Back to Journals » Journal of Pain Research » Volume 16
Comparing Continuous and Intermittent Infusion Effects on Serratus Anterior Plane Blocks in Video-Assisted Thoracoscopic Surgery: A Randomized Clinical Trial
Authors He K ![]() , Meng Y
, Meng Y ![]() , Zhu Y, Wang S
, Zhu Y, Wang S ![]() , Zong Y
, Zong Y
Received 17 August 2023
Accepted for publication 14 November 2023
Published 22 November 2023 Volume 2023:16 Pages 4015—4024
DOI https://doi.org/10.2147/JPR.S431453
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Jinlei Li
Keqiang He,1,* Yan Meng,1,* Yun Zhu,2 Sheng Wang,1 Yu Zong1
1Department of Anesthesiology, the First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China, Hefei, People’s Republic of China; 2Department of Radiology, the First Affiliated Hospital of Bengbu Medical College, Bengbu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yu Zong, Department of Anesthesiology, the First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China, 17 Lujiang Road, Hefei, Anhui, People’s Republic of China, Email [email protected]
Objective: The programmed intermittent bolus infusion (PIBI) of local anesthetic produces wider sensory blockade and better analgesia than continuous infusion (CI). We designed this trial to compare the effects of these two different infusion methods combined with Serratus Anterior Plane Blocks (cSAPBs) on postoperative pain relief in patients undergoing video-assisted thoracoscopic surgery.
Methods: We randomly allocated 66 patients under going elective video-assisted thoracoscopic unilateral lung resection surgery to two groups (PIBI group and CI group, n=33 per group). After the surgical operation, the patients received ultrasound-guided ipsilateral SAPB, we randomized them to receive either automated intermittent boluses or continuous infusion of 0.3% ropivacaine. Tramadol consumption during the 48 hours following surgery was the primary outcome. Secondary outcomes included cumulative tramadol consumption during the first 24-h and the second 24-h periods after surgery, pain scores, patient satisfaction, blocked dermatomes, and adverse events.
Results: During 48h, tramadol consumption in the PIBI group was significantly lower than in the CI group (190 mg [125, 305] vs 220 mg [170, 480], p= 0.034). As compared to the CI group, the PIBI group consumed less tramadol during the first 24 hours (145 mg [87.5, 210] vs 190 mg [140, 400], p=0.012). The dermatomes anesthetized to the pinprick and cold test were significantly more abundant in the PIBI group than in the CI group (3 [3,4] vs. 5 [4,5], p< 0.001). Both groups had similar VAS scores at rest and when moving (p> 0.05). Additionally, the PIBI group showed greater patient satisfaction. Both groups experienced similar adverse events (p> 0.05).
Conclusion: Compared with CI, PIBI administration regimen (0.3% ropivacaine 5 mL/h) for cSAPBs resulted in lower tramadol consumption, superior analgesia during the initial 12 h after the operation, and higher patient satisfaction. PIBI combined with cSAPBs was a better choice for postoperative analgesia in patients undergoing video-assisted thoracoscopic surgery.
Keywords: continuous serratus anterior plane block, programmed intermittent bolus infusion, video-assisted thoracoscopic surgery, perioperative analgesic therapy
Introduction
Thoracoscopic surgery frequently results in severe pain that may contribute to respiratory compromise and an increased risk of pulmonary morbidity.1,2 Additionally, inadequate postoperative analgesia hinders early mobilization and functional recovery. Therefore, appropriate pain management after thoracoscopic surgery is crucial The European Society of Thoracic Surgeons’ guidelines for enhanced thoracic surgery recovery suggest that regional anesthesia-based, opioid-sparing analgesia regimens provide improved analgesia.3
Serratus anterior plane blocks (SAPBs) have widely been used for multi-modal analgesia strategies in the clinic. They have shown to effectively relieve postoperative pain for procedures such as breast4 and thoracoscopic surgery,5 rib fractures6 and minimally invasive heart surgery.7 Studies comparing traditional regional anesthesia techniques such as thoracic epidural,8 thoracic paravertebral blockade,9 and intercostal nerve blocks9 to SAPB have shown equal analgesic efficacy and better pain scores, with less opioid consumption in favor of SAPB.
Factors that affect the efficacy of regional anesthesia, such as the concentration and volume of local anesthetic used, catheter placement, and the type of nerve block approach, do so mainly by influencing the spread of local anesthetic.1 However, the local anesthetic infusion method may also influence the anesthetic efficacy. Commonly used infusion methods include programmed intermittent bolus infusion (PIBI) and continuous infusion (CI). PIBI has drawn interest recently due to its better analgesia and wider sensory blockade when compared with CI in numerous studies.10–12
Compared to other analgesic modalities, SAPB is a new analgesic technique applied to the clinic proposed, and can offer a straight forward procedure, minimal complications, stable hemodynamics, and enhanced pain relief for patients undergoing VATS.13 However, few studies have compared the analgesic effect of PIBI in combination with PCA vs. CI in combination with PCA during a continuous thoracic SAPB. We hypothesized that PIBI combined with cSAPBs is superior to CI for postoperative analgesia in patients after a video-assisted thoracoscopic lung resection.
Methods
Recruitment
The First Affiliated Hospital of the University of Science and Technology of China (USTC) Ethics Committee approved this study (number 2022 KY 064; date of approval, April 12, 2022). In accordance with the Helsinki Declaration, written informed consent was obtained from all patients participating in the trial. At https://www.chictr.org.cn/bin/project/edit?pid=173328, we registered the trial before patient enrollment.(ChiCTR2200062753; principal investigator, Zong Yu; date of registration, 2022/8/18). We conducted the study in the First Affiliated Hospital of USTC from August 2022 to December 2022. This article adhered to the applicable Consolidated Standards of Reporting Trials (CONSORT) guidelines.
We enrolled 66 patients scheduled to undergo elective video-assisted thoracoscopic lung resection surgery who agreed to have a continuous SAPB (cSAPB) for postoperative analgesia.
Patients aged 18–70 years, classified as American Society of Anesthesiologists physical status I–III, body mass index (BMI) between 18.5 and 30 kg/m2 and scheduled for video-assisted thoracoscopic unilateral lung resection surgery were recruited. Exclusion criteria included SAPB refusal, contraindication to peripheral nerve block, allergy to study medication, preoperative use of opioids and steroids, apparent neuropathy and and intraoperative conversion of thoracoscopic surgery to open thoracotomy.
Randomization and Blinding
We randomly distributed the 66 patients meeting the enrolment criteria into the PIBI or CI groups by a computer-generated random number table An anesthesiologist (A1) unknown to the other study anesthesiologists (A2–A3) generated the computerized randomization list. In the PIBI group, patients received an initial 20 mL bolus of 0.3% ropivacaine, followed by intermittent boluses with 0.3% ropivacaine (5mL/h). In the CI group, patients received an initial 20-mL bolus of 0.3% ropivacaine, followed by CI at a rate of 5 mL/h of 0.3% ropivacaine. A PCA pump (ZZB-I/IV; AiPeng Medical Technology, Jiangsu, China) was also available for the patients to self-inject tramadol boluses as needed. The infusion pressure of the PCA pumps was 82.5–95.5 Kpa. PCA pumps were used to deliver all drugs. An anesthesiologist (A1) set the pump parameters, and patients and other anesthesiologists (A2–A3) were blinded to the drugs’ infusion regimens.
Anesthesia Management and Postoperative Analgesia
All patients were fasted state for 8 h and prevented from drinking for 4 h before the operation. In the operation room, an intravenous line was secured.We inserted a radial artery catheter and a standard monitor was applied. After induction of general anesthesia with midazolam (0.05mg/kg), propofol (2mg/kg), sufentanil (0.4 µg/kg), and rocuronium (1 mg/kg), a double-lumen tube was intubated and confirmed its position by bronchoscopy. During surgery, general anesthesia was maintained with sevoflurane, propofol to maintain bispectral index of 40–60 and remifentanil was infused for intraoperative analgesia. An additional sufentanil (0.15μg/kg) was administered before incision closure.
Atracurium cisphenylate was infused intra-operatively as needed. Intravenous infusions of 100 mg of flurbiprofen axetil and 0.06 mg/kg of oxycodone were administered at skin closure. Subsequently, we started a PCA pump with tramadol boluses of 10 mg (without a background infusion dose) and a 10-min lockout for 48 h after the operation. In addition, all the patients received 100 mg of flurbiprofen intravenously every 12 h for 48 h after the operation. When pain scores at rest were reported as 4 or more, or at the patient’s request, both groups received additional tramadol (50mg).
cSAPB Procedure
After the surgical procedures, the patients were kept in a lateral position and general anesthesia was continued by infusion of propofol as needed. An experienced attending anesthesiologist (A2) skilled in ultrasound-guided SAPB used a linear probe (13–6 MHz) to scan along the midaxillary line and identify the serratus anterior and latissimus dorsi muscles overlying the fourth to sixth ribs. To avoid the chest tube, the anesthesiologist inserted the epidural needle (Tuoren, China) into the plane underneath the serratus anterior muscle (SAM) at the fourth, fifth, or sixth rib in the mid-axillary line. After injecting 3 mL of saline and confirming the position of the needle tip, the anesthesiologist opened the potential interfacial space between the ribs and positioned the peripheral nerve catheter to block the SAM. Using ultrasound, the catheter-over-needle position was verified and the needle was withdrawn. Subsequently, a loading bolus of 20 mL of 0.3% ropivacaine was administered via the catheter. An injection of 0.3% ropivacaine was then given using a PCA pump.
Outcome Assessment
Tramadol consumption within 48 hours after surgery was the primary outcome. In addition to the VAS pain scores, the cumulative tramadol consumption in the first 24 and second 24 hours post-operatively, patient satisfaction and blocked dermatomes, adverse events were also assessed as secondary outcomes. During 2 hours, 4 hours, 8 hours, 12 hours, 24 hours, and 48 hours after the operation, at rest and coughing, we assessed postoperative pain using a 10-point VAS. A 5-point Likert scale, from 1 very unsatisfactory to 5 very satisfactory, was used to evaluate the patient’s satisfaction with the analgesia 48 h after the operation.14 The anesthesiologist (A3) tested the blocked dermatomere 24h post-operatively and assessed and recorded nausea, vomiting, and other adverse events 48 h after the operation. We used alcohol swabs to test the nerve block effect and defined the block as successful when coldness was lost or markedly reduced.
Sample Size Calculation
We determined the sample size using Power Analysis and Sample Size (PASS) 15, considering that a 20% decrease in total tramadol consumption with a PIBI combined with cSAPB would be clinically relevant. Gao W et al,15 found that patients with a CI combined with cSAPB had a mean tramadol consumption of 250 mg at 48 h postoperatively. We assumed that the standard deviation for both groups was 45. We estimated 30 patients in each group for a significance level of 0.05 and a power of 0.9. To account for a 10% loss to follow-up, we planned to recruit at least 33 patients each group.
Statistical Analysis
We conducted the data analysis using SPSS 27 (IBM Corp, Armonk, NY, USA). Descriptive data are displayed as means (with SD) or medians (with interquartile range) depending on the distribution of data (normal or skewed), and categorical data are displayed as percentages. The Chi-square test or Fisher’s exact test was used for categorical data and the Mann–Whitney U-test were used for nonparametric statistics. All statistical tests were 2-tailed. A p value <0.05 was considered statistically significant.
Results
We obtained our results between August and December 2022 at the First Affiliated Hospital of USTC, China. As shown in Figure 1, after screening 107 patients for recruitment, 41 patients were excluded and a total of 66 patients were randomly assigned to groups CI and PIBI (n=33 in each group), with 61 patients receiving primary outcomes. A flow chart illustrating the study conditions is shown in Figure 1. Both groups had similar demographic characteristics and surgical procedures (p>0.05; Table 1).
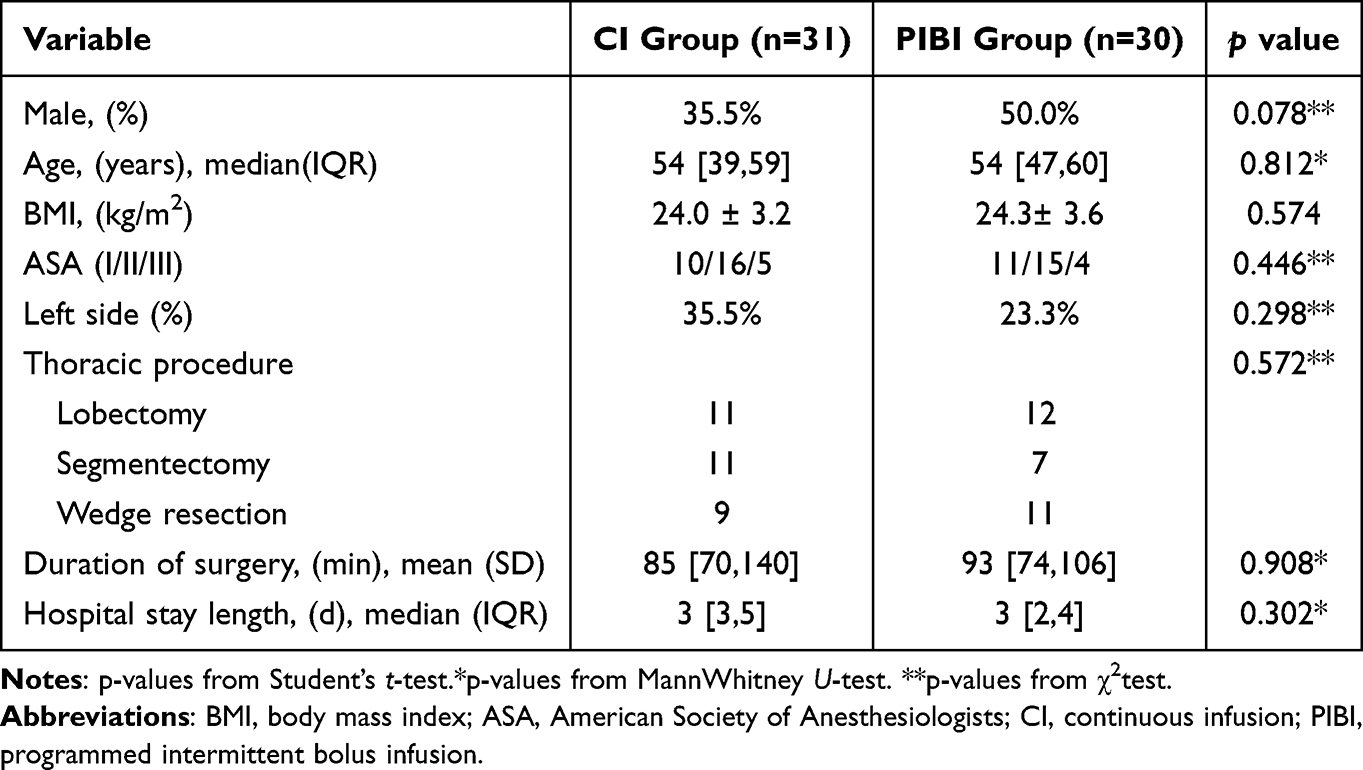 |
Table 1 Demographic and Clinical Characteristics of the Patients (n=61) |
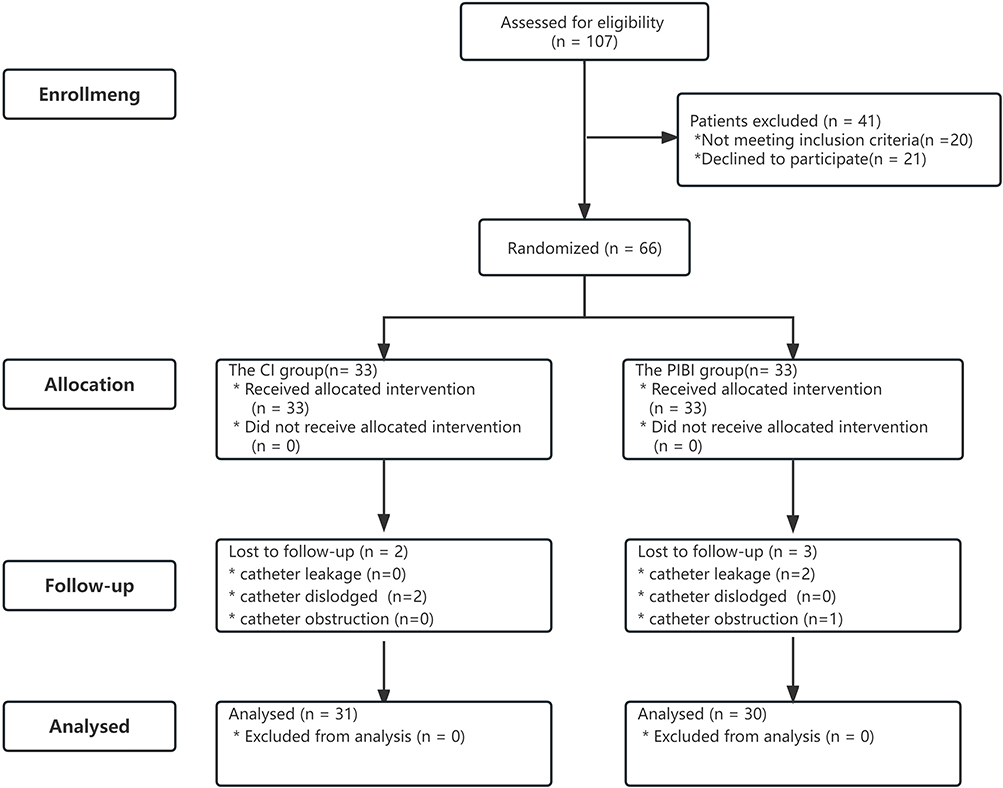 |
Figure 1 Flow diagram of the study. |
Tramadol Consumption
As shown in Table 2, during the first 24 h and the 48h after the operation, as compared to the CI group, the PIBI group had lower cumulative tramadol levels (145 mg [87.5, 210] vs 190 mg [140, 400], p=0.012; 190 mg [125, 305] vs 220 mg [170, 480], p= 0.034; respectively). We found similarly tramadol consumptions in the two groups during the second 24 h after surgery (20 mg [20,42.5] vs. 30 mg [20,60], p= 0.259). Compared to the first postoperative day, the cumulative amount of tramadol showed remarkably reduced in the second postoperative day in the two group (30 mg [20,60] vs 190 mg [140,400]; 20 mg [20,42.5] vs 145 mg [87.5,210], all p=0.001; respectively; Table 2).
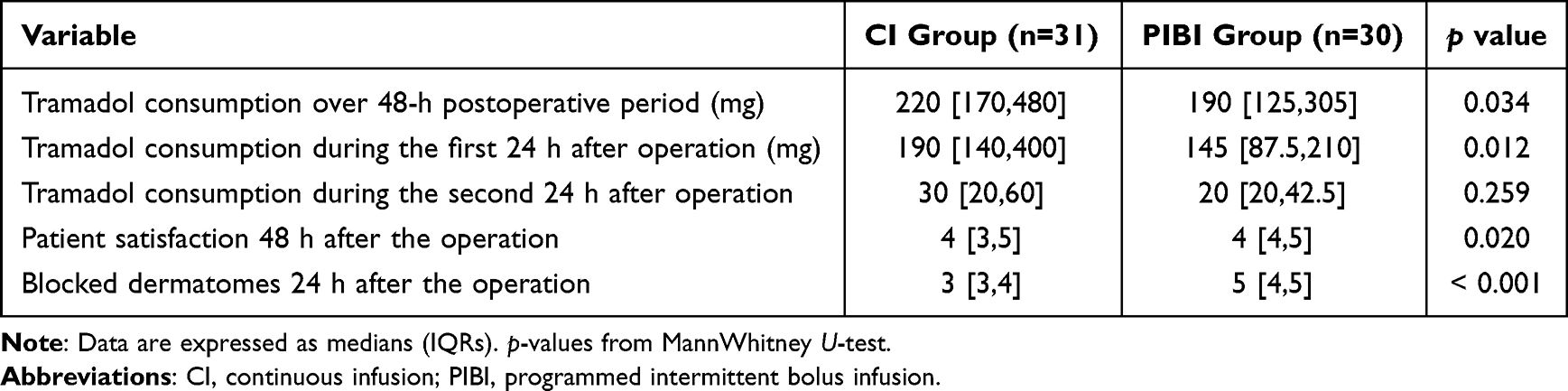 |
Table 2 Tramadol Consumption, Patient Satisfaction, and Blocked Dermatomes by Group |
Postoperative Pain VAS Scores
According to Figure 2, both groups experienced similar levels of pain at rest and during movement (p > 0.05). A slight difference in VAS scores on movement was observed between the PIBI group and the CI group at 8 and 12 h postoperatively, however, these differences were not statistically significant (3 [3,3.25] vs 4 [3,4], p= 0.056, and 3 [3,4] vs 4 [3,4], p=0.052). At 8 and 12 h postoperatively, the proportion of patients with VAS scores ≥4 on movement in the PIBI group (22.6% or 7/30 at 8 h and 30% or 9/30 at 12 h; p= 0.012) was statistically lower than in the CI group (54.8% or 17/31 at 8 h and 64.6% or 20/31 at 12 h; p= 0.007).
 |
Figure 2 Violin plot of VAS scores at rest and upon movement at 2, 4, 8, 12, 24, and 48 h after operation. p-values from MannWhitney U-test. Abbreviations: CI, continuous infusion; PIBI, programmed intermittent bolus infusion; VAS, visual analogue scale. |
Blocked Dermatomes
As summarized in Table 2, we observed a statistically significant difference in the presence of a sensory block 24 h postoperatively between the groups. The PIBI group anesthetized significantly more dermatomes than the CI group (3 [3,4] vs. 5 [4,5], p<0.001).
Adverse Events
No complications such as hypotension, respiratory depression, or local anesthetic toxicity were encountered by patients during the perioperative study period.
Patient Satisfaction
As compared to the CI group, the PIBI group scored significantly higher in terms of patient satisfaction (p<0.001) (Table 2).
Discussion
Many studies in various clinical settings, including epidural analgesia for labor,12 popliteal sciatic nerve block,16 paravertebral block,17 and femoral nerve block,18 have been demonstrated the enhanced benefits of PIBI compared to CI. However, there are also studies with contradictory results.19,20 Hamdani et al19 showed that in patients undergoing cIBPB after shoulder surgery, PIBI combined with PCA did not reduce local anaesthetic consumption or rescue analgesia compared to CI combined with PCA. Similarly, Oxlund et al20 also concluded that PIBI did not show obvious advantages over CI in reducing pain or opioid consumption. However, studies of PIBI in anterior serratus plane block is rarely.
The aim of this prospective randomized trial was to evaluate the efficacy of PIBI and CI with cSAPB on pain relief following thoracoscopic surgery. Our findings demonstrate that cumulative tramadol consumption was lower in patients in the PIBI group compared with those in the CI groups at 48 h postoperatively. In the PIBI group, the width of the dermatomal sensory block was larger than that of the CI group. With the highest median VAS pain score occurring 8 to 12 h postoperatively. In addition, our results revealed that the PIBI regimen, compared to the CI regimen, reduced patients’ VAS scores on movement from 8 to 12 h postoperatively, although this difference did not reach statistical significance. The magnitude of the reduction in VAS scores was small (<1 point), but the proportion of patients with VAS scores ≥4 (moderate pain requiring further medical intervention) in the PIBI group was statistically significantly less than that in the CI group.
Overall, our results indicate that the PIBI regimen provided relatively satisfactory pain relief following thoracoscopic surgery, marginally better than the CI regimen. In addition, compared with the CI regimen, the PIBI regimen allowed for a significant reduction in the total amount of IV tramadol in the early postoperative period, with a wider dermatomal sensory block, even though small differences in patients’ VAS scores on movement postoperatively. It21 was considered a greater usage of opioids postoperatively a simple marker for identifying patients who might be at risk for postoperative chronic pain syndrome. An opioid-sparing anesthesia/analgesia technique could reduce the incidence of this complication. Taken together, these results suggest that the PIBI regimen might be superior to the CI regimen.
In order to ensure accurate and reliable results, we carefully considered the factors that may have influenced our findings. We used ultrasound to precisely position the catheters, as ultrasound can clearly distinguish anatomic structures and accurately locate the needle tip while avoiding blood vessel clusters and pleura. Additionally, we used cSAPB, are liable technique. During the study period, 5 of 66 patients developed treatment failure: 2 failures due to accidently removed catheters caused by the patients’ unintentional violent pull, 2 failures due to catheter leakage only in the PIBI group. We hypothesized this was due to the short subcutaneous tunnel of the catheter, as well as the single high dose of local anesthetics infused rapidly to the serratus anterior plane with a higher speed and pressure in the PIBI group. The leakage disappeared when we prolonged the subcutaneous tunnel. The catheter we inserted had a side hole to facilitate the diffusion of local anesthetics, and to avoid catheter obstruction. We only encountered one patient with catheter obstruction, and we can exclude any impact of cSAPB failure on our results. As a result, we decreased the heterogeneity of the clinical intervention by using the same anesthesiologist for every cSAPB procedure. Moreover, the participants were only subjected to unilateral thoracoscopic wedge resections performed through a single incision in order to reduce bias associated with different levels of surgical trauma. Finally, the intercostal space we blocked was located at the surgical port chosen by the surgeon to access the tumor site, and was thus covered by analgesia.
Thoracoscopic surgery has become preferable to thoracotomy due to its lower stress reaction and smaller surgical incision.22 However, thoracoscopic operations still require adequate analgesia due to the pain they may cause.23 Potential explanations for the mechanisms of this pain include cuts to the skin, subcutaneous tissue, and muscle and nerve injury from ports, surgical instruments, and retractors.24 Compression injuries of intercostal nerves may also cause neuropathic pain.25 Many studies have reported similar incidences of neuropathic pain after VATS and thoracotomies.26,27 Additionally, chest tubes are essential for thoracic surgery, and postoperative pain can result from traction or injury of the intercostal nerves, compression or injury of the pleura, and stimulation by the chest tube.28 Yang et al29 found that the most painful time for patients undergoing thoracoscopic surgery is during the first day after the procedure. Our results confirmed that the consumption of rescue analgesics in the second postoperative day was lower comparing with the first day. Taketa et al30 reported that, without adequate pain control during the perioperative period, patients may experience moderate to severe pain during the first 2 to 6 h postoperatively. However, our results indicate that VAS scores were only significantly increased in both groups at 8 and 12 h postoperatively. We adopted a multimodal analgesia protocol for postoperative analgesia: an intravenous infusion of 100 mg of flurbiprofen axetil and 0.06 mg/kg of oxycodone at skin closure, and then an initial bolus of 0.3% ropivacaine (20 mL) after the catheter had been successfully placed. The multimodal analgesia protocol resulted in excellent postoperative analgesia in the immediate and early postoperative periods. However, this benefit largely disappeared after the first postoperative 8 h, a finding consistent with the reported duration of analgesia.31,32
Throughout our follow-up period, we found that chest tube-related pain was the most frequent complaint, with fewer complaints of incisional pain. The thorax and lungs are innervated by the intercostal, vagus, and phrenic nerves,33 while the lobectomy area is innervated by the thoracodorsal, long thoracic, medial and lateral pectoral nerves.28 The difficulty of completely blocking nociceptive signals from the long thoracic nerve (LTN)and the phrenic, thoracic dorsal, vagus, and intercostal nerves, via thoracic epidural anesthesia, thoracic paravertebral block, or selective intercostal nerve block, is the primary cause of chest tube-related pain. Anatomically, the serratus anterior is a quadrilateral muscle located on the lateral chest, and the thoracic dorsal nerve, the lateral cutaneous branch of the intercostal nerve, and the LTN are distributed around the muscle.13 Blanco et al34 introduced SAPBs for the first time in 2013 and confirmed that the technology achieves numbness from T2 to T9. Mayes et al35 conducted a study on ultrasound-guided SAPB with 20 mL of methylene blue on cadavers, and their results suggested that SAPB blocks the lateral cutaneous branches of the intercostal nerves, rather than directly blocking the intercostal nerves. Khemka et al36 proposed that SAPB can block the LTN and dorsal thoracic nerves without the risk of complications such as epidural hematoma or hypotension. Varghese et al37 demonstrated that a properly performed SAP block spreads sufficiently to cover the LTN and the lateral cutaneous branches fromT2 to T5 intercostal nerves. SAPB has been shown to be an appropriate analgesia technique for different procedures (thoracotomy,38 breast surgery,39 rib fractures,40 thoracoscopic surgery.41 Chu et al42 reported that patients scheduled for thoracotomy may benefit from SAPBs, providing evidence through a case report of the complementary effects of SAPB and paravertebral nerve blocks in reducing chest tube-related pain.
The serratus anterior plane is a virtual space containing the thoracic dorsal nerve, the lateral cutaneous branch of the intercostal nerve, and the LTN. Injectin glocal anesthetic into the plane produces a nerve blockade around the injection site, theoretically reducing nociceptive signal transmission and providing effective analgesia after thoracoscopic surgery. The volume, pressure, infusion rate, and intervals of local anesthetics are crucial in determining the extent of the continuous peripheral nerve block.11 Compared with the CI regimen, PIBI allows procedure specific volumes of local anesthetic to be released rapidly and can generate higher local pressures that can probably compensate for the distance between the catheter orifice and the target nerve, making it easy to block more target nerves. Studies on the efficacies of PIBI and CI regimes for continuous peripheral nerve block have reported PIBI advantages,10,11,43 and our data also confirms those. We observed a wider dermatome spread with the PIBI regimen at 24 h than with the CI regimen. This resulted in better analgesia, improved patient and reduced postoperative tramadol consumption. However, the pain scores remained similar in the two groups. We assume this may be due to the following reasons: First, to avoid bias from to different extents of surgical trauma, patients undergoing unilateral thoracoscopic wedge resection with a single incision were enrolled. As a result, the need for dermatomal blocking may have been reduced and the difference between the two groups in postoperative pain scores may have been influenced. The advantages of the PIBI regimen may be more evident in procedures with a wide incision, such as open thoracotomy or extended radical mastectomy. Second, to provide pain management for all patients, were confirmed the catheter tip position with ultrasound before administering a 20-mL loading dose of 0.3% ropivacaine via the catheter. This bolus contributed to relieve acute pain in the early postoperative period, but it may have also performed a hydrodissection expanding the serratus anterior plane space to facilitate the diffusion of the local anesthetic. Taketa et al17 revealed that the initial bolus injection may obscure the detection of differences between infusion methods. It may have confounded the postoperative analgesic outcomes during the early period of time because of the combined effects of the first bolus injection and the subsequent infusion. Alternatively, the early analgesic effects produced by the initial bolus injection may have a pre-emptive effect on the long-term analgesia.44 The current study, though limited, supports the efficacy and safety of PIBI regimen in serratus anterior plane blocks as analgesic options to reduce pain and opioid consumption for multimodal analgesia strategies in Video-Assisted Thoracoscopic Surgery.
We are aware of other limitations of our study in addition to those already mentioned. First, the differences in local anesthetic dose may have impaired detection of differences between the infusion methods. We maintained the infusion protocol of the local anesthetic constant throughout the study and administered tramadol as postoperative supplemental analgesia. Despite this, a major advantage of peripheral nerve block is its ability to reduce postoperative opioid use and prevent adverse side effects. Second, the optimal delivery regimen for PIBI remains unclear. Studies have shown that the mean duration of a single peripheral nerve block with ropivacaine lasts 2–6h.39 Additionally, our previous study demonstrated that 0.2% ropivacaine (8 mL/2 h) for continuous interscalene brachial plexus block provides superior analgesia after surgery compared with 4mL/h.10 As 0.3% ropivacaine infusion (5 mL/h) is the basal method, a longer interval with a larger injection volume of ropivacaine may better highlight the advantages of the PIBI regimen for cSAPB and result in superior outcomes. Vandepitte et al45 describes that small changes in volume of ropivacaine may have significant clinical effect. Even though, in theory, a larger volume can produce stronger analgesic effects, but may also increase the frequency of side effects. Future studies will be needed to determinate the optimal volume and dose of ropivacaine for postoperative pain relief in both automated intermittent bolus and continuous infusion regimens.
Conclusion
Compared with the CI regimen, the PIBI regimen with 0.3% ropivacaine (5 mL/h) for cSAPB can result in lower tramadol consumption, better analgesia after thoracoscopic surgery, and higher patient satisfaction. This study, supports the efficacy and safety of PIBI regimen in serratus anterior plane blocks as analgesic options to reduce pain and opioid consumption for multimodal analgesia strategies in Video-Assisted Thoracoscopic Surgery. Future studies should focus on the optimal volume of ropivacaine and time intervals in PIBI regimens for postoperative analgesia.
Data Sharing Statement
The authors state that all data in the manuscript are accessible if requested (contact e-mail address [email protected]). The authors verify that all data intended for sharing is de-identified.
Funding
This study was supported by the “Rui” Special Fund for Scientific Research from Hubei Chen Xiaoping Science and Technology Development Foundation (CXPJJH1200000-07-113). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Chen L, Wu Y, Cai Y, et al. Comparison of programmed intermittent bolus infusion and continuous infusion for postoperative patient-controlled analgesia with thoracic paravertebral block catheter: a randomized, double-blind, controlled trial. Reg Anesth Pain Med. 2019;44(2):240–245. doi:10.1136/rapm-2018-000031
2. Wei X, Yu H, Dai W, et al. Patient-Reported Outcomes of Video-Assisted Thoracoscopic Surgery Versus Thoracotomy for Locally Advanced Lung Cancer: a Longitudinal Cohort Study. Ann Surg Oncol. 2021;28:8358–8371.
3. Batchelor TJP, Rasburn NJ, Abdelnour-Berchtold E, et al. Guidelines for enhanced recovery after lung surgery: recommendations of the Enhanced Recovery After Surgery (ERAS®) Society and the European Society of Thoracic Surgeons (ESTS). Eur J Cardiothorac Surg. 2019;55(1):91–115. doi:10.1093/ejcts/ezy301
4. Mazzinari G, Rovira L, Casasempere A, et al. Interfascial block at the serratus muscle plane versus conventional analgesia in breast surgery: a randomized controlled trial. Reg Anesth Pain Med. 2019;44:52–58.
5. Park MH, Kim JA, Ahn HJ, et al. A randomised trial of serratus anterior plane block for analgesia after thoracoscopic surgery. Anaesthesia. 2018;73:1260–1264.
6. Rose P, Ramlogan R, Sullivan T, et al. Serratus anterior plane blocks provide opioid-sparing analgesia in patients with isolated posterior rib fractures: a case series. Can J Anaesth. 2019;66:1263–1264.
7. Berthoud V, Ellouze O, Nguyen M, et al. Serratus anterior plane block for minimal invasive heart surgery. BMC Anesthesiol. 2018;18:144.
8. Kaur R, Anwar S. Serratus anterior plane block versus thoracic epidural analgesia for post-thoracotomy pain relief. J Cardiothoracic Vascular Anesthesia. 2018;32(6):e11–e12.
9. Kaushal B, Chauhan S. Comparison of the efficacy of ultrasound-guided serratus anterior plane block, pectoral nerves II block, and intercostal nerve block for the management of postoperative thoracotomy pain after pediatric cardiac surgery. J Cardiothoracic Vascular Anesthesia. 2018;33(2):418–425.
10. Meng Y, Wang S, Zhang W, et al. Effects of Different 0.2% Ropivacaine Infusion Regimens for Continuous Interscalene Brachial Plexus Block on Postoperative Analgesia and Respiratory Function After Shoulder Arthroscopic Surgery: a Randomized Clinical Trial. J Pain Res. 2022;15:1389–1399. doi:10.2147/JPR.S362360
11. Yang L, Huang X, Cui Y, et al. Combined Programmed Intermittent Bolus Infusion With Continuous Infusion for the Thoracic Paravertebral Block in Patients Undergoing Thoracoscopic Surgery: a Prospective, Randomized, and Double-blinded Study. Clin J Pain. 2022;38(6):410–417. doi:10.1097/AJP.0000000000001037
12. Mo X, Zhao T, Chen J, et al. Programmed Intermittent Epidural Bolus in Comparison with Continuous Epidural Infusion for Uterine Contraction Pain Relief After Cesarean Section: a Randomized, Double-Blind Clinical Trial. Drug Des Devel Ther. 2022;16:999–1009.
13. Chen JQ, Chen JR, Wang S, et al. Effect of Perineural Dexamethasone with Ropivacaine in Continuous Serratus Anterior Plane Block for Postoperative Analgesia in Patients Undergoing Video-Assisted Thoracoscopic Surgery. J Pain Res. 2022;15:2315–2325. doi:10.2147/JPR.S372071
14. Jebb AT, Ng V, Tay L. A review of key Likert scale development advances: 1995–2019. Front Psychol. 2021;12:637547. doi:10.3389/fpsyg.2021.637547
15. Gao W, Yang XL, Hu JC, et al. Continuous Serratus Anterior Plane Block Improved Early Pulmonary Function After Lung Cancer Surgical Procedure. Ann Thorac Surg. 2022;113(2):436–443. doi:10.1016/j.athoracsur.2021.02.032
16. Taboada M, Rodríguez J, Bermudez M, et al. Comparison of continuous infusion versus automated bolus for postoperative patient-controlled analgesia with popliteal sciatic nerve catheters. Anesthesiology. 2009;110(1):150–154. doi:10.1097/ALN.0b013e318191693a
17. Taketa Y, Irisawa Y, Fujitani T. Programmed intermittent bolus infusion versus continuous infusion of 0.2% levobupivacaine after ultrasound-guided thoracic paravertebral block for video-assisted thoracoscopic surgery: a randomised controlled trial. Eur J Anaesthesiol. 2019;36(4):272–278. doi:10.1097/EJA.0000000000000945
18. Hillegass MG, Field LC, Stewart SR, et al. The efficacy of automated intermittent boluses for continuous femoral nerve block: a prospective, randomized comparison to continuous infusions. J Clin Anesth. 2013;25(4):281–288. doi:10.1016/j.jclinane.2012.11.015
19. Hamdani M, Chassot O, Fournier R. Ultrasound-guided continuous interscalene block: the influence of local anesthetic background delivery method on postoperative analgesia after shoulder surgery: a randomized trial. Reg Anesth Pain Med. 2014;39(5):387–393. doi:10.1097/AAP.0000000000000112
20. Oxlund J, Clausen AH, Venø S, et al. A randomized trial of automated intermittent ropivacaine administration vs. continuous infusion in an interscalene catheter. Acta Anaesthesiol Scand. 2018;62(1):85–93. doi:10.1111/aas.13011
21. Toscano A, Capuano P, Costamagna A, et al. The Serratus Anterior Plane Study: continuous Deep Serratus Anterior Plane Block for Mitral Valve Surgery Performed in Right Minithoracotomy. J Cardiothorac Vasc Anesth. 2020;34(11):2975–2982. doi:10.1053/j.jvca.2020.05.021
22. Petersen RH, Holbek BL, Hansen HJ, Kehlet H. Video-assisted thoracoscopic surgery-taking a step into the future. Eur J Cardiothorac Surg. 2017;51(4):694–695. doi:10.1093/ejcts/ezw381
23. Bai Y, Sun K, Xing X, et al. Postoperative analgesic effect of hydromorphone in patients undergoing single-port video-assisted thoracoscopic surgery: a randomized controlled trial. J Pain Res. 2019;12:1091–1101. doi:10.2147/JPR.S194541
24. Kaplowitz J, Papadakos PJ. Acute pain management for video-assisted thoracoscopic surgery: an update. J Cardiothorac Vasc Anesth. 2012;26(2):312–321. doi:10.1053/j.jvca.2011.04.010
25. Landrenau RJ, Hazelrigg SR, Mack MJ, et al. Postoperative pain related morbidity: video assisted thoracoscopic surgery vs. thoracotomy. Ann Thoracic Surg. 1993;56:1285–1289.
26. Steegers MAH, Snik DM, Verhagen AF, et al. Only half of the chronic pain after thoracic surgery shows a neuropathic component. J Pain. 2008;9:955–961.
27. Wildgaard K, Ravn J, Nikolajsen L, Jakobsen E, Jensen TS, Kehlet H. Consequences of persistent pain after lung cancer surgery: a nationwide questionnaire study. Acta Anaesthesiol Scand. 2011;55(1):60–68. doi:10.1111/j.1399-6576.2010.02357
28. Zeng J, Tang ZH, Liang JQ, et al. Comparison of Various Regional Analgesia Methods for Postoperative Analgesic Effects in Video-assisted Thoracoscopic Surgery: a Systematic Review and Network Meta-analysis. Pain Physician. 2022;25(7):865.
29. Yang XL, Gu H, Hu JC, et al. Operation, Effectiveness, and Limitations of Continuous Serratus Anterior Plane Blocks for Thoracoscopic Surgery in Adults. J Pain Res. 2020;13:2401–2410. doi:10.2147/JPR.S264139
30. Taketa Y, Irisawa Y, Fujitani T. Comparison of analgesic efficacy between two approaches of paravertebral block for thoracotomy: a randomised trial. Acta Anaesthesiol Scand. 2018;62:1274–1279.
31. Zhang P, Liu S, Zhu J, Rao Z, Liu C. Dexamethasone and dexmedetomidine as adjuvants to local anesthetic mixture in intercostal nerve block for thoracoscopic pneumonectomy: a prospective randomized study. Reg Anesth Pain Med. 2019;rapm-2018–100221. doi:10.1136/rapm-2018-100221
32. Wu Y, Kang Y, Li Y, Fu B. Impact of Ultrasound-Guided Deep Serratus Anterior Plane Block Combined With Dexmedetomidine as an Adjuvant to Ropivacaine Inpatient Quality of Recovery Scores Undergoing Modified Radical Mastectomy: a Randomized Controlled Trial. Front Oncol. 2022;12:858030. doi:10.3389/fonc.2022.858030
33. Baytar Ç, Aktaş B, Aydin BG, Pişkin Ö, Çakmak GK, Ayoğlu H. The effects of ultrasound-guided serratus anterior plane block on intraoperative opioid consumption and hemodynamic stability during breast surgery: a randomized controlled study. Medicine. 2022;101(35):e30290. doi:10.1097/MD.0000000000030290
34. Blanco R, Parras T, McDonnell JG, Prats-Galino A. Serratus plane block: a novel ultrasound- guided thoracic wall nerve block. Anaesthesia. 2013;68:1107–1113.
35. Mayes J, Davison E, Panahi P, et al. An anatomical evaluation of the serratus anterior plane block. Anaesthesia. 2016;71(9):1064–1069. doi:10.1111/anae.13549
36. Khemka R, Chakraborty A, Ahmed R, Datta T, Agarwal S. Ultrasound-Guided Serratus Anterior Plane Block in Breast Reconstruction Surgery. A Galion Case Rep. 2016;6(9):280–282. doi:10.1213/XAA.0000000000000297
37. Varghese L, Johnson M, Barbeau M, Rakesh SV, Magsaysay P, Ganapathy S. The serratus anterior plane (SAP) block: an anatomical investigation of the regional spread of anesthetic using ultrasound-guided injection. FASEB J. 2016;30:
38. Qiu L, Bu X, Shen J, et al. Observation of the analgesic effect of superficial or deep anterior serratus plane block on patients undergoing thoracoscopic lobectomy. Medicine. 2021;100(3):e24352. doi:10.1097/MD.0000000000024352
39. Shi K, Chen Y, Liu L, et al. Comparison of the effect of different volumes ropivacaine on deep serratus anterior plane block in patients undergoing breast surgery: a prospective randomized double-blinded trial. Ann Palliat Med. 2021;10(6):6104–6111. doi:10.21037/apm-21-199
40. Schnekenburger M, Mathew J, Fitzgerald M, Hendel S, Sekandarzad MW, Mitra B. Regional anaesthesia for rib fractures: a pilot study of serratus anterior plane block. Emerg Med Australas. 2021;33(5):788–793. doi:10.1111/1742-6723.13724
41. Chen JQ, Yang XL, Gu H, Chai XQ, Wang D. The Role of Serratus Anterior Plane Block During in Video-Assisted Thoracoscopic Surgery. Pain Ther. 2021;10(2):1051–1066. doi:10.1007/s40122-021-00322-4
42. Chu GM, Jarvis GC. Serratus Anterior Plane Block to Address Postthoracotomy and Chest Tube-Related Pain: a Report on 3 Cases. A Post Thoracotomy Case Rep. 2017;8(12):322–325. doi:10.1213/XAA.0000000000000502
43. Hansen TG. Ropivacaine: a pharmacological review. Expert Rev Neurother. 2004;4(5):781–791. doi:10.1586/14737175.4.5.781
44. Vogt A, Stieger DS, Theurillat C, Curatolo M. Single-injection thoracic paravertebral block for postoperative pain treatment after thoracoscopic surgery. Br J Anaesth. 2005;95:816–821.
45. Vandepitte C, Gautier P, Xu D, Salviz EA, Hadzic A. Effective volume of ropivacaine 0.75% through a catheter required for interscalene brachial plexus blockade. Anesthesiology. 2013;118(4):863–867. doi:10.1097/ALN.0b013e3182850dc7
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect of Perineural Dexamethasone with Ropivacaine in Continuous Serratus Anterior Plane Block for Postoperative Analgesia in Patients Undergoing Video-Assisted Thoracoscopic Surgery
Chen JQ, Chen JR, Wang S, Gao W, Gu H, Yang XL, Hu JC, Chai XQ, Wang D
Journal of Pain Research 2022, 15:2315-2325
Published Date: 13 August 2022