")
Back to Journals » Clinical Ophthalmology » Volume 17
Comparison of Color Fundus Photography and Multicolor Fundus Imaging for Detection of Lesions in Diabetic Retinopathy and Retinal Vein Occlusion
Authors Castro C , Marques JH , Silva N , Abreu AC , Furtado MJ , Lume M
Received 11 April 2023
Accepted for publication 18 July 2023
Published 23 August 2023 Volume 2023:17 Pages 2515—2524
DOI https://doi.org/10.2147/OPTH.S414603
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Catarina Castro,1 João Heitor Marques,1 Nisa Silva,1 Ana Carolina Abreu,1 Maria João Furtado,1,2 Miguel Lume1
1Department of Ophthalmology, Centro Hospitalar Universitário de Santo António, Porto, Portugal; 2Department of Ophthalmology, Instituto de Ciências Biomédicas Abel Salazar – Universidade do Porto, Porto, Portugal
Correspondence: Catarina Castro, Largo Prof. Abel Salazar, Porto, 4099-001, Portugal, Tel +351222077500, Email [email protected]
Purpose: To evaluate the agreement between conventional fundus photography (CFP) and multicolor fundus imaging (MFI) for the detection of lesions of diabetic retinopathy (DR) and retinal vein occlusion (RVO).
Methods: Cross-sectional analysis of eyes with DR or RVO who underwent CFP and MFI. All images were independently analyzed by two observers (O1 and O2), and the evaluated lesions were classified as “present” or “absent”. Then, a paired comparison between both exams of the same eye was performed, to assess which made it easier to detect the lesions.
Results: Considering DR, the agreement was substantial for cotton wool spots and photocoagulation scars for both observers (O1: κ=0.75 and κ=0.67; O2: κ=0.71 and κ=0.64, respectively) and for hard exudates for O1 (κ=0.80). These lesions were detected more frequently on MFI. Regarding RVO, the agreement was considered substantial for venous sheathing by O1 (κ=0.64) and moderate for optociliary shunts by O2 (κ=0.60). Optociliary shunts were detected more frequently in CPF by both observers and venous sheathing on MFI by O1. For microaneurysms, retinal hemorrhages, retinal neovascularization, and proliferative membranes, in DR, and retinal hemorrhages, venous engorgement, and retinal neovascularization in RVO, the agreement was almost perfect (κ> 0.82). In the paired analysis, both observers considered that, in DR, microaneurysms and retinal hemorrhages were easier to detect on CFP and that retinal neovascularization, cotton wool spots, and photocoagulation scars were easier to identify on MFI. Regarding RVO, optocilliary shunts were easier to identify on CFP and venous engorgement on MFI.
Conclusion: The agreement of MFI and CFP was substantial to almost perfect for most lesions. MFI seems better to detect cotton wool spots and photocoagulations scars in DR and venous sheathing in RVO. Optocilliary shunts seem easier to detect on CFP.
Keywords: diabetic retinopathy, retinal vein occlusion, multicolor, color fundus photography
Introduction
Diabetic retinopathy (DR) is a common microvascular complication of diabetes and one of the leading causes of blindness worldwide.1 On turn, retinal vein occlusions (RVO) are a heterogeneous group of disorders that encompass branch retinal vein occlusion, central retinal vein occlusion and hemiretinal vein occlusion, and represent the second leading cause of retinal vascular blindness, following DR.2
Retinal imaging is a key part in the ophthalmologic evaluation, treatment, and follow-up of patients with retinal disease. Color fundus photography (CFP) became available for clinical practice in the 1950s and provides fundus images identical to the fundoscopic findings.3,4 Over the years, there have been many enhancements to this type of camera, such as wide- and ultra-field views, stereoscopic photography, and non-mydriatic options.5–7 The scanning laser ophthalmoscope (SLO), on the other side, was introduced in the 1980s, providing an alternative method for acquiring fundus images. SLO devices use a single point of laser light at specific wavelengths, which is scanned across the retina in a series of parallel horizontal lines. Since only a small part of the eye fundus is illuminated at each time, the effects of light scatter are reduced, allowing these devices to produce images with higher contrast than conventional fundus cameras.4 Confocal SLO, additionally, allows image acquisition at different planes and higher contrast due to suppression of scattered light.3 The multicolor mode developed by Heidelberg Engineering® uses the confocal SLO system to capture three reflectance images (blue, green and infrared). Due to the different depth of penetration of the different wavelengths it is possible to obtain details at different layers of the retina.3 The infrared laser (815 nm) offers a better visualization of the deeper levels, such as the retinal pigment epithelium and the choroid, the green wavelength (518 nm) offers a better visualization of the intraretinal features, such as blood vessels, hemorrhages, and exudates, and the blue wavelength (486 nm) is better to detect changes in the superficial layers, such as the vitreoretinal interface and the retinal nerve fiber layer.8
Ophthalmic imaging modalities have an increasingly important role in the screening, diagnosis, and monitoring of retinal diseases. Currently, the gold standard photography method for the detection of DR is the CFP.9–11 Regarding, RVO, The EURETINA guidelines do not specify which image method is more appropriate for documentation and follow-up or retinal lesions.12 The Royal College of Ophthalmologistshas suggested that CFP should be performed as part of the baseline evaluation, and the American Academy of Ophthalmology also recommends that fundus photography should be performed.13,14 However, advantages and disadvantages of CFP and MFI are not stated.9–12,14
As many patients undergo fundus imaging in clinical practice, our purpose was to evaluate the degree of agreement between CFP and MFI for detection of lesions, in eyes with DR or RVO.
Methods
This study is a cross-sectional analysis of consecutive eyes with DR or RVO scheduled for angiography, submitted to CFP and MFI, between January 1 and March 31, 2021, in Centro Hospitalar Universitário de Santo António, Portugal. Both exams of the same eye were performed on the same day, by the same experienced operator, after pupil dilation. All stages of DR and all types of RVO (central vein occlusion, branch vein occlusion or hemiretinal vein occlusion) were included. Eyes with other retinal pathologies besides DR or RVO or in which proper pupil dilation was not possible were not included. Images in which media transparency precluded clear visualization of the details of the optic disc, macula or vascular arcades, either on CFP or MFI, were excluded. Spherical equivalent or history of previous retinal treatments (eg, panretinal photocoagulation) were not used as exclusion criteria. All images were centered in the macula and included the optic disc.
This study was performed in accordance with the tenets of the Declaration of Helsinki. Ethical approval was obtained from the local Institutional Review Board (Departamento de Ensino, Formação e Investigação, Centro Hospitalar Universitário de Santo António) and all participants gave written informed consent after explanation of the study protocol and purpose.
CFP was performed using the Topcon TRC-50DX® digital fundus camera (Topcon Positioning Systems, Inc, Tokyo, Japan) to capture images with a 50° field of view. MFI was performed using the Spectralis HRA+OCT Heidelberg Engineering® platform (Heidelberg Engineering, Inc, Heidelberg, Germany, version 1.10.4.0) to capture images with a 55° field of view. Infrared, blue reflectance, and green reflectance monochromatic images were not used for analysis. Images were then saved in the same computer as JPG files with the same resolution and, due to the different field of view between the two image methods, they were cropped to the same dimensions using the retinal vasculature to identify corresponding points. All images were evaluated by the two observers in the same computer, in the same room with the same light conditions, with screen settings standardized to the highest possible resolution.
The following lesions were considered in DR: microaneurysms, retinal hemorrhages, cotton wool spots, hard exudates, retinal neovascularization, fibrovascular proliferative membranes, and photocoagulation scars. In RVO we considered retinal hemorrhages, venous engorgement, venous sheathing, retinal neovascularization, and optociliary shunts. Macular edema was not evaluated because its assessment in fundus images is very dependent on the pattern and extent of the edema and optical coherence tomography is the preferred method for its evaluation and follow-up. In this study we opted to evaluate and compare each individual lesion, rather than the stage of disease, to understand the differences that can be expected in each lesion between exams and if any exam is superior in the detection of a particular lesion.
Two distinct analyses were performed. At first, all images (both CFP and MFI) were anonymized, and an independent and blind analysis was carried out by two experienced medical retina specialists (Observer 1 [O1] and Observer 2 [O2]), and lesions were classified as “present” or “absent”. In this step the number of each type of lesion was not considered, only its presence. Both observers started by analyzing half of the CFP images and half of the MFI images. After 2 weeks, the same observers analyzed the remaining images. CFP and MFI of the same eye were never analyzed at the same time. In a second phase, in cases in which the same lesions were previously identified in both exams of the same eye, a paired comparison was performed, and each observer subjectively classified the lesions as “equally detectable in both exams”, “easier to identify on CFP”, or “easier to identify on MFI”. In this step the observers took into consideration the number of lesions identified in each exam (eg, how many microaneurysms identified in each exam), the clarity of visualization of each lesion, and the degree of attention that was necessary to identify the lesions in each exam. None of the observers participated in the image selection or in the anonymization procedure.
Statistical analysis was performed using IBM® SPSS® Statistics version 26. Categorical variables are summarized as relative frequencies. The degree of agreement between observers and between exams was assessed with a Cohen’s Kappa Coefficient (κ). Cohen’s Kappa values between 0.41 and 0.60 indicate moderate agreement, between 0.61 and 0.80 indicate substantial agreement, and from 0.81 to 1.00 indicate almost perfect agreement.15 Cohen’s Kappa values are presented with the respective 95% confidence interval (CI). Statistical significance was defined as a p value inferior to 0.05.
Results
Diabetic Retinopathy
We included 123 eyes of 62 patients with DR. Due to low definition of the details of the optic disc and vascular arcades, eight eyes (seven patients) were excluded. A total of 115 eyes of 61 patients (mean age 62.6 ± 11.1 years old, 57.4% females) were analyzed. The frequencies of each lesion reported by O1 and O2 are summarized in Table 1. The agreement between CFP and MFI for O1 was almost perfect for microaneurysms (κ=0.96), retinal hemorrhages (κ=0.93), retinal neovascularization (κ=1.00), and fibrovascular proliferative membranes (κ=1.00), and substantial for cotton wool spots (κ=0.75), hard exudates (κ=0.80), and photocoagulation scars (κ=0.67). For O2 the agreement was almost perfect for microaneurysms (κ=0.87), retinal hemorrhages (κ=0.92), retinal neovascularization (κ=0.82), hard exudates (κ=0.86), and fibrovascular proliferative membranes (κ=0.91), and substantial for cotton wool spots (κ=0.71) and photocoagulation scars (κ=0.64). The agreement analysis is detailed in Table 2. Figure 1 shows the paired MFI and CFP of an eye with DR. Considering lesions with only substantial agreement by at least one of the observers, cotton wool spots were detected more frequently on MFI by both observers (O1: 17.4% vs 11.3%; O2: 17.4% vs 10.4%), as well as photocoagulation scars (O1: 54.8% vs 38.3%; O2: 52.2% vs 35.7%) and hard exudates (O1: 44.3% vs 38.3%; O2: 45.2% vs 40.0%). The agreement between observers was almost perfect for all lesions (κ>0.82).
 |
Table 1 Frequency of Detection of Retinal Lesions in Diabetic Retinopathy |
 |
Table 2 Agreement of Lesion Detection Between Color Fundus Photography and Multicolor Fundus Imaging for Diabetic Retinopathy |
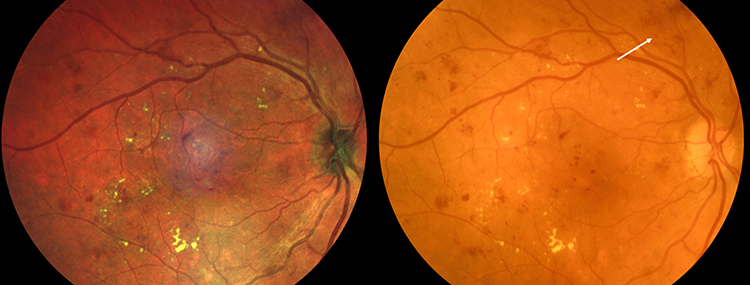 |
Figure 1 MFI and CFP of a patient with diabetic retinopathy. The white arrow shows an example of hemorrhages and microaneurysms that are more clearly visible and delineated on CFP. Abbreviations: MFI, Multicolor fundus imaging; CPF, Color fundus photography. |
Regarding the paired analysis, O1 considered that in 23.3% and 23.2% of cases microaneurysms and retinal hemorrhages, respectively, were easier to detect on CFP, that in 71.4% of cases retinal neovascularization was easier to identify on MFI, in 84.6% of cases cotton wool spots were more evident on MFI, and that in 29.5% of cases photocoagulation scars were present on both exams they were more evident on MFI. O2 considered that in 40.3% and 37.7% of cases microaneurysms and hemorrhages, respectively, were easier to identify on CFP, that in 60.0% of cases retinal neovascularization was more evident on MFI, in 66.7% of cases cotton wool spots were easier to detect on MFI, and in 47.5% of cases photocoagulation scars were easier to detect on MFI. Detailed paired data is available in Table 3.
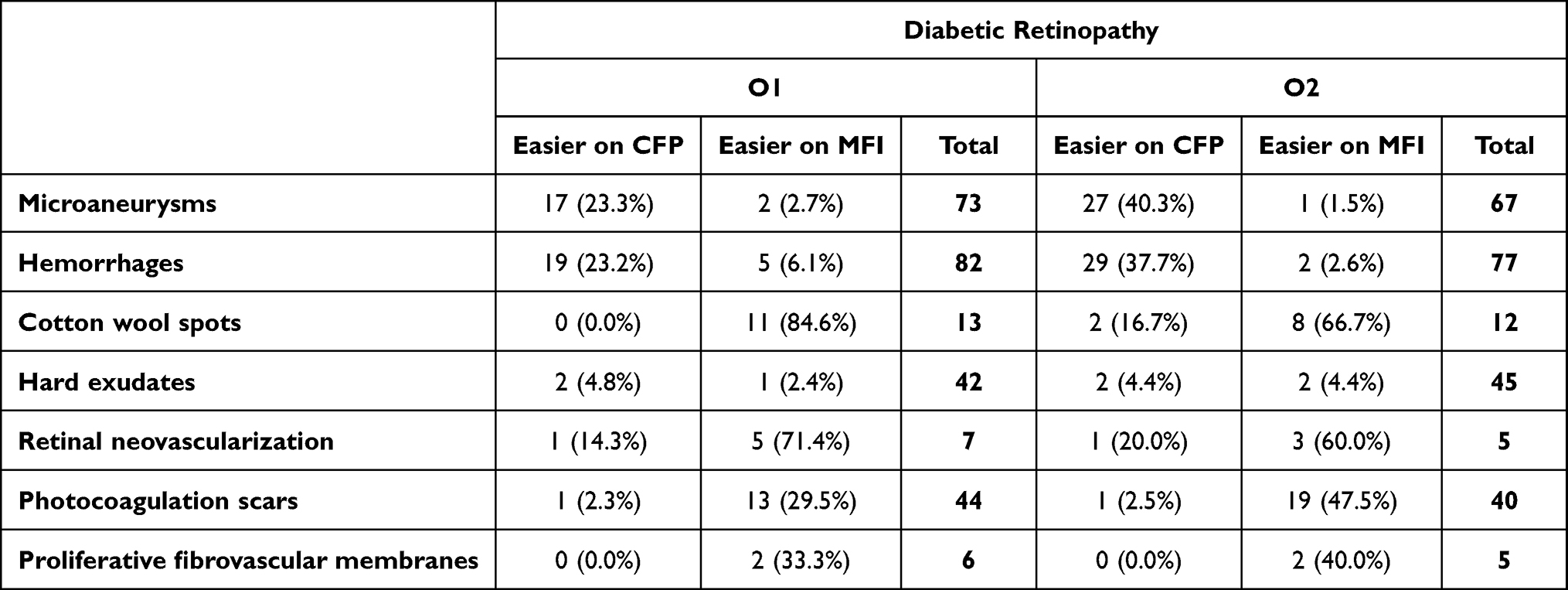 |
Table 3 Paired Comparison of Lesions Detected in Both Exams of the Same Eye of Patients with Diabetic Retinopathy |
Retinal Vein Occlusion
Regarding RVO, 35 eyes (33 patients) were included, but two eyes (two patients) were excluded due to the presence of vitreous hemorrhage that precluded good visualization of the optic disc and vascular arcades. A total of 33 eyes of 31 patients (mean age 64.6 ± 13.2 years old, 51.6% females) were then analyzed. The reported frequencies of each lesion are summarized in Table 4. For O1 the agreement was almost perfect for retinal hemorrhages (κ=0.92), retinal neovascularization (κ=1.00), venous engorgement (κ=0.86), and optociliary shunts (κ=0.91) and substantial for venous sheathing (κ=0.64). For O2 the agreement was almost perfect for retinal hemorrhages (κ=0.84), retinal neovascularization (κ=1.00), venous engorgement (κ=1.00), and venous sheathing (κ=1.00), and moderate for optociliary shunts (κ=0.60). The agreement analysis is detailed in Table 5. Regarding cases with substantial or moderate agreement by at least one of the observers, venous sheathing was detected more frequently on MFI by O1 (12.1% vs 6.1%) and optociliary shunts on CFP by both observers (O1: 24.4% vs 21.2%; O2: 24.2% vs 12.1%). Figure 2 shows the corresponding MFI and CFP of an inferior branch RVO. The agreement between observers was almost perfect for all lesions in both exams (κ>0.85), except for venous sheathing on CFP (κ=0.64 [0.18–1.09], p<0.001, substantial) and optociliary shunts on MFI (κ=0.60 [0.27–0.94], p<0.001, moderate).
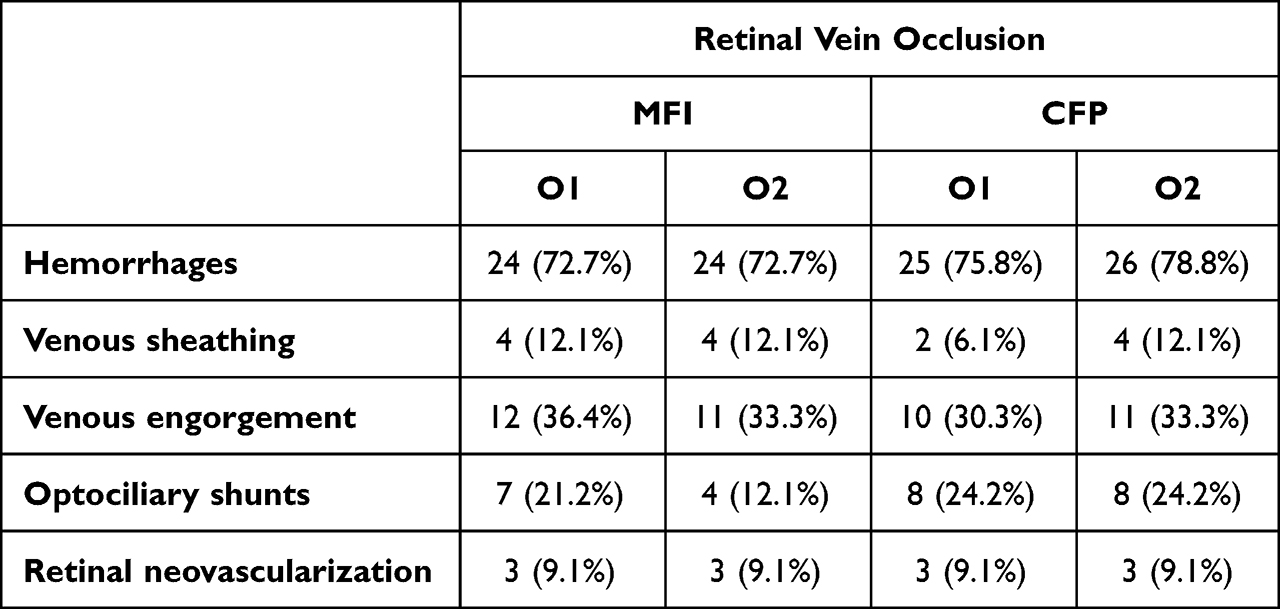 |
Table 4 Frequency of Detection of Retinal Lesions in Retinal Vein Occlusion |
 |
Table 5 Agreement of Lesion Detection Between Color Fundus Photography and Multicolor Fundus Imaging for Retinal Vein Occlusion |
 |
Figure 2 MFI and CFP of a patient with an inferior branch retinal vein occlusion. Abbreviations: MFI, Multicolor fundus imaging; CPF, Color fundus photography. Note: A central light artifact is present in the MFI. |
When considering lesions that were present in both exams, O1 considered that in 71.4% of cases optociliary shunts were easier to identify on CFP and that in 60.0% of cases venous engorgement was easier to identify on MFI. O2 considered that all cases of optociliary shunts were easier to identify on CFP, that in 36.4% of cases venous engorgement was easier to detect on MFI and in 75.0% of cases, venous sheathing was easier to identify on MFI. Detailed paired data is represented in Table 6.
 |
Table 6 Paired Comparison of Lesions Detected in Both Exams of the Same Eye of Patients with Retinal Vein Occlusion |
Discussion
Both CFP and MFI can be used in daily clinical practice for diagnosis and follow-up of retinal diseases.
The agreement between both exams was substantial to almost perfect for most lesions of both DR and RVO, except for optociliary shunts, in which the agreement was only moderate for O2. Considering lesions with only substantial or moderate agreement by at least one of the observers, cotton wool spots, photocoagulation scars, and hard exudates were detected more frequently on MFI and optociliary shunts on CFP by both observers. Additionally, venous sheathing was detected more frequently on MFI by O1.
In the subjective paired comparison both observers found that, in DR, microaneurysms and retinal hemorrhages were easier to detect on CFP and, on the opposite side, retinal neovascularization, cotton wool spots, and photocoagulation scars were easier to identify on MFI. Microaneurysms and hemorrhages appear as red lesions on both exams, but on MFI they have a darker red color and the observers found that the contrast against the orange-red fundus was lower compared to CFP, which, in some cases, made them harder to identify and more time consuming. Cotton wool spots, on turn, appear as white-yellowish pale lesions with poorly defined borders on CFP and as yellow-greenish lesions with well-defined borders on MFI, making the identification on MFI more straightforward. Photocoagulation scars either appear as pale-white or dark pigmented lesions on CFP and are either bright-white or brown/black on MFI. Pale-white lesions are often very subtle on CFP and can easily go unnoticed, while the bright-white aspect on MFI makes them easier to identify (Figure 3). Regarding retinal neovascularization, some vascular branches were very subtle on CFP but clearly visible on MFI (Figure 3). In RVO, optociliary shunts were considered easier to identify on CFP. Both observers found that, on MFI, branches within the optic disc were either not visible or had less defined boundaries, while on CFP they were perfectly defined (Figure 3). Venous engorgement, on turn, was more evident on MFI. O1 detected venous sheathing more frequently on MFI and O2 also considered it easier to identify on MFI. Once again, venous sheathing appears as a pale-white contour on the vessel wall on CFP and as a bright green contour on MFI, making the identification straightforward in this last exam (Figure 3). Globally, both observers found that vascular changes (except for microaneurysms and optociliary shunts) were easier to detect with MFI.
 |
Figure 3 Differences between MFI and CFP. In image (1a and 1b) it is possible to see venous sheathing (black arrow) that is more evident in the MFI (1b); In (2a) (CFP) there is an optociliary shunt (white arrow) that in not clearly visible in (2b) (MFI); In (3) there is retinal neovascularization (blue arrows) and photocoagulation scars (yellow arrows) that are more clearly visible in the MFI (3b) than in the CFP (3a). Abbreviations: MFI, Multicolor fundus imaging; CPF, Color fundus photography. |
Roy et al16 also compared the two image modalities in patients with DR. Hard exudates were visible in 71.2% of eyes, both on CFP and MFI, cotton wool spots in 27.9% of eyes on MFI and in 26.0% on CFP, and retinal hemorrhages in 79.8% on MFI and in 72.8% on CFP. In our study, hard exudates and cotton-wool spots were detected more frequently on MFI and retinal hemorrhages were similarly detected in the two exams by both observers. Roy et al16 also analyzed in which exam the lesions were better seen, concluding that hard exudates, cotton wool spots, and retinal hemorrhages were better seen on MFI. In contrast, in our subjective analysis, retinal hemorrhages were considered harder to detect on MFI. In a study by Graham et al,17 that compared both types of fundus image in patients with age-related macular degeneration, the authors also concluded that hemorrhages were better seen on CFP than on MFI.
Li et al,18 who also performed a comparison between MFI and CFP in DR, found that microaneurysms, intraretinal hemorrhages, hard exudates, retinal neovascularization, photocoagulation scars, and fibrous proliferation were detected more frequently on MFI and cotton wool spots on CFP. Despite this, the difference was only statistically significant for microaneurysms. They considered that microaneurysms were better demarcated on MFI, as well as the size and the precise boundaries of fibrovascular proliferative membranes.
Regarding RVO, Unno et al19 compared the detection of vessel whitening between the two image modalities, concluding that MFI had a superior vessel whitening visibility score than CFP.
In current clinical practice many physicians prefer to use MFI, as it is usually integrated in a multimodal imaging device, encompassing not only the MFI, but also the spectral domain optical coherence tomography, fundus angiography, and autofluorescence. In addition, besides the composite image, it also offers the possibility to analyze distinct monochromatic laser images (like infrared, green reflectance, and blue reflectance) allowing for a pseudo-segmentation effect.8 Despite this, it is important to understand how the findings on MFI correlate to CFP, which offers an image closer to the real fundus exam, and to understand the advantages of each technique.
Few studies compare CFP and MFI to detect retinal lesions. Graham et al17 compared both exams in age-related macular degeneration. For early-stage features, MFI detected all type of drusen more frequently, as well as non-geographic atrophy hypopigmentation, but CFP detected pigment clumping more often. Regarding late features, hemorrhages were detected more frequently on CFP, but fibrosis and atrophy were observed more often on MFI. De Rosa et al20 evaluated the presence of fibrotic scars in exudative age-related macular degeneration, concluding that fibrosis was fully visible, and the margins more sharply defined in more cases with MFI, comparing to CFP and ultra-widefield CFP. MFI also provided superior distinction between fibrosis and atrophy and, so, the authors concluded that MFI was superior regarding visualization and analysis of subretinal fibrosis when compared to CFP. Tan et al21 compared the two image modalities in patients with polypoidal choroidal vasculopathy, concluding that, despite differences in the appearance, they are comparable in the detection of multiple features of the disease. Saurabh et al22 compared the ability of MFI to detect a typical lesion of central serous chorioretinopathy against CFP, concluding that MFI had higher sensitivity and lower specificity for retinal pigment epithelium atrophy, that serous pigment epithelium detachment was more easily detected on MFI, and that both image modalities were similar in their ability to detect subretinal fluid. Regarding the presence of fibrin, it was seen more distinctly on CFP. Song et al23 compared MFI and CFI in the evaluation of epiretinal membranes, finding that it was more clearly detectable and widely demarcated on MFI.
Our study has some limitations, in particular the small number or participants. We also did not include images in which the optic disc, macula, and vascular arcades were not clearly visualized. Additionally, due to the different field of view between the two image methods, images were cropped using the retinal vasculature. Therefore, there was some subjectivity in the selection and preparation of the images that were then analyzed. We did not correlate our findings with other image modalities, such as fluorescein angiography and the optical coherence tomography, that could help to understand with greater detail the differences between CFP and MFI. We only compared CFP obtained with the Topcon® and MFI obtained with the Spectralis®. Different devices generate images with different characteristics, and our results may not be generalizable to other devices. Another limitation is that only two observers were included in this study. However, both observers were experienced, which is important for the reliability of the results. Finally, in some cases MFI generates a central acquisition artifact that precludes perfect visualization of the underneath retina. However, when present, this artifact still allows identification of underneath lesions. We believe excluding images with this artifact would represent a selection bias and would not represent the real-life conditions in which these exams are usually requested. Despite these limitations, this is one of the few studies comparing both exams in DR and RVO, and, to our best knowledge, the only one that evaluates more than one type of lesion in RVO. Another positive point of our study is performing a subjective paired analysis. Despite being detected in both exams, some lesions appear to be more easily seen in one of them. This can have a significant impact in daily life practice, as the use of both exams in combination may increase the rate of detection of lesions that otherwise could be missed, as well as, depending on the expected retinal changes, the more suitable exam can be performed to improve diagnostic accuracy. Furthermore, choosing the most appropriate exam or combining both can provide better documentation of fundus changes, which is important for patient’s follow-up. Concerning MFI, the advantage of performing different image modalities with the same device should also be highlighted, as well as the pseudo-segmentation effect.
In conclusion, the agreement of MFI and CFP to detect lesions in DR and RVO was substantial to almost perfect for most lesions, making them both appropriate exams for screening, diagnosis, or monitoring of retinal changes. Despite this, MFI seems more appropriate to detect cotton wool spots, hard exudates, and photocoagulation scars in eyes with DR and venous sheathing in eyes with RVO. On turn, optociliary shunts seem easier to detect on CFP. Regarding DR, as the earlier changes of the disease (microaneurysms and hemorrhages) seem easier to identify in CFP, we believe it to be a good screening exam, and that it should keep on being used as the screening tool for the general population, as is recommended in current clinical practice.9,11 In turn, MFI may be a better option, in a hospital setting, to evaluate more advanced stages of the disease. Hence, we believe that, in DR and RVO, in the hospital setting, both CFP and MFI should be performed, to increase diagnostic accuracy and provide more reliable follow-up images. If this is not possible, then the exam of choice should be based on the lesions detected in the fundus observation.
Data Sharing Statement
Data is available upon reasonable request.
Acknowledgments
The authors are grateful to the Orthoptists of our Department for their valuable contribution to this work.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cheung N, Mitchell P, Wong TY. Diabetic retinopathy. Lancet. 2010;376(9735):124–136. doi:10.1016/S0140-6736(09)62124-3
2. Ip M, Hendrick A. Retinal vein occlusion review. Asia Pac J Opthalmol. 2018;7(1):40–45.3.
3. Tan ACS, Fleckenstein M, Schmitz-Valckenberg S, Holz FG. Clinical application of multicolor imaging technology. Ophthalmologica. 2016;236(1):8–18. doi:10.1159/000446857
4. Keane PA, Sadda SR. Retinal imaging in the twenty-first century. Ophthalmology. 2014;121(12):2489–2500. doi:10.1016/j.ophtha.2014.07.054
5. Witmer MT, Kiss S. Wide-field imaging of the retina. Surv Ophthalmol. 2013;58(2):143–154. doi:10.1016/j.survophthal.2012.07.003
6. Li HK, Hubbard LD, Danis RP, Esquivel A, Florez-Arango JF, Krupinski EA. Monoscopic versus stereoscopic retinal photography for grading diabetic retinopathy severity. Invest Opthalmol Vis Sci. 2010;51(6):3184–3192. doi:10.1167/iovs.09-4886
7. Piyasena MMPN, Yip JLY, MacLeod D, Kim M, Gudlavalleti VSM. Diagnostic test accuracy of diabetic retinopathy screening by physician graders using a hand-held non-mydriatic retinal camera at a tertiary level medical clinic. BMC Ophthalmol. 2019;19(1):89. doi:10.1186/s12886-019-1092-3
8. Tan CS, Ting DS, Lim LW. Multicolor fundus imaging of polypoidal choroidal vasculopathy. Ophthalmol Retina. 2019;3(5):400–409. doi:10.1016/j.oret.2019.01.009
9. Das T, Takkar B, Sivaprasad S, et al. Recently updated global diabetic retinopathy screening guidelines: commonalities, differences, and future possibilities. Eye. 2021;35(10):2685–2698. doi:10.1038/s41433-021-01572-4
10. Flaxel CJ, Adelman RA, Bailey ST, et al. Diabetic retinopathy preferred practice pattern®. Ophthalmology. 2020;127(1):66–P145.
11. Nanegrungsunk O, Patikulsila D, Sadda SR. Ophthalmic imaging in diabetic retinopathy: a review. Clin Experiment Ophthalmol. 2022;50(9):1082–1096. doi:10.1111/ceo.14170
12. Schmidt-Erfurth U, Garcia-Arumi J, Gerendas, BS, et al. Guidelines for the Management of Retinal Vein Occlusion by the European Society of Retina Specialists (EURETINA). Ophthalmologica. 2019;242(3): 123–162. doi:10.1159/000502041.
13. Royal College of Ophthalmologists. Clinical Guidelines. Retinal Vein Occlusion (RVO); 2022. Available from: https://www.rcophth.ac.uk/resources-listing/retinal-vein-occlusion-rvo-guidelines/.
14. Flaxel CJ, Adelman RA, Bailey ST, et al. Retinal vein occlusions preferred practice pattern®. Ophthalmology. 2020;127(2):P288–P320. doi:10.1016/j.ophtha.2019.09.029
15. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159–174. doi:10.2307/2529310
16. Roy R, Saurabh K, Thomas NR, Chowdhury M, Shah DK. Validation of multicolor imaging of diabetic retinopathy lesions vis a vis conventional color fundus photographs. Ophthalmic Surg Lasers Imaging Retina. 2019;50(1):8–15. doi:10.3928/23258160-20181212-02
17. Graham KW, Chakravarthy U, Hogg RE, Muldrew KA, Young IS, Kee F. Identifying features of early and late age-related macular degeneration: a comparison of multicolor versus traditional color fundus photography. Retina. 2018;38(9):1751–1758. doi:10.1097/IAE.0000000000001777
18. Li S, Wang X, Du X, Wu Q. Clinical application of multicolour scanning laser imaging in diabetic retinopathy. Lasers Med Sci. 2018;33(6):1371–1379. doi:10.1007/s10103-018-2498-5
19. Unno N, Lando L, Alex V, et al. Comparison of multicolor scanning laser imaging and color fundus photography in evaluating vessel whitening in branch retinal vein occlusion. Ophthalmic Res. 2022. doi:10.1159/000528251
20. De Rosa I, Ohayon A, Semoun O, et al. Real-color versus pseudo-color imaging of fibrotic scars in exudative age-related macular degeneration. Retina. 2020;40(12):2277–2284. doi:10.1097/IAE.0000000000002771
21. Tan ACS, Yanagi Y, Cheung GCM. Comparison of multicolor imaging and color fundus photography in the detection of pathological findings in eyes with polypoidal choroidal vasculopathy. Retina. 2020;40(8):1512–1519. doi:10.1097/IAE.0000000000002638
22. Saurabh K, Roy R, Goel S, Garg B, Mishra S. Validation of multicolor imaging signatures of central serous chorioretinopathy lesions vis-a-vis conventional color fundus photographs. Indian J Ophthalmol. 2020;68(5):861–866. doi:10.4103/ijo.IJO_1187_19
23. Song JH, Moon KY, Jang S, Moon Y. Comparison of multicolor fundus imaging and colour fundus photography in the evaluation of epiretinal membrane. Acta Ophthalmol. 2019;97(4):e533–e539. doi:10.1111/aos.13978
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.