pôle Information Médicale Evaluation Recherche, Hospices Civils de Lyon, Lyon, France
Correspondence: Cyrielle Caussy, Service d’Endocrinologie, Diabète et Nutrition, Hôpital Lyon Sud, 165 Chemin du Grand Revoyet, Pierre-Bénite, 69495, France, Tel +33478864448, Fax + 33478863019, Email [email protected]
Purpose: A systematic screening for the presence of nonalcoholic fatty liver disease (NAFLD)-related advanced fibrosis is currently recommended in patients with type 2 diabetes mellitus (T2DM) and obesity. However, real-world data of such liver fibrosis risk stratification pathway from diabetology and nutrition clinics towards hepatology clinics are scarce. Therefore, we compared data from two pathways with or without transient elastography (TE) performed in diabetology and nutrition clinics.
Patients and Methods: This is a retrospective study comparing the proportion of patients with intermediate/high risk of advanced fibrosis (AF) as defined by a liver stiffness measurement (LSM) ≥ 8kPa, among patients referred in hepatology from two diabetology-nutrition departments at Lyon University Hospital, France between November 1st 2018 to December 31st 2019.
Results: Among the two diabetology and nutrition departments using TE or not, 27.5% (62/225) versus 44.2% (126/285) were referred to hepatology, respectively. The pathway using TE in diabetology and nutrition referred to hepatology a higher proportion of patients with intermediate/high risk of AF compared to the pathway without TE: 77.4% versus 30.9%, p< 0.001. In the pathway with TE, the odds of patients with intermediate/high risk of AF referred to hepatology was significantly higher: OR: 7.7, 95% CI: 3.6– 16.7, p< 0.001 after adjustment for age, sex and presence of obesity and T2D compared to the pathway without TE in diabetology and nutrition clinics. However, among the patients not referred, 29.4% had an intermediate/high risk of AF.
Conclusion: A pathway-referral using TE performed in diabetology and nutrition clinics, significantly improves the liver fibrosis risk stratification and avoids over-referral. However, collaboration between diabetologist, nutritionists and hepatologists is needed to avoid under-referral.
Keywords: nonalcoholic fatty liver disease, FibroScan, cirrhosis, transient elastography, obesity, type 2 diabetes, screening
Introduction
Non-alcoholic fatty liver disease (NAFLD) is being recognized as the most common chronic liver disease worldwide, affecting approximately 25% of the global adult population.1 While the majority of patients with NAFLD exhibit benign hepatic steatosis or nonalcoholic fatty liver (NAFL) with minimal risk of progression towards cirrhosis, approximately 25 to 30% will progress towards non-alcoholic steatohepatitis (NASH). This increases the risk of progression towards advanced fibrosis and cirrhosis.2–4 Furthermore, liver fibrosis portends a worse longitudinal prognosis with a long-term increase of overall mortality, liver transplantation, and liver-related events justifying the need to detect patients with advanced fibrosis in order to improve their management and clinical care.5–8 Given the large prevalence of NAFLD, including a majority of patients without advanced fibrosis, population-based screening is not warranted due to the lack of cost-effectiveness which would lead to overwhelming health care systems.9 However, risk stratification and case-finding strategies, based upon risk factors in selected population at high risk for advanced fibrosis, is currently recommended by several society guidelines.10–13
Patient with type 2 diabetes mellitus (T2DM) and obesity are recognized as population at high risk of NAFLD-related advanced fibrosis and are identified as priority target for these screening strategies.10–13 Recent guidelines have reinforced the need for such screening and recommend a two-step approach based upon easily available blood-based non-invasive tests (NIT), such as FIB-4 score as a first-line test, followed by more specific patented blood-based tests or imaging-based tests, such as transient elastography, depending on their availability.10–12,14 Despite these guidelines, NAFLD and advanced fibrosis are largely underdiagnosed and the implementation of the two-step screening strategy remains challenging as it requires multidisciplinary collaboration, especially between endocrinologists and hepatologists. Furthermore, whether the second line NITs should be performed prior to the referral in hepatology or in the liver clinics, varies across the guidelines. This pivotal point would need clarification in order to ensure a successful implementation in clinical practice. Hence, real-world data of scenarios implementing these pathways are crucially needed and are currently scarce.15 Indeed, providing real-world data from routinely collected clinical data have the potential to better inform clinical care decision making that could lead to public health benefit by enabling the development of new models of care. Therefore, we report real-world data comparing two different pathway referral strategies implemented in diabetology and nutrition clinics for patients with NAFLD according TE availability in diabetology and nutrition clinics.
Materials and Methods
Population and Study Design
This is a retrospective comparative study from two diabetology and nutrition departments in the Lyon University Hospital (Hospices Civils de Lyon) which implemented distinct screening strategies for NAFLD-related advanced fibrosis based upon availability of TE assessment in diabetology and nutrition.
Data from adult patients who underwent a screening for liver advanced fibrosis in the departments of diabetology and nutrition at the Lyon South Hospital and at the Lyon East Hospital within Hospices Civils de Lyon between November 1st 2018 to December 31st 2019, were systematically extracted from electronic medical records and collected using a specifically dedicated computerized database. Clinical data including demographic, anthropometric, biological and imaging data were extracted from electronic charts. Other causes of chronic liver diseases were excluded including: viral hepatitis, autoimmune hepatitis, excessive alcohol consumption (defined as >30g/day for males and >15g/day for females for a period longer than 2 years at any times in the last 10 years), hemochromatosis, Wilson disease, medications known to produce steatosis, such as corticosteroids, high-dose estrogen, tamoxifen, methotrexate, amiodarone in the previous 6 months or genetic lipid disorders, including hypobetalipoproteinemia.
Definition and Endpoints
Patients with intermediate/high risk of advanced fibrosis were defined as patients with a valid liver stiffness measurement (LSM) ≥ 8 kPa.11 Patients with low risk of advanced fibrosis were defined as patients with a valid LSM < 8kPa or invalid LSM, and other second line tests such as Fibrotest® <0.48, according to the recent EASL guidelines.11
The primary endpoint of the study was the proportion of patients with intermediate/high risk of AF among patients referred in the hepatology department.
Liver Stiffness Assessment
LSM was performed using a FibroScan® (Echosens, Paris) by trained medical doctors at the fasting state of at least 4 hours using either M or XL probe when indicated and according to the manufacturer recommendations as previously described.16
Ethic Statement
All the data was collected in the context of clinical care and were pseudonymized. The study was performed in strict compliance with the French reference methodology MR-004, established by French National Commission on Informatics and Liberties (CNIL). Patients received a written notice and had the possibility to object to the use of their data. The study was approved by the Research Ethics Commission of Lyon-University-Hospital IRB 22_584.
Statistical Analysis
Descriptive analyses were performed using SPSS 21.0 (IBM, SPSS, Chicago, IL, USA). Continuous variables were expressed as mean ± standard deviation (SD) or median, IQR when appropriate and categorical variables as a percentage. Comparisons between groups were performed using Student’s unpaired t-test, Mann Whitney test, Chi-Square or Fisher exact test, as appropriate. The comparison of the proportion of patients with intermediate/high probability of AF between the two referral pathways were performed by logistic regression in univariate and multivariable model. A 2-sided p-value < 0.05 was considered statistically significant.
Results
Description of the Two Pathway Referrals for Risk Stratification of Patient with NAFLD in Diabetology and Nutrition
The referral pathway 1 implemented at Lyon South Hospital had no TE assessment available on site. It applied a systematic and standardized screening based upon the 2016 EASL-EASD-EASO clinical practice guidelines for the Management of NAFLD.14 Patients with either T2DM or obesity with hepatic steatosis, diagnosed by abdominal ultrasound, were systematically screened for NAFLD-related advanced fibrosis with a first line test using the NAFLD Fibrosis Score (NFS).17 Patients with abnormal liver enzymes or with mild/moderate or high risk of advanced fibrosis, as defined by an NFS ≥ −1.455, were referred to the hepatology department for additional tests including TE assessment using a FibroScan® and if needed, specialized care and follow-up.
The referral pathway 2, implemented at Lyon East Hospital, had a TE assessment available, performed on site using a FibroScan® prior to referral to the hepatology department. Patients with T2DM or obesity and hepatic steatosis, underwent a non-systematic and non-standardized screening for NAFLD-related advanced fibrosis. The indication for TE assessment by FibroScan® was not standardized, leaving it to the endocrinologist’s clinical appreciation of either abnormal liver enzymes or NFS.17 Likewise, referral in hepatology department was not standardized and left to the clinical appreciation of the physician.
Baseline Characteristics of the Studied Population
A total of 510 patients with either T2DM or obesity and NAFLD underwent a screening for advanced fibrosis in the two diabetology and nutrition departments Table 1. The pathway 1 included 285 patients with a mean (±SD) age of 53.9 (±13.6) years, BMI of 39.1 (±8.0) kg/m2, 62.8% had T2DM and 87% had obesity Table 1. The pathway 2 included 225 patients with a mean age of 57.1 (±10.8) years, BMI of 33.5 (±6.0) kg/m2, 84.4% had T2DM. Both departments included patients with similar FIB-4 score and AST to ALT ratio Table 1. Among the studied population, 135 patients had intermediate or high risk of advanced fibrosis. As expected, they were significantly older and exhibited a significant higher prevalence of T2DM, hypertension and abnormal liver enzymes compared to patients with low risk of advanced fibrosis Table 2.
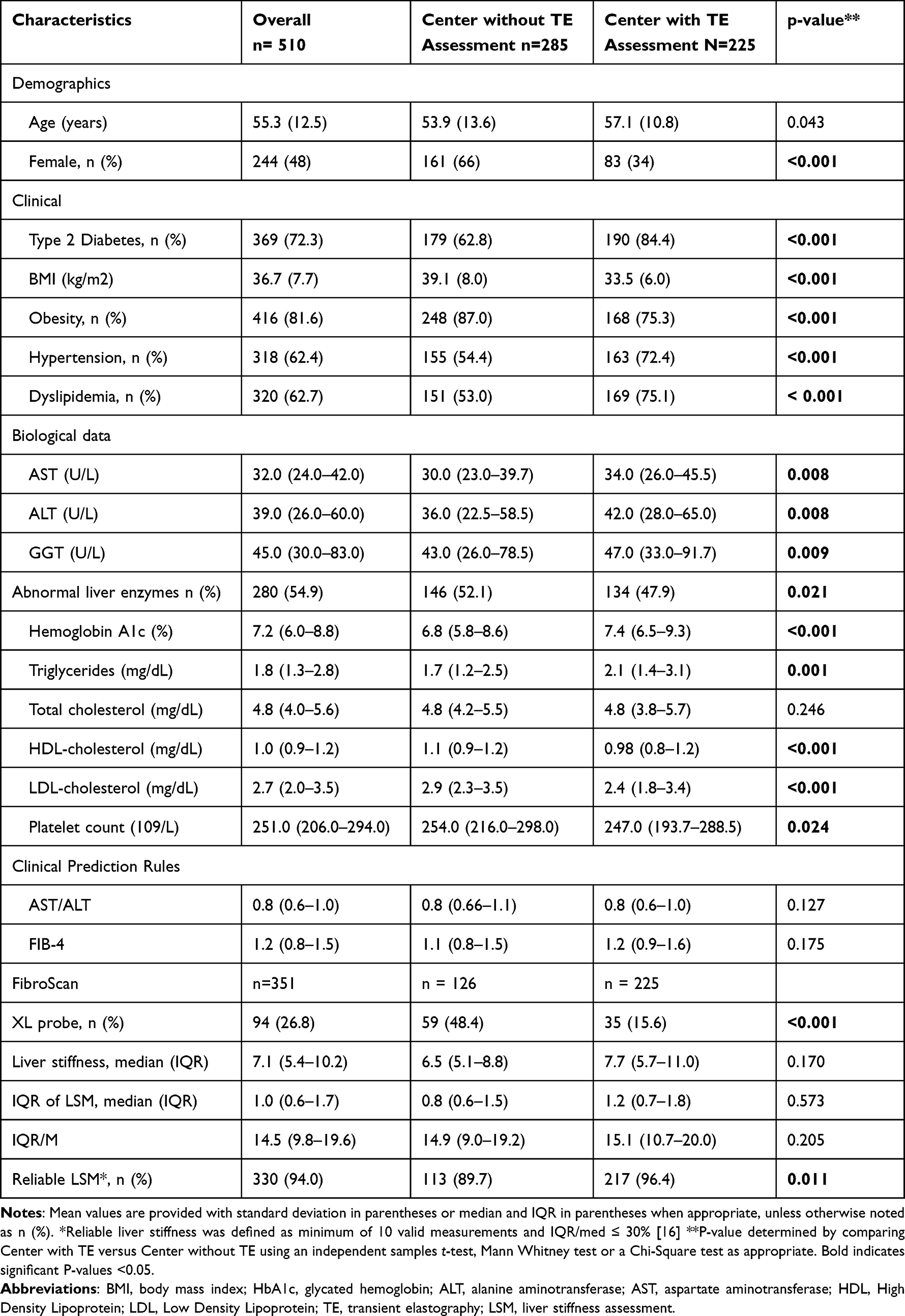 |
Table 1 Patient’s Characteristics |
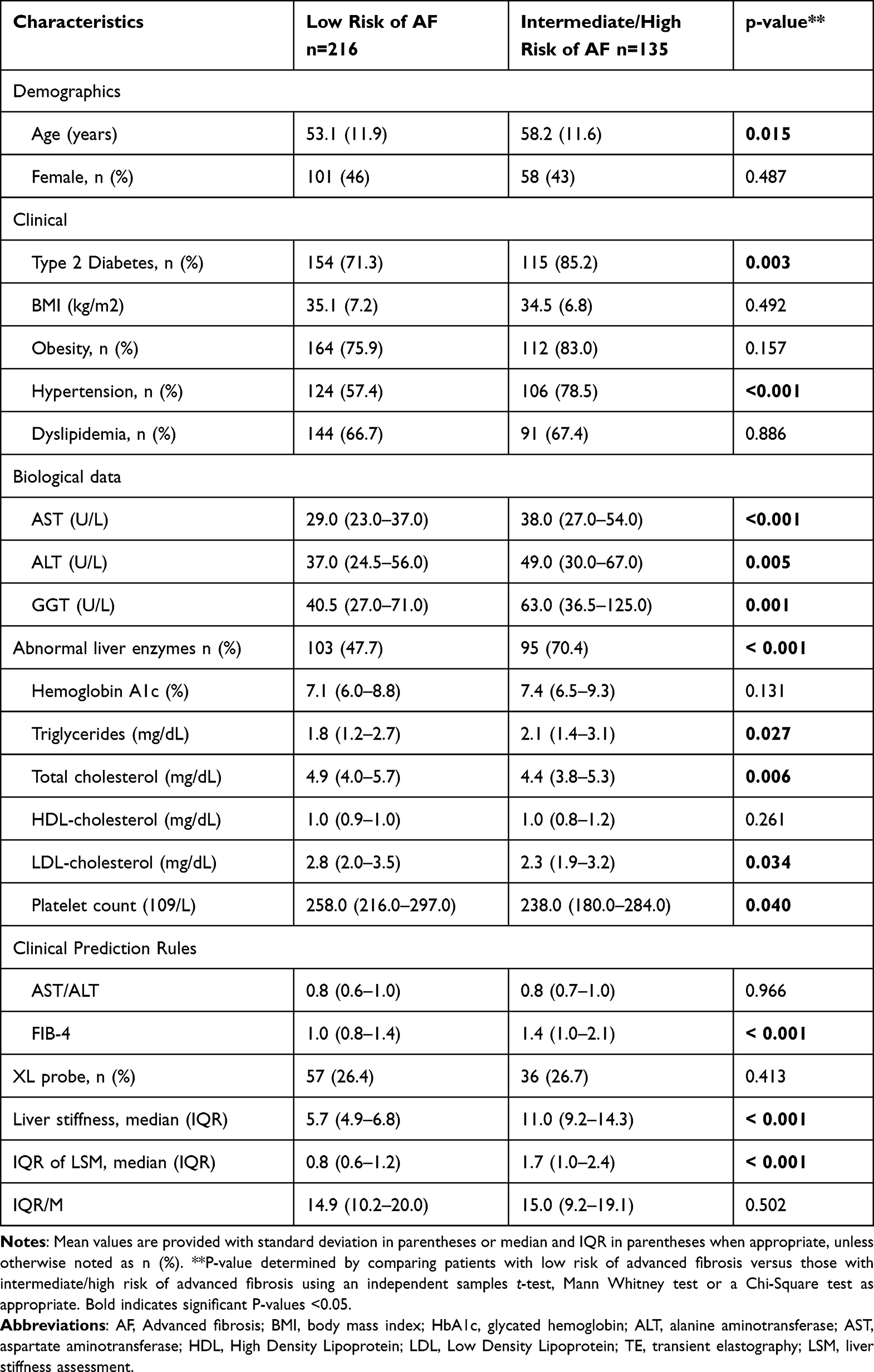 |
Table 2 Patient’s Characteristics Stratified by Risk of Advanced Fibrosis |
Over-Referral of Patients in a Pathway Without TE Performed in Diabetology and Nutrition Clinic
Among the 285 patients with a suspicion of advanced fibrosis referred to hepatology from pathway 1 without TE performed in diabetology and nutrition clinics, only 44.2% (n=126) had a TE assessment in the hepatology department due to the saturation of the pathway referral. Among the 225 patients from the pathway 2 with TE performed in diabetology and nutrition clinics, the proportion of patient referred ito hepatology was lower 27.5% (n=62) and without any over-referral.
Identification of Patients with Advanced Fibrosis in the Pathway Referral with TE Performed in Diabetology and Nutrition Clinic
The proportion of patients with an intermediate/high risk of AF referred to hepatology was significantly higher in the pathway referral with TE performed in diabetology and nutrition clinics: 77.4% (n=48) compared to 30.9% (n=39) in the pathway referral without TE performed in diabetology and nutrition, p<0.001 Figure 1. The odds of patients with intermediate/high risk of AF referred to hepatology was significantly higher in the pathway with TE performed in the diabetology and nutrition clinic than in the pathway without TE performed in diabetology and nutrition: OR: 7.6, 95% CI: 3.8–15.5, p<0.001. These results remained clinically and statistically significant after multivariable adjustment for age, sex, the presence of obesity and T2DM: OR: 7.7, 95% CI: 3.6–16.7, p<0.001.
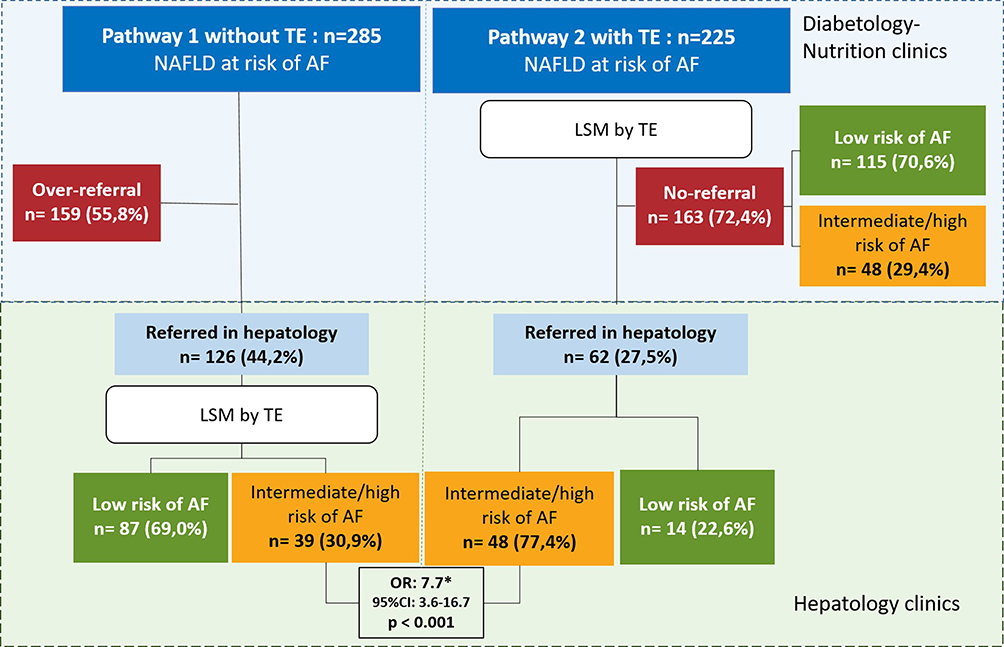 |
Figure 1 Comparison of pathway referrals for risk stratification of liver fibrosis with and without TE in diabetology and nutrition clinics. Abbreviations: TE, Transient elastography; LSM, liver stiffness measurement; AF, advanced fibrosis. Note: *Odd ratios after adjustment for multivariable including age, sex, the presence of DT2M and obesity. |
Potential Under-Referral of Patient with Advanced Fibrosis in the Pathway Referral with TE Performed in Diabetology and Nutrition
In the pathway 2, with TE performed in diabetology and nutrition, the majority (72.4%) of the patients were not referred to hepatology after TE assessment and, among them, 70.6% (n=115) had a low risk of AF. However, among the patients who were not referred to hepatology, 29.2% (n=48) had an intermediate/risk of AF including 6 (3.6%) patients with a high risk of AF with a valid LSM ≥12 kPa.
Discussion
The retrospective comparison of two distinct pathways for the liver fibrosis risk stratification of patients with NAFLD in diabetology and nutrition demonstrates that a pathway with early TE assessment performed in diabetology and nutrition improves the screening strategy for NAFLD-related AF. By reducing the risk of over-referral to hepatology, the screening strategy is improved for NAFLD-related AF and significantly increases the proportion of patients with intermediate/high risk of AF referred to hepatology. However, it also highlights that the lack of standardized pathway referral and education for the interpretation of the NITs, such as threshold of LSM for intermediate/high risk of AF that warrant specialist referral, could lead to an under-referral of these patients to hepatology. Therefore, a close collaboration between diabetologists, nutritionists and hepatologists is needed to implement an optimal multidisciplinary pathway referral for the risk stratification of patients with T2DM and/or obesity and NAFLD in diabetology and nutrition clinics.
Real-world data of risk stratification pathway are scarce. To our knowledge, this is the first study reporting real-world data comparing two pathways of referral with or without TE assessment performed in diabetology and nutrition during the same period.15 A few uncontrolled studies have reported such data of liver fibrosis risk stratification and pathways of referral of patients with NAFLD in primary care based upon other NITs such as shear wave elastography or ELFTM test.18–20 These real-world data studies would greatly help to disseminate and improve the multidisciplinary approaches for case finding of patients with advanced fibrosis. These patients currently remain under-diagnosed, although they require specialized care, follow-up in hepatology and may potentially benefit from novel pharmacological therapies in the near future.21,22 In addition, real world data will help to improve the accessibility of the NITs, providing a better insight into their context of use, utility and patient’s characteristics implemented in such pathways. Overall, this will assist in proposing a uniform model of care supported by health care policies.21
The current study encompasses several strengths, of which comprehensive data from patients with T2DM and/or obesity enrolled in a systematic screening performed by diabetology and nutrition departments during the same 14-month period, is included. Patients entering the pathway were identified using a systematic extraction of electronic medical records, minimizing the risk of missing patients. The same type device was used in diabetology and nutrition and hepatology departments avoiding a systematic bias of measurement of the liver stiffness, and enabling direct comparison.
However, some limitations need to be considered. We were not able to determine the proportion of patients with confirmed histological diagnosis of advanced fibrosis, as only a few patients underwent a liver biopsy in hepatology. However, this also reflects the real-world data of the clinical care of the patients with NAFLD. Indeed, very few patients with NAFLD underwent a liver biopsy which is a procedure performed mostly for clinical-trial purposes in very select population.23 In the lack of liver biopsy results available, we used LSM as an endpoint in order the stratify the risk of advanced fibrosis as LSM using a FibroScan® has been widely studied in large cohorts of patients with biopsy-proven NAFLD including patients with T2DM and is validated for the assessment of the risk of advanced fibrosis.11,24 However the use of LSM as an endpoint whereas it was performed in diabetology in the pathway 2 remains a limitation as it influenced the hepatology referral even though no structural approach were implemented in the pathway 2 and no standardized thresholds of LSM were systematically used for the referral in hepatology in this pathway. Furthermore, the generalization of our findings may not be applicable in other clinical setting using a standardized and structural approach for the screening of NAFLD-related advanced fibrosis. In addition, the population of each center is heterogeneous with different distribution of BMI and prevalence of T2DM. All patients included had metabolic comorbidities associated with a higher risk of liver fibrosis and our results remained clinically and statistically significant after adjustment for these potential confounding factors. The study was performed in a tertiary university hospital and the patient characteristics may differ from other diabetology and nutrition departments thus, the generalization of the data requires additional studies. Finally, we were only able to conduct the study over a 14 month period for the head to head comparison of the two pathways, as the pathway referral 1 without TE was implemented on November 2018. Due to the over-referral in hepatology, this pathway has been equipped with TE after December 2019. Finally, the pathways did not use FIB-4 score as first line NITs, as proposed by the most recent guidelines, but NAFLD Fibrosis Score based upon the previous guideline from 201614 which may have enriched the pathway with patients with FIB-4 below 1.3. Indeed the use of NFS in the pathway 1 may have impacted the over-referral in hepatology as it has been shown that NFS score were less discriminant than the FIB-4 in populations with severe obesity and T2DM.25,26 However, the accuracy of FIB-4 <1.30 in patients with T2DM to rule out patients with intermediate/high risk of AF has been questioned and requires further investigation.27,28 Finally, the retrospective design cannot exclude potential bias in the patient selection and medical decision for hepatology referral, furthering the need for prospective studies using a standardized protocol.29 Such a study is currently ongoing in the two diabetology and nutrition departments from Lyon University Hospital and will help to determine the optimal pathway referral for risk stratification of patients with TD2M and/or obesity and NAFLD in diabetology and nutrition clinics (NCT04435054).
Conclusion
This study demonstrates that a screening strategy for NAFLD-related AF using TE assessment performed in diabetology and nutrition clinics is more efficient compared to a screening strategy without TE assessment performed diabetology and nutrition clinics. However, it highlights the necessity of multidisciplinary interaction between diabetologists, nutritionists and hepatologists in order to ensure optimal clinical care for the patients with NAFLD and avoid any under-referral. Further prospective studies are needed in order to assess the implementation of liver fibrosis risk stratification strategies in high-risk population, such as patients with T2DM and obesity.
Disclosure
Pr Cyrielle Caussy received consultant fees from Gilead, NovoNordisk, AstraZeneca, Lilly, Bayer, E-scopics, Intercept, MSD, Bayer and Echosens. She received grant support from Gilead and E-scopics. Pr Philippe Moulin received honoraria from AKCEA AMGEN AMRYT IONIS NovoNordisk paid to him and/or his institutions. The authors report no other conflicts of interest in this work.
References
1. Younossi ZM, Henry L. Fatty liver through the ages: nonalcoholic steatohepatitis. Endocr Pract. 2022;28(2):204–213. doi:10.1016/j.eprac.2021.12.010
2. Singh S, Allen AM, Wang Z, Prokop LJ, Murad MH, Loomba R. Fibrosis progression in nonalcoholic fatty liver vs nonalcoholic steatohepatitis: a systematic review and meta-analysis of paired-biopsy studies. Clin Gastroenterol Hepatol. 2015;13(4):643–54 e1–e9; quiz e39–e40. doi:10.1016/j.cgh.2014.04.014
3. Vernon G, Baranova A, Younossi ZM. Systematic review: the epidemiology and natural history of non-alcoholic fatty liver disease and non-alcoholic steatohepatitis in adults. Aliment Pharmacol Ther. 2011;34(3):274–285. doi:10.1111/j.1365-2036.2011.04724.x
4. Harrison SA, Torgerson S, Hayashi PH. The natural history of nonalcoholic fatty liver disease: a clinical histopathological study. Am J Gastroenterol. 2003;98(9):2042–2047. doi:10.1111/j.1572-0241.2003.07659.x
5. Angulo P, Kleiner DE, Dam-Larsen S, et al. Liver fibrosis, but no other histologic features, is associated with long-term outcomes of patients with nonalcoholic fatty liver disease. Gastroenterology. 2015;149(2):389–97 e10. doi:10.1053/j.gastro.2015.04.043
6. Ekstedt M Hagstrom H, Nasr P, et al. Fibrosis stage is the strongest predictor for disease-specific mortality in NAFLD after up to 33 years of follow-up. Hepatology. 2015;61 5 :1547–54. doi:10.1002/hep.27368.
7. Loomba R, Chalasani N. The hierarchical model of NAFLD: prognostic significance of histologic features in NASH. Gastroenterology. 2015;149(2):278–281. doi:10.1053/j.gastro.2015.06.016
8. Simon TG, Roelstraete B, Hagstrom H, Sundstrom J, Ludvigsson JF. Non-alcoholic fatty liver disease and incident major adverse cardiovascular events: results from a nationwide histology cohort. Gut. 2022;71(9):1867–1875. doi:10.1136/gutjnl-2021-325724
9. Kanwal F, Shubrook JH, Younossi Z, et al. Preparing for the NASH epidemic: a call to action. Gastroenterology. 2021;161(3):1030–1042 e8. doi:10.1053/j.gastro.2021.04.074
10. Kanwal F, Shubrook JH, Adams LA, et al. Clinical care pathway for the risk stratification and management of patients with nonalcoholic fatty liver disease. Gastroenterology. 2021;161(5):1657–1669. doi:10.1053/j.gastro.2021.07.049
11. European Association for the Study of the Liver. Electronic address eee, Clinical Practice Guideline P, Chair, representative EGB, Panel M. EASL Clinical Practice Guidelines on non-invasive tests for evaluation of liver disease severity and prognosis - 2021 update. J Hepatol. 2021;75(3):659–689. doi:10.1016/j.jhep.2021.05.025
12. Cusi K, Isaacs S, Barb D, et al. American Association of Clinical Endocrinology Clinical Practice Guideline for the diagnosis and management of nonalcoholic fatty liver disease in primary care and endocrinology clinical settings: co-sponsored by the American Association for the Study of Liver Diseases (AASLD). Endocr Pract. 2022;28(5):528–562. doi:10.1016/j.eprac.2022.03.010
13. Draznin B, Aroda VR, Bakris G, et al.; American Diabetes Association Professional Practice C, American Diabetes Association Professional Practice C. 4. Comprehensive medical evaluation and assessment of comorbidities: standards of medical care in diabetes-2022. Diabetes Care. 2022;45(Suppl 1):S46–S59. doi:10.2337/dc22-S004
14. European Association for the Study of the Liver. Electronic address eee, European Association for the Study of D, European Association for the Study of O. EASL-EASD-EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. J Hepatol. 2016;64(6):1388–1402. doi:10.1016/j.jhep.2015.11.004
15. Abeysekera KWM, Macpherson I, Glyn-Owen K, et al. Community pathways for the early detection and risk stratification of chronic liver disease: a narrative systematic review. Lancet Gastroenterol Hepatol. 2022;7(8):770–780. doi:10.1016/S2468-1253(22)00020-6
16. Castera L, Forns X, Alberti A. Non-invasive evaluation of liver fibrosis using transient elastography. J Hepatol. 2008;48(5):835–847. doi:10.1016/j.jhep.2008.02.008
17. Angulo P, Hui JM, Marchesini G, et al. The NAFLD fibrosis score: a noninvasive system that identifies liver fibrosis in patients with NAFLD. Hepatology. 2007;45(4):846–854. doi:10.1002/hep.21496
18. Shaheen AA, Riazi K, Medellin A, et al. Risk stratification of patients with nonalcoholic fatty liver disease using a case identification pathway in primary care: a cross-sectional study. CMAJ Open. 2020;8(2):E370–E376. doi:10.9778/cmajo.20200009
19. Srivastava A, Gailer R, Tanwar S, et al. Prospective evaluation of a primary care referral pathway for patients with non-alcoholic fatty liver disease. J Hepatol. 2019;71(2):371–378. doi:10.1016/j.jhep.2019.03.033
20. Alexander M, Loomis AK, Fairburn-Beech J, et al. Real-world data reveal a diagnostic gap in non-alcoholic fatty liver disease. BMC Med. 2018;16(1):130. doi:10.1186/s12916-018-1103-x
21. Lazarus JV, Anstee QM, Hagstrom H, et al. Defining comprehensive models of care for NAFLD. Nat Rev Gastroenterol Hepatol. 2021;18(10):717–729. doi:10.1038/s41575-021-00477-7
22. Lazarus JV, Mark HE, Anstee QM, et al. Advancing the global public health agenda for NAFLD: a consensus statement. Nat Rev Gastroenterol Hepatol. 2022;19(1):60–78. doi:10.1038/s41575-021-00523-4
23. Anstee QM, Hallsworth K, Lynch N, et al. Real-world management of non-alcoholic steatohepatitis differs from clinical practice guideline recommendations and across regions. JHEP Rep. 2022;4(1):100411. doi:10.1016/j.jhepr.2021.100411
24. Cazac GD, Lacatusu CM, Mihai C, Grigorescu ED, Onofriescu A, Mihai BM. Ultrasound-based hepatic elastography in non-alcoholic fatty liver disease: focus on patients with type 2 diabetes. Biomedicines. 2022;10(10):2375. doi:10.3390/biomedicines10102375
25. Ciardullo S, Muraca E, Perra S, et al. Screening for non-alcoholic fatty liver disease in type 2 diabetes using non-invasive scores and association with diabetic complications. BMJ Open Diabetes Res Care. 2020;8(1):e000904. doi:10.1136/bmjdrc-2019-000904
26. Ciardullo S, Ronchetti C, Muraca E, et al. Impact of using different biomarkers of liver fibrosis on hepatologic referral of individuals with severe obesity and NAFLD. J Endocrinol Invest. 2020;43(7):1019–1026. doi:10.1007/s40618-020-01188-7
27. Boursier J, Hagstrom H, Ekstedt M, et al. Non-invasive tests accurately stratify patients with NAFLD based on their risk of liver-related events. J Hepatol. 2022;76(5):1013–1020. doi:10.1016/j.jhep.2021.12.031
28. Gracen L, Hayward KL, Irvine KM, Valery PC, Powell EE. Low accuracy of FIB-4 test to identify people with diabetes at low risk of advanced fibrosis. J Hepatol. 2022;77(4):1219–1221. doi:10.1016/j.jhep.2022.06.016
29. Gracen L, Hayward KL, Aikebuse M, et al. Implementing the right care in the right place at the right time for non-alcoholic fatty liver disease (NAFLD-RRR study): a study protocol for a community care pathway for people with type 2 diabetes. BMC Health Serv Res. 2022;22(1):487. doi:10.1186/s12913-022-07808-7
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Evaluation of miRNA-143 and miRNA-145 Expression and Their Association with Vitamin-D Status Among Obese and Non-Obese Type-2 Diabetic Patients
Aladel A, Khatoon F, Khan MI, Alsheweir A, Almutairi MG, Almutairi SO, Almutairi FK, Osmonaliev K, Beg MMA
Journal of Multidisciplinary Healthcare 2022, 15:2979-2990
Published Date: 28 December 2022
Association of Serum Leptin and Adiponectin Concentrations with Type 2 Diabetes Biomarkers and Complications Among Saudi Women
Mohammed Saeed W, Nasser Binjawhar D
Diabetes, Metabolic Syndrome and Obesity 2023, 16:2129-2140
Published Date: 13 July 2023
DR10627, a Novel Dual Glucagon‑like Peptide‑1 and Gastric Inhibitory Polypeptide Receptor Agonist for the Treatment of Obesity and Type 2 Diabetes Mellitus
Shao Y, Chen Y, Zhu M, Liu Y, Fang C, Wang M, Sun P, Fu W, Huang J, Sheng S, Huang Y
Diabetes, Metabolic Syndrome and Obesity 2024, 17:1563-1573
Published Date: 6 April 2024
The Regulation of Metabolic Homeostasis by Incretins and the Metabolic Hormones Produced by Pancreatic Islets
Reed J, Bain SC, Kanamarlapudi V
Diabetes, Metabolic Syndrome and Obesity 2024, 17:2419-2456
Published Date: 13 June 2024
Relative Effectiveness and Safety of the GLP-1 (Glucagon-Like Peptide 1) Receptor Agonists, Semaglutide and Liraglutide in the Treatment of Obese Type 2 Diabetics: A Prospective Observational Cohort Study in Poland
Hoffmann K, Michalak M, Paczkowska A
Diabetes, Metabolic Syndrome and Obesity 2025, 18:2723-2738
Published Date: 7 August 2025