")
Back to Journals » International Journal of General Medicine » Volume 16
Comparing Outcomes of Critically Ill Patients in Intensive Care Units and General Wards: A Comprehensive Analysis
Authors Maluangnon C, Kanogpotjananont P, Tongyoo S
Received 24 May 2023
Accepted for publication 19 August 2023
Published 25 August 2023 Volume 2023:16 Pages 3779—3787
DOI https://doi.org/10.2147/IJGM.S422791
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Satish Chandrasekhar Nair
Chailat Maluangnon,1 Paweena Kanogpotjananont,1,2 Surat Tongyoo1
1Department of Medicine, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand; 2Department of Medicine, Chaopraya Abhaiphubejhr Hospital, Prachinburi, Thailand
Correspondence: Surat Tongyoo, Department of Medicine, Faculty of Medicine Siriraj Hospital, Mahidol University, 2, Wanglang Road, Siriraj, Bangkok Noi, Bangkok, 10700, Thailand, Tel +66 2 419 8534, Fax +66 2 419 8597, Email [email protected]
Background: The admission of critically ill patients to intensive care unit (ICU) plays a crucial role in reducing mortality. However, the scarcity of available ICU beds presents a significant challenge. In resource-limited settings, the outcomes of critically ill patients, particularly those who are not accepted for ICU admission, have been a topic of ongoing debate and contention.
Objective: This study aimed to explore the outcomes and factors associated with ICU admission and mortality among critically ill patients in Thailand.
Methods: This prospective cohort study enrolled critically ill adults indicated for medical ICU admission. Patients were followed for 28 days regardless of whether they were admitted to an ICU. Data on mortality, hospital length of stay, duration of organ support, and factors associated with mortality and ICU admission were collected.
Results: Of the 180 patients enrolled, 72 were admitted to ICUs, and 108 were cared for in general wards. The ICU group had a higher 28-day mortality rate (44.4% vs 20.4%; P=0.001), but other outcomes of interest were comparable. Multivariate analysis identified alteration of consciousness, norepinephrine use, and epinephrine use as independent predictors of 28-day mortality. Higher body mass index (BMI), higher APACHE II score, and acute kidney injury were predictive factors associated with ICU acceptance.
Conclusion: Among patients indicated for ICU admission, those who were admitted had a higher 28-day mortality rate. Higher mortality was associated with alteration of consciousness and vasopressor use. Patients who were sicker and had higher BMI were more likely to be admitted to an ICU.
Keywords: acceptance, general ward, intensive care units, mortality, outcomes
Introduction
Various factors influence hospital mortality in critically ill patients. While admitting diagnosis, age, sex, and underlying conditions exhibit a strong association with mortality, they are unmodifiable.1,2 Conversely, a few factors, such as admission to intensive care units (ICUs), can be modified.3–5 ICUs offer continuous monitoring of physiologic parameters, advanced organ support, and a higher nurse-to-patient ratio. These advantages contribute to a reduction in mortality rates compared to general wards, despite the provision of exceptional care in that setting.
The scarcity of available ICU beds presents a global challenge that affects both developing nations and industrialized countries.6 Determining whether a patient should be admitted to an ICU involves a complex decision-making process influenced by factors such as the severity of the illness, staffing availability, facility utilization, and predicted outcomes.6–8 Various strategies have been developed to address this issue, with scoring systems being the most prominent. One noteworthy example is the Acute Physiology and Chronic Health Evaluation (APACHE II), implemented in 1985. This system combines baseline health status and physiological parameters to stratify patients across acute illnesses, providing valuable insights for clinical decision-making and ICU admission criteria.9 Another widely recognized scoring system is the Sequential Organ Failure Assessment (SOFA) scoring system, introduced in 1996, which focuses on the quantitative assessment of multiorgan dysfunction over time.10 While serial evaluations using SOFA have shown promise as prognostic indicators, the performance of a single time-point evaluation is limited in this regard.11
However, it is essential to acknowledge that no single scoring system or parameter can perfectly determine ideal candidates for ICU admission. Thus, the final decision lies with the healthcare authority, who must assess individual patient information during the assessment process.8 Furthermore, while extensive research has been conducted on the outcomes of critically ill patients admitted to ICUs, limited information exists regarding the outcomes of patients not admitted to these specialized units.
This study aimed to investigate the outcomes of critically ill patients who received optimal treatment, regardless of whether they were admitted to an ICU or treated in a general ward. Additionally, we aimed to identify the factors associated with ICU acceptance and mortality among critically ill patients.
Materials and Methods
Study Setting and Population
This prospective cohort study enrolled adult patients admitted to Siriraj Hospital in Bangkok, Thailand, between July 4, 2018, and July 3, 2019. The study population comprised patients who met the criteria for medical ICU admission, which included the following conditions:
- Acute respiratory failure requiring either invasive or noninvasive respiratory support.
- Hypotension necessitating the administration of vasopressors or inotropes for at least 24 hours.
- Acute kidney injury (AKI) necessitating renal replacement therapy (RRT).
- Critically ill patients for whom the attending physician deemed ICU admission necessary.
Patients with long-term ventilator or noninvasive respiratory support dependency, terminal illness, or do-not-resuscitate orders were excluded from the study.
Ethics Approval and Informed Consent
Before inclusion in the study, written informed consent was obtained from each patient or their legal representatives, as applicable, per the Code of Ethics outlined by the World Medical Association (Declaration of Helsinki). The Institutional Review Board of the Faculty of Medicine Siriraj Hospital, Mahidol University, approved the research protocol before commencement (Si400/2018).
Study Design
Following enrollment, comprehensive data were collected on baseline characteristics, the diagnosis indicated for ICU admission, pertinent laboratory tests, physiological parameters, and crucial organ support interventions. Regardless of ICU acceptance, the investigators diligently tracked each patient’s progress until day 28 postenrollment without influencing the attending physician’s management decisions, diagnostic procedures, or treatment protocols.
Outcome Measurement
The primary outcome of this study was the assessment of 28-day mortality rates in patients admitted to ICUs compared to those who were not admitted. The secondary endpoints analyzed were hospital length of stay, duration of mechanical ventilator support, duration of vasoactive/inotropic agent administration, and duration of RRT. Additionally, we identified factors associated with both 28-day mortality and ICU acceptance.
Statistical Analysis
The sample size calculation was based on institutional data. At our institute, patients meeting the inclusion criteria had a 20% mortality rate in ICUs, whereas those treated in general wards had a mortality rate of 40%. Using a 95% confidence interval (Z=1.96), a power of 80% (β=0.2), and an enrollment ratio of 2 (ratio of general ward mortality to ICU mortality of 2), we performed a sample size calculation using independent sample proportions. At least 60 subjects needed to be prospectively enrolled in the ICU group, while at least 120 subjects were required for the general ward group.
For continuous variables with a normal distribution, independent samples t-tests were used for comparison, while nonnormally distributed data were assessed using the Mann–Whitney U-test. Categorical variables were compared using Pearson’s χ2 test or Fisher’s exact test, as appropriate. A P value of less than 0.05 was considered statistically significant in all analyses.
We conducted receiver operating characteristic (ROC) curve analysis on continuous variables and identified the optimal cut-point using the Youden index to transform them into categorical data. Subsequently, univariate analysis was performed on all potential clinical parameters to identify predictive factors for the primary outcome. Clinical parameters exhibiting an association with the primary outcome, indicated by a P value of <0.1 in the univariate analysis, were included in a multivariable binary logistic regression model.
All statistical analyses were conducted using PASW Statistics, version 18.0 (SPSS Inc, Chicago, IL, USA).
Results
A total of 180 patients were enrolled in the study, with 72 patients in the ICU group and 108 in the general ward group. The ICU group exhibited significant differences in age (58.3±18.7 vs 68.7±15.8 years; P<0.001), body mass index (BMI; 24.2±6.1 vs 22.3±5.1; P=0.03), and disease severity (APACHE II score: 17.9±7.7 vs 13.3±5.6 with P<0.001; Sequential Organ Failure Assessment score: 5.8±3.2 vs 4.4±3.0, with P=0.003) compared to the general ward group. The proportion of female patients in the ICU group was nonsignificantly lower (40.3% vs 50.9%; P=0.16), with no significant differences observed in underlying diseases. The most common diagnosis at the time of ICU request was sepsis, with no significant difference in the prevalence of the condition in the 2 groups (ICU group: 81.9%; general ward group: 76.9%; P=0.41).
The ICU group presented with a higher incidence of hypotension (65.3% vs 39.8%; P=0.01), AKI (63.9% vs 29.6%; P<0.001), and alteration of consciousness (23.6% vs 6.5%; P<0.01). Laboratory parameters of the ICU group indicated more severe conditions, with significantly higher serum creatinine levels (2.98±2.81 vs 1.96±1.90 mg/dL; P=0.005), lower pH values (7.32±0.14 vs 7.39±0.10; P=0.004), and elevated lactate levels (6.4±6.3 vs 4.0±3.6 mmol/L; P=0.03; Table 1).
 |
Table 1 Baseline Characteristic |
There were no significant differences in the proportions of patients in each group who required mechanical ventilation (75.0% vs 68.5%; P=0.35) or other forms of respiratory support. However, the ICU group underwent more intensive monitoring and organ support interventions. These included a significantly higher utilization of inferior vena cava ultrasound (66.7% vs 6.5%; P<0.001), central venous catheterization (86.1% vs 10.2%; P<0.001), arterial line placement (88.9% vs 3.7%; P<0.001), and RRT (40.3% vs 7.4%; P<0.001).
Norepinephrine administration was more frequently prescribed for patients admitted to an ICU than for those admitted to a general ward (65.3% vs 39.8%; P=0.001). Nevertheless, the mean doses of the groups did not differ significantly (0.19±0.21 vs 0.12±0.14 mcg/kg/min, respectively; P=0.07; Table 2).
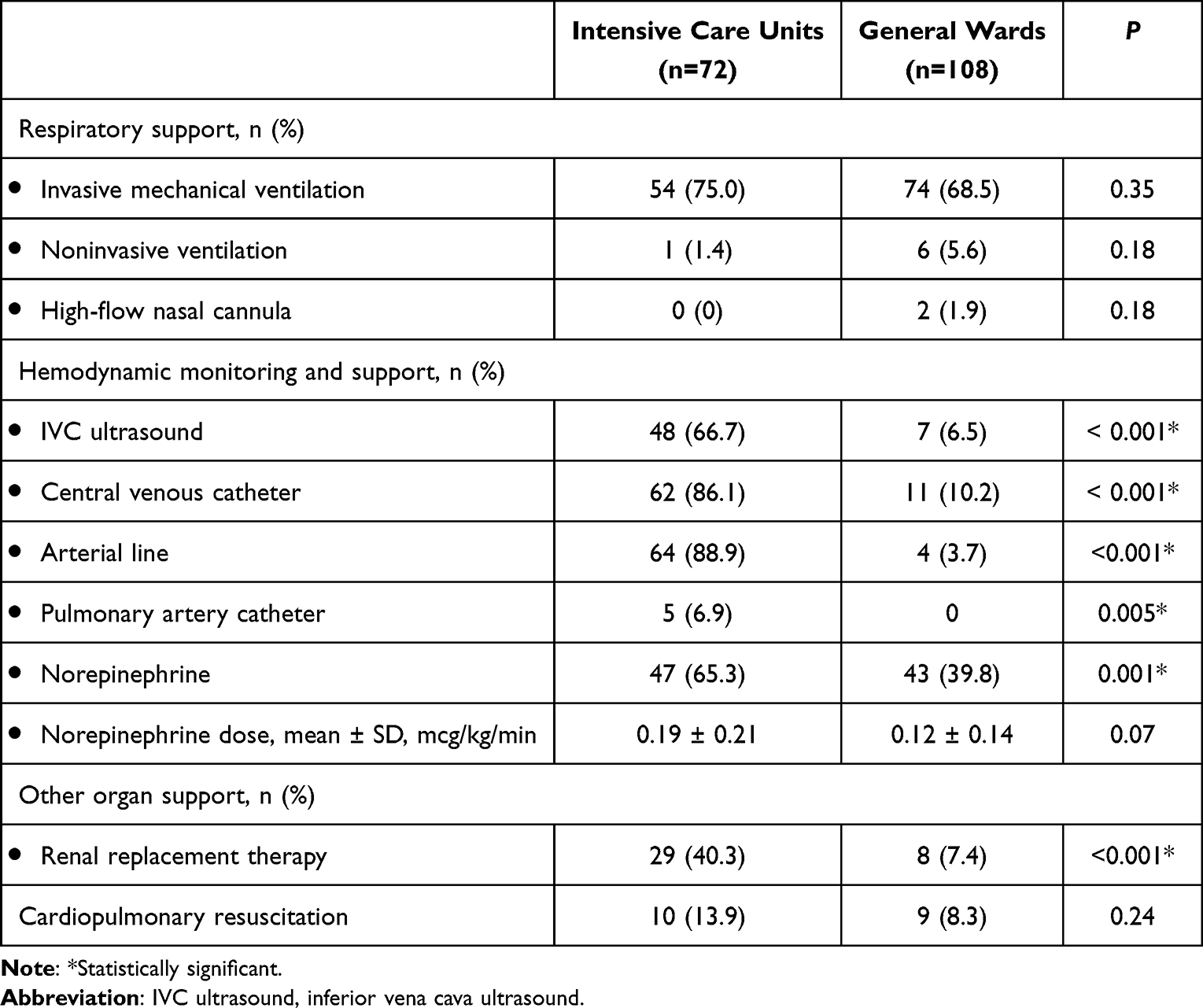 |
Table 2 Procedure and Organ Support During Admission |
The overall 28-day mortality rate in the study population was 30% (54/180). Among the patients in the ICU group, the 28-day mortality rate was 44.4% (32/72), whereas in the general ward group, it was 20.4% (22/108). In the unadjusted model, patients admitted to an ICU had a significantly higher risk of 28-day mortality than those treated in a general ward (odds ratio [OR]: 3.17; 95% CI: 1.64–6.15; P<0.001). However, no significant differences were observed in other outcomes of interest (Table 3).
 |
Table 3 Outcomes |
A multivariate analysis model was conducted to determine the factors significantly associated with 28-day mortality. The factors identified were alteration of consciousness (adjusted odds ratio [aOR]: 9.15; 95% CI: 1.11–75.16; P=0.04), norepinephrine use (aOR: 57.81; 95% CI: 1.29–581.4; P=0.04), and epinephrine use (aOR: 15.78; 95% CI: 1.86–133.65; P=0.01). However, ICU admission did not significantly correlate with 28-day mortality (aOR: 3.24; 95% CI: 0.41–25.76; P=0.27; Table 4).
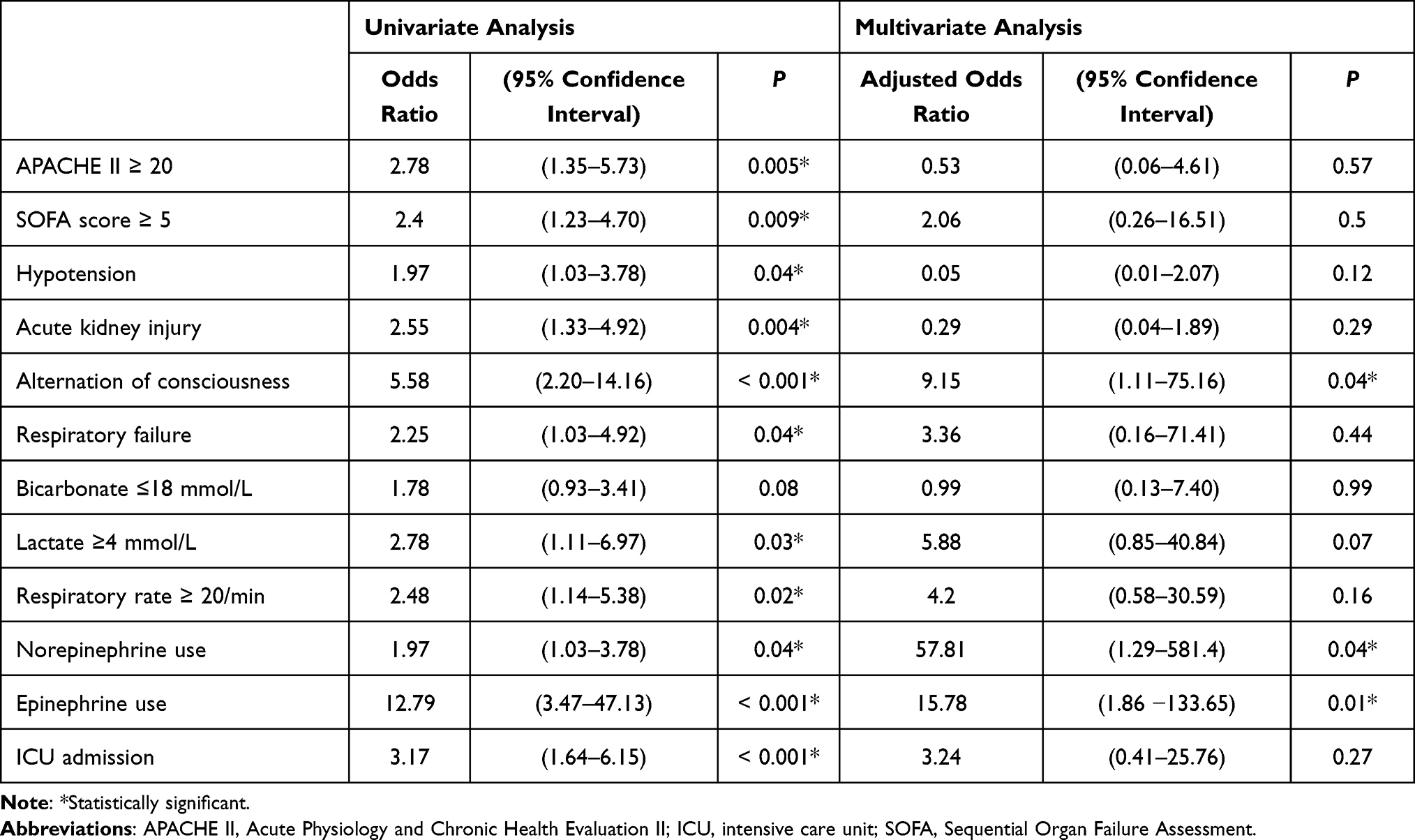 |
Table 4 Factors Associated with 28-Day Mortality |
Another multivariate analysis model was employed to identify factors associated with ICU acceptance. The 3 significantly associated factors revealed were higher BMI (≥23; aOR: 10.63; 95% CI: 1.32–85.86; P=0.03), greater disease severity (APACHE II score ≥20; aOR: 10.87; 95% CI: 1.24–95.10; P=0.03), and AKI (aOR: 10.39; 95% CI: 1.30–82.88; P=0.03; Table 5).
 |
Table 5 Factors Associated with Intensive Care Unit Acceptance (n=72) |
Discussion
Our institute, a tertiary referral university hospital, has an ICU-to-general bed ratio of approximately 5%. The ratio at our institute is similar to that of many Western European countries (2–5%) but half that of the United States (9–10%).12 All requests for ICU admission at our hospital are evaluated by an attending intensivist and other members of an ICU team to determine whether the patients will be accepted. Less than half of the requests in our study were approved, a rate similar to those reported in other studies.3,6,13 This low acceptance rate is likely due to the persisting issue of ICU bed shortages worldwide, even though the number of ICU beds has increased over the years.6,14
In this study, an unexpected finding emerged, as critically ill patients who were indicated for ICU admission and subsequently accepted had double the 28-day mortality compared to those treated in the general medical wards. This finding stands in contrast to previous studies that demonstrated a reduction in mortality associated with ICU admission.3–5,15,16
A plausible explanation for this finding lies in the more severe condition of the patients in the ICU group. The ICU group exhibited significantly worse disease severity than the general ward group, with a mean APACHE II score of 17.9 vs 13.3.
Furthermore, a substantial proportion of patients in the ICU group (63.9%) presented with AKI at the time of their ICU request, with 40% requiring RRT. In contrast, among patients treated in the general ward, only 29.6% had AKI, and 7.4% needed RRT. It is noteworthy that previous research has consistently associated the presence and severity of AKI, as well as the need for RRT, with3,15 increased mortality in critically ill patients.17–19
Additionally, the ICU group exhibited a higher incidence of hypotension, greater utilization of norepinephrine, and elevated serum lactate levels than the general ward group. Each of these parameters has been consistently linked to higher mortality in numerous studies.20–22
Upon admission to ICUs, patients commonly undergo more invasive monitoring and procedures, including central venous catheter insertion, arterial line insertion, and, occasionally, pulmonary artery catheter placement, than patients in general wards.15 In our study, nearly 90% of ICU patients had a central line in place, while a similar proportion also had an arterial line inserted. Conversely, these procedures were performed in only 10% and 4% of general ward patients, respectively. However, there is limited substantial evidence demonstrating the efficacy of these interventions in improving patient outcomes.23,24 Previous research has highlighted the safe administration of vasopressors via peripheral veins, minimizing the risk of local complications.25 Additionally, noninvasive blood pressure measurements have shown a reliable correlation with arterial blood pressure, even during vasopressor administration.26 These findings suggest a potential tendency toward overutilization of central venous catheters and arterial line insertion in our ICU setting. Consequently, it is advisable to re-evaluate the benefits these routine procedures offer patients.
The factors associated with ICU acceptance in our study were higher BMI, higher APACHE II score, and AKI. Notably, a study in Greece identified different ICU acceptance factors: a higher Glasgow Coma Scale, absence of cardiac arrest, and lower Charlson comorbidity score.13 Furthermore, a systematic review indicated that refusal of ICU admission was linked to factors such as age over 65, poor performance status, underlying malignancy, and chronic respiratory or cardiac failure.6 These findings shed light on global selection biases in ICU acceptance. Decisions regarding ICU admission are influenced not only by the severity of illness and the necessity for hemodynamic and organ support but also by a preference for younger patients with better baseline health statuses.3,27
In the context of the limited availability of ICU beds, selecting the most appropriate patients for admission lacks universally applicable guidelines. However, an expert panel has emphasized the importance of prioritizing the comprehensive optimization of resources to enhance patient outcomes.8 This underscores the critical role of experienced intensivists who can allocate ICU resources based on their clinical judgment and ethical considerations. They aim to admit the most critically ill patients to the ICU while striving to achieve satisfactory outcomes by providing less invasive measures for patients who are declined admission to the ICUs.6,7
A major strength of this study is its prospective cohort design. This allowed for a clear identification of the actual practices involved in ICU bed allocation within a resource-limited developing country. The study highlights that ICU acceptance alone is not the sole determinant for reducing 28-day mortality. Nevertheless, disease severity plays a primary role in patient outcomes.
There are several notable limitations to our study. First, being a single-center study without predefined criteria for ICU admission limits the generalizability and reproducibility of our results. However, the situations described in our study are likely comparable to those in most ICUs, where ICU acceptance primarily depends on the attending intensivist’s judgment. Second, we did not account for the participants’ baseline health status, which could have influenced the decision-making process of the attending intensivist as well as the mortality outcomes. Last, the baseline characteristics between the groups were not matched, resulting in a selection bias that may confound the association with mortality. However, it is essential to note that such selection bias is common in most ICUs, and attempting to correct it may yield limited benefits. Future large-scale prospective cohorts or registry-based studies with baseline matching are warranted to address these limitations.
Conclusions
In our study, patients admitted to an ICU had higher 28-day mortality rates than those assigned to a general ward. Notably, patients with a more severe condition and higher BMI were more likely to be accepted into an ICU. The mortality of critically ill patients was strongly associated with disease severity, and ICU admission did not confer additional mortality benefits.
Data Sharing Statement
The dataset supporting this study’s findings will be available from the corresponding author 1 year after publication for a period of 1 year upon reasonable request.
Acknowledgments
The authors are indebted to Mr David Park for the English-language editing of this paper.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors have no conflicts of interest to disclose.
References
1. Schwartz N, Sakhnini A, Bisharat N. Predictive modeling of inpatient mortality in departments of internal medicine. Intern Emerg Med. 2018;13(2):205–211. doi:10.1007/s11739-017-1784-8
2. Glick N, Vaisman A, Negru L, Segal G, Itelman E. Mortality prediction upon hospital admission - the value of clinical assessment: a retrospective, matched cohort study. Medicine. 2022;101(39):E30917. doi:10.1097/MD.0000000000030917
3. Hersch M, Sonnenblick M, Karlic A, Einav S, Sprung CL, Izbicki G. Mechanical ventilation of patients hospitalized in medical wards vs the intensive care unit-an observational, comparative study. J Crit Care. 2007;22(1):13–17. doi:10.1016/j.jcrc.2006.06.004
4. Valley TS, Sjoding MW, Ryan AM, Iwashyna TJ, Cooke CR. Association of intensive care unit admission with mortality among older patients with pneumonia. J Am Med Assoc. 2015;314(12):1272–1279. doi:10.1001/jama.2015.11068
5. Iwashita Y, Yamashita K, Ikai H, Sanui M, Imai H, Imanaka Y. Epidemiology of mechanically ventilated patients treated in ICU and non-ICU settings in Japan: a retrospective database study. Crit Care. 2018;22(1):329. doi:10.1186/s13054-018-2250-3
6. Sinuff T, Kahnamoui K, Cook DJ, Luce JM, Levy MM. Rationing critical care beds: a systematic review. Crit Care Med. 2004;32(7):1588–1597. doi:10.1097/01.CCM.0000130175.38521.9F
7. Scheunemann LP, White DB. The ethics and reality of rationing in medicine. Chest. 2011;140(6):1625–1632. doi:10.1378/chest.11-0622
8. Nates JL, Nunnally M, Kleinpell R, et al. ICU admission, discharge, and triage guidelines: a framework to enhance clinical operations, development of institutional policies, and further research. Crit Care Med. 2016;44(8):1553–1602. doi:10.1097/CCM.0000000000001856
9. Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med. 1985;13(10):818–829.
10. Vincent JL, Moreno R, Takala J, et al. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the working group on sepsis-related problems of the European Society of intensive care medicine. Inten Care Med. 1996;22(7):707–710. doi:10.1007/BF01709751
11. Ferreira FL, Bota DP, Bross A, Mélot C, Vincent JL. Serial evaluation of the SOFA score to predict outcome in critically ill patients. JAMA. 2001;286(14):1754–1758. doi:10.1001/jama.286.14.1754
12. Wunsch H, Angus DC, Harrison DA, et al. Variation in critical care services across North America and Western Europe. Crit Care Med. 2008;36(10):2787–2793. doi:10.1097/CCM.0b013e318186aec8
13. Basoulis D, Liatis S, Skouloudi M, Makrilakis K, Daikos GL, Sfikakis PP. Survival predictors after intubation in medical wards: a prospective study in 151 patients. PLoS One. 2020;15(6). doi:10.1371/journal.pone.0234181
14. Wallace DJ, Seymour CW, Kahn JM. Hospital-level changes in adult ICU bed supply in the United States. Crit Care Med. 2017;45(1):e67–e76. doi:10.1097/CCM.0000000000002051
15. Surat T, Viarasilpa T, Permpikul C. The impact of intensive care unit admissions following early resuscitation on the outcome of patients with severe sepsis and septic shock. J Med Assoc Thai. 2014;97(Suppl 1):S69–76.
16. Naorungroj T, Viarasilpa T, Tongyoo S, et al. Characteristics, outcomes, and risk factors for in-hospital mortality of COVID-19 patients: a retrospective study in Thailand. Front Med. 2023:9. doi:10.3389/fmed.2022.1061955
17. Nisula S, Kaukonen KM, Vaara ST, et al. Incidence, risk factors and 90-day mortality of patients with acute kidney injury in Finnish intensive care units: the FINNAKI study. Intensive Care Med. 2013;39(3):420–428. doi:10.1007/s00134-012-2796-5
18. Hoste EAJ, Bagshaw SM, Bellomo R, et al. Epidemiology of acute kidney injury in critically ill patients: the multinational AKI-EPI study. Intensive Care Med. 2015;41(8):1411–1423. doi:10.1007/s00134-015-3934-7
19. Hoste EAJ, Kellum JA, Selby NM, et al. Global epidemiology and outcomes of acute kidney injury. Nat Rev Nephrol. 2018;14(10):607–625. doi:10.1038/s41581-018-0052-0
20. Casserly B, Phillips GS, Schorr C, et al. Lactate measurements in sepsis-induced tissue hypoperfusion: results from the surviving sepsis campaign database. Crit Care Med. 2015;43(3):567–573. doi:10.1097/CCM.0000000000000742
21. Juneja D, Singh O, Dang R. Admission hyperlactatemia: causes, incidence, and impact on outcome of patients admitted in a general medical intensive care unit. J Crit Care. 2011;26(3):316–320. doi:10.1016/j.jcrc.2010.11.009
22. Tongyoo S, Tanyalakmara T, Naorungroj T, Promsin P, Permpikul C. The association of high dose vasopressor and delayed vasopressor titration with 28-day mortality in adult patients with septic shock. J Health Sci Med Res. 2022;41(1). doi:10.31584/jhsmr.2022886
23. Gershengorn HB, Wunsch H, Scales DC, Zarychanski R, Rubenfeld G, Garland A. Association between arterial catheter use and hospital mortality in intensive care units. JAMA Intern Med. 2014;174(11):1746–1754. doi:10.1001/jamainternmed.2014.3297
24. Evans L, Rhodes A, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Crit Care Med. 2021;49(11):e1063–e1143. doi:10.1097/CCM.0000000000005337
25. Permpikul C, Tongyoo S, Viarasilpa T, Trainarongsakul T, Chakorn T, Udompanturak S. Early use of norepinephrine in septic shock resuscitation (CENSER) a randomized trial. Am J Respir Crit Care Med. 2019;199(9):1097–1105. doi:10.1164/rccm.201806-1034OC
26. Tongyoo S, Visuthisakchai S, Permpikul C. Blood pressure measurement compared between oscillometric blood pressure monitoring and gold standard intra-arterial blood pressure monitoring in adult shock resuscitation patients. J Crit Intensive Care. 2022;13(3):102–109. doi:10.37678/dcybd.2022.3230
27. Lieberman D, Nachshon L, Miloslavsky O, et al. Elderly patients undergoing mechanical ventilation in and out of intensive care units: a comparative, prospective study of 579 ventilations. Crit Care. 2010;14(2):R48. doi:10.1186/cc8935
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.