Back to Journals » Drug Design, Development and Therapy » Volume 17
Comparative Study on the Efficacy of Two Perioperative Chemotherapy Regimens for Lumbar Brucellosis
Authors Wang J ![]() , Deng L, Ding Z, Zhang Y, Zhang Y, Li K, Zhao C, Zhang Q
, Deng L, Ding Z, Zhang Y, Zhang Y, Li K, Zhao C, Zhang Q
Received 25 June 2023
Accepted for publication 15 November 2023
Published 27 November 2023 Volume 2023:17 Pages 3523—3536
DOI https://doi.org/10.2147/DDDT.S427477
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Tin Wui Wong
Jie Wang,1,* Lei Deng,2,* Zihao Ding,3,* Yaosheng Zhang,3 Yao Zhang,1 Kangpeng Li,1 Changsong Zhao,1 Qiang Zhang1
1Department of Orthopedics, Beijing Ditan Hospital, Capital Medical University, Beijing, 100015, People’s Republic of China; 2Department of First School of Clinical Medicine, Henan University of Chinese Medicine, Henan, 450003, People’s Republic of China; 3Department of Orthopedics, Beijing Chaoyang Hospital, Capital Medical University, Beijing, 100020, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qiang Zhang, Department of Orthopedics, Beijing Ditan Hospital, Capital Medical University, Beijing, 100015, People’s Republic of China, Email [email protected]
Objective: The clinical efficacy of perioperative chemotherapy regimen (rifampicin, doxycycline, levofloxacin, ceftriaxone) was evaluated for lumbar brucellosis spondylitis patients with neurological injury.
Methods: In Beijing Ditan Hospital affiliated with Capital Medical University, 32 patients with lumbar brucellosis spondylitis underwent surgery and triple perioperative chemotherapy (rifampicin, doxycycline, levofloxacin) between 2011 and 2021 due to neurological injury, and 34 patients matched up with the triple group underwent rifampicin, doxycycline, levofloxacin, and ceftriaxone. Both groups were compared in terms of changes in inflammation index, low back/leg pain, lumbar function, neurological function, and adverse drug reactions.
Results: There was no significant difference in erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), low back pain visual analogue scale (VAS), leg pain VAS, lumbar Oswestry disability index (ODI) and nerve function injury rate between the two groups before chemotherapy (P> 0.05). The ESR, CRP at 1 week and 2 weeks after chemotherapy and 1 week, 2 weeks, 1 month postoperatively in the quadruple group were significantly lower than those in the triple group, which is the same to ESR 3 months postoperatively (P< 0.05). The low back pain VAS, leg pain VAS and lumbar ODI in the quadruple group were significantly lower than those in the triple group at 1 month and 3 months postoperatively (P< 0.05). The recovery rate of neurological function in the quadruple group was significantly higher than that in the triple group at 3 and 6 months postoperatively (P< 0.05). Both groups did not experience significantly different perioperative and postoperative adverse reactions (P> 0.05).
Conclusion: For lumbar brucellosis spondylitis with neurological injury, quadruple perioperative chemotherapy of rifampicin, doxycycline, levofloxacin and ceftriaxone can significantly reduce perioperative inflammation, and improve low back/leg pain, as well as promoting neurological function recovery in the short term.
Keywords: lumbar brucellosis spondylitis, neurological injury, perioperative chemotherapy, efficacy
Introduction
As Brucella infects intervertebral discs and adjacent vertebrae, brucellosis spondylitis most commonly affects the lumbar spine.1 Since the disease has no specific clinical manifestations at the beginning, it is easy to be misdiagnosed, delaying the appropriate time for conservative treatment in the early stages of the disease. When the spinal infection aggravates and damages the intervertebral disc and vertebral body, the inflammatory granulation tissue or abscess can impair the dural sac and nerve root, causing lower limb sensation or motor symptoms that usually require surgery.2 Surgical treatment is usually administered after erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) have been controlled clearly; the symptoms of brucellosis spondylitis may worsen without timely treatment, even leading to paraplegia; prognosis is also significantly impacted by perioperative inflammatory index control.3 There are no explicit guidelines or norms available for perioperative chemotherapy for lumbar patients with neurological impairment at the present time. The chemotherapy regimens of brucellosis include duplex, triplet and quadruple. When the bone and joint system is involved, duplex or triplet regimens are commonly administered, while the quadruple regimen is effective for complex cases of brucellosis.4 Several drugs are available for treating brucellosis, including rifamycin, tetracyclines, fluoroquinolones, aminoglycosides, and cephalosporins.4–7 During this study, we compared the efficacy and safety of triple (rifampicin, doxycycline, levofloxacin) and quadruple (rifampicin, doxycycline, levofloxacin, ceftriaxone) perioperative chemotherapy regimens. For patients with lumbar brucellosis spondylitis with neurological impairment, the perioperative chemotherapy regimen was evaluated, thus providing a clinical reference point for choosing perioperative chemotherapy.
Materials and Methods
General Information
In the Department of Orthopedics of Beijing Ditan Hospital affiliated with Capital Medical University who underwent surgery due to neurological impairment from 2011 to 2021 with lumbar brucellosis spondylitis, patients were divided into triple groups (rifampicin, doxycycline, levofloxacin) and quadruple groups (rifampicin, doxycycline, levofloxacin, ceftriaxone) based on their perioperative chemotherapy regimens. Both groups were matched in terms of age, gender, disease course, body mass index, lesion segment, paraspinal inflammation, psoas muscle inflammation, operation time, intraoperative blood loss, single segment fusion, double segment fusion, unilateral decompression, bilateral decompression, and follow-up time. The ethics committee of the hospital approved this retrospective study.
Inclusion criteria: (1) the diagnosis of lumbar brucellosis spondylitis is definite; (2) the preoperative imaging data showed that the inflammatory tissue in the spinal canal oppressed the nerve, and the physical examination confirmed the nerve function injury of the lower extremities; (3) the operative method is one-stage posterior focus debridement, decompression, internal fixation and bone graft fusion; (4) the perioperative chemotherapy regimen in the triple group was rifampicin (0.6g po qd; Guangdong Hengjian Pharmaceuticals), doxycycline (0.1g po bid; Jiangsu Lianhuan Pharmaceuticals), levofloxacin (0.2g ivgtt bid; Yangtze River Pharmaceuticals) and that in the quadruple group was rifampicin (0.6g po qd; Guangdong Hengjian Pharmaceuticals), doxycycline (0.1g po bid; Jiangsu Lianhuan Pharmaceuticals), levofloxacin (0.2g ivgtt bid; Yangtze River Pharmaceuticals), ceftriaxone (2g ivgtt qd; Zhejiang Yatai Pharmaceuticals); (5) the follow-up period is more than one year; (6) complete perioperative and follow-up data.
Exclusion criteria: (1) there was no nerve function injury of lower extremities before operation; (2) emergency operation is needed for progressive neurological dysfunction; (3) the mode of operation is focus debridement under intervertebral foramen endoscope; (4) perioperative use of two or other types of triple or quadruple chemotherapy regimens; (5) the focus of the spine is located outside the lumbar spine or multi-segmental brucellosis spondylitis (lumbar vertebrae with thoracic vertebrae, lumbar vertebrae with cervical vertebrae); (6) complicated with other types of spinal infection; (7) age ≥65 years old; (8) complicated with other severe organ dysfunction or disorders that cannot tolerate surgery.
Preoperative Treatment
The lesions were evaluated based on X-ray, CT and magnetic resonance imaging (MRI) of the lumbar spine, and an individualized preoperative plan was prepared (Figure 1, Figure 2). A two-week preoperative chemotherapy regimen was administered to all patients with lumbar brucellosis spondylitis with surgical indications. A triple treatment group was administered rifampicin (600 mg/d) plus doxycycline (200 mg/d) plus levofloxacin (500 mg/d), and a quad treatment group was administered rifampicin (600 mg/d) plus doxycycline (200 mg/d) plus levofloxacin (500 mg/d) plus ceftriaxone sodium (2g/d). The changes of infection indexes were dynamically monitored, and generally speaking, patients are required to undergo surgical treatment after the relief of systemic symptoms and ESR <30mm/h, CRP <10mg/L. Following two weeks of chemotherapy, if the ESR is >30mm/h but is declining and the systemic symptoms have been alleviated, surgical treatment should also be undertaken. Polyetheretherketone (PEEK) cage was used as the material of interbody fusion, prior to the operation of one-stage posterior focus debridement, decompression, internal fixation and bone graft fusion (Figures 1–3), we actively treat the patients’ basic diseases.
 |
Figure 1 Typical cases of perioperative triple chemotherapy. Preoperative X-ray: intervertebral space stenosis of L1/2 and hyperosteogeny at the anterior edge of the vertebral body, formation of beak-like spur (A and B); preoperative CT: intervertebral space of L1/2 is narrow and there is bone destruction of adjacent vertebral body, “lace vertebra” was formed (C and D); preoperative MRI: inflammatory destruction of L1/2 and adjacent vertebrae, formation of inflammatory tissue in spinal canal, inflammatory tissue of psoas major muscle and paraspinal inflammatory tissue, and compression of posterior dural sac and nerve root by inflammatory tissue in spinal canal (E–I); X-ray immediately postoperatively: internal fixation system firmly in place (J and K). |
 |
Figure 2 Typical cases of perioperative quadruple chemotherapy. Preoperative X-ray: a stenosis of the intervertebral space of L4/5 accompanied by a beak-like spur in front of the infected vertebral body (A and B); preoperative CT: there is bone destruction of adjacent vertebral bodies in the intervertebral space of L4/5, forming “lace vertebra” (C and D); preoperative MRI: destruction of L4/5 and adjacent vertebrae, inflammatory tissue formation in spinal canal, inflammatory tissue of psoas major muscle, paraspinal inflammation, and compression of posterior dural sac and nerve root (E–I); X-ray immediately postoperatively: a firmly installed internal fixation system (J and K). |
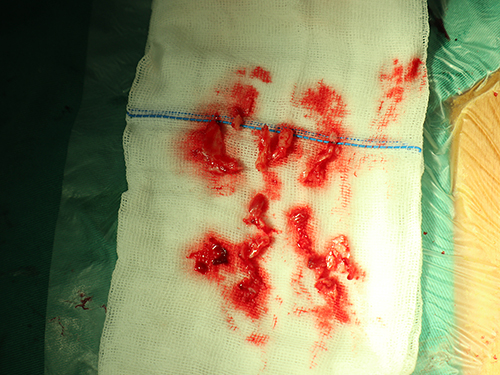 |
Figure 3 The inflammatory tissue of the spinal canal that was surgically removed in triple group. |
Postoperative Treatment
During the first 2 weeks following surgery, patients were continued to receive triple or quadruple chemotherapy, then switched to a dual chemotherapy regimen for 6 months when they were discharged from the hospital 2 weeks after surgery: rifampicin (600mg/day) plus doxycycline (200mg/day). The changes in blood routine, biochemical, and infection indexes after surgery were closely monitored, and in some diabetic patients, the blood glucose level was actively controlled to prevent infection at the surgical site. The drainage tube is removed when the drainage volume is less than 50mL in 24 hours and the drainage fluid consists of clear, light blood. It is mandatory for all patients to wear a thoracolumbar brace to move on the ground for 5–7 days after the operation, to use the brace for 2–3 months, to gradually increase their lumbar activity, and to be able to move independently after 3 months. Outpatient services were instructed to follow up with patients regularly (Figures 4–6).
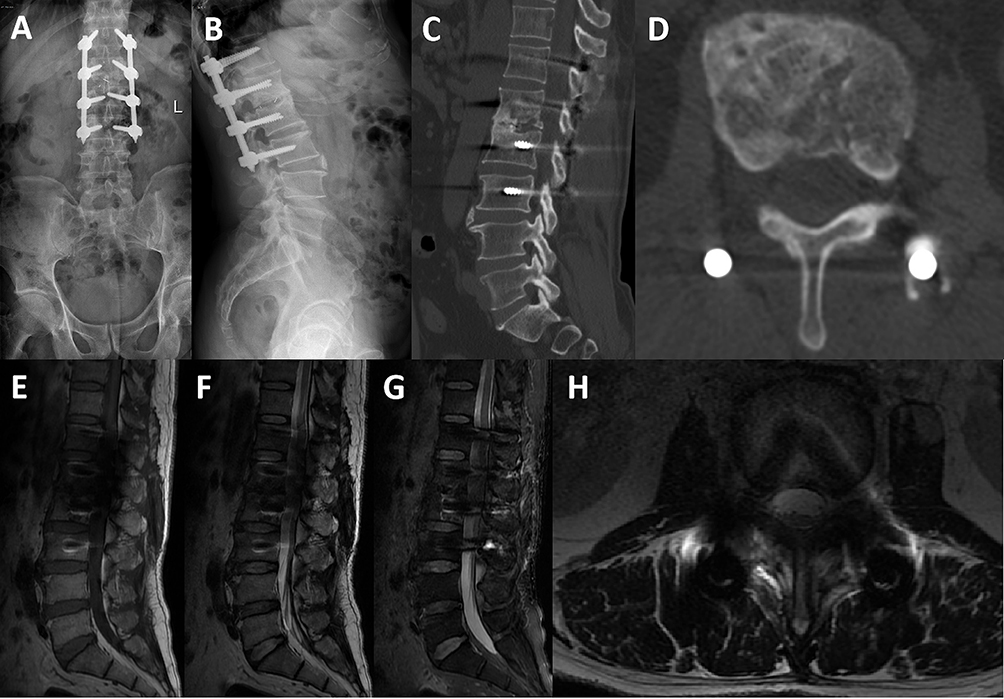 |
Figure 4 Typical cases of perioperative triple chemotherapy. X-ray 3 months postoperatively: firm internal fixation without loosening (A and B); CT 3 months postoperatively: bony fusion occurred, and the bone of the lesion was repaired obviously than before (C and D); MRI 3 months postoperatively: the diseased intervertebral disc and its adjacent soft tissue were repaired well (E–H). |
 |
Figure 5 Typical cases of perioperative quadruple chemotherapy. X-ray 3 months postoperatively: no loosening of the internal fixation (A and B); CT 3 months postoperatively: bone damage from the lesion was evidently repaired (C and D); MRI 3 months postoperatively: a good repair was achieved for the diseased intervertebral disc as well as its adjacent soft tissues (E–H). |
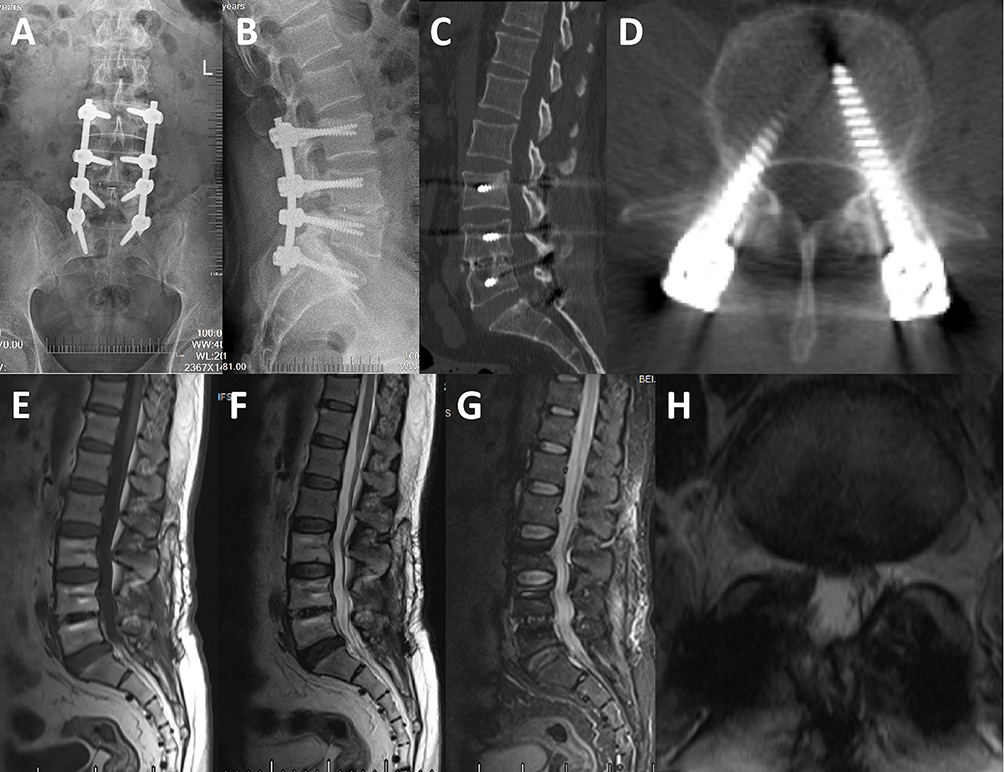 |
Figure 6 Typical cases of perioperative quadruple chemotherapy. X-ray 6 months postoperatively: no loosening of the internal fixation (A and B); CT 6 months postoperatively: formation of bony fusion between L4/5 (C and D); MRI 6 months postoperatively: no obvious abnormality (E–H). |
Observation Index
Perioperative infection control was observed in the two groups (before chemotherapy, 1 week and 2 weeks after chemotherapy, 1 week and 2 weeks postoperatively, 1 month, 3 months and 6 months postoperatively); statistics were made on the changes of low back pain, lumbar function, neurological function (before operation, 1 month, 3 months, 6 months and the last follow-up postoperatively), and the incidence of perioperative adverse drug reactions. The infection control was evaluated by using ESR and CRP, the low back pain score by VAS, the lumbar spine function score by ODI, and the neurological function evaluation by ASIA score.
Statistical Analysis
The qualitative data were analyzed using statistical package for the social science (SPSS) 22.0 statistical software, and they were presented in terms of examples and percentages (%). An analysis of the differences among the groups was conducted using the chi-square test/Fisher’s exact test. Quantitative data are expressed by mean±standard deviation (mean±SD). For intragroup comparisons before and after treatment, paired sample t-tests were used, repeated measurement analysis of variance was used for comparisons of three or more time points of the same index, and independent sample t-tests were used for intergroup comparisons. The rank data were tested by a nonparametric rank sum test. The standard of statistical significance is P<0.05.
Results
Among the triple group, twenty-four cases had a history of contact with cattle and sheep, five cases had eaten raw beef and mutton, and three cases had consumed dairy products; twenty-nine cases in the quadruple group had contact with cattle and sheep, two cases had eaten raw beef and mutton, and three cases had consumed dairy products. Both groups of patients experienced lower limb pain/numbness along with low back pain. In the triple group, there were 9 cases of American Spinal Injury Association (ASIA) grade C and 23 cases of grade D, while in the quadruple group, there were 12 cases of ASIA grade C and 22 cases of grade D. It was demonstrated that both groups had lumbar involvement, and inflammatory tissue had compressed the dural sac/nerve root in the diseased segment of the spinal canal. In the triple group, lumbar X-ray and computed tomography (CT) showed the formation of beak-like spur in front of the diseased vertebral body in 26 patients, with lumbar CT showed “lace vertebra” of lesion in 29 patients. In the quadruple group, lumbar X-ray and CT showed the formation of beak-like spur in front of the diseased vertebral body in 28 patients, with lumbar CT showed “lace vertebra” of lesion in 31 patients. In the triple group, 32 cases were positive for Rose-Bengal plate agglutination test (RBPT), and 2 cases were positive for Brucella in blood culture at admission; ESR was 59.94±11.98mm/h (36–87mm/h) and CRP 64.40±16.09mg/L (40.0–114.7mg/L). In the quadruple group, 34 cases were positive for RBPT, and five cases were positive for Brucella in blood cultures at admission; ESR was 60.03±11.78mm/h (38~89mm/h) and CRP 64.99±14.48mg/L (37.9–112.4mg/L). The comparison of the two groups of baseline data is shown in Table 1.
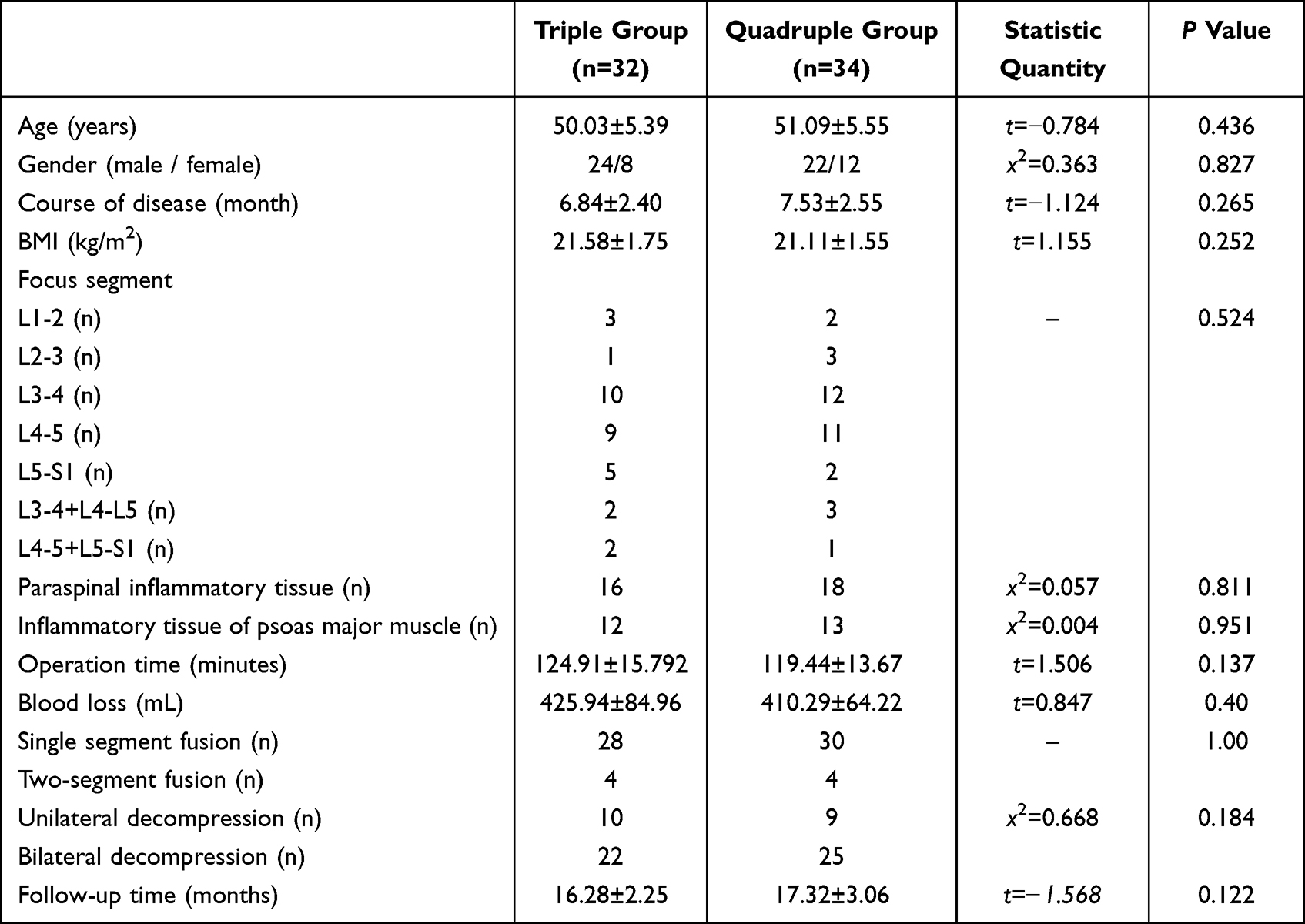 |
Table 1 Comparison of General Data Between Two Groups of Patients |
Comparison of Serum Inflammatory Indexes Between the Two Groups
There was no significant difference of ESR indexes between the two groups before chemotherapy and 6 months postoperatively (t=−0.031, 1.704, P=0.975, 0.093). The ESR indexes of 1 week and 2 weeks after chemotherapy, 1 week, 2 weeks, 1 month, 3 months postoperatively in the quadruple group were significantly lower than those in the triple group (t=2.059, 3.799, 3.682, 7.692, 6.932, 11.30, P<0.05), as shown in Figure 7(A).
There was also no significant difference of CRP indexes between the two groups before chemotherapy, 3 months and 6 months postoperatively (t=−0.158, 1.870, 1.946, P=0.875, 0.066, 0.056). The CRP indexes of 1 week and 2 weeks after chemotherapy, 1 week, 2 weeks, 1 month postoperatively in the quadruple group were significantly lower than those in the triple group (t=6.974, 9.449, 2.856, 11.131, 9.057, P<0.05) as shown in Figure 7(B).
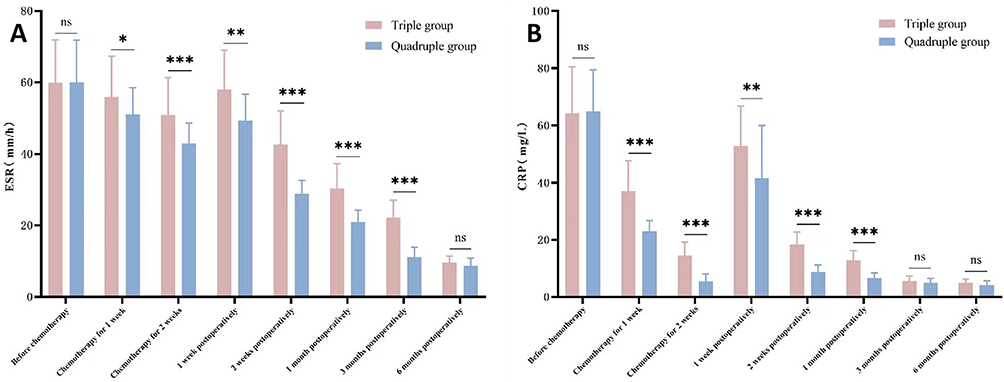 |
Figure 7 Characteristics of ESR (A), CRP (B) changes during perioperative period and after discharge in both groups. Notes: *P<0.05; **P<0.01; ***P<0.001; ns-The difference was not statistically significant. |
Comparison of Pain and Function Scores Between the Two Groups
There was no significant difference in the VAS of low back pain between the two groups before operation, 6 months and last follow-up postoperatively (t=−0.195, 1.167, 0.436, P=0.846, 0.248, 0.664). The VAS of low back pain in the quadruple group was significantly lower than that in the triple group at 1 month and 3 months postoperatively (t=3.04, 4.31, P<0.05) as shown in Figure 8(A).
There was no significant difference in the VAS of leg pain between the two groups before operation, 6 months and last follow-up postoperatively (t=0.362, 1.167, 0.671, P=0.719, 0.247, 0.505). The VAS of low back pain in the quadruple group was significantly lower than that in the triple group at 1 month and 3 months postoperatively (t=5.033, 2.03, P<0.05) as shown in Figure 8(B).
There was no significant difference in the lumbar ODI between the two groups before operation, 6 months and last follow-up postoperatively (t=−0.708, 1.875, 0.558, P=0.482, 0.065, 0.579). The lumbar ODI in the quadruple group was significantly lower than that in the triple group at 1 month and 3 months postoperatively (t=3.642, 4.839, P<0.05) as shown in Figure 8(C).
 |
Figure 8 Comparison of low back pain VAS (A), leg pain VAS (B) and lumbar ODI (C) between two groups before and after operation. Notes: *P<0.05; **P<0.01; ***P<0.001; ns-The difference was not statistically significant. |
Comparison of Neurological Function Recovery Rate Between the Two Groups
In the triple group, there were 9 patients with ASIA grade C and 23 patients with grade D before operation, 20 patients recovered to grade E 3 months postoperatively, 24 patients recovered to grade E 6 months postoperatively, and 31 patients recovered to grade E at the last follow-up as shown in Table 2.
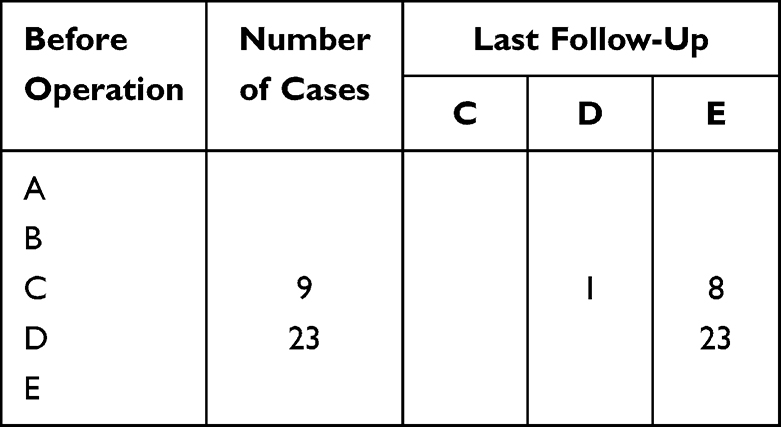 |
Table 2 ASIA Grading of Patients in Triple Group Before Operation and at Last Follow-Up |
In the quadruple group, there were 12 patients with ASIA grade C and 22 patients with grade D before operation, 29 patients recovered to grade E 3 months postoperatively, 32 patients recovered to grade E 6 months postoperatively, and all recovered to grade E at the last follow-up as shown in Table 3.
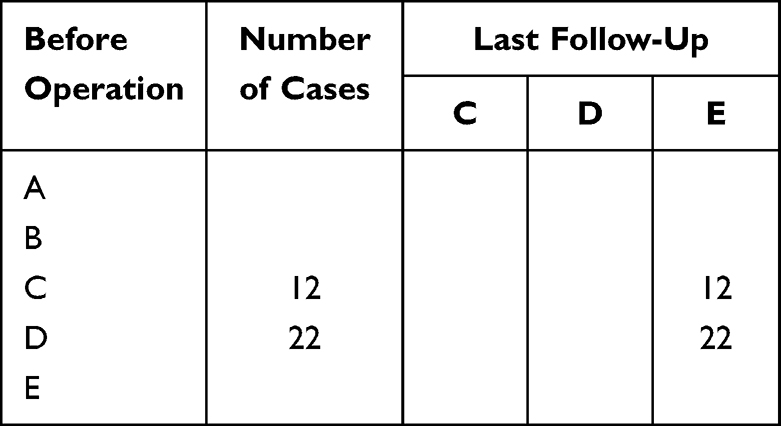 |
Table 3 ASIA Grading of Patients in Quadruple Group Before Operation and at Last Follow-Up |
There was no significant difference in the ASIA grade of the last follow-up between the two groups (Z=−1.031, P=0.303), and there was no significant difference in the recovery rate of neurological function between the two groups at the last follow-up (P=0.485). The recovery rate of neurological function in the quadruple group was significantly higher than that in the triple group at 3 months and 6 months postoperatively (x2=4.479, -, P=0.034, 0.041) as shown in Figure 9.
 |
Figure 9 Comparison of neurological function recovery rate between the two groups. Notes: *P<0.05; ns-The difference was not statistically significant. |
Comparison of the Incidence of Adverse Drug Reactions Between the Two Groups
There was no significant difference in perioperative gastrointestinal reaction, drug allergic reaction, liver function injury and renal function injury between the two groups (P>0.05), and there was no significant difference in the total incidence of adverse drug reactions between the two groups (P>0.05) as shown in Table 4.
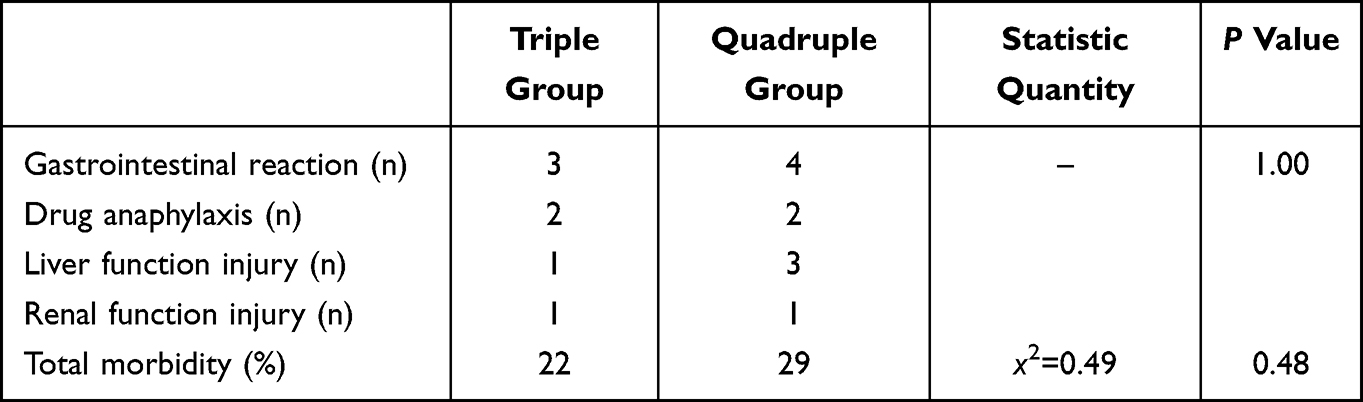 |
Table 4 Comparison of the Incidence of Adverse Drug Reactions Between the Two Groups |
Discussion
The mainstay of treatment for brucellosis spondylitis in the early stages is conservative drug treatment, when conservative treatment fails to relieve pain, patients who meet surgical criteria may undergo surgery. Currently, the principles of treating brucellosis are early, combined, adequate and adequate; rifampicin, tetracycline, sulfonamides, fluoroquinolones, macrolides, aminoglycosides, and cephalosporins are some of the antibiotics available.8 Bactericidal mechanisms vary from antibiotic to antibiotic: rifampicin inhibits the transcription of deoxyribonucleic acid (DNA) and synthesis of ribonucleic acid (RNA) in bacteria and have antibacterial activity against a wide range of pathogenic organisms; the tetracycline antibiotics affect protein synthesis and change the permeability of bacterial cell membranes by binding mainly to the bacterial ribosomal 30s subunit; sulfonamides can penetrate into cells; antibiotics like fluoroquinolones can inhibit bacteria’s DNA rotase, effectively killing them; macrolide antibiotic binds irreversibly to the 50s subunit of the ribosomal RNA of bacteria and inhibits protein synthesis by blocking transpeptide action and messenger ribonucleic acid (mRNA) shift; aminoglycoside antibiotics exert their bactericidal effect by binding to bacterial ribosomal proteins; cephalosporins are capable of destroying the cell wall of bacteria as well as killing bacteria during their breeding season.9,10 Various drugs have been shown to penetrate bone tissue well and provide good protection against bone infections, including rifampicin, doxycycline, levofloxacin, and ceftriaxone.11–13
The recommended treatment for brucellosis in patients who are not pregnant and over the age of 8 without focal disease is doxycycline plus streptomycin/gentamicin or doxycycline plus rifampicin.14 According to Chinese guidelines and World Health Organization recommendations, the most common drug regimens for treating bone and joint infection are rifampicin plus doxycycline; rifampicin plus doxycycline plus fluoroquinolones; or rifampicin plus doxycycline plus third-generation cephalosporins; as brucellosis cannot be completely eliminated by two combinations, and the recurrence rate is high, triple combinations remain the most popular treatment method.4 Quadruple drugs have been found to be effective and safe even in severe neurobrucellosis or cardiovascular complications.4,15–17
Recurrence is one of the biggest problems in treating brucellosis, inappropriate drug combinations, treatment courses, drug doses, low host immunity, wide range of lesions, incomplete surgical debridement, or unstable internal fixation may result in recurrence. The low permeability of drugs, the inactivation of intracellular environment and the degradation of lysosomal enzymes are the main reasons for the poor efficacy of anti-brucellosis drugs, and brucellosis usually recurs within six months of stopping treatment.18 The titer of serum agglutination test (SAT) should be greater than 1:160 in areas with brucellosis endemic, and patients tittering more than 1:160 should be treated with antibiotics for at least six weeks.19 As a result of delayed diagnosis, complications such as focal involvement can develop; focal brucellosis requires multiple antibiotics and a longer treatment course than uncomplicated brucellosis; relapse or irreversible loss of function may result from inappropriate treatment and treatment.20 Accordingly, brucellosis should be treated based upon the principle of individualization, and the treatment course should be prolonged (3–6 months) if paraspsoas/psoas muscle, spondylitis, or nerve involvement is evident.21
A study by Yang et al found that a triple antibiotic regimen containing doxycycline, compound sulfamethoxazole, and rifampicin was more effective for brucellosis spondylitis than a regimen of compound sulfamethoxazole and rifampicin for conservative treatment of lumbar brucellosis spondylitis without clear surgical indications.9 This is the first study to compare perioperative chemotherapy regimens for patients with lumbar brucellosis spondylitis with surgical indications. In patients with lumbar brucellosis spondylitis and impaired neurological function, a quadruple perioperative chemotherapy regimen (rifampicin, doxycycline, levofloxacin and ceftriaxone) was applied. This study examines perioperative quadruple drugs’ efficacy and safety in reducing ESR and CRP, reducing inflammation, improving low back pain, and improving neurological function, to provide a basis for clinical promotion.
For brucellosis spondylitis, open surgery still remains the main treatment option (one-stage anterior approach, posterior approach, combined anterior and posterior approach, transforaminal approach). The surgical treatment plan depends on which segments of the spinal cord are affected. Presently, the treatment for cervical brucellosis spondylitis involves anterior or anterior and posterior debridement, decompression, fusion, and internal fixation, while the treatment for thoracic and lumbar vertebrae is a one-stage posterior debridement, fusion, and internal fixation.22–24 While early spinal endoscopy is controversial in infectious spondylitis, the development of spinal endoscopy and the advancement of treatment concepts are expanding the indications of minimally invasive surgery for infectious spondylitis. The application of unilateral biportal endoscopy (UBE) technology in brucellosis spondylitis has been studied and proved to be effective.25
Infective spondylitis can be monitored effectively with spinal CT and MRI, but there is still limited correlation between disease activity and epidural abscess/bone destruction; perioperative inflammatory index changes may be useful in determining the severity of the disease.3,26 Postoperative failure may be increased by a high preoperative infection index in infectious spondylitis. According to most studies, preoperative ESR does not correlate significantly with prognosis due to the fact that in many cases, it is not consistent with clinical manifestations and is easily affected by a variety of disease states, while CRP is highly sensitive and specific.27,28 It has been proven that a rapid decrease in CRP after spinal tuberculosis correlates with an improvement in neurological function, in addition to surgical removal of casein-like materials from the spinal canal, the use of chemotherapeutic agents is also effective in reducing spinal cord and nerve root inflammation.3 In clinical settings, therefore, it is advantageous to find a combination of drugs that reduces perioperative infection index (ESR, CRP) faster and does not have any obvious adverse effects.
Brucellosis spondylitis is primarily characterized by fever and low back pain, with a much lower risk of nerve damage in the lower extremities than in spinal tuberculosis.2 A combination of dual and triple chemotherapy has been reported to be effective for patients suffering from lumbar brucellosis spondylitis without definite neurological impairment.2,6 As long as there is no progressive neurological dysfunction, preoperative standard chemotherapy is recommended for Brucellosis spondylitis with neurological impairment in order to reduce activity and prevent a number of possible postoperative complications; furthermore, surgery is required to promote neurological improvement as quickly as possible, which is inherently contradictory, which emphasizes the importance of perioperative chemotherapy in this population. As a complement to existing international and domestic guidelines for the treatment of brucellosis, our study is of high clinical value, particularly for orthopedic colleagues involved in spinal infections.
It was concluded in this study that quadruple chemotherapy regimens were superior to triple chemotherapy regimens in rapidly reducing disease activity by observing changes in infection indexes (ESR, CRP) during and after the perioperative period. Both groups showed a peak in their ESR and CRP, and their levels were significantly higher after surgery than before, possibly as a result of the surgical stimulation. In both groups, chemotherapy was administered for 2 weeks before and after the operation, and CRP index decreased significantly more than ESR index did. Upon surgical treatment two weeks after surgery, CRP indexes returned to normal in both groups, but ESR indexes decreased by only a small amount, still above 30mm/h in many patients. Postoperatively, patients continued receiving adequate chemotherapy, and no complications occurred. Similarly, CRP and ESR levels returned to normal in the quadruple group 3 months after surgery, which confirms the conclusion of previous scholars that ESR levels often do not accurately reflect disease activity.
The changes of low back pain VAS, leg pain VAS and lumbar ODI were followed up before and after operation in the two groups, demonstrating that perioperative quadruple chemotherapy regimens were superior to triple chemotherapy regimens in relieving pain and improving lumbar function. During the operation, we focused on debridement and decompression, which effectively removed the pathogenic factors of leg pain, such as intraspinal abscesses or granulomas, which resulted in a significantly greater decrease in leg pain in both groups. In addition to adjacent vertebral osteomyelitis, intraoperative paraspinal muscle exfoliation may also cause a relatively slow decrease in low back pain. However, there were no difference among two groups in 6 months post surgery and final follow-up. Thus, quadruple chemotherapy (rifampicin, doxycycline, levofloxacin, ceftriaxone) reduces perioperative infection index, improves low back/leg pain and lumbar function more rapidly compared to triple chemotherapy (rifampicin, doxycycline, levofloxacin) in the short term. For patients with lumbar brucellosis spondylitis without neurological impairment, triple chemotherapy is sufficient, but quadruple chemotherapy provides the best short-term outcome for patients with neurological impairment. We must not only reduce inflammation indicators quickly to control activity in patients with neurological impairment but also perform surgery to restore neurological function as soon as possible.
Efficacy and adverse effects of drugs should be considered in any study. Neither the triple group nor the quadruple group had significantly different gastrointestinal reactions, drug allergic reactions, liver function injuries, renal function injuries, or total adverse reactions. In previous clinical and basic studies, ceftriaxone has been shown to improve neurological function, and the rapid decrease in perioperative infection index (CRP) is clearly associated with this improvement.3,29,30 This study found that the quadruple group recovered neurological function at 3 and 6 months after operation significantly more quickly than the triad group, which may be explained by two factors: the quadruple group had significantly lower ESR and CRP levels than the triad group, and the quadruple group had a milder inflammatory reaction to the injured spinal cord/nerve root than the triad group.
The more common age range of brucellosis spondylitis is 40–60 years old in China, brucellosis spondylitis is rare in the elderly (≥ 65 years old).31 And Beijing Ditan hospital is the National Infectious Disease Medical Center of China and the designated diagnosis and treatment institution for brucellosis spondylitis, our team’s long-term study found that elderly patients with brucellosis spondylitis have low immunity due to slow metabolism and many underlying diseases (hypertension, diabetes, coronary heart disease, malnutrition). The body has a mild response to inflammatory lesions of the vertebral body and intervertebral disc, the symptoms and signs in the early stage of the disease are not obvious, and the inflammation index (ESR, CRP) may be normal. Related research is in the process of submitting. Thus, the exclusion criteria of this research included patient age ≥65 years old.
In summary, for patients with lumbar brucellosis spondylitis with impaired neurological function, perioperative quadruple chemotherapy (rifampicin, doxycycline, ceftriaxone, levofloxacin) was significantly better than triple chemotherapy (rifampicin, doxycycline, levofloxacin); quadruple groups can reduce the index of perioperative infection, reduce inflammation, improve back pain and function, and promote neurological recovery more effectively than single groups; neither the quadruple group nor the triple group showed evident adverse drug reactions, suggesting similar drug safety. It is worth noting that the advantages of the four regimens were mainly short-term post surgery.
Patient Consent and Ethics Statement
The Ethics Committee of the Beijing Ditan Hospital of Capital Medical University approved the study. Patient consent was obtained for the use of their clinical data and images and occurred out according to the Helsinki Declaration.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work received no funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Luan H, Liu K, Deng X, et al. One-stage posterior surgery combined with anti-Brucella therapy in the management of lumbosacral brucellosis spondylitis: a retrospective study. BMC Surg. 2022;22(1):394. doi:10.1186/s12893-022-01847-x
2. Zhao R, Ding R, Zhang Q. Safety and efficacy of polyetheretherketone (PEEK) cages in combination with one-stage posterior debridement and instrumentation in Lumbar Brucella Spondylitis. Clin Neurol Neurosurg. 2020;199:106259. doi:10.1016/j.clineuro.2020.106259
3. Sudprasert W, Piyapromdee U, Lewsirirat S. Neurological recovery determined by c-reactive protein, erythrocyte sedimentation rate and two different posterior decompressive surgical procedures: a retrospective clinical study of patients with spinal tuberculosis. J Med Assoc Thai. 2015;98(10):993–1000.
4. Tuon FF, Cerchiari N, Cequinel JC, et al. Brucellosis Workgroup. Guidelines for the management of human brucellosis in the State of Paraná, Brazil. Rev Soc Bras Med Trop. 2017;50(4):458–464. doi:10.1590/0037-8682-0319-2016
5. Deng Y, Liu X, Duan K, et al. Research Progress on Brucellosis. Curr Med Chem. 2019;26(30):5598–5608. doi:10.2174/0929867325666180510125009
6. Bosilkovski M, Keramat F, Arapović J. The current therapeutical strategies in human brucellosis. Infection. 2021;49(5):823–832. doi:10.1007/s15010-021-01586-w
7. Jiang H, O’Callaghan D, Ding JB. Brucellosis in China: history, progress and challenge. Infect Dis Poverty. 2020;9(1):55. doi:10.1186/s40249-020-00673-8
8. Wareth G, Dadar M, Ali H, et al. The perspective of antibiotic therapeutic challenges of brucellosis in the middle east and north African countries: current situation and therapeutic management. Transbound Emerg Dis. 2022;69(5):e1253–e1268. doi:10.1111/tbed.14502
9. Yang X-M, Jia Y-L, Zhang Y, et al. Clinical effect of doxycycline combined with compound sulfamethoxazole and rifampicin in the treatment of brucellosis spondylitis. Drug Des Devel Ther. 2021;15:4733–4740. doi:10.2147/DDDT.S341242
10. Majzoobi MM, Hashmi SH, Emami K, et al. Combination of doxycycline, streptomycin and hydroxychloroquine for short-course treatment of brucellosis: a single-blind randomized clinical trial. Infection. 2022;50(5):1267–1271. doi:10.1007/s15010-022-01806-x
11. Thabit AK, Fatani DF, Bamakhrama MS, et al. Antibiotic penetration into bone and joints: an updated review. Int J Infect Dis. 2019;81:128–136. doi:10.1016/j.ijid.2019.02.005
12. Metallidis S, Topsis D, Nikolaidis J, et al. Penetration of moxifloxacin and levofloxacin into cancellous and cortical bone in patients undergoing total Hip arthroplasty. J Chemother. 2007;19(6):682–687. doi:10.1179/joc.2007.19.6.682
13. Lovering AM, Walsh TR, Bannister GC, et al. The penetration of ceftriaxone and cefamandole into bone, fat and haematoma and relevance of serum protein binding to their penetration into bone. J Antimicrob Chemother. 2001;47(4):483–486. doi:10.1093/jac/47.4.483
14. Hashemi SH, Gachkar L, Keramat F, et al. Comparison of doxycycline-streptomycin, doxycycline-rifampin, and ofloxacin-rifampin in the treatment of brucellosis: a randomized clinical trial. Int J Infect Dis. 2012;16(4):e247–51. doi:10.1016/j.ijid.2011.12.003
15. Soares CN, da Silva MTT, Lima MA. Neurobrucellosis. Curr Opin Infect Dis. 2023;36(3):192–197. doi:10.1097/QCO.0000000000000920
16. Jin M, Fan Z, Gao R, et al. Research progress on complications of Brucellosis. Front Cell Infect Microbiol. 2023;13:1136674. doi:10.3389/fcimb.2023.1136674
17. Zhang Y, Zhang Q, Zhao CS. Cervical brucellar spondylitis causing incomplete limb paralysis. Rev Soc Bras Med Trop. 2019;52:e20180243. doi:10.1590/0037-8682-0243-2018
18. Mohammadbeigi A, Saghafipour A, Hamta A, et al. Epidemiological features of brucellosis and factors affecting its treatment failure and relapse in Qom Province, Iran. Ghana Med J. 2021;55(3):206–212. doi:10.4314/gmj.v55i3.5
19. Unuvar GK, Kilic AU, Doganay M. Current therapeutic strategy in osteoarticular brucellosis. North Clin Istanb. 2019;6(4):415–420. doi:10.14744/nci.2019.05658
20. Copur B, Sayili U. Laboratory and clinical predictors of focal involvement and bacteremia in brucellosis. Eur J Clin Microbiol Infect Dis. 2022;41(5):793–801. doi:10.1007/s10096-022-04436-1
21. Erdem H, Kilic S, Sener B, et al. Diagnosis of chronic brucellar meningitis and meningoencephalitis: the results of the Istanbul-2 study. Clin Microbiol Infect. 2013;19(2):E80–6. doi:10.1111/1469-0691.12092
22. Li HK, Du JP, Huang DG, et al. Surgical treatment of the lower cervical brucellosis with osteoporosis in the northwest region of China: review of 22 cases. Am J Transl Res. 2022;14(2):909–917.
23. Feng Z, Wang X, Yin X, et al. Analysis of the curative effect of posterior approach on lumbar brucellar spondylitis with abscess through magnetic resonance imaging under improved watershed algorithm. Contrast Media Mol Imaging. 2021;2021:1933706. doi:10.1155/2021/1933706
24. Zhang Y, Zhao C, Chen J, et al. Beneficial influence of single-stage posterior surgery for the treatment of lumbar Brucella spondylitis combined with spondylolisthesis. Sci Rep. 2022;12(1):19459. doi:10.1038/s41598-022-24223-4
25. Wang X, Long Y, Li Y, et al. Biportal endoscopic decompression, debridement, and interbody fusion, combined with percutaneous screw fixation for lumbar brucellosis spondylitis. Front Surg. 2023;9:1024510. doi:10.3389/fsurg.2022.1024510
26. Risantoso T, Hidayat M, Suyuti H, et al. The experimental study of TNF-α & CRP expression in the spinal tuberculosis after instrumentation. Ann Med Surg. 2021;72:103048. doi:10.1016/j.amsu.2021.103048
27. Chen L, Liu C, Liang T, et al. Monocyte-to-lymphocyte ratio was an independent factor of the severity of spinal tuberculosis. Oxid Med Cell Longev. 2022;2022:7340330. doi:10.1155/2022/7340330
28. Kagujje M, Mwanza W, Somwe P, et al. Sensitivity and specificity of CRP and symptom screening as tuberculosis screening tools among HIV-positive and negative outpatients at a primary healthcare facility in Lusaka, Zambia: a prospective cross-sectional study. BMJ Open. 2023;13(4):e061907. doi:10.1136/bmjopen-2022-061907
29. Weng JC, Tikhonova MA, Chen JH, et al. Ceftriaxone prevents the neurodegeneration and decreased neurogenesis seen in a Parkinson’s disease rat model: an immunohistochemical and MRI study. Behav Brain Res. 2016;305:126–139. doi:10.1016/j.bbr.2016.02.034
30. Tikhonova MA, Ho SC, Akopyan AA, et al. Neuroprotective effects of ceftriaxone treatment on cognitive and neuronal deficits in a rat model of accelerated senescence. Behav Brain Res. 2017;330:8–16. doi:10.1016/j.bbr.2017.05.002
31. Liang C, Wei W, Liang X, et al. Spinal brucellosis in Hulunbuir, China, 2011-2016. Infect Drug Resist. 2019;12:1565–1571. doi:10.2147/IDR.S202440
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.