Back to Journals » International Journal of General Medicine » Volume 16
Comparison of Hematological Parameters Between Survivors and Non-Survivors COVID-19 Patients in Saudi Arabia
Authors Binsaleh NK ![]() , Eltayeb R, Sherwani S
, Eltayeb R, Sherwani S ![]() , Almishaal AA, Hindi EA, Qanash H
, Almishaal AA, Hindi EA, Qanash H ![]() , Bazaid AS
, Bazaid AS ![]() , Alharbi AO, Bazaid MB, Altamimi SA
, Alharbi AO, Bazaid MB, Altamimi SA
Received 15 May 2023
Accepted for publication 15 August 2023
Published 31 August 2023 Volume 2023:16 Pages 3955—3962
DOI https://doi.org/10.2147/IJGM.S421418
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Naif K Binsaleh,1,2 Reem Eltayeb,1 Subuhi Sherwani,2,3 Ali A Almishaal,4 Emad A Hindi,5 Husam Qanash,1,2 Abdulrahman S Bazaid,1 Abdulmajeed Owayed Alharbi,6 Mohammed B Bazaid,7 Shayaa Alsaadi Altamimi8
1Department of Medical Laboratory Science, College of Applied Medical Sciences, University of Ha’il, Hail, Saudi Arabia; 2Medical and Diagnostic Research Centre, University of Ha’il, Hail, 55476, Saudi Arabia; 3Department of Biology, College of Sciences, University of Hail, Hail, Saudi Arabia; 4Department of Speech-Language Pathology and Audiology, College of Applied Medical Sciences, University of Hail, Hail, Saudi Arabia; 5Department of Clinical Anatomy, Faculty of Medicine, King Abdulaziz University, Jeddah, Saudi Arabia; 6Laboratory Department, King Fahad General Hospital, Jeddah, Saudi Arabia; 7Pediatric Department, East Jeddah Hospital, Jeddah, Saudi Arabia; 8Quality Department, King Khalid Hospital, Hail, Saudi Arabia
Correspondence: Naif K Binsaleh, Department of Medical Laboratory Science, College of Applied Medical Sciences, University of Hail, P.O. Box 2440, Hail, Saudi Arabia, Tel +966505274077, Email [email protected]
Objective: Coronavirus disease 2019, caused by the severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2), is a communicable disease transmitted through the respiratory route and bodily contact. The severity of infection and mortality rate of COVID-19 cases was significantly high in the initial stages of the pandemic. This study aims to investigate the hematological profile of COVID-19 survivors and non-survivors.
Methods: This is a single-center retrospective study. A total of 108 hospitalized patients with laboratory-confirmed COVID-19 at East Jeddah Hospital between April and August 2020 were categorized into two groups based on outcome as survivors (n = 54) and non-survivors (n = 54). Hematological parameters and clinical profiles were analyzed and compared between the two groups.
Results: The mean age and standard deviation of the survived (30– 71 years) and non-survived (33– 83) groups was 53 ± 10.8 and 57.9 ± 12.2 years, respectively, with no statistically significant difference in age between groups (p = 0.0513). Non-survivors had a significantly longer median length of stay in the intensive care unit (ICU) (7 days, IQR: 4.24 to 12) compared to survivors COVID-19 patients (5 days, IQR: 0 to 11.75) (p = 0.0151). For the survivors group, the participant’s age positively correlated with the length of hospital stay (r(52) = 0.21, p = 0.0005) and ICU length of stay r(52) = 0.18, p = 0.001). The median red blood cells (RBC) counts were significantly higher in the survived group (4.56x109/L, IQR: 4.02 to 5.11) in comparison with the non-survived (4.23x109/L, IQR: 3.75 to 4.23) group (p = 0.0011). All COVID-19 patients exhibited lymphocytopenia and a significant negative correlation was observed between the lymphocyte values and length of hospital stay among the survived group (p < 0.001) as well as length of ICU stay among the survived group (p < 0.0480). Disease-related mortality was significantly associated with reduced white blood cells (WBCs) (8.5× 109/L, IQR: 6.1 to 11.7) and reduced basophils (0.09%, IQR: 0.02 to 0.19). Additionally, statistically significant differences were found between the survived and non-survived groups with respect to prothrombin time (PT) (12.5 sec. vs 14 sec., p < 0.0001) and partial thromboplastin time (PTT) (31.8 sec. vs 40 sec., p = 0.0008).
Conclusion: Hematological parameters can serve as valuable indicators to identify patients with severe COVID-19 and expected poor-prognosis/outcomes upon hospital admission. Cell counts of lymphocytes, WBCs, basophils and parameters such as PT and PTT can serve as clinical indicators to assess disease severity and predict progression to critical illness.
Keywords: SARS-CoV-2, hematology, COVID-19
Introduction
Corona virus (SARS-CoV-2) has rapidly spread around the world since early 2020, potentially causing a communicable respiratory infectious disease known as “COVID-19”, with signs differing from person-to-person. As of December 2022, 651,918,402 cases were revealed globally, resulting in 6,656,601 disease-related deaths (including the Middle East).1 Despite the variety of medical systems in the Eastern Mediterranean region, the regulation of educational, social, and economic movements has restricted the infection’s enormous incidence.2 The COVID-19-related mortality rate has been estimated to vary between 2% and 20%, primarily according to the availability of medical resources and the patient’s or region’s economic standing overall.3 The impact of manifestation of illness varies from person to person. Therefore, the intensity and mortality rates differ between regions, and this can be explained by the virus polymorphisms that were present in that region at the time.4,5 Both mortality and morbidity from COVID-19 are higher in the aged and those with pre-existing chronic and comorbid conditions. Strong evidence now shows that people with certain health conditions, such as chronic kidney disease, diabetes, lung and liver disease, cardiovascular disease, obesity, immunodeficiency, certain disabilities, and mental health conditions, are at a higher risk.6 However, it has been noticed that young and healthy individuals succumbed to COVID19 in an unpredictable manner. While physical examination and the patient’s evaluation are essential, laboratory characteristics can help provide additional and indispensable data and insight into the patients’ disease, thereby improving patient management.7 Hematological alterations are linked with viral infectious diseases such as influenza, varicella, dengue, and acquired immunodeficiency virus, as well as the Middle East respiratory syndrome coronavirus (MERS CoV). The modifications have not only assisted in tracking the infectious process, but also expected severity.8
Several research findings have recognized various predictors of mortality, such as demographic characteristics, clinical characteristics, and comorbidities.9–14 A meta-analysis of 60 studies involving 51,225 patients from various hospitals in 13 countries discovered a higher in-hospital fatality rate in elderly patients and people who smoke, as well as those with dyspnea and renal problems, high blood pressure, cancers, metabolic syndrome, and respiratory disease.15
Saudi Arabia has a distinct epidemiological structure, with a younger generation predominating. Saudi Arabia’s largest age range is 35–39 years.16 According to the most recent demographic survey conducted by the Saudi General Authority for Statistics, nearly fifty percent of the population was aged 25–54 years, with the age group of 35–39 years predominating.17 In addition to the risk variables, several lab tests were found to be linked to COVID-19 patient outcomes. Creatinine, raised C-reactive protein (CRP), reduced lymphocyte count and magnesium concentration upon admission, for example, are proposed as predictors of increased death in COVID-19.18 A recent study demonstrated that significantly increased CRP, white blood cell (WBC) count, neutrophil-to-lymphocyte ratio, and reduced prognostic nutritional index could be used as predictors for COVID-19 in-hospital fatality rate.19
One of the most critical aspects of COVID-19 management is the accurate and timely recognition of high-risk patients. Early risk stratification can aid in medical planning and allocating resources. As a result, the study was undertaken to analyze-selected variables in order to predict patient survival and non-survival characteristics in our cohort.
Materials and Methods
Study Design and Participants
A retrospective observational study was performed at East Jeddah Hospital, Jeddah, Kingdom of Saudi Arabia. Data from hospitalized patients with confirmed COVID-19 from April to August 2020 were collected. Infection with SARS-CoV-2 was confirmed by RT-PCR (Reverse Transcriptase Polymerase Chain Reaction) assay using nasopharyngeal or oropharyngeal swabs. Clinical and laboratory data measurements were available at admission. In the current study, a total of 108 patients were recruited and categorized into two groups based on outcome as survivors (n = 54) and non-survivors (n = 54).
Data Collection
Information from each patient was collected from the electronic health report system at hospital admission, including demographic characteristics (age and gender) and laboratory investigations including white blood cells, leukocyte subtypes, platelets, and red blood cells (RBCs) counts; hemoglobin; activated Partial Thromboplastin Time (PTT) and prothrombin time (PT). Hematological parameters were assessed using a fully automated hematology analyzer (Sysmex XN- 1000 - Japan).
Statistical Analysis
Continuous variables were summarized as median (IQR) and categorical variables as absolute frequency (relative frequency, %). Summary statistics were performed for the whole cohort and grouping patients in survivors and non-survivors. Differences between the two groups were evaluated using Mann–Whitney U-test for quantitative variables and χ2 test or Fisher’s exact test for categorical variables. Statistical inference was performed using two-tailed test and with type I error rate of 0.05. All statistical analyses were performed using Graph Pad Prism software (version 10.0.1).
Ethical Approval
The study was conducted in accordance with the Declaration of Helsinki and ethical approval was obtained from the Jeddah Institute Review Board (approval number: H-02-J-002/1268). Informed consent was waived due to the retrospective nature of the study and the analysis used anonymous clinical data.
Results
Demographics and Clinical Characteristics
The demographic and clinical characteristics of the participants are shown in Table 1. A total of 108 patients with laboratory confirmed COVID-19 and admitted to hospital from April to August 2020 were enrolled in this study, 86 (79.63%) were males and 22 (20.37%) were females. Patients were admitted to hospital with symptoms including fever, cough, and shortness of breath. Out of the 108 patients, 54 patients died during the study period. The non-survived group comprises 44 (81.48%) males and 10 (18.52%) patients were females. The survived group comprises 42 (77.78%) males and 12 patients (22.22%) were females. The mean age and standard deviation of the survived (30–71 years) and non-survived (33–83) groups was 53 ± 10.8 and 57.9 ± 12.2 years, respectively, with no statistically significant difference in age between groups (p = 0.0513). The median hospital length of stay was not statistically different between survived (10 days, IQR: 5 to 15) and non-survived (9 days, IQR: 7 to 14) patients (p = 0.751). Furthermore, 31 (56.6%) and 52 (96.4%) of the survived and non-survived groups, respectively, were admitted to the ICU (Table 1). The median length of stay in ICU was higher among non-survived (7 days, IQR: 4.24 to 12) compared to survived (5 days, IQR: 0 to 11.75) patients (p = 0.0151). Correlation analysis revealed that age was not correlated with the length of hospital stay (r(52)= 0.0005, p = 0.8112) and length of ICU admission (r(52)=.017, p = 0.17) for the non-survived but positively correlated with the length of hospital stay (r(52)= 0.21, p = 0.0005) and ICU length of stay r(52)= 0.18, p = 0.001) for the survived group. Increases in age of survived participants with COVID-19 were correlated with increases in length of stay in hospital and ICU stay.
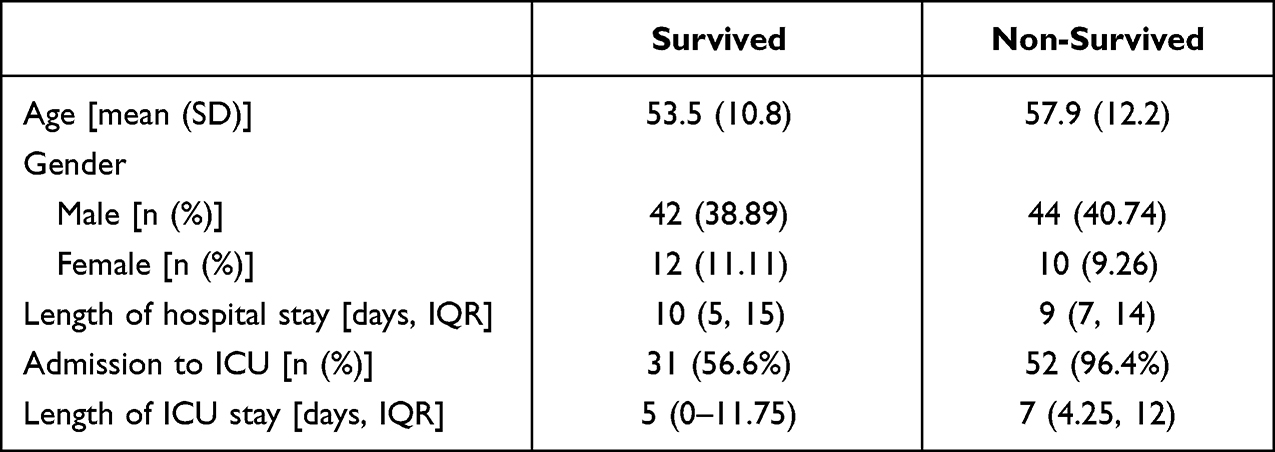 |
Table 1 Demographics and Clinical Characteristics of COVID-19 Survived and Non-Survived Participants |
Red Blood Cells Indices
A comparison of the median RBC parameters for the survived and non-survived groups is shown in Table 2 and Supplementary Figure S1. The median red blood cells (RBCs) counts were significantly higher in the survived group (4.56x109/L, IQR: 4.02 to 5.11) in comparison with the non-survived (4.23x109/L, IQR: 3.75 to 4.23) group (p=0.0011). The hemoglobin (HGB) values were not statistically different between the survived (13.3 gm/dl, IQR: 11.2 to 14.35) and non-survived (12.7 gm/dl, IQR: 11.45 to 13.55) groups (p=0.3704). Likewise, hematocrit (HCT) values were not significantly different between the survived (39.05%, IQR: 34.90 to 42.55) and non-survived (37.95%, IQR: 34.28 to 40.50) groups (p=0.1767).
 |
Table 2 Hematological Parameters Among COVID-19 Survived and Non-Survived Participants (Values in Parentheses in the First Column Represent Normal Range) |
Serum Ferritin Level
There was no statistically significant difference in serum ferritin level between the survived (874, IQR: 636.2 to 1536.3) and non-survived (1560, IQR: 838 to 2524) groups (p=0.1767) (Table 2).
Leukocytes Parameters
WBCs were significantly reduced in the non-survived group (8.5×109/L, IQR: 6.1 to 11.7) compared to the survived (10.2×109/L, IQR: 7.4 to 16.7) group (p = 0.0477) (Table 2, see also Supplementary Figure S2 that shows box-whisker plots for various leukocytes parameters). In addition, the laboratory results demonstrated no significant difference in neutrophils between the survived (83.9%, IQR: 72.7 to 89.3) and non-survived (81%, IQR: 73.9 to 84) groups (p=0.0929). Laboratory test results demonstrated lymphocytopenia for all COVID-19 infected patients with no statistically significant difference between the survived (9.4%, IQR: 5.1 to 14.7) and non-survived (11%, IQR: 8 to 14.8) groups (p=0.4870). The percentage of eosinophils was not statistically significantly different between the survived (0.40%, IQR: 0.01 to 1.67) and non-survived (0.15%, IQR: 0.02 to 0.68) groups (p=0.2008). With regards to basophils, the non-survived group (0.09%, IQR: 0.02 to 0.19) demonstrated significant reduction in basophils compared to survived (0.20%, IQR: 0.02 to 0.19) group (p=0.0047). Additionally, there was no statistically significant differences in monocytes between survived (5%, IQR: 2.9 to 8.5) and non-survived (5.7%, IQR: 4 to 7) groups (p=0.1649).
Coagulation Profile of COVID-19 Survivors and Non-Survivors
There was no statistically significant difference in platelet count between survived (266.1x109/L±132.5) and non-survived (248x109/L ±95.7) patients (p = 0.4164) (Table 2 and Supplementary Figure S3). A statistically significant difference was found between the survived and non-survived groups regarding PT (12.5 sec. vs 14 sec., p<0.0001) and PTT (31.8 sec. vs 40 sec., p=0.0008) (Table 2 and Supplementary Figure S3).
Correlation Between Lymphocytes and Hospital and ICU Stay
Correlation analysis was conducted to assess the association of hematological profiles with the length of stay in hospital and ICU between survived (Figure 1A and C) and non-survived (Figure 1B and D) COVID-19 patients. There was significant negative correlation between the lymphocyte values and length of hospital stay among the survived group (p < 0.001) but not for the non-survived group (p = 0.1863). There was a significant weak negative correlation between the lymphocyte values and length of ICU stay among the survived group (p < 0.0480) but not the non-survived group (p = 0.395).
 |
Figure 1 Correlation between Lymphocytes Percentage and Duration of Hospital and Intensive Care Unit (ICU) Stay among Survived (A and C) and Non-survived (B and D) COVID-19 Patients. |
Discussion
Since the start of the COVID-19 pandemic, most of the world’s population has been affected either directly or indirectly. The effects have ranged from psychological, economic or direct effects of infection with SARS CoV-2, often with adverse outcomes.20,21 The pandemic posed numerous challenges to hospital setups worldwide due to factors ranging from the rapid spread of a highly transmissible novel coronavirus, a fairly high admission rate of infected patients in hospitals within the first few months of the pandemic and a range of symptoms due to COVID-19 and complications from pre-existing conditions.22,23
Early studies assessed clinical, demographic, and hematological indicators in the COVID-19 outbreak. Our study retrospectively investigated hematological parameters such as RBCs, platelets, and WBCs of 108 patients admitted to East Jeddah Hospital, Jeddah, Saudi Arabia during the initial phase of the pandemic. Demographic and clinical data from these patients, including hematological parameters, were analyzed to understand prognosis and determinants of outcomes in critically ill patients admitted to the ICU. Out of the total patients admitted to the hospital, the majority were males (79.36%). In addition, of the total patients investigated, 50% died due to COVID-19 disease or its complications. A possible reason for the increased death rate in this study group may be that the patients who reached the hospital were already in a critical state. Due to the fear of hospital environments at the start of the pandemic and the stigma of infection, many patients with less severe symptoms preferred to stay home. Moreover, individuals with mild symptoms were instructed to take medication by doctors and recover at home. Most hospitals were unable to admit all COVID-19 cases due to an unprecedented burden on health care facilities.24 Patients of higher age and with pre-existing chronic health conditions were at an increased risk of fatal disease outcome. These findings are consistent with the previous studies.25–31
Of the 108 hospitalized patients, 83 patients were admitted to the ICU. It was observed that patients who died in hospital spent more days in ICU as compared to the patients who survived. A study showed that the COVID-19 ICU mortality ranged from 20% to 62% around the world.3
Lymphocytopenia was a major hematological abnormality observed in patients hospitalized with severe COVID-19.32 Anemia due to hemolysis was an important independent predictor of the severity of COVID-19 disease.33,34 RBCs can be lysed during infections such as sepsis.35 COVID-19 spike proteins and complement activation products were observed on RBC membranes in COVID-19 patients, affecting the RBCs structure and function.36 This may lead to decreased RBC numbers which was also observed in patients in our study.34 However, the decrease in hemoglobin levels was non-significant.
To understand disease severity in light of increased rates of RBS breakdown, coagulation factors in patients require analysis. Commonly used laboratory tests for exogenous and endogenous coagulating system factors such as DD, PT, and PTT were used for early diagnosis of disseminated intravascular coagulation, associated with severe COVID-19.37 Significantly higher levels of PT and PTT levels were observed in patients who died in hospital due to severe COVID-19. This showed a significant correlation between coagulating factors and disease outcome, suggesting diagnostic value of such markers in predicting disease progression and severity.
Hematological parameters such as HGB, HTC, platelets serum ferritin, neutrophils, lymphocytes, monocytes and eosinophil counts did not show any statistical differences between survived and non-survived patients in our study. However, both groups exhibited lower levels of platelets.38 The levels of ferritin, an inflammatory indicator studied in COVID-19 patients, was found to increase many-fold in critically ill COVID-19 patients.39
In severe cases of COVID-19 disease, an excessive immune response called the cytokine storm is generated against the virus, together with increased levels of lymphocytes.40 These cells have a crucial role in cell immunity. Some studies suggest that lymphocytes were found to significantly decrease in COVID-19 patients compared to healthy individuals.38 These findings are similar to our results. However, no significant differences were observed in lymphocyte levels between both survived and non-survived groups. Furthermore, the numbers of neutrophils, eosinophils, and basophils were significantly reduced in critically ill COVID-19 patients.38 Similar patterns of reduction were observed in our study. However, only basophil counts differed significantly between survived and non-survived groups.
Limitation and Future Studies
Sample size was small due to non-availability of complete clinical data and was conducted at a single-center in Jeddah, Saudi Arabia which may limit external validity. Further multicenter studies with larger samples size are required in Saudi Arabia to highlight any potential demographic variability that might exist. History of pre-existing comorbid conditions and treatment regimen, which might have influenced clinical and hematological parameters, were not available. Data with more clinical parameters may provide more accurate and specific predictive indications for outcomes for COVID-19 patients admitted to hospitals.
Conclusion
The current study showed that RBC levels, WBC, coagulation factors (PT and PTT) and basophil levels are predictive markers for the survival of COVID-19 patients in the Saudi population. Such alterations in hematological parameters are common in patients with severe COVID-19 disease and could be used as potential biomarkers for cases requiring hospitalization. Demographic data, clinical tests and hematological characterizations are crucial predictors of disease progression and outcomes, enabling development of strategy for improved treatment and diagnostics.
Acknowledgments
This research has been funded by Deanship of Scientific Research at University of Ha’il-Saudi Arabia through project number RG-21111. We would like to thank the patients for their participation and health care providers who assisted in data collection. Portions of this research were presented at the XXXVth International Symposium on Technical Innovations in Laboratory Hematology in New Orleans, Louisiana.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. WHO coronavirus (COVID-19) dashboard. Available from: https://covid19.who.int/.
2. Yu N, Li W, Kang Q, et al. Clinical features and obstetric and neonatal outcomes of pregnant patients with COVID-19 in Wuhan, China: a retrospective, single-centre, descriptive study. Lancet Infect Dis. 2020;20(5):559–564. doi:10.1016/S1473-3099(20)30176-6
3. Bhatraju PK, Ghassemieh BJ, Nichols M, et al. Covid-19 in critically ill patients in the Seattle region - case series. N Engl J Med. 2020;382:2012–2022. doi:10.1056/NEJMoa2004500
4. Leticia de oliveira toledo S, Sousa Nogueira L, Das Gracas Carvalho M, Romana Alves Rios D, de Barros Pinheiro M. COVID-19: review and hematologic impact. Clin Chim Acta. 2020;510:170–176. doi:10.1016/j.cca.2020.07.016
5. Samprathi M, Jayashree M. Biomarkers in COVID-19: an Up-To-Date Review. Front Pediatr. 2020;8:607647. doi:10.3389/fped.2020.607647
6. Adab P, Haroon S, O’Hara ME, Jordan RE. Comorbidities and covid-19. BMJ. 2022;377:o1431. doi:10.1136/bmj.o1431
7. Cataudella E, Giraffa CM, Di marca S, et al. Neutrophil-to-lymphocyte ratio: an emerging marker predicting prognosis in elderly adults with community-acquired pneumonia. J Am Geriatr Soc. 2017;65:1796–1801. doi:10.1111/jgs.14894
8. Merekoulias G, Alexopoulos EC, Belezos T, Panagiotopoulou E, Jelastopulu DM. Lymphocyte to monocyte ratio as a screening tool for influenza. PLoS Curr. 2010;2:RRN1154. doi:10.1371/currents.rrn1154
9. Angelidi AM, Belanger MJ, Mantzoros CS. Commentary: COVID-19 and diabetes mellitus: what we know, how our patients should be treated now, and what should happen next. Metabolism. 2020;107:154245. doi:10.1016/j.metabol.2020.154245
10. Bonow RO, Fonarow GC, O’Gara PT, Yancy CW. Association of coronavirus disease 2019 (COVID-19) with myocardial injury and mortality. JAMA Cardiol. 2020;5(7):751–753. doi:10.1001/jamacardio.2020.1105
11. Guo T, Fan Y, Chen M, et al. Cardiovascular implications of fatal outcomes of patients with coronavirus disease 2019 (COVID-19). JAMA Cardiol. 2020;5(7):811–818. doi:10.1001/jamacardio.2020.1017
12. Kanne JP. Chest CT findings in 2019 Novel coronavirus (2019-nCoV) infections from Wuhan, china: key points for the radiologist. Radiology. 2020;295(1):16–17. doi:10.1148/radiol.2020200241
13. Mehraeen E, Karimi A, Barzegary A, et al. Predictors of mortality in patients with COVID-19–a systematic review. Eur J Integr Med. 2020;40:101226. doi:10.1016/j.eujim.2020.101226
14. Tian W, Jiang W, Yao J, et al. Predictors of mortality in hospitalized COVID-19 patients: a systematic review and meta-analysis. J Med Virol. 2020;92(10):1875–1883. doi:10.1002/jmv.26050
15. Mesas AE, Cavero-Redondo I, Alvarez-Bueno C, et al. Predictors of in-hospital COVID-19 mortality: a comprehensive systematic review and meta-analysis exploring differences by age, sex and health conditions. PLoS One. 2020;15(11):e0241742. doi:10.1371/journal.pone.0241742
16. General Authority for Statistics. Demography in Saudi Arabia; 2020. Available from: https://www.stats.gov.sa/sites/default/files/Population%20by%20Age%20Groups%20%2Cand%20Gender_0.pdf.
17. General Authority for Statistics. General authority for statistics demographic survey. population by age groups, and gender mid year 2019. Available from: https://www.stats.gov.sa/sites/default/files/population_by_age_groups_and_gender_ar.pdf.
18. Alamdari NM, Afaghi S, Rahimi FS, et al. Mortality risk factors among hospitalized COVID-19 patients in a major referral center in Iran. Tohoku J Exp Med. 2020;252(1):73–84. doi:10.1620/tjem.252.73
19. Doganci S, Ince ME, Ors N, et al. A new COVID-19 prediction scoring model for in-hospital mortality: experiences from Turkey, single center retrospective cohort analysis. Eur Rev Med Pharmacol Sci. 2020;24(19):10247–10257. doi:10.26355/eurrev_202010_23249
20. Sherwani S, Raafat M, Rajendrasozhan S, et al. Increased levels of autoantibodies against ROS-modified proteins in depressed individuals with decrease in antibodies against SARS-CoV-2 antigen (S1-RBD). Curr Issues Mol Biol. 2022;44(11):5260–5276. doi:10.3390/cimb44110358
21. Wilson JM, Lee J, Fitzgerald HN, Oosterhoff B, Sevi B, Shook NJ. Job insecurity and financial concern during the COVID-19 pandemic are associated with worse mental health. J Occup Environ Med. 2020;62(9):686–691. doi:10.1097/JOM.0000000000001962
22. Alyami MH, Naser AY, Orabi MAA, Alwafi H, Alyami HS. Epidemiology of COVID-19 in the Kingdom of Saudi Arabia: an ecological study. Front Public Health. 2020;8:506. doi:10.3389/fpubh.2020.00506
23. Birkmeyer JD, Barnato A, Birkmeyer N, Bessler R, Skinner J. The impact of the COVID-19 pandemic on hospital admissions in the United States. Health Aff. 2020;39(11):2010–2017. doi:10.1377/hlthaff.2020.00980
24. Kim Y, Gandhi RT. COVID-19: management in hospitalized adults. Available from: https://www.uptodate.com/contents/covid-19-management-in-hospitalized-adults.
25. Alharthy A, Aletreby W, Faqihi F, et al. Clinical characteristics and predictors of 28-day mortality in 352 critically ill patients with COVID-19: a retrospective study. J Epidemiol Glob Health. 2020;11(1):98–104. doi:10.2991/jegh.k.200928.001
26. Baena-Diez JM, Barroso M, Cordeiro-Coelho SI, Diaz JL, Grau M. Impact of COVID-19 outbreak by income: hitting hardest the most deprived. J Public Health. 2020;42(4):698–703. doi:10.1093/pubmed/fdaa136
27. Grasselli G, Zangrillo A, Zanella A, et al. Baseline characteristics and outcomes of 1591 patients infected with SARS-CoV-2 admitted to ICUs of the Lombardy Region, Italy. JAMA. 2020;323(16):1574–1581. doi:10.1001/jama.2020.5394
28. Vila-Corcoles A, Satue-Gracia E, Vila-Rovira A, de Diego-Cabanes C, Forcadell-Peris MJ, Ochoa-Gondar O. Development of a predictive prognostic rule for early assessment of COVID-19 patients in primary care settings. Aten Primaria. 2021;53(9):102118. doi:10.1016/j.aprim.2021.102118
29. Wang Z, Wang Z. Identification of risk factors for in-hospital death of COVID - 19 pneumonia -- lessions from the early outbreak. BMC Infect Dis. 2021;21(1):113. doi:10.1186/s12879-021-05814-4
30. Yang J, Zheng Y, Gou X, et al. Prevalence of comorbidities and its effects in patients infected with SARS-CoV-2: a systematic review and meta-analysis. Int J Infect Dis. 2020;94:91–95. doi:10.1016/j.ijid.2020.03.017
31. Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395:1054–1062. doi:10.1016/S0140-6736(20)30566-3
32. Rahi MS, Jindal V, Reyes SP, Gunasekaran K, Gupta R, Jaiyesimi I. Hematologic disorders associated with COVID-19: a review. Ann Hematol. 2021;100:309–320. doi:10.1007/s00277-020-04366-y
33. Bellmann-Weiler R, Lanser L, Barket R, et al. Prevalence and predictive value of anemia and dysregulated iron homeostasis in patients with COVID-19 infection. J Clin Med. 2020;9. doi:10.3390/jcm9082429
34. Bouchla A, Kriebardis AG, Georgatzakou HT, et al. Red blood cell abnormalities as the mirror of SARS-CoV-2 disease severity: a pilot study. Front Physiol. 2021;12:825055. doi:10.3389/fphys.2021.825055
35. Bateman RM, Sharpe MD, Singer M, Ellis CG. The effect of sepsis on the erythrocyte. Int J Mol Sci. 2017;18. doi:10.3390/ijms18091932
36. Lam LKM, Reilly JP, Rux AH, et al. Erythrocytes identify complement activation in patients with COVID-19. Am J Physiol Lung Cell Mol Physiol. 2021;321:L485–L489. doi:10.1152/ajplung.00231.2021
37. Long H, Nie L, Xiang X, et al. D-dimer and prothrombin time are the significant indicators of severe COVID-19 and poor prognosis. Biomed Res Int. 2020;2020:6159720. doi:10.1155/2020/6159720
38. Gu X, Sha L, Zhang S, Shen D, Zhao W, Yi Y. Neutrophils and lymphocytes can help distinguish asymptomatic COVID-19 from moderate COVID-19. Front Cell Infect Microbiol. 2021;11:654272. doi:10.3389/fcimb.2021.654272
39. Kaushal K, Kaur H, Sarma P, et al. Serum ferritin as a predictive biomarker in COVID-19. A systematic review, meta-analysis and meta-regression analysis. J Crit Care. 2022;67:172–181. doi:10.1016/j.jcrc.2021.09.023
40. Sherwani S, Khan MWA. Cytokine response in SARS-CoV-2 infection in the elderly. J Inflamm Res. 2020;13:737–747. doi:10.2147/JIR.S276091
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
COVID-19 and Saudi Arabia: Awareness, Attitude, and Practice
Fawzy MS, AlSadrah SA
Journal of Multidisciplinary Healthcare 2022, 15:1595-1618
Published Date: 26 July 2022
Comparison of the Diagnostic Performance of a Rapid Antigen Test with Real-Time Polymerase Chain Reaction for Detection of SARS-CoV-2 Among Patients Diagnosed with COVID-19 at Selected Hospitals in Addis Ababa, Ethiopia
Desalegn Z, Sebre S, Yohannes M, Seman A, Shiferaw W, Ademe M, Biazin H, Firdawoke E, Asemamaw Y, Teka B, Teshome S, Amogne W, Addissie A, Gebrehiwot Y, Kantelhardt E, Abebe T
Infection and Drug Resistance 2022, 15:4299-4305
Published Date: 6 August 2022
A Pilot Study of 0.4% Povidone-Iodine Nasal Spray to Eradicate SARS-CoV-2 in the Nasopharynx
Sirijatuphat R, Leelarasamee A, Puangpet T, Thitithanyanont A
Infection and Drug Resistance 2022, 15:7529-7536
Published Date: 21 December 2022
Distinct Features of Vascular Diseases in COVID-19
Ceasovschih A, Sorodoc V, Shor A, Haliga RE, Roth L, Lionte C, Onofrei Aursulesei V, Sirbu O, Culis N, Shapieva A, Tahir Khokhar MA, Statescu C, Sascau RA, Coman AE, Stoica A, Grigorescu ED, Banach M, Thomopoulos C, Sorodoc L
Journal of Inflammation Research 2023, 16:2783-2800
Published Date: 6 July 2023
Re-Emerging COVID-19: Controversy of Its Zoonotic Origin, Risks of Severity of Reinfection and Management
Chala B, Tilaye T, Waktole G
International Journal of General Medicine 2023, 16:4307-4319
Published Date: 20 September 2023