Back to Journals » Cancer Management and Research » Volume 14
Comparative Study of Perioperative and Oncological Outcomes Between Elderly Patients and Younger Patients Who Received Radical Cystectomy and Pelvic Lymph Node Dissection: A Single-Center Retrospective Study
Authors Wang H ![]() , Huang H, Shang M, Hao H, Xi Z
, Huang H, Shang M, Hao H, Xi Z ![]()
Received 1 December 2021
Accepted for publication 27 January 2022
Published 15 February 2022 Volume 2022:14 Pages 603—613
DOI https://doi.org/10.2147/CMAR.S350587
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Seema Singh
Haixin Wang,1– 4,* Haiwen Huang,1– 3,* Meixia Shang,5 Han Hao,1– 3 Zhijun Xi1– 3
1Department of Urology, Peking University First Hospital, Beijing, People’s Republic of China; 2Institute of Urology, Peking University, National Urological Cancer Center, Beijing, People’s Republic of China; 3National Research Center for Genitourinary Oncology, Beijing, People’s Republic of China; 4Department of Urology, Yankuang New Journey General Hospital, Zoucheng, Shandong, People’s Republic of China; 5Department of Medical Statistics, Peking University First Hospital, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhijun Xi; Han Hao, Department of Urology, Peking University First Hospital, 8 Xishiku Street, Xicheng District, Beijing, 100034, People’s Republic of China, Tel +86-10-83572481, Fax +86-10-66175710, Email [email protected]; [email protected]
Purpose: To compare the perioperative and survival outcomes of patients over 75 years and younger patients who received radical cystectomy.
Patients and methods: A total of 119 patients aged ≥ 75 years and 488 patients aged < 75 years were enrolled. All patients underwent radical cystectomy with pelvic lymph node dissection. Clinical characteristics and perioperative outcomes were compared between the two groups. Overall survival and progression-free survival were analyzed by using the Kaplan–Meier method. Cox regression analysis and logistic regression analysis were used to identify the risk factors affecting the outcomes observed.
Results: There was no significant difference in perioperative complications between the elderly patient group and the younger patient group (p = 0.349). The 5-year overall survival of elderly patients was lower than that of young patients (p < 0.001). Age ≥ 75 years was a risk factor for overall survival (HR = 1.69 [95% CI: 1.22– 2.35]; p = 0.002) and progression-free survival (HR = 1.69 [95% CI: 1.14– 2.50]; p = 0.008) for patients who received radical cystectomy but was not a poor risk factor for major complications (HR = 1.25 [95% CI: 0.47– 3.31]; p = 0.658) after radical cystectomy. In addition, preoperative renal insufficiency was associated with a higher risk of major complications.
Conclusion: In our cohort, compared with younger patients, elderly patients aged ≥ 75 years had worse survival outcomes, but age ≥ 75 years was not a risk factor for major complications after radical cystectomy with pelvic lymph node dissection. Radical surgery should be encouraged for elderly patients who can tolerate aggressive treatments.
Keywords: radical cystectomy, elderly, survival outcomes, complications
Introduction
Bladder cancer is the 10th most common and 13th most deadly cancer worldwide1 and accounts for 3% of global cancer diagnoses. Age is considered to be one of the risk factors for the development of bladder cancer.2 In the United States, approximately 80% of cases of bladder cancer are diagnosed in adults aged 65 or older,1 and approximately 32% of diagnoses are made in those between 75 and 84.3 According to data published in 2019, the incidence rate of bladder cancer in China was 5.80 per 100,000 in 2015, and the incidence increased with age.4 Radical cystectomy with pelvic lymph node dissection (PLND) is the gold standard for muscle-invasive bladder cancer (MIBC) and recurrent high-grade non-muscle-invasive bladder cancer (NMIBC).5 However, its morbidity of complications was as high as 54–58% because of great surgical trauma.6–8 For elderly patients, who have more comorbidities and poorer physical conditions, the morbidity of complications increases to 54–72%.3,8–10
With the improvement of surgical techniques and perioperative management, radical cystectomy could be an acceptable option for elderly patients. Although some studies have illustrated the decrement of overall survival for elderly patients receiving radical cystectomy, its survival outcomes remain controversial because of poor comparability.11–13
This study aims to compare the perioperative and survival outcomes of patients over 75 years old and younger patients receiving radical cystectomy, and the risk factors affecting the outcomes observed were identified.
Methods
Patient Population
In the present study, retrospective analysis of data from chart review was performed. The inclusion criteria were as follows: (1) patients underwent radical cystectomy from January 2006 to April 2017 at Peking University First Hospital; and (2) postoperative pathology indicated urothelial carcinoma of the bladder. The exclusion criteria were (1) distant metastasis (n=23); (2) PLND not performed (n=164); and (3) loss to follow-up (n=227) and lack of complete survival data (n=5). Finally, we enrolled a total of 607 consecutive patients with bladder cancer who underwent radical cystectomy plus PLND. Imaging and pathological examination were performed for all patients before the operation. The indications for radical cystectomy were T2-4aN0-xM0 tumor, high-risk and recurrent NMIBC, and BCG-resistant Tis, as well as extensive papillary disease that could not be controlled with transurethral resection of bladder tumor and intravesical therapy alone. En bloc resection of the bladder, removal of internal iliac lymph nodes, external iliac lymph nodes, obturator lymph nodes, and presacral lymph nodes were carried out for all patients, and extracorporeal urinary diversion was performed after radical cystectomy, which included ureterocutaneostomy, ileal conduit or orthotopic neobladder. This study was approved by the clinical research ethics committee of Peking University First Hospital, Beijing, China.
Outcomes Measures
Clinical and Pathological Data
Clinical and pathological data were obtained from chart review. Patients were categorized into two groups: young patients aged < 75 years and elderly patients aged ≥ 75 years. Clinical characteristics, including the American Society of Anesthesiologists (ASA) score, time of operation, estimated blood loss (EBL), postoperative stay, and complication rate, were compared between the two groups. Renal function was analyzed on the basis of the last recorded preoperative serum creatinine (sCr) value, and sCr ≥ 1.5 mg/dL was classified as renal insufficiency. Complications within 30 days after radical cystectomy were extracted from the review of electronic patient records, and each complication was graded according to the Clavien–Dindo classification system.14,15 The highest Clavien–Dindo class was summarized for each patient. Major complication was characterized as complications of Clavien–Dindo class III–V. In addition, the perioperative comorbidity assessment for elderly patients was performed using the Charlson Comorbidity Index.16 Histological type, surgical margin status, lymph node yield, and the number of positive lymph nodes were collected in pathological data. The TNM staging system of bladder cancer of the American Joint Committee on Cancer Staging Manual 8th edition was used in this study.
Oncologic Outcomes
Postoperative surveillance for all patients was performed through outpatient visits. All patients received examinations, including physical examination, laboratory measurements of blood and urine, and computer tomography scans every six months until the third year and annually thereafter. Overall survival (OS) was characterized as the period from the operation to death from any cause, cancer-specific survival (CSS) referred to the period from the operation to cancer-related death, and progression-free survival (PFS) was defined as the period from the operation to the time of recurrence of cancer.
Statistical Analysis
For the continuous variables, the Kolmogorov-Smirnov test was used first to identify normality. The independent t test was used to compare the variables following a normal distribution, and variables following a nonnormal distribution were analyzed by the Mann–Whitney U-test. The x2-test or Fisher’s exact test was used to compare the disordered categorical variables, while the ordered categorical variables were analyzed by using the Mann–Whitney U-test. The OS and PFS of all patients were determined by using Kaplan–Meier curves. Cox regression analysis of all patients was used to identify the risk factors affecting the prognosis outcomes, adjusting for age (<75, ≥75), ASA score, pathologic stage (Ta/Tis/T1, T2, T3, T4), pathologic nodal stage (N0, N+), major complications (no, yes), chemotherapy (no, yes), and surgery margin (no, yes). The proportional hazards (PH) assumption was examined using log-minus-log plots of the hazard functions. There were no significant violations of the proportional hazards assumption. Logistic regression analysis of all patients was used to identify the risk factors associated with the major complications. Variables that showed a univariate relationship with major complications or that were considered clinically relevant were entered into the logistic regression model. In addition, to identify the factors affecting the OS of elderly patients, Cox regression analysis of elderly patients was also performed, adjusting for sex (female, male), Charlson comorbidity index (≤2, ≥3), type of urinary diversion (ileal conduit, ureterocutaneostomy), pathologic stage (Ta/Tis/T1, T2, T3, T4), pathologic nodal stage (N0, N+), major complications (no, yes), and chemotherapy (no, yes). All analyses in this study were performed using IBM SPSS version 25 (IBM Corporation, Armonk, NY, USA), and all p values were two-sided. p < 0.05 was considered to be statistically significant.
Results
Patient Characteristics
There were 607 patients with bladder cancer enrolled in the present study. Among them, 119 patients were aged ≥ 75 years, whose median age was 77 (interquartile range 76–80) years, and 488 patients were aged < 75 years, with a median of 62 (interquartile range 56–68) years. The median follow-up time was 52 months (interquartile range 29–78).
The perioperative and pathological outcomes are presented in Table 1. Compared with younger patients, elderly patients had higher ASA scores (p < 0.001) and higher clinical T stages (p = 0.002). However, there was no significant difference in pathological T stage or pathological nodal stage between the two groups. In addition, more elderly patients received ureterocutaneostomy (52.9% vs 14.5%, p < 0.001), and fewer elderly patients were treated with neoadjuvant or adjuvant chemotherapy (7.6% vs 23.2%, p < 0.001). The time of operation was shorter in the group of elderly patients (259 vs 313 mins, p < 0.001), but no significant difference was found in the postoperative complications and postoperative stay.
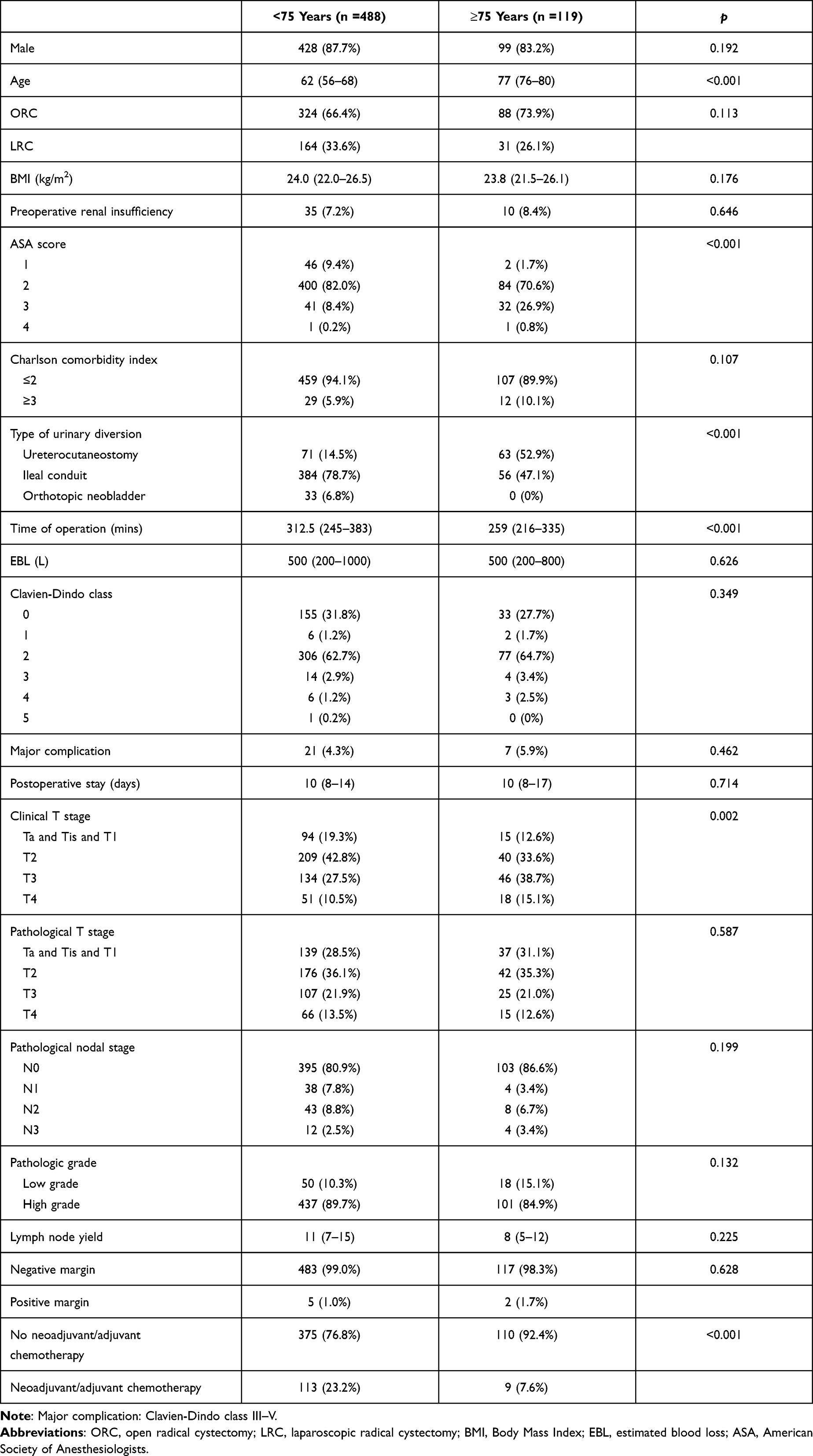 |
Table 1 The Clinicopathologic Characteristics of All Patients |
Oncologic Outcomes
To identify oncologic outcomes of radical cystectomy between the two groups, Kaplan–Meier curves (see Figure 1) were used to analyze OS and PFS. The 5-year OS of elderly patients was lower than that of young patients (p < 0.001), which was 0.456 versus 0.628. Furthermore, the 5-year PFS was 0.620 versus 0.670, and the 5-year CSS was 0.638 versus 0.725 in the elderly patient group and young patient group, respectively, but there was no significant difference between the two groups. In addition, Cox regression analysis was performed to further verify the factors affecting the OS and PFS of all patients. As shown in Table 2, age ≥ 75 years (HR = 1.69 [95% CI: 1.22–2.35]; p = 0.002), higher pathological T stage (p < 0.001), higher pathological nodal stage (HR = 1.97 [95% CI: 1.41–2.75]; p < 0.001), and major complications (HR = 2.71 [95% CI: 1.56–4. 70]; p < 0.001) were risk factors for OS in patients who underwent radical cystectomy. Age ≥ 75 years (HR = 1.69 [95% CI: 1.14–2.50]; p = 0.008), higher pathological T stage (p < 0.001), and higher pathological nodal stage (HR = 1.67 [95% CI: 1.17–2.39]; p = 0.005) were poor prognostic factors for PFS.
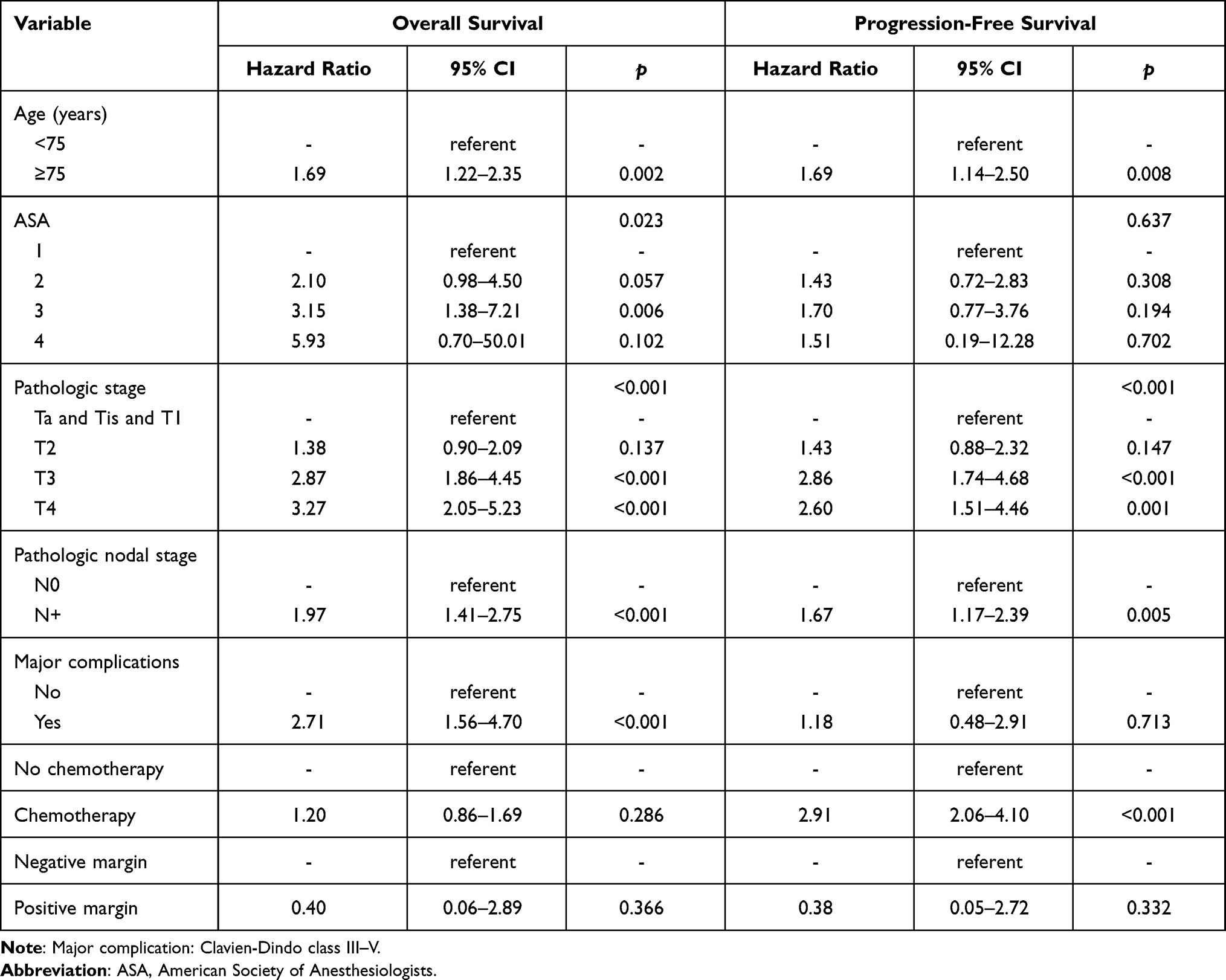 |
Table 2 Multivariable Cox Regression Analysis of Variables Associated with Overall Survival and Progression-Free Survival for All Patients Received Radical Cystectomy |
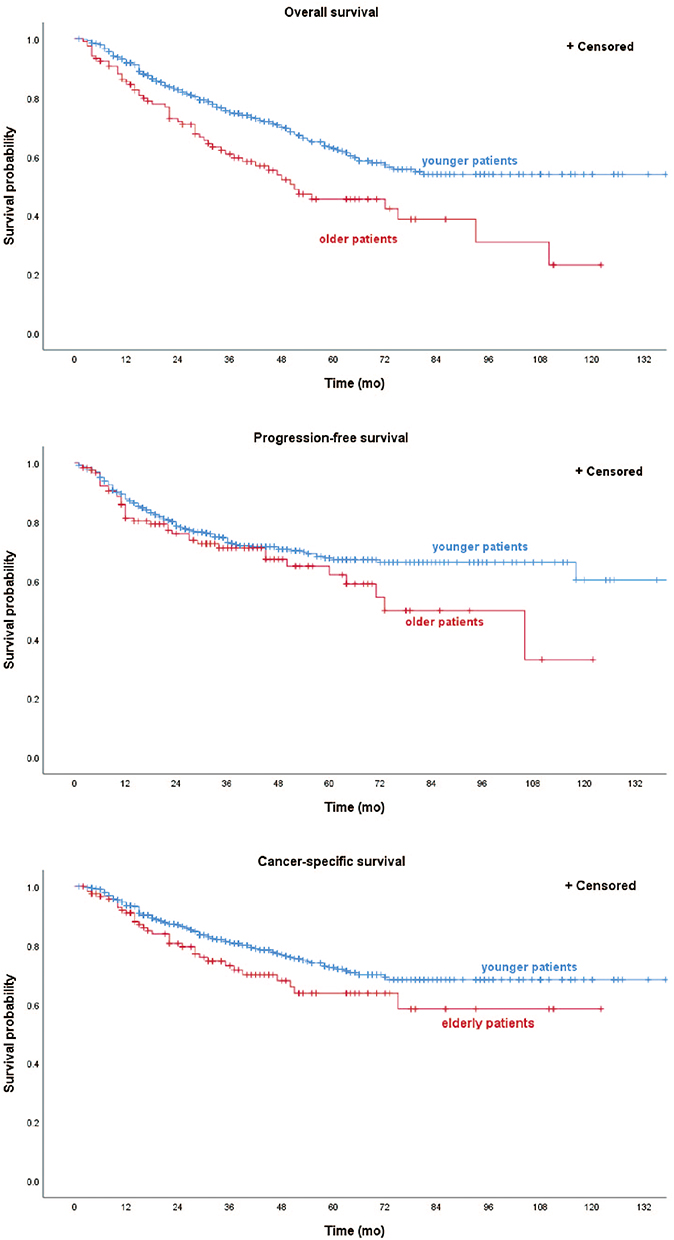 |
Figure 1 Kaplan–Meier curves of OS probability (p < 0.001), PFS (p =0.131), and CSS probability (p = 0.065) in elderly patients and younger patients who received radical cystectomy and pelvic lymph node dissection. The 5-year OS of elderly patients and young patients was 0.456 versus 0.628, respectively. The 5-year PFS was 0.620 versus 0.670, and the 5-year CSS was 0.638 versus 0.725 in the elderly patient group and the young patient group, respectively. Abbreviations: OS, overall survival; PFS, progression-free survival; CSS, cancer-specific survival. |
Moreover, Cox regression analysis was used to identify the factors affecting the OS of elderly patients. We found that male sex (HR = 4.01 [95% CI: 1.39–11.51]; p = 0.010), Charlson comorbidity index ≥ 3 (HR = 2.29 [95% CI: 1.06–4.98]; p = 0.036), ureterocutaneostomy (HR = 1.84 [95% CI: 1.02–3.34]; p = 0.043), T4 (HR = 2.63 [95% CI: 1.04–6.65]; p = 0.042), and major complications (HR = 5.05 [95% CI: 1.87–13.64]; p = 0.001) were associated with poor OS outcomes for elderly patients (see in Table 3).
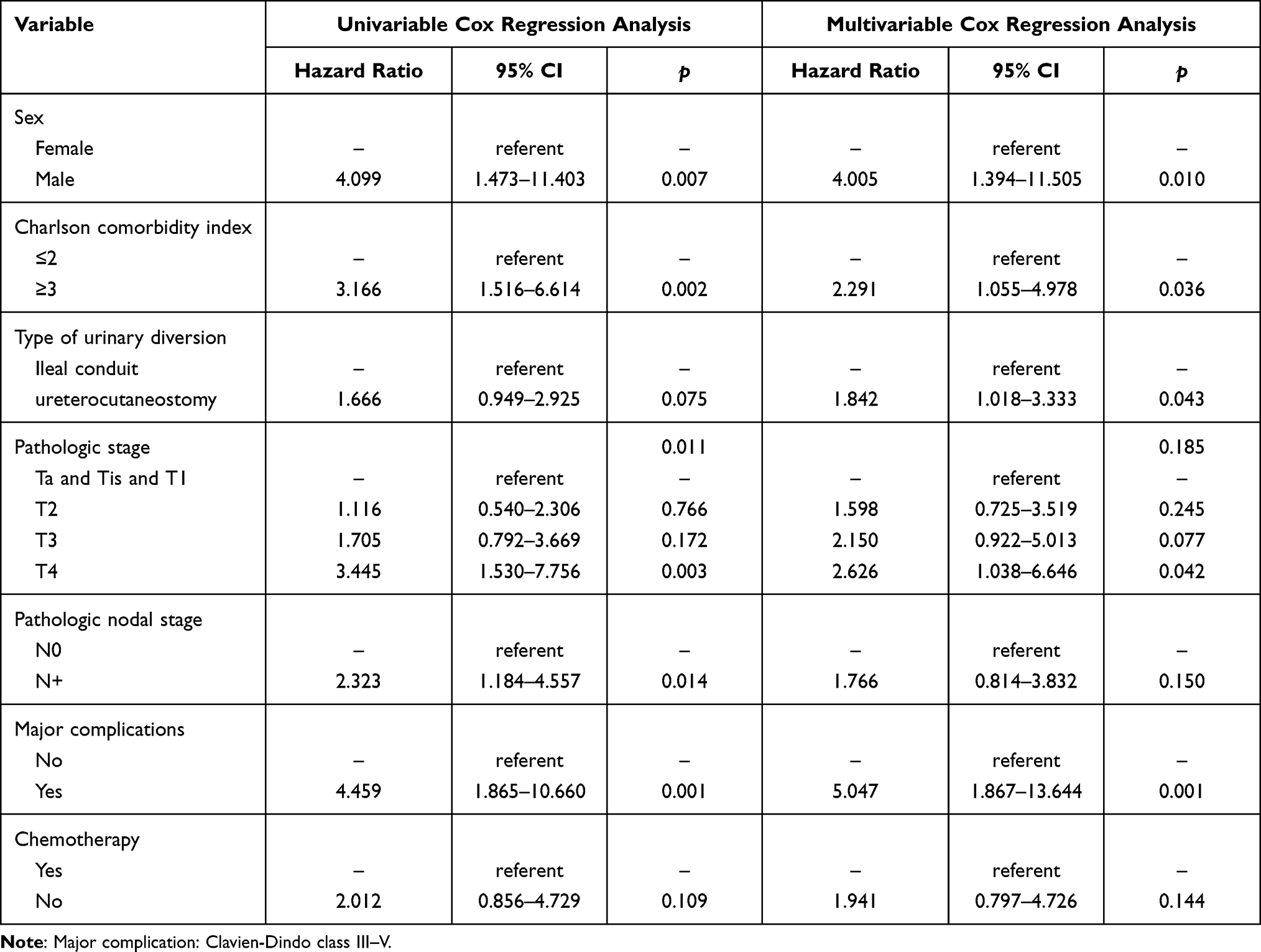 |
Table 3 Univariable/Multivariable Cox Regression Analysis of Variables Associated with Overall Survival for Elderly Patients |
Perioperative Complications
There was no significant difference in terms of perioperative complications (p = 0.349), major complications (p = 0.462), or estimated blood loss (p = 0.626) between the group of elderly patients and the group of younger patients. Then, the risk factors for major complications were identified in this study. As shown in Table 4, age ≥ 75 years was not a risk factor for major complications (OR = 1.25 [95% CI: 0.47–3.31]; p = 0.658), while preoperative renal insufficiency was associated with a higher risk of major complications (OR = 4.33 [95% CI: 1.64–11.38]; p = 0.003).
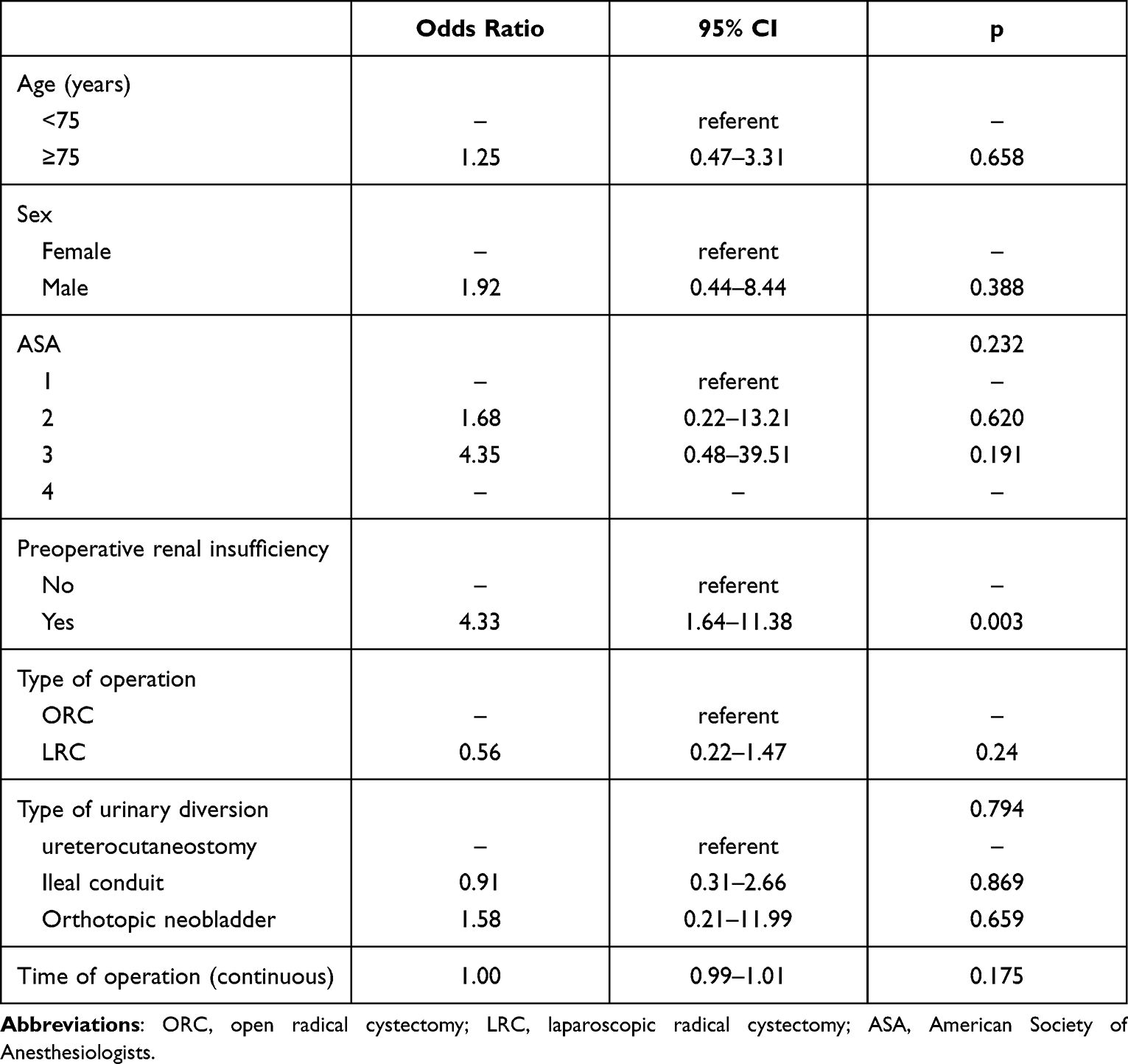 |
Table 4 Logistic Regression Analysis of Variables Associated with Major Complication for All Patients |
Discussion
In this study, we focused on the perioperative and survival outcomes of patients over 75 years old and younger patients receiving radical cystectomy. The OS of elderly patients was lower than that of younger patients, while there was no significant difference in PFS between the two groups. Furthermore, age ≥ 75 years was one of the poor prognostic factors of OS and PFS for patients who received radical cystectomy. In addition, we found that there was no significant difference in perioperative complications between the elderly patient group and the younger patient group. Age ≥ 75 years was not a risk factor for major complications, while preoperative renal insufficiency was associated with a higher risk of major complications.
Radical cystectomy with PLND remains the standard treatment for nonmetastatic muscle-invasive bladder cancer.5 However, as a challenging operation, its morbidity of complications is high, with a risk of 40–65%.17 High therapy-induced risk of severe complications and shorter estimated life expectancy caused many elderly patients to refuse more aggressive treatment.18 Past studies have suggested that only some elderly patients receive radical surgeries, and cystectomy rates decrease with advanced age.19 However, aggressive surgical management of bladder cancer in elderly patients would significantly improve oncological outcomes;20 in patients with T3 MIBC left untreated, the OS was less than 1 year.21 In addition, with the improvement of surgical instruments and perioperative care and with the spread of minimally invasive surgery, the surgical safety of elderly patients has been greatly improved. We also compared the perioperative and oncological outcomes of patients in the first 5 years and last 5 years (Supplementary Figure 1 and Table 1). For the 2012–2017 group, the time of operation, EBL, and complication rate decreased, and the postoperative stay increased, with the improvement of overall survival. A recent study from China also illustrated that elderly patients who received robot-assisted radical cystectomy showed no increased perioperative risks compared with younger patients.22
In some previous studies performed in the United States, France, Canada, and Australia, worse overall survival was found in elderly patients receiving radical cystectomy, but most studies defined elderly patients as patients aged >65 or 70 years.23–25 Considering that the median age at diagnosis of MIBC was above 70 years and an aging population, an age cutoff of 75 years for defined elderly patients was applied in our study. We found that overall survival was worse in patients older than 75 years old, and age ≥ 75 years was associated with poor oncological outcomes. More comorbidities and poor health status could account for the worse overall survival of elderly patients. In our study, a high Charlson Comorbidity Index score was identified as a risk factor for the overall survival of elderly patients. However, not only overall survival but also progression-free survival was worse for elderly patients, although there was no significant difference in PFS, which means that there might be some other reasons responsible for the worse outcomes. Neoadjuvant chemotherapy and adjuvant chemotherapy have been proven to be significantly beneficial to survival.26,27 However, the use of neoadjuvant chemotherapy and adjuvant chemotherapy decreased for elderly patients because of impaired renal function and poor performance status.28,29
Moreover, perioperative complication was found to be a risk factor for overall survival in this study, although there was no difference in terms of any perioperative complications or major complications between elderly patients and younger patients, which was the same as some previous studies.30,31 The improvement of surgical instruments and advances in perioperative care may cover up the difference in complications caused by increasing age. Patel et al showed an improving trend of perioperative mortality at high volume centers.25 It is necessary to refer elderly patients who need aggressive surgery to high-volume hospitals.
In our study, preoperative renal insufficiency was found to be a risk factor for major perioperative complications in elderly patients, which means that the physical status of elderly patients affects the perioperative outcomes after radical cystectomy. Hence, the potential benefits and harms from radical cystectomy should be weighed before surgery. It is important to recognize elderly patients suitable for curative treatment. With increasing age, physical function and functional reserve decreased, resulting in the decrement of tolerance for aggressive treatment. Frailty is the phenotype of declining physiologic function and loss of functional reserve across organ systems, leading to vulnerability against disease and death.32,33 Frailty rates were proven to be associated with higher complications after radical cystectomy.34 The incidence of frailty increased with advanced age. It is necessary to screen frailty for elderly patients before surgery in routine clinical practice. The use of some form of geriatric assessments was beneficial to select the appropriate candidates for aggressive treatments for urologists.35 Geriatric assessments for elderly patients are a multidomain assessment of functional, medical, and psychosocial aspects of health. However, there was no recommendation of optimal assessment tools for clinical practice. In our center, a multidisciplinary assessment was performed for all elderly patients before radical cystectomy. Further studies of the best tools of geriatric assessments should be encouraged.
For elderly patients with nonmetastatic bladder cancer, radical cystectomy improves the survival outcomes, although it is inferior to younger patients, and the morbidity of perioperative complications is similar to that of younger patients. Hence, radical surgeries should be encouraged for elderly patients who could tolerate aggressive treatments. However, more studies are needed to explore better approaches to select the appropriate candidates.
There were certain limitations in our study. First, there were some inherent selection biases because of the retrospective design. Second, the elderly patients enrolled were highly selective, and patients who received radical cystectomy but not lymphonodectomy were excluded from this study, which was too idealistic. In clinical practice, to decrease operative time and reduce the risk of perioperative complications, pelvic lymph node dissection is often omitted.36 Furthermore, there were no data on 30-, 60-, and 90-day mortality because of the retrospective nature of the study, which was associated with inpatient treatment.
Conclusion
In our cohort, compared with younger patients, elderly patients aged ≥ 75 years had worse survival outcomes, but age ≥ 75 years was not a risk factor for major complications after radical cystectomy with pelvic lymph node dissection. Radical surgery should be encouraged for elderly patients who could tolerate aggressive treatments.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval
The present study was approved by the clinical research ethics committee of Peking University First Hospital (Protocol number: 2015[977]). The informed consent requirement was exempted by the ethics committee because of the retrospective design. The data used in this study were anonymized and maintained with confidentiality, and the study complied with the Declaration of Helsinki.
Acknowledgments
This study was supported by the National Natural Science Foundation of China (grant number: 81272829).
Funding
This study was supported by the National Natural Science Foundation of China (grant number: 81272829).
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Saginala K, Barsouk A, Aluru JS, Rawla P, Padala SA, Barsouk A. Epidemiology of bladder cancer. Med Sci. 2020;8(1). doi:10.3390/medsci8010015
2. Burger M, Catto JW, Dalbagni G, et al. Epidemiology and risk factors of urothelial bladder cancer. Eur Urol. 2013;63(2):234–241. doi:10.1016/j.eururo.2012.07.033
3. Taylor JA
4. Chen W, Zheng R, Baade PD, et al. Cancer Statistics in China, 2015. CA: a Cancer Journal for Clinicians. 2016;66(2):115–132. doi:10.3322/caac.21338
5. Witjes JA, Bruins HM, Cathomas R, et al. EAU guidelines on muscle invasive and metastatic bladder cancer. EAU Guidelines; 2021.
6. Novara G, De Marco V, Aragona M, et al. Complications and mortality after radical cystectomy for bladder transitional cell cancer. J Urol. 2009;182(3):914–921. doi:10.1016/j.juro.2009.05.032
7. Hautmann RE, de Petriconi RC, Volkmer BG. Lessons learned from 1000 neobladders: the 90-day complication rate. J Urol. 2010;184(3):
8. Wuethrich PY, Vidal A, Burkhard FC. There is a place for radical cystectomy and urinary diversion, including orthotopic bladder substitution, in patients aged 75 and older: results of a retrospective observational analysis from a high-volume center. Urol Oncol. 2016;34(2):58e19–27. doi:10.1016/j.urolonc.2015.08.011
9. Farnham SB, Cookson MS, Alberts G, Smith JA
10. Donat SM, Siegrist T, Cronin A, Savage C, Milowsky MI, Herr HW. Radical cystectomy in octogenarians–does morbidity outweigh the potential survival benefits?. J Urol. 2010;183(6):2171–2177. doi:10.1016/j.juro.2010.02.015
11. Konety BR, Joslyn SA. Factors influencing aggressive therapy for bladder cancer: an analysis of data from the SEER program. J Urol. 2003;170(5):1765–1771. doi:10.1097/01.ju.0000091620.86778.2e
12. Prout GR, Wesley MN, Yancik R, Ries LAG, Havlik RJ, Edwards BK. Age and comorbidity impact surgical therapy in older bladder carcinoma patients. Cancer. 2005;104(8):1638–1647. doi:10.1002/cncr.21354
13. Koppie TM, Serio AM, Vickers AJ, et al. Age-adjusted Charlson comorbidity score is associated with treatment decisions and clinical outcomes for patients undergoing radical cystectomy for bladder cancer. Cancer. 2008;112(11):2384–2392. doi:10.1002/cncr.23462
14. Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240(2):205–213. doi:10.1097/01.sla.0000133083.54934.ae
15. Clavien PA, Barkun J, de Oliveira ML, et al. The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg. 2009;250(2):187–196. doi:10.1097/SLA.0b013e3181b13ca2
16. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
17. Challacombe BJ, Bochner BH, Dasgupta P, et al. The role of laparoscopic and robotic cystectomy in the management of muscle-invasive bladder cancer with special emphasis on cancer control and complications. Eur Urol. 2011;60(4):767–775. doi:10.1016/j.eururo.2011.05.012
18. Fonteyne V, Ost P, Bellmunt J, et al. Curative treatment for muscle invasive bladder cancer in elderly patients: a systematic review. Eur Urol. 2018;73(1):40–50. doi:10.1016/j.eururo.2017.03.019
19. Fedeli U, Fedewa SA, Ward EM. Treatment of muscle invasive bladder cancer: evidence from the National Cancer Database, 2003 to 2007. J Urol. 2011;185(1):72–78. doi:10.1016/j.juro.2010.09.015
20. Hollenbeck BK, Miller DC, Taub D, et al. Aggressive treatment for bladder cancer is associated with improved overall survival among patients 80 years old or older. Urology. 2004;64(2):292–297. doi:10.1016/j.Urology.2004.03.034
21. Marshall VF, Whitmore WF
22. Xie S, Zhao Z, Feng B, et al. A comparative study of perioperative and survival outcomes of robot-assisted radical cystectomy in patients over 80 and under 80 years old. World J Surg Oncol. 2021;19(1):202. doi:10.1186/s12957-021-02312-4
23. Guillotreau J, Miocinovic R, Gamé X, et al. Outcomes of laparoscopic and robotic radical cystectomy in the elderly patients. Urology. 2012;79(3):585–590. doi:10.1016/j.Urology.2011.11.042
24. Fairey AS, Kassouf W, Aprikian AG, et al. Age ≥ 80 years is independently associated with survival outcomes after radical cystectomy: results from the Canadian Bladder Cancer Network Database. Urol Oncol. 2012;30(6):825–832. doi:10.1016/j.urolonc.2011.07.014
25. Patel MI, Bang A, Gillatt D, Smith DP. Contemporary radical cystectomy outcomes in patients with invasive bladder cancer: a population-based study. BJU Int. 2015;116(Suppl 3):18–25. doi:10.1111/bju.13152
26. Yin M, Joshi M, Meijer RP, et al. Neoadjuvant chemotherapy for muscle-invasive bladder cancer: a systematic review and two-step meta-analysis. oncologist. 2016;21(6):708–715. doi:10.1634/theoncologist.2015-0440
27. Leow JJ, Martin-Doyle W, Rajagopal PS, et al. Adjuvant chemotherapy for invasive bladder cancer: a 2013 updated systematic review and meta-analysis of randomized trials. Eur Urol. 2014;66(1):42–54. doi:10.1016/j.eururo.2013.08.033
28. Leveridge MJ, Siemens DR, Mackillop WJ, et al. Radical cystectomy and adjuvant chemotherapy for bladder cancer in the elderly: a population-based study. Urology. 2015;85(4):791–798. doi:10.1016/j.urology.2014.12.027
29. Reardon ZD, Patel SG, Zaid HB, et al. Trends in the use of perioperative chemotherapy for localized and locally advanced muscle-invasive bladder cancer: a sign of changing tides. Eur Urol. 2015;67(1):165–170. doi:10.1016/j.eururo.2014.01.009
30. Fairey A, Chetner M, Metcalfe J, et al. Associations among age, comorbidity and clinical outcomes after radical cystectomy: results from the Alberta Urology Institute radical cystectomy database. J Urol. 2008;180(1):
31. Schmid M, Rink M, Traumann M, et al. Evidence from the “PROspective MulticEnTer RadIcal Cystectomy Series 2011 (PROMETRICS 2011)” study: how are preoperative patient characteristics associated with urinary diversion type after radical cystectomy for bladder cancer?. Ann Surg Oncol. 2015;22(3):1032–1042. doi:10.1245/s10434-014-4029-3
32. Clegg A, Young J, Iliffe S, Rikkert MO, Rockwood K. Frailty in elderly people. Lancet. 2013;381(9868):752–762. doi:10.1016/S0140-6736(12)62167-9
33. Grimberg DC, Shah A, Molinger J, et al. Assessments of frailty in bladder cancer. Urol Oncol. 2020;38(9):698–705. doi:10.1016/j.urolonc.2020.04.036
34. Chappidi MR, Kates M, Patel HD, et al. Frailty as a marker of adverse outcomes in patients with bladder cancer undergoing radical cystectomy. Urol Oncol. 2016;34(6):
35. Gadzinski AJ, Psutka SP. Risk stratification metrics for bladder cancer: comprehensive geriatric assessments. Urol Oncol. 2020;38(9):725–733. doi:10.1016/j.urolonc.2020.01.003
36. Abdollah F, Sun M, Shariat SF, et al. The importance of pelvic lymph node dissection in the elderly population: implications for interpreting the 2010 National Comprehensive Cancer Network practice guidelines for bladder cancer treatment. J Urol. 2011;185(6):2078–2084. doi:10.1016/j.juro.2011.02.022
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.