Back to Journals » Journal of Pain Research » Volume 19
Comparing Medicare Claims in Patients with Lumbar Discogenic Pain Managed Conservatively or with Intradiscal Nucleus Pulposus Allograft
Authors Girardi GE, Wilson DK, Patel RG ![]() , Yazdani S
, Yazdani S
Received 11 March 2026
Accepted for publication 19 May 2026
Published 6 June 2026 Volume 2026:19 596149
DOI https://doi.org/10.2147/JPR.S596149
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Andrea Tinnirello
George E Girardi,1 Derron K Wilson,2 Raj G Patel,3 Shiraz Yazdani4
1UCHealth Pain Management Clinic, Fort Collins, CO, USA; 2Goodman Campbell Brain and Spine, Carmel, IN, USA; 3Capital Pain Institute, Austin, TX, USA; 4Lubbock Spine Institute, Lubbock, TX, USA
Correspondence: George E Girardi, UCHealth Pain Management Clinic, Fort Collins, CO, USA, Email [email protected]
Background: Minimally invasive intradiscal procedures such as nucleus pulposus (NP) allograft have been advocated as first-line interventions in patients with lumbar discogenic pain that fail to respond to conservative care.
Methods: The objective of this retrospective study was to assess the impact of a commercially available NP allograft (VIA Disc NP) on claims-based outcomes among Medicare beneficiaries with symptomatic degenerative disc disease (DDD). NP allograft patients were compared with a matched group of DDD patients managed conservatively. Use of the 100% Medicare database identified a sample size of 1804 cases per group matched on a one-to-one basis on age, sex, baseline Charlson-Comorbidity Index, disc degeneration, radiculopathy, disc displacement (herniation), spondylosis/facet arthropathy, and baseline chronic opioid therapy. Data extraction was restricted to the period, August 2021 to December 31, 2024. All patients had ≥ 12 months of continuous enrollment with medical benefits preceding and following the index date. Outcomes included opioid usage, imaging utilization, physical therapy, epidural steroid injections, spinal fusion procedures, and physician preference.
Results: There was a significant reduction in the mean total number of opioid prescriptions (3.3 ± 4.9 vs. 2.6 ± 3.9, P=0.001), the mean total days’ supply of opioids (129.3 ± 165.1 vs. 89.8 ± 133.2 days, P=0.001), and imaging utilization frequency (81% vs. 46%, P=0.0001) between the 12-month baseline period and the 12-month follow-up period after the index NP allograft procedure. There were statistically significant differences in utilization rates between study groups for physical therapy (76% vs. 40%, P=0.0001) and epidural steroid injections (55% vs. 31%, P=0.0001), equating to reductions in resource utilization of 47% and 44%, respectively, following intradiscal treatment. Fusion rates were low in both study groups (6% vs. 6%, P=0.53).
Conclusion: This analysis showed that the commercial introduction of a clinically effective first-line intervention in the continuum of care of patients with lumbar discogenic pain is associated with a reduction in the number and type of medical claims for this condition in the Medicare population.
Keywords: discogenic, low back pain, opioid, nucleus pulposus, allograft, Medicare
Introduction
Lumbar discogenic pain associated with degenerative disc disease (DDD) has recently been distinguished from other sources of chronic low back pain with a specific International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) diagnostic code.1 This designation recognized the intensive research and development effort that has identified the anterior column of the spine as a unique and highly prevalent pain generator.2 A diagnostic and treatment algorithm has been proposed to serve as a clinical practice guideline for managing patients with lumbar discogenic pain as they experience disease progression and advance through the continuum of care.3
Conservative care consisting of physical therapy, anti-inflammatory medications and epidural steroid injections, remains the preferred first step in managing discogenic pain in the absence of deteriorating neurological symptoms.4 However, for many patients, conservative care is only moderately efficacious in terms of the magnitude and duration of effectiveness, with symptoms often becoming refractory to these interventions.5
Because they do not disrupt normal spinal anatomy, minimally invasive intradiscal procedures have been advocated as first-line interventions in patients with persistent discogenic pain that fail to experience adequate symptom relief from conservative care measures.3,6 Aside from autologous products such as platelet-rich plasma and bone marrow aspirate concentrate, the only commercially available intradiscal product is nucleus pulposus (NP) allograft tissue.7 This product is a minimally manipulated, micronized NP allograft processed from allogeneic disc tissue and reconstituted in sterile saline at the time of the procedure. Delivered intradiscally under fluoroscopic guidance, it is intended to supplement the degenerated native nucleus with allogeneic matrix material while preserving spinal anatomy. Accumulating clinical evidence shows that this product has an excellent safety profile that provides clinically meaningful improvements in pain, function and quality of life through two years of follow-up after a single treatment.8–12
Since its introduction into the US medical marketplace in 2021, intradiscal NP allograft has enjoyed high clinical adoption with over 25,000 discs treated, to date.12 This study was undertaken to examine the impact of the commercial introduction of this product on the continuum of care of patients with lumbar discogenic pain. The Medicare claims database was utilized to provide large, representative cohorts clinically managed under real-world practice conditions that allowed an evaluation of changes in procedures, healthcare utilization, and outcomes over time.
Methods
The objective of this investigation was to assess the impact of the commercial introduction of a first-line intradiscal treatment, VIA Disc NP (Vivex Biologics, Inc. Miami, FL, USA), on claims-based outcomes among Medicare beneficiaries with chronic lumbar discogenic pain associated with DDD. Specifically, DDD patients treated with NP allograft were compared with a matched group of DDD patients managed conservatively with respect to opioid usage, imaging utilization, physical therapy, epidural steroid injections, spinal fusion procedures, and physician preference. Physician preference included pain management, chiropractor, orthopedic surgeon, interventional radiology, neurosurgeon, and physical medicine and rehabilitation specialists.
This study employed a retrospective, within-subjects design using the 100% Medicare Fee for Service (FFS) database. This method utilized de-identified administrative claims from the FFS Research Identifiable Files which resulted in complete capture of Parts A/B encounters and Part D Prescription Drug Event data for enrolled beneficiaries. Dissemination safeguards were applied, including the ≤20% cohort limit per year and suppression of any cell with n<11. Access, processing, and analysis of data were undertaken by an independent data management and health econometric firm (Inovalon, Bowie, MD, USA). The authors received access to use the data from the FFS database under a data use agreement that ensures compliance with the Privacy Act and restricts data usage to approved specific research or business purposes. Data extraction was restricted to the time period, August 2021 to December 31, 2024, which corresponds with the initial commercial introduction of VIA Disc NP through the most currently available date when the Centers for Medicare & Medicaid Services (CMS) release data on claims for medical benefits.
To identify patients treated with VIA Disc NP, the index event was set to the earliest claim with a procedure code for 0627T or 0629T and contained a National Provider Identifier (NPI) number of a provider known to administer the VIA Disc NP procedure (NPI list furnished by Vivex Biologics). Demographic measures were assessed on the index procedure date. A 12-month pre-index time window immediately preceding the index date served as the baseline period, in which patient characteristics and baseline levels of the primary endpoints were assessed. During the time immediately following the index date, post-procedure outcomes were assessed. This analysis included outcomes among patients with ≥12 months of continuous enrollment with medical benefits preceding and following the index date.
A comparison group of patients with a diagnosis of DDD without NP allograft treatment was also identified in the 100% Medicare FFS claims database. These patients were required to evidence a claim for a non-surgical intervention, including an epidural steroid injection, platelet-rich plasma injection, or physical therapy. The earliest date of treatment was set as the index date.
Conservatively managed control patients were directly matched to VIA Disc NP patients with the same 12-month period of enrollment in a many-to-one ratio on age, gender, baseline Charlson-Comorbidity Index, presence of a baseline disc degeneration diagnosis, radiculopathy diagnosis, disc displacement (herniation) diagnosis, spondylosis / facet arthropathy diagnosis, and baseline chronic opioid therapy. For patients with more than one successful match, a single control patient was selected at random for the final analyses to ensure a one-to-one final match. Comorbidities of interest relevant to back pain were captured using ICD-10-CM codes. These measures were drawn from the pre-index window and summarized at index.
Statistical analyses summarize continuous variables with means/medians/SDs and categorical variables with counts/proportions. Within group changes were assessed using the paired t-test, 2-tailed. Between group differences were assessed using the 2-sample t-test, 2-tailed and categorial outcomes were compared using the chi-square test. Two-sided α=0.05 defined statistical significance for all comparisons. All statistical analyses were conducted using SAS 9.4 (version M9).
Results
The presence of ≥1 medical claim for a specific percutaneous injection procedure (CPT code 0627T or 0629T) on or following August 1, 2021, resulted in 3,999 patients. Of these, 3,283 (82%) included an NPI known to administer VIA Disc NP in addition to the index percutaneous injection claim.
In identifying the conservative care control group, the presence of ≥1 medical claim with an ICD-10-CM code for DDD on or following August 1, 2021 (index diagnosis date) resulted in 3,334,858 patients. Among these patients, the absence of any medical claim under CPT code 0627T or 0629T reduced the eligible patient pool to 3,329,868 (99.9%). The additional presence of ≥1 medical claim for non-surgical treatment (epidural steroid injection, platelet-rich plasma injection, and/or physical therapy) following the index diagnosis date refined the eligible population to 2,135,611 (64%).
There were 1,877 patients and 1,439,116 patients treated with NP allograft and conservative care, respectively, with ≥12 months of continuous enrollment with medical benefits preceding and following the index date. Employing the prespecified matching criteria resulted in 1,804 patients matched one-to-one.
Table 1 provides the baseline demographic and clinical characteristics by study group. Exact comparability was achieved between groups on all matching variables without any standardized difference exceeding 0.1 for all other comparisons.
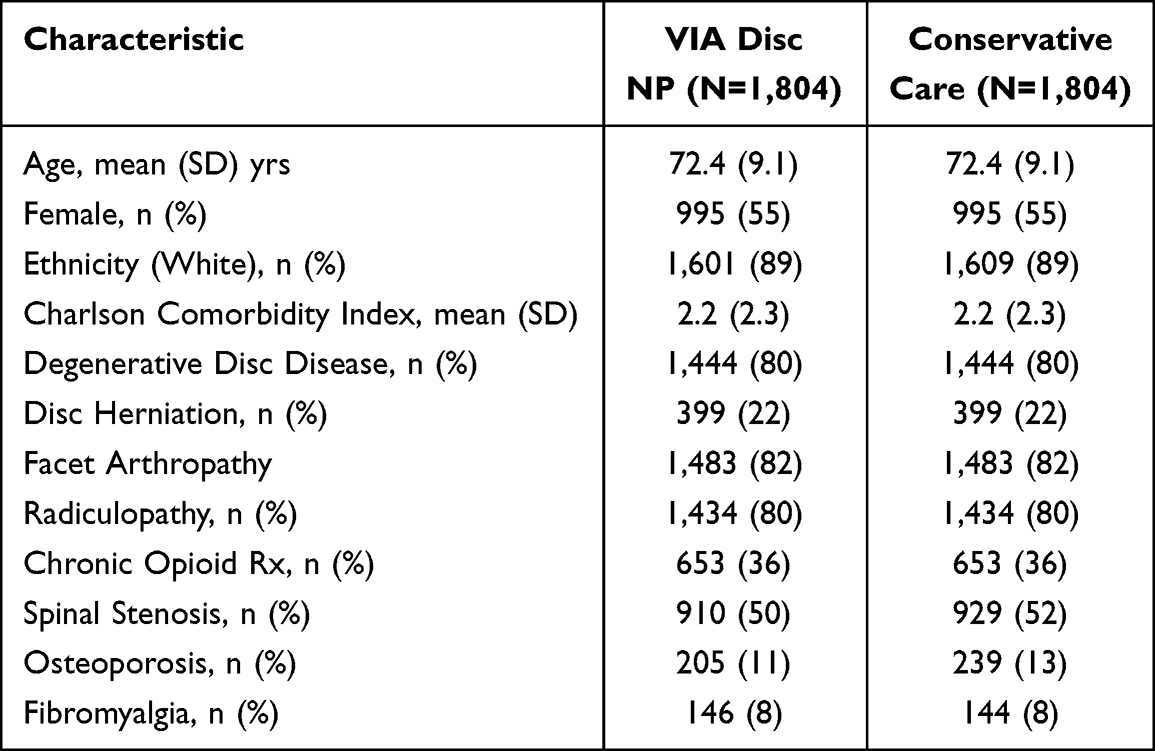 |
Table 1 Background Demographic and Clinical Comorbidities |
Among patients having an intradiscal NP allograft procedure, there was a significant reduction in the average total number of opioid prescriptions between the baseline and follow-up periods (3.3 ± 4.9 vs. 2.6 ± 3.9, P=0.001). A smaller reduction was found in the conservative care group (2.8 ± 5.0 vs. 2.2 ± 4.7, P=0.002). Following NP allograft treatment, there was a similar significant diminution in the average total days’ supply of opioids compared to baseline levels (129.3 ± 165.1 vs. 89.8 ± 133.2 days, P=0.001). Again, a smaller reduction was found in the conservative care group (113.9 ± 164.5 vs. 90.6 ± 139.8 days, P=0.001). This metric represents the number of days a prescription is intended to last based on the dosage and frequency prescribed. During the 12-month follow-up window, the average daily supply of opioids was similar between NP allograft patients and patients treated conservatively (89.8 ± 133.2 vs. 90.6 ± 139.8, P=0.86).
For NP allograft patients, lumbar imaging utilization which included plain and dynamic radiographs, MRI, CT, ultrasound and discography, dropped significantly from 81% (1,459 of 1,804) during the 12-month baseline period to 46% (828 of 1,804) during the follow-up period after the index NP allograft intradiscal procedure (P=0.0001). This reduction was particularly robust with respect to the utilization of MRI which decreased from 63% (1,132 of 1,804) during the baseline period to 25% (458 of 1,804) following NP allograft treatment (P=0.0001). Corresponding reductions in the conservative care group were 73% to 42% (P<0.01) and 55% to 24% (P<0.01) for overall imaging and MRI utilization, respectively. MRI utilization was similar during the 12-month follow-up period for NP allograft (25%, 458 of 1,804) and conservatively managed patients (24%, 426 of 1,804) (P=0.22).
All conservatively managed patients (100%) availed themselves to a minimally invasive procedure, including physical therapy and epidural steroid injection, during the follow-up period. In comparison, 66% (1,193 of 1,804) of NP allograft patients utilized some form of minimally invasive intervention during the same period (P=0.0001). Figure 1 illustrates the frequency of utilization of physical therapy and epidural steroid injection between study groups indicating reductions in resource utilization of 47% and 44%, respectively, following intradiscal treatment. This figure also shows a low (~ 6%) occurrence of spinal fusion procedures irrespective of study group.
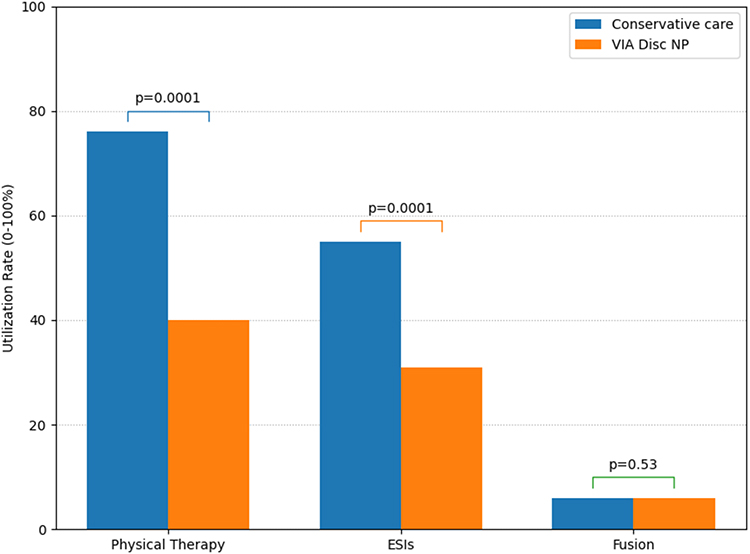 |
Figure 1 Bar graph illustrating the comparative utilization rates between study groups for physical therapy (76% vs. 40%), epidural steroid injections (ESIs, 55% vs. 31%), and fusion (6% vs. 6%). Total sample size, N=1,804 per group. |
There was a notable difference in physician preference between study groups. For example, most NP allograft patients were managed by a pain medicine specialist (72%) or by a physical medicine and rehabilitation physician (22%). Choice of physician was much more varied among conservatively managed patients with 25% and 13% treated by the same specialists, respectively.
Discussion
This study provides real-world evidence of the impact of the introduction of a new intervention into the continuum of care of patients experiencing chronic lumbar discogenic pain associated with DDD. There were statistically significant differences in the utilization of physical therapy and epidural steroid injections between DDD patients receiving conservative care and those having an intradiscal NP allograft procedure (Figure 1). This finding not only represents a logical progression in the care continuum but, more importantly, confirms the clinical efficacy of NP allograft in reducing the necessity for conservative measures that have become inadequate in ameliorating symptoms.
Patients treated with NP allograft experienced statistically significant reductions in opioid usage metrics and utilization of advanced imaging, particularly MRI, between the 12-month baseline period and the 12-month post-procedural follow-up period after the index intradiscal procedure. These findings mirror clinical trial evidence showing almost 60% of participants treated with NP allograft reporting a 12-month back pain severity score of ≤3.10 These patients have achieved an acceptable symptom state and feel well enough to function acceptably in daily life without the need for medications, injections, physical therapy or the need to seek imaging confirmation for recalcitrant symptomatology.13,14
We noted similar values for opioid usage and imaging utilization between study groups during the 12-month follow-up period. We highlighted the parity in these metrics as patients undergoing the NP allograft procedure tended to demonstrate greater levels of baseline disability with 18% greater total opioid prescriptions (3.3 versus 2.8) and 11% greater overall imaging utilization (81% versus 73%) compared to conservatively managed patients during the 12-month baseline period prior to the index date.
Examining physician preference, patients at the beginning of the continuum of care for lumbar discogenic pain tended to seek out a pain management specialist only 25% of the time whereas those with more advanced disease and further along in the continuum utilized a pain specialist over 70% of the time. This suggests a shift in point of care corresponding with disease progression, severity and chronicity.
One of the primary advantages of using the Medicare claims database is the robust sample sizes that can be yielded to substantially reduce the uncertainty and enhance the precision of comparative estimates of outcomes. This study employed comprehensive one-to-one matching to ensure study group comparability across a wide set of potential confounders and nevertheless maintained a sample size of 1,804 unique Medicare beneficiaries in each group. This large sample of patients provides confidence that the shifts noted in resource utilization between groups are tangible and represent a positive clinical impact of the NP allograft intervention. This was underscored by the maintenance of a low rate of fusion surgery (~6%) in both study groups despite DDD progression.
The primary limitation of utilizing the Medicare administrative database is the restriction to patients ≥65 years of age. Indeed, many patients present with specific discogenic pain symptoms and imaging evidence of DDD at an earlier time point in the lifespan.15 Medicare beneficiaries, in contrast, may present clinically with more advanced DDD coupled with posterior column involvement, confounding diagnosis and treatment efficacy. Most importantly, the Medicare claims data are primarily collected for billing and management, not for measuring clinical outcomes. Thus, these findings should be considered inferential with respect to the clinical effectiveness of NP allograft in this patient population.
Conclusion
This retrospective study presents a snapshot of aggregated claims-based clinical outcomes from the 100% Medicare database in symptomatic DDD patients, providing a large body of real-world evidence on resource utilization for patients managed conservatively as well as those receiving intradiscal NP allograft for lumbar discogenic pain. The robust data set provides a useful approach to compare the number and type of medical claims at contiguous points in the continuum of care. Commercial introduction of NP allograft in 2021 is associated with a reduction in the number and type of medical claims for this condition in the Medicare population. Further research is warranted as clinical adoption of this procedure expands.
Institutional Review Board Statement
The Centers for Medicare & Medicaid Services (CMS) administrative database used for this study adhered to HIPAA guidelines for de-identification. Ethics approval and informed consent were not required. All patient records were de-identified and complied fully with the confidentiality standards outlined in the Health Insurance Portability and Accountability Act of 1996 (HIPAA). According to Title 45 of CFR, Part 46, this analysis of administrative claims data was exempt from Institutional Review Board (IRB) oversight as it was based solely on existing data without patient intervention or direct interaction, and no identifiable patient information was included in the dataset.
Data Sharing Statement
Requests for data sharing can be made by contacting the corresponding author. Individual participant data that underlie the results reported in this article will be made available (after deidentification) from 9 to 36 months after article publication. Data sharing will be limited to investigators whose proposed use of the data has been approved by an independent review committee identified for this purpose.
Acknowledgments
Financial support for this work was provided by Vivex Biologics (Miami, FL, USA). The authors appreciate the thorough review by Jon E. Block, Ph.D., and the manuscript preparation by Malahki Thorn.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This research was supported by VIVEX Biologics, Inc., Miami, FL, USA.
Disclosure
Dr Derron Wilson reports personal fees for speakers bureau, consulting and/or research from Abbott Medical, Saluda Medical, Boston Scientific, and ViVex, outside the submitted work. Dr Raj Patel is a consultant for Vivex, outside the submitted work. Dr Shiraz Yazdani is a consultant for Medtronic, Abbott, and Vivex, outside the submitted work. The authors declare no other conflicts of interest in this work.
References
1. Lorio MP, Yuan HA, Beall DP, Block JE, Andersson GBJ. The role of ISASS in evolving the spine code landscape: lumbar discogenic pain receives specific ICD-10-CM code. Int J Spine Surg. 2024;18(4):353–7. doi:10.14444/8622
2. Bogduk N, Aprill C, Derby R. Lumbar discogenic pain: state-of-the-art review. Pain Med. 2013;14(6):813–836.
3. Lorio MP, Beall DP, Myers TJ, et al. A proposed diagnostic and treatment algorithm for the management of lumbar discogenic pain. J Pain Res. 2025;18:3331–3343. doi:10.2147/JPR.S522750
4. Ravikanth R. A review of discogenic pain management by interventional techniques. J Craniovertebr Junction Spine. 2020;11(1):4–8. doi:10.4103/jcvjs.JCVJS_19_20
5. Remotti E, Nduaguba C, Woolley PA, et al. Review: discogenic back pain: update on treatment. Orthop Rev. 2023;15:84649.
6. Lorio MP, Tate JL, Myers TJ, Block JE, Beall DP. Perspective on intradiscal therapies for lumbar discogenic pain: state of the science, knowledge gaps, and imperatives for clinical adoption. J Pain Res. 2024;17:1171–1182.
7. Grider JS, Deer TR, Beall DP, et al. A primer on anatomy, biophysics, pathology, imaging and treatment of the intervertebral disc and the anterior spinal column: the Discogenic, Intervertebral, Spinal Column (DISC) ASPN workgroup. J Pain Res. 2025;18:6651–6698.
8. Azeem N, Myers TJ, Tate JL, Gilmore CA, Harper AS, Block JE. Supplemental nucleus pulposus allograft in patients with lumbar discogenic pain: evaluation of clinical outcomes and quality of life in medicare beneficiaries. Clin Interv Aging. 2025;20:717–726.
9. Beall DP, Davis TT, Amirdelfan K, et al. Nucleus pulposus allograft supplementation in patients with lumbar discogenic pain: initial 6-month outcomes from a prospective clinical pilot study. Pain Physician. 2024;27(8):E865–E871. doi:10.36076/ppj.2024.7.E865
10. Beall DP, Davis TT, Amirdelfan K, et al. Supplemental nucleus pulposus allograft in patients with lumbar discogenic pain: results of a prospective feasibility study. BMC Musculoskelet Disord. 2025;26(1):437.
11. Costandi S, Beall DP, Davis TT, et al. Durability of supplemental nucleus pulposus allograft in patients with lumbar discogenic pain. J Pain Res. 2025;18:1901–1908. doi:10.2147/JPR.S516571
12. Langhorst ML, Kendall DR, Umapathy S, Soin A, Lorio MP. Safety evaluation of intradiscal delivery of nucleus pulposus allograft for lumbar discogenic pain. Int J Spine Surg. 2025;19(S3):S48–S53. doi:10.14444/8808
13. Fekete TF, Haschtmann D, Kleinstuck FS, Porchet F, Jeszenszky D, Mannion AF. What level of pain are patients happy to live with after surgery for lumbar degenerative disorders? Spine J. 2016;16(4 Suppl):S12–18. doi:10.1016/j.spinee.2016.01.180
14. Pham T, Tubach F. Patient acceptable symptomatic state (PASS). Joint Bone Spine. 2009;76(4):321–323. doi:10.1016/j.jbspin.2009.03.008
15. Lorio MP, Beall DP, Calodney AK, Lewandrowski KU, Block JE, Mekhail N. Defining the patient with lumbar discogenic pain: real-world implications for diagnosis and effective clinical management. J Pers Med. 2023;13(5):821.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.