Back to Journals » International Journal of General Medicine » Volume 16
Comparison of Dydrogesterone and GnRH-a Effects After Laparoscopic Surgery in Patients with Stage III and IV Endometriosis
Authors Deng T, Lin Y, Chen L, Jiang JY
Received 11 July 2023
Accepted for publication 14 September 2023
Published 25 September 2023 Volume 2023:16 Pages 4357—4364
DOI https://doi.org/10.2147/IJGM.S429953
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Woon-Man Kung
Ting Deng, Yin Lin, Li Chen, Jun-Ying Jiang
Department of Obstetrics and Gynecology, Fujian Maternity and Child Health Hospital, College of Clinical Medicine for Obstetrics & Gynecology and Pediatrics, Fujian Medical University, Fuzhou, 350001, People’s Republic of China
Correspondence: Jun-Ying Jiang, Email [email protected]
Objective: To compare the spontaneous pregnancy rates between dydrogesterone and Gonadotropin-releasing hormone agonist (GnRH-a) treatments in patients with endometriosis stage III and IV after laparoscopy.
Methods: The clinical data of patients with endometriosis stage III and IV administered laparoscopic surgery in our hospital from January 2018 to March 2020 were retrospectively analyzed. Totally 151 cases were divided into two groups according to postoperative medication, including the study (70 cases) and control (81 cases) groups treated with dydrogesterone and GnRH-a, respectively. The spontaneous pregnancy and subsequent pregnancy outcomes were assessed within 12 months.
Results: Totally 49 patients had spontaneous pregnancy. Among them, there were 31 cases in the dydrogesterone group (spontaneous pregnancy rate of 44.3%, 31/70), including 25 live birth cases (35.7%, 25/70), 4 miscarriage cases, and 2 ectopic pregnancy cases. The time to conception was 1– 10 months (median value of 5 months). Totally 18 cases in the GnRH-a group had spontaneous pregnancy (22.2%, 18/81), including 16 live birth cases (19.8%, 16/81). 81) and 2 miscarriage cases; the time to conception was 3– 11 months (median value of 6 months). There were significant differences in spontaneous pregnancy rate and cumulative spontaneous pregnancy rate between the two groups (P = 0.005 and 0.003, respectively).
Conclusion: Dydrogesterone after laparoscopic surgery in patients with endometriosis stage III and IV improved the natural pregnancy rate.
Keywords: endometriosis, laparoscopic surgery, dydrogesterone, gonadotropin-releasing hormone agonist, spontaneous pregnancy
Introduction
Endometriosis, an estrogen-dependent disease that causes multiple symptoms, including pain and infertility, is a complex chronic gynecological disease affecting female reproductive potential. Approximately 10% of women in their reproductive years suffer from endometriosis, amounting to an estimated 176 million women in the world have endometriosis, with a prevalence of 20% to 50% of infertile women. At present, endometriosis treatment options mainly include surgery and drug treatment. However, due to the various conditions of different patients, the postoperative recurrence rate is high, while the postoperative pregnancy rate is low.1–3 How to improve the pregnancy rate while effectively managing disease recurrence after surgery has become an urgent clinical problem. For patients with stage III–IV endometriosis, several cycles of GnRH-a therapy are administered after surgery to reduce residual lesions and delay or prevent recurrence. However, these drugs cannot meet the pregnancy needs of patients with endometriosis due to substantially inhibited ovarian function, suppressed ovulation, and delayed conception. Dydrogesterone has been shown to relieve endometriosis symptoms, shrink lesions, and improve pregnancy rates in infertile patients.4,5 However, limited clinical data are available to support the improvement of postoperative pregnancy outcomes in patients with moderate-to-severe endometriosis desiring pregnancy. This study analyzed the clinical data of patients with stage III-IV endometriosis in our center retrospectively and explored spontaneous pregnancy outcomes after dydrogesterone and GnRH-a treatments following laparoscopic surgery, in order to provide a better understanding of postoperative outcomes after laparoscopic surgery. Our findings provide a reference for the treatment of endometriosis patients with natural pregnancy needs.
Materials and Methods
Data Sources
The medical records of Fujian Maternity and Child Health Hospital were reviewed, and the clinical data of patients with pelvic endometriosis diagnosed by laparoscopic surgery in our hospital from January 2018 to March 2020 were analyzed. The subsequent spontaneous pregnancy outcomes of the patients were followed up by face-to-face consultation, consulting the medical record system of our hospital, telephone or WeChat. Endometriosis diagnosis was confirmed by laparoscopy and pathology. Inclusion criteria were: (1) stage III-IV endometriosis confirmed by laparoscopic surgery and pathological examination; (2) 18–38 years of age, normal menstrual cycle, and normal preoperative anti-Müllerian hormone (AMH); (3) postoperative spontaneous pregnancy requirements; (4) postoperative treatment with dydrogesterone or GnRH-a. Exclusion criteria were: (1) use of hormone drugs within 3 months before operation; (2) previous history of ovarian endometriosis cyst surgery before this operation.; (3) bilateral tubal obstruction; (4) intramural uterine fibroids larger than 4 cm or intraoperative myomectomy; (5) combination with intrauterine adhesions and malformations of reproductive organs; (6) abnormal male semen examination; (7) postoperative assisted reproduction; (8) incomplete clinical data or loss of visitors. Totally 151 patients were included in this study, which was approved by the ethics committee of our hospital (2018 Approval No.155), and all patients provided signed informed consent.
Methods
Grouping
Totally 151 patients with endometriosis were treated by laparoscopic ovarian endometriosis cystectomy and tubal patency after hysteroscopy. According to the different drugs used after operation, the patients were divided into the dydrogesterone (70 cases) and GnRH-a (81 cases) groups. Intraoperative staging was performed according to the American Fertility Society’s 1985 revised staging criteria for endometriosis (r-AFS). The general data of the two groups were recorded, including age, body mass index (BMI), parity, infertility, dysmenorrhea, preoperative serum CA125 levels, maximum diameter of endometriomas, side of endometriomas, uterine cavity depth, preoperative uterine rectal fossa patency, and r-AFS stage.
Surgical Method
All patients were operated within 3–7 days after menstruation. Surgery was performed under general anesthesia with tracheal intubation, and staging was performed according to the r-AFS standard. The operative method and scope were as follows. (1) Ovarian endometriosis cystectomy: puncture and cyst fluid aspiration, cyst wall stripping from the ovary, ovarian wound suture to stop bleeding or low power spot electrocoagulation to stop bleeding. Attention should be paid to ovarian function protection, and the damage to normal ovarian tissue should be avoided as far as possible. (2) Lysis of pelvic adhesions and electrocoagulation of endometriosis: blunt and sharp separation of pelvic adhesions to restore the normal anatomical structure of the pelvis; electrocoagulation and cauterization of lesions with obvious pigmentation. (3) Tubal plastic surgery in patients with tubal adhesions or lesions: the adhesions around the fallopian tube were bluntly and sharply separated, and salpingostomy was performed in case of atresia. (4) Hysteroscopy was performed to remove or exclude intrauterine lesions; intubation was performed in the interstitial part of both fallopian tubes, and diluted methylene blue solution was injected to revealed the patency of fallopian tubes. If hysteroscopic catheterization and hydrotubation effect were not ideal after hysteroscope withdrawal, a double-lumen tube was placed in the uterine cavity, and diluted methylene blue solution was injected. The patency of the fallopian tube was observed under laparoscopy. At the end of the operation, the pelvic and abdominal cavities were washed repeatedly with a large amount of normal saline until a clear washing fluid was obtained.
Postoperative Treatment
In the dydrogesterone group, patients began to take oral dydrogesterone (Abbott Biologicals B. V) twice a day at 10 mg each time for 14 days in the second half of the menstrual cycle the month after operation, and continued until 8–10 weeks after pregnancy if it occurred during the follow-up period (twice a day at 10 mg each time). The GnRH-a group received GnRH-a from the 2nd to 3rd day after operation (3.75 mg Diphereline by Ipsen Pharma Biotech, 3.75 mg Enantone by Takeda Pharmaceutical Company Limited, or 3.6 mg Zoladex by AstraZeneca), and intramuscular or subcutaneous injection according to the drug instructions (1 dose every 4 weeks, for a total of 3 doses).
Observation Indexes and Definitions
Spontaneous pregnancy outcome during follow-up. The dydrogesterone group was observed until 12 months after the first menstruation. The GnRH-a group was observed until 12 months after the first menstruation following the withdrawal of the third dose; if pregnancy occurred during the observation period, they were followed up until pregnancy termination. The time of conception was defined as the time from the first menstruation after operation, assessed by “month”. Pregnancy was defined as a clinical pregnancy, in which the gestational sac was observed in the uterine cavity on early ultrasound. Live birth was defined as natural delivery and cesarean section with pregnancy ≥ 28 weeks, with newborns surviving at birth. Abortion was defined as pregnancy termination with pregnancy below 28 weeks. Ectopic pregnancy was defined as a pregnancy outside the uterine cavity.
Statistical Methods
SPSS25.0 was used for statistical analysis. Measurement data was expressed as Mean ± SD. The mean values were compared by the independent samples T and Wilcoxon signed rank sum tests for data with normal and skewed distributions, respectively. Enumeration data were expressed as number and percentage, and were compared by the Wilcoxon signed rank test. The Chi-square test was performed to compare postoperative spontaneous pregnancy rates. Kaplan-Meier survival analysis was performed to compare the cumulative spontaneous pregnancy rate after surgery. P < 0.05 was considered statistically significant.
Results
General Patient Information
There were no significant differences in general data between the two groups (P > 0.05), as shown in Table 1.
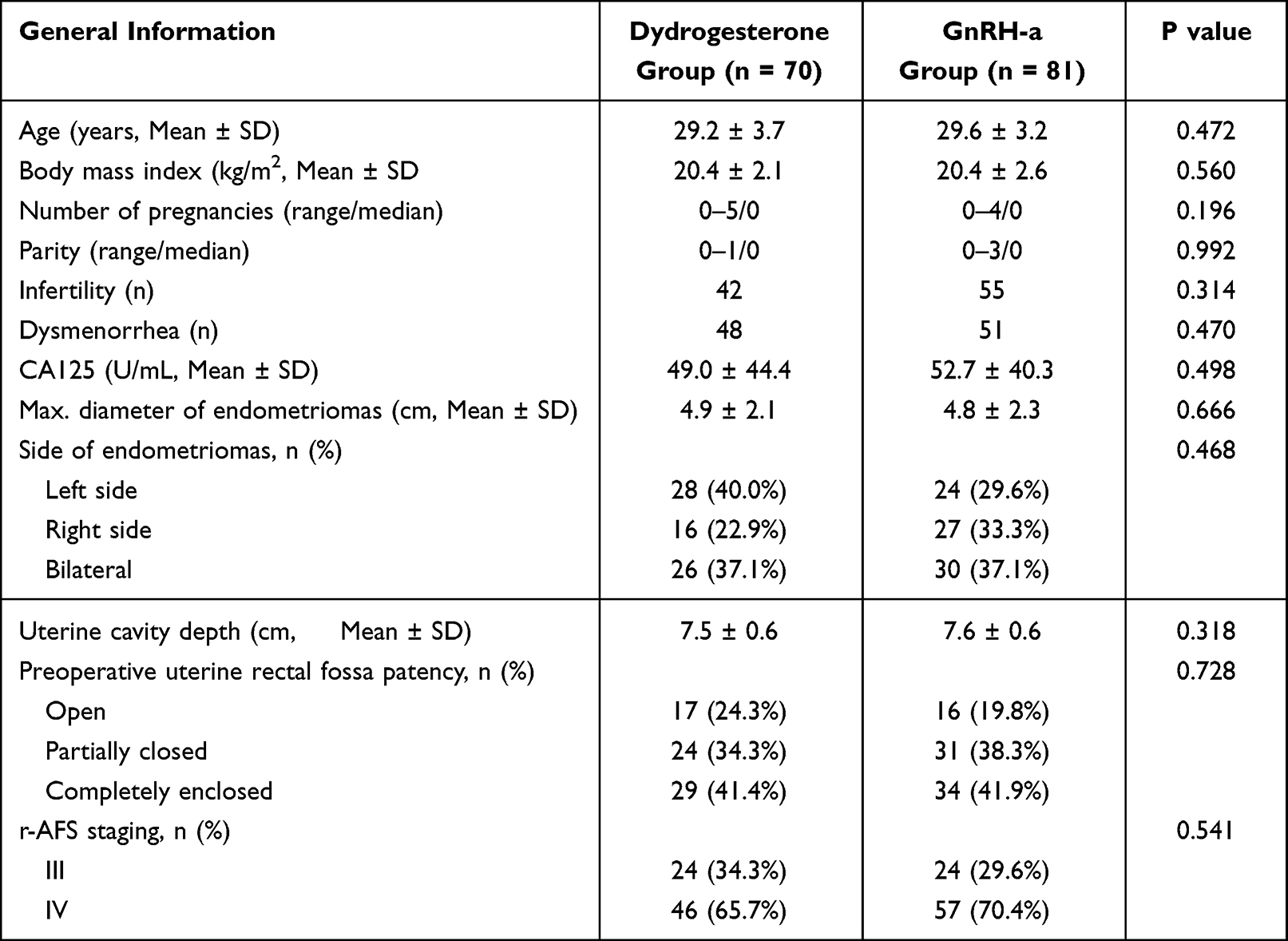 |
Table 1 General Patient Data |
Spontaneous Pregnancy Outcomes of the Two Groups After Operation
There were 49 spontaneous pregnancies during the 12 months of follow-up. In the dydrogesterone group, the spontaneous pregnancy rate was 44.3% (31/70), including 25 live births, 4 abortions, and 2 ectopic pregnancies; the median time to conception was 5 months (range, 1–10 months). In the GnRH-a group, the spontaneous pregnancy rate was 22.2% (18/81), including 16 live births and 2 abortions; the median time to conception was 6 months (range, 3–11 months). There were significant differences in spontaneous pregnancy rates (P = 0. 005), as shown in Table 2.
 |
Table 2 Spontaneous Pregnancy Rates in the Two Groups |
Postoperative Cumulative Spontaneous Pregnancy Rates
According to Kaplan-Meier analysis, the conception rate was higher in the dydrogesterone group compared with the GnRH-a group, and cumulative spontaneous pregnancy rates were statistically different (P = 0.003, Figure 1).
 |
Figure 1 Cumulative spontaneous pregnancy rates in both groups. |
Discussion
Endometriosis is a common and rarely treated disease in women of childbearing age. Its primary clinical manifestations are progressive dysmenorrhea, dyspareunia, pelvic pain and infertility. The exact prevalence of endometriosis is unknown, but approximately 10% to 15% of women of reproductive age are affected, with a morbidity as high as 35% to 50% in women with pelvic pain or infertility. Endometriosis is a complex chronic gynecological disease affecting the female reproductive potential. Typically, endometriosis is classified into the peritoneal, ovarian (ovarian endometriotic cysts) and deep types according to lesion type and location. Data on the prevalence of ovarian endometriotic cysts are limited, but it is estimated that 17% to 44% of patients with endometriosis have ovarian endometriotic cysts.1–5
Current treatment options for endometriosis include surgery and/or medication. Laparoscopic resection of ovarian endometriosis cysts is the first choice over abdominal surgery. Laparoscopic surgery has advantages in terms of complications, postoperative pain, length of hospital stay and cost.1 In 2014, the American Society for Reproductive Medicine guidelines firstly proposed that endometriosis should be treated with drugs to the maximum extent possible and avoid repeated surgery; in addition, short-term temporary medication regimen should be avoided, emphasizing lifelong management for the purpose of preventing recurrence.6 Medications play a key role in the long-term treatment of endometriosis, usually referred to as hormone therapy that suppresses ovarian function. These include combination hormonal contraceptives, progestins, gonadotropin-releasing hormone agonists, and gonadotropin-releasing hormone antagonists.7 Postoperative administration of GnRH-a therapy atrophies the residual lesions and reduces the risk of recurrence of endometriosis-related pain and improves the patient’s quality of life.1,3 However, it should be noted that these protocols do not improve endometriosis-related infertility.8 Previous studies have shown 3–6 months of pre-cycle GnRH-a therapy increases pregnancy rates in patients with endometriosis requiring assisted reproduction. However, the use of GnRH-a also results in decreased endometrial receptivity.9 The 2018 French National College of Obstetricians and Gynaecologists (CNGOF) and 2022 European Society of Human Reproduction and Embryology (ESHER) guidelines do not recommend postoperative antigonadotrophic therapy for women with endometriosis and infertility (Grade A).1,3 Therefore, in women with fertility needs, the choice of drug treatment is very important, and the therapy should relieve symptoms without inhibiting ovulation or causing amenorrhea or other adverse reactions.10
Dydrogesterone is a progesterone derivative, which is structurally and pharmacologically similar to endogenous progesterone. As a selective progesterone receptor agonist, it has high selectivity for progesterone receptor, strong pro-gestational activity and high oral bioavailability, and is effective at relatively low doses to minimize side effects.11 Dydrogesterone has been used worldwide for almost 60 years.12 In the 1960s, dydrogesterone was firstly reported to be effective in the treatment of endometriosis and licensed for use in more than 100 countries worldwide.13,14 Dydrogesterone can relieve endometriosis symptoms, reduce pathological changes, and improve the pregnancy rate of infertility cases.15–18 A recent observational, open-label, prospective study also confirmed that dydrogesterone is an effective treatment option for endometriosis.19 Dydrogesterone does not inhibit normal endometrium or alter the natural progression of endometriosis, while causing ectopic endometrial atrophy.20 At a therapeutic dose of 30 mg daily, dydrogesterone does not inhibit ovulation, with normal menstruation during normative use. Compared with other progestins, dydrogesterone has relatively lower glucocorticoid and mineralocorticoid receptor antagonist activities, and associated side effects are rare.11,21,22
This study showed that the spontaneous pregnancy rate in the dydrogesterone group was 44.3% at 12 months after operation, which was significantly different from that of the control group (P = 0.005) and higher than reported in published studies.16,20,23 The cumulative pregnancy rate at 12 months was significantly higher in the dydrogesterone group than in the GnRH-a group (P = 0.003). The discrepancy may be explained by inclusion criteria differences between this and previous studies. The study population was young (18–38 years old) in this study, with normal ovarian function, good fallopian tube condition, normal male semen examination results, and dydrogesterone use until 8–10 weeks of pregnancy to maintain the luteal function of the ovary and support embryonic development. These conditions promote pregnancy continuation. Endometriosis infertility is affected by many factors, including embryo implantation failure caused by decreased endometrial receptivity.24 Progesterone has long been considered a key physiological factor in pregnancy implantation and maintenance.25 Studies have shown that progesterone and its metabolite 17α-hydroxyprogesterone are significantly associated with endometrial receptivity, and progesterone supplementation improves endometrial receptivity.26 Implantation failure and miscarriage are associated with luteal deficits. The maintenance of early pregnancy must depend on a functioning corpus luteum until the placenta begins to produce progesterone. Patients with pelvic endometriosis may be associated with luteal phase defect.27,28 Dydrogesterone supports the development of corpus luteum in vivo and reduces the abortion rate in women with threatened or recurrent abortion.29–31 Dydrogesterone regulates the immune status of the body, induces important T cell inhibitory response, inhibits NK cells, and plays a synergistic role with prostaglandin E2 (PGE2), with a significant clinical effect on recurrent abortion. It effectively increases the levels of hCG and related cellular immune factors (IL-4, IL-10, IL-6, IFN-γ, etc.) in patients with recurrent abortion.32,33 Endometriosis is also an immune dysfunction disease.34–36 We speculate that dydrogesterone may also improve the immune disorder status of patients with endometriosis, thereby improving the pregnancy rate.
There is limited data comparing the use of dydrogesterone and GnRH-a uses for spontaneous pregnancy in patients with endometriosis after surgery. The post-operative period is a crucial golden period for endometriosis patients desiring pregnancy. It is particularly important to choose a drug that does not inhibit ovulation for the treatment of endometriosis following laparoscopic surgery. Therefore, because dydrogesterone does not inhibit ovulation and can sustain pregnancy, it may be an excellent choice for long-term management of endometriosis.
This study had limitations. It was a retrospective study, and the choice of the regimen depended on physicians due to the lack of treatment consensus or guidelines. There may be a selection bias due to the experience of doctors. Additionally, the proportion of deep invasive endometriosis was not assessed. Due to the characteristics of the study population, the results are not generalizable. Regarding dydrogesterone, there are mainly two dosing regimens reported in existing studies, including the extended full-cycle regimen (from the 5th to the 25th day of the cycle, at 20–30 mg/day) and the second half-cycle regimen (from the 15th to the 25th day of the cycle, at 30 mg/day). There is currently no evidence to suggest which regimen is better. In the future, larger randomized controlled studies will be required.
Conclusions
The administration of dydrogesterone following laparoscopic surgery in patients diagnosed with endometriosis stage III and IV is associated with an enhancement in the rate of natural pregnancies.
Data Sharing Statement
The original contributions presented in the study are included in the article. Further inquiries can be directed to the corresponding authors.
Ethics Statement and Consent to Participate
Our research conformed to the Declaration of Helsinki. Our research protocol was approved by the Ethics Committee of Fujian Maternity and Child Health Hospital.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Collinet P, Fritel X, Revel-Delhom C, et al. Management of endometriosis: CNGOF/HAS clinical practice guidelines - Short version. J Gynecol Obstetrics Human Reproduction. 2018;47(7):265–274. doi:10.1016/j.jogoh.2018.06.003
2. Zondervan KT, Becker CM, Missmer SA. Endometriosis. N Engl J Med. 2020;382(13):1244–1256. doi:10.1056/NEJMra1810764
3. Becker CM, Bokor A, Heikinheimo O, et al. ESHRE guideline: endometriosis. Human Reproduction Open. 2022;2022(2):hoac009. doi:10.1093/hropen/hoac009
4. Shafrir AL, Farland LV, Shah DK, et al. Risk for and consequences of endometriosis: a critical epidemiologic review. Best Pract Res Clin Obstet Gynaecol. 2018;51:1–15. doi:10.1016/j.bpobgyn.2018.06.001
5. Kiesel L, Sourouni M. Diagnosis of endometriosis in the 21st century. Climacteric. 2019;22(3):296–302. doi:10.1080/13697137.2019.1578743
6. Practice Committee of the American Society for Reproductive Medicine. Treatment of pelvic pain associated with endometriosis: a committee opinion. Fertil Steril. 2014;101(4):927–935. doi:10.1016/j.fertnstert.2014.02.012
7. Vercellini P, Viganò P, Somigliana E, Fedele L. Endometriosis: pathogenesis and treatment. Nat Rev Endocrinol. 2014;10(5):261–275. doi:10.1038/nrendo.2013.255
8. Ferrero S, Evangelisti G, Barra F. Current and emerging treatment options for endometriosis. Expert Opin Pharmacother. 2018;19(10):1109–1125. doi:10.1080/14656566.2018.1494154
9. Iwami N, Kawamata M, Ozawa N, et al. New treatment strategy for endometriosis using progestin-primed ovarian stimulation with dienogest: a prospective cohort study, comparison of dienogest versus dydrogesterone. Reprod Biol. 2021;21(1):100470. doi:10.1016/j.repbio.2020.100470
10. Practice Committee of the American Society for Reproductive Medicine. Endometriosis and infertility: a committee opinion. Fertil Steril. 2012;98(3):591–598. doi:10.1016/j.fertnstert.2012.05.031
11. Griesinger G, Tournaye H, Macklon N, et al. Dydrogesterone: pharmacological profile and mechanism of action as luteal phase support in assisted reproduction. Reprod Biomed Online. 2019;38(2):249–259. doi:10.1016/j.rbmo.2018.11.017
12. Ott J, Egarter C, Aguilera A. Dydrogesterone after 60 years: a glance at the safety profile. Gynecol Endocrinol. 2022;38(4):279–287. doi:10.1080/09513590.2021.2016692
13. Schweppe KW. The place of dydrogesterone in the treatment of endometriosis and adenomyosis. Maturitas. 2009;65(Suppl 1):S23–7. doi:10.1016/j.maturitas.2009.11.011
14. Griesinger G, Blockeel C, Tournaye H. Oral dydrogesterone for luteal phase support in fresh in vitro fertilization cycles: a new standard? Fertil Steril. 2018;109(5):756–762. doi:10.1016/j.fertnstert.2018.03.034
15. Taylor PJ, Kredentser JV. Nonsurgical management of minimal and moderate endometriosis to enhance fertility. Int J Fertil. 1992;37(3):138–143.
16. Trivedi P, Selvaraj K, Mahapatra PD, Srivastava S, Malik S. Effective post-laparoscopic treatment of endometriosis with dydrogesterone. Gynecol Endocrinol. 2007;23(Suppl 1):73–76. doi:10.1080/09513590701669583
17. Liu S, Xin X, Hua T, et al. Efficacy of Anti-VEGF/VEGFR Agents on Animal Models of Endometriosis: a Systematic Review and Meta-Analysis. PLoS One. 2016;11(11):e0166658. doi:10.1371/journal.pone.0166658
18. Ceyhan ST, Onguru O, Fidan U, et al. Comparison of aromatase inhibitor (letrozole) and immunomodulators (infliximab and etanercept) on the regression of endometriotic implants in a rat model. Eur J Obstet Gynecol Reprod Biol. 2011;154(1):100–104. doi:10.1016/j.ejogrb.2010.09.003
19. Sukhikh GT, Adamyan LV, Dubrovina SO, Baranov II, Bezhenar VF. Prolonged cyclical and continuous regimens of dydrogesterone are effective for reducing chronic pelvic pain in women with endometriosis: results of the ORCHIDEA study. Fertil Steril. 2021;116(6):1568–1577. doi:10.1016/j.fertnstert.2021.07.1194
20. Overton CE, Lindsay PC, Johal B, et al. A randomized, double-blind, placebo-controlled study of luteal phase dydrogesterone (Duphaston) in women with minimal to mild endometriosis. Fertil Steril. 1994;62(4):701–707. doi:10.1016/s0015-0282(16)56991-x
21. Rižner TL, Brožič P, Doucette C, et al. Selectivity and potency of the retroprogesterone dydrogesterone in vitro. Steroids. 2011;76(6):607–615. doi:10.1016/j.steroids.2011.02.043
22. Trivedi N, Chauhan N, Vaidya V. Effectiveness and safety of dydrogesterone in regularization of menstrual cycle: a post-marketing study. Gynecol Endocrinol. 2016;32(8):667–671. doi:10.3109/09513590.2016.1152238
23. Makhmudova GM, Nazhmutdinova DK, Gafarova D, Lukmanova Iu D. Efektivnost na lechenieto s duphaston na zheni prekarali rekonstruktivno-plastichni operatsii pri endometrioza [Efficacy of duphaston treatment in women with endometriosis after reconstructive surgery]. Akusherstvo I Ginekologiia. 2003;42(4):42–46.
24. Miravet-Valenciano J, Ruiz-Alonso M, Gómez E, Garcia-Velasco JA. Endometrial receptivity in eutopic endometrium in patients with endometriosis: it is not affected, and let me show you why. Fertil Steril. 2017;108(1):28–31. doi:10.1016/j.fertnstert.2017.06.002
25. Nagy B, Szekeres-Barthó J, Kovács GL, et al. Key to Life: physiological Role and Clinical Implications of Progesterone. Int J Mol Sci. 2021;22(20):11039. doi:10.3390/ijms222011039
26. Labarta E, Sebastian-Leon P, Devesa-Peiro A, et al. Analysis of serum and endometrial progesterone in determining endometrial receptivity. Human Reproduction. 2021;36(11):2861–2870. doi:10.1093/humrep/deab184
27. Cahill DJ, Hull MG. Pituitary-ovarian dysfunction and endometriosis. Human reproduction update. Human Reproduction Update. 2000;6(1):56–66. doi:10.1093/humupd/6.1.56
28. Cunha-Filho JS, Gross JL, Bastos de Souza CA, et al. Physiopathological aspects of corpus luteum defect in infertile patients with mild/minimal endometriosis. J Assist Reprod Genet. 2003;20(3):117–121. doi:10.1023/a:1022625106489
29. Arab H, Alharbi AJ, Oraif A, et al. The Role Of Progestogens In Threatened And Idiopathic Recurrent Miscarriage. In j Women’s Health. 2019;11:589–596. doi:10.2147/ijwh.S224159
30. Lee HJ, Park TC, Kim JH, Norwitz E, Lee B. The Influence of Oral Dydrogesterone and Vaginal Progesterone on Threatened Abortion: a Systematic Review and Meta-Analysis. Biomed Res Int. 2017;2017:3616875. doi:10.1155/2017/3616875
31. Saccone G, Schoen C, Franasiak JM, Scott RT Jr, Berghella V. Supplementation with progestogens in the first trimester of pregnancy to prevent miscarriage in women with unexplained recurrent miscarriage: a systematic review and meta-analysis of randomized, controlled trials. Fertil Steril. 2017;107(2):430–438.e3. doi:10.1016/j.fertnstert.2016.10.031
32. Di Renzo GC, Giardina I, Clerici G, Brillo E, Gerli S. Progesterone in normal and pathological pregnancy. Horm Mol Biol Clin Investig. 2016;27(1):35–48. doi:10.1515/hmbci-2016-0038
33. Guo H, Lu Q. Efficacy of dydrogesterone on treating recurrent miscarriage and its influence on immune factors: a systematic review and meta-analysis. Ann Palliat Med. 2021;10(10):10971–10985. doi:10.21037/apm-21-2605
34. Vallvé-Juanico J, Houshdaran S, Giudice LC. The endometrial immune environment of women with endometriosis. Hum Reprod Update. 2019;25(5):564–591. doi:10.1093/humupd/dmz018
35. Agostinis C, Balduit A, Mangogna A, et al. Immunological Basis of the Endometriosis: the Complement System as a Potential Therapeutic Target. Front Immunol. 2020;11:599117. doi:10.3389/fimmu.2020.599117
36. Matteo M, Cicinelli E, Neri M, et al. Pro-inflammatory M1/Th1 type immune network and increased expression of TSG-6 in the eutopic endometrium from women with endometriosis. Eur J Obstet Gynecol Reprod Biol. 2017;218:99–105. doi:10.1016/j.ejogrb.2017.08.014
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy of Intraoperative Adhesion Barrier Use in Laparoscopic Surgery for Endometriosis: A Single-Center Retrospective Study on Long-Term Recurrence and Pelvic Pain
Hu Y, Chen Y, Li G, Zou Q, Zhan J, Li D
International Journal of Women's Health 2026, 18:592896
Published Date: 9 May 2026