Back to Journals » Advances in Medical Education and Practice » Volume 17
Comparison of Arterial Puncture Skill Improvement Between Training with an Arterial Puncture Part-Task Trainer Simulator and Conventional Training in Fifth-Year Medical Students: A Pilot Study
Authors Athinartrattanapong N, Chamchoi P, Chalermdamrichai P, Tangkulpanich P ![]() , Yuksen C
, Yuksen C ![]() , Palee C
, Palee C ![]() , Seesuklom S
, Seesuklom S ![]()
Received 10 January 2026
Accepted for publication 4 April 2026
Published 16 April 2026 Volume 2026:17 530106
DOI https://doi.org/10.2147/AMEP.S530106
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Natsinee Athinartrattanapong, Parinda Chamchoi, Phanorn Chalermdamrichai, Panvilai Tangkulpanich, Chaiyaporn Yuksen, Chantarat Palee, Suteenun Seesuklom
Department of Emergency Medicine, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, 10400, Thailand
Correspondence: Chaiyaporn Yuksen, Department of Emergency Medicine, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, 10400, Thailand, Email [email protected]
Introduction: Arterial puncture is a fundamental procedural skill that medical trainees must acquire. However, it carries a risk of serious complications, particularly when performed by inexperienced operators. This study aimed to develop an arterial puncture part-task trainer to enhance skill acquisition among medical students and to compare arterial puncture performance between simulator-based training and conventional training in fifth-year medical students.
Methods: This experimental study was conducted from January 26, 2024, to April 11, 2024, and included twenty-two fifth-year medical students undergoing emergency department training at Ramathibodi Hospital. Participants performed arterial punctures on patients, and all procedures were recorded on video. Three independent raters evaluated the recordings using a standardized procedural checklist. The primary outcome was the total arterial puncture procedural checklist score during the initial patient-based assessment. The intervention group additionally underwent a reassessment two weeks after simulator training to evaluate skill retention. Continuous variables were analyzed using Student’s t-test, while categorical variables were analyzed using the chi-square test. Statistical significance was set at P < 0.05.
Results: During the study period, the intervention group (n=10) achieved a significantly higher total skill score (37.1 ± 3.2) compared to the control group (n=12), which had a score of 33.25 ± 3.8 (p = 0.016). Additionally, the total self-confidence scores significantly increased from 23.5 to 25.6 (p = 0.040). Participants expressed strong satisfaction with the arterial puncture part-task trainer, with a mean rating of 3.68 for its suitability for practicing arterial puncture and a mean rating of 3.86 for its potential use in medical student training.
Conclusion: Although this pilot study involved a relatively small sample size, the arterial puncture part-task trainer simulator significantly improved both procedural skill performance and self-confidence in performing arterial punctures.
Keywords: arterial blood gas, arterial puncture part-task trainer, simulation training
Introduction
Arterial puncture for arterial blood gas analysis is a commonly performed procedure in adult patients and is a fundamental skill that all medical trainees must acquire. The primary indication for blood gas analysis is to determine the partial pressures of oxygen and carbon dioxide, as well as arterial pH.1 This information is essential for assessing patients experiencing acute, severe respiratory distress.2 In emergency conditions, in addition to performing arterial puncture for arterial blood gas analysis in the emergency department, point-of-care testing (POCT) arterial blood gas analysis is also utilized in prehospital settings. Studies have shown that POCT arterial blood gas analysis can significantly improve the rate of sustained return of spontaneous circulation in critically ill patients.3
The radial artery, located on the thumb side of the wrist, is typically the preferred site for blood collection due to its superficial location, ease of post-procedural hemostasis, and the presence of collateral circulation, which helps maintain adequate blood flow.4 However, arterial puncture carries several potential complications, including arteriospasm, hematoma, nerve injury, finger necrosis,5 and vasovagal syncope, particularly when performed by inexperienced operators.
Currently, arterial puncture training in medical schools and training centers is primarily conducted on real patients under the supervision of experienced physicians. While this method provides valuable hands-on learning, it carries inherent risks, including procedural complications such as infection and bleeding. Despite its importance, opportunities for medical students to perform arterial puncture under supervision are often limited and highly variable depending on clinical exposure. This variability can result in insufficient procedural practice, reduced learner confidence, and concerns regarding patient safety when inexperienced trainees perform the procedure on real patients. Therefore, comprehensive training in arterial puncture is essential to enhance proficiency while minimizing risks to patients.
Simulation-based training (SBT) has emerged as a transformative approach in medical education, significantly improving skill acquisition and clinical competency among healthcare professionals. Key benefits of SBT include enhanced procedural accuracy, reduced error rates, and the opportunity for repeated practice in a controlled environment without jeopardizing patient safety.6 Arterial puncture is a complex psychomotor procedure requiring accurate palpation of the radial artery, appropriate needle angle control, coordinated hand movements, and effective post-procedural hemostasis. Part-task trainers are particularly suitable for this type of procedural training because they allow learners to repeatedly practice these specific technical components in a controlled environment.
The development of an arterial puncture part-task trainer using locally sourced materials, such as natural rubber, offers a practical and cost-effective solution for skill training. This simulation-based approach provides medical students with hands-on experience, fostering both proficiency and confidence in arterial puncture techniques. In addition to objective procedural performance, learner confidence is an important educational outcome because self-confidence has been shown to influence procedural readiness, willingness to perform clinical skills, and overall learning engagement.
By refining students’ procedural skills in a risk-free setting, simulation-based training (SBT) ultimately contributes to improved patient safety and reduced complication rates in clinical practice.
In this study, we aim to compare the proficiency of fifth-year medical students in performing radial arterial punctures following training with an arterial puncture part-task trainer simulator versus conventional training. Additionally, we seek to assess changes in students’ self-confidence before and after training with the part-task trainer, as well as evaluate participants’ satisfaction with the training experience. In addition to evaluating immediate skill performance, the present study also examined short-term skill retention through reassessment after two weeks. However, longer-term retention beyond this two-week period was not evaluated and should be investigated in future studies. Future studies should explore long-term retention of arterial puncture skills and evaluate the effectiveness of this trainer in earlier-year medical students to improve the generalizability of simulation-based training.
Methods
Study Design and Setting
This study was conducted as a single-center pilot randomized controlled trial within the Emergency Department (ED) of Ramathibodi Hospital. The Department of Emergency Medicine, Faculty of Medicine, Ramathibodi Hospital was established on September 6, 2010. The department has developed multiple academic programs related to emergency medicine, including the Emergency Medicine Residency Program, which has been offered since 2004, and the Bachelor’s Degree Program in Paramedicine, which was introduced in 2015. Additionally, the department has been responsible for delivering emergency medicine education to fifth- and sixth-year medical students since 1984 and continues to do so to the present day.
The emergency medicine curriculum for fifth-year medical students is conducted in collaboration with the Critical Care Unit of the Department of Medicine, Faculty of Medicine, Ramathibodi Hospital. Each six-week rotation includes approximately 15–20 students and incorporates a comprehensive teaching approach. The curriculum consists of didactic lectures, emergency case discussions, hands-on workshops, and workplace-based learning in the emergency department alongside sixth-year medical students, emergency medicine residents, and faculty staff. This structured training ensures that students develop essential clinical competencies and gain practical experience in managing acute and life-threatening conditions in an emergency setting.
Study Participants
Fifth-year medical students currently undergoing clinical training in the Emergency Department of Ramathibodi Hospital from January 26, 2024, to April 11, 2024, were eligible for inclusion in this study. Exclusion criteria included a known allergy to latex, refusal to enroll in the study, or incomplete data on primary outcomes.
Eligible participants received a detailed explanation of the study protocol, and informed consent was obtained before participation.
Participants in both the control and intervention groups received instruction and a demonstration of radial arterial puncture skills using real patients once during their regular clinical training period in the Department of Emergency Medicine under the supervision of emergency medicine staff.
In this study, conventional training refers to the standard clinical teaching approach in which medical students observe and perform radial arterial puncture on real patients under direct supervision of emergency medicine faculty without the use of simulation-based training.
The assessment process for evaluating radial arterial puncture skill performance followed the standard evaluation criteria outlined in the emergency medicine curriculum.
Randomization and Study Protocol
Control Group
During the second week of the emergency medicine rotation, participants in the control group were assigned to perform radial arterial punctures on real patients, with procedural records maintained. The procedure was video recorded, focusing exclusively on the participants’ hands to ensure privacy. No identifiable patient information or images of participants’ or patients’ faces were captured.
After completing the radial arterial puncture, participants filled out questionnaires to assess their self-confidence in performing the procedure.
Interventions Group
During the second week of the emergency medicine rotation, participants in the intervention group were assigned to perform radial arterial punctures on real patients, with procedural records maintained. After completing the procedure, they filled out self-confidence assessment questionnaires following the same protocol as the control group.
Subsequently, they received instruction through a video demonstration of radial arterial puncture. The entire training session lasted one hour.
Two weeks later, participants in the intervention group were reassessed on their radial arterial puncture skills on real patients. The procedure was video recorded, focusing exclusively on the participants’ hands to ensure privacy. No identifiable patient information or images of participants’ or patients’ faces were captured.
After completing the procedure, participants filled out additional questionnaires assessing their self-confidence and satisfaction with the arterial puncture part-task trainer.
The primary comparison between the intervention and control groups was based on the initial arterial puncture performance recorded during week 2 for both groups. The reassessment performed two weeks later in the intervention group was used only to evaluate short-term skill retention and was not included in the primary between-group comparison.
The arterial puncture part-task trainer simulator (Figure 1) is constructed from natural rubber, designed to closely resemble human skin with a flexible surface that enables realistic pulse palpation.
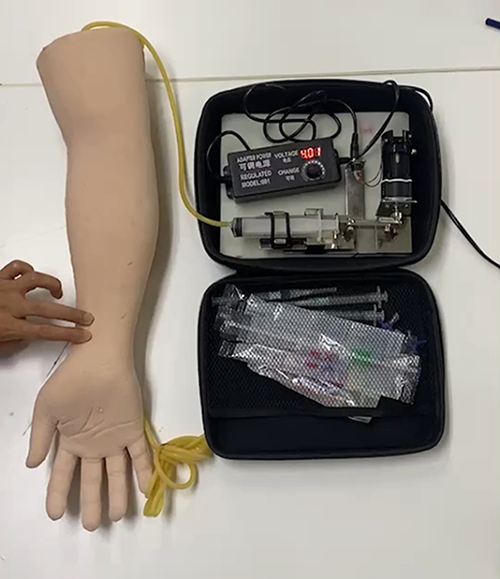 |
Figure 1 Arterial puncture part-task trainer simulator. |
The overall design and structure of the simulator are illustrated in Figure 1. The pulse rate and strength can be adjusted via a control panel, enhancing the training experience. The simulated artery is made from a blood pressure cuff (tourniquet), allowing for multiple punctures, with a replaceable component if damaged.
This locally produced trainer is a cost-effective solution, with an estimated production cost of 15,000–20,000 baht. The Department of Emergency Medicine, Ramathibodi Hospital, Mahidol University developed this part-task trainer as an academic innovation to enhance medical education and procedural training.
Randomization
We employed simple urn randomization to assign eligible students to either the intervention or conventional training group, maintaining a 1:1 allocation ratio.
The random allocation sequence was generated by an independent research assistant using computer-generated random numbers. Allocation concealment was ensured using sequentially numbered opaque sealed envelopes, which were opened only after participant enrollment.
Blinding
This study employed an assessor-blinded design rather than a fully double-blind design. Outcome assessors and patients undergoing arterial puncture were unaware of the participants’ training group assignments. However, participants themselves were aware of whether they received simulator training.
The assessors evaluated performance using video-recorded procedures focusing solely on the participants’ hands to maintain privacy and minimize bias.
Data Gathering
Participant characteristics, including gender, Grade Point Average (GPA), prior experience, and the number of successful radial arterial punctures, were recorded using a structured questionnaire. Self-confidence in performing radial arterial puncture and satisfaction with the arterial puncture part-task trainer were also assessed through questionnaires.
Patient characteristics, such as age, gender, BMI, systolic blood pressure (SBP), mean arterial pressure (MAP), and underlying medical conditions, were documented using a standardized data collection form.
Outcome Measurement
The primary outcome of this study was to assess skill performance in radial arterial puncture as recorded on video.
Three blinded emergency medicine resident raters independently evaluated the skill performance scores.
The skill performance checklist consisted of eight procedural items, each scored on a five-point scale. The total score ranged from 0 to 40, with higher scores indicating better procedural performance.
The secondary outcomes included a comparison of self-confidence levels before and after radial arterial puncture training and an evaluation of participant satisfaction with the arterial puncture part-task trainer.
Development of a Skill Performance Tool for the Assessment of Radial Arterial Puncture
Validation of the Skill Performance Tool
The researcher developed a skill assessment questionnaire specifically for radial arterial puncture, which was reviewed through a comprehensive literature review and evaluated for content validity. The radial arterial puncture skill assessment checklist is presented in Table S1. Content validity was assessed using the Item-Level Content Validity Index (I-CVI) for eight items. A panel of five emergency physicians reviewed the questionnaire and confirmed that all items were relevant to the assessment of skill performance in radial arterial puncture. The I-CVI values for the items ranged from 0.8 to 1. Subsequently, the Scale-Level Content Validity Index (S-CVI) was calculated at 0.98, indicating excellent content validity for the assessment tool.7
Interrater Reliability of the Skill Performance Tool
Prior to data collection, all raters will undergo training to familiarize themselves with the assessment tool. To evaluate the consistency among the three emergency raters, five arterial blood gas (ABG) puncture videos were reviewed. The Intraclass Correlation Coefficient (ICC) was calculated to be 0.852 (P = 0.002) using a two-way random effects model. The analysis demonstrated a strong level of absolute agreement among the raters.8
Sample Size Estimation
The sample size for this study was calculated based on data from a previous pilot study conducted with sixth-year medical students.
Using a health science research application (Version 2.3, App Store; 2024), the sample size was calculated assuming a confidence level of 95% (Z = 1.96), a statistical power of 80% (Z = 0.84), and a 1:1 allocation ratio.
The intervention group had a mean score of 35.6 (SD 6.05), while the control group had a mean score of 29.8 (SD 5.41). The required sample size was calculated as 16 participants per group, for a total of 32 participants.
However, due to the limited number of eligible students during the study period, only 22 participants were included in the final analysis. Therefore, the study should be interpreted as a pilot randomized trial designed to evaluate feasibility and estimate preliminary effect sizes.
Statistical Analysis
Data analyses were conducted using Stata version 17.0. Continuous variables were presented as means and standard deviations (SD), while categorical variables were reported as frequencies and percentages. The Student’s t-test was used to compare radial arterial puncture skill scores, self-confidence levels, and participant and patient characteristics. The Chi-square test was used to analyze categorical variables.
A sensitivity analysis using linear regression adjusting for patient BMI was performed to evaluate potential confounding effects.
All statistical results were considered significant at a P-value < 0.05. The effect size was calculated using Cohen’s d (d = 1.04), indicating a large effect size and suggesting that training using the arterial puncture part-task trainer significantly improved procedural performance compared with conventional training methods.9
Results
The study included 24 fifth-year medical students undergoing clinical rotations in the Emergency Department of Ramathibodi Hospital from January 26 to April 11, 2024. Participants were randomized into two groups: the conventional training group (N = 12) and the arterial puncture part-task training group (N = 12).
All participants in the conventional training group completed evaluations and self-confidence questionnaires. In the part-task training group, two participants were excluded due to missing primary outcome data, leaving 10 participants who completed additional satisfaction questionnaires regarding the part-task trainer.
The final sample size for the study was 22 participants. The participant flow diagram is shown in Figure 2.
 |
Figure 2 Study flow diagram. |
Table 1 shows no significant difference between the arterial puncture part-task trainer simulator and conventional training groups in terms of gender (p = 0.105), GPA (p = 0.548), number of ABG procedures performed (p = 0.345), and number of successful ABG procedures (p = 0.598).
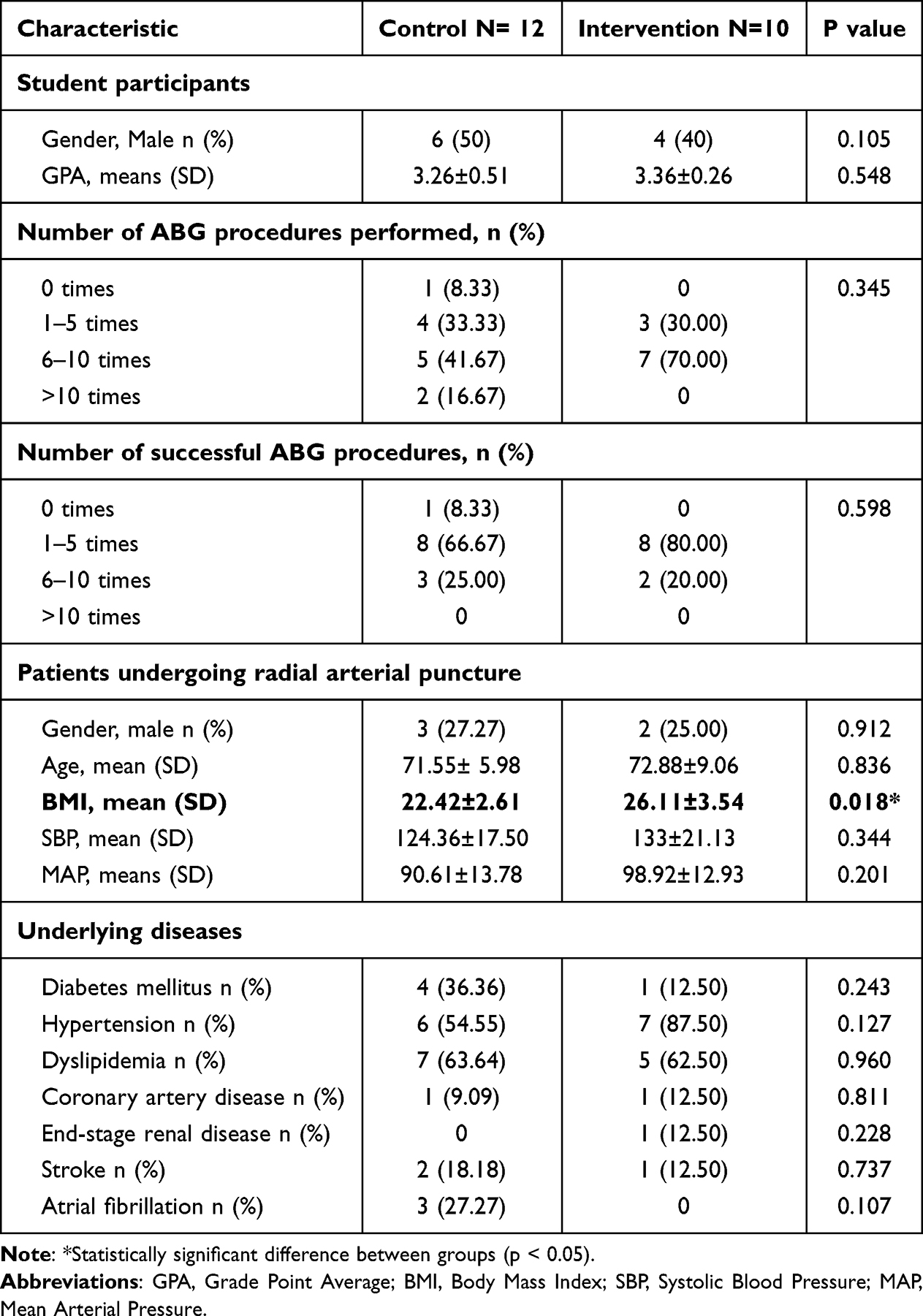 |
Table 1 Baseline Characteristics |
Furthermore, the baseline characteristics of the patients in both groups did not reveal significant differences in gender (p = 0.912), age (p = 0.836), SBP (p = 0.344), MAP (p = 0.201), or underlying diseases, including diabetes mellitus (p = 0.243), hypertension (p = 0.127), dyslipidemia (p = 0.960), coronary artery disease (p = 0.811), end-stage renal disease (p = 0.228), stroke (p = 0.737), and atrial fibrillation (p = 0.107).
The only patient characteristic that showed a statistically significant difference between the two groups was body mass index (BMI), with a p-value of 0.018.
Patients in the intervention group had a higher mean BMI compared with those in the control group, which may increase the technical difficulty of arterial puncture procedures.
The mean BMI in the intervention group was 26.11 ± 3.54, while the control group had a mean BMI of 22.42 ± 2.61.
Although the intervention group treated patients with a higher mean BMI, which may increase the technical difficulty of arterial puncture, this group still demonstrated higher procedural performance.
Compare the Radial Arterial Puncture Skills Between Training with an Arterial Puncture Part-Task Trainer Simulator and Conventional Training in Fifth-year Medical Students
Table 2 shows that the intervention group achieved a significantly higher total skill score (p = 0.012), indicating improved overall performance in radial arterial blood gas (ABG) puncture skills compared with the control group.
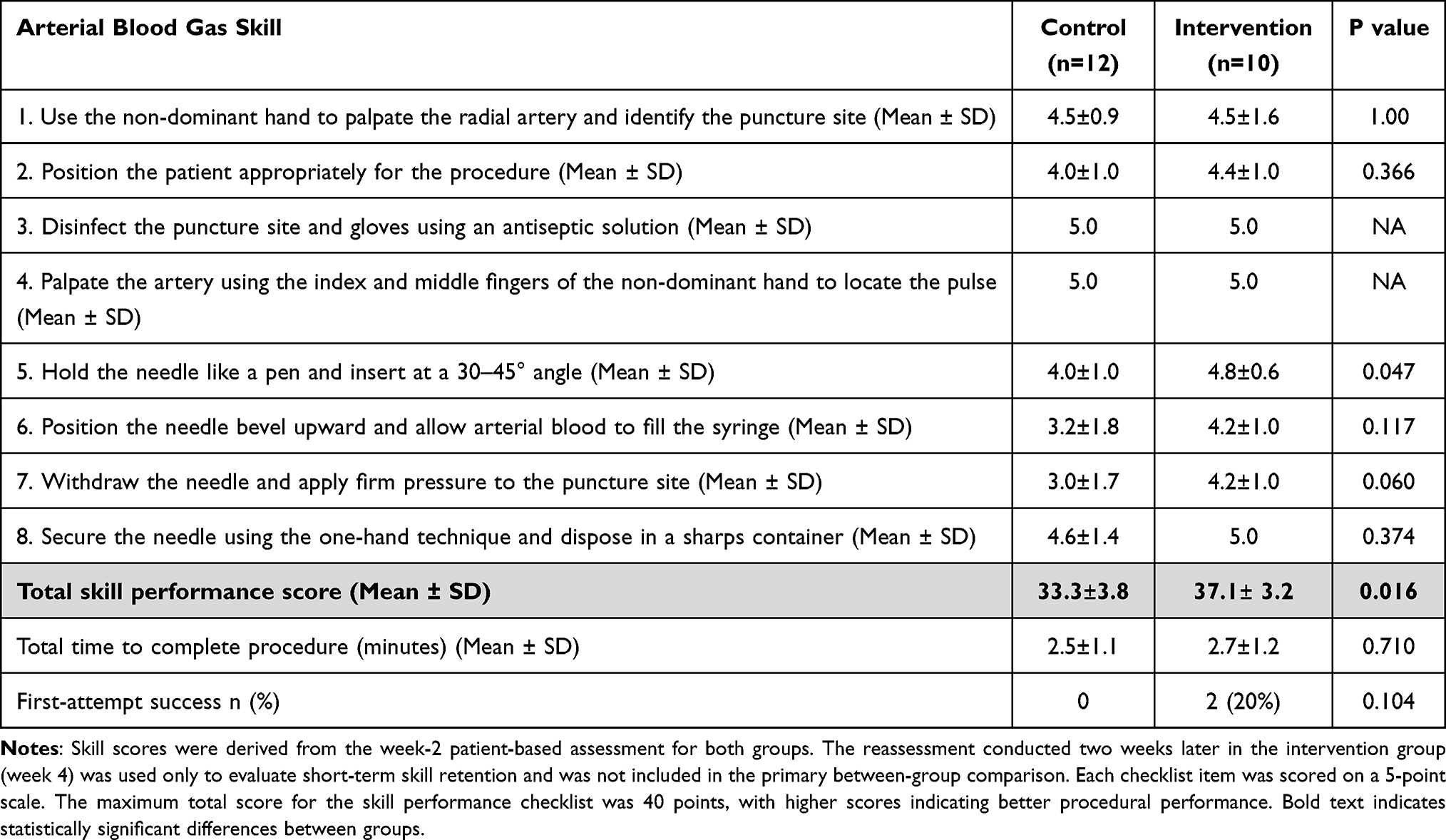 |
Table 2 Comparison of Arterial Puncture Skills Between Training with an Arterial Puncture Part-Task Trainer Simulator and Conventional Training in Fifth-year Medical Students Based on the week-2 Assessment |
In specific skill domains, the intervention group scored higher than the control group in several procedural aspects. Notably, there was a significant improvement in the use of the needle and syringe (p = 0.047), indicating better needle control and technique.
A positive trend was also observed in the application of pressure after needle removal (p = 0.060), although this did not reach statistical significance.
The intervention group also demonstrated a higher first-attempt success rate (20%); however, this difference was not statistically significant (p = 0.104).
The time required to complete the procedure did not differ significantly between the two groups.
The primary comparison between the intervention and control groups was based on the arterial puncture procedures performed during week 2 of the rotation for both groups.
Because this study was conducted as a pilot trial with a relatively small sample size, analyses of individual checklist components should be interpreted as exploratory.
Comparison of Self-Confidence Before and After Training
Table 3 demonstrates a significant increase in the total self-confidence score from 23.5 ± 3.3 to 25.6 ± 2.2 (p = 0.040), indicating that the intervention positively influenced participants’ confidence in performing radial arterial puncture.
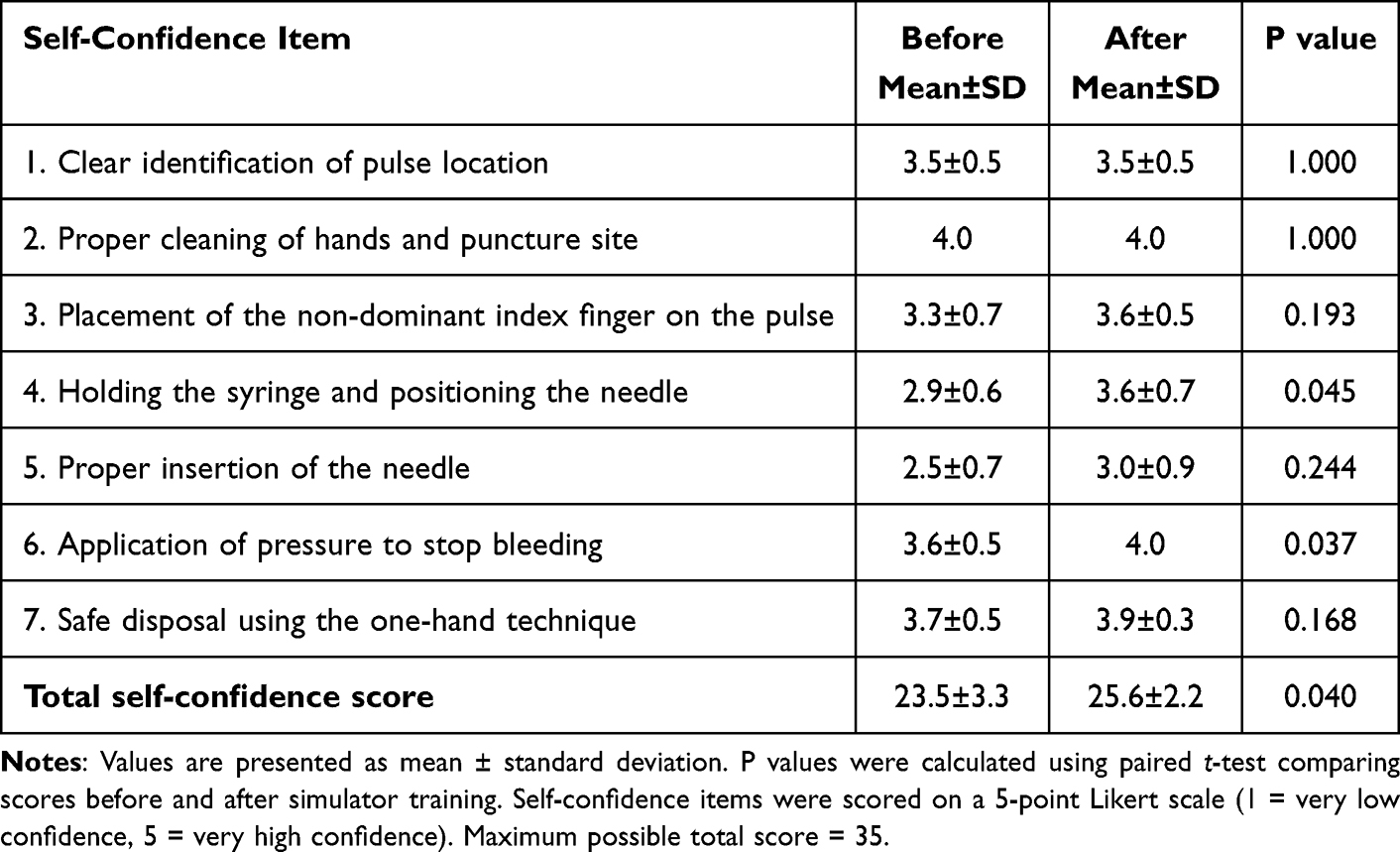 |
Table 3 Comparison of Self-Confidence in Performing Radial Arterial Puncture Before and After Simulator Training in the Intervention Group (n = 10) |
Significant improvements were observed in the ability to hold the syringe and position the needle correctly (p = 0.045) and in applying pressure effectively to control bleeding (p = 0.037).
However, some procedural components, such as locating the radial pulse and using the one-hand technique, did not show statistically significant improvement (p = 1.000 and p = 0.168, respectively).
Overall, these findings indicate that the intervention improved learner confidence, particularly in technical components of radial arterial puncture.
Participant Satisfaction with the Arterial Puncture Part-Task Trainer
Table 4 demonstrates that participants were generally satisfied with the arterial puncture part-task trainer.
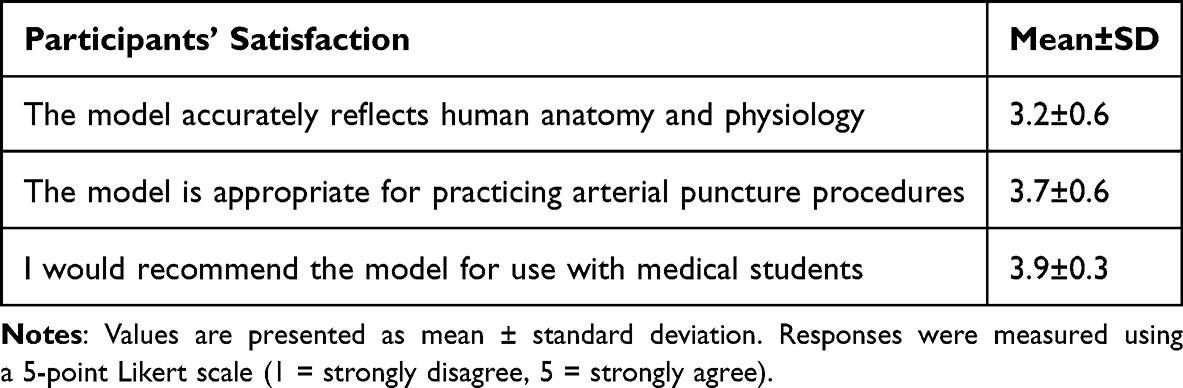 |
Table 4 Participant Satisfaction with the Arterial Puncture Part-Task Trainer |
The model’s anatomical realism received a mean score of 3.2 ± 0.6, indicating moderate satisfaction, although participants suggested potential improvements.
For example, participants noted that the vessels appeared slightly larger and softer than those encountered in real patients and that additional anatomical structures such as veins, bones, and simulated blood flow could enhance realism.
The model’s suitability for practicing radial arterial puncture received a mean score of 3.7 ± 0.6, reflecting strong satisfaction with its use as a training tool.
The highest rating was observed for its potential use in medical education (mean score 3.9 ± 0.3), demonstrating strong support for incorporating this simulator into procedural skills training for medical students.
Discussion
This study compared the arterial puncture skills of fifth-year medical students trained with an arterial puncture part-task trainer simulator to those trained using conventional methods. The results demonstrated significantly higher total mean scores for the group trained with the simulator, indicating that the intervention positively impacted participants’ performance, particularly in essential skills such as needle positioning and blood collection techniques. Training with the part-task trainer proved to be a more effective method, allowing students to develop a stronger understanding of the necessary skills compared to traditional training approaches.
In addition to skill improvement, the intervention significantly enhanced participants’ self-confidence. Students reported substantial improvements in specific skills, such as needle angle positioning and bleeding control. This suggests that hands-on practice with the simulator not only enhances technical proficiency but also fosters a sense of competence and readiness.
The importance of confidence in clinical practice has been well documented. A previous study by Shbeer et al found that simulation significantly enhanced students’ self-confidence.10 Simulated environments allow students to practice skills and gain hands-on experience without the risks associated with real patient care. Additionally, simulation provides a safe space for students to make mistakes, learn from them, and refine their skills without compromising patient safety. Moreover, simulation-based training has been shown to improve students’ readiness to perform procedures in real-life scenarios, reducing anxiety and enhancing overall clinical performance.6,10,11
Participants expressed strong satisfaction with the arterial part-task trainer, rating its suitability for practicing radial arterial puncture and its potential use in medical education. This positive feedback highlights the trainer’s perceived value, with many participants advocating for its incorporation into medical curricula and clinical training. The arterial puncture part-task trainer is made from natural rubber, which can be locally produced in Thailand, making it a cost-effective solution. In contrast, similar models imported from abroad—capable of simulating pulse palpation and adjusting pulse speed and strength—are significantly more expensive, costing up to ten times more. This comparison underscores the affordability and practicality of the locally produced trainer.12,13
Based on the Kirkpatrick Model, participants were highly satisfied with the arterial puncture part-task trainer, and participants trained with the simulator achieved significantly higher skill scores.14 According to the Kirkpatrick Model of training evaluation, the present findings primarily represent Level 1 (learner reaction and satisfaction) and Level 2 (learning outcomes reflected by improved procedural skills and self-confidence). However, evidence for Level 3 behavioral change in clinical practice and Level 4 patient outcomes remains limited and requires further investigation in larger studies.
It should also be noted that participants in the intervention group received additional simulator training and a follow-up reassessment two weeks later. Therefore, part of the observed improvement in performance may reflect the additional practice exposure rather than the simulator intervention alone.
Another factor to consider is the difference in patient body mass index (BMI) between the two groups. Higher BMI may increase the technical difficulty of radial arterial puncture due to deeper vessel location and reduced palpation accuracy. Interestingly, the intervention group encountered patients with a higher mean BMI yet still demonstrated superior performance. A sensitivity analysis adjusting for BMI did not substantially alter the main findings; however, this imbalance should be considered when interpreting the results.
Radial artery puncture is a high-risk and technically challenging procedure. Therefore, medical students should receive structured training and competency assessment before performing radial arterial punctures on live patients. Training with an arterial puncture part-task trainer provides students with the opportunity to develop essential procedural skills in a safe environment. This approach enhances technical proficiency, improves learner confidence, and promotes better preparedness for performing arterial punctures in real clinical settings.
Limitations
This study has several notable limitations. Firstly, this pilot trial was conducted at a single medical center and involved a relatively small sample of fifth-year medical students at Ramathibodi Hospital between January 26, 2024, and April 11, 2024. Because the final sample size (n = 22) did not reach the calculated requirement, the study may have been underpowered to detect differences in some clinical outcomes.
Secondly, the intervention group received additional simulator training and a follow-up reassessment, which may introduce a practice effect that could partially influence the observed improvement in performance.
Thirdly, the reassessment period was limited to two weeks, which only allows evaluation of short-term learning retention. Long-term skill retention was not assessed.
Future studies should include larger multi-center cohorts and longer follow-up periods to confirm these findings and improve the generalizability of simulation-based training for arterial puncture.
Conclusion
This pilot trial demonstrated that the use of an arterial puncture part-task trainer simulator was associated with short-term improvements in overall performance and specific technical skills compared with traditional training methods. The results highlight the value of simulator-based training in enhancing the technical proficiency and self-confidence of medical students when learning complex procedures such as radial arterial blood gas puncture.
Although improvements in procedural skill scores were observed, no statistically significant difference was found in first-attempt success rates, which may reflect the limited statistical power of this pilot study. Therefore, these findings should be interpreted as preliminary evidence of educational benefit rather than definitive improvement in clinical outcomes.
Using Artificial Intelligence Chatbots
During the preparation of this work, the author(s) utilized ChatGPT-4.0 to check and correct grammatical errors during the manuscript writing process. After using this tool, the author(s) reviewed and edited the content as necessary and take full responsibility for the content of the publication.
Clinical Trial Registration
This study was registered in the Thai Clinical Trials Registry (TCTR) with the registration number TCTR20250325003. The registry can be accessed at: https://www.thaiclinicaltrials.org/show/TCTR20250325003.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Considerations
The Institutional Review Board of the Faculty of Medicine at Ramathibodi Hospital granted ethical approval for this experimental investigation, with the approval code COA MURA2023/264. Each participant provided written informed consent in accordance with the ethical principles governing research involving human subjects, as outlined in the Declaration of Helsinki.
Acknowledgments
The authors would like to express my gratitude to Lunlita Chukaew, Panitiporn Saikaew, and Piramon Chairattanawan for their encouragement and invaluable assistance, which made this journey more enjoyable. Additionally, they wish to acknowledge the Rubber Authority of Thailand for providing essential resources and support for this project.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Rubber Authority of Thailand (Budget: 450,000 Baht).
Disclosure
The authors declare that they have no competing interests.
References
1. Dev SP, Hillmer MD, Ferri M. Arterial puncture for blood gas analysis. N Engl J Med. 2011;364(5):e7. doi:10.1056/NEJMvcm0803851
2. Awasthi S, Rani R, Malviya D. Peripheral venous blood gas analysis: an alternative to arterial blood gas analysis for initial assessment and resuscitation in emergency and intensive care unit patients. Anesth Essays Res. 2013;7(3):355–12. doi:10.4103/0259-1162.123234
3. Tienpratarn W, Yuksen C, Chukaew L, Jenpanitpong C, Triganjananun C, Seesuklom S. Point-of-Care Testing (POCT) for blood gas and electrolyte analysis in out-of-hospital cardiac arrests’ management; a cross-sectional study. Arch Acad Emerg Med. 2025;13(1):e32. doi:10.22037/aaemj.v13i1.2590
4. WHO guidelines on drawing blood: best practices in phlebotomy. Geneva: WHO Guidelines Approved by the Guidelines Review Committee; 2010.
5. Kang JS, Lee TR, Cha WC, et al. Finger necrosis after accidental radial artery puncture. Clin Exp Emerg Med. 2014;1(2):130. doi:10.15441/ceem.14.045
6. Elendu C, Amaechi DC, Okatta AU, et al. The impact of simulation-based training in medical education: a review. Medicine. 2024;103(27):e38813. doi:10.1097/MD.0000000000038813
7. Shi J, Mo X, Sun Z. Content validity index in scale development. J Central South Univ. 2012;37(2):152–155.
8. Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. 2016;15(2):155–163. doi:10.1016/j.jcm.2016.02.012
9. Sullivan GM, Feinn R. Using effect size—or why the P value is not enough. J Grad Med Educ. 2012;4(3):279–282. doi:10.4300/JGME-D-12-00156.1
10. Shbeer A. Evaluating student satisfaction and self-confidence in simulation-based anesthesiology training among final-year medical students. Healthcare. 2024;12(15):1521. doi:10.3390/healthcare12151521
11. Hernández-Padilla J, Granero-Molina J, Hernández VV, Cortés-Rodríguez A, Fernández-Sola C. Efeitos de um workshop de simulação sobre a competência em punção arterial de estudantes de enfermagem [Effects of a simulation-based workshop on nursing students’ competence in arterial puncture]. Acta Paulista de Enfermagem. 2016;29:678–685. Portuguese. doi:10.1590/1982-0194201600095
12. Simulab Corporation. Ultrasound ArterialLine & ABG Trainer. 2024. Available from: https://simulab.com/products/ultrasound-arterialine-abg-trainer-1.
13. Nasco Healthcare. Nasco - Life/form Arterial Puncture Arm Light. 2024. Available from: https://shop.nascohealthcare.com/products/lf00995?pr_prod_strat=e5_desc&pr_rec_id=4e338532e&pr_rec_pid=4456699494455&pr_ref_pid=4457045786679&pr_seq=uniform.
14. Quinton ML, Tidmarsh G, Parry BJ, Cumming J. A Kirkpatrick model process evaluation of reactions and learning from my strengths training for life™. Int J Environ Res Public Health. 2022;19(18):11320. doi:10.3390/ijerph191811320
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.