Back to Journals » Journal of Hepatocellular Carcinoma » Volume 10
Comparison of Ablation Volume Between Emprint® and Mimapro® Systems for Hepatocellular Carcinoma –A Preliminary Study
Authors Ishikawa T ![]() , Hasegawa I, Hirosawa H, Honmou T, Sakai N, Igarashi T, Yamazaki S, Kobayashi T, Sato T, Iwanaga A, Sano T, Yokoyama J, Honma T
, Hasegawa I, Hirosawa H, Honmou T, Sakai N, Igarashi T, Yamazaki S, Kobayashi T, Sato T, Iwanaga A, Sano T, Yokoyama J, Honma T ![]()
Received 29 March 2023
Accepted for publication 31 May 2023
Published 22 June 2023 Volume 2023:10 Pages 979—985
DOI https://doi.org/10.2147/JHC.S412642
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Xin Wei Wang
Toru Ishikawa,1 Iori Hasegawa,2 Hiroshi Hirosawa,2 Tsubasa Honmou,2 Nobuyuki Sakai,2 Takanori Igarashi,1 Shun Yamazaki,1 Takamasa Kobayashi,1 Toshifumi Sato,1 Akito Iwanaga,1 Tomoe Sano,1 Junji Yokoyama,1 Terasu Honma1
1Department of Gastroenterology, Saiseikai Niigata Hospital, Niigata, Japan; 2Department of Clinical Engineering, Saiseikai Niigata Hospital, Niigata, Japan
Correspondence: Toru Ishikawa, Department of Gastroenterology, Saiseikai Niigata Hospital, Teraji 280-7, Niigata, Japan, Tel +81-25-233-6161, Fax +81-25-233-8880, Email [email protected]
Background: Microwave ablation (MWA) is a standard percutaneous local therapy for hepatocellular carcinoma (HCC). Next-generation MWA is reported to create a more spherical ablation zone than radiofrequency ablation (RFA). We compared the ablation zone and aspect ratio of two 2.45 GHz MWA ablation probes; Emprint® (13G) and Mimapro® (17G). We compared the ablation zone to the applied energy after MWA in patients with hepatocellular carcinoma (HCC). Furthermore, we investigated local recurrence.
Materials and Methods: We included 20 patients with HCC, with an average tumour diameter of 33.2 ± 12.2 mm, who underwent MWA using Emprint®, and 9 patients who underwent MWA using Mimapro® with an average tumour diameter of 31.1 ± 10.5 mm. Both groups underwent the same ablation protocol using the same power settings. The images obtained after MWA showed the treatment ablation zone and aspect ratio, which were measured and compared using three-dimensional image analysis software.
Results: The aspect ratios in the Emprint® and Mimapro® groups were 0.786 ± 0.105 and 0.808 ± 0.122, respectively, with no significant difference (p = 0.604). The ablation time was significantly shorter in the Mimapro® group than in the Emprint® group, and there was no significant difference in the frequency of popping or the ablation volume. There were no significant differences in local recurrence between the two groups.
Conclusion: There was no significant difference in the aspect ratios of the ablation diameter, and the ablation zone was almost spherical in both cases. Mimapro® at 17G was less invasive than Emprint® at 13G.
Keywords: hepatocellular carcinoma, microwave ablation, ablation zone
Introduction
Hepatocellular carcinoma (HCC) was the sixth most commonly diagnosed cancer and the third leading cause of cancer-related deaths worldwide in 2020.1 The treatment policy in Japan is based on the consensus-based Clinical Practice Guidelines for HCC management proposed by the Japan Society of Hepatology.2 Radiofrequency ablation (RFA) or surgical resection is recommended for patients with 1 to 3 tumours of ≤ 3 cm.2 Microwave ablation (MWA) is a recent development in the field of tumour ablation that uses electromagnetic waves to establish a microwave near-field with direct tissue heating.
MWA is minimally invasive compared with conventional surgery and is easy to use for repeated treatment, achieving a high complete ablation rate. MWA is a good alternative treatment option for patients who are unwilling or unable to undergo surgery. The major advantages of ultrasound-guided MWA include real-time monitoring, accurate guidance and targeting of the tumour, minimal tissue trauma and damage, higher safety, and the ability to reach a larger target area than RFA.3,4
However, early versions of MWA suffered from ablation zone predictability issues. New generations of MWA, including Emprint® (a 2450 MHz 100 W generator model) (Emprint® ablation system, Covidien/Medtronic, Minneapolis, MN, USA) and Mimapro® (MTC‑3C microwave generator and a 20‑cm‑long, 17G cooled‑shaft electrode probe) (Mima-pro Scientific Inc. Nantong, China), are commonly used in Japan for MWA in patients with HCC and have recently helped address these issues.5,6
Owing to the high risk of HCC recurrence, it is essential to ensure that the ablation zone is sufficient. In particular, it is important to be able to cauterise spherically. However, it is unclear whether there is a difference in the performance between the Emprint® and Mimapro® systems.
In this study, we compared the Emprint® and Mimapro® MWA systems regarding the ablation zone and local recurrence in patients with HCC.
Materials and Methods
Patient Population
In this study, we analysed patients who underwent percutaneous ultrasonography-guided MWA for HCC at our hospital from January 2017 to June 2022.
HCC was diagnosed using dynamic computed tomography (CT) or dynamic magnetic resonance imaging, or both, in accordance with the consensus-based Clinical Practice Guidelines for HCC.
All patient’s conditions were discussed at a multidisciplinary tumour board meeting in which the decision to use US-guided MWA was made. Patients were included in this study if they (1) Were treated for HCC and (2) Were treated with either an Emprint® device or a Mimapro® device. The decision regarding which device to use depended on the operator.
Patients were excluded if (1) They were previously treated for MWA site recurrence, (2) There was an inability to separate the ablation zones of multiple tumours located close to each other, (3) They did not have contrast-enhanced CT (CE-CT) scans, (4) there was an unclear demarcation of the tumour on CE-CT, (5) There was missing energy data, and (6) They underwent simultaneous multi-probe ablations.
First, we assessed the electrode ablation zones of the Emprint® and Mimapro® systems. Next, we investigated local recurrence in patients who underwent MWA using the Emprint® MWA system (Emprint® group) and those who underwent MWA using the Mimapro® MWA system (Mimapro® group). After MWA treatment, patients were followed up every 6–8 weeks until June 2022.
MWA Procedure
MWA was performed using the Emprint® or Mimapro® MWA system with an antenna. All MWA sessions were conducted using a percutaneous approach under ultrasound guidance (LOGIQ E9 XD clear 2.0; GE Healthcare, Chicago, IL, USA). During MWA, patients underwent intravenous conscious sedation, and their vital signs were continuously monitored.
The output energy during MWA was gradually increased from 45 W for 60 sec to 60 W for 60 sec, 75 W for 60 sec, and then 100 W until the end of the treatment. Treatments were terminated when the ablation margin was included in the hyperechoic area on the ultrasound screen.
After ablation of the tumour, the antenna was slowly withdrawn (1 cm at a time), and MWA emission was continued at a power of 20 W until the antenna was pulled to just under the skin entrance site. This method allowed needle-tract cauterisation to prevent tumour seeding and minimise bleeding after ablation.
Follow-Up
The follow-up period was calculated starting from the beginning of MWA in all patients. Patients underwent CE-CT examinations 1 month after MWA, every 3 months in the first year, and every 6 months thereafter.
Local tumour progression was defined as the appearance of a tumour at the edge of the ablation zone.7
Furthermore, we determined the biggest and smallest diameters of the ablated zone.
Following a medical image analysis procedure (SYNAPSE VINCENT ver3.0.), a three-dimensional reconstruction of tumour volume was performed using volumetry.
Complications
Treatment complications were described according to the reporting standards of the Society of Interventional Radiology (SIR).8
Major complications were defined as events that led to substantial morbidity and disability that increased the level of care, resulted in hospital admission, or substantially lengthened the hospital stay (SIR classifications C–E). This included any case in which a blood transfusion or interventional drainage procedure was required. All other complications were considered minor.
Ethical Considerations
This study was approved by the Institutional Review Board of Saiseikai Niigata Hospital (No. E18-18) and conducted in accordance with the principles of the Declaration of Helsinki (as revised in 2013). Before participating in this study, written informed consent was provided by all patients.
Statistical Analyses
All statistical analyses were performed using EZR (version 1.54; Saitama Medical Center, Jichi Medical University), a graphical user interface for R (version 4.0.3; R Foundation for Statistical Computing, https://www.r-project.org, accessed on 10 January 2022). EZR is a modified version of R commander version 2.7–1 that includes statistical functions frequently used in biostatistics.9 Results were expressed as medians and interquartile ranges. Differences between the groups (continuous variables) were analysed using the Mann–Whitney U-test, whereas categorical data were analysed using Fisher’s exact test. A two-tailed p < 0.05 was considered statistically significant.
Results
Patient Characteristics
Patient characteristics are shown in Table 1. The study population consisted of 21 males and 8 females. Age, aetiology, tumour diameter, and tumour location were not significantly different between the Emprint® and Mimapro® groups.
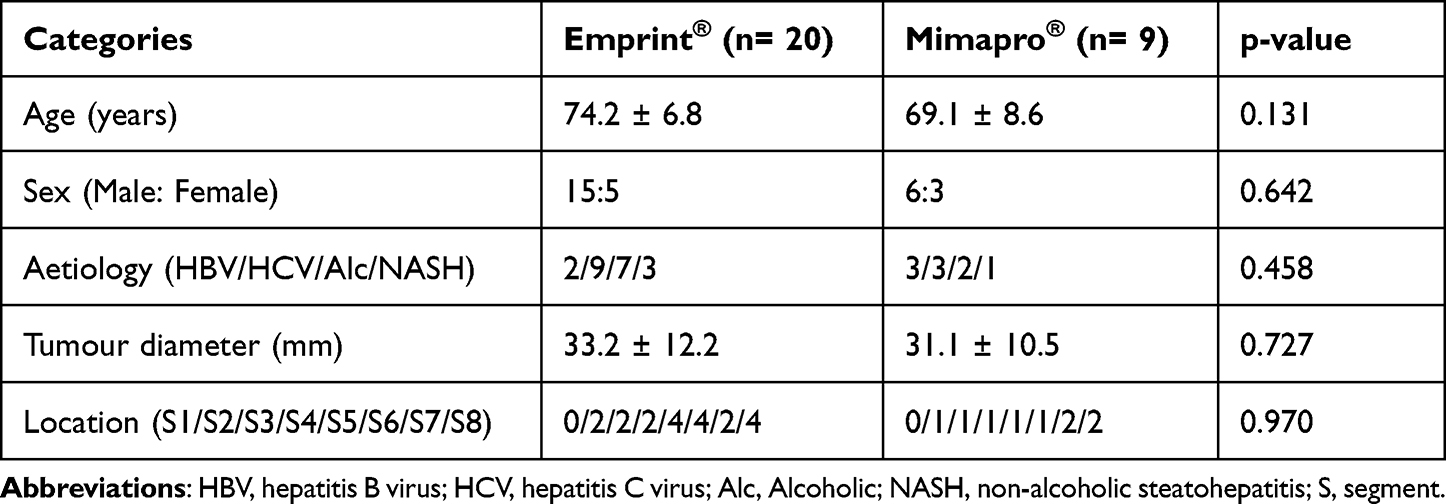 |
Table 1 Clinicopathological Characteristics |
Comparison of Ablation Zone
The aspect ratios were 0.786 ± 0.105 and 0.808 ± 0.122 in the Emprint® and Mimapro® groups, respectively, with no significant difference (p = 0.604) (Table 2).
 |
Table 2 Ablation Outcome Parameters by Device |
There was no significant difference in the ablation volume between the two groups (p = 0.186) (Table 2).
Popping Phenomena
There was no significant difference in the frequency of popping between the groups (p = 0.396) (Table 2).
Recurrence-Free Survival
During the follow-up period, local tumour recurrence occurred in 6 patients (20.6%) and did not occur in 23 patients (79.4%).
In the Emprint® group, local tumour recurrence occurred in 4 patients (20.0%). In contrast, local tumour recurrence occurred in 2 patients (22.2%) in the Mimapro® group. Recurrence-free survival was not significantly different between the groups. No significant difference was observed between the groups’ local recurrence rates (Figure 1).
 |
Figure 1 Kaplan–Meier curves depicting local tumour control over time based on microwave ablation devices. No significant difference was observed in the local recurrence rates between the groups. |
Adverse Events
Ablation-related complications, including pain, fever, and fatigue, were observed in 50.0% (10/22) of patients in the Emprint® group and 33.3% (3/9) of patients in the Mimapro® group (p = 0.403); these symptoms were alleviated after symptom-mitigating treatment. No tumour seeding was observed along the MWA needle tracts. No ablation-related deaths occurred in our study.
Discussion
Treatment for hepatocellular carcinoma is expected to treat various tumour stages due to advances in systemic drug therapy, including immune checkpoint inhibitors10–13 and the position of MWA is also being discussed. However, during the course of systemic chemotherapy, ablation is expected as, well as resection as a conversion treatment.
In this context, more effective targeting of MWA, which has a higher possibility of local control than RFA among ablation, is important.
In this study, we evaluated patients with HCC who underwent MWA at our hospital. The Emprint® MWA and Mimapro® MWA systems were used. Patients in the Emprint® and Mimapro® groups were compared.
MWA is a thermal ablation modality based on increasing the temperature above the normal physiological threshold to kill cancer cells with minimal damage to surrounding tissues.14–19
The aspect ratios of both the Emprint® and Mimapro® groups were similar to the clinical results of experiments with excised bovine livers, and nearly spherical ablation volumes were obtained. However, the Emprint® antenna probe is only 13G, whereas Mimapro® has three types: 14G, 17G, and 18G. In particular, 17G Mimapro® has approximately the same thickness as RFA and can cauterise more spherically than RFA. Next-generation MWA is less susceptible to heat sinks (blood flow in blood vessels) and may lead to a wider area of ablation than that expected from RFA.
While MWA was developed to overcome many of the issues of RFA, the initial systems suffered from the predictability of ablation zone issues.5,6,20–24
Emprint® was developed as a new next-generation MWA system using thermosphere technology. MWA can create predictable spherical zones of ablation by incorporating thermal, field, and wavelength control technologies into the system.
Human data concerning MWA have shown good clinical outcomes. More data is necessary on the accuracy of the manufacturer-provided ablation zone model for predicting in vivo human results.
In this study, we compared Emprint® MWA (13G) and Mimapro® MWA (17G) as next-generation MWAs.
The aspect ratio was not significantly different between the Emprint® and Mimapro® groups; however, the Mimapro® gauge was thinner than the Emprint® gauge.
The ablation time was significantly shorter in the Mimapro® group, and there was no significant difference in the frequency of popping or the ablation volume. Furthermore, there were no significant differences in local recurrence between the groups.
The study’s limitations included, firstly, inevitable selection biases in the study population owing to its retrospective nature, single-centre design, and small sample size. Secondly, the inability to assess therapeutic efficacy; thus, there is an urgent need for controlled clinical trials to compare this therapeutic modality with surgical resection or other percutaneous local treatments. Thirdly, a study on conversion after systemic chemotherapy has not been conducted. Fourthly, not only the systemic chemotherapy but also the therapeutic effect when used in combination with transarterial chemoembolization (TACE) has not been investigated at this time. Finally, the follow-up period was inadequate.
In conclusion, there were no significant differences in the ablation diameter and volume aspect ratios between the two groups, and the ablation zone was almost spherical in both cases.
Hence, irrespective of the 17G Mimapro® being thinner than the 13G Emprint®, the same ablation volume was obtained. MWA using Mimapro® or Emprint® is expected to be useful as a minimally invasive technique in the future; nevertheless, long-term studies should be conducted.
Acknowledgments
The Authors would like to thank Editage (www.editage.com) for English language editing.
Author Contributions
All authors made a significant contribution to the work, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; they took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; agreed to submit to the current journal; and agreed to be accountable for all aspects of the work.
Disclosure
The authors have no conflicts of interest to declare in relation to this study.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71:209–249.
2. Kudo M, Kawamura Y, Hasegawa K, et al. Management of hepatocellular carcinoma in Japan: JSH consensus statements and recommendations 2021 update. Liver Cancer. 2021;10(3):181–223. Epub 2021 May 19. PMID: 34239808. doi:10.1159/000514174
3. Parkin DM, Bray F, Ferlay J, et al. Global cancer statistics, 2002. CA Cancer J Clin. 2005;55(2):74–108.
4. Poulou LS, Botsa E, Thanou I, et al. Percutaneous microwave ablation vs radiofrequency ablation in the treatment of hepatocellular carcinoma. World J Hepatol. 2015;7:1054–1063. doi:10.4254/wjh.v7.i8.1054
5. Cornelis FH, Marcelin C, Bernhard JC. Microwave ablation of renal tumors: a narrative review of technical considerations and clinical results. Diagn Interv Imaging. 2017;98:287–297. doi:10.1016/j.diii.2016.12.002
6. Brace CL. Microwave tissue ablation: biophysics, technology, and applications. Crit Rev Biomed Eng. 2010;38(1):65–78. doi:10.1615/CritRevBiomedEng.v38.i1.60
7. Ahmed M, Solbiati L, Brace CL; International Working Group on Image-guided Tumor Ablation; Interventional Oncology Sans Frontières Expert Panel; Technology Assessment Committee of the Society of Interventional Radiology; Standard of Practice Committee of the Cardiovascular and Interventional Radiological Society of Europe. Image-guided tumor ablation: standardization of terminology and reporting criteria-a 10-year update. Radiology. 2014;273(1):241–260. Epub 2014 Jun 13. PMID: 24927329. doi:10.1148/radiol.14132958
8. Sacks D, McClenny TE, Cardella JF, Lewis CA. Society of interventional radiology clinical practice guidelines. J Vasc Interv Radiol. 2003;14(9 Pt 2):S199–S202. doi:10.1097/01.RVI.0000094584.83406.3e
9. Kanda Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013;48(3):452–458. PMID: 23208313. doi:10.1038/bmt.2012.244
10. Rizzo A, Ricci AD, Di Federico A, et al. Predictive biomarkers for checkpoint inhibitor-based immunotherapy in Hepatocellular Carcinoma: where do we stand? Front Oncol. 2021;11:803133. PMID: 34976841. doi:10.3389/fonc.2021.803133
11. Viscardi G, Tralongo AC, Massari F, et al. Comparative assessment of early mortality risk upon immune checkpoint inhibitors alone or in combination with other agents across solid malignancies: a systematic review and meta-analysis. Eur J Cancer. 2022;177:175–185. PMID: 36368251. doi:10.1016/j.ejca.2022.09.031
12. Di Federico A, Rizzo A, Carloni R, et al. Atezolizumab-bevacizumab plus Y-90 TARE for the treatment of hepatocellular carcinoma: preclinical rationale and ongoing clinical trials. Expert Opin Investig Drugs. 2022;31:361–369. PMID: 34798793. doi:10.1080/13543784.2022.2009455
13. Rizzo A, Cusmai A, Gadaleta-Caldarola G, et al. Which role for predictors of response to immune checkpoint inhibitors in hepatocellular carcinoma? Expert Rev Gastroenterol Hepatol. 2022;16(4):333–339. PMID: 35403533. doi:10.1080/17474124.2022.2064273
14. Abdelaziz AO, Nabeel MM, Elbaz TM, et al. Microwave ablation versus transarterial chemoembolization in large hepatocellular carcinoma: prospective analysis. Scand J Gastroenterol. 2015;50:479–484. doi:10.3109/00365521.2014.1003397
15. Zaidi N, Okoh A, Yigitbas H, et al. Laparoscopic microwave thermosphere ablation of malignant liver tumors: an analysis of 53 cases. J Surg Oncol. 2016;113(2):130–134. doi:10.1002/jso.24127
16. Itoh S, Ikeda Y, Kawanaka H, et al. Efficacy of surgical microwave therapy in patients with unresectable hepatocellular carcinoma. Ann Surg Oncol. 2011;18(13):3650–3656. doi:10.1245/s10434-011-1831-z
17. Berber E. Laparoscopic microwave thermosphere ablation of malignant liver tumors: an initial clinical evaluation. Surg Endosc. 2016;30(2):692–698. doi:10.1007/s00464-015-4261-3
18. Facciorusso A, Abd El Aziz MA, Tartaglia N, et al. Microwave ablation versus radiofrequency ablation for treatment of Hepatocellular Carcinoma: a meta-analysis of randomized controlled trials. Cancers. 2020;12(12):3796. doi:10.3390/cancers12123796
19. Poggi G, Tosoratti N, Montagna B, Picchi C. Microwave ablation of hepatocellular carcinoma. World J Hepatol. 2015;7:2578–2589. doi:10.4254/wjh.v7.i25.2578
20. Bleicher RJ, Allegra DP, Nora DT, et al. Radiofrequency ablation in 447 complex unresectable liver tumors: lessons learned. Ann Surg Oncol. 2003;10:52–58. doi:10.1245/ASO.2003.03.018
21. Crocetti L, de Baere T, Lencioni R. Quality improvement guide-lines for radiofrequency ablation of liver tumours. Cardiovasc Intervent Radiol. 2010;33:11–17. doi:10.1007/s00270-009-9736-y
22. Wright AS, Sampson LA, Warner TF, et al. Radiofrequency versus microwave ablation in a hepatic porcine model. Radiology. 2005;236:132–139. doi:10.1148/radiol.2361031249
23. Awad MM, Devgan L, Kamel IR, et al. Microwave ablation in a hepatic porcine model: correlation of CT and histopathologic findings. HPB. 2007;9(5):357–362. doi:10.1080/13651820701646222
24. Yu J, Liang P, Yu X, et al. A comparison of microwave ablation and bipolar radiofrequency ablation both with an internally cooled probe: results in ex vivo and in vivo porcine livers. Eur J Radiol. 2011;79(1):124–130. doi:10.1016/j.ejrad.2009.12.009
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Machine Learning Model Based on Health Records for Predicting Recurrence After Microwave Ablation of Hepatocellular Carcinoma
An C, Yang H, Yu X, Han Z, Cheng Z, Liu F, Dou J, Li B, Li Y, Li Y, Yu J, Liang P
Journal of Hepatocellular Carcinoma 2022, 9:671-684
Published Date: 28 July 2022
Clinical Results, Risk Factors, and Future Directions of Ultrasound-Guided Percutaneous Microwave Ablation for Hepatocellular Carcinoma
Dong TT, Wang L, Li M, Yin C, Li YY, Nie F
Journal of Hepatocellular Carcinoma 2023, 10:733-743
Published Date: 15 May 2023
Hepatocellular Carcinoma with Radiological Progression: Lenvatinib Plus PD-1 Inhibitor Combined with Microwave Ablation and Synchronous Transarterial Chemoembolization
Shi Q, Huang P, Zhang Z, Zhang W, Liu L, Yan Z
Journal of Hepatocellular Carcinoma 2023, 10:1861-1871
Published Date: 21 October 2023
Prediction of Tumor Progression After Microwave Ablation of Hepatocellular Carcinoma by Contrast-Enhanced Ultrasound Combined with Immunohistochemical Markers
Dong TT, Li M, Li YY, Yin C, Nie F
Journal of Hepatocellular Carcinoma 2026, 13:539184
Published Date: 24 February 2026
Impact of Microwave Ablation on Growth Kinetics of Residual versus Synchronous Untreated Hepatocellular Carcinoma: A Retrospective Cohort Study
Yi W, Pang C, Xue J, Zhang Y, Chen X, Luo T, Zhang D, Gao X, Yu J, Liang P
Journal of Hepatocellular Carcinoma 2026, 13:603442
Published Date: 4 June 2026