Back to Journals » Medical Devices: Evidence and Research » Volume 19
Comparing Post-Occlusion Surge at Decreasing Intraocular Pressures with Pressure Sensing Handpiece
Authors Montgomery JA, Soule C ![]() , Sherbotie N
, Sherbotie N ![]() , Cardenas IA
, Cardenas IA ![]() , Jensen JL
, Jensen JL ![]() , Bell JA
, Bell JA ![]() , Barlow Jnr WR
, Barlow Jnr WR ![]() , Klug K, Wagner L, Pettey JH
, Klug K, Wagner L, Pettey JH ![]()
Received 27 December 2025
Accepted for publication 29 May 2026
Published 26 June 2026 Volume 2026:19 592098
DOI https://doi.org/10.2147/MDER.S592098
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mohamad Bashir
Jessie A Montgomery,1,2 Coby Soule,1,2 Nathan Sherbotie,1,2 Ivan A Cardenas,1,2 Jenna L Jensen,1,2 Jacob A Bell,1,2 William R Barlow Jnr,1 Kolja Klug,3 Lincoln Wagner,3 Jeff H Pettey1
1Department of Ophthalmology and Visual Sciences, John A Moran Eye Center, University of Utah, Salt Lake City, UT, USA; 2School of Medicine, University of Utah, Salt Lake City, UT, USA; 3Department of Engineering, Center for Medical Innovation, University of Utah, Salt Lake City, UT, USA
Correspondence: Jeff H Pettey, Department of Ophthalmology and Visual Sciences, John A Moran Eye Center, University of Utah, Salt Lake City, UT, USA, Tel +1 801 581 2352, Fax +1 801 581 3357, Email [email protected]
Purpose: To compare post-occlusion surge pressure at various intraocular pressures using the Active Sentry handpiece.
Methods: This experimental (in vitro chamber) study used the Alcon Centurion platform and Active Sentry handpiece with balanced tips. Quad preset was used with settings: vacuum 500 mmHg, aspiration flow 50 mmHg, and IOPs of 30, 50, and 70 mmHg. A rubber disk was fixed within a sealed chamber fitted with an electric pressure sensor to monitor pressure changes. The phacoemulsification tip was inserted into the water-tight port of the pressure chamber, and the foot pedal was set to position two. The tip was put in contact with the disk to replicate tip occlusion and pulled from the disk to simulate occlusion break. Ten trials were performed at each IOP; pressure changes were recorded continuously.
Results: At 70 mmHg IOP, average post-occlusion surge magnitude was 5.76 mmHg ± 0.54; average surge duration was 0.45 s ± 0.10. At 50 mmHg IOP, surge magnitude was 5.76 mmHg ± 1.15; surge duration surge was 0.52 s ± 0.23. At 30 mmHg IOP, surge magnitude was 10.46 mmHg ± 2.86; surge duration was 1.27 s ± 0.51. There was a statistically significant difference between surge magnitude and duration at 30 vs. 50 mmHg IOP (P < 0.05) and at 30 vs. 70 mmHg IOP (P < 0.05).
Conclusion: When utilizing the Active Sentry handpiece, an increased surge risk was not observed when operative IOP was decreased from 70 mmHg to 50 mmHg. However, our data suggest that surge risk increases when operative IOP is decreased to 30 mmHg. The Active Sentry handpiece at 50 mmHg IOP would not introduce greater surge risk than at 70 mmHg IOP.
Plain Language Summary: Cataracts are most frequently removed with a procedure called phacoemulsification. Though phacoemulsification is safe and effective, there are some serious risks, such as breakage of the eye’s back capsule. One of the events that can lead to this breakage is a post-occlusion surge, in which there is a drop in pressure after clearing of the blockage of the phaco probe. Because of this, it is important to use settings on the phacoemulsification machine that balance an “intraocular pressure” (pressure within the eye) that is high enough to decrease the risk of eye damage, but low enough to avoid excess internal eye inflammation.
This study seeks to understand how a phacoemulsification handpiece that is designed to allow for tighter control of intraoperative intraocular pressure will impact post-occlusion surge when operating at lower intraocular pressures.
Using a specially designed chamber, this handpiece was tested at different intraocular pressure settings: 30, 50, and 70 mmHg. We found that when using the handpiece at an intraocular pressure of 50 vs. 70 mmHg, there was no difference in post-occlusion surge. However, there was an increase in post-occlusion surge when using the handpiece at an intraocular pressure of 30 vs. 50 mmHg and 30 vs. 70 mmHg. This suggests that this handpiece can decrease post-occlusion surge down to an intraocular pressure of 50 mmHg, though it appears to lose this ability at an intraocular pressure between 30 and 50 mmHg.
Keywords: ultrasound energy, cataract, surge, intraocular pressure, complications
Introduction
The phacoemulsification (phaco) technique is the modern-day standard for cataract removal surgery in the US and Western Europe. The procedure is considered safe and effective, with low complication rates.1,2 However, there are serious risks of phacoemulsification including anterior chamber instability and posterior capsule rupture.3
Both complications can be precipitated by post-occlusion surge, in which there is a measurable drop in intraocular pressure (IOP) causing changes in the stability of the anterior chamber. Post-occlusion surge occurs when the tip of the phaco probe is occluded, causing an increase in vacuum power and buildup of negative pressure within the tubing. Once the phaco tip is cleared, ocular fluid is pulled into the aspiration port by the negative pressure, causing a decrease in IOP. During this period of low IOP, the anterior chamber can become shallow, or even collapse, and the posterior capsule may be pulled forward into contact with the phaco tip, which may result in a tear, termed a posterior capsular rent.4
Additionally, there is evidence that operating at a lower IOP allows for increased corneal clarity and decreased anterior chamber inflammation, as well as improved perfusion to the central retinal artery.5–7 Thus, there is an incentive to find technology that allows surgeons to operate at a low IOP while minimizing post-occlusion surge. The Active Sentry handpiece was designed to strike this balance.
The Active Sentry handpiece incorporates the irrigation pressure sensor within the handpiece itself rather than within the console. This design theoretically allows for more rapid detection of pressure changes compared to handpieces with pressor sensors within the phaco machine, minimizing post-occlusion surge and possibly allowing for operation at lower IOP. Prior research has shown that the Active Sentry handpiece, with pressor sensor within the handpiece, has a decreased magnitude and duration of surge compared to the Ozil handpiece, with pressor sensor within the machine.8 However, there are currently little data supporting the effects of surge at lower IOPs with the Active Sentry handpiece.
In order to address this gap in current research, this study used a chamber capable of measuring pressure in real time to evaluate post-occlusion surge using the Active Sentry at various IOPs. We hypothesized that by using a handpiece with built-in pressure sensor there would be quicker response times to surge events leading to decreased magnitude and duration of post-occlusion surge at lower IOPs when compared to phaco machines with a pressor sensor within the machine. We sought to compare the Active Sentry handpiece to itself at different settings to better understand and optimize settings that would reduce post-occlusion surge magnitude and duration while still minimizing intraocular pressure as is desired in cataract surgery. Additionally, we sought to determine how to optimize use and balance low IOP with minimizing surge.
Materials and Methods
This study did not involve human subjects or animals, so Institutional Review Board approval was not required.
Pressure Chamber
In partnership with a team of engineers (KK, LW), a water-tight chamber was created to allow for pressure measurements (Figure 1). An entry port at the top of the chamber allowed for insertion of the phaco handpiece into the chamber (Figure 2). A rubber sleeve was fitted around the phaco handpiece, which met the entry port and allowed for a water-tight introduction of the handpiece into the machine. A rubber disk was fixed within the chamber to model the occlusion caused by lens fragments during phaco surgery. A valve that could be opened and closed was placed at the top of the chamber to allow for the dismissal of excess air from the system and allow for pressure equilibration between experimental trials. The chamber contained a pressure sensor that collected 10 data points per second to measure pressure changes during trials.
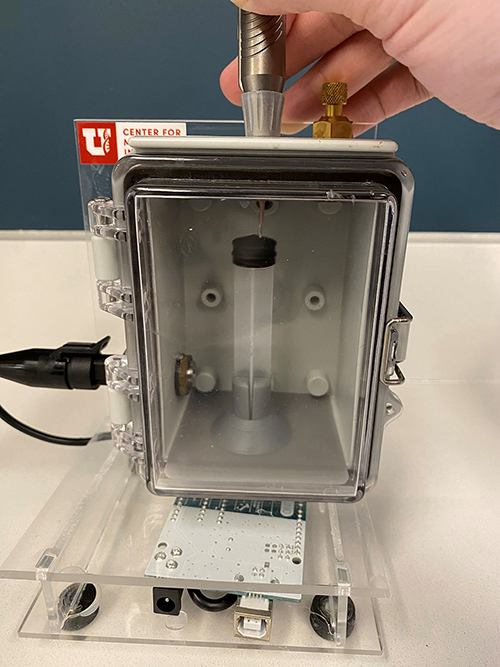 |
Figure 1 Photograph of the pressure chamber designed for and used in this experiment to simulate the intraocular environment. This was designed with the University of Utah Center for Medical Innovation. |
 |
Figure 2 Close-up photograph of the pressure chamber detailing the phacoemulsification handpiece insertion point, which seals to create a watertight barrier around the handpiece. The brass fitting serves as a bleed valve, used to evacuate air from the chamber and normalize intra-chamber pressure between trials. |
Post-Occlusion Surge Testing
Trials were run using the Quad preset with the following settings: vacuum 500 mmHg, aspiration flow 50 mmHg, and varying IOP of 30, 50, and 70 mmHg. These settings were used to reflect common vacuum and aspiration flow settings used by surgeons during chop and quadrant portions of surgery in which surge events are most likely to occur.5,9,10 Variable IOP settings were used to compare the magnitude and duration of surge as IOP decreased.
During each trial, the phaco handpiece was inserted into the water-tight port of the pressure chamber and the foot pedal was set to position 1 to fill the chamber, to get rid of remaining air, and to test the water-tight seal between the handpiece and the port.
At the beginning of each trial, the foot pedal was set to position 2 for 7 seconds to equilibrate the pressure chamber at the desired IOP. At 7 seconds, the handpiece was shifted so that the tip was occluded against the rubber stopper. Pressure changes were measured for another 7 seconds. At 14 seconds, the handpiece was shifted again to un-occlude the tip, and pressure changes were measured for an additional 7 seconds to allow for pressure equilibrium post-occlusion.
Ten trials were performed at each intraocular pressure, and pressure changes within the chamber were recorded.
This study used an in vitro method, with limitations in reflecting real eye conditions.
Data Analysis
Data were compiled in Microsoft Excel with a methodology created by Whitaker et al.10 The research team defined the beginning of post-occlusion surge as the point at which the slope of the line between adjacent points on the pressure tracing curve was more negative than −6.0. This slope was chosen to minimize random pressure fluctuations that are present due to limitations of the pressor sensor’s sensitivity. This method was first established in Dr. Whitaker’s paper.10 The end of post-occlusion surge was defined as the first positive inflection in the slope of the pressure tracing curve after the start of surge, indicating that the phaco machine had sensed the pressure drop and had halted aspiration. The pressure at the time point defined as either the beginning or ending of surge was used to calculate the magnitude of surge for each trial. We used Student’s T-test to compare each group; IOP of 70 mmHg vs IOP of 50 mmHg, IOP of 70 mmHg vs IOP of 30 mmHg, and IOP of 50 mmHg vs IOP of 30 mmHg. Statistical significance was defined as P ≤ 0.05.
The nomenclature used to describe the segments of the pressure tracing was also created by Dr. Whitaker.10 The segment from A to B details the increase in pressure that occurs when the foot pedal is set to position 2. The segment from B to C details the time during which the phaco tip is occluded. The segment from C to D details the post-occlusion surge segment containing a negative pressure period. Segment D to E details the un-occluded equilibrium with the foot position still at position 2.
Results
There was no statistically significant difference between the magnitude and duration of post-occlusion surge using the Active Sentry handpiece at an IOP of 50 mmHg vs. an IOP of 70 mmHg (P > 0.05). There was a statistically significant difference between the magnitude and duration of surge at an IOP of 30 mmHg vs. an IOP of 50 mmHg (P < 0.05). There was also a statistically significant difference between the magnitude and duration of surge at an IOP of 30 mmHg vs. an IOP of 70 mmHg (P < 0.05). At an IOP of 70 mmHg, the average magnitude of post-occlusion surge was 5.76 mmHg ± 0.54, 95% CI [6.15, 5.37] and the average duration of surge was 0.45 s ± 0.10, 95% CI [0.52, 0.38]. At an IOP of 50 mmHg, the magnitude of surge was 5.76 mmHg ± 1.15, 95% CI [6.58, 4.94] and the duration of surge was 0.52 s ± 0.23, 95% CI [0.68, 0.36]. At an IOP of 30 mmHg, the magnitude of surge was 10.46 mmHg ± 2.86, 95% CI [12.51, 8.42] and the duration of surge was 1.27 s ± 0.51, 95% CI [1.64, 0.90] (Figure 3).
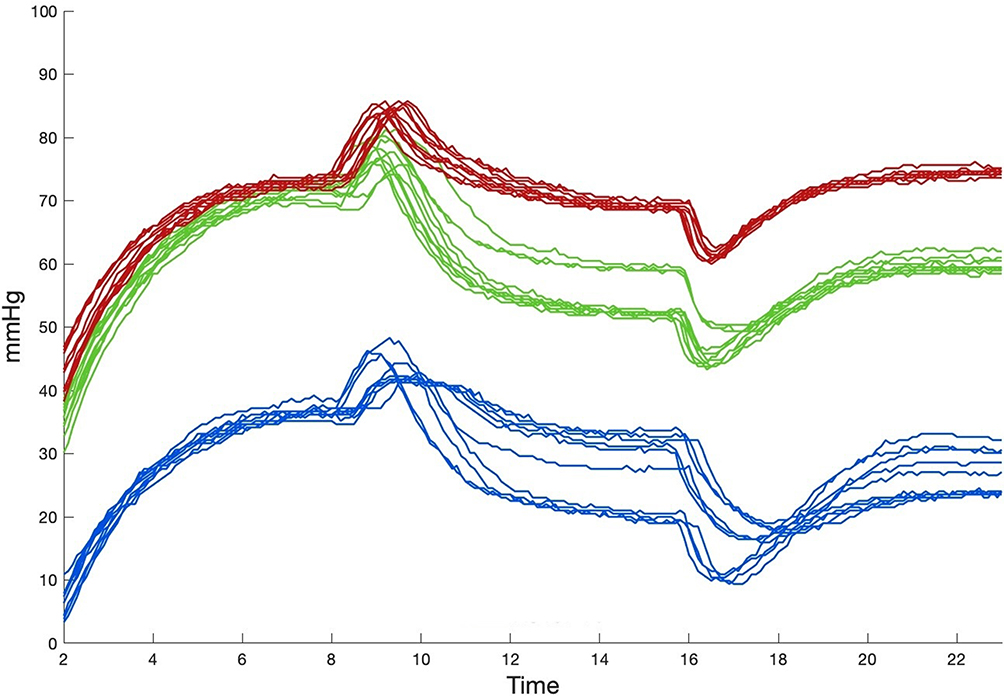 |
Figure 3 A line graph comparing the average magnitude and duration of pressure changes in mmHg during simulation of post-occlusion surge at different intraocular pressures within a chamber that models the intraocular environment at varying intraocular pressures. Blue represents an IOP of 30, green represents an IOP of 50, and red represents an IOP of 70. |
Discussion
In this experiment, we used a pressure chamber to monitor and compare the differences in the magnitude and duration of post-occlusion surge at traditional (70 mmHg) and decreasing intraocular pressures. We did this using the Active Sentry handpiece, which has a pressure sensor built into the handpiece itself. While prior research has shown that the Active Sentry handpiece does demonstrate decreased post-occlusion surge when compared to handpieces with the pressor sensor within the machine, we sought to see if post-occlusion surge could still be minimized at lower IOPs using the Active Sentry handpiece.8 Our team hypothesized that using a handpiece with a built-in pressure sensor would allow a phaco machine to respond more quickly to pressure changes in the intraocular environment, thus reducing the magnitude and duration of surge events at decreasing intraocular pressures. Our data showed that this is true to a limited extent. There was no significant difference between the magnitude or duration of surge at an IOP of 50 mmHg vs. an IOP of 70 mmHg, suggesting that using the Active Sentry handpiece at an IOP of 50 mmHg would not introduce a greater risk of post-occlusion surge than operating at an IOP of 70 mmHg. However, there was a significant difference between the magnitude and duration of surge at an IOP of 30 mmHg vs. an IOP of 50 mmHg (P < 0.05), with the surge magnitude increasing by a factor of 1.8 and the surge duration increasing by 2.4 when decreasing the IOP from 50 mmHg to 30 mmHg. There was also a significant difference between the magnitude and duration of surge at an IOP of 30 mmHg vs an IOP of 70 mmHg (P < 0.05), with the magnitude of surge increasing by a factor of 1.8 and the duration of surge increasing by a factor of 2.8. This suggests that operating at an IOP of 30 mmHg could introduce a greater risk of post-occlusion surge than operating at an IOP above 50 mmHg. These results show that the Active Sentry handpiece with built-in pressure sensor may minimize both the magnitude and duration of post-occlusion surge when IOP is decreased from 70 mmHg to 50 mmHg; however, the handpiece loses this ability at some value between an IOP of 50 mmHg and 30 mmHg.
Generally, surgeons are taught to adjust flow and vacuum with significant reductions in IOP. Our study design might be criticized for not taking this into account. Other limitations of this study include the small sample size. We chose to use the same sample size of 10 that we used for our previous study.8 An additional limitation was not performing a power calculation prior to performing the experiments described in this article. Differences between a laboratory model and clinical surgery, as well as our use of fixed machine settings, constitute additional limitations. In the future, we will endeavor to look at this subject in more detail to better understand the benefit limits to the handpiece technology utilized in this study.
Conclusion
This experiment sought to provide preliminary evidence as to whether the Active Sentry handpiece might possibly allow surgeons to safely operate at lower IOPs. We plan to determine the exact location within the 50-to-30 mmHg IOP range where this handpiece loses its ability to minimize surge magnitude and duration in the future.
Abbreviations
IOP, intraocular pressure; phaco, phacoemulsification.
Acknowledgment
Susan Schulman assisted with editing and manuscript preparation.
Funding
This study was supported in part by a grant from Research to Prevent Blindness, Inc., New York, New York, USA. The sponsor had no involvement in any of the stages from study design to submission of the paper for publication.
Disclosure
Mr. Sherbotie reports voluntary involvement with Merit Medical Systems, outside the submitted work. The other authors report no conflicts of interest in this work.
The abstract of this paper was presented at the American Society of Cataract and Refractive Surgery Annual Meeting, on April 7, 2024, Session SPS-206 – Cataract Surgery – Other II, as a conference talk with interim findings. The poster’s abstract may be accessed at https://ascrs.confex.com/ascrs/24am/meetingapp.cgi/Paper/100604.
References
1. Magyar M, Sándor GL, Ujváry L, Nagy ZZ, Tóth G. Intraoperative complication rates in cataract surgery performed by resident trainees and staff surgeons in a tertiary eyecare center in Hungary. Int J Ophthalmol. 2022;15(4):586–7. doi:10.18240/ijo.2022.04.10
2. Haripriya A, Chang DF, Reena M, Shekhar M. Complication rates of phacoemulsification and manual small-incision cataract surgery at Aravind Eye Hospital. J Cataract Refract Surg. 2012;38(8):1360–1369. doi:10.1016/j.jcrs.2012.04.025
3. Bhagat N, Nissirios N, Potdevin L, et al. Complications in resident-performed phacoemulsification cataract surgery at New Jersey Medical School. Br J Ophthalmol. 2007;91(10):1315–1317. doi:10.1136/bjo.2006.111971
4. Sharif-Kashani P, Fanney D, Injev V. Comparison of occlusion break responses and vacuum rise times of phacoemulsification systems. BMC Ophthalmol. 2014;14:96. doi:10.1186/1471-2415-14-96
5. Vasavada V, Raj SM, Praveen MR, Vasavada AR, Henderson BA, Asnani PK. Real-time dynamic intraocular pressure fluctuations during microcoaxial phacoemulsification using different aspiration flow rates and their impact on early postoperative outcomes: a randomized clinical trial. J Refract Surg. 2014;30(8):534–540. doi:10.3928/1081597X-20140711-06
6. Vasavada AR, Praveen MR, Vasavada VA, et al. Impact of high and low aspiration parameters on postoperative outcomes of phacoemulsification: randomized clinical trial. J Cataract Refract Surg. 2010;36:588–593. doi:10.1016/j.jcrs.2009.11.009
7. Takhtaev YV, Kiseleva TN, Shliakman RB. The effect of preset intraoperative intraocular pressure during phacoemulsification on the blood flow velocity in the central retinal artery. Ophthalmol J. 2019;12(4):5–12.
8. Yalamanchili S, Aboughaida A, Rohani OS, Dyk DW. Evaluation of the occlusion break surge volume in five different phacoemulsification systems. Clin Ophthalmol. 2025;19:1357–1364. doi:10.2147/OPTH.S516801
9. Boulter T, Bernhisel A, Mamalis C, et al. Phacoemulsification in review: optimization of cataract removal in an in vitro setting. Surv Ophthalmol. 2019;64(6):868–875. doi:10.1016/j.survophthal.2019.06.007
10. Whitaker T, Nelson TK, Ricks RG, et al. Comparison of post-occlusion pressure surge between pressure sensing and traditional phacoemulsification handpieces. J Ophthalmol. 2025;2025(3264880):1–5.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Multicenter Effectiveness and Disease Stability Through 3 Years After iStentTrabecular Micro-Bypass with Phacoemulsification in Glaucoma and Ocular Hypertension
Clement C, Howes F, Ioannidis A, Shiu M, Manning D, Lusthaus JA, Skalicky SE, Goodwin TW
Clinical Ophthalmology 2022, 16:2955-2968
Published Date: 1 September 2022
Bio-Interventional Cyclodialysis and Allograft Scleral Reinforcement for Uveoscleral Outflow Enhancement in Open-Angle Glaucoma Patients: One-Year Clinical Outcomes
Ianchulev T, Weinreb RN, Calvo EA, Lewis J, Kamthan G, Sheybani A, Rhee DJ, Ahmed IK
Clinical Ophthalmology 2024, 18:3605-3614
Published Date: 6 December 2024
Comparison of Ultrasound Energy Delivered to the Anterior Segment Across Different Phacoemulsification Surgical Platforms
Nelson TK, Ricks RG, Cardenas IA, Whitaker T, Jensen JL, Olson RJ, Pettey JH
Medical Devices: Evidence and Research 2025, 18:29-35
Published Date: 14 January 2025