")
Back to Journals » International Journal of General Medicine » Volume 16
Comparison of Immunological and Virological Recovery with Rapid, Early, and Late Start of Antiretroviral Treatment in Naive Plwh: Real-World Data
Authors Sarıgül Yıldırım F , Candevir A , Akhan S, Kaya S, Çabalak M, Ersöz G, İnan D, Ceren N , Karaoğlan İ, Damar Çakırca T, Özer Balin Ş, Alkan S, Kandemir Ö, Üser Ü, Karabay O, Çelen MK
Received 19 October 2022
Accepted for publication 1 April 2023
Published 17 May 2023 Volume 2023:16 Pages 1867—1877
DOI https://doi.org/10.2147/IJGM.S393370
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Figen Sarıgül Yıldırım,1 Aslıhan Candevir,2 Sıla Akhan,3 Selçuk Kaya,4 Mehmet Çabalak,5 Gülden Ersöz,6 Dilara İnan,7 Nurgül Ceren,8 İlkay Karaoğlan,9 Tuba Damar Çakırca,10 Şafak Özer Balin,11 Sevil Alkan,12 Özlem Kandemir,6 Ülkü Üser,13 Oğuz Karabay,14 Mustafa Kemal Çelen15
1Antalya Life Hospital, Department of Infectious Diseases and Clinical Microbiology, Antalya, Turkey; 2Cukurova University, Medical Faculty, Department of Infectious Diseases and Clinical Microbiology, Adana, Turkey; 3Kocaeli Üniversity, Medical Faculty, Department of Infectious Diseases and Clinical Microbiology, Kocaeli, Turkey; 4Karadeniz Teknik University, Medical Faculty, Department of Infectious Diseases and Clinical Microbiology, Trabzon, Turkey; 5Mustafa Kemal University Medical Faculty, Department of Infectious Diseases and Clinical Microbiology, Hatay, Turkey; 6Mersin University, Medical Faculty, Department of Infectious Diseases and Clinical Microbiology, Mersin, Turkey; 7Akdeniz University Medical Faculty, Department of Infectious Diseases and Clinical Microbiology, Antalya, Turkey; 8Health Science University, Haydarpaşa Numune Education and Research Hospital, Department of Infectious Diseases and Clinical Microbiology, İstanbul, Turkey; 9Gaziantep University, Medical Faculty, Department of Infectious Diseases and Clinical Microbiology, Gaziantep, Turkey; 10Health Science University, Şanlıurfa Numune Education and Research Hospital, Department of Infectious Diseases and Clinical Microbiology, Şanlıurfa, Turkey; 11Fırat University Medical Faculty, Department of Infectious Diseases and Clinical Microbiology, Elazığ, Turkey; 12Çanakkale 18 Mart University, Medical Faculty, Department of Infectious Diseases and Clinical Microbiology, Çanakkale, Turkey; 13Health Science University, Antalya Education and Research Hospital, Department of Infectious Diseases and Clinical Microbiology, Antalya, Turkey; 14Sakarya University Medical Faculty, Department of Infectious Diseases and Clinical Microbiology, Hatay, Turkey; 15Dicle University, Medical Faculty, Department of Infectious Diseases and Clinical Microbiology, Diyarbakır, Turkey
Correspondence: Figen Sarıgül Yıldırım, Antalya Life Hospital, Department of Infectious Diseases and Clinical Microbiology, Antalya, Turkey, Tel +90 532 473 44 46, Email [email protected]
Background: Rapid initiation of antiretroviral therapy (ART) reduces the transmission of HIV infection in the community. This study aimed to determine whether rapid ART initiation is effective compared to standard ART treatment in our country.
Methods: Patients were grouped based on time to treatment initiation. HIV RNA levels, CD+4 T cell count, CD4/CD8 ratio, and ART regimens were recorded at baseline and follow-up visits for 12 months.
Results: There were 368-ART naive adults (treatment initiated at the time of HIV diagnosis; 143 on the first day, 48 on the second-seventh day, and 177 after the seventh day). Although virological suppression rates at 12th months were higher in all groups, over 90% on average, there were no statistically significant differences in HIV-1 RNA suppression rates, CD+4 T cell count, and CD4/CD8 ratio normalization in the studied months but in multivariate logistic regression analysis; showed a significant correlation between both virological and immunological response and those with CD4+ T < 350 cells/mL at 12th month in total patients.
Conclusion: Our findings support the broader application of recommendations for rapid ART initiation in HIV patients.
Keywords: HIV, ART, antiretroviral, rapid start
Introduction
With the introduction of effective combination antiretroviral therapy (ART) for people living with HIV (PLWH) in 1996,1 their life expectancy has now reached parity with that of individuals not infected with HIV, provided that they are diagnosed and treated upon infection.2,3 Clinical guidelines for HIV treatment were updated after 2015 to recommend initiating ART in PLWH regardless of CD4+T cell count.4–6 These updates were based on randomized controlled trials and observational studies in which ART was initiated at higher CD4+T cell counts (≥500 cells/mm3).7,8 This approach has reduced the risk of AIDS and non-AIDS events and the mortality rate for PLWH.
Subsequent research has shown that initiating therapy on the first day or within a week of diagnosis results in the following outcomes: rapid and effective viral suppression, early immune system recovery, increased treatment adherence and persistence, improvement in quality and length of life, reduction in the development of HIV-related and noncommunicable diseases, prevention of complications, and, most importantly, reduction in the transmission of HIV in the community.9–13
While no standard for rapid ART has yet been established, it generally involves starting treatment within the first 24 hours of diagnosis.5 However, the World Health Organization (WHO) defines it as starting ART within seven days of a diagnosis. In other research, it has been defined as starting ART within 14 days of a diagnosis.5,9,11
Until the initiation of ART, an individual diagnosed with HIV needs to make many hospital visits to arrange for counseling, laboratory tests, and other procedures, which can burden patients and delay the start of therapy.4 This is most common in low-income countries, especially Sub-Saharan Africa.9,11 In 2017, WHO advised that all persons living with HIV start rapid ART after a confirmed HIV diagnosis and clinical evaluation, to increase treatment adherence and follow-up by reducing lost to follow-up rates (LTFU).5,14 Studies on rapid ART initiation were also performed in the United States (US). The time to reach viral suppression was found to be shorter, with higher viral suppression rates and lower LTFU.15–18 This strategy has been recommended by several guidelines, including those issued by the US Department of Health and Human Services (DHHS), the International AIDS Society (IAS), and the European AIDS Clinical Society (EACS).19–21
HIV infections are officially reported in Turkey, and the number of cases is increasing every year. With the cumulative decrease observed in the last year due to the COVID-19 pandemic, a total of 25,745 adults were reported to be infected with HIV-1 as of the end of 2020, and the rate of patients receiving ART was 79%.22,23 According to the Turkish Ministry of Health, the primary strategy to minimize HIV transmission in 2019 could be achieved via early detection, viral suppression, access to care, and retention in care.24
When a new case of HIV infection is diagnosed in Turkey, the average time to start ART after the initial visit is not exactly known. The first step is to select and prescribe an appropriate ART regimen. After the diagnosis, certain test results (such as CD4+T cell count, HIV viral load, genotypic viral resistance test results) are expected and counseling is provided to the patients if necessary. A team of health counselors, if available, also prepares the patient for ART. This process usually takes two to four weeks.
The rapid treatment initiation approach started to be used in our country after the studies were conducted when guidelines updated their recommendations to include rapid treatment. So far, there has been no published study on the rapid start of ART. This study aimed to determine whether rapid ART initiation is effective compared to standard ART initiation in Turkey.
METHODOLOGY Study Design
This study was a retrospective, multicenter comparative case series study conducted in 15 centers across Turkey. All eligible HIV-1 positive, treatment-naive patients were included between February 2, 2018, and December 28, 2020. A case report form was developed to collect age and gender data, HIV RNA levels, CD+4 and CD+8 T cell counts, and the ART regimens of the newly diagnosed patients. In total, 368 patients were included in the study, 143 in the rapid ART start group (RS) (38.8%), 48 in the early ART start group (ES) (13.2%), and 177 in the late ART start group (LS) (48%). The RS group was defined as those who initiated ART within the first 24 hours after admission to the clinic. The ES group was defined as those who started ART between the second day and the seventh day after arriving at the clinic. Those who began ART on Day eight and beyond were defined as the LS group.
The date of HIV diagnosis was determined as the first confirmed positive HIV antibody test, detectable HIV viral load, or the day the doctor made the diagnosis on the day of the first visit to the clinic. The time to start ART after diagnosis was defined as the time to treatment initiation.
The data were collected on-site by the treating physicians. The centers included in this study cover the Mediterranean, Marmara, Eastern Anatolia, Central Anatolia, Southeastern Anatolia, and Black Sea regions.
Patient records were analyzed retrospectively. Plasma HIV-1 RNA levels, CD4+ and CD8+ T cell counts were recorded at baseline and follow-up visits at Months 1, 3, 6, 9, and 12. At the same visits, the CD4/CD8 ratio was calculated by dividing the number of CD4+ T cells obtained by the number of CD8+ T cells.
For the demographic data of the three groups, age, sex, baseline HIV-1 RNA, CD4+ T cell count, CD4/CD8 ratio, and regimens used in ART were reported. ART regimens included dolutegravir (DTG) + tenofovir/emtricitabine (TDF/FTC), elvitegravir/cobicistat/tenofovir alafenamide/emtricitabine (EVG/COB/TAF/FTC), bictegravir/tenofovir alafenamide/emtricitabine (BIC/TAF/FTC), dolutegravir/abacavir/lamivudine (DTG/ABC/3TC). Others were lopinavir/ritonavir + TDF/FTC, darunavir/ritonavir + TDF/FTC, efavirenz + TDF/FTC and DTG+3TC.
Laboratory Analysis
Plasma HIV-1 RNA detection and quantification levels were measured using real time- PCR (Abbott TagMan 2000, Illinois-Des Plaines USA) (lower limit as quantification, 10 IU/mL). CD4 and CD8+ T cell counts were analyzed with BD Simultest™ CD4/CD8 (Becton, Dickinson and Company BD Biosciences 2350 Qume Drive San Jose, CA 95131 USA).
Study Population
Patients older than 18 years of age, diagnosed with HIV, and receiving ART for at least 12 months were included in this study.
Study Endpoints
We analyzed the virological suppression (HIV-1 RNA ≤200 copies/mL) and immunological response (CD4+ T cell count and CD4/CD8 ratio) at Months 1, 3, 6, 9, and 12 for the three treatment groups.
Statistical Analysis
Statistical analysis was made using IBM SPSS Statistics for Windows, version 22.0 (IBM Corp., Armonk, NY). Descriptive statistics were used to summarize baseline characteristics. Data were expressed as median (minimum-maximum) and percentage (%), and the continuous variables and categorical ones were compared with Mann Whitney U (or Student’s t-test) where appropriate. A p value of <0.05 was set as the level of significance.
Age, gender, ART start time, initial HIVRNA level (Log10), initial CD+4 T cell levels identified as possible significant variables or confounding factors on virologic response (HIVRNA<200 copies/mL) and immunologic response (raise in CD4+T cell more than 150 cells/mL) at 12th month. Therefore, in this study, following the Hosmer–Lemeshow suggestion, variables with p < 0.25 in univariable analyses were included in the multivariable analysis.25
Results
Between February 2, 2018, and December 28, 2020; a total of 368 patients were investigated from the 15 centers’ records, 143 in the rapid ART start group (RS) (38.8%), 48 in the early ART start group (ES) (13.2%), and 177 in the late ART start group (LS) (48%). Baseline (the time-point of HIV diagnosis) demographics and laboratory characteristics of the patients were comparable between arms. The median age of patients in the RS, ES, and LS groups were 34, 35, 35 (p=0.990), and the percentages of female patients was %12.6, %14.6, %13.0 (p=0.938) respectively. The median baseline CD4+ T cell count: 403, 413, 438 cells/mm3 (p=0.761), median baseline CD4/CD8 ratio: 0.44, 038, 0.40 (p=0.522), median baseline HIV-1 RNA log10: 4.9, 6.0, 5.0 copies/mL (p=0.540) respectively. The three groups were balanced for all parameters except types of ART. The baseline characteristics of patients are summarized in Table 1.
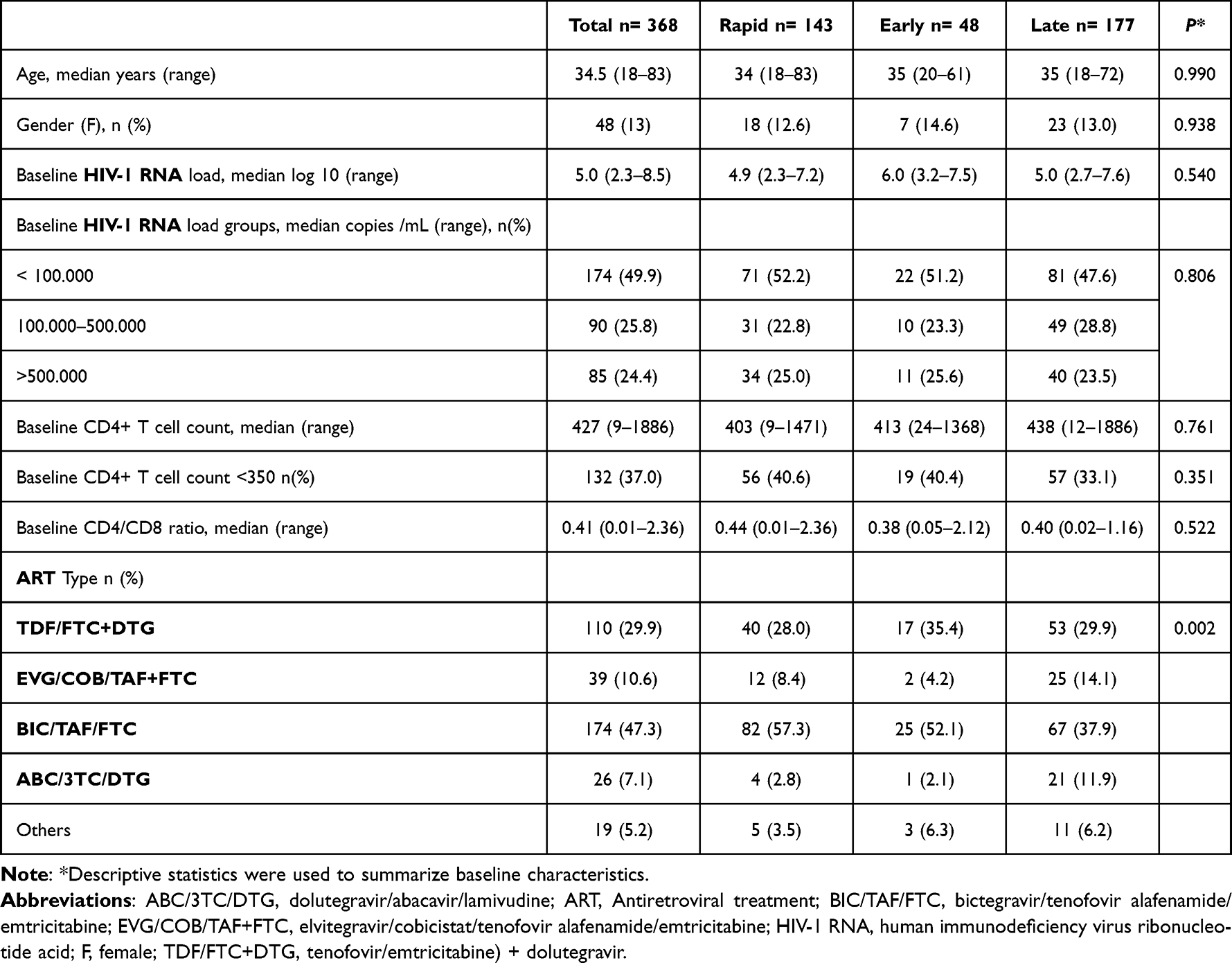 |
Table 1 Baseline Demographic and Laboratory Characteristics of the Study Patients |
Virological Response
There were no statistically significant differences in HIV-1 RNA suppression rates (<200 copies/mL) between the groups at Months 1, 3, 6, 9, and 12 (p>0.05) (Figure 1).
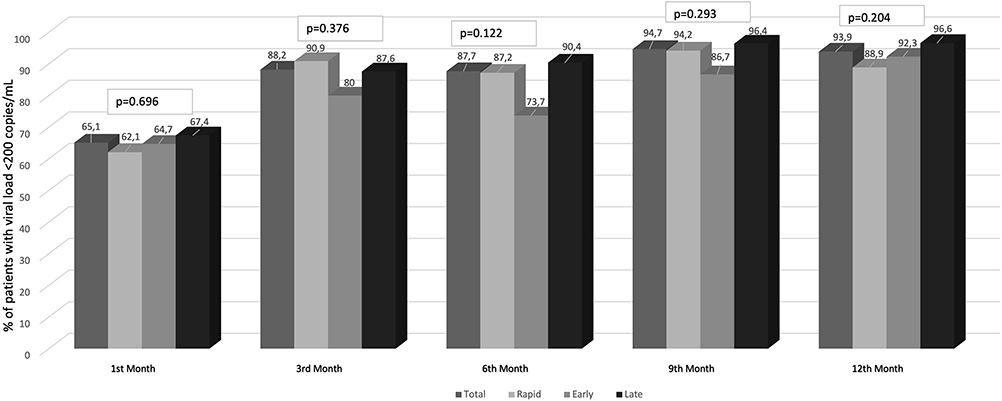 |
Figure 1 Proportional (%) HIV RNA<200 copies/mL of the patients (virological response). |
Changes in CD4+ T Cell Count and CD4/CD8 Ratio Normalization
No statistically significant difference was found in CD4+ T cell numbers and CD4/CD8 ratio normalization in the follow-up. Although there was no statistically significant difference between the groups, CD4/CD8 ratio was found to be higher in the RS group than others at Months 9 and 12. On the other hand, the LS group had higher CD4+ T cell counts, particularly in the last three months of the study (Figures 2 and 3).
 |
Figure 2 CD4+ T cells levels in patients. |
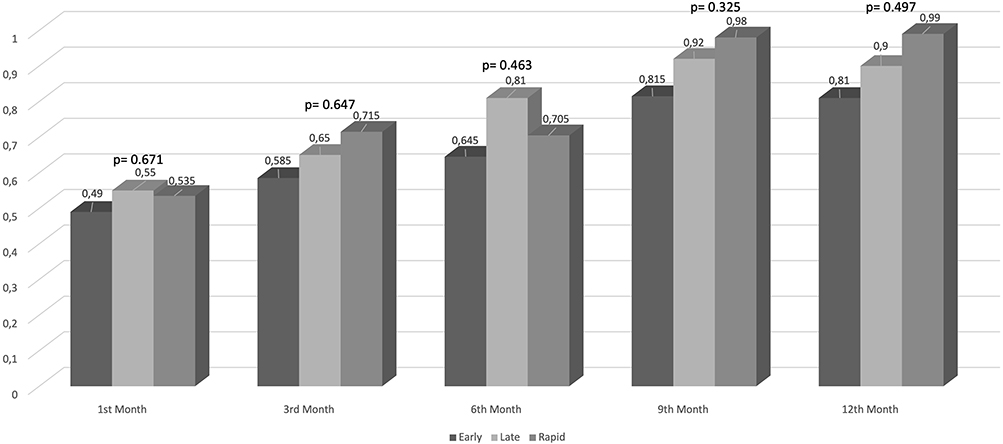 |
Figure 3 The ratio of CD4/CD8 ratio between the groups. |
Factors Associated with HIV Viral Load Suppression (< 200 Copies/mL); and CD4+ T Cell Count Increase (>150 Cells/mL) at 12th Month in Total Patients
Univariate analysis showed a significant association between virological response and those with late onset of ART, HIV RNA >5 log 10, CD4+ T <350 cells/mL, and between immunological response and CD4+ T <350 cells/mL (Table 2). In multivariate logistic regression analysis; showed a significant correlation between both virological and immunological response and those with CD4+ T <350 cells/mL (Table 2).
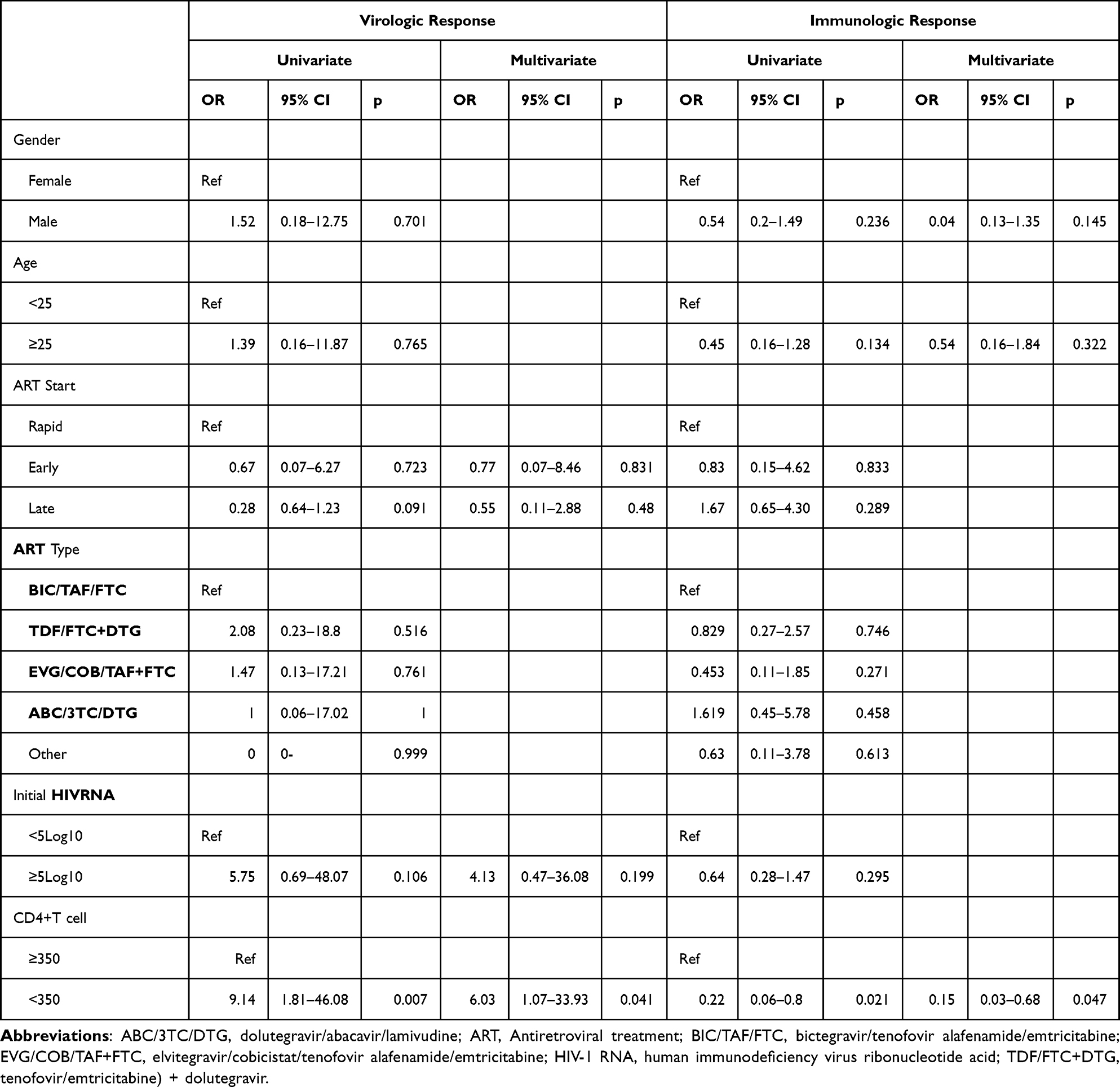 |
Table 2 Factors Associated with HIV Viral Load Suppression (< 200 Copies/mL); and CD4+ T Cell Count Increase (>150 Cells/mL) at 12th Month |
Discussion
Current studies on the rapid start of ART in the real-world setting are limited. This study aimed to compare the treatment efficacy of RS, ES, LS of ART in the real world in naive PLWH at Months 1, 3, 6, and 12 in our country. We used the CD4+ T cell count, CD4/CD8 ratio normalization, and HIV RNA level to assess immunological and virological responses.
In our study, in newly diagnosed HIV-1 infected individuals between 2018 and 2020, the median time from HIV diagnosis to the start of ART was 7 (0–452) days (data not shown). There had been no data about the time of ART initiation in our country. This is intended to be the first of such data. Before 2018, the time to treatment initiation may have been longer than seven days as the clinics in our country implemented rapid start after 2018, and RS was applied in many outpatient clinics only after the emergence of the Covid-19 pandemic (after March 2020). Early treatment for PLWH began to be provided in most countries after 2015 when WHO implemented the “Treat All” policy.26–29 This was best demonstrated in a French cohort, where the median delay between HIV diagnosis and start of ART decreased from 9.07 months in 2007 to 0.77 months in 2017.29
In 2017, there was an increase in the rates of rapid treatment start, with the WHO’s recommendation to start treatment on the day of diagnosis or within the first seven days.16,30 As mentioned earlier, there is no standard definition of early ART initiation. The average time of ART initiation may vary depending on region, city, and country. For example, in studies conducted in London and Taiwan, rapid ART was two and seven days, respectively. In our study, about 62% of patients started ART within seven days of HIV diagnosis. This rate was relatively high compared to other studies.9,13,17,18 This might be because hospital visits had to be limited during the Covid-19 pandemic, and the patients were treated early after diagnosis.
The first clinical trials of rapid ART were conducted in developing countries such as South Africa, yielding high virological responses. A first-visit ART initiation trial in South Africa resulted in a higher viral suppression rate at Month 10 in the rapid ART group compared to other participants (64% vs 51%).10 On the other hand, in most studies, 29–50% of the patients did not achieve viral suppression 1012 months after rapid ART initiation.10–14 As a result of these studies, rapid ART started to be investigated in developed countries.31,32 In a San Francisco city clinic, serving patients with high rates of mental illness, substance abuse, and homelessness, 90% of patients achieved viral suppression in an average of 1.09 years, with rapid ART within the RAPID program.18 In the same study, the rapid ART group had a higher rate of virological suppression at the final viral load measurement (94%) than the late ART group (81%). In another study from the US, the rapid ART approach was found to reduce time to first provider appointment, time to ART start, and time to viral suppression, but not the proportion of patients who achieved viral suppression.33 In our study, we did not find a significant difference in virological suppression rates between the groups. However, we had high rates of virological suppression in all groups. Yet, the rate of viral suppression at Month 12 in the RS group (88.9%) was lower than in other groups (92.3% in the ES and 96.6% in the LS group). We plan to follow these patients further in the future. Virological suppression rates close to 90% in 12 months are quite high and sufficient for improvement. In our study, we found that the virological response was better in PWLH (CD4+ T < 350 cells/mL) presenting with late presentation. To further shorten the time to viral suppression and increase virological suppression rates to end the HIV epidemic, innovative approaches that reduce barriers to testing, care, and adherence are required.34
A multicenter study conducted in our country found that 79% of newly diagnosed cases were retained in care. Among these cases, viral suppression was achieved in 73% after six months of ART.23 These ratios are higher than most European countries.34–36 In our study, viral suppression rates were also found to be higher. Rapid ART initiation is linked to faster viral suppression in PLWH, resulting in a significantly reduced risk of transmission. Although in our study the rapid initiation of ART did not affect the viral suppression rates, it should be noted that faster viral suppression would mean fewer cases of transmission: so early “ART equals early viral suppression equals lower transmission.”
The rapid increase in CD4+ T cell count shortens the duration of prophylaxis against opportunistic infections and reduces AIDS-associated morbidity and mortality.19 However, late presenters treated with INSTIs may carry a greater risk of developing immune reconstitution inflammatory syndrome (IRIS) due to a rapid increase in CD4+ T cell count. It is known that the number of CD4+ T cells increases annually by 100–150 cells/mm3 on average.37 Therefore, in our univariate and multivariate analysis, we evaluated the immunological response as an increase in CD4+ T cell count of more than 150 cells/mL at 12 months. In our study, the median CD4+ T cell count was 427 cells/mm3 and the increase observed was higher than 200 cells/mm3 at Month 12. After INSTI use, the one-year increase in CD+4 T-cell should be modified by 200 cells/mm3 or more per year. We found a similar result in our other study comparing INSTIs two years ago.38 We found no difference in immunological response between the groups and that the rapid ART initiation did not affect the immunological response but we found that CD4+ T cell count increase (>150 cells/mL) at 12th month was better in PWLH (CD4+ T < 350 cells/mL) presenting with late presentation in total patients.
Despite ART, immune activation and inflammation persist in PWLH, leading to future comorbidities.37 Starting treatment early leads to reduced inflammation,39 and one of the best and established biomarkers of inflammation is the normalization of the CD4/CD8 ratio.40 The CD4/CD8 ratio is indicative of immune dysfunction and a prognostic marker for non-AIDS mortality, and it also reflects the size of the viral reservoir in PLWH.37 This rate is higher than 1 in immunocompetent individuals.41 Although we could not find a significant difference between the groups in terms of normalization of the CD4/CD8 ratio in our study, it was higher in the RS group in the last two months of the study. Several studies have shown that early initiation of ART is associated with a shorter time to normalization of the CD4/CD8 ratio.42,43 In addition, there was no normalization in the CD4/CD8 ratio in our study groups after 12 months. Generally, the CD4/CD8 ratio normalization may not be achieved after three years, even in patients with CD4+ T cell >350 mm3 at the start of antiretroviral therapy.39,44,45
The increase in CD4+ T cell counts in terms of immunological response is similar to the rise in CD4/CD8 ratios in chronic inflammation, showing us that starting ART early did not deteriorate either parameter. Rapid ART may be a method that can be used to increase the virological suppression in countries where the population of PLWH is high. It may be used to reduce the time to virological suppression in countries like Turkey with increased access to treatment and virological suppression.
Guidelines recommend ART regimens with a high barrier to resistance for rapid ART initiation, such as BIC/FTC/TAF, ritonavir-boosted DRV + (FTC or 3TC)/(TAF or TDF) or DTG + (FTC or 3TC)/(TAF or TDF).19–21 Early virological suppression is achieved more rapidly with INSTIs than with protease inhibitors.46,47 In our study, 81% of the treatment regimens were INSTI-based. In the San Francisco study, 90% of rapid ART regimens were INSTI-based, and 10% were DRV/r + FTC/TDF.16 In our study, the most commonly used regimen in the RS and ES groups was BIC/FTC/TAF, with rates of 57.3% and 52.1%, respectively. DTG+TDF/FTC and BIC/FTC/TAF were the most commonly used regimens in the LS group (29.9% and 37.9% respectively). One of the reasons for selecting BIC/FTC/TAF for Rapid and Early ART groups in Turkey is believed to be that physicians preferred a regimen with low side effects due to hospital visit restrictions during the COVID-19 pandemic, as well as the ease of use of the single tablet.47 Our number of patients with a Rapid ART before the COVID-19 pandemic was 13% after the pandemia, this rate increased to 45% (data is not shown). Real-world data of BIC/FTC/TAF in rapid start were also presented at the IDWeek 2020 by Zuppeli et al. It had been shown that patients had shorter time to virological suppression and higher virological suppression rates.48
A national cohort study conducted in a country with unlimited access to rapid ART, such as France, found that starting ART sooner did not benefit every patient. The viral and immunological evaluations were not performed in this study, suggesting that it is challenging to keep PLWH in care.49 However, in many studies, it had been determined that the rate of retention in care was higher with rapid and early initiation of ART.9,50
There are certain limitations to this study. The rates of retention in care could not be evaluated. Our study was retrospective and coincided with the time of the COVID-19 pandemic during the planning and data collection phases. Most patients could not attend the follow-up visits, therefore, the data could not be included in the analysis as it would not be considered retention in follow-up. The patients included in this study were also followed up during that period. The main limitation of the study is that there is no information concerning the time since HIV infection. It is unclear how long the patients have been infected until they are diagnosed or they start the treatment. However, the multicenter design as well as the relatively high number of patients included are the strengths of this study.
Conclusion
To our knowledge, this is the first national-based study of rapid ART initiation in newly diagnosed PLWH. We were able to demonstrate that in ART-naive PLWH, it is feasible to start ART on the same day or within the first seven days of the initial clinical visit, which results in faster viral load suppression, and higher virological suppression rates. Our findings support the feasibility of the guidelines recommended rapid ART initiation.
Data Sharing Statement
The authors hereby confirm that the data supporting the results and findings of this study are available within the article.
Ethics Approval
Ethics committee approval was obtained at Health Sciences University Antalya Research and Training.
Hospital in Turkey in accordance with the 2008 Declaration of Helsinki (Registration No: 06.05.2021 6/11). The requirement for written informed consent was waived because of the retrospective design of this study. Demographic information and laboratory analysis were collected from medical records. We confirmed that all the data was anonymized and maintained with confidentiality.
Consent for Publication
Individual consent was not mandatory as this was a record-based study. No individual data was captured.
Human and Animal Rights
No animals were used in this research. All human research procedures were in accordance with the articles set forth in the Declaration of Helsinki of 1975, as revised in 2013 (http://ethics.iit.edu/ecodes/node/3931).
Standard of Reporting
The study conforms to the STROBE guidelines.
Acknowledgment
We would like to thank İlker Kürkçü for statistical analysis support.
Disclosure
The authors declare no conflicts of interest, financial or otherwise.
References
1. Yoshimura K. Current status of HIV/AIDS in the ART era. J Infect Chemother. 2017;23(1):12–16. doi:10.1016/j.jiac.2016.10.002
2. Nakagawa F, Lodwick RK, Smith CJ, et al. Projected life expectancy of people with HIV, according to the timing of diagnosis. AIDS. 2012;26(3):335–343. doi:10.1097/QAD.0b013e32834dcec9
3. Walker BD, Hirsch MS. Antiretroviral therapy in early HIV infection. N Engl J Med. 2013;368(3):279–281. doi:10.1056/NEJMe1213734
4. Panel on antiretroviral guidelines for adults and adolescents; 2017. Available from: https://aidsinfo.nih.gov/contentfiles/lvguidelines/adultandadolescentgl.pdf.
5. World Health Organization. 2016, Diagnosis, treatment and care for key populations; 2016. Available from: http://apps.who.int/iris/bitstream/10665/246200/1/9789241511124-eng.pdf?ua=13.
6. EACS guidelines, version 9.0; 2017. Available from: http://www.eacsociety.org/guidelines/eacsguidelines/eacs-guidelines.html.
7. Lundgren JD, Babiker AG, Gordin F, et al.; Insight Start Study Group. Initiation of antiretroviral therapy in early asymptomatic HIV infection. N Engl J Med. 2015;373:795–807.
8. Danel C, Moh R; Tempranoanrs Study Group. Atrial of early antiretrovirals and isoniazid preventive therapy in Africa. N Engl J Med. 2015;373(9):808–822.
9. Ford N, Migone C, Calmy A, et al. Benefits and risks of rapid initiation of antiretroviral therapy. AIDS. 2018;32(1):17–23. doi:10.1097/QAD.0000000000001671
10. Rosen S, Maskew M, Fox MP, et al. Affiliations expand initiating antiretroviral therapy for HIV at a patient’s first clinic visit: the RapIT randomized controlled trial. PLoS Med. 2016;13(5):e1002015. doi:10.1371/journal.pmed.1002015
11. Amanyir G, Semitala FC, Namusobya J, et al. Effects of a multicomponent intervention to streamline the initiation of antiretroviral therapy in Africa: a stepped-wedge cluster-randomized trial. Lancet HIV. 2016;3(11):539–548. doi:10.1016/S2352-3018(16)30090-X
12. Koenig SP, Dorvil N, Dévieux JG, et al. Same-day HIV testing with the initiation of antiretroviral therapy versus standard care for persons living with HIV: a randomized unblinded trial. PLOS Med. 2017;14(7):e100235. doi:10.1371/journal.pmed.1002357
13. Labhardt ND, Ringera I, Lejone TI, et al. Effect of offering same-day ART vs. usual health facility referral during home-based HIV testing on linkage to care and viral suppression among adults with HIV in Lesotho: the CASCADE randomized clinical trial. JAMA. 2018;319(11):1103–1112. doi:10.1001/jama.2018.1818
14. Guidelines for managing advanced HIV disease and rapid initiation of antiretroviral therapy; 2017. Geneva, Switzerland. Available from: https://apps.who.int/iris/bitstream/handle/10665/255884/9789241550062-eng.pdf?sequence=1.
15. Halperin J, Butler I, Conner K, et al. Linkage, and antiretroviral therapy within 72 hours at a federally qualified health center in New Orleans. AIDS Patient Care STDS. 2018;32(2):39–41. doi:10.1089/apc.2017.0309
16. Pilcher CD, Ospina-Norvell C, Dasgupta A, et al. The effect of same-day observed initiation of antiretroviral therapy on HIV viral load and treatment outcomes in a US public health setting. J Acquir Immune Defic Syndr. 2017;74(1):44–45. doi:10.1097/QAI.0000000000001134
17. Olsen HA, Sarkodie E, Coleman M, et al. Fast forward to viral suppression: immediate initiation of ARVs following Reactive HIV+ test result or engagement in HIV Care for the first time at a community health center in Washington. In
18. Colasanti J, Sumitani J, Mehta CC, et al. Implementation of a rapid entry program decreases time to viral suppression among vulnerable persons living with HIV in the Southern United States. Open Forum Infect Dis. 2018;5(6):ofy104. doi:10.1093/ofid/ofy104
19. US Department of Health and Human Services. Guideline for use antiretroviral agents in adults and adolescents with HIV; 2019. Available from: https://clinicalinfo.hiv.gov/sites/default/files/guidelines/documents/AdultandAdolescentGL.pdf.
20. Saag M, Benson CA, Gandhi RT, et al. Antiretroviral drugs for treatment and prevention of HIV infection in adults: 2020 recommendations of the international antiviral society–USA panel. JAMA. 2018;320(4):379–396. doi:10.1001/jama.2018.8431
21. European AIDS Clinical Society (EACS) Guidelines. Version 10.1; 2020. Available from: http://www.eacsociety.org/guidelines/eacs-guidelines/eacs-guidelines.htlm.
22. General Directorate of Public Health. Statistical data of communicable diseases department: HIV/AIDS. Ankara: T.C. Ministry of Health. Available from: http://www.thsk.gov.tr/component/k2/353-istatiksel-veriler/bulasici-hastaliklar-dairebaskanligi-istatiksel-veriler.html.
23. Erdinc FS, Dokuzoguz B, Unal S, et al. Temporal trends in the epidemiology of HIV in Turkey. Curr HIV Res. 2020;18(4):258–266. doi:10.2174/1570162X18666200427223823
24. Turkish Ministry of Health. Turkey HIV/AIDS control program, Türkiye HIV/AIDS control programı; 2019. https://hsgm.saglik.gov.tr/depo/birimler/Bulasici-hastaliklardb/hastaliklar/HIV-ADS/Tani-Tedavi_Rehberi/HIV_AIDS_Kontrol_Programi.pdf.
25. Hosmer DW, Lemeshow S. Model-Building Strategies and Methods for Logistic Regression. in Applied Logistic Regression 91–142. Hoboken: John Wiley & Sons, Inc.; 2005. doi:10.1002/0471722146.ch4
26. World Health Organization. Guideline on when to start antiretroviral therapy and on preexposure prophylaxis for HIV; 2015. www.who.int/hiv/pub/guidelines/earlyrelease-arv/en/.
27. Medland NA, Chow EPF, McMahon JH, et al. Time from HIV diagnosis to commencement of antiretroviral therapy as an indicator to supplement the HIV cascade: dramatic fall from 2011 to 2015. PLoS One. 2017;12(5):e0177634.
28. Le Guillou A, Pugliese P, Raffi F. Reaching the Second and Third Joint United Nations Programme on HIV/AIDS 90–90-90 targets is accompanied by a dramatic reduction in primary human immunodeficiency virus (HIV) infection and recent HIV infections in a large French nationwide HIV cohort. Clin Infect Dis. 2020;71(2):293–300. doi:10.1093/cid/ciz800
29. Whitlock G, Carbonell M, Blackwell S, et al. G. Rapid initiation of antiretroviral therapy in those with newly diagnosed HIV infection in London. UK HIV Med. 2019;20(10):699–703. doi:10.1111/hiv.12780
30. Huang YC, Sun HY, Chuang YC, et al. Short-term outcomes of rapid initiation of antiretroviral therapy among HIV-positive patients: real-world experience from a single-center retrospective cohort in Taiwan. BMJ Ope. 2019;9(9):e033246. doi:10.1136/bmjopen-2019-033246
31. Scheer S, Hsu L, Schwarcz S, et al. Trends in the san francisco human immunodeficiency virus epidemic in the “Getting to Zero” Era. Clin Infect Dis. 2018;66(7):1027–1034. doi:10.1093/cid/cix940
32. Coffeya S, Bacchettib P, Sachdevc D, et al. RAPID antiretroviral therapy: high virologic suppression rates with immediate antiretroviral therapy initiation in a vulnerable urban clinic population. AIDS. 2019;33(5):825–832. doi:10.1097/QAD.0000000000002124
33. Halperin J, Conner K, Butler I, et al. A care continuum of immediate ART for newly diagnosed patients and patients presenting later to care at a federally qualified health center in New Orleans. Open Forum Infect Dis. 2019;6(4):ofz161. doi:10.1093/ofid/ofz161
34. Raymond A, Hill A, Pozniak A. Large disparities in HIV treatment cascades between eight European and high-income countries - analysis of breakpoints. J Int AIDS Soc. 2014;17(3):19507. doi:10.7448/IAS.17.4.19507
35. Levi J, Pozniak A, Heath K, Hill A. The impact of HIV prevalence, conflict, corruption, and GDP/capita on treatment cascades: data from 137 countries. J Virus Erad. 2018;4(2):80–90. doi:10.1016/S2055-6640(20)30249-1
36. Drew RS, Rice B, Rüütel K, et al. HIV continuum of care in Europe and Central Asia. HIV Med. 2017;18(7):490–499. doi:10.1111/hiv.12480
37. Le Moing V, Thiébaut R, Chêne G, et al.; APROCO Study Group SO. Predictors of long-term increase in CD4(+) cell counts in human immunodeficiency virus-infected patients receiving a protease inhibitor-containing antiretroviral regimen. J Infect Dis. 2002;185(4):471. doi:10.1086/338929
38. Sarigul F, User U, Oztoprak N. Comparison of ımmunologıcal and virological recovery of raltegravır, elvitegravir and dolutegravir ın HIV-1 ınfected naive patients. Acta Medica Mediterranea. 2019;35:3077.
39. Hileman C, Funderburg NT. Inflammation, immune activation, and antiretroviral therapy in HIV. Curr HIV/AIDS Rep. 2017;14(3):93–100. doi:10.1007/s11904-017-0356-x
40. Mussini C, Lorenzini P, Cozzi-Lepri A, et al.; Icona Foundation Study Group. CD4/CD8 ratio normalization and non-AIDS-related events in individuals with HIV who achieve viral load suppression with antiretroviral therapy: an observational cohort study. Lancet HIV. 2015;3(2):98–106. doi:10.1016/S2352-3018(15)00006-5
41. Torti C, Prosperi M, Motta D, et al. Factors influencing the normalization of CD4+ T-cell count, percentage and CD4+/CD8+ T-cell ratio in HIV infected patients on long-term suppressive antiretroviral therapy. Clin Microbiol Infect. 2012;18(5):449–458. doi:10.1111/j.1469-0691.2011.03650.x
42. Thornhill J, Inshaw J, Kaleebu P, et al. Enhanced Normalization of CD4/CD8 ratio with earlier antiretroviral therapy at primary HIV infection. J Acquir Immune Defic Syndr. 2016;73(1):69–73. doi:10.1097/QAI.0000000000001013
43. Davy-Mendez T, Napravnik S, Zakharova O, et al. Acute HIV Infection and CD4/CD8 ratio normalization after antiretroviral therapy initiation. J Acquir Immune Defic Syndr. 2018;79(4):510–518. doi:10.1097/QAI.0000000000001843
44. Cao W, Mehraj V, Trottier B, et al. Early initiation rather than prolonged duration of antiretroviral therapy in HIV infection contributes to the normalization of CD8 T-cell counts. Clin Infect Dis. 2016;62(2):250–257. doi:10.1093/cid/civ809
45. Trickey A, May MT, Schommers P, et al. CD4:CD8 Ratio and CD8 count as prognostic markers for mortality in human immunodeficiency virus-infected patients on antiretroviral therapy: the antiretroviral therapy cohort collaboration (ART-CC). Clin Infect Dis. 2017;65(6):959–966. doi:10.1093/cid/cix466
46. Veil R, Poizot-Martin I, Reynes J, et al. Virological and immunological impact of integrase inhibitor-based regimens initiated during primary HIV-1 infection. AIDS. 2020;34(4):493–500. doi:10.1097/QAD.0000000000002447
47. Deeks ED, Deeks ED. Bictegravir/Emtricitabine/Tenofovir Alafenamide: a Review in HIV-1 Infection. Drugs. 2018;78(17):1817–1828. doi:10.1007/s40265-018-1010-7
48. Zuppelli A, Mancenid M, Scutaru J, et al.; Gilead Sciences, Foster City, CA. Real world community-based HIV rapid start antiretroviral with BFTAF versus conventional HIV antiretroviral therapy start - The RoCHaCHa Study, a pilot study IDWeek 2020 Oct 21–25 virtual reported by Jules Levin; 2020.
49. Cuzin L, Cotte L, Delpierre C, et al. Dat’AIDS Study group Too fast to stay on track? Shorter time to the first anti-retroviral regimen is not associated with better retention in care in the French Dat’AIDS cohort. PLoS One. 2019;14(9):e022206. doi:10.1371/journal.pone.0222067
50. Zhao Y, Wu Z, McGoogan JM, et al. Nationwide cohort study of antiretroviral therapy timing: treatment dropout and virological failure in China, 2011–2015. Clin Infect Dis. 2019;68(1):43–50. doi:10.1093/cid/ciy400
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.