Back to Journals » International Journal of Women's Health » Volume 18
Comparison of High-Intensity Electromagnetic Therapy and Pelvic Floor Muscle Exercises in Women with Urinary Incontinence: A Randomized Controlled Trial
Authors Kilicoz Bakar M, Ozkocak G ![]() , Algun ZC
, Algun ZC
Received 28 March 2026
Accepted for publication 29 June 2026
Published 8 July 2026 Volume 2026:18 612726
DOI https://doi.org/10.2147/IJWH.S612726
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Marta Barba
Mehtap Kilicoz Bakar,1 Gokhan Ozkocak,2 Zeliha Candan Algun3
1Department of Physiotherapy and Rehabilitation, Faculty of Health Sciences, Istanbul Aydın University, Istanbul, Türkiye; 2Department of Physical Medicine and Rehabilitation, Faculty of Medicine, Istanbul Aydın University, Istanbul, Türkiye; 3Department of Physiotherapy and Rehabilitation, Faculty of Health Sciences, Istanbul Medipol University, Istanbul, Türkiye
Correspondence: Mehtap Kilicoz Bakar, Department of Physiotherapy and Rehabilitation, Faculty of Health Sciences, Istanbul Aydın University, Beşyol Mahallesi, İnönü Caddesi No: 38, Küçükçekmece, Istanbul, Türkiye, Tel +90 534 882 36 58, Email [email protected]
Background: Stress urinary incontinence is common in women and can negatively affect quality of life. This study evaluated the effects of pelvic floor muscle training alone and combined with high-intensity focused electromagnetic therapy on pelvic floor muscle function, urinary symptoms, and quality of life.
Methods: This randomized controlled trial included 44 women with stress urinary incontinence, randomly assigned to either the high-intensity focused electromagnetic therapy group or the pelvic floor muscle training group (22 per group). Both groups received supervised pelvic floor muscle training three times weekly for 8 weeks. In addition, the high-intensity focused electromagnetic therapy group received twice-weekly treatment for 6 weeks, with 28-minute sessions. The primary outcome measure was pelvic floor muscle activity, assessed using surface electromyography biofeedback. The secondary outcome measures were urinary symptoms and quality of life, evaluated using the Urogenital Distress Inventory-6, the International Consultation on Incontinence Questionnaire-Short Form, and the King’s Health Questionnaire. Appropriate parametric and nonparametric tests were used for data analysis, and statistical significance was set at p< 0.05.
Results: No significant between-group differences were found at baseline (p> 0.05). Both groups showed significant post-treatment improvements in pelvic floor muscle function and urinary symptoms. In the high-intensity focused electromagnetic therapy group, significant improvements were observed in electromyography parameters, UDI-6, and ICIQ-SF scores (all p< 0.001). Improvements in the pelvic floor muscle training group were also significant but less pronounced. After treatment, the high-intensity focused electromagnetic therapy group showed significantly better outcomes than the pelvic floor muscle training group in electromyography parameters, UDI-6, ICIQ-SF, and King’s Health Questionnaire total score (all p≤ 0.03). After Holm correction, the HIFEM + PFMT group showed significantly greater improvements than the PFMT group in Work Peak EMG activity, maximum voluntary contraction, and UDI-6 scores, with large effect sizes (g = 1.41, 1.26, and − 1.22, respectively; adjusted p ≤ 0.035). Other outcomes did not remain significant after adjustment for multiple comparisons.
Conclusion: Both pelvic floor muscle training alone and in combination with high-intensity focused electromagnetic therapy were effective in women with stress urinary incontinence. However, the combined approach provided greater improvements in several objective and subjective outcomes, suggesting that high-intensity focused electromagnetic therapy may be a useful adjunct to exercise-based conservative treatment.
Trial Registration: ClinicalTrials.gov, NCT06450795. Registered June 8, 2024.
Keywords: high-intensity focused electromagnetic stimulation, muscle function, pelvic floor muscle training, quality of life, stress urinary incontinence
Background
Urinary incontinence (UI) is a common health problem characterized by involuntary urine leakage, is more prevalent in women, and can affect individuals of all age groups.1,2 Although it is not life-threatening, it may substantially reduce quality of life by causing marked limitations in physical, psychological, social, and sexual domains. Stress urinary incontinence (SUI) is defined by the International Continence Society as the complaint of involuntary loss of urine on effort or physical exertion, or on sneezing or coughing.3 Advanced age, female sex, parity, menopause, obesity, history of pregnancy, genetic predisposition, smoking, chronic cough, and constipation are among the main risk factors associated with the development of SUI.4,5
Urine leakage, the sensation of wetness, and concerns about unpleasant odor caused by UI may lead to embarrassment, loss of self-confidence, and social isolation in women.6,7 In the long term, this condition has been reported to be associated with anxiety, psychological distress, and restrictions in social relationships.7 The literature indicates that the negative effects of UI on quality of life are closely related not only to symptom frequency but also to psychosocial and functional consequences.3
Conservative, pharmacological, and surgical approaches are available for the treatment of UI, and current clinical guidelines recommend conservative methods as first-line treatment.8 Conservative treatments include behavioral and lifestyle modifications, pelvic floor muscle training (PFMT), electrical stimulation, and biofeedback.9,10 PFMT aims to improve urethral support by increasing the strength, endurance, and functional control of the pelvic floor muscles and is considered the first-line physiotherapy approach for the treatment of UI.11–13 Cochrane systematic reviews have shown that PFMT improves quality of life, reduces urine leakage, and increases treatment satisfaction in women with stress or mixed UI.13
In recent years, innovative treatment methods that stimulate the pelvic floor muscles through electromagnetic fields have attracted increasing attention. Functional magnetic stimulation (FMS) is a non-invasive method approved by the U.S. Food and Drug Administration in 1998 for pelvic floor muscle stimulation.14,15 Based on Faraday’s law of electromagnetic induction, this method induces pelvic floor muscle contractions through neuromodulation of the sacral nerve roots (S2–S4).16–18 Since it does not require skin contact and can be applied over clothing while the patient remains seated, it has been described as a more comfortable approach than conventional electrical stimulation.18
High-intensity focused electromagnetic therapy (HIFEM), a more advanced form of functional magnetic stimulation, has recently received increasing attention because it can generate deeper and stronger contractions in the pelvic floor muscles. A recent meta-analysis highlighted the non-invasive nature of HIFEM, its ability to provide meaningful clinical improvements even with short treatment sessions, and its ease of application as important innovative features. Unlike low-intensity magnetic stimulation methods, HIFEM has been reported to activate both fast- and slow-twitch muscle fibers simultaneously, resulting in more pronounced improvements in muscle strength and endurance. In addition, HIFEM may be effective not only for symptom control but also for enhancing pelvic floor muscle awareness and supporting the motor learning process. High-intensity electromagnetic therapy has recently been proposed as a non-invasive treatment option that may stimulate pelvic floor muscle contractions. However, the current literature reveals considerable heterogeneity in HIFEM protocols and outcome measures, and objective assessments of pelvic floor muscle function remain limited. Therefore, further comparative studies using objective outcome measures are needed to clarify its clinical effectiveness.19
Although previous studies have investigated the effects of high-intensity electromagnetic therapy and pelvic floor muscle training in women with stress urinary incontinence, evidence directly comparing these two interventions within a randomized design remains limited. Moreover, few studies have used objective pelvic floor muscle activity assessed by surface electromyography biofeedback as a primary outcome alongside patient-reported urinary symptoms and quality of life measures. Therefore, the aim of this study was to compare the effectiveness of pelvic floor muscle training and high-intensity electromagnetic therapy on pelvic floor muscle function, quality of life, and urinary parameters in women with stress urinary incontinence.
Methods
This study was designed as a randomized controlled clinical trial and was conducted at Medipol Acıbadem Regional Hospital between June 2024 and June 2025. The study protocol was approved by the Non-Interventional Clinical Research Ethics Committee of İstanbul Medipol University (Decision No: E-10840098-202.3.02–2981). The study was carried out in accordance with the principles of the Declaration of Helsinki. Written informed consent was obtained from all participants before enrollment. The study was registered in the ClinicalTrials.gov database (Registration No: NCT06450795).
A total of 44 women diagnosed with stress urinary incontinence who were followed at Medipol Acıbadem Regional Hospital and met the eligibility criteria were included in the study. The aim, scope, and treatment procedures of the study were explained in detail to eligible participants by the principal investigator, and written informed consent was obtained. The inclusion criteria were as follows: having a physician-confirmed diagnosis of stress urinary incontinence, being between 20 and 65 years of age, having no history of recurrent vaginitis, having had no more than three urinary tract infections within the previous year and no active urinary tract infection, and meeting the indications specified in the user manual of the study device. The diagnosis of stress urinary incontinence was established by a physician prior to study enrollment. Only women with a physician-confirmed diagnosis of stress urinary incontinence were included in the study.The exclusion criteria were the presence of a cardiac implant or a history of untreated cardiac arrhythmia, the presence of any metal implant in the body, vaginal or pelvic surgery within the last six months, childbirth within the last 12 weeks or miscarriage within the last six weeks, any recent surgical intervention, receiving any concurrent treatment for urinary incontinence, renal or hepatic failure, the presence of neurological or neuromuscular disease, or any contraindication specified in the study device manual.
The sample size was calculated using G*Power software. The effect size was determined based on data from a previous study evaluating pelvic floor muscle function and/or urinary incontinence-related outcomes in women with urinary incontinence.20 Based on an effect size of f = 0.229, 80% statistical power, and a significance level of 5%, and considering a possible dropout rate of 10%, a total of 44 women were planned to be included in the study. Participants were allocated into two groups of 22 each. (Figure 1) Randomization was performed using the sealed-envelope method. Participants were assigned to the first or second group according to the number contained in the envelope they selected. The envelopes were sealed and opaque to ensure allocation concealment before group assignment. Due to the nature of the interventions, participants and therapists could not be blinded to group allocation.
 |
Figure 1 CONSORT flow diagram of participant enrollment, allocation, follow-up, and analysis. |
The study was conducted with two groups. Group 1 (HIFEM) received pelvic floor muscle training and high-intensity focused electromagnetic therapy (HIFEM), whereas Group 2 (PFMT) received pelvic floor muscle training only.
All participants underwent a baseline assessment. Participants in both groups were enrolled in a pelvic floor muscle training (PFMT) program supervised by a specialist physiotherapist. The PFMt program was performed three days per week for eight weeks, with each session lasting 30–45 minutes. In addition to PFMT, participants in the first group received HIFEM treatment twice weekly for six weeks, with each session lasting 28 minutes. Accordingly, total intervention time and treatment exposure were not identical between groups, as the first group received additional device-based HIFEM sessions. This difference was inherent to the comparative intervention design and was considered when interpreting the findings. All assessments were repeated after completion of the treatment period. For ethical reasons, participants in the second group were offered HIFEM treatment after the completion of the study.
Assessments
The primary outcome measure was pelvic floor muscle activity assessed using surface electromyography biofeedback. Assessments were performed at baseline and immediately after the intervention period. Secondary outcome measures included urinary symptoms and quality of life, evaluated using the Urogenital Distress Inventory-6, the International Consultation on Incontinence Questionnaire-Short Form, and the King’s Health Questionnaire.
Demographic and clinical characteristics of the participants, including age, height, body weight, body mass index (BMI), educational level, occupation, smoking and alcohol use, history of chronic disease, and menopausal status, were recorded using a structured data collection form.
The severity of urinary incontinence symptoms and their impact on quality of life were assessed using the International Consultation on Incontinence Questionnaire–Short Form (ICIQ-SF), the Turkish validity and reliability of which were established by Çetinel et al21 This questionnaire consists of six items evaluating the frequency, amount, and type of incontinence, as well as its impact on daily life. The total score ranges from 0 to 21, with higher scores indicating greater severity of incontinence.12
The impact of urinary symptoms on quality of life was assessed using the King’s Health Questionnaire (KHQ), whose Turkish validity and reliability were established by Kaya et al22 The KHQ consists of 32 items and includes two main sections. The first section assesses general health perception and the impact of incontinence, whereas the second section evaluates quality of life across seven subdomains: role limitations, physical limitations, social limitations, personal relationships, emotions, sleep/energy, and symptom severity. Scores obtained from the subscales range from 0 to 100, with higher scores indicating poorer quality of life. In addition, the symptom severity scale is scored between 0 and 30, with higher scores indicating increased symptom severity.22
The Urogenital Distress Inventory–Short Form (UDI-6) was used to assess incontinence-related symptoms. This scale consists of six items rated on a four-point Likert scale. The total score ranges from 0 to 18 and is converted into a percentage score. Higher scores indicate a greater level of symptom-related distress. The Turkish validity and reliability of the scale were established by Çam et al.23
Pelvic floor muscle activity was assessed using a dual-channel surface electromyography device (NeuroTrac Myoplus 4, Verity Medical Ltd., UK) according to the protocol described by Pekbay et al24 Before measurement, participants were asked to empty their bladder and rectum. The assessment was performed in the supine crook-lying position. During the assessment, the active electrode was placed around the anal sphincter, while the reference electrode was positioned over the adductor muscle group on the medial aspect of the right thigh. Following the device’s auditory cues, participants were instructed to perform a maximum voluntary contraction for 5 seconds, followed by 5 seconds of relaxation. A total of 10 repetitions were completed according to this protocol, and electromyographic signals corresponding to the contraction and relaxation phases were recorded. Resting EMG values represented the average electromyographic activity recorded during the relaxation phases of the assessment protocol and were obtained under standardized testing conditions for all participants. The analyzed parameters were as follows:
● Work Average (µV): Mean EMG activity across all contractions
● Average Deviation (µV): Mean variation in the EMG signal during the contraction period
● Peak (µV): Highest contraction value recorded during the measurement
● Rest Average (µV): Mean EMG activity during the relaxation phase
Interventions
Pelvic Floor Muscle Training
All participants received a structured pelvic floor muscle training (PFMT) program consisting of both sustained and rapid voluntary pelvic floor muscle contractions. The program was designed to target endurance-related and rapid response components of pelvic floor muscle performance. Correct activation of the pelvic floor muscles was initially taught and confirmed by a specialist physiotherapist using vaginal palpation.
The exercise program consisted of sets including 10 rapid contractions and 10 sustained contractions. For sustained contractions, participants were instructed to maintain each contraction for 10 seconds, followed by a complete relaxation phase. Participants performed the exercises three days per week for eight weeks, with three exercise sessions per day. The training load was progressively increased, starting with one set during the first week and reaching a total of 10 sets by the eighth week through gradual weekly increments.
The exercise program was progressed throughout the intervention period by increasing the number of sets and introducing more challenging exercise positions. During the first week, exercises were performed in the supine position with legs extended and in the crook-lying position. As training progressed, exercises were also performed in sitting and standing positions to enhance motor control and functional performance. The reported 40–45-minute duration represented the total duration of the supervised training session, including exercise instruction, supervised practice, technique correction, and rest intervals. Pelvic floor muscle contractions were not performed continuously throughout the entire session. Participants were also instructed to continue the prescribed exercises as a home exercise program throughout the intervention period. All supervised exercise sessions were conducted by a specialist physiotherapist (Table 1).
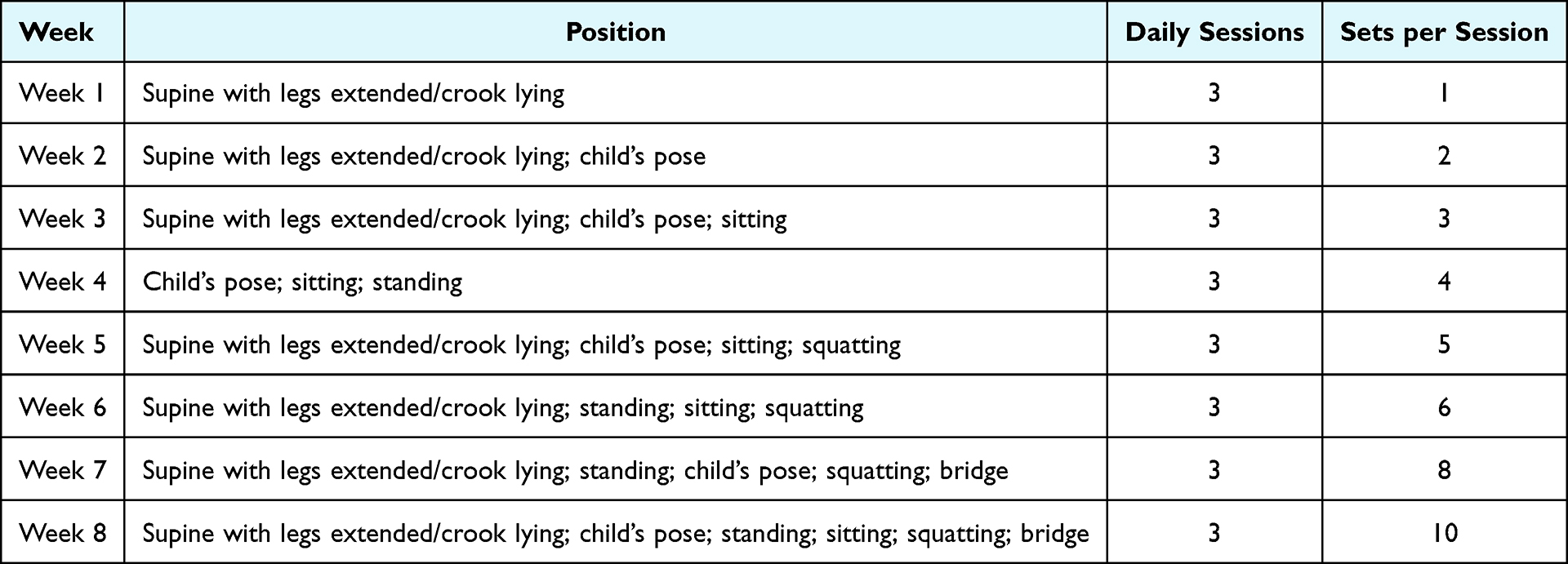 |
Table 1 Progressive Pelvic Floor Muscle Training Program |
High-Intensity Focused Electromagnetic Therapy (HIFEM)
To strengthen the pelvic floor muscles, participants in the first group received high-intensity focused electromagnetic therapy. A non-invasive device using HIFEM technology (BTL EMSELLA®, BTL Industries Ltd., Czech Republic) was used for treatment. The device is CE-certified under the European Union Medical Device Directive (93/42/EEC) and is suitable for clinical use in the conservative treatment of urinary incontinence. During HIFEM therapy, participants were seated on a specially designed chair with the coil applicator integrated into the seat, and a focused electromagnetic field was applied to the pelvic region. During the application, alternating electromagnetic fields of up to 2.5 Tesla depolarized the pelvic floor motor neurons and induced supramaximal contractions of the pelvic floor muscles. This mechanism enables selective and deep activation of the pelvic floor muscles.25,26
HIFEM therapy was administered concurrently with pelvic floor muscle training for six weeks, twice weekly, with each session lasting 28 minutes. The stimulation frequency was set between 10 and 50 Hz, and the intensity was gradually increased to the maximum level tolerated by the participant. Throughout the treatment period, participants received the intervention in a seated position while fully clothed. Participants did not perform voluntary pelvic floor muscle exercises during HIFEM sessions. HIFEM was administered as a separate device-based intervention, while PFMT was performed during supervised exercise sessions.
Statistical Analysis
Statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) version 23.0. Data distribution was assessed using the Shapiro–Wilk test, and the assumption of normality was further supported by examining skewness and kurtosis values. For normally distributed variables, paired samples t-test was used for within-group comparisons and independent samples t-test was used for comparisons between two independent groups. For non-normally distributed variables, the Wilcoxon signed-rank test was used for within-group comparisons and the Mann–Whitney U-test was used for between-group comparisons. Descriptive statistics were presented as mean and standard deviation according to data distribution. Categorical variables were analyzed using the chi-square test and reported as frequency and percentage. A p value of <0.05 was considered statistically significant. Change scores were calculated by subtracting baseline values from post-treatment values for each outcome. Between-group comparisons of change scores were used as the primary analytical approach to evaluate the comparative effectiveness of the interventions. Effect sizes were reported as Hedges’ g, and 95% confidence intervals were calculated for between-group mean differences. To reduce the risk of type I error due to multiple comparisons, Holm-adjusted p-values were additionally reported. Within-group comparisons were considered supplementary and were not used as the main basis for interpretation.
Results
Descriptive data on age, height, body weight, body mass index, number of deliveries, age at menopause, presence of chronic disease, medication use, smoking and alcohol consumption, and educational level are presented by group in Table 2. No statistically significant differences were found between the groups in terms of these demographic and clinical characteristics (p > 0.05).
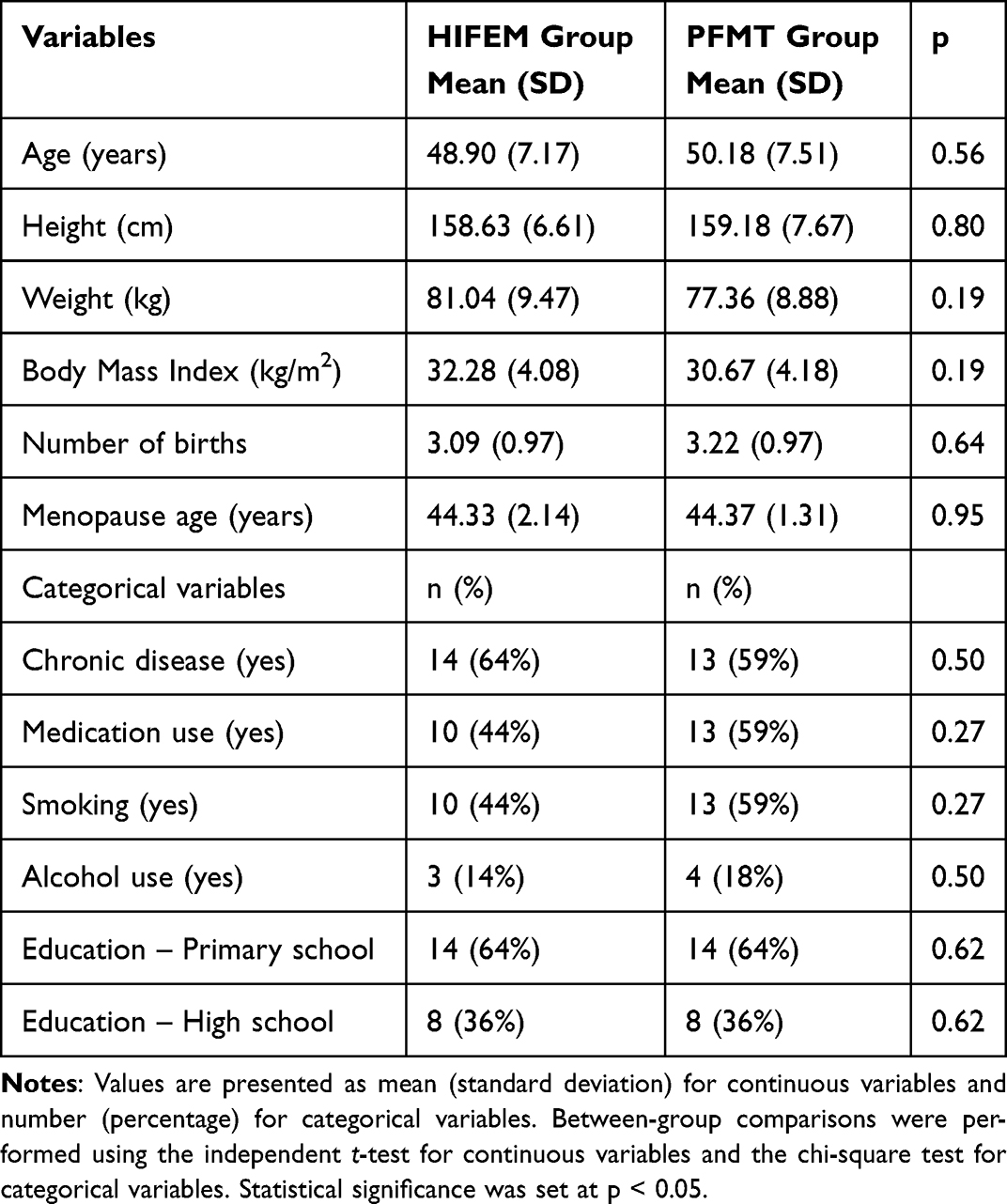 |
Table 2 Participants’ Demographic and Clinical Characteristics |
In the within-group pre- and post-treatment comparisons, the HIFEM group showed statistically significant improvements after treatment in EMG-biofeedback parameters, including work average, work peak, maximum voluntary contraction, and rest average, as well as in UDI, ICIQ-SF, and KHQ scores (p < 0.05). In the PFMT group, significant improvements were observed in EMG-biofeedback parameters and in UDI and ICIQ-SF scores (p < 0.05). In addition, for the KHQ, statistically significant post-treatment changes were found in all subdomains and in the total score except for the physical limitation subdomain (p < 0.05) (Table 3).
 |
Table 3 Within-Group Pre–Post Comparisons of EMG Parameters, Clinical Outcomes and KHQ Subscale Scores |
Before treatment, the HIFEM and PFMT groups were compared in terms of EMG-biofeedback parameters, severity of urinary symptoms, quality of life, and the subdomains of the King’s Health Questionnaire. No statistically significant differences were found between the groups in any of the parameters evaluated at baseline (p > 0.05) (Table 3).
After treatment, the HIFEM and PFMT groups were compared in terms of EMG-biofeedback parameters, severity of urinary symptoms, and quality-of-life outcomes. Statistically significant differences were found in favor of the HIFEM group for all EMG parameters except rest average, as well as for most of the clinical scales (p < 0.05) (Table 4).
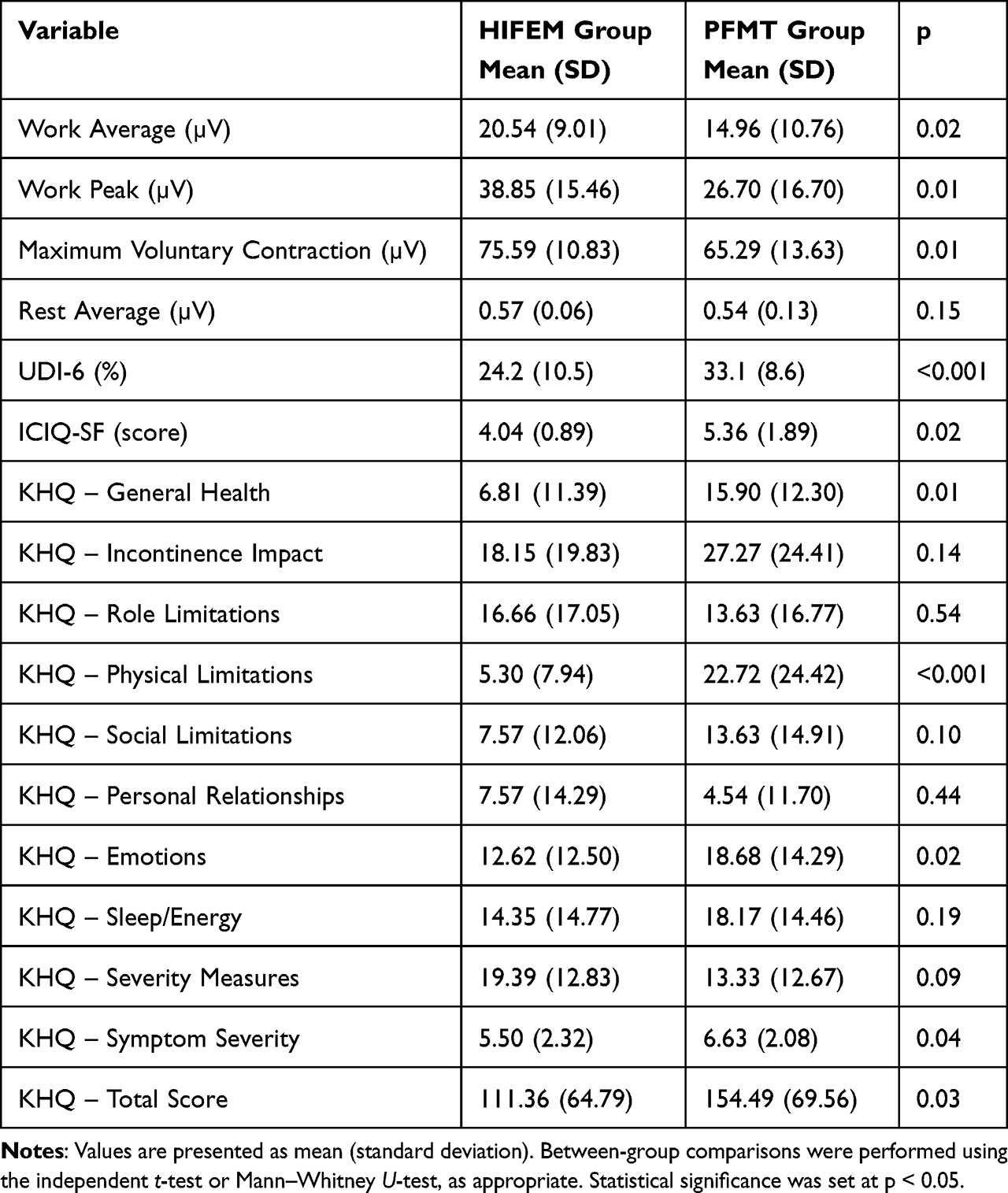 |
Table 4 Between-Group Post-Treatment Comparisons of EMG Parameters, Clinical Outcomes and KHQ Subscale Scores |
Between-group analyses showed greater improvements in several EMG parameters and urinary symptom outcomes in the HIFEM + PFMT group compared with the PFMT group. After Holm adjustment for multiple comparisons, significant between-group differences remained for Work Peak, maximum voluntary contraction, and UDI-6, favoring the HIFEM + PFMT group. Although unadjusted analyses also suggested significant differences in Work Average, ICIQ-SF, KHQ-General Health, KHQ-Physical Limitations, KHQ-Emotions, KHQ-Symptom Severity, and KHQ-Total Score, these findings did not remain statistically significant after adjustment for multiple comparisons. Therefore, these secondary and subdomain findings should be interpreted cautiously (Table 5).
 |
Table 5 Between-Group Comparison of Baseline-to-Post-Treatment Change Scores in EMG Parameters, Urinary Symptoms, and Quality of Life Outcomes |
Discussion
In this study, the effects of pelvic floor muscle training alone and pelvic floor muscle training combined with high-intensity focused electromagnetic therapy were evaluated in women with stress urinary incontinence. The findings suggest that both interventions were associated with improvements in pelvic floor muscle function, urinary symptoms, and quality of life. However, when the results were interpreted primarily according to between-group change score analyses, the additional benefit of HIFEM appeared to be most evident in selected EMG parameters and UDI-6 scores.
The effectiveness of PFMT in the treatment of SUI is strongly supported in the literature. Systematic reviews and meta-analyses have shown that PFMT, either alone or in combination with other conservative methods, reduces the frequency of urine leakage and improves quality of life.19,27 Programs that include isolated and repeated pelvic floor muscle contractions and are performed with sufficient frequency and duration appear to be particularly effective.19 The PFMT protocol used in the present study, which included both slow and rapid isolated contractions and was maintained at a consistent weekly frequency with gradual progression, is in line with the characteristics recommended in the literature. Accordingly, improvements observed in both groups are consistent with previous evidence supporting PFMT as a first-line conservative treatment approach for women with stress urinary incontinence.
Nevertheless, the literature indicates that the response to PFMT may be limited in some cases and that additional neuromuscular facilitation may be needed.27,28 In this context, magnetic stimulation-based approaches have emerged as a complementary option to pelvic floor muscle training. Sham-controlled randomized studies have shown that magnetic stimulation provides improvements beyond placebo effects in the number of incontinence episodes, pad test outcomes, and quality of life in women with urinary incontinence.20,29,30 In addition, the non-invasive nature of these methods, their high level of patient comfort, and the possibility of administration over clothing have been reported as important advantages.30
Recent studies have suggested that approaches using higher-intensity electromagnetic fields may have beneficial effects on pelvic floor muscle activation. In randomized and comparative studies with different designs, magnetic stimulation applications have been reported to reduce symptom severity, improve quality of life, and increase pelvic floor muscle awareness.31–33 Assessments performed using objective methods such as electromyography and ultrasonography have also suggested that these treatments may be associated with neuromuscular changes in addition to subjective symptom improvement.32,33 High-intensity focused electromagnetic therapy has attracted increasing attention because it may induce repeated involuntary contractions in the pelvic floor muscles. Previous randomized controlled, sham-controlled, and observational studies have reported that HIFEM applications may reduce symptom severity, improve quality of life, and enhance pelvic floor muscle function in women with stress or mixed urinary incontinence.20,26,34–37 However, the current literature remains heterogeneous in terms of stimulation protocols, treatment duration, session frequency, outcome measures, and comparator groups. Therefore, further randomized comparative studies using objective outcome measures are needed to clarify the clinical role of HIFEM.
The findings of previous studies suggest that even short-term HIFEM protocols may be associated with improvements in pelvic floor muscle activity and clinical outcomes.26,34–37 These findings are also supported by recent evidence syntheses. A recent systematic review and meta-analysis reported that non-invasive HIFEM significantly reduced urinary incontinence symptoms, improved quality of life, and increased patient satisfaction. The same study also emphasized ease of application and high patient tolerability as major advantages of HIFEM, while simultaneous activation of fast- and slow-twitch muscle fibers was proposed as a possible mechanism underlying gains in muscle strength and endurance.38 However, because muscle fiber recruitment and neuromuscular activation patterns were not directly assessed in the present study, such physiological mechanisms should be interpreted cautiously and considered as possible explanations rather than definitive conclusions.
The direct comparison of HIFEM technology combined with PFMT versus a structured PFMT program alone in the present study helps address an important gap in the literature. Most previous studies have compared magnetic stimulation with sham or passive control groups, and studies directly comparing HIFEM-supported interventions with PFMT in the field of stress urinary incontinence remain limited. In the present study, the use of surface EMG-biofeedback as an objective assessment method for pelvic floor muscle function is a methodological strength, particularly because many previous studies have relied primarily on subjective symptom scales. Nevertheless, the findings should be interpreted cautiously because of the limited sample size and the short-term nature of the follow-up.
The interpretation of the findings was primarily based on between-group differences in change scores rather than within-group improvements. Although both groups showed improvements from baseline, the adjusted between-group analyses indicated that the additional effect of HIFEM was most evident in selected EMG parameters and UDI-6 scores. After adjustment for multiple comparisons, significant between-group differences remained for Work Peak, maximum voluntary contraction, and UDI-6 scores, favoring the HIFEM group. Other outcomes showed favorable unadjusted differences; however, these did not remain statistically significant after Holm correction. Therefore, findings from secondary outcomes and KHQ subdomains should be interpreted cautiously.
In addition to statistical significance, the clinical relevance of the observed changes should be considered. Improvements in urinary symptom scores, particularly UDI-6 and ICIQ-SF, were interpreted in relation to previously reported minimal clinically important difference values where available. This approach is important because statistically significant differences may not always correspond to clinically meaningful improvements from the patient perspective. In the present study, the greater improvement in UDI-6 in the HIFEM group suggests a potentially meaningful reduction in urinary symptom burden; however, this finding should be confirmed in larger randomized trials with longer follow-up periods.
This study has several limitations. First, the sample size was relatively small, which may limit statistical power and the precision of effect estimates. Second, the data were obtained from a single center, which may limit the generalizability of the findings. Third, there was no separate group to evaluate the isolated effects of HIFEM; therefore, the independent contribution of HIFEM could not be determined. Fourth, participants and therapists could not be blinded due to the nature of the interventions. This may have introduced performance bias, particularly for subjective outcomes such as self-reported urinary symptoms and quality of life. Fifth, total intervention time and therapist contact were not identical between groups because the HIFEM + PFMT group received additional device-based treatment sessions. Sixth, adherence to the home-based PFMT program was not systematically recorded; therefore, the extent to which participants fully complied with the prescribed exercise program could not be objectively evaluated. Finally, only short-term post-treatment outcomes were assessed, and the long-term sustainability of the observed improvements remains unclear.
This study compared pelvic floor muscle training alone with pelvic floor muscle training combined with adjunct high-intensity focused electromagnetic therapy in women with stress urinary incontinence. The findings suggest that adding HIFEM to PFMT may provide additional short-term benefits in selected pelvic floor muscle activity parameters and urinary symptom outcomes. However, given the relatively small sample size, lack of participant and therapist blinding, unequal intervention exposure, absence of systematic adherence monitoring, and short-term follow-up, these results should be interpreted cautiously. Further larger-scale randomized controlled trials with longer follow-up periods, standardized adherence monitoring, and balanced comparator designs are needed to confirm the clinical effectiveness of HIFEM as an adjunct to PFMT.
Abbreviations
HIFEM, High-intensity focused electromagnetic therapy; ICIQ-SF, International Consultation on Incontinence Questionnaire-Short Form; KHQ, King’s Health Questionnaire; PFMT, Pelvic floor muscle training; SPSS, Statistical Package for the Social Sciences; SUI, Stress urinary incontinence; UDI-6, Urogenital Distress Inventory-6.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available due to privacy and ethical restrictions but are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The study protocol was approved by the Non-Interventional Clinical Research Ethics Committee of Istanbul Medipol University (Decision No: E-10840098-202.3.02-2981). The study was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants prior to enrollment. The trial was registered at ClinicalTrials.gov (NCT06450795).
Acknowledgments
The authors would like to thank all participants who took part in this study. The authors also thank TÜBİTAK for the financial support provided through the BİDEB 2211 Domestic Graduate Scholarship Program. In addition, the authors would like to thank Ezgi Gök for her support during the study process. Generative artificial intelligence was used only for English language editing. All scientific content, interpretation, and final approval of the manuscript were performed by the authors.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Scientific and Technological Research Council of Türkiye (TÜBİTAK), Presidency of Scientists Support Programs (BİDEB), through the 2211 Domestic Graduate Scholarship Program. The funder had no role in the design of the study, data collection, analysis, interpretation of data, or writing of the manuscript.
Disclosure
The authors declare that they have no competing interests.
References
1. Bø K. Pelvic floor muscle training is effective in treatment of female stress urinary incontinence, but how does it work? Int Urogynecol J Pelvic Floor Dysfunct. 2004;15(2):76–14. doi:10.1007/s00192-004-1125-0
2. de Andrade RL, Bø K, Antonio FI, et al. An education program about pelvic floor muscles improved women’s knowledge but not pelvic floor muscle function, urinary incontinence or sexual function: a randomised trial. J Physiother. 2018;64(2):91–96. doi:10.1016/j.jphys.2018.02.010
3. Basak T, Uzun S, Arslan F. Incontinence features, risk factors, and quality of life in Turkish women presenting at the hospital for urinary incontinence. J Wound Ostomy Continence Nurs. 2012;39(1):84–89. doi:10.1097/WON.0b013e31823efd47
4. Delancey JO. Why do women have stress urinary incontinence? Neurourol Urodyn. 2010;29(Suppl 1):S13–S17. doi:10.1002/nau.20888
5. Leroy Lda S, Lopes MH. Urinary incontinence in the puerperium and its impact on the health-related quality of life. Rev Lat Am Enfermagem. 2012;20(2):346–353. doi:10.1590/s0104-11692012000200018
6. Petros P. The Female Pelvic Floor: Function, Dysfunction and Management According to the Integral Theory.
7. Aoki Y, Brown HW, Brubaker L, Cornu JN, Daly JO, Cartwright R. Urinary incontinence in women. Nat Rev Dis Primers. 2017;3:17042. doi:10.1038/nrdp.2017.42
8. Demaagd GA, Davenport TC. Management of urinary incontinence. PT. 2012;37(6):345–361H.
9. Sussman RD, Syan R, Brucker BM. Guideline of guidelines: urinary incontinence in women. BJU Int. 2020;125(5):638–655. doi:10.1111/bju.14927
10. Faiena I, Patel N, Parihar JS, Calabrese M, Tunuguntla H. Conservative management of urinary incontinence in women. Rev Urol. 2015;17(3):129–139.
11. Freeman RM. The role of pelvic floor muscle training in urinary incontinence. BJOG. 2004;111(Suppl 1):37–40. doi:10.1111/j.1471-0528.2004.00464.x
12. Riaz H, Nadeem H, Rathore FA. Recent advances in the pelvic floor assessment and rehabilitation of women with pelvic floor dysfunction. J Pak Med Assoc. 2022;72(7):1456–1459. doi:10.47391/JPMA.22-83
13. Dumoulin C, Cacciari LP, Hay-Smith EJC. Pelvic floor muscle training versus no treatment, or inactive control treatments, for urinary incontinence in women. Cochrane Database Syst Rev. 2018;10(10):CD005654. doi:10.1002/14651858.CD005654.pub4
14. Antić A, Pavčnik M, Lukanović A, Matjašič M, Lukanović D. Magnetic stimulation in the treatment of female urgency urinary incontinence: a systematic review. Int Urogynecol J. 2023;34(8):1669–1676. doi:10.1007/s00192-023-05492-7
15. Braga A, Castronovo F, Caccia G, et al. Efficacy of 3 Tesla functional magnetic stimulation for the treatment of female urinary incontinence. J Clin Med. 2022;11(10):2805. doi:10.3390/jcm11102805
16. Barker AT, Freeston IL, Jalinous R, Jarratt JA. Magnetic stimulation of the human brain and peripheral nervous system: an introduction and the results of an initial clinical evaluation. Neurosurgery. 1987;20(1):100–109. doi:10.1097/00006123-198701000-00024
17. Galloway NT, El-Galley RE, Sand PK, Appell RA, Russell HW, Carlan SJ. Extracorporeal magnetic innervation therapy for stress urinary incontinence. Urology. 1999;53(6):1108–1111. doi:10.1016/s0090-4295(99)00037-018
18. Lo TS, Tseng LH, Lin YH, Liang CC, Lu CY, Pue LB. Effect of extracorporeal magnetic energy stimulation on bothersome lower urinary tract symptoms and quality of life in female patients with stress urinary incontinence and overactive bladder. J Obstet Gynaecol Res. 2013;39(11):1526–1532. doi:10.1111/jog.12090
19. Hay-Smith EJC, Starzec-Proserpio M, Moller B, et al. Comparisons of approaches to pelvic floor muscle training for urinary incontinence in women. Cochrane Database Syst Rev. 2024;12(12):CD009508. doi:10.1002/14651858.CD009508.pub2
20. Ptaszkowski K, Malkiewicz B, Zdrojowy R, Ptaszkowska L, Paprocka-Borowicz M. Assessment of the short-term effects after high-inductive electromagnetic stimulation of pelvic floor muscles: a randomized, Sham-Controlled Study. J Clin Med. 2020;9(3):874. doi:10.3390/jcm9030874
21. Cetinel B, Ozkan B, Can G. The validation study of ICIQ-SF Turkish version. Turk J Urol. 2004;30(3):332–338.
22. Kaya S, Akbayrak T, Toprak Çelenay Ş, Dolgun A, Ekici G, Beksaç S. Reliability and validity of the Turkish King’s Health Questionnaire in women with urinary incontinence. Int Urogynecol J. 2015;26(12):1853–1859. doi:10.1007/s00192-015-2786-6
23. Cam C, Sakalli M, Ay P, Cam M, Karateke A. Validation of the short forms of the incontinence impact questionnaire (IIQ-7) and the urogenital distress inventory (UDI-6) in a Turkish population. Neurourol Urodyn. 2007;26(1):129–133. doi:10.1002/nau.20292
24. Pekbay Y, Ergin O, Topuz B, et al. The effects of pelvic floor muscle therapy on symptoms, voiding, and pelvic floor muscle activity parameters in children with overactive bladder. Neurourol Urodyn. 2019;38(5):1430–1442. doi:10.1002/nau.24007
25. Alinsod R, Vasilev V, Yanev K, Buzhov B, Stoilov M, Georgiev M. HIFEM Technology - A New Perspective in Treatment of Stress Urinary Incontinence. Lasers Surg Med. 2018;50(S29):S4–S56.
26. Silantyeva E, Zarkovic D, Astafeva E, et al. A comparative study on the effects of high-intensity focused electromagnetic technology and electrostimulation for the treatment of pelvic floor muscles and urinary incontinence in parous women: analysis of posttreatment data. Female Pelvic Med Reconstr Surg. 2021;27(4):269–273. doi:10.1097/SPV.0000000000000807
27. Alouini S, Memic S, Couillandre A. Pelvic floor muscle training for urinary incontinence with or without biofeedback or electrostimulation in women: a systematic review. Int J Environ Res Public Health. 2022;19(5):2789. doi:10.3390/ijerph19052789
28. Ahlund S, Nordgren B, Wilander EL, Wiklund I, Fridén C. Is home-based pelvic floor muscle training effective in treatment of urinary incontinence after birth in primiparous women? A randomized controlled trial. Acta Obstet Gynecol Scand. 2013;92(8):909–915. doi:10.1111/aogs.12173
29. Yamanishi T, Suzuki T, Sato R, Kaga K, Kaga M. Fuse M.Effects of magnetic stimulation on urodynamic stress incontinence refractory to pelvic floor muscle training in a randomized sham-controlled study. Lower Urinary Tract Symptoms. 2019;11:61–65. doi:10.1111/luts.12197
30. Suzuki T, Yasuda K, Yamanishi T, et al. Randomized, double-blind, sham-controlled evaluation of the effect of functional continuous magnetic stimulation in patients with urgency incontinence. Neurourol Urodyn. 2007;26(6):767–772. doi:10.1002/nau.20423
31. Lopopolo G, Salsi B, Banfi A, Isaza PG, Fusco I. Is it possible to improve urinary incontinence and quality of life in female patients? A clinical evaluation of the efficacy of top flat magnetic stimulation technology. Bioengineering. 2022;9(4):140. doi:10.3390/bioengineering9040140
32. Frigerio M, Barba M, Cola A, et al. Flat magnetic stimulation for stress urinary incontinence: a prospective comparison study. Bioengineering. 2023;10(3):295. doi:10.3390/bioengineering10030295
33. Barba M, Cola A, Rezzan G, et al. Flat magnetic stimulation for stress urinary incontinence: a 3-month follow-up study. Healthcare. 2023;11(12):1730. doi:10.3390/healthcare11121730
34. Long CY, Lin KL, Yeh JL, Feng CW, Loo ZX. Effect of high-intensity focused electromagnetic technology in the treatment of female stress urinary incontinence. Biomedicines. 2024;12(12):2883. doi:10.3390/biomedicines12122883
35. Tosun H, Akınsal EC, Sönmez G, Baydilli N, Demirci D. Is the high-intensity focused electromagnetic energy an effective treatment for urinary incontinence in women? Ther Clin Risk Manag. 2024;20:811–816. doi:10.2147/TCRM.S478919
36. Samuels JB, Pezzella A, Berenholz J, Alinsod R. Safety and efficacy of a non-invasive High-Intensity Focused Electromagnetic Field (HIFEM) device for treatment of urinary incontinence and enhancement of quality of life. Lasers Surg Med. 2019;51(9):760–766. doi:10.1002/lsm.23106
37. Jongjakapan A, Temtanakitpaisan T, Pinjaroen K, Chongsomchai C, Temtanakitpaisan A. Effectiveness of High-Intensity Focused Electromagnetic (HIFEM) therapy in women with urinary incontinence. Int Urogynecol J. 2026;37(4):921–928. doi:10.1007/s00192-025-06362-0
38. Leonardo K, Rahardjo HE, Afriansyah A. Noninvasive high-intensity focused electromagnetic therapy in women with urinary incontinence: a systematic review and meta-analysis. Neurourol Urodyn. 2025;44(2):424–433. doi:10.1002/nau.25658
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy and Adverse Effects After Single-Incision Slings for Women with Stress Urinary Incontinence: A 12-Year Follow-Up
Barba M, Cola A, Costa C, Liberatore A, Frigerio M
International Journal of Women's Health 2023, 15:1077-1082
Published Date: 18 July 2023
Enhancing Pelvic Floor Muscle Training Efficacy for Middle-Aged Women with Stress Urinary Incontinence Through Square Dance Integration: A Quasi-Experimental Study

Du F, Dong Y, Tian T, Li W, Wan F, Shi S
Journal of Multidisciplinary Healthcare 2024, 17:3863-3873
Published Date: 9 August 2024