Back to Journals » Journal of Inflammation Research » Volume 19
Comparative Predictive Value of Nine Composite Inflammatory Markers for Atrial Fibrillation Recurrence After Catheter Ablation
Authors Ji T, Yuan Y, Du M ![]() , Liu S, Wei J, Luan C, Xue J
, Liu S, Wei J, Luan C, Xue J
Received 1 December 2025
Accepted for publication 24 February 2026
Published 7 March 2026 Volume 2026:19 572912
DOI https://doi.org/10.2147/JIR.S572912
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Qing Lin
Tengfei Ji,* Yide Yuan,* Mei Du, Su Liu, Jia Wei, Chunhong Luan, Jiahong Xue
The Second Affiliated Hospital of Xi'an Jiaotong University, Department of Cardiology, Xi'an 710004, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chunhong Luan, Email [email protected] Jiahong Xue, Email [email protected]
Purpose: Recurrence of atrial fibrillation (AF) following catheter ablation (CA) is a common clinical challenge in AF management. Chronic inflammation plays a crucial role in the mechanism of AF recurrence. Although preliminary studies have explored the predictive value of composite inflammatory markers for AF recurrence, there remains a notable lack of research that directly compares multiple composite markers simultaneously. This study aims to investigate and compare the associations between nine composite inflammatory markers and the risk of AF recurrence after CA in patients with AF.
Patients and Methods: This study prospectively included 744 AF patients who underwent their first CA at the Second Affiliated Hospital of Xi’an Jiaotong University between October 2017 and July 2024.We calculated nine composite inflammatory markers from pre-procedure peripheral blood cell counts. After adjusting for confounders, Cox regression, restricted cubic splines (RCS), and receiver operating characteristic (ROC) curves assessed their association with AF recurrence. Sensitivity analysis verified result robustness.
Results: Higher levels of the Systemic Immune-Inflammation Index (SII), Neutrophil-to-Lymphocyte Ratio (NLR), Systemic Immune-Inflammation Response Index (SIRI), and Pan-Immune-Inflammation Value (PIV) were significantly associated with increased recurrence risk. After full model adjustment, Q4 vs Q1 HRs [95% CIs] were: SII 1.88 (1.23– 2.88), NLR 1.85 (1.21– 2.84), SIRI 2.03 (1.31– 3.14), PIV 1.58 (1.06– 2.38), with risk rising as indices increased. The Neutrophil-to-Platelet Ratio (NPR) Q3 risk was higher than Q1 (HR=1.58; 95% CI:1.07– 2.32). In terms of prognostic predictive efficacy, NLR demonstrated the best performance among the inflammatory indicators (AUC: 0.62). Sensitivity analysis confirmed each index’s robustness.
Conclusion: The SII, NLR, SIRI, NPR, and PIV may serve as valuable biomarkers for AF recurrence, among which NLR exhibits superior predictive capability compared to the other indices. These markers should be considered in clinical risk stratification and hold promise for providing new strategies and directions to reduce the recurrence rate.
Keywords: atrial fibrillation, radiofrequency catheter ablation, inflammation, composite inflammatory markers, risk
Introduction
Atrial fibrillation (AF) constitutes the most common type of clinical arrhythmia. Data derived from the Framingham Heart Study indicate that its incidence has tripled over a span of fifty years.1 Survey data reveal that by the year 2010, the global prevalence of patients diagnosed with AF had reached an estimated 33.5 million individuals. In the United States, the annual healthcare expenditures attributable to AF were projected to fall between $16 billion and $26 billion.2 AF not only induces distressing symptoms, including chest tightness and palpitations, but also substantially elevates the risk of cardiovascular and cerebrovascular complications, such as stroke and heart failure (HF), thereby profoundly affecting patients’ physical and psychological well-being. It has emerged as a critical public health issue demanding urgent attention worldwide.3–5
Catheter ablation (CA) has been recognized as a key therapeutic approach for AF in recent international guidelines and clinical research, aiming primarily to maintain sinus rhythm in order to improve patients’ quality of life and long-term clinical outcomes.6–8 Nevertheless, a substantial recurrence rate of atrial arrhythmias remains following the procedure, which is intricately linked to its complex underlying pathophysiological mechanisms. Specifically, radiofrequency ablation results in cardiac tissue necrosis that is accompanied by an inflammatory response. Prior research has demonstrated that inflammatory biomarkers, such as C-reactive protein and interleukin-6, reach their highest levels within 1 to 2 days post-ablation, and this increase is associated with the recurrence of atrial arrhythmias.9–11 Inflammation plays a key role in the initiation and persistence of AF and may be significantly involved in atrial remodeling and electrophysiological abnormalities. Elevated neutrophil levels indicate an active inflammatory pathway, increased lymphocytes reflect an active immune pathway, changes in platelets are associated with thrombosis, elevated monocytes often suggest chronic inflammation or tissue repair processes, and albumin levels are related to liver function, nutritional intake, or chronic consumption.12 These factors may form a substrate for arrhythmias and promote AF recurrence.13,14 The nine composite inflammatory markers screened in this study—the Systemic Immune-Inflammation Index (SII), Neutrophil-to-Lymphocyte Ratio (NLR), Platelet-to-Lymphocyte Ratio (PLR), Lymphocyte-to-Monocyte Ratio (LMR), Neutrophil-to-Platelet Ratio (NPR), Systemic Immune-Inflammation Response Index (SIRI), Platelet-to-Albumin Ratio (PAR), Pan-Immune-Inflammation Value (PIV), and the Hemoglobin, Albumin, Lymphocyte, and Platelet Score (HALP)—are all calculated based on routine peripheral blood tests. These markers are clinically convenient to obtain and demonstrate high stability. Composed of different combinations of the aforementioned individual cellular components, these various composite inflammatory markers can reflect pathophysiological states such as inflammatory activation, immune imbalance, coagulation abnormalities, and nutritional and metabolic disorders from different dimensions.15 They capture the complex systemic inflammatory and immunomodulatory changes during the occurrence and progression of AF. For example, SII reflects the overall systemic inflammatory state, while NLR indicates the balance between inflammation and immunity in the body. This overcomes the limitation of single inflammatory markers, which can only reflect local pathological changes. SII shows an independent and strong positive correlation with AF recurrence after CA in both hypertensive and diabetic patients.16,17 NLR also demonstrates a high correlation with AF recurrence.18 Furthermore, these nine markers have been confirmed to have significant prognostic value in various cardiovascular and metabolic diseases, including heart failure, myocardial infarction, cerebrovascular accidents, and non-alcoholic fatty liver disease.19–24 Although preliminary studies have explored the prognostic significance of single composite inflammatory markers for AF recurrence, direct comparative analyses of multiple composite inflammatory markers are still lacking in the current academic literature.
This research seeks to examine and contrast the relationships between multiple composite inflammatory biomarkers—namely SII, NLR, PLR, LMR, NPR, SIRI, PAR, PIV, and HALP—and the likelihood of AF recurrence after CA. The objective is to provide new understanding that may contribute to minimizing AF recurrence in this patient cohort, ultimately guiding clinical management approaches.
Materials and Methods
Study Design and Participants
This study was conducted at the Department of Cardiovascular Medicine, the Second Affiliated Hospital of Xi’an Jiaotong University, and represents a retrospective analysis of a prospectively maintained database. The study was performed in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of the Second Affiliated Hospital of Xi’an Jiaotong University (Approval No. G-2023036). This report was developed in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement, as well as its extension for research utilizing routinely collected health data, namely the REporting of studies Conducted using Observational Routinely-collected Data (RECORD) guidelines.25 Written informed consent was obtained from each patient. In cases where the patient was illiterate or incapacitated, the written informed consent was provided and signed by an immediate family member.
Inclusion Criteria: The study population includes patients aged 18 years and older who were diagnosed with AF based on ICD-9 or ICD-10 codes. These patients underwent their first catheter-based radiofrequency ablation treatment between October 2017 and July 2024 (HF: ICD-10-CM: I48.x; CA: ICD-9-CM: 37.34).26 All participants received circumferential pulmonary vein isolation (CPVI) as a standard treatment. Additional ablation procedures beyond pulmonary vein isolation(PVI), including linear ablation, substrate modification, or ablation targeting non-pulmonary vein triggers, were conducted based on the clinical judgment of the operating physician.
Exclusion Criteria: The exclusion criteria for this study included the following: (1) presence of comorbid rheumatic heart disease or valvular heart disease; (2) severe hepatic or renal impairment; (3) lack of essential baseline data; and (4) inability to complete the 12-month follow-up period. Ultimately, a total of 744 patients were incorporated into the final analysis. Patients who were lost to follow-up before 12 months without experiencing recurrence were censored. (Figure 1).
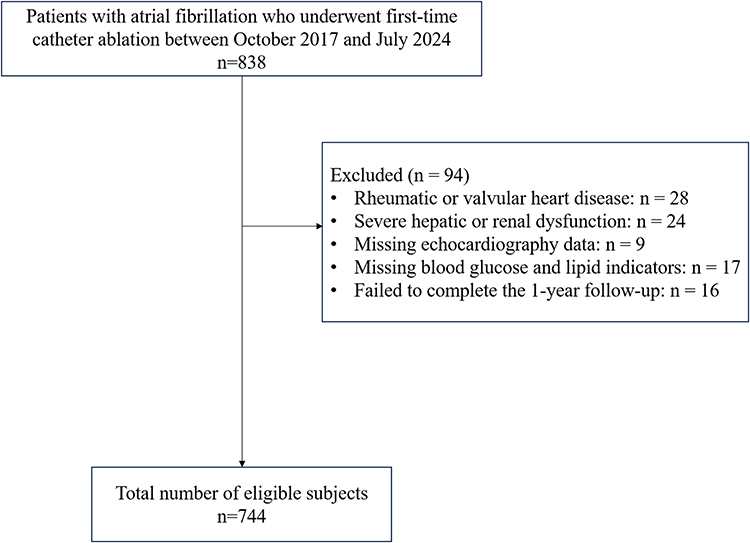 |
Figure 1 Flow chart of our research. |
All clinical and laboratory information was retrieved from the electronic medical record system. Baseline characteristics, medical histories, and results of auxiliary examinations were collected for all participants included in the study. Data extraction was performed by a computer technician who remained blinded to the study hypothesis. Subsequently, the extracted data underwent verification by an independent clinician, also blinded to the study hypothesis, to ensure accuracy. In compliance with relevant data protection regulations, all patient-related information was provided exclusively in a de-identified format.
Ablation Procedure and Postablation Management Strategy
All ablation procedures were conducted under the guidance of either the EnSite system (St. Jude Medical, St. Paul, MN) or the Carto 3 system (Biosense Webster, Inc., Irvine, CA). All patients underwent CPVI. Additional ablation beyond PVI was carried out at the discretion of the operating physician. The procedural endpoint was defined as the successful achievement of electrical PVI; in cases where linear ablation was performed, an additional endpoint of bidirectional conduction block across the linear lesion was required. All interventions were executed by a team of experienced cardiac electrophysiologists. Postprocedural management and follow-up were subsequently conducted. An echocardiogram was performed immediately after ablation for each patient to rule out cardiac tamponade. All patients who underwent radiofrequency CA were routinely administered oral antiarrhythmic drugs for 3 months and oral anticoagulants for at least 2 months post-procedure. At the third-month follow-up, the decision regarding long-term oral anticoagulation therapy was based on the patient’s CHA2DS2-VASc score.
All patients received standard 12-lead electrocardiograms and 24-hour Holter monitoring at 3, 6, 9, and 12 months post-procedure. When considered clinically appropriate by the outpatient physician, transthoracic echocardiography and supplementary diagnostic assessments were performed. Additionally, electrocardiograms and 24-hour Holter monitoring were administered whenever patients presented with palpitations outside the scheduled evaluations. Subsequent follow-up appointments were arranged at six-month intervals.
Definition of Composite Inflammatory Indices
In this study, all inflammatory markers were calculated based on parameters from peripheral blood samples. All parameters were collected prior to CA and included neutrophil count (×109/L), lymphocyte count (×109/L), monocyte count (×109/L), platelet count (×109/L), hemoglobin level (g/L), and albumin level (g/L). The specific calculation formulas for each marker are as follows:
SII = platelet count × neutrophil count/lymphocyte count; NLR = neutrophil count/lymphocyte count; PLR = platelet count/lymphocyte count; LMR = lymphocyte count/monocyte count; NPR = neutrophil count/platelet count; SIRI = neutrophil count × monocyte count/lymphocyte count; PAR = platelet count/albumin; PIV = neutrophil count × monocyte count × platelet count/lymphocyte count; HALP = (hemoglobin × albumin × lymphocyte count)/platelet count.
Definition of the Endpoint
AF recurrence was defined as an episode of atrial arrhythmia (AF, atrial flutter, or atrial tachycardia) lasting for >30 seconds after a 3- month blanking period.
Statistical Analysis
A stratified analysis of baseline characteristics was performed according to the presence or absence of AF recurrence. Continuous variables are presented as means ± standard deviations (SD), whereas categorical variables are expressed as counts and percentages (n, %). Comparisons of continuous variables between groups were conducted using either the two-sample t-test or the Mann–Whitney U-test, contingent upon the distribution of the data. Categorical variables were compared using the Pearson chi-square test. Survival distributions were estimated via the Kaplan-Meier method, with group differences evaluated for statistical significance using the Log rank test.
The prognostic value of composite inflammatory indices was examined through multivariable Cox proportional hazards regression models. Three progressively adjusted models were constructed: Model 1 adjusted for sex, age, and body mass index (BMI); Model 2 included the covariates from Model 1 plus AF type, HF status, AF duration, and the CHA2DS2-VASc score; Model 3 further incorporated triglyceride levels, high-density lipoprotein, left ventricular ejection fraction (LVEF), and left atrial diameter (LAD) in addition to the variables in Model 2. To explore the relationship between composite inflammatory indices and AF recurrence, restricted cubic spline (RCS) analyses were performed, controlling for relevant confounders. Upon identification of a non-linear association, the inflection point with the highest likelihood was determined, and a two-piecewise Cox proportional hazards model was applied to assess the relationship on either side of this threshold.
Receiver operating characteristic (ROC) curve analyses were conducted to compare the predictive performance of SII, NLR, NPR, SIRI, and PIV with respect to AF recurrence. Areas under the curve (AUC) were compared, and the optimal cutoff value was identified for the inflammatory marker demonstrating the highest predictive accuracy. Based on this cutoff, continuous variables were dichotomized. Kaplan-Meier survival analyses were subsequently performed to evaluate the association between categorized inflammatory markers and AF recurrence.
The robustness of the findings was confirmed through multiple sensitivity analyses. Initially, the risk of AF recurrence during follow-up was assessed across subgroups stratified by sex, age (≥65 vs. <65 years), BMI (≥24 vs. <24), AF type, AF duration (≥12 vs. <12 months), LVEF (≥0.5 vs. <0.5), and LAD (≥35 vs. <35 mm). Thereafter, primary analyses were repeated following imputation of missing data—constituting less than 10% of the dataset—using the random forest imputation method. Prior to these analyses, the proportional hazards assumption was evaluated through visual inspection of Schoenfeld residuals. Multicollinearity was assessed by calculating variance inflation factors (VIFs), with values exceeding 10 indicating significant multicollinearity; no such issues were observed. All statistical analyses were conducted using SAS version 9.4 (SAS Institute, Cary, NC, USA) and R version 4.3.2 (R Foundation for Statistical Computing, Vienna, Austria). A two-sided p-value of less than 0.05 was considered indicative of statistical significance throughout all analyses.
Results
Participant Baseline Characteristics
This study included 744 patients (62.94 ± 10.96 years old, of whom 469 [63.04%] were male). The average follow-up duration was 17.38 months, with a recurrence rate of 27.69%. Patients experiencing recurrent AF predominantly demonstrated the following characteristics: a higher prevalence among males with persistent AF, extended duration of AF, increased risk of HF, and generally elevated CHA2DS2-VASc scores. Laboratory analyses revealed that these patients exhibited increased white blood cell and neutrophil counts, elevated high-density lipoprotein levels, and LAD, alongside decreased red blood cell and lymphocyte counts, lower triglyceride concentrations, and reduced LVEF. Additionally, significant variations were identified in composite inflammatory markers, with SII, NLR, PLR, NPR, SIRI, PAR, and PIV all elevated, whereas LMR and HALP score were diminished (Table 1).
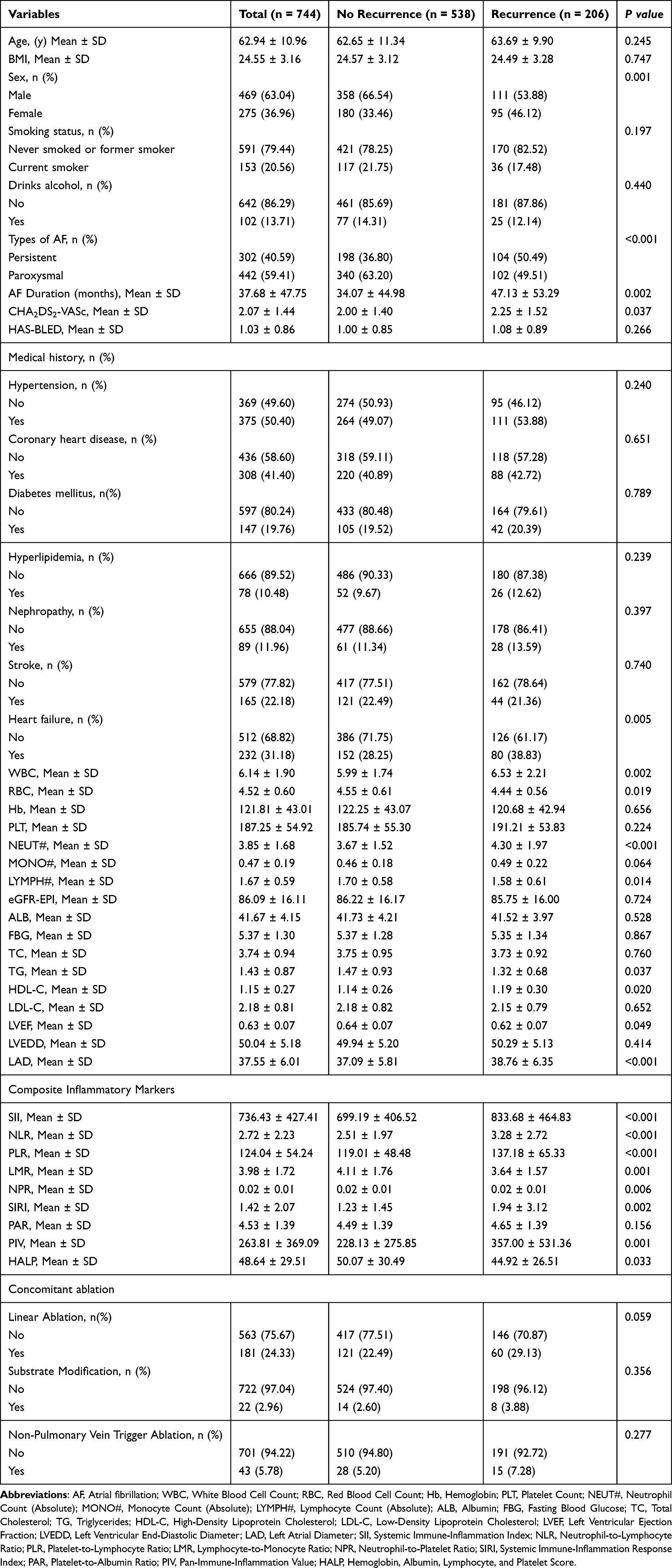 |
Table 1 Baseline Characteristics of the Study Population |
Primary Endpoint
Figure 2 illustrates the Kaplan-Meier survival curves depicting recurrence rates stratified by quartiles of composite inflammatory indices. The analysis revealed that patients exhibiting elevated levels of the SII, NLR, NPR, SIRI, and PIV experienced significantly increased recurrence rates relative to those with lower levels (Log rank test, P < 0.05). Conversely, the LMR, PAR, and HALP score did not demonstrate a statistically significant association with recurrence rates (Log rank test, P > 0.05).
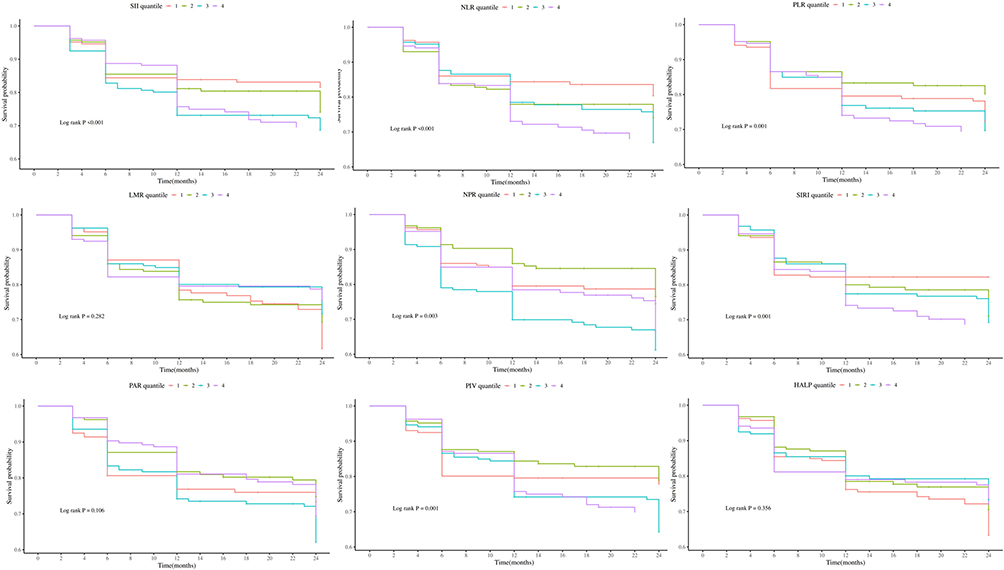 |
Figure 2 Kaplan–Meier curves stratified by Composite Inflammatory Markers. |
Table 2 presents three multivariate Cox proportional hazards models analyzing the association between composite inflammatory indices and post-ablation recurrence. In the fully adjusted Model 3, per 1SD increase in each index, the risk of recurrence was significantly elevated by 17% (HR=1.17; 95% CI: 1.05–1.30; P=0.004) for the SII, 12% (HR=1.12; 95% CI: 1.01–1.24; P=0.026) for the NLR, 16% (HR=1.16; 95% CI: 1.03–1.31; P=0.012) for the PLR, 13% (HR=1.13; 95% CI: 1.01–1.27; P=0.042) for the NPR, 13% (HR=1.13; 95% CI: 1.03–1.24; P=0.009) for the SIRI, and 15% (HR=1.15; 95% CI: 1.04–1.26; P=0.005) for the PIV. A per 1SD increase in the LMR was associated with a statistically significant 15% reduction in the risk of recurrence (HR = 0.85; 95% CI: 0.73–0.99; P = 0.044). To further clarify the association between composite inflammatory indices and AF recurrence, they were analyzed by quartile groups. The results revealed that patients with higher levels of the SII, NLR, SIRI, and PIV had a significantly increased risk of recurrence. In the fully adjusted model, the HRs and 95% CIs for Q4 VS Q1 were 1.88 (1.23–2.88, P=0.004) for SII, 1.85 (1.21–2.84, P=0.005) for NLR, 2.03 (1.31–3.14, P=0.002) for SIRI, and 1.58 (1.06–2.38, P=0.026) for PIV, demonstrating a significant increasing trend in recurrence risk with rising index levels. For the NPR, Q3 showed a significantly higher recurrence risk compared to Q1 (HR=1.58; 95% CI: 1.07–2.32; P=0.021) in the fully adjusted model.RCS regression models demonstrated nonlinear correlations of SII and NLR with post-ablation recurrence (all P for nonlinearity <0.05), whereas SIRI, NPR, and PIV showed linear correlations with recurrence (all P for nonlinearity >0.05) (Figure 3).
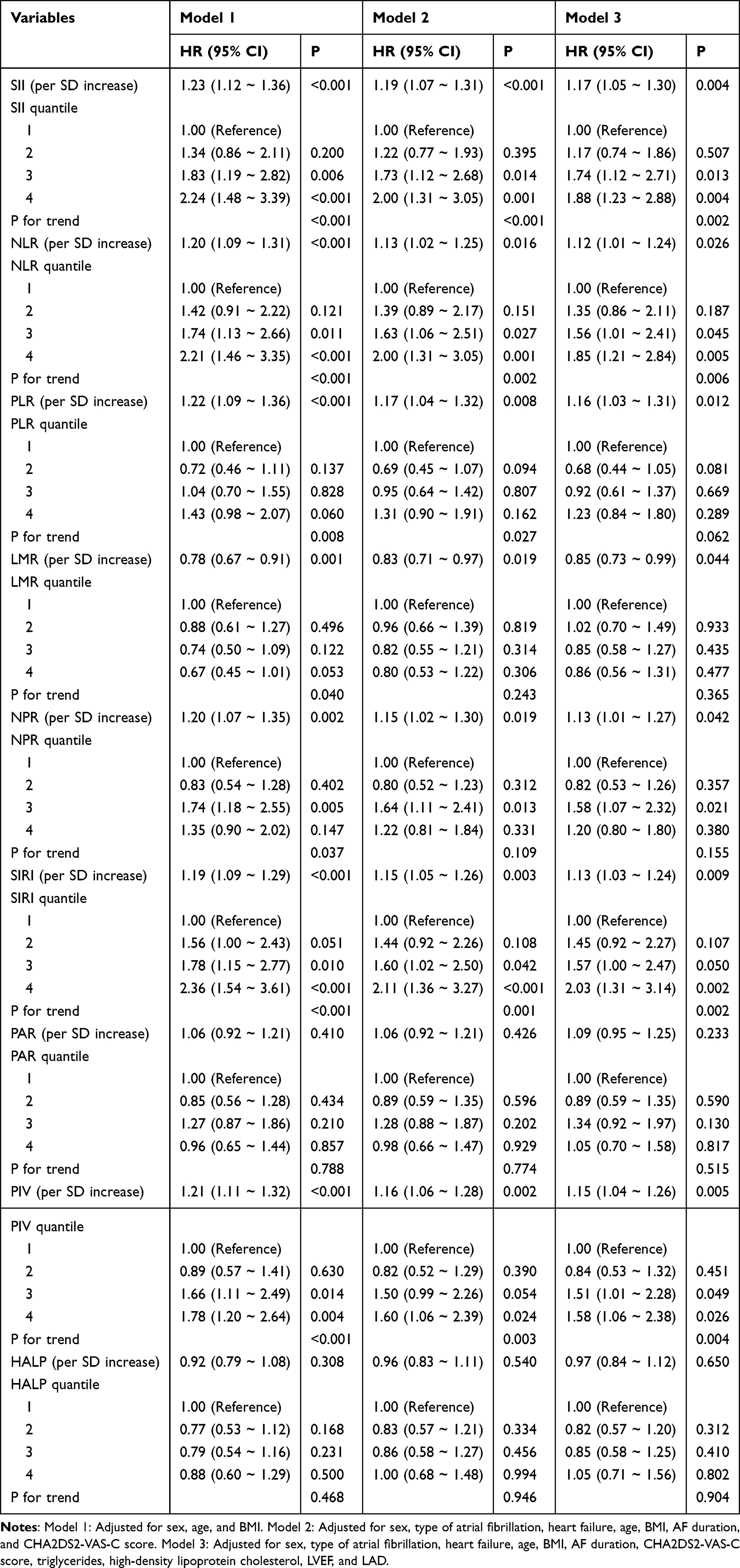 |
Table 2 Association Between Composite Inflammatory Markers and Atrial Fibrillation Recurrence |
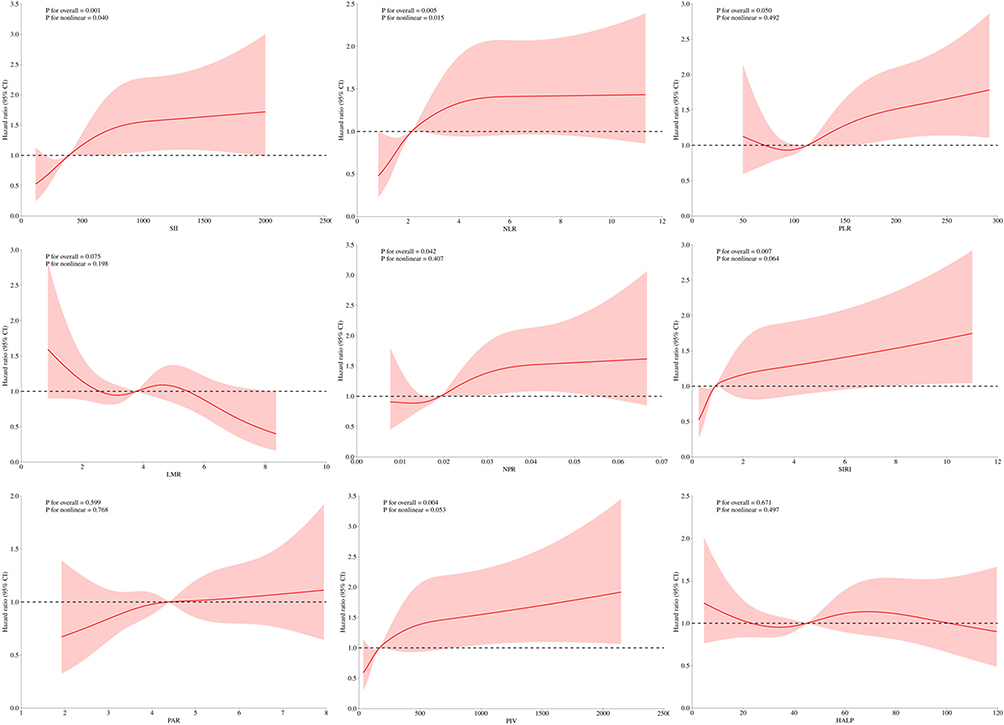 |
Figure 3 Association between composite inflammatory indices and AF recurrence. The solid line and the shaded red area represent the estimated values and their corresponding 95% CIs, respectively. Adjusted for sex, type of atrial fibrillation, heart failure, age, BMI, AF duration, CHA2DS2-VAS-C score, triglycerides, high-density lipoprotein cholesterol, LVEF, and LAD. |
The association between SII, NLR, and AF recurrence was fitted using a 2-piece Cox proportional hazards regression model. The inflection points were identified at 524.75 for SII and 2.63 for NLR.A threshold effect was observed in the association between SII and AF recurrence (P for likelihood test = 0.036). Overall, a positive association was found between SII and recurrence [HR (95% CI): 2.57 (1.24–5.33)]. When SII was below 524.75, a positive association was observed [HR (95% CI): 1.08 (0.89–1.30)]. No significant association was found when SII exceeded 524.75. Similarly, a threshold effect was present in the association between NLR and AF recurrence (P for likelihood test = 0.015). Overall, NLR showed a positive association with recurrence [HR (95% CI): 1.05 (1.01–1.10)]. When NLR was below 2.63, a positive association was observed [HR (95% CI): 1.60 (1.05–2.43)]. No significant association was found when NLR exceeded 2.63 (Supplementary Table 1).
ROC curves were constructed for SII, NLR, NPR, SIRI, and PIV to evaluate their prognostic value for AF recurrence. The analysis results showed that NLR achieved the largest area under the curve value compared to other inflammatory markers [AUC (95% CI): 0.62 (0.57–0.66)] (Figure 4, Supplementary Table 2).
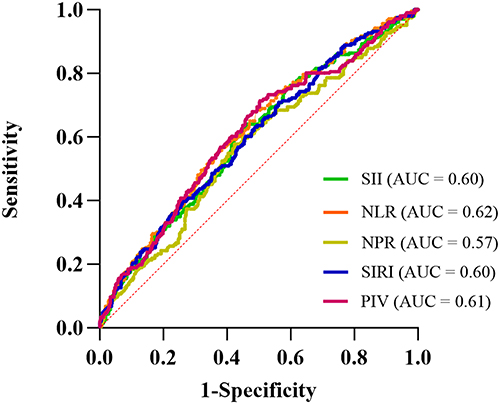 |
Figure 4 ROC curve analysis of Composite Inflammatory Markers for predicting AF recurrence. |
The optimal cutoff value of NLR for predicting AF recurrence was determined to be 2.032. Based on this cutoff, patients were stratified into high-NLR (≥2.032) and low-NLR (<2.032) groups. Kaplan-Meier survival analysis demonstrated that patients in the high-NLR group had a significantly elevated risk of AF recurrence (log-rank P <0.001) (Figure 5).
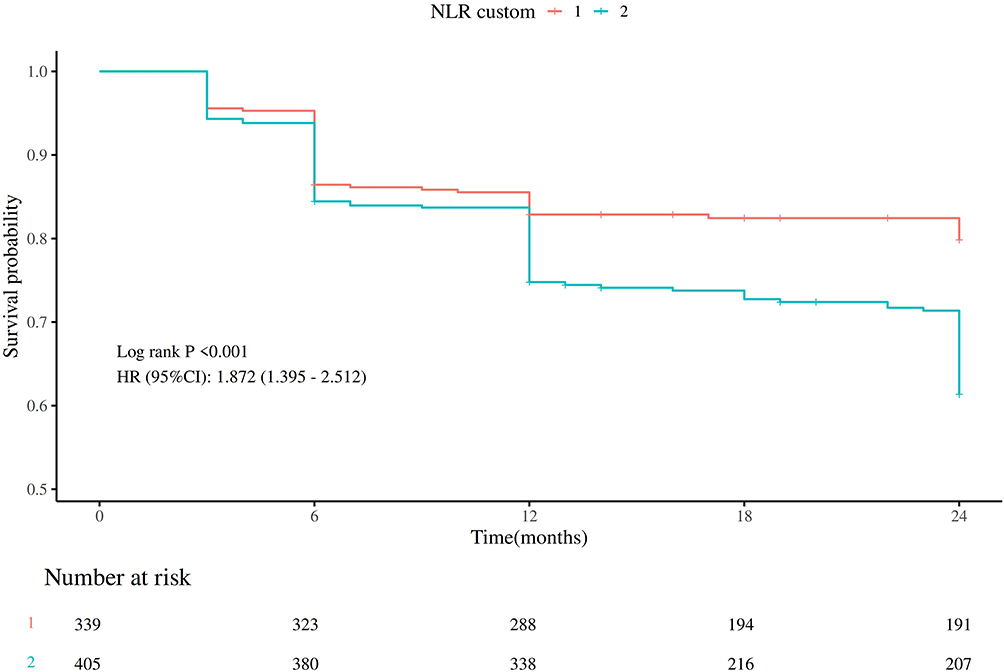 |
Figure 5 Kaplan-Meier Survival Curves for AF Recurrence Stratified by the Optimal NLR Cutoff Value. |
Sensitivity Analyses
The results remained robust in two sensitivity analyses. First, we assessed the risk of AF recurrence during follow-up across various subgroups stratified by sex, age, BMI, AF type, AF duration, LVEF, and LAD levels (Supplementary Figure 1). Elevated levels of SII, NLR, NPR, SIRI, and PIV were consistently associated with an increased risk of AF recurrence in most subgroups, with no significant interaction observed (P for interaction >0.05). Second, repeating the primary analysis after imputing missing values using the random forest method yielded consistent results (Supplementary Table 3).
Discussion
This is the first large-scale cohort study to compare the associations between multiple composite inflammatory markers and the risk of AF recurrence after CA. The results show that elevated levels of the SII, NLR, SIRI, PIV, and NPR are linked to greater risk of AF recurrence. The NLR had superior predictive ability compared to the other indices. These findings held up across subgroup analyses. Overall, our results highlight the potential role of systemic inflammation measured by blood tests in AF recurrence. They also provide important evidence that supports the predictive value of inflammatory markers for estimating AF recurrence risk after CA.
Previous research has demonstrated that composite inflammatory markers obtained from peripheral blood tests are closely correlated with the incidence and adverse prognosis of cardiovascular diseases (CVD).19–24 Extensive research has established the essential role of inflammatory mechanisms in the development and progression of CVD. Increasing clinical and experimental data indicate that AF is associated with oxidative stress and inflammation, where oxidative damage and inflammatory processes in the atria of AF patients contribute to changes in atrial structure and electrical function remodeling.27 Increased levels of biomarkers indicative of oxidative stress and inflammation have been observed in patients with AF.28 Numerous prior studies have explored the value of single inflammatory markers, such as high-sensitivity C-reactive protein (hs-CRP) and interleukin (IL)-6, in the context of AF.29 Nonetheless, research investigating the relationship between novel composite inflammatory indices and the risk of AF recurrence remains scarce, potentially due to difficulties associated with longitudinal follow-up for AF recurrence. Among these composite inflammatory markers, SII and NLR have been the most thoroughly examined. A prospective cohort study encompassing 423,701 participants revealed positive associations between NLR, PLR, SII, and SIRI with the incidence of cardiovascular events, findings that align with the results of the present study.30 Scholars such as Yi Luo et al31 suggested that elevated levels of NLR and SIRI are associated with a higher risk of developing AF. An additional retrospective cohort study concentrating on female subjects demonstrated that both NLR and SIRI were significantly associated with all-cause mortality and CVD mortality among postmenopausal women diagnosed with osteoporosis or osteopenia.32 A meta-analysis also explained the association between elevated levels of NLR, SII, and SIRI and an increased risk of mortality in HF patients.33 A study conducted by Rohan Magoon and colleagues demonstrated that the albumin-adjusted platelet-white cell index is correlated with the incidence of new-onset AF following coronary artery bypass grafting.34
It is important to highlight that, although the majority of composite inflammatory markers demonstrated significant predictive value, the notably superior predictive accuracy of NLR identified in this study represents a critical finding. This superiority can be attributed to the roles of neutrophils and lymphocytes as principal effector cells within the innate and adaptive immune systems, respectively. Consequently, the NLR provides a dynamic and sensitive reflection of systemic inflammatory status. Derived from routine complete blood count parameters, the NLR is characterized by high stability, widespread availability, and cost-effectiveness, which collectively reduce analytical variability. In contrast, inflammatory indices that incorporate platelet counts—such as SII, PIV, and NPR—may be subject to confounding influences from non-inflammatory factors. For example, the administration of anticoagulants in AF management to prevent intracardiac thrombosis may introduce additional confounding variables affecting these indices.35 The elevated AUC value, along with the independent association of NLR observed in multivariate analyses, collectively indicate its enhanced discriminatory capacity. This finding implies that the NLR index specifically represents the fundamental inflammatory burden that is closely implicated in the pathogenesis of AF. In this study, SII and NLR demonstrated a significant non-linear association with the risk of AF recurrence after CA, whereas SIRI, NPR, and PIV exhibited linear associations. This suggests distinct patterns in how different inflammatory indices influence the risk of AF recurrence. Both SII and NLR incorporate the neutrophil-to-lymphocyte ratio, enabling them to sensitively reflect the critical balance between pro-inflammatory and anti-inflammatory states.36 Within the low-to-moderate elevation range, inflammatory levels correlate in a graded manner with atrial remodeling and the response to post-ablation injury; however, once a certain threshold is exceeded, the impact of inflammation on prognosis enters a plateau or saturation phase, thus exhibiting typical non-linear characteristics.37 This non-linear relationship aligns more closely with the pathophysiological concept of an “inflammatory threshold effect” in AF recurrence. In contrast, SIRI, NPR, and PIV did not show significant non-linearity, indicating that within this study population, their association with recurrence risk approximates a dose-dependent, linear increasing relationship. These markers tend to reflect the proportions or composite counts of immune cell subsets and are less capable of capturing the “pro-inflammatory/anti-inflammatory critical point”, making them more suitable for use as continuous risk markers. Notably, despite the superior predictive performance of NLR over other composite inflammatory markers in this study, its single-index AUC is not ideal, and we recommend incorporating NLR into the currently established mature prediction models for AF recurrence to enhance the overall predictive capacity of the models.
Accumulating evidence substantiates the role of inflammation in the pathogenesis of AF. The initial hypothesis regarding the relationship between inflammation and AF was introduced by P. Bruins and colleagues,38 who observed frequent AF episodes following coronary artery bypass grafting. Subsequent investigations have detected circulating autoantibodies directed against myosin heavy chains in a substantial subset of patients with idiopathic paroxysmal AF, indicating a possible role of autoimmune mechanisms in the pathogenesis of certain cases of paroxysmal AF.39 The pathophysiological mechanisms underlyingAF recurrence following CA are multifaceted, encompassing elements such as residual pre-existing substrates, myocardial and electrical remodeling subsequent to ablation, dysfunction of the autonomic nervous system, and the continued presence of contributing risk factors.40,41 Underlying mechanisms include oxidative stress, cell death, fibrosis, endothelial dysfunction, and platelet activation.42 Inflammation observed in patients with AF may arise from multiple origins, given that numerous underlying conditions, including hypertension and obesity, are linked to a chronic low-grade inflammatory state characterized by increased concentrations of pro-inflammatory cytokines.43,44 CA itself may also induce inflammation. An observational study demonstrated that elevated postoperative CRP levels were correlated with a heightened risk of AF. Additionally, several inflammatory cytokines have been shown to influence ion channel function and calcium homeostasis.45 For example, tumor necrosis factor (TNF) has the capacity to directly modulate calcium handling mechanisms within cardiomyocytes, a process that is pivotal in the onset of AF and the associated atrial electrical remodeling.36 Furthermore,TNF has the capacity to activate the transforming growth factor-beta (TGF-β) signaling pathway and stimulate fibroblast activity. Concurrently, it enhances the secretion of matrix metalloproteinase-2 (MMP-2) and matrix metalloproteinase-9 (MMP-9), collectively facilitating the process of atrial remodeling.46 Extensive experimental data demonstrate that pro-inflammatory cytokines can directly disrupt the function of multiple ion channels in ventricular cardiomyocytes, resulting in an extended action potential duration and QT interval. Additionally, systemic changes triggered by inflammatory cytokines produce considerable indirect impacts on cardiac function.47,48 Inflammation may induce hyperactivation of the cardiac sympathetic nervous system, consequently intensifying the prolongation of cardiomyocyte action potential duration and promoting calcium overload.49 Variations in body temperature can induce modifications in the biophysical characteristics of myocardial ion channels.50,51 Moreover, inflammatory processes have the potential to suppress hepatic cytochrome P450 (CYP450) enzyme activity, thereby altering drug metabolism and resulting in the accumulation of medications that prolong the QT interval within the circulatory system.52,53 At present, there are no pharmacological agents specifically designed to target inflammatory pathways in patients with AF. While medications including angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, and statins have been evaluated in prospective clinical trials, the outcomes have been largely unsatisfactory.54 A recent randomized, placebo-controlled study investigating the efficacy of colchicine in preventing AF recurrence following CA produced comparably unfavorable outcomes. Specifically, a 10-day course of colchicine administration post-CA did not result in a reduction in the recurrence rate of atrial arrhythmias, nor did it lower the incidence of composite clinical endpoints associated with AF.55 However, colchicine did alleviate post-ablation chest pain symptoms consistent with pericarditis, while simultaneously increasing the incidence of diarrhea. Additionally, several studies have suggested that diabetic patients treated with SGLT2i following AF ablation exhibit a reduced risk of AF recurrence. Moreover, individuals presenting with elevated BMI, persistent AF, and prolonged AF duration seem to derive greater therapeutic benefit from SGLT2i treatment post-ablation.56 This advantage may be attributed to the effects of SGLT2 inhibitors in promoting glycosuria and natriuresis, which in turn may alleviate atrial structural remodeling.57
This study presents several limitations. First, this study was conducted at a single center and involved a relatively small number of endpoint events. It is a retrospective analysis of a prospectively maintained database. The analysis was based on a single blood sample measurement, thereby not capturing temporal variations in composite inflammatory indices. Furthermore, the absence of a standardized protocol for detecting arrhythmia recurrence, such as the use of implantable loop recorders, may have resulted in an underestimation of AF recurrence rates. The study population was restricted to patients with non-valvular AF, which limits the generalizability of the findings to broader AF cohorts. Additionally, potential confounding variables, including dietary patterns and physical activity levels, were not measured and may have introduced bias. To overcome these limitations, future research should involve high-quality, prospective, multicenter studies that incorporate longitudinal assessments of composite inflammatory indices alongside other pertinent factors to more robustly evaluate their predictive utility for AF recurrence following CA.
Conclusion
The SII, NLR, NPR, SIRI, and PIV are independent predictors of recurrence in patients with AF after CA, and the predictive value of each index demonstrates robustness in subgroup analyses, with NLR exhibiting relatively superior predictive efficacy compared to the other indicators. NLR shows a non-linear relationship with AF recurrence following CA, with a threshold of 2.63. The findings of this study suggest that incorporating composite inflammatory indices, particularly NLR, into clinical practice could optimize risk stratification for patients with AF and provide a basis for developing personalized management strategies for those undergoing CA. Further research is needed to validate its robustness, further elucidate the underlying mechanisms, and develop therapeutic interventions targeting inflammation to improve outcomes in this population.
Abbreviations
AF, Atrial fibrillation; HALP, Hemoglobin, Albumin, Lymphocyte, and Platelet Score; LMR, Lymphocyte-to-Monocyte Ratio; NLR, Neutrophil-to-Lymphocyte Ratio; NPR, Neutrophil-to-Platelet Ratio; PAR, Platelet-to-Albumin Ratio; PIV, Pan-Immune-Inflammation Value; PLR, Platelet-to-Lymphocyte Ratio; SII, Systemic Immune-Inflammation Index; SIRI, Systemic Immune-Inflammation Response Index.
Data Sharing Statement
Data supporting the findings of this study are available from the corresponding author upon reasonable request.
Ethical Guidelines Statement
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of the Second Affiliated Hospital of Xi’an Jiaotong University (Approval No. G-2023036). In compliance with applicable data protection regulations, patient-related data were provided solely in a de-identified format. This report was developed in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement, as well as its extension for research utilizing routinely collected health data, namely the REporting of studies Conducted using Observational Routinely-collected Data (RECORD) guidelines. Written informed consent was obtained from each patient. In cases where the patient was illiterate or incapacitated, the written informed consent was provided and signed by an immediate family member.
Acknowledgments
We would like to express our sincere gratitude to Professor Chunhong Luan for her dedicated work in patient follow-up. The authors gratefully acknowledge the computer technician for the extraction of electronic medical record information for this study.
Author Contributions
Tengfei Ji (Conceptualization, Writing – Original Draft, Data Curation, Investigation); Yide Yuan (Writing – Original Draft, Data Curation, Formal Analysis, Methodology); Mei Du (Software, Supervision, Methodology); Su Liu (Supervision, Investigation); Jia Wei (Validation); Chunhong Luan (Writing – Review & Editing, Investigation); and Jiahong Xue (Writing – Review & Editing, Funding Acquisition, Conceptualization, Software, Data Curation).
All authors took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Key Research and Development Program of Shaanxi Province (S2024-YF-YBSF-0667) and the National Natural Science Foundation of China (No. 82360608).
Disclosure
The authors have no conflicts of interest to disclose.
References
1. Zhang J, Johnsen SP, Guo Y, Lip GYH. Epidemiology of atrial fibrillation: geographic/ecological risk factors, age, sex, genetics. Cardiac Electrophysiol Clin. 2021;13(1):1–16. doi:10.1016/j.ccep.2020.10.010
2. Chugh SS, Havmoeller R, Narayanan K, et al. Worldwide epidemiology of atrial fibrillation: a global burden of disease 2010 study. Circulation. 2014;129(8):837–847. doi:10.1161/CIRCULATIONAHA.113.005119
3. Hindricks G, Potpara T, Dagres N, et al. 2020 ESC guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European association for cardio-thoracic surgery (EACTS): the task force for the diagnosis and management of atrial fibrillation of the European society of cardiology (ESC) developed with the special contribution of the European heart rhythm association (EHRA) of the ESC. Euro Heart J. 2010;42(5):373–498. doi:10.1093/eurheartj/ehaa612
4. Aune D, Mahamat-Saleh Y, Kobeissi E, Feng T, Heath AK, Janszky I. Blood pressure, hypertension and the risk of atrial fibrillation: a systematic review and meta-analysis of cohort studies. Euro J Epidemiol. 2023;38(2):145–178. doi:10.1007/s10654-022-00914-0
5. Pistoia F, Sacco S, Degan D, Tiseo C, Ornello R, Carolei A. Hypertension and stroke: epidemiological aspects and clinical evaluation. High Blood Pressure Cardiovascu Prev. 2016;23(1):9–18. doi:10.1007/s40292-015-0115-2
6. Packer DL, Mark DB, Robb RA, et al; CABANA Investigators. Effect of catheter ablation vs antiarrhythmic drug therapy on mortality, stroke, bleeding, and cardiac arrest among patients with atrial fibrillation: the CABANA randomized clinical trial. JAMA. 2019;321(13):1261–1274. doi:10.1001/jama.2019.0693
7. Mark DB, Anstrom KJ, Sheng S, et al. Effect of catheter ablation vs medical therapy on quality of life among patients with atrial fibrillation: the CABANA randomized clinical Trial. JAMA. 2019;321(13):1275–1285.2019. doi:10.1001/jama.2019.0692
8. Kuck KH, Brugada J, Fürnkranz A, et al. Cryoballoon or radiofrequency ablation for paroxysmal atrial fibrillation. New England J Med. 2016;374(23):2235–2245. doi:10.1056/NEJMoa1602014
9. Richter B, Gwechenberger M, Socas A, et al. Markers of oxidative stress after ablation of atrial fibrillation are associated with inflammation, delivered radiofrequency energy and early recurrence of atrial fibrillation. Clin Res Cardiol. 2012;101(3):217–225. doi:10.1007/s00392-011-0383-3
10. Koyama T, Sekiguchi Y, Tada H, et al. Comparison of characteristics and significance of immediate versus early versus no recurrence of atrial fibrillation after catheter ablation. Ame J Cardiol. 2009;103(9):1249–1254. doi:10.1016/j.amjcard.2009.01.010
11. Lim HS, Schultz C, Dang J, et al. Time course of inflammation, myocardial injury, and prothrombotic response after radiofrequency catheter ablation for atrial fibrillation. Circulation. 2014;7(1):83–89. doi:10.1161/CIRCEP.113.000876
12. Wang YJ, Liu KS, Meng XJ, et al. Role of a new inflammation predictor in predicting recurrence of atrial fibrillation after radiofrequency catheter ablation. World J Cardiol. 2024;16(12):740–750. doi:10.4330/wjc.v16.i12.740
13. Adamo M, Gardner RS, McDonagh TA, et al. The ‘ten commandments’ of the 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2022;43(6):440–441. doi:10.1093/eurheartj/ehab853
14. Wada H, Dohi T, Miyauchi K, et al. Neutrophil to lymphocyte ratio and long-term cardiovascular outcomes in coronary artery disease patients with low high-sensitivity C-reactive protein level. Int Heart J. 2020;61(3):447–453. doi:10.1536/ihj.19-543
15. Hu B, Yang XR, Xu Y, et al. Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma. Clin Cancer Res. 2014;20(23):6212–6222. doi:10.1158/1078-0432.CCR-14-0442
16. Zhang Z, Li S, Tu T, et al. Nonlinear relationship and predictive value of systemic immune-inflammation index for atrial fibrillation recurrence after catheter ablation in hypertensive patients. Heart Rhythm. 2025;22(9):2257–2268. doi:10.1016/j.hrthm.2025.03.1958
17. Zhao Z, Jiang B, Zhang F, et al. Association between the systemic immune-inflammation index and outcomes among atrial fibrillation patients with diabetes undergoing radiofrequency catheter ablation. Clin Cardiol. 2023;46(11):1426–1433. doi:10.1002/clc.24116
18. Guo X, Zhang S, Yan X, et al. Postablation neutrophil/lymphocyte ratio correlates with arrhythmia recurrence after catheter ablation of lone atrial fibrillation. Chin Med J. 2014;127(6):1033–1038.
19. Zhao Y, Shao W, Zhu Q, et al. Association between systemic immune-inflammation index and metabolic syndrome and its components: results from the national health and nutrition examination survey 2011-2016. J Transl Med. 2023;21(1):691. doi:10.1186/s12967-023-04491-y
20. Emgin Ö, Kılıç ER, Taşkıran İ, Haftacı E, Ata A, Yılmaz M. Systemic inflammation index (SII) as a predictor of mortality in intensive care units. Biomedicines. 2015;13(7):1669. doi:10.3390/biomedicines13071669
21. Lattanzi S, Brigo F, Trinka E, et al. Neutrophil-to-lymphocyte ratio in acute cerebral hemorrhage: a system review. Transl Stroke Res. 2019;10(2):137–145. doi:10.1007/s12975-018-0649-4
22. Balta S, Ozturk C. The platelet-lymphocyte ratio: a simple, inexpensive and rapid prognostic marker for cardiovascular events. Platelets. 2015;26(7):680–681. doi:10.3109/09537104.2014.979340
23. Tan S, Yang X, Mu X, et al. The predictive role of peripheral serum inflammatory markers NLR, PLR, and LMR in ulcerative colitis and Crohn’s disease: a systematic review and meta-analysis. Front Immunol. 2025;16:1623899. doi:10.3389/fimmu.2025.1623899
24. Xia Y, Xia C, Wu L, Li Z, Li H, Zhang J. systemic immune inflammation index (SII), system inflammation response index (SIRI) and risk of all-cause mortality and cardiovascular mortality: a 20-year follow-up cohort study of 42,875 US adults. J Clin Med. 2023;12(3):1128. doi:10.3390/jcm12031128
25. Benchimol EI, Smeeth L, Guttmann A, et al. The reporting of studies conducted using observational routinely-collected health data (RECORD) statement. PLoS Med. 2015;12(10):e1001885. doi:10.1371/journal.pmed.1001885
26. Hernandez-Ibarburu G, Perez-Rey D, Alonso-Oset E, et al. ICD-10-CM extension with ICD-9 diagnosis codes to support integrated access to clinical legacy data. Int J Med Informat. 2019;129:189–197. doi:10.1016/j.ijmedinf.2019.06.010
27. Huang CX, Liu Y, Xia WF, Tang YH, Huang H. Oxidative stress: a possible pathogenesis of atrial fibrillation. Med Hypotheses. 2009;72(4):466–467. doi:10.1016/j.mehy.2008.08.031
28. Boos CJ, Anderson RA, Lip GY. Is atrial fibrillation an inflammatory disorder? Euro Heart J. 2006;27(2):136–149. doi:10.1093/eurheartj/ehi645
29. Korantzopoulos P, Kolettis TM, Kolettis TM, Kountouris E, et al. Variation of inflammatory indexes after electrical cardioversion of persistent atrial fibrillation. Is there an association with early recurrence rates? Int J Clin Prac. 2005;59(8):881–885. doi:10.1111/j.1368-5031.2005.00569.x
30. Qin P, Ho FK, Celis-Morales CA, Pell JP. Association between systemic inflammation biomarkers and incident cardiovascular disease in 423,701 individuals: evidence from the UK biobank cohort. Cardiovascu Diabetol. 2025;24(1):162. doi:10.1186/s12933-025-02721-9
31. Luo Y, Yang L, Cheng X, Bai Y, Xiao Z. The association between blood count based inflammatory markers and the risk of atrial fibrillation heart failure and cardiovascular mortality. Sci Rep. 2025;15(1):10056. doi:10.1038/s41598-025-94507-y
32. Qu L, Zuo X, Yu J, Duan R, Zhao B. Association of inflammatory markers with all-cause mortality and cardiovascular mortality in postmenopausal women with osteoporosis or osteopenia. BMC Women’s Health. 2023;23(1):487. doi:10.1186/s12905-023-02631-6
33. Vakhshoori M, Nemati S, Sabouhi S, et al. Neutrophil to lymphocyte ratio (NLR) prognostic effects on heart failure; a systematic review and meta-analysis. BMC Cardiovascu Disord. 2023;23(1):555. doi:10.1186/s12872-023-03572-6
34. Magoon R, Shri I, Kashav RC, et al. Atrial fibrillation and perioperative inflammation (FIBRILLAMMED study): a retrospective analysis of the predictive role of preoperative albumin-adjusted platelet-leukocytic indices in OPCABG. Turkish J Anaesthesiol Reanimat. 2023;51(4):331–340. doi:10.4274/TJAR.2023.22995
35. Brundel BJJM, Ai X, Hills MT, et al. Atrial fibrillation. Nat Rev Disease Primers. 2022;8(1):21. doi:10.1038/s41572-022-00347-9
36. Hu YF, Chen YJ, Lin YJ, Chen SA. Inflammation and the pathogenesis of atrial fibrillation. Nat Rev Cardiol. 2015;12(4):230–243. doi:10.1038/nrcardio.2015.2
37. Andrade J, Khairy P, Dobrev D, Nattel S. The clinical profile and pathophysiology of atrial fibrillation: relationships among clinical features, epidemiology, and mechanisms. Circ Res. 2014;114(9):1453–1468. doi:10.1161/CIRCRESAHA.114.303211
38. Bruins P, te Velthuis H, Yazdanbakhsh AP, et al. Activation of the complement system during and after cardiopulmonary bypass surgery: postsurgery activation involves C-reactive protein and is associated with postoperative arrhythmia. Circulation. 1997;96(10):3542–3548. doi:10.1161/01.cir.96.10.3542
39. Maixent JM, Paganelli F, Scaglione J, Lévy S. Antibodies against myosin in sera of patients with idiopathic paroxysmal atrial fibrillation. J Cardiovascu Electrophys. 1998;9(6):612–617. doi:10.1111/j.1540-8167.1998.tb00942.x
40. Olsson A, Gustavsen S, Gisselø Lauridsen K, et al. Neutrophil-to-lymphocyte ratio and CRP as biomarkers in multiple sclerosis: a systematic review. Acta Neurologica Scandinavica. 2021;143(6):577–586. doi:10.1111/ane.13401
41. Mureșan AV, Russu E, Arbănași EM, et al. The predictive value of NLR, MLR, and PLR in the outcome of end-stage kidney disease patients. Biomedicines. 2022;10(6):1272. doi:10.3390/biomedicines10061272
42. Nguyen MN, Kiriazis H, Gao XM, Du XJ. Cardiac fibrosis and arrhythmogenesis. Comprehens Physiol. 2017;7(3):1009–1049. doi:10.1002/cphy.c160046
43. Gregor MF, Hotamisligil GS. Inflammatory mechanisms in obesity. Ann Rev Immunol. 2011;29:415–445. doi:10.1146/annurev-immunol-031210-101322
44. Marzilli M, Merz CN, Boden WE, et al. Obstructive coronary atherosclerosis and ischemic heart disease: an elusive link! J Ame College Cardiol. 2012;60(11):951–956. doi:10.1016/j.jacc.2012.02.082
45. Patti G, Chello M, Candura D, et al. Randomized trial of atorvastatin for reduction of postoperative atrial fibrillation in patients undergoing cardiac surgery: results of the ARMYDA-3 (atorvastatin for reduction of myocardial dysrhythmia after cardiac surgery) study. Circulation. 2006;114(14):1455–1461. doi:10.1161/CIRCULATIONAHA.106.621763
46. Liew R, Khairunnisa K, Gu Y, et al. Role of tumor necrosis factor-α in the pathogenesis of atrial fibrosis and development of an arrhythmogenic substrate. Circulation J. 2013;77(5):1171–1179. doi:10.1253/circj.cj-12-1155
47. Saba S, Janczewski AM, Baker LC, et al. Atrial contractile dysfunction, fibrosis, and arrhythmias in a mouse model of cardiomyopathy secondary to cardiac-specific overexpression of tumor necrosis factor-{alpha}. Ame J Phys. 2005;289(4):H1456–H1467. doi:10.1152/ajpheart.00733.2004
48. Sawaya SE, Rajawat YS, Rami TG, et al. Downregulation of connexin40 and increased prevalence of atrial arrhythmias in transgenic mice with cardiac-restricted overexpression of tumor necrosis factor. Ame J Phys. 2007;292(3):H1561–H1567. doi:10.1152/ajpheart.00285.2006
49. Schwartz PJ. Cardiac sympathetic denervation to prevent life-threatening arrhythmias. Nat Rev Cardiol. 2014;11(6):346–353. doi:10.1038/nrcardio.2014.19
50. Lim SM, Pak HN, Lee MH, Kim SS, Joung B. Fever-induced QTc prolongation and ventricular fibrillation in a healthy young man. Yonsei Med J. 2011;52(6):1025–1027. doi:10.3349/ymj.2011.52.6.1025
51. Zhao Y, Wang T, Guo J, et al. Febrile temperature facilitates hERG/IKr degradation through an altered K(+) dependence. Heart Rhythm. 2016;13(10):2004–2011. doi:10.1016/j.hrthm.2016.06.019
52. Dickmann LJ, Patel SK, Rock DA, Wienkers LC, Slatter JG. Effects of interleukin-6 (IL-6) and an anti-IL-6 monoclonal antibody on drug-metabolizing enzymes in human hepatocyte culture. Drug Metabol Disposition. 2011;39(8):1415–1422. doi:10.1124/dmd.111.038679
53. White CM. Inflammation suppresses patients’ ability to metabolize cytochrome P450 substrate drugs. Ann Pharmacotherapy. 2022;56(7):809–819. doi:10.1177/10600280211047864
54. January CT, Wann LS, Alpert JS, et al. AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American college of cardiology/American heart association task force on practice guidelines and the heart rhythm society. J Ame College Cardiol. 2014;64(21):e1–e76. doi:10.1016/j.jacc.2014.03.022
55. Benz AP, Amit G, Connolly SJ, et al. Colchicine to prevent atrial fibrillation recurrence after catheter ablation: a randomized, placebo-controlled trial. Circul Arrhythmia Electrophysiol. 2024;17(1):e01238. doi:10.1161/CIRCEP.123.012387
56. Zhao Z, Jiang C, He L, et al. Impact of sodium-glucose cotransporter 2 inhibitor on recurrence after catheter ablation for atrial fibrillation in patients with diabetes: a propensity-score matching study and meta-analysis. J Ame Heart Assoc. 2023;12(24):e031269. doi:10.1161/JAHA.123.031269
57. Mazidi M, Rezaie P, Gao HK, Kengne AP. Effect of sodium-glucose cotransport-2 inhibitors on blood pressure in people with type 2 diabetes mellitus: a systematic review and meta-analysis of 43 randomized control trials with 22 528 patients. J Ame Heart Assoc. 2017;6(6):e004007. doi:10.1161/JAHA.116.004007
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.