Back to Journals » Journal of Pain Research » Volume 14
Comparison of Outcomes After Breast Cancer Surgery Between Inhalational and Propofol-Based Intravenous Anaesthesia: A Systematic Review and Meta-Analysis
Authors Pang QY ![]() , Duan LP, Jiang Y, Liu HL
, Duan LP, Jiang Y, Liu HL
Received 12 April 2021
Accepted for publication 6 June 2021
Published 16 July 2021 Volume 2021:14 Pages 2165—2177
DOI https://doi.org/10.2147/JPR.S315360
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ellen Soffin
Qian-Yun Pang, Li-Ping Duan, Yan Jiang, Hong-Liang Liu
Department of Anesthesiology, Chongqing University Cancer Hospital, Chongqing University, Chongqing, 400030, People’s Republic of China
Correspondence: Hong-Liang Liu
Department of Anesthesiology, Chongqing University Cancer Hospital, Chongqing University, No. 181, Hanyu Road, Shapingba District, Chongqing, 400030, People’s Republic of China
Tel +86 13883686721
Email [email protected]
Background: General anaesthesia is the commonly provided for breast cancer surgery, but the effects of inhalational anaesthesia and propofol-based intravenous anaesthesia on short- and long-term outcomes after breast cancer surgery are not clear. In this study, we conduct a meta-analysis of randomized controlled trials (RCTs) to explore the superior anaesthetic for breast cancer surgery patients.
Methods: We searched the Embase, Medline, Cochrane Library, Web of Science, CNKI, and Wanfang databases (up to January, 2021) for RCTs in which inhalational anaesthesia and propofol-based intravenous anaesthesia were compared and short- and long-term outcomes were assessed in breast cancer surgical patients. The meta-analysis was performed by Stata 12.0.
Results: Twenty RCTs with a total of 2201 patients were included. Compared with inhalational anaesthesia, propofol-based intravenous anaesthesia was associated with more postoperative rescue analgesia (I2=0%, RR: 1.18, 95% CI: 1.07– 1.30, P=0.001) but a lower incidence of postoperative nausea and vomiting (PONV) (I2=25.5%, RR: 0.71, 95% CI: 0.62– 0.81, P< 0.001) and postoperative rescue antiemetics (I2=0%, RR: 0.69, 95% CI: 0.58– 0.82, P< 0.001). Propofol-based intravenous anaesthesia preserved nature killer cell cytotoxicity (I2=86.2%, SMD: 0.76, 95% CI: 0.13– 1.39, P=0.018), decreased IL-6 level (I2=98.0%, SMD: − 3.09, 95% CI: − 5.70– − 0.48, P=0.021) and neutrophil-to-lymphocyte ratio (I2=0%, SMD: − 0.28, 95% CI: − 0.53– − 0.03, P=0.030), and increased 2-year recurrence-free survival rate (I2=0%, RR: 1.10, 95% CI: 1.00– 1.20, P=0.043) but did not affect recurrence or the overall survival rate (P> 0.05).
Conclusion: Propofol-based intravenous anaesthesia increases postoperative rescue analgesia but reduces PONV compared with inhalational anaesthesia in breast cancer surgery. The benefit of propofol over inhalational anaesthetics in the preservation of anti-cancer immunity is obvious, but it is difficult to conclude that propofol can exert long-term benefits due to the small sample size.
Keywords: inhalational anaesthesia, propofol, breast cancer, surgery, outcome, analgesia
Introduction
Breast cancer is one of the most common types of malignancy and is the leading cause of cancer mortality in women.1 Surgical excision is the principle treatment, but surgery-induced stress, anaesthetics, and opioids are factors that adversely influence postoperative recovery and anti-cancer immunity.2,3
General anaesthesia is the main technique for breast surgery, and it includes propofol-based intravenous anaesthesia and inhalational anaesthesia. It was shown that propofol-based intravenous anaesthesia was associated with lower postoperative pain intensity and analgesic consumption in abdominal, orthopaedic, gynaecological surgeries as well as neurosurgery in one meta-analysis,4 but the relationship between propofol and inhalational anaesthetics with postoperative pain outcomes in breast cancer surgery is unclear, and the results are conflicting according to previous studies.5–8 Acute postoperative pain, if not managed properly, can prolong the hospital stay, increase healthcare costs, delay recovery and even lead to chronic pain after breast surgery.9 Opioids are essential during breast surgery and provide analgesia for postoperative pain when necessary, but perioperative opioids can cause many side effects, including postoperative nausea and vomiting (PONV), pruritus and constipation; can inhibit cell-mediated immunity; and can exert potential adverse effects on long-term prognosis.10,11 Therefore, it is necessary and meaningful to elucidate how propofol-based intravenous anaesthesia and inhalational anaesthesia affect postoperative pain outcomes and opioid consumption in breast cancer surgery.
It is known from basic studies that inhalational anaesthetics induce immunosuppression and promote cancer progression and metastasis, but propofol can not.12–14 It seems that propofol-based intravenous anaesthesia has an advantage over inhalational anaesthesia in the preservation of cell-mediated immunity and long-term prognosis in cancer patients. Some recent retrospective observational studies showed that there were no differences between the two anaesthesia methods in recurrence or recurrence-free survival in breast cancer.15,16
Thus, in this study, we conducted a meta-analysis, pooled the related results from prospective randomized controlled trials, and tried to determine the relationship between short- and long-term outcomes with propofol-based intravenous anaesthesia and inhalational anaesthesia in breast cancer surgery.
Methods
This meta-analysis was conducted in accordance with the recommendations from the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines. There was no registered protocol.
Literature Search and Outcome
Databases (Embase, Medline, Cochrane Library, Web of Science, CNKI and Wanfang) were searched. The searched terms were intravenous anaesthesia, TIVA, propofol, propofol-based intravenous anaesthesia, inhalational anaesthesia, sevoflurane, desflurane, isoflurane, xenon, breast cancer, breast surgery, mastectomy and radical mastectomy. The literature search strategy in the Medline database is shown in Appendix 1. The references of related articles were also checked for any further potential eligible trials. The published languages included were English and Chinese. The search ended in January, 2021. The primary outcome was postoperative pain including postoperative rescue analgesia and VAS scores. The secondary outcomes were opioid consumption, PONV, immune function, and long-term prognosis.
Inclusion and Exclusion Criteria
The inclusion criteria were as follows: adult patients, elective surgeries for primary breast cancer in female patients, RCTs of inhalational anaesthesia versus propofol-based intravenous anaesthesia, and inclusion of the primary outcome with or without other outcomes included in the trials. The exclusion criteria were as follows: patients with chronic pain or a history of oral intake analgesics before surgery and studies comparing propofol combined with paravertebral block or epidural block with inhalational anaesthesia.
Data Extraction and Quality Assessment
Data extraction was performed following the predefined criteria by two authors (Pang QY and Duan LP). If necessary, data presented as medians were transferred to mean ± SD,17 and data shown in graphs were transformed to numbers using Plot-digitizer software. We also requested relevant information from the authors via email when necessary. Any discrepancy was resolved after discussion with another two researchers (Jiang Y and Liu HL).
The risk of bias was checked by the modified Jadad score. The highest score was 7, and a study with a Jadad score greater than or equal to 4 was included. Grading of Recommendations, Assessment, Development and Evaluation (GRADE) methodology was used to appraise the overall evidence- based quality of each outcome.
Statistical Analysis
Meta-analysis was conducted using Stata 12.0 software (STATA, College Station). The effect size for continuous data was expressed as the standard mean difference (SMD) with a 95% confidence interval (CI). The effect size for dichotomous outcomes was expressed as the risk ratio (RR) with 95% CI. The χ2test and the I2value were used to determine the level of heterogeneity; in the case of heterogeneity (P<0.1 or I2≥ 50%), a random effect model was used, and subgroup analysis was performed whenever possible to identify the sources of heterogeneity and to test the robustness of uncertainty. In the case of homogeneity (P≥0.1 or I2< 50%), a fixed effect model was used. Publication bias was evaluated using Egger’s test, and there was no significant publication bias if P>0.05.
Trial sequential analysis (TSA) was conducted using TSA0.9.5.5 Beta software (www.ctu.dk/tsa); the required information size (RIS) was estimated using 0.05 for type 1 error, 0.20 for type 2 error, and the relative risk reduction from the control group event rate in low-bias-risk trials included in the meta-analysis. The TSA can be interpreted by viewing the boundaries and assessing whether the cumulative meta-analysis has crossed them.
Results
Literature Search and Retrieval
A total of 1210 articles were initially retrieved, and 20 RCTs with 2201 patients were eventually included in this meta-analysis. One RCT was from Europe, and the others were from Asia. Fourteen studies compared sevoflurane and propofol; 2 studies compared desflurane and propofol; 4 studies compared isoflurane and propofol. The characteristics and quality evaluation of the included RCTs are presented in Table 1, and the literature screening procedure is shown in Figure 1.
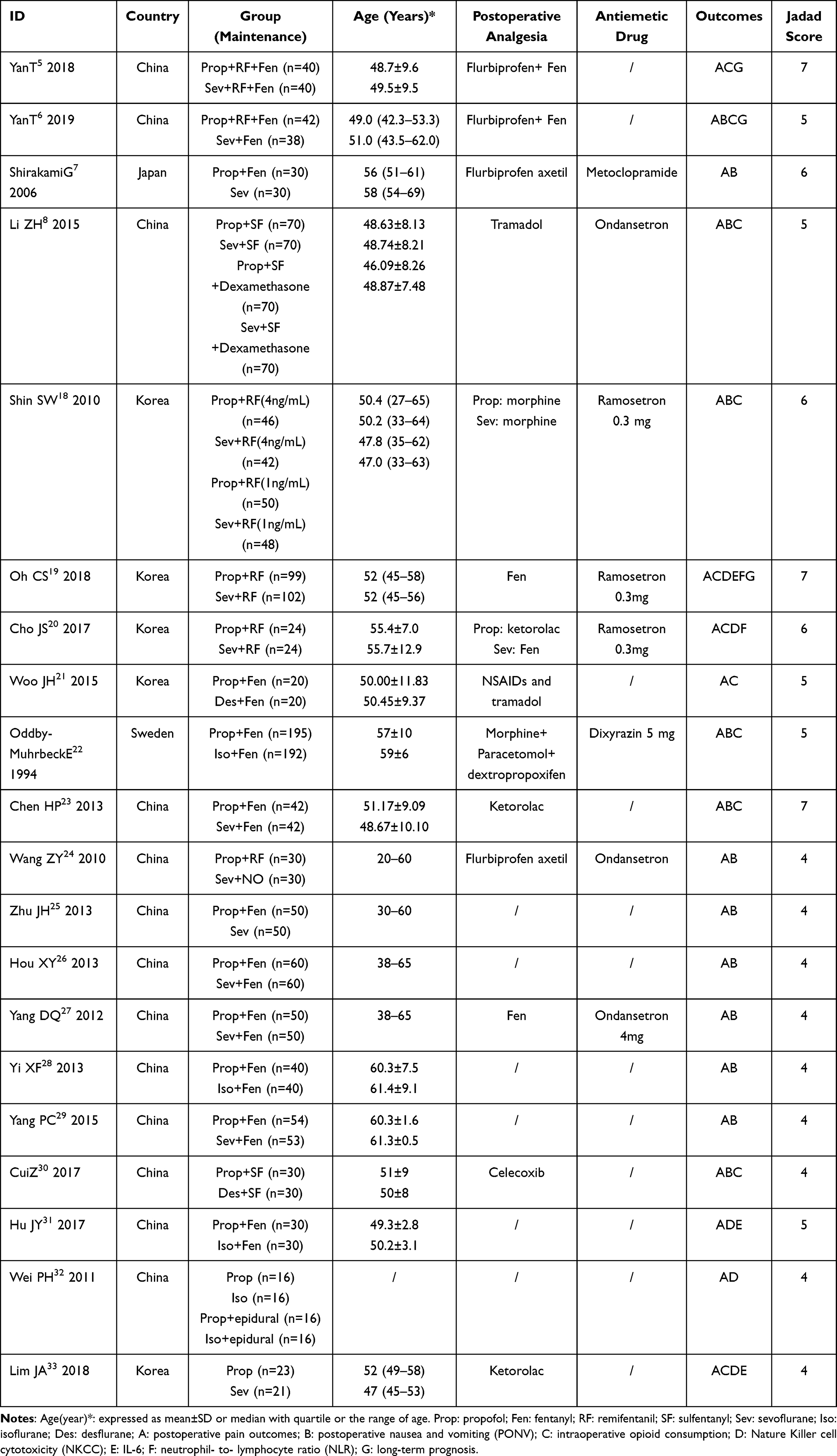 |
Table 1 Characteristics of the Trials |
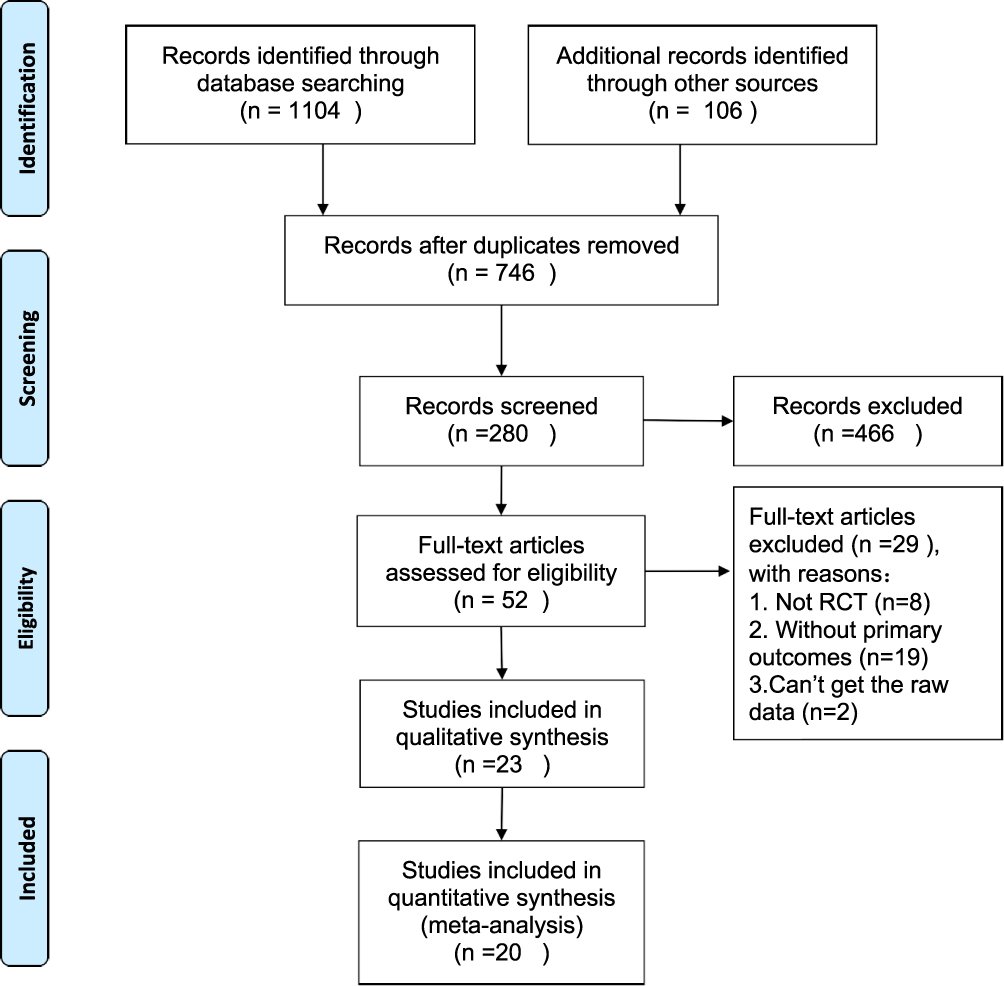 |
Figure 1 PRIMA flow diagram. |
Meta-Analysis results (TABLE 2)
Primary Outcome: Postoperative Pain Outcomes
- Postoperative rescue analgesia
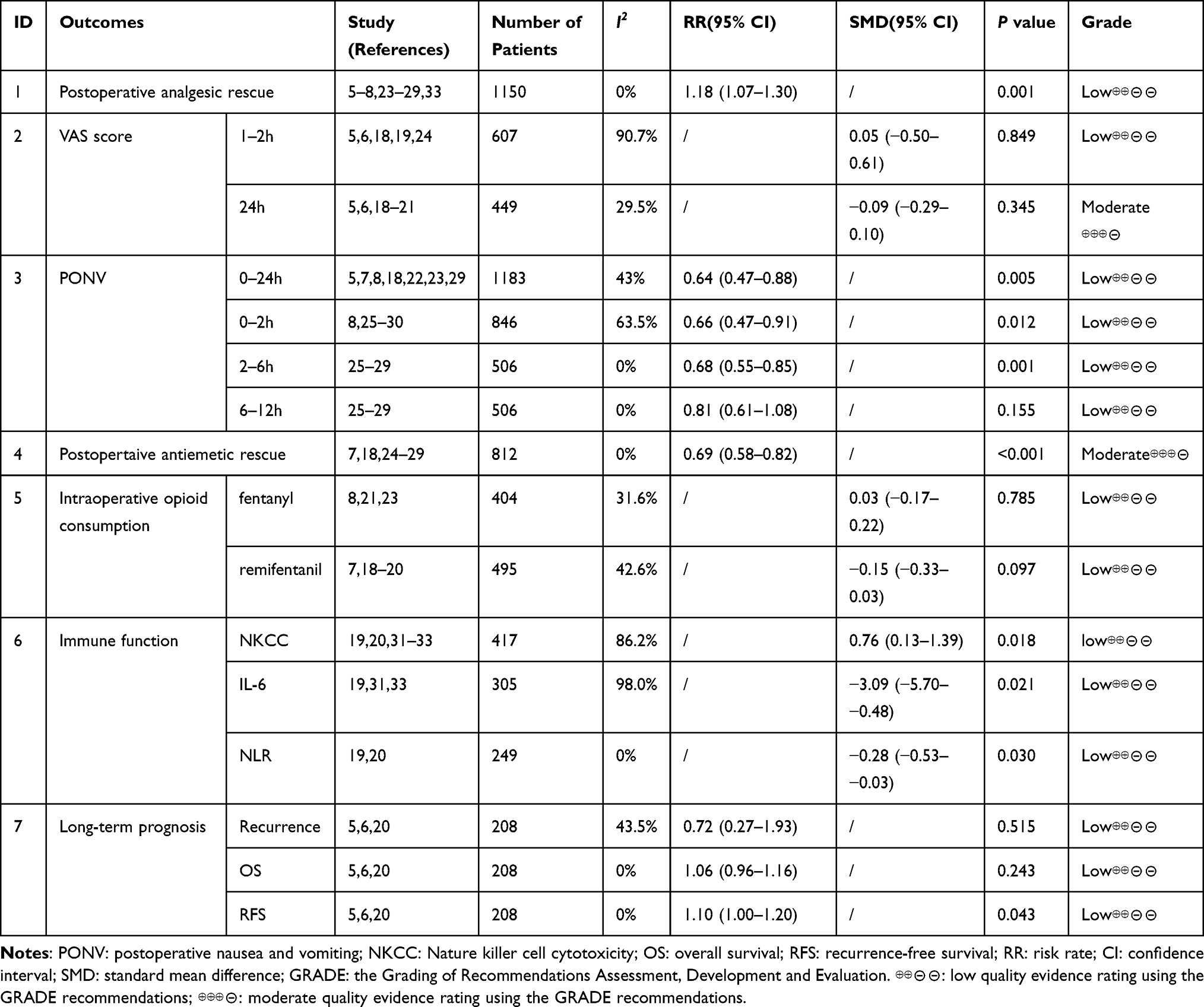 |
Table 2 Summary of Meta-Analysis |
Data on the rate of postoperative rescue analgesia were obtained from 12 RCTs (n=1194).5–8,23–29,33 The fixed effect model showed that the rate of postoperative rescue analgesia in the propofol group was higher than that in the inhalational group (I2=0%, RR: 1.18, 95% CI: 1.07–1.30, P=0.001) (Figure 2), and no significant publication bias was found according to Egger’s test (P=0.717). TSA indicated that the sample size in the meta-analysis was higher than the required sample size (n=143).
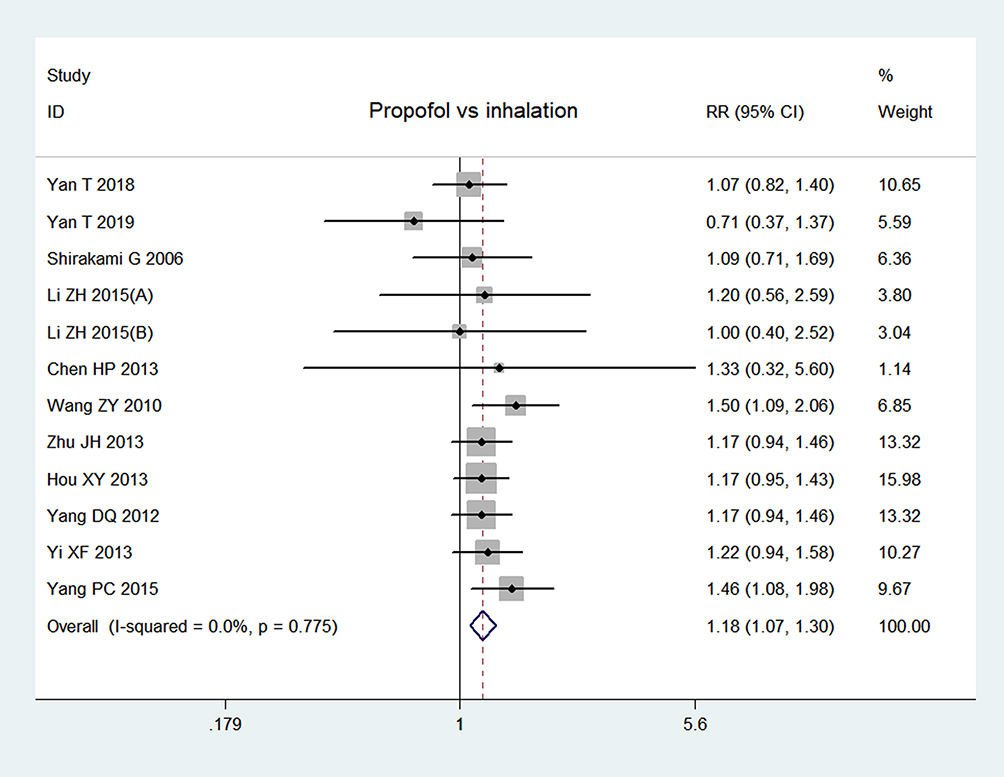 |
Figure 2 Forest plot of postoperative rescue analgesia. Li ZH 2015(A)8: propofol vs sevoflurane; Li ZH 2015(B)8: propofol and dexamethasone vs sevoflurane and dexamethasone. |
A total of 7 RCTs (n=635) reported the postoperative VAS scores at different time points.5,6,18–21,24 The random effect model showed that the VAS scores were not significantly different at 1–2 h (I2=90.7%, SMD: 0.05, 95% CI: −0.50–0.61, P=0.849) or 24 h (I2=29.5%, SMD: −0.09, 95% CI: −0.29–0.10), P=0.652) postoperatively between the propofol and inhalational groups. There was no significant publication bias according to Egger’s test (P=0.353).
Secondary Outcomes
- PONV
Data on the incidence of PONV were obtained from 12 RCTs (n=1643).5,7,8,18,22,23,25–30 The results showed that the incidence of PONV was significantly lower in the propofol group than that in the inhalational group during 0–24 h (I2=43%, RR: 0.64, 95% CI: 0.47–0.88, P=0.005), 0–2 h (I2=63.5%, RR: 0.66, 95% CI: 0.47–0.91, P=0.012), 2–6 h (I2=0%, RR: 0.68, 95% CI: 0.55–0.85, P=0.001) but not during 6–12 h (I2=0%, RR: 0.81, 95% CI: 0.61–1.08, P=0.155) (Figure 3). However, publication bias existed according to Egger’s test (P=0.003). TSA indicated that the sample size for 0–2 h PONV was higher than the required sample size (n=603) but was lower than the required sample size for 0–24 h, 2–6 h, and 6–12 h.
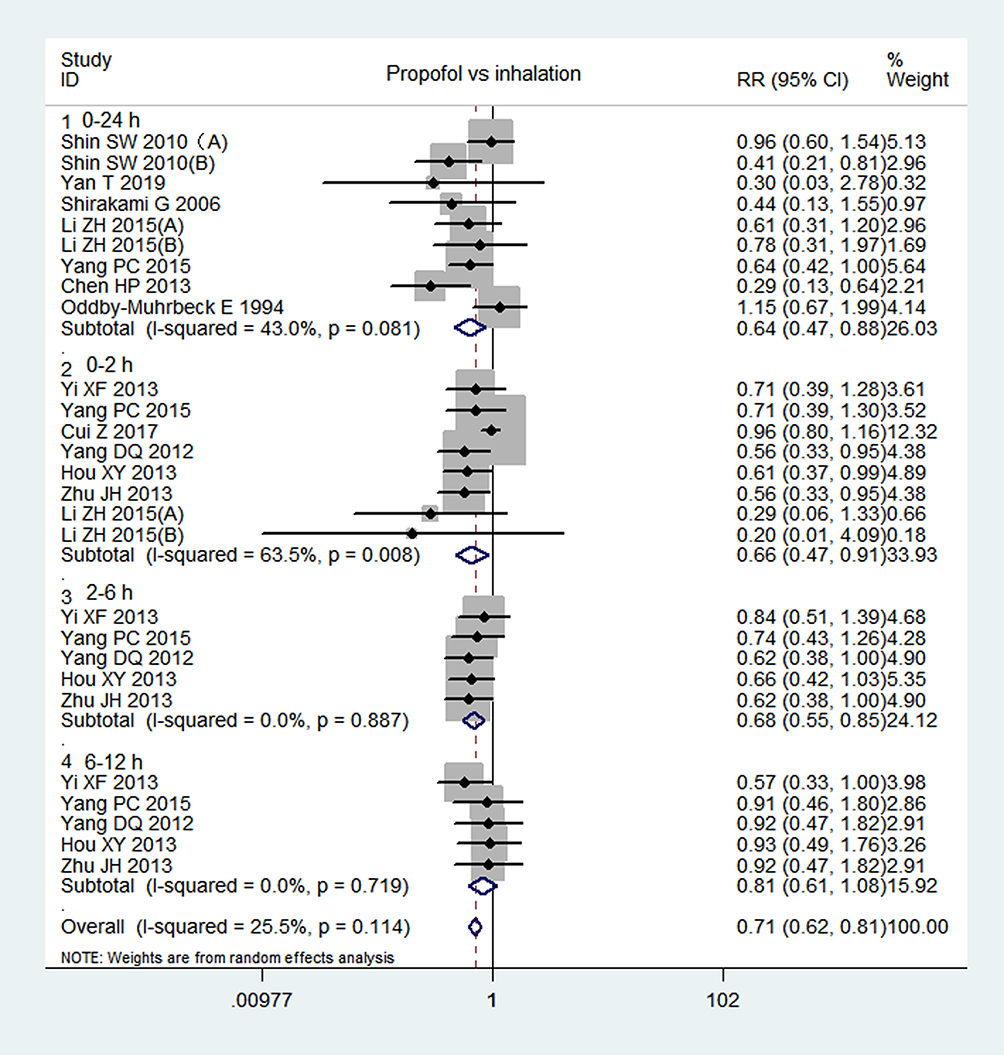 |
Figure 3 Forest plot: comparison of the incidence of PONV between propofol and inhalational anesthesia. Shin SW 2010(A)18: propofol and remifentanil (4 ng/mL) vs sevoflurane and remifentanil (4 ng/mL); Shin SW 2010(B)18: propofol and remifentanil (1 ng/mL) vs sevoflurane and remifentanil (1 ng/mL); Li ZH 2015(A)8: propofol vs sevoflurane; Li ZH 2015(B)8: propofol and dexamethasone vs sevoflurane and dexamethasone. |
Eight RCTs (n=812) reported postoperative rescue antiemetics.7,18,24–29 The fixed effect model showed that the rate of postoperative rescue antiemetics was lower in the propofol group than in the inhalational group (I2=0%, RR: 0.69, 95% CI: 0.58–0.82, P<0.001) (Figure 4), and no significant publication bias was found according to Egger’s test (P=0.979). TSA indicated that the sample size in the meta-analysis was higher than the required sample size (n=392).
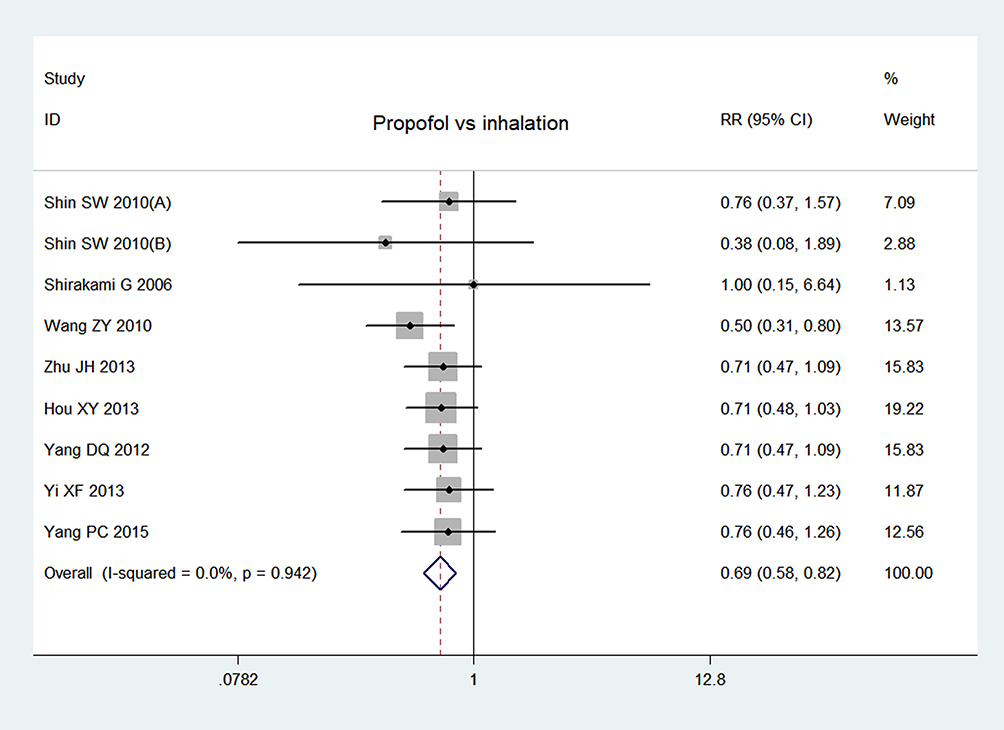 |
Figure 4 Forest plot of postoperative rescue antiemetics. Shin SW 2010(A):18 propofol and remifentanil (4 ng/mL) vs sevoflurane and remifentanil (4 ng/mL); Shin SW 2010(B)18 propofol and remifentanil (1 ng/mL) vs sevoflurane and remifentanil (1 ng/mL). |
Seven RCTs (n=812) reported intraoperative opioid consumption, of which, 3 RCTs8,21,23 and 4 RCTs7,18–20 reported the consumption of fentanyl or remifentanil. The subgroup analysis showed that there were no significant differences between groups in fentanyl (I2=31.6%, SMD:0.03, 95% CI: −0.17–0.22, P=0.785) or remifentanil consumption (I2=42.6%, SMD: −0.15, 95% CI: −0.33–0.03, P=0.097). Publication bias existed according to Egger’s test (P=0.034).
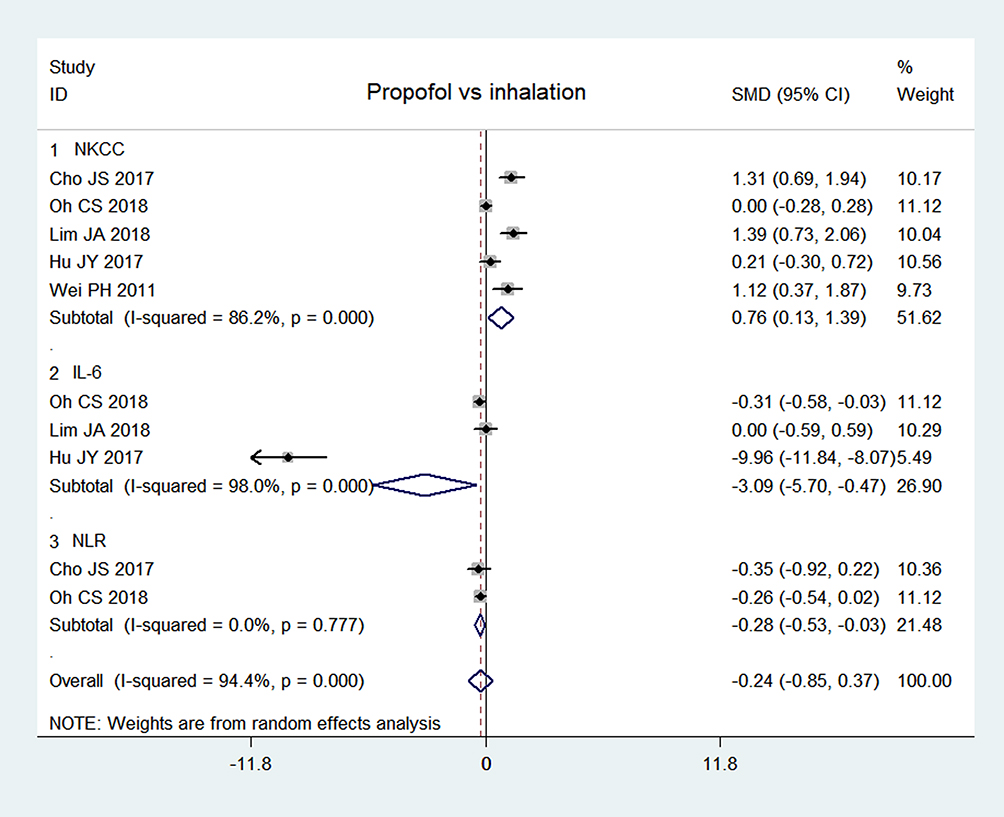 |
Figure 5 Forest plot of immune function. Abbreviations: NKCC, nature killer cell cytotoxicity; NLR, neutrophil to leukomonocyte ratio. |
Data on immune function were obtained from 5 RCTs (n=417), of which, 519,20,31–33, 319,31,33 and 2 RCTs19,20 reported NK cell cytotoxicity (NKCC), IL-6 levels and the NLR respectively. The results showed that NKCC was higher in the propofol group than in the inhalational group (I2=86.2%, SMD: 0.76, 95% CI: 0.13–1.39, P=0.018). The IL-6 level (I2=98.0%, SMD: −3.09, 95% CI: −5.7– −0.48, P=0.021) and NLR (I2=0%, SMD: −0.28, 95% CI: −0.53– −0.03, P=0.030) were lower in the propofol group than in the inhalational group. There was no significant publication bias according to Egger’s test (P=0.731).
Data on long-term prognosis were obtained from only 3 RCTs (n=208).5,6,20 The fixed effect model showed that the 2 year- RFS rate was significantly higher in the propofol group than that in the inhalational group (I2=0%, RR: 1.10, 95% CI: 1.00–1.20, P=0.043). There were no significant between-group differences in the 2 year-recurrence (I2=43.5%, RR: 0.72, 95% CI: 0.27–1.93, P=0.515) or 2 year-OS rate (I2=0%, RR: 1.06, 95% CI: 0.96–1.16, P=0.243) (Figure 6). There was no significant publication bias according to Egger’s test (P=0.634). TSA showed that the required sample size for RFS, recurrence, OS, was 321, 1444, 860, respectively, and the sample size in this meta-analysis was much smaller than the required sample size.
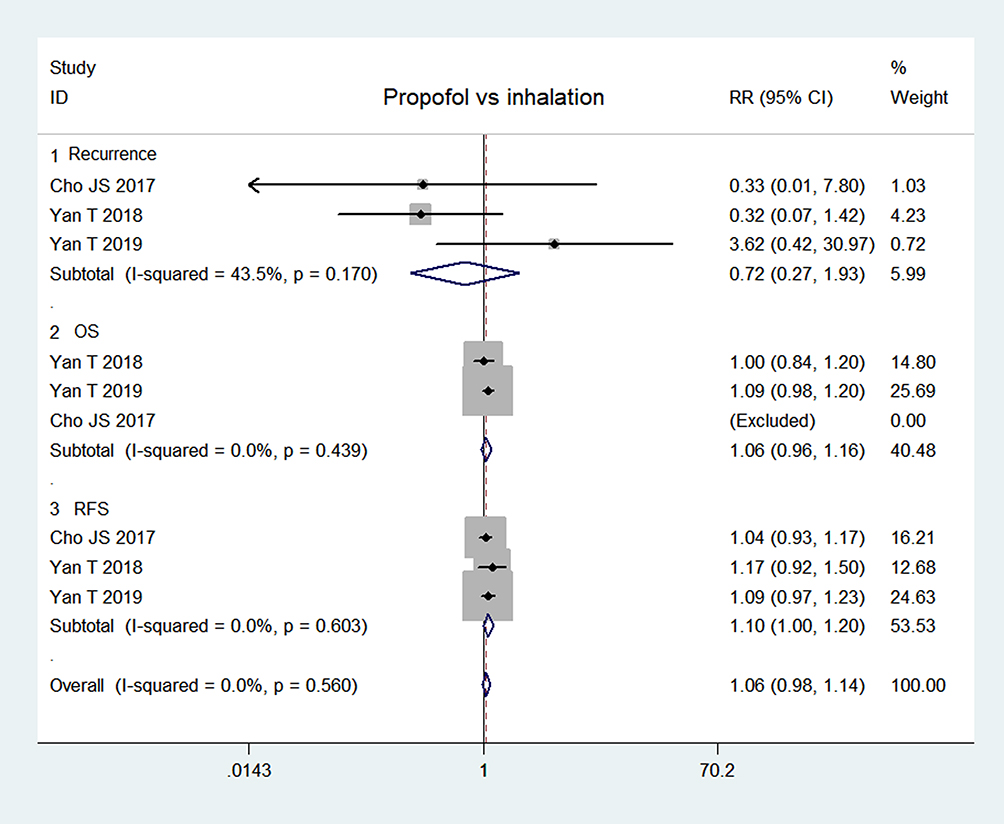 |
Figure 6 Forest plot of long-term outcomes: 2-year recurrence, OS and RFS rates. Abbreviations: OS, overall survival; RFS, recurrence-free survival. |
Discussion
This meta-analysis recruited 20 RCTs that compared propofol-based intravenous anaesthesia and inhalational anaesthesia in terms of postoperative pain outcomes and showed that propofol was associated with higher postoperative rescue analgesia, but the intraoperative opioid consumption and postoperative pain scores were not different between the two anaesthesia methods. As few of the included trials compared postoperative analgesic consumption, and the raw data were difficult to achieve, the evidence of postoperative analgesic consumption could not be pooled in this meta-analysis.
Inhalational anaesthetic suppress sensory afferent input at clinically related concentrations,34 and propofol can reduce neuronal firing at the spinal dorsal horn following noxious stimuli.35,36 However, the clinical evidence from this meta-analysis indicated a benefit of inhalational anaesthesia in alleviating postoperative pain, which conflicted with one earlier meta-analysis in which 39 RCTs were included and only one focused on breast cancer surgery.4 The pooled results showed that propofol reduced postoperative pain intensity, opioid consumption, and rescue analgesia compared with inhalational anaesthesia. The discrepancy might be that the evidence was from different surgical types, and the pain sensitivities were dependent on the type and location of the surgeries.
The incidence of PONV can reach 75% after breast cancer surgery without antiemetics, and approximately 20% of patients still develop PONV even after receiving antiemetic prophylaxis.37 In this study, the incidence of PONV and rescue antiemetics were lower after propofol-based intravenous anaesthesia. Propofol has an antiemetic effect and can reduce PONV by 30–45%.38 However, different kinds of analgesics were used to rescue postoperative pain, and different kinds of antiemetics were administered to reduce PONV in those RCTs, which might influence the results.
Propofol anaesthesia reduced IL-6 levels after breast cancer surgery as shown in the results of this meta-analysis. IL-6 is closely related to the progression and metastasis of breast cancer,39 it facilitates breast cancer cells to produce matrix metallo proteinases (MMPs), and it increases the progression of tumour entities.40 It was reported that targeted IL-6 silencing could reduce the invasion and migration of breast cancer cells.41 NK cells area critical part of cell-mediated immunity and are the main defence against cancer cell propagation.42 It is known that reduced NKCC is associated with poor prognosis in breast cancer.43 The evidence in this study revealed that propofol-based intravenous anaesthesia could preserve NKCC, which was consistent with experimental studies that showed inhalational anaesthetics suppressed NKCC, while propofol did not.44,45 In this study, the NLR was lower after propofol anaesthesia than after inhalational anaesthesia. A high NLR is considered an adverse prognostic indicator for breast cancer.46 Propofol provided a more protective effect against NLR increases than inhalational anaesthetics. Overall, the pooled results of the effects of propofol and inhalational anaesthetics on IL-6, NKCC, and the NLR indicated that propofol could exert a potential beneficial effect on long-term prognosis after breast cancer surgery.
Evidence from 3 RCTs in this meta-analysis showed that propofol was associated with a higher recurrence-free survival rate after breast surgery,5,6,20 but could not reduce recurrence or the overall survival rate. A recent large multicentre RCT (n=2108) from 13 hospital (from Argentina, Austria, China, Germany, Ireland, New Zealand, Singapore, the USA, et al) showed that propofol/paravertebral anaesthesia could not reduce long-term recurrence compared with sevoflurane/opioid anaesthesia in breast cancer surgery,47 but some retrospective studies showed the advantage of propofol-based intravenous anaesthesia over inhalational anaesthesia in reducing long-term recurrence and metastasis.48,49 Different populations have variations of sensitivities to propofol and volatile anesthetics, which is probably due to genetic differences and differences in lifestyle.50 The inconsistency between the results on long-term survival from our meta-analysis and from the previous retrospective studies might be, the populations in our meta-analysis are from China and South Korea, and the sample size is relatively small, so that the results from our meta-analysis are too low to say anything about the long-term outcome. Therefore, it is necessary to conduct a large and international multicentre RCT to verify the potential protective effect of propofol-based intravenous anaesthesia on long-term prognosis.
There are some limitations in this meta-analysis. First, few studies reported postoperative analgesic consumption, and it was difficult to pool the related results for the comparison between propofol-based intravenous anaesthesia and inhalational anaesthesia. Second, only 3 RCTs compared long-term outcomes;5,6,20 the patients were from eastern Asian countries, the sample size was small, and the follow-up time was relatively short. Third, heterogeneity existed in some of the results, so biases cannot be ignored in the meta-analysis. Forth, most of the included RCTs were conducted in Asian countries, as different populations are differently sensitive to propofol and volatile anesthetics, probably modified by both genetic differences and differences in lifestyle, so that the results might not be generalizable. More multinational RCTs need to be done in the near future.
Conclusions
Propofol-based intravenous anaesthesia increases postoperative rescue analgesia in breast cancer surgery and reduces PONV compared with inhalation anaesthesia; the benefit of propofol in the preservation of anti-cancer immunity is obvious over inhalational anaesthetics, but it is difficult to conclude that propofol can exert long-term beneficial effects, and the evidence in this regard should be anticipated from large multinational RCTs.
Abbreviations
RCTs, randomized controlled trials; VAS, visual analogue scale; PONV, postoperative nausea and vomiting; NKCC, nature killer cell cytotoxicity; NLR, neutrophil to leukomonocyte ratio; RFS, recurrence-free survival; OS, overall survival.
Funding
Chongqing Science and health commission medical research project, No: 2021MSXM001.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Siegel RL, Miller KD, Jemal A. Cancer statistics 2017. CA Cancer J Clin. 2017;67(1):7–30. PMID: 17237035. doi:10.3322/caac.21387
2. Ben-Eliyahu S. The price of anticancer intervention. Does surgery promote metastasis? Lancet Oncol. 2002;3(9):578–579. PMID: 12233735.
3. Tylman M, Sarbinowski R, Bengtson JP, et al. Inflammatory response in patients undergoing colorectal cancer surgery: the effect of two different anesthetic techniques. Minerva Anestesiol. 2011;77(3):275–282. PMID: 21150855.
4. Peng K, Liu HY, Wu SR, et al. Does propofol anaesthesia lead to less postoperative pain compared with inhalational anaesthesia?: a systematic review and meta-analysis. Anesth Analg. 2016;123(4):846–858. PMID: 27636574. doi:10.1213/ANE.0000000000001504
5. Yan T, Zhang GH, Wang BN, et al. Effects of propofol/remifentanil-based total intravenous anaesthesia versus sevoflurane-based inhalational anaesthesia on the release of VEGF-C and TGF-β and prognosis after breast cancer surgery: a prospective, randomized and controlled study. BMC Anesthesiol. 2018;18(1):131. PMID: 27636574. doi:10.1186/s12871-018-0588-3
6. Yan T, Zhang GH, Cheng YZ, et al. Effects of anesthetic technique and surgery on myeloid-derived suppressor cells and prognosis in women who underwent breast cancer surgery: a prospective study. Cancer Manag Res. 2019;11:5513–5522. PMID: 31417304. doi:10.2147/CMAR.S183519
7. Shirakami G, Teratani Y, Fukuda K. Nocturnal episodic hypoxemia after ambulatory breast cancer surgery: comparison of sevoflurane and propofol-fentanyl anaesthesia. J Anesth. 2006;20(2):78–85. PMID: 16633762. doi:10.1007/s00540-005-0371-8
8. Li ZH, Liu D, He ZJ, et al. Influance of dexamethasone on the incidence of postoperative anusea and vomiting in breast cancer patients with neoadjuvant chemotherapy. J Peking Univ. 2015;47(4):685–689. PMID: 26284410.
9. Wu CL, Raja SN. Treatment of acute postoperative pain. Lancet. 2011;377(9784):2215–2225. PMID: 21704871. doi:10.1016/S0140-6736(11)60245-6
10. Yardeni IZ, Beilin B, Mayburd E, et al. Relationship between fentanyl dosage and immune function in the postoperative period. J Opioid Manag. 2008;4(1):27–33. PMID: 18444445. doi:10.5055/jom.2008.0005
11. Juneja R. Opioids and cancer recurrence. Curr Opin Support Palliat Care. 2014;8(2):91–101. PMID: 24759319. doi:10.1097/SPC.0000000000000056
12. Ecimovic P, McHugh B, Murray D, et al. Effects of sevoflurane on breast cancer cell function in vitro. Anticancer Res. 2013;33(10):4255–4260. PMID: 24122989.
13. Ecimovic P, Murray D, Doran P, et al. Propofol and bupivacaine in breast cancer cell function in vitro-role of the NET1 gene. Anticancer Res. 2014;34(3):1321–1331. PMID: 24596379.
14. Kushida A, Inada T, Shingu K. Enhancement of antitumor immunity after propofol treatment in mice. Immunopharmacol Immunotoxical. 2007;29(3–4):477–486. PMID: 18075859. doi:10.1080/08923970701675085
15. Kim MH, Kim DW, Kim JH, et al. Does the type of anaesthesia really affect the recurrence-free survival after breast cancer surgery? Oncotarget. 2017;8(52):90477–90487. PMID: 29163846. doi:10.18632/oncotarget.21014
16. Yoo S, Lee HB, Han W, et al. Total intravenous anesthesia versus inhalation anesthesia for breast cancer surgery. Anesthesiology. 2019;130(1):31–40. PMID: 30376457. doi:10.1097/ALN.0000000000002491
17. Hozo SP, Djulbegovic B, Hozo I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol. 2005;5(1):13. PMID: 15840177. doi:10.1186/1471-2288-5-13
18. Shin SW, Cho AR, Lee HJ, et al. Maintenance anaesthetics during remifentanil-based anaesthesia might affect postoperative pain control after breast cancer surgery. Br J Anaesth. 2010;105(5):661–667. PMID: 20876698. doi:10.1093/bja/aeq257
19. Oh CS, Lee J, Yoon TG, et al. Effect of equipotent doses of propofol versus sevoflurane anaesthesia on regulatory T Cells after breast cancer surgery. Anesthesiology. 2018;129(5):921–931. PMID: 30074934. doi:10.1097/ALN.0000000000002382
20. Cho JS, Lee MH, Kim SI, et al. The effects of perioperative anaesthesia and analgesia on immune function in patients undergoing breast cancer resection: a prospective randomized study. Int J Med Sci. 2017;14(10):970–976. PMID: 28924368. doi:10.7150/ijms.20064
21. Woo JH, Baik HJ, Kim CH, et al. Effect of propofol and desflurane on immune cell populations in breast cancer patients: a randomized trial. J Korean Med Sci. 2015;30(10):1503–1508. PMID: 26425050. doi:10.3346/jkms.2015.30.10.1503
22. Oddby-Muhrbeck E, Jakobsson J, Andersson L, et al. Postoperative nausea and vomiting. A comparison between intravenous and inhalation anaesthesia in breast surgery. Acta Anaesthesiol Scand. 1994;38(1):52–56. PMID: 8140874. doi:10.1111/j.1399-6576.1994.tb03837.x
23. Chen HP, Hsu YH, Hua KC, et al. Comparison of sevoflurane versus propofol under auditory evoked potential monitoring in female patients undergoing breast surgery. Biomed J. 2013;36(3):125–131. PMID: 23806882. doi:10.4103/2319-4170.113228
24. Wang ZY, Wang Y, Han F, et al. Anesthetic effects of propofol-remifentanil compared with sevoflurane-nitrous oxide for modified radical mastectomy of breast cancer. J Harbin Med Univ. 2010;44(6):600–604.
25. Zhu JH. Compare the incidence of nausea and vomiting after modified radical mastectomy under three different anaesthesia methods. Guide China Med. 2013;11(11):206–207.
26. Hou XY. Incidence comparison of post-operative nausea and vomiting of modified radical mastectomy for breast cancer under three methods of anaesthesia. Chin Med Pharm. 2013;3(6):101–102.
27. Yang DQ, Li GJ, Shen ZY. Effect of different anaesthesia methods on nausea and vomiting after modified radical mastectomy. J Clin Anesthesiol. 2012;28(1):54–55.
28. Yi XF, Ji FH. Effect of different anaesthesia methods on patients with modified radical mastectomy. Chin J Gerontol. 2013;33:2548–2549. doi:10.3969/j.issn.1005-9202.2013.11.031
29. Yang PC. Effect analysis of patients PONV symptoms of modified radical mastectomy under different anaesthesia methods. Heilongjiang Med J. 2015;39(9):998–1001. doi:10.3969/j.issn.1004-5775.2015.09.003
30. Cui Z, Zhang HJ, Zhang FK, et al. Influence of desflurane or propofol anaesthesia on postoperative cognitive recovery in breast cancer patients. Clin Med J. 2017;15(10):50–52. doi:10.3969/j.issn.1672-3384.2017.10.012
31. Hu JY, Deng JH. Effects of inhalation maintenance anaesthesia and intravenous general anaesthesia on perioperative immune function and stress level on breast cancer patients. Mod Pract Med. 2017;29(10):1295–1297. doi:10.3969/j.issn.1671-0810.2017.10.019
32. Wei PH. The influence of different general anaesthesia technique on immune function in patients undergoing radical mammotomy. J Taishan Med Coll. 2011;32(9):664–666.
33. Lim JA, Oh CS, Yoon TG, et al. The effect of propofol and sevoflurane on cancer cell, natural killer cell, and cytotoxic T lymphocyte function in patients undergoing breast cancer surgery: an in vitro analysis. BMC Cancer. 2018;18(1):159. doi:10.1186/s12885-018-4064-8.
34. Freye E, Bruckner J, Latasch L. No difference in electroencephalographic power spectra or sensory-evoked potentials in patients anaesthetized with desflurane or sevoflurane. Eur J Anaesthesiol. 2004;21(5):373–378. PMID: 15141795. doi:10.1017/s0265021504005046
35. O’Connor TC, Abram SE. Inhibition of nociception-induced spinal sensitization by anesthetic agents. Anesthesiology. 1995;82(1):259–266. PMID: 7832309. doi:10.1097/00000542-199501000-00031
36. Antognini JF, Wang XW, Piercy M, et al. Propofol directly depresses lumbar dorsal horn neuronal responses to noxious stimulation in goats. Can J Anaesth. 2000;47(3):273–279. PMID: 10730741. doi:10.1007/BF03018926
37. Reihner E, Grunditz R, Giesecke K, et al. Postoperative nausea and vomiting after breast surgery: efficacy of propylactic ondansetron and droperidol in a randomized placebo-conrolled study. Eur J Anaesthesiol. 2000;17(3):197–203. PMID: 10758471. doi:10.1046/j.1365-2346.2000.00627.x
38. Ostman PL, Faure E, Glosten B, et al. Is the antiemitic effect of the emulsion of propofol due to the lipid emulsion? Anesth Analg. 1990;71(5):536–540. PMID: 2221415.
39. Coussens LM, Werb Z. Inflammation and cancer. Nature. 2002;420(6917):860–867. PMID: 12490959. doi:10.1038/nature01322
40. Zergoun AA, Zebboudj A, Sellam SL, et al. IL-6/NOS2 inflammatory signals regulate MMP-9 and MMP-2 activity and disease outcome in nasopharyngeal carcinoma patients. Tumour Biol. 2016;37(3):3505–3514. PMID: 26453114. doi:10.1007/s13277-015-4186-4
41. Zhou WJ, Wang S, Xia SG, et al. Effect of IL-6 silencing on invasion and migration of breast cancer cells. Chin J Pathophysiol. 2019;35:81–86.
42. Chester C, Fritsch K, Kohrt HE. Natural killer cell immunomodulation: targeting activating, inhibitory, and co-stimulatory receptor signaling for cancer immunotherapy. Front Immunol. 2015;6:601. PMID: 26697006. doi:10.3389/fimmu.2015.00601
43. Konjevic G, Spuzic I. Stage dependence of NK cell activity and its modulation by interleukin 2 in patients with breast cancer. Neoplasma. 1993;40(2):81–85. PMID: 8350959.
44. Kim R. Effects of surgery and anesthetic choice on immunosuppression and cancer recurrence. J Transl Med. 2018;16(1):8. PMID: 29347949. doi:10.1186/s12967-018-1389-7
45. Stollings LM, Jia LJ, Tang P, et al. Immune modulation by volatile anaesthetics. Anesthesiology. 2016;125(2):399–411. PMID: 27286478. doi:10.1097/ALN.0000000000001195
46. Chen J, Deng Q, Pan Y, et al. Prognostic value of neutrophil-to-lymphocyte ratio in breast cancer. FEBS Open Bio. 2015;5(1):502–507. PMID: 26137435. doi:10.1016/j.fob.2015.05.003
47. Sessler DI, Pei L, Huang Y, et al. Recurrence of breast cancer after regional or general anaesthesia: a randomised controlled trial. Lancet. 2019;394(10211):1807–1815. PMID: 31645288. doi:10.1016/S0140-6736(19)32313-X.
48. Lee JH, Kang SH, Kim Y, et al. Effects of propofol-based total intravenous anesthesia on recurrence and overall survival in patients after modified radical mastectomy: a retrospective study. Korean J Anesthesiol. 2016;69(2):126–132. PMID: 27066202; PMCID: PMC4823406. doi:10.4097/kjae.2016.69.2.126.
49. Horazeck C, Lyes M, Fuller M, et al. Paravertebral blocks and propofol sedation reduce recurrence and 5-year mortality in patients undergoing mastectomy for breast cancer - A retrospective cohort study. Soc Sci Electronic Publishing. 2019;18:16–46. doi:10.2139/ssrn.3337882
50. Behrooz A. Pharmacogenetics and anaesthetic drugs: implications for perioperative practice. Ann Med Surg (Lond). 2015;4(4):470–474. PMID: 26779337; PMCID: PMC4685230. doi:10.1016/j.amsu.2015.11.001.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.